1. Introduction
Today, cochlear implant (CI) technology is the standard procedure for the treatment of children born deaf or of adults who become deaf during their lives. Therefore, the CI undisputedly represents a major clinical success. The indication also holds great potential for increasingly older people to maintain and improve their quality of life with hearing prostheses. Nevertheless, the results vary from patient to patient. Some patients have no or only very limited improvement in hearing despite a CI. One possible reason for this is the interface between the electrode array and the auditory nerve. The CI uses electrical pulses to stimulate the auditory nerve via an electrode. After implantation of the electrode in the cochlea, connective tissue forms around the electrode array, ranging from a few cells to new bone formation [
1]. This connective tissue impairs signal transmission to the neurons of the auditory nerve, leading to unpredictable stimulus propagation in the cochlea and, thus, to poorer frequency selectivity, which is contrary to a hearing impression that should be as natural as possible for the patient. Measurements of these changes can be obtained by observing changes in impedances [
2].
Impedances increase sharply in the first days after implantation; after about three weeks, they remain stable, and a plateau is formed [
3]. Thus, connective tissue growth should be complete by this time. It is possible to influence the growth of connective tissue by using anti-inflammatory substances [
4]. Less tissue growth should be reflected in impedance measurements in the form of lower impedances compared to untreated groups.
In clinical practice, medications can be applied systemically [
5] and locally [
6] into the inner ear in the context of cochlear implantations. These are mostly anti-inflammatory glucocorticoids such as dexamethasone (DEX), prednisolute, or triamcinolone. Other drug delivery systems take advantage of the permeability of the round window membrane by applying a drug-carrying hydrogel to the round window membrane via the middle ear [
7]. The gel releases the drug and allows it to diffuse through the round window membrane into the inner ear [
8]. However, when administered via the round window membrane, the distribution of substances in the cochlea is very limited [
9].
Several approaches are being explored for direct delivery of compounds into the cochlea [
10]. These include pump-based drug delivery [
11] as well as incorporation of substances into implant coatings [
12,
13] or colonization of the implant surface with drug-releasing cells [
14]. Most of these approaches aim to preserve cochlear neurons (spiral ganglion neurons, SGNs) through the administration of neurotrophic factors. Others, such as the use of pumps, carry an additional infection risk due to the need for permanent access to the cochlea [
15].
In other areas of implant technology, the coating of implant surfaces with drug-containing polymers is already a proven concept for targeted control of implant–tissue interaction. For example, stents are coated with drug-containing polymeric coatings to prevent in-stent restenosis by controlled, long-lasting drug release [
16]. Initial tests have also been carried out on CIs with regard to drug coating. To control and adjust the drug release depending on the site of action, different modifications of the matrix or coating systems can be used [
17]. Particular attention was paid to possible carriers for drugs as coatings for silicone bodies. Poly-L-lactides (PLLAs) have been shown to have no negative effects on the survival of inner ear neurons compared to pure silicone bodies [
18]. In addition, it was reported that a PLLA-coated electrode shows no difference in the generated pressure and friction during insertion compared to an uncoated electrode at higher insertion speeds [
19]. In contrast, possible effects on connective tissue growth have not yet been investigated.
Different substances have inhibitory effects on anti-inflammatory processes. Diclofenac is a drug already approved in human medicine, which is mainly used for musculoskeletal problems. It is a COX-1 and COX-2 inhibitor and has antiphlogistic, analgesic, and antipyretic effects [
20]. Thus far, it has not been used in the inner ear.
In in vitro experiments, diclofenac was shown to be compatible with the SGNs, making it a candidate for use in the inner ear [
21]. A reducing effect on connective tissue growth can be expected [
22]. Similarly, the immunophilin inhibitor MM284, which is a cyclosporine derivate that reduces the recruitment of T cells and macrophages and leads to a reduction in inflammatory processes without affecting the immune system, appeared suitable for application to the ear at concentrations of or below 4 × 10
−5 mol/L [
23].
Both compounds were tested for their tolerability (SGN survival) and efficacy (reduction in connective tissue growth) when released from a PLLA coating on CIs in vivo in this study. Each electrode body contained 5% DEX mixed into the silicone. Previous studies have demonstrated that DEX has anti-inflammatory and immune suppressive functions [
24] and is not toxic for cultured SGNs in concentrations up to 1 × 10
−4 mol/L [
13]. There are already many studies in which DEX has been incorporated in the silicone of the CI electrode in different concentrations [
13,
25]. Despite the positive results of previous studies [
26], impedances continued to increase significantly over a 28-day period compared to day 0 after CI implantation when electrode arrays with 1% and 10% DEX were used [
2]. After 28 days, impedances reached a plateau. To reduce the increase in impedances during the first 28 days, we tested whether a combination of DEX with modified surfaces provides better results in terms of connective tissue reduction. Electrodes with DEX in the silicone body were examined. Electrodes were additionally provided with a PLLA coating, which contained either diclofenac or MM284. The performance of the modified electrodes was tested in vivo regarding impedances, tissue growth, and SGN density.
2. Materials and Methods
2.1. Ethical Statement
The in vivo experiments in this study were conducted in accordance with the German Animal Welfare Law and the European Directive 2010/63 and approved by the State Office for Consumer Protection and Food Safety, Dept. of Animal Welfare under the number 20/3502. Guinea pigs were housed in the animal facility of the Lower Saxony Center for Biomedical Engineering, Implant Research and Development (NIFE) of Hannover Medical School, and the experiments were performed with regard to the valid directives regarding accommodation, care, and usage of experimental animals. The guinea pigs were maintained in a temperature- and humidity-controlled room, exposed to a 24 h light–dark cycle (14 h/10 h) with free access to food and water.
2.2. Electrode Arrays
Cochlear implant guinea pig electrode arrays (MED-EL GmbH, Innsbruck, Austria) comprised four platinum (Pt) contacts at the distal tip and an additional reference electrode. Furthermore, the connector had an attached mesh for better fixation of the setup to the guinea pig skull. Electrode insertion depth was controlled with two black marker dots at 3 and 4 mm. The diameter of the electrode at the tip was approximately 300 µm (
Figure 1). For each electrode, 5% DEX (Sanofi, Paris, France) was incorporated into the silicone. A shielded cable connected the electrode array to a MED-EL PULSAR CI100 cochlear implant, which, in turn, was inductively coupled via a coil to the MED-EL MAX-Box.
2.3. Coating of the Electrodes
The coating of the electrodes from the tip to the marker dot at 4 mm was performed according to Wulf et al. 2022 [
21]. In order to achieve a stable PLLA coating, the electrode arrays were rinsed three times with ethanol and subsequently activated via O
2-plasma using a 100 W power at 0.3 mbar for 1 min in a plasma chamber (Diener, Ebhausen, Germany). Then, the samples were incubated in pure (3-glycidyloxypropyl) trimethoxysilane (GOPS) (Merck, Darmstadt, Germany) for 4 h at 90 °C. The activated samples were rinsed three times with ethanol and dried at 80 °C overnight under vacuum at 40 mbar. The polymer coating of the electrode array was prepared via an established and characterized in-house-manufactured spray coating process. First, the activated electrodes were spray coated with a thin polymer layer of PLLA-NH
2 (VWR, Dresden, Germany) using a chloroform PLLA-NH
2 (2 wt%) spray solution. Afterward, the samples were dried at 80 °C overnight and coated with chloroform PLLA (0.2 wt%) spray solutions containing either pure PLLA Resomer L210 (Evonik, Schwerte, Germany) or a polymer/drug mixture. These mixtures contained either diclofenac sodium salt (Merck, Darmstadt, Germany) to PLLA at ratios of 20:80 wt% or the immunophilin inhibitor MM284 (G. Fischer, MPIBC, Halle/S., Germany) to PLLA at a ratio 10:90 wt% in order to reach layer thicknesses of about 10 µm corresponding to a 70 µg coating mass. Thus, drug contents resulted in 14 µg diclofenac and 7 µg MM284 per electrode, respectively. Afterward, the modified electrodes were dried at 80 °C overnight. As the four electrode contacts were masked during the manufacturing process of the electrode, the coating was removed from the contacts by removing the masked areas according to [
21]. Electrodes were sterilized using ethylene oxide.
2.4. Animal Groups
Four groups of six animals were formed (
Table 1). Each animal received a CI unilaterally in the left inner ear. The right side remained untreated and served as a reference.
2.5. Animals and Experimental Design
Twenty-four adult male Dunkin Hartley guinea pigs (Charles River Laboratories, Châtillon, France) weighing 375 to 540 g were used. All animals were normal hearing as proven by initial hearing threshold determination (see
Section 2.7, AABR). After hearing threshold determination on day 0, the CI electrode was implanted. Subsequently, impedances were measured on all four contacts. From day 1 to 14, impedances were measured daily on the awake animal. After day 14, impedances were measured weekly on days 21 and 28. On the final day (day 28), an additional hearing threshold determination was performed under anesthesia and perilymph was collected from the apex of the cochleae as described in [
27]. Still under general anesthesia, the animals were euthanized immediately through transcardial perfusion with 200 mL of phosphate-buffered saline (PBS, Gibco™, Thermo Fisher Scientific, Paisley, UK) followed by 100 mL of 4% paraformaldehyde (PFA, Merck KGAA, Darmstadt, Germany). After perfusion, animals were decapitated and temporal bones were removed and dissected under a dissection microscope to expose the cochleae. The apex and oval window were pierced to enable rinsing. The electrode arrays remained in situ.
2.6. Anesthesia, Medication, and Surgery
Anesthesia and medication after surgery were previously published in detail by Malfeld et al. [
28]. The implantation was performed under general anesthesia (intramuscular medetomidine hydrochloride 0.2 mg/kg, midazolam 1 mg/kg, and fentanyl 0.025 mg/kg) with previous sedation (oral diazepam 4 mg/kg). In addition, the animals received Bepanthen
® eye ointment to avoid eye desiccation, and analgesia (Meloxicam 0.2 mg/kg s.c.) and antibiotics (Enrofloxacin 10 mg/kg s.c.) to reduce pain and to prevent infections, respectively. After anesthetizing and determination of the hearing threshold (see
Section 2.7 AABR), animals were placed on a heating mat at 38 °C. On day 0, after hearing threshold determination, all animals were implanted unilaterally in the left inner ear via cochleostomy and using an electrode insertion trauma approach [
2]. Areas of the skin to be incised were locally infiltrated with prilocaine (Xylonest 1%, Aspen Germany GmbH, Munich, Germany). On the guinea pig skull, the skin was opened and the top of the skull was dissected. The electrode and reference electrode were then guided underneath the skin and muscles toward the
bulla tympanica using a tunnel tube. Via an approach behind the ear, the periosteum of the bulla was abscised and the middle ear was opened with a scalpel and a forceps. A 0.7 mm hole was drilled (AccuPen 6V+; RISystem AG, Landquart, CH) in the cochlea 1 mm below the round window, into which the electrode was subsequently inserted up to the second black marker dot (
Figure 1) resulting in 4 mm insertion of the active electrode array. The electrode was fixed to the edge of the bulla using dental UV-cement (Tetric EvoFlow
®, Ivoclar Vivadent, Ellwangen, Germany) and the hole in the bulla was sealed. The reference electrode was placed above the bulla defect in the musculature. Then, the postauricular wound was closed in two layers. With the aid of two screws anchored in the skull and using Tetric EvoFlow and methyl methacrylate (Paladur
®, Kulzer GmbH, Hanau, Germany), the connector was fixed to the skull (
Figure 2). The UV-cement was used as a foundation and the Paladur was applied generously around the connector. Thereafter, the anesthesia was antagonized with Naloxon (0.03 mg/kg s.c., Naloxon, Inresa Arzneimittel GmbH, Freiburg, Germany), Flumazenil (0.1 mg/kg s.c., Flumazenil, Hameln pharma GmbH, Hameln, Germany), and Atipamezol (1.0 mg/kg s.c., Atipazole, Prodivet pharmaceuticals sa/nv, Eynatten, Belgium). Following antagonization, the guinea pig was placed under red light until it could maintain its body temperature, but at least for one hour.
2.7. Acoustically Evoked Auditory Brainstem Response (AABR)
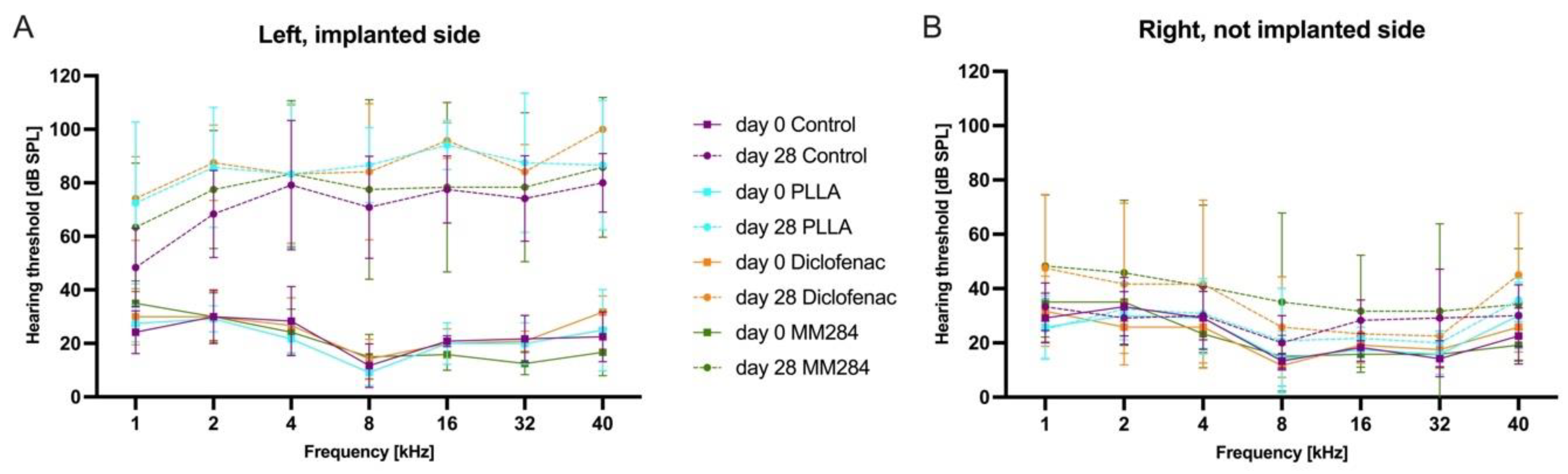
The AABR measurements were performed under general anesthesia on day 0 and day 28 in a sound attenuating chamber using a TDT System (Tucker-Davis Technologies, Alachua, FL, USA), and data were analyzed using the corresponding BioSigRP software. Acoustic tone stimuli with frequencies of 1, 2, 4, 8, 16, 32, and 40 kHz were generated and presented at sound pressure levels (SPLs) from 100 dB down to 0 dB in 5 dB steps by an EC1 speaker (Tucker-Davis Technologies) positioned in the external ear canal. One speaker was used first for the left ear and subsequently for the right ear. Subdermal needle electrodes (CareFusion Nicolet, Middleton, WI, USA) were placed at the vertex (common positive), left and right mastoid (references), and in the neck (ground). The tone pulses had a duration of 10 ms with a square cosine rise and fall time of 1 ms. The repetition rate was 10 tones per second and the recorded signal was bandpass-filtered from 300 to 3000 Hz to suppress the inclusion of background noise. All recorded neurological signals were sampled 300 times and averaged for analysis. Thresholds were defined as the lowest stimulus required to evoke a visually replicable waveform. When no thresholds could be detected, a value of 100 dB was used for calculation of mean values and threshold shifts.
2.8. Impedance Measurements
Impedance measurements were performed on days 0 and 28 in the anesthetized animal and on all other days on the awake animal. For the impedance measurements, the clinical system from MED-EL was used consisting of a MAX-Box and the MAESTRO software (version 8.0). Electrode impedances were measured via the Impedance Field Telemetry (IFT) task in monopolar mode.
2.9. Histology
2.9.1. Tissue Preparation
Histologic treatment of the cochleae was adapted from MacDonald and Rubel 2008 [
29]. All preparation steps were performed at room temperature on a platform rotator. The dissected cochleae were post-fixed in PFA overnight and rinsed in PBS for 10 min three times the next day. They were then decalcified in 10% ethylenediaminetetraacetic acid disodium salt (EDTA, Sigma-Aldrich Chemie GmbH, Schnelldorf, Germany) in PBS, pH 7.4, for three to four weeks, with regular EDTA change every one to three days. After decalcification, the cochleae were immunohistochemically stained.
To prepare staining, the cochleae were stored in 1% Triton X-100 (Sigma-Aldrich) in PBS at room temperature for six to eight hours. The primary antibody (Anti-vimentin antibody produced in goat, Sigma-Aldrich Chemie GmbH) was diluted in blocking solution (5% NHS (normal horse serum, Biozol, Eching, Germany) and 1% Triton in PBS). It was then applied to the cochleae and incubated for three days at 4 °C. After the incubation, the samples were washed with PBS three times for 2 h each. The second antibody (Alexa Fluor 647-conjugated AffiniPure Bovine Anti-Goat igG, Jackson ImmunoResearch, Pennsylvania) was applied, incubated, and washed in the same way. As a next step, the cochleae were dehydrated (70% ethanol overnight, 95% ethanol for 30 min, and ethanol absolute for 2 h on a rotation platform). The last step was the refractive index adjustment. For this, MSBB (methyl salicylate benzyl benzoate) was made by mixing five parts methyl salicylate with three parts benzyl benzoate (Merck KGAA). The MSBB was mixed 1:1 with ethanol absolute and the cochlea was placed in it for four hours at room temperature on a rotation platform. The cochlea was placed in pure MSBB overnight at room temperature and then stored at 4 °C.
2.9.2. Imaging
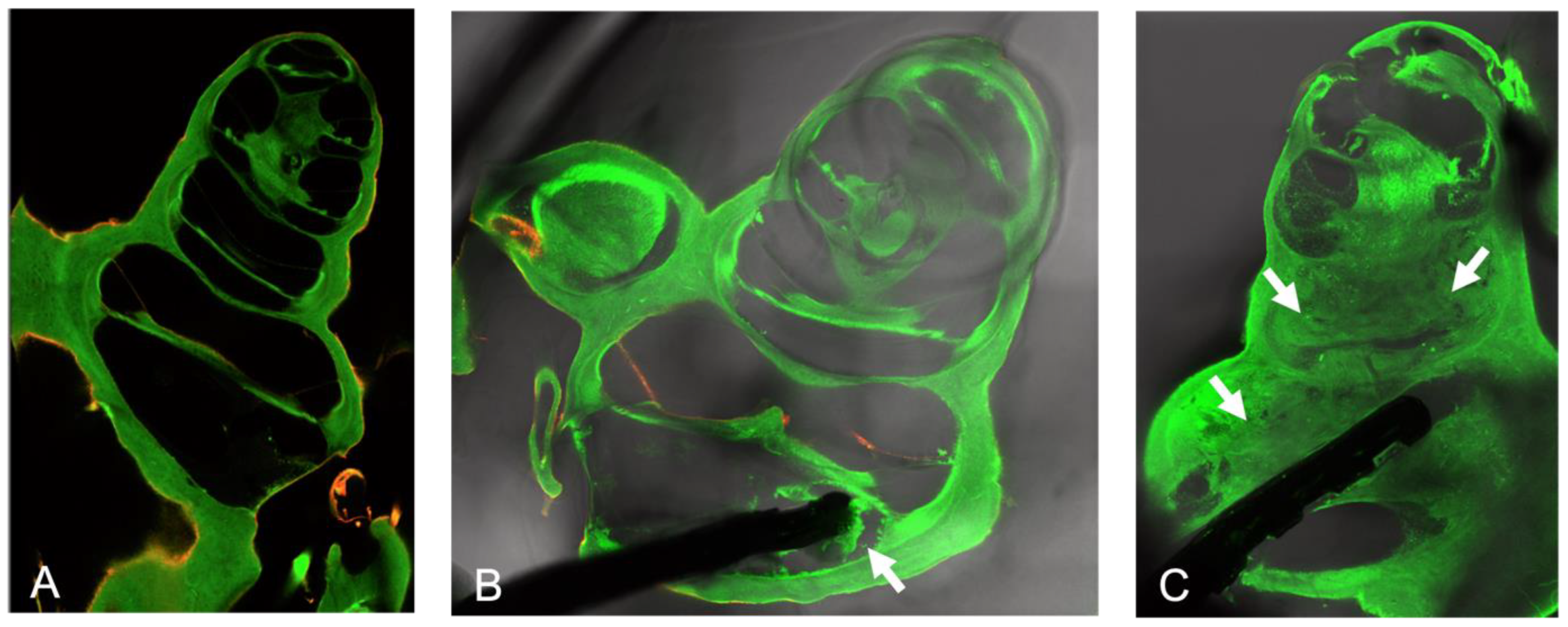
For microscopy, a Leica SP8 laser scanning confocal microscope (Leica Microsystems GmbH, Wetzlar, Germany) equipped with a white light laser was used combined with the Leica Confocal Software (LAS X Science Microscope Software; version LAS X 3.5.7.23225). An objective lens with 10× magnification (HC PL Fluotar 10x/0.30 Dry, Fa. Leica) was used. The laser provided the excitation lines at 492 nm (for PFA-induced autofluorescence) and 652 nm (for Alexa Fluor 647). The slices were generated with 20 µm steps (z-stack on) at a scanning speed of 400 Hz, 5× line averaging, and 3× frame averaging. To be able to see the electrode, the TLD (brightfield detector/through the lens detector) was switched on as third channel.
2.9.3. Connective Tissue Quantification
To assess the tissue response in each turn of the cochlea, the Leica Confocal software (LAS X Science Microscope Software) was used. With two custom-made ranking scores (adapted from [
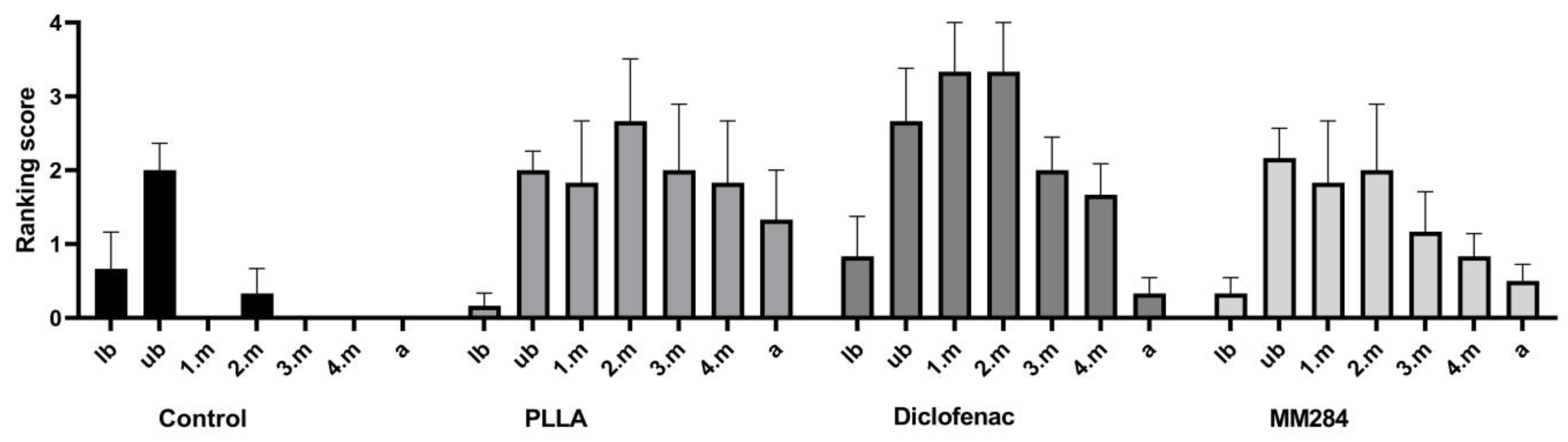
30]), the connective tissue growth was evaluated. One subjective scoring for all 7 cross-sections of the cochlea (lower basal turn (lb), upper basal turn (ub), first middle turn (1.m), second middle turn (2.m), third middle turn (3.m), fourth middle turn (4.m), and apical turn (a)) was defined as described in
Table 2 applying the percentage of filling of the respective cross-sectional scala tympani area.
A second ranking score for the connective tissue growth around the single contacts of the electrode array was defined: score 0 = no connective tissue; score 1 = thin film of tissue directly on the contact; score 2 = reticular growth of connective tissue on the contact; score 3 = contact completely covered by compact connective tissue.
2.9.4. Spiral Ganglion Neuron Counting
In the sections, the circumferences of Rosenthal’s canal were measured at the different turns as previously described [
31]. Due to the preparation methods, the 4.m and a turns could not always be analyzed separately. Therefore, SGN densities of these areas were averaged for analysis if available. In general, cells larger than 17 µm in diameter were counted. Depending on image quality, Rosenthal’s canal was partially covered by shadows caused by the electrode, so not all cells could be detected. The number of vital SGNs was related to the measured cross-sectional area of the Rosenthal canal to achieve the SGN density, expressed as cells/10,000 µm
2.
2.10. ELISA Analysis of DEX Levels in Perilymph Samples
DEX concentration was measured using a competitive commercial enzyme-linked immunosorbent assay (ELISA) kit (Neogen Corp., Lexington, MA, USA). Due to the small sample volume, the samples from each group were pooled and filled up to 45 µL, and a double determination was performed. Artificial perilymph (145 mM NaCl (Merck KGAA), 1.2 mM CaCl2 (Merck KGAA), 5 mM HEPES (Merck KGAA)) was used for the negative control. A microplate reader (Tecan Trading AG, Männedorf, Switzerland) with a 650 nm filter was used to scan the plate. The sensitivity of the test was 0.23 ng/mL.
2.11. Statistics
Statistical evaluations were performed using GraphPad Prism 9. First, all data were tested for normal distribution using the Shapiro–Wilk test. Hearing thresholds were statistically analyzed using ANOVA. The Kruskal–Wallis test was used to compare clinical impedances between groups. In addition, unpaired t-tests or Mann–Whitney tests (depending on the result of the normality test) were performed for each individual day to compare clinical impedances between the individual groups. For the evaluation of connective tissue growth, each group was compared once with the control group and once with the PLLA group using the Wilcoxon test. For the evaluation of SGN density, a paired t-test or a Wilcoxon test was used to compare the implanted ears with the untreated ears within each group. The Kruskal–Wallis test was used for comparison between the four groups. p-values below 0.05 were considered to indicate significant differences.
4. Discussion
CIs have been around for decades, yet the system still presents many challenges—one of which is connective tissue growth around the electrode. This leads to poorer signal transduction and increased impedances at the electrode contacts [
32,
33]. Many factors affect the formation of connective tissue in the inner ear after implantation of a CI. On the one hand, the implantation procedure itself plays a major role, as one can already set significant damage during the surgery, and on the other hand, the implant leads to a foreign body reaction [
34]. Local drug application in the cochlea is a possible approach to reduce connective tissue growth. In this context, a slow long-term release from the implant is desirable [
13]. In addition to a potential drug, an appropriate carrier is also needed. As PLLA has already been shown to be suitable as a carrier for drugs and shows no negative effects in the inner ear [
18], it was used in these experiments. The behavior of an electrode with DEX combined with a drug-eluting PLLA coating has not been previously reported.
The limitation of extended damage to PLLA-coated electrodes and the high number of damaged cochleae (
Table 5) can only be explained by altered mechanical properties of the electrode array. In contrast to many positive effects of PLLA, it leads to stiffening of the electrode when used as a coating. This seems to be contradictory to the results of [
19] where the generated pressure and friction during insertion of PLLA-coated electrode carriers were not increased. In the cited study, linear models of the scala tympani were used, preventing a measurable influence of altered bending characteristics of the electrode array. It is possible that the PLLA coating was too thick in combination with the electrode. In an earlier study, no increased damage was reported for PLLA-coated electrode models compared to electrode models without a coating [
18]. As, in the earlier study, pure silicone models of CI electrodes (no metal parts) were used, we might speculate that the combination of an electrode array with wires and contacts and the PLLA coating leads to an increased stiffness that finally was too high for insertion in the cochlea. Therefore, in future studies, attention should be on improvement of the flexibility of the electrode. The influence of the used trauma model [
2] on these observations remains unclear. As the model was also used for the control group and, in this group, no extended damage was observed, we might speculate that the observed greater trauma can be attributed to an increased stiffness of the PLLA-coated electrode arrays. However, as drug-loaded and plain PLLA coatings were used, the effects of the drugs diclofenac and immunophilin inhibitor MM284 could still be investigated. Nevertheless, the extended trauma with—at least in some cases—the tip of the electrode being located in the second turn remains disadvantageous in order to compare the study results with previous investigations using local DEX application [
30].
Diclofenac and the immunophilin inhibitor MM284 were used in the ear for the first time in this project based on in vitro studies from Wulf et al. 2022 [
21] and Goblet et al. 2022 [
23]. There, the authors showed no ototoxic effects of the drugs on SGNs. Four animals from the diclofenac group showed a reaction in the middle ear that did not occur in animals from the other groups. As, to the best of our knowledge, it is the first time reporting this phenomenon, a species-dependent reaction would be the most obvious cause even though also a general effect of diclofenac in the ear cannot be excluded. However, the exact pathogenesis is not clear and requires further investigation especially as most but not all animals of this group were affected.
All animals showed a hearing loss of more than 30 dB after 28 days on the implanted ear, which can be explained by the electrode insertion trauma [
35]. Increased hearing loss due to increased fibrosis has been described in the literature [
36]. Ceschi et al. [
18] showed lower absolute values for threshold shifts using coated and plain electrode models but, in their study, no trauma model was applied and also no extended damage was reported. Therefore, it is concluded that the larger threshold shifts in the current study are caused by the increased damage and not directly by the coating material and drugs applied. Additionally, the drilling of the cochleostomy caused intense noise, which also contributes to the hearing loss [
37]. However, this study focused on the investigation of connective tissue growth. As, with a cochleostomy, more tissue growth can be expected [
38], the cochleostomy approach was chosen.
Impedances obtained with the clinical system tended to be lower in the first ten days with diclofenac and MM284, especially at contacts one and two. From day 10, impedances increased to a similar level in all groups. This behavior over time indicates a delay in the impedance increase that can be attributed to diclofenac and MM284, as controls and empty PLLA-coatings exhibited a fast increase in impedance and all electrodes contained the same amount of DEX. Unfortunately, also in the current study, a long-lasting reduction in impedance was not achieved.
Confocal laser scanning microscopy was chosen for histological examinations in order to prevent loss of material due to embedding and further processing. Visualization of the material under examination proved a good performance, allowing for the study of the cochlea from all sides [
12]. Despite the used trauma model, there was less connective tissue growth in the control group, as the electrode without the PLLA coating caused no extended damage. Even though a direct comparison to electrode arrays without dexamethasone is not possible, the low tissue reaction in the control group despite the application of a trauma model might also indicate a beneficial effect of the released DEX, which should be expected according to [
39].
The concentration of DEX in the perilymph was highest in the control group. With an amount of 15.27 ng/mL, this concentration can be considered as not toxic for the SGNs [
40]. In the coated electrodes, it was much lower. A PLLA coating reduces the release of DEX from the silicone [
21] to less than half the value of uncoated silicone. In the current study, this difference was much larger than expected. Most likely, the amount of connective tissue contributes to this difference. In all groups with the PLLA coating, the connective tissue extended to and, in most cases, beyond the second middle turn. This tissue might have provided a diffusion barrier for the released DEX as perilymph was sampled from the apex of the cochleae. This, in turn, resulted in low volumes of collected perilymph such that all samples of a study group had to be pooled. However, most importantly, DEX was still released from the electrode array in vivo despite the PLLA coating and the tissue growth.
Regarding the amount of connective tissue, a direct comparison between the coated electrodes and the controls remains difficult. The much larger amount of tissue in the groups with the coated electrodes can most likely be attributed to the extended damage that was caused using these electrodes. Nevertheless, an influence of the PLLA itself on fibrosis cannot completely be excluded. Only little tissue was observed on PLLA-coated electrode models in an earlier study but, in that study, a detailed analysis of the connective tissue was not performed, due to explantation of most of the electrode models [
18]. Comparison of the drug-loaded groups with the PLLA group allowed an assessment on the efficacy of the drugs. No significant differences in connective tissue growth were detected, yet comparison of MM284 with diclofenac indicated less connective tissue growth in animals implanted with MM284. Thus, there was a positive trend in favor of MM284.
This positive trend toward MM284 was also supported by the numbers of surviving SGNs. Despite the extended damage, the numbers of surviving SGNs were not different between treated and untreated sides. The density of spiral ganglion neurons of the untreated sides was, on average, between 16 SGNs/10,000 µm
2 and 25 SGNs/10,000 µm
2. These values match those described in the literature, which were detected by confocal laser scanning microscopy and analyzed with ImageJ as in the current study [
31,
41]. In contrast, with PLLA and PLLA containing diclofenac, SGN numbers were reduced when compared to the respective untreated side. As SGN numbers were not different between PLLA-coated samples and uncoated samples in [
18], we speculate that the reduction in SGNs in the current study was caused by the increased trauma with coated electrodes. Then, MM284 prevented this trauma-induced reduction in SGN numbers.

 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}