

Multilocus Genetic Profile Reflecting Low Dopaminergic Signaling Is Directly Associated with Obesity and Cardiometabolic Disorders Due to Antipsychotic Treatment

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Sample Characteristics, Obesity Indicators, and Cardiometabolic Parameters
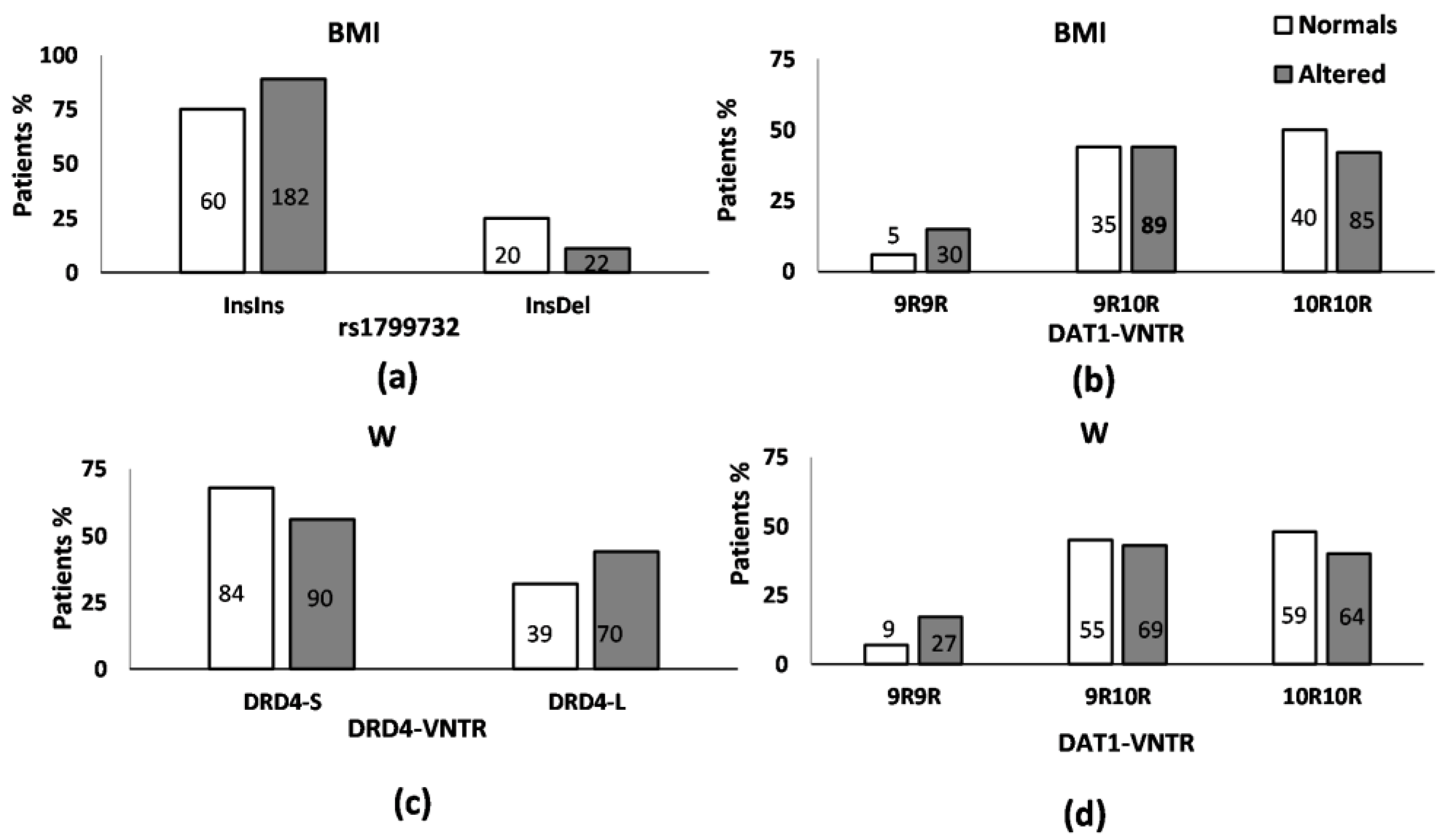
3.2. Relationship between the Presence/Absence of Obesity, BMI, and Abdominal Obesity and the Studied Genotypes
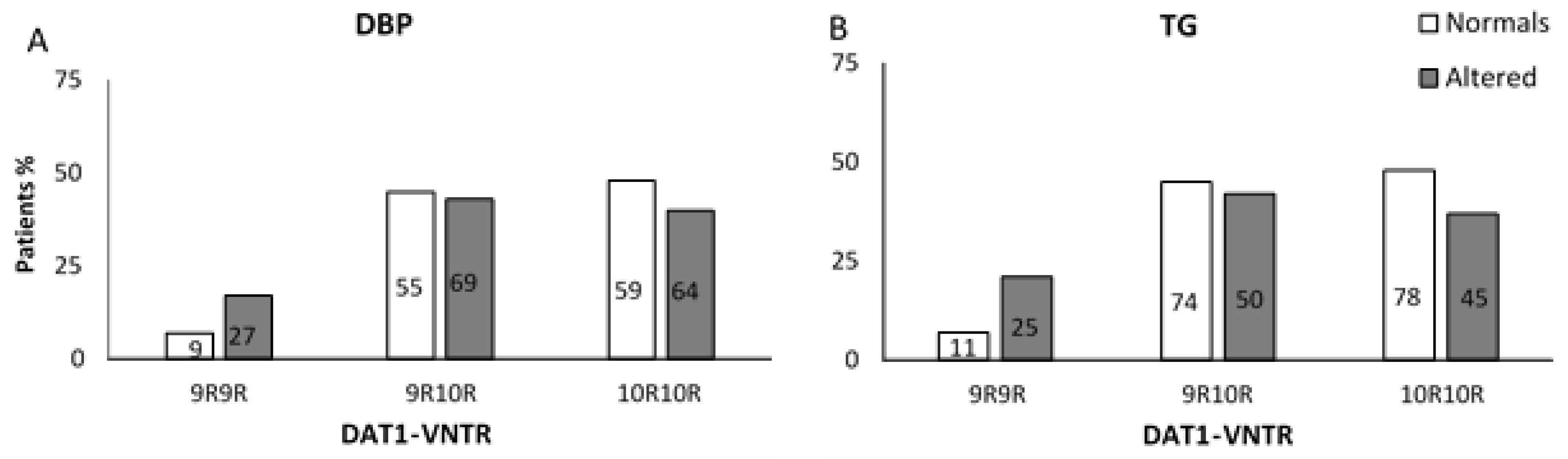
3.3. Relationship between the Presence of High Diastolic Blood Pressure, Hyperlipidaemia, and Hyperglycaemia and the Studied Genotypes
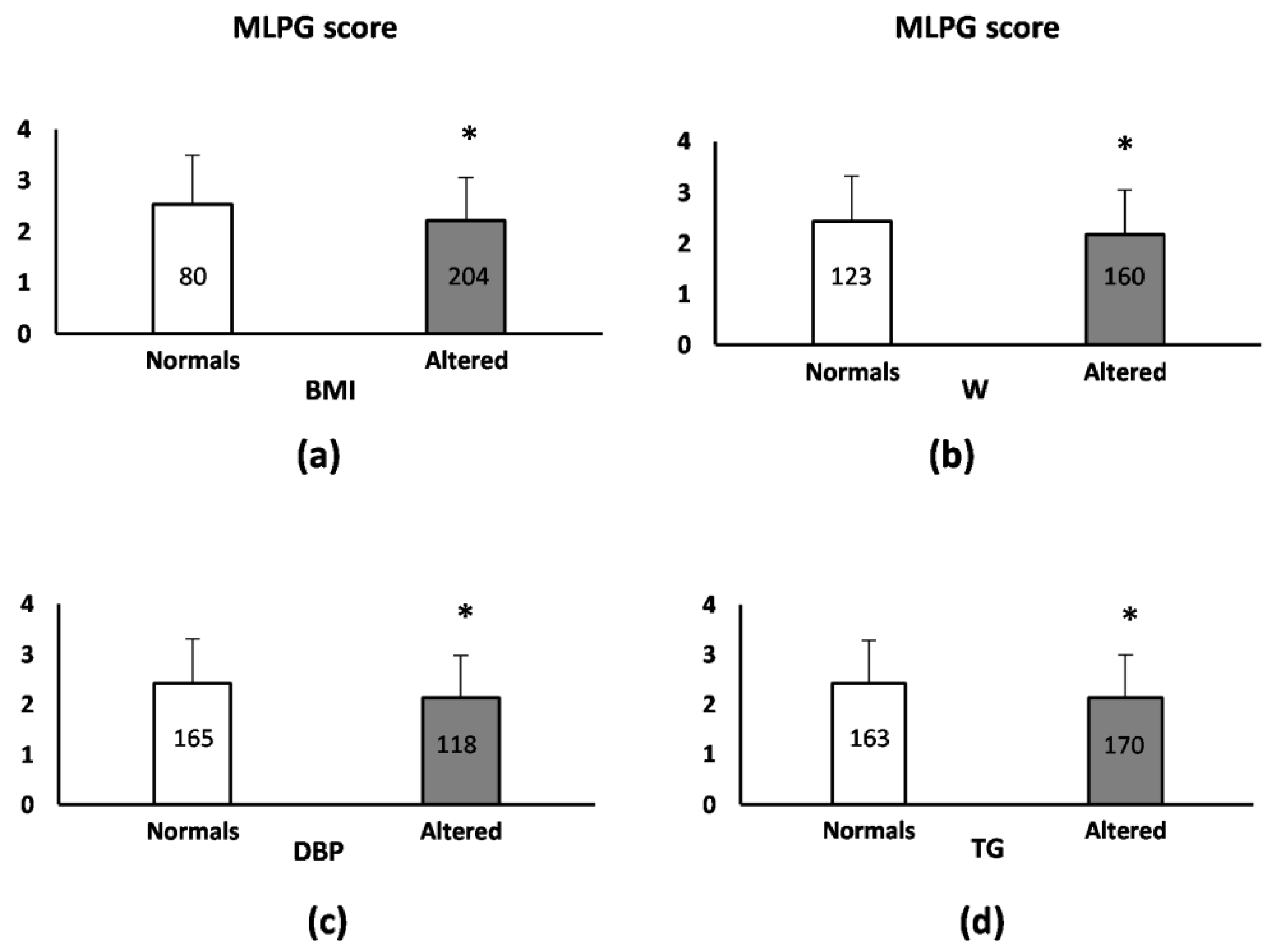
3.4. Relationship of the Presence/Absence of Obesity and Cardiometabolic Disorder Parameters Alterations with MLGP Score
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Newcomer, J.W. Antipsychotic Medications: Metabolic and Cardiovascular Risk. J. Clin. Psychiatry 2007, 68, 8–13. [Google Scholar] [PubMed]
- Correll, C.U.; Lencz, T.; Malhotra, A.K. Antipsychotic Drugs and Obesity. Trends Mol. Med. 2011, 17, 97–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mottillo, S.; Filion, K.B.; Genest, J.; Joseph, L.; Pilote, L.; Poirier, P.; Rinfret, S.; Schiffrin, E.L.; Eisenberg, M.J. The Metabolic Syndrome and Cardiovascular Risk a Systematic Review and Meta-Analysis. J. Am. Coll. Cardiol. 2010, 56, 1113–1132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vancampfort, D.; Stubbs, B.; Mitchell, A.J.; De Hert, M.; Wampers, M.; Ward, P.B.; Rosenbaum, S.; Correll, C.U. Risk of Metabolic Syndrome and Its Components in People with Schizophrenia and Related Psychotic Disorders, Bipolar Disorder and Major Depressive Disorder: A Systematic Review and Meta-Analysis. World Psychiatry Off. J. World Psychiatr. Assoc. WPA 2015, 14, 339–347. [Google Scholar] [CrossRef]
- Correll, C.U.; Robinson, D.G.; Schooler, N.R.; Brunette, M.F.; Mueser, K.T.; Rosenheck, R.A.; Marcy, P.; Addington, J.; Estroff, S.E.; Robinson, J.; et al. Cardiometabolic Risk in Patients with First-Episode Schizophrenia Spectrum Disorders: Baseline Results from the RAISE-ETP Study. JAMA Psychiatry 2014, 71, 1350–1363. [Google Scholar] [CrossRef] [Green Version]
- Gebhardt, S.; Theisen, F.M.; Haberhausen, M.; Heinzel-Gutenbrunner, M.; Wehmeier, P.M.; Krieg, J.-C.; Kühnau, W.; Schmidtke, J.; Remschmidt, H.; Hebebrand, J. Body Weight Gain Induced by Atypical Antipsychotics: An Extension of the Monozygotic Twin and Sib Pair Study. J. Clin. Pharm. Ther. 2010, 35, 207–211. [Google Scholar] [CrossRef]
- Arranz, M.J.; de Leon, J. Pharmacogenetics and Pharmacogenomics of Schizophrenia: A Review of Last Decade of Research. Mol. Psychiatry 2007, 12, 707–747. [Google Scholar] [CrossRef]
- Zhang, J.-P.; Lencz, T.; Zhang, R.X.; Nitta, M.; Maayan, L.; John, M.; Robinson, D.G.; Fleischhacker, W.W.; Kahn, R.S.; Ophoff, R.A.; et al. Pharmacogenetic Associations of Antipsychotic Drug-Related Weight Gain: A Systematic Review and Meta-Analysis. Schizophr. Bull. 2016, 42, 1418–1437. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, G.P.; McGowan, O.O. Mechanisms Underlying Metabolic Disturbances Associated with Psychosis and Antipsychotic Drug Treatment. J. Psychopharmacol. Oxf. Engl. 2017, 31, 1430–1436. [Google Scholar] [CrossRef]
- Mathews, J.; Newcomer, J.W.; Mathews, J.R.; Fales, C.L.; Pierce, K.J.; Akers, B.K.; Marcu, I.; Barch, D.M. Neural Correlates of Weight Gain with Olanzapine. Arch. Gen. Psychiatry 2012, 69, 1226–1237. [Google Scholar] [CrossRef] [Green Version]
- Baptista, T.; Parada, M.; Hernandez, L. Long Term Administration of Some Antipsychotic Drugs Increases Body Weight and Feeding in Rats. Are D2 Dopamine Receptors Involved? Pharmacol. Biochem. Behav. 1987, 27, 399–405. [Google Scholar] [CrossRef] [PubMed]
- de Leeuw van Weenen, J.E.; Auvinen, H.E.; Parlevliet, E.T.; Coomans, C.P.; Schröder-van der Elst, J.P.; Meijer, O.C.; Pijl, H. Blocking Dopamine D2 Receptors by Haloperidol Curtails the Beneficial Impact of Calorie Restriction on the Metabolic Phenotype of High-Fat Diet Induced Obese Mice. J. Neuroendocrinol. 2011, 23, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Perez-Iglesias, R.; Vazquez-Barquero, J.L.; Amado, J.A.; Berja, A.; Garcia-Unzueta, M.T.; Pelayo-Terán, J.M.; Carrasco-Marín, E.; Mata, I.; Crespo-Facorro, B. Effect of Antipsychotics on Peptides Involved in Energy Balance in Drug-Naive Psychotic Patients after 1 Year of Treatment. J. Clin. Psychopharmacol. 2008, 28, 289–295. [Google Scholar] [CrossRef]
- Kahn, R.S.; Fleischhacker, W.W.; Boter, H.; Davidson, M.; Vergouwe, Y.; Keet, I.P.M.; Gheorghe, M.D.; Rybakowski, J.K.; Galderisi, S.; Libiger, J.; et al. Effectiveness of Antipsychotic Drugs in First-Episode Schizophrenia and Schizophreniform Disorder: An Open Randomised Clinical Trial. Lancet Lond. Engl. 2008, 371, 1085–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenny, P.J. Common Cellular and Molecular Mechanisms in Obesity and Drug Addiction. Nat. Rev. Neurosci. 2011, 12, 638–651. [Google Scholar] [CrossRef]
- Volkow, N.D.; Wang, G.-J.; Baler, R.D. Reward, Dopamine and the Control of Food Intake: Implications for Obesity. Trends Cogn. Sci. 2011, 15, 37–46. [Google Scholar] [CrossRef] [Green Version]
- Stice, E.; Yokum, S.; Bohon, C.; Marti, N.; Smolen, A. Reward Circuitry Responsivity to Food Predicts Future Increases in Body Mass: Moderating Effects of DRD2 and DRD4. NeuroImage 2010, 50, 1618–1625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volkow, N.D.; Wang, G.J.; Fowler, J.S.; Tomasi, D.; Baler, R. Food and Drug Reward: Overlapping Circuits in Human Obesity and Addiction. In Brain Imaging in Behavioral Neuroscience. Current Topics in Behavioral Neurosciences; Springer: Berlin/Heidelberg, Germany, 2012; Volume 11, pp. 1–24. [Google Scholar] [CrossRef] [Green Version]
- Fetissov, S.O.; Meguid, M.M.; Sato, T.; Zhang, L.-H. Expression of Dopaminergic Receptors in the Hypothalamus of Lean and Obese Zucker Rats and Food Intake. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2002, 283, R905–R910. [Google Scholar] [CrossRef] [Green Version]
- Kalyanasundar, B.; Perez, C.I.; Luna, A.; Solorio, J.; Moreno, M.G.; Elias, D.; Simon, S.A.; Gutierrez, R. D1 and D2 Antagonists Reverse the Effects of Appetite Suppressants on Weight Loss, Food Intake, Locomotion, and Rebalance Spiking Inhibition in the Rat NAc Shell. J. Neurophysiol. 2015, 114, 585–607. [Google Scholar] [CrossRef] [Green Version]
- Kuo, D.-Y. Co-Administration of Dopamine D1 and D2 Agonists Additively Decreases Daily Food Intake, Body Weight and Hypothalamic Neuropeptide Y Level in Rats. J. Biomed. Sci. 2002, 9, 126–132. [Google Scholar] [CrossRef]
- Parada, M.A.; Hernandez, L.; Hoebel, B.G. Sulpiride Injections in the Lateral Hypothalamus Induce Feeding and Drinking in Rats. Pharmacol. Biochem. Behav. 1988, 30, 917–923. [Google Scholar] [CrossRef]
- Auger, F.; Martin, F.; Pétrault, O.; Samaillie, J.; Hennebelle, T.; Trabelsi, M.-S.; Bailleul, F.; Staels, B.; Bordet, R.; Duriez, P. Risperidone-Induced Metabolic Dysfunction Is Attenuated by Curcuma Longa Extract Administration in Mice. Metab. Brain Dis. 2018, 33, 63–77. [Google Scholar] [CrossRef]
- Comings, D.E.; Gade, R.; MacMurray, J.P.; Muhleman, D.; Peters, W.R. Genetic Variants of the Human Obesity (OB) Gene: Association with Body Mass Index in Young Women, Psychiatric Symptoms, and Interaction with the Dopamine D2 Receptor (DRD2) Gene. Mol. Psychiatry 1996, 1, 325–335. [Google Scholar] [PubMed]
- Davis, C.; Levitan, R.D.; Yilmaz, Z.; Kaplan, A.S.; Carter, J.C.; Kennedy, J.L. Binge Eating Disorder and the Dopamine D2 Receptor: Genotypes and Sub-Phenotypes. Prog. Neuropsychopharmacol. Biol. Psychiatry 2012, 38, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Bergen, A.W.; Yeager, M.; Welch, R.A.; Haque, K.; Ganjei, J.K.; van den Bree, M.B.M.; Mazzanti, C.; Nardi, I.; Fichter, M.M.; Halmi, K.A.; et al. Association of Multiple DRD2 Polymorphisms with Anorexia Nervosa. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 2005, 30, 1703–1710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winkler, J.K.; Schultz, J.-H.; Woehning, A.; Piel, D.; Gartner, L.; Hildebrand, M.; Roeder, E.; Nawroth, P.P.; Wolfrum, C.; Rudofsky, G. Effectiveness of a Low-Calorie Weight Loss Program in Moderately and Severely Obese Patients. Obes. Facts 2013, 6, 469–480. [Google Scholar] [CrossRef]
- Kvaløy, K.; Kulle, B.; Romundstad, P.; Holmen, T.L. Sex-Specific Effects of Weight-Affecting Gene Variants in a Life Course Perspective--The HUNT Study, Norway. Int. J. Obes. 2005 2013, 37, 1221–1229. [Google Scholar] [CrossRef] [Green Version]
- Stice, E.; Spoor, S.; Bohon, C.; Small, D.M. Relation between Obesity and Blunted Striatal Response to Food Is Moderated by TaqIA A1 Allele. Science 2008, 322, 449–452. [Google Scholar] [CrossRef] [Green Version]
- Epstein, L.H.; Temple, J.L.; Neaderhiser, B.J.; Salis, R.J.; Erbe, R.W.; Leddy, J.J. Food Reinforcement, the Dopamine D2 Receptor Genotype, and Energy Intake in Obese and Nonobese Humans. Behav. Neurosci. 2007, 121, 877–886. [Google Scholar] [CrossRef] [Green Version]
- Lek, F.-Y.; Ong, H.-H.; Say, Y.-H. Association of Dopamine Receptor D2 Gene (DRD2) Taq1 Polymorphisms with Eating Behaviors and Obesity among Chinese and Indian Malaysian University Students. Asia Pac. J. Clin. Nutr. 2018, 27, 707–717. [Google Scholar] [CrossRef]
- Epstein, L.H.; Dearing, K.K.; Erbe, R.W. Parent-Child Concordance of Taq1 A1 Allele Predicts Similarity of Parent-Child Weight Loss in Behavioral Family-Based Treatment Programs. Appetite 2010, 55, 363–366. [Google Scholar] [CrossRef] [Green Version]
- Jönsson, E.G.; Nöthen, M.M.; Grünhage, F.; Farde, L.; Nakashima, Y.; Propping, P.; Sedvall, G.C. Polymorphisms in the Dopamine D2 Receptor Gene and Their Relationships to Striatal Dopamine Receptor Density of Healthy Volunteers. Mol. Psychiatry 1999, 4, 290–296. [Google Scholar] [CrossRef] [Green Version]
- Duan, J.; Wainwright, M.S.; Comeron, J.M.; Saitou, N.; Sanders, A.R.; Gelernter, J.; Gejman, P.V. Synonymous Mutations in the Human Dopamine Receptor D2 (DRD2) Affect MRNA Stability and Synthesis of the Receptor. Hum. Mol. Genet. 2003, 12, 205–216. [Google Scholar] [CrossRef]
- Asghari, V.; Sanyal, S.; Buchwaldt, S.; Paterson, A.; Jovanovic, V.; Van Tol, H.H. Modulation of Intracellular Cyclic AMP Levels by Different Human Dopamine D4 Receptor Variants. J. Neurochem. 1995, 65, 1157–1165. [Google Scholar] [CrossRef]
- Seeger, G.; Schloss, P.; Schmidt, M.H. Marker Gene Polymorphisms in Hyperkinetic Disorder--Predictors of Clinical Response to Treatment with Methylphenidate? Neurosci. Lett. 2001, 313, 45–48. [Google Scholar] [CrossRef]
- Stice, E.; Yokum, S.; Zald, D.; Dagher, A. Dopamine-Based Reward Circuitry Responsivity, Genetics, and Overeating. Curr. Top. Behav. Neurosci. 2011, 6, 81–93. [Google Scholar] [CrossRef] [PubMed]
- Levitan, R.D.; Masellis, M.; Lam, R.W.; Muglia, P.; Basile, V.S.; Jain, U.; Kaplan, A.S.; Tharmalingam, S.; Kennedy, S.H.; Kennedy, J.L. Childhood Inattention and Dysphoria and Adult Obesity Associated with the Dopamine D4 Receptor Gene in Overeating Women with Seasonal Affective Disorder. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 2004, 29, 179–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mill, J.; Asherson, P.; Browes, C.; D’Souza, U.; Craig, I. Expression of the Dopamine Transporter Gene Is Regulated by the 3’ UTR VNTR: Evidence from Brain and Lymphocytes Using Quantitative RT-PCR. Am. J. Med. Genet. 2002, 114, 975–979. [Google Scholar] [CrossRef] [PubMed]
- Bieliński, M.; Jaracz, M.; Lesiewska, N.; Tomaszewska, M.; Sikora, M.; Junik, R.; Kamińska, A.; Tretyn, A.; Borkowska, A. Association between COMT Val158Met and DAT1 Polymorphisms and Depressive Symptoms in the Obese Population. Neuropsychiatr. Dis. Treat. 2017, 13, 2221–2229. [Google Scholar] [CrossRef] [Green Version]
- Yokum, S.; Marti, C.N.; Smolen, A.; Stice, E. Relation of the Multilocus Genetic Composite Reflecting High Dopamine Signaling Capacity to Future Increases in BMI. Appetite 2015, 87, 38–45. [Google Scholar] [CrossRef] [Green Version]
- Lachman, H.M.; Papolos, D.F.; Saito, T.; Yu, Y.M.; Szumlanski, C.L.; Weinshilboum, R.M. Human Catechol-O-Methyltransferase Pharmacogenetics: Description of a Functional Polymorphism and Its Potential Application to Neuropsychiatric Disorders. Pharmacogenetics 1996, 6, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Kring, S.I.I.; Werge, T.; Holst, C.; Toubro, S.; Astrup, A.; Hansen, T.; Pedersen, O.; Sørensen, T.I.A. Polymorphisms of Serotonin Receptor 2A and 2C Genes and COMT in Relation to Obesity and Type 2 Diabetes. PLoS ONE 2009, 4, e6696. [Google Scholar] [CrossRef]
- Mikołajczyk, E.; Smiarowska, M.; Grzywacz, A.; Samochowiec, J. Association of Eating Disorders with Catechol-o-Methyltransferase Gene Functional Polymorphism. Neuropsychobiology 2006, 54, 82–86. [Google Scholar] [CrossRef]
- Lencz, T.; Robinson, D.G.; Napolitano, B.; Sevy, S.; Kane, J.M.; Goldman, D.; Malhotra, A.K. DRD2 Promoter Region Variation Predicts Antipsychotic-Induced Weight Gain in First Episode Schizophrenia. Pharmacogenet. Genom. 2010, 20, 569–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, D.J.; Zai, C.C.; Sicard, M.; Remington, E.; Souza, R.P.; Tiwari, A.K.; Hwang, R.; Likhodi, O.; Shaikh, S.; Freeman, N.; et al. Systematic Analysis of Dopamine Receptor Genes (DRD1-DRD5) in Antipsychotic-Induced Weight Gain. Pharm. J. 2012, 12, 156–164. [Google Scholar] [CrossRef]
- Pinto, J.A.F.; de Freitas, P.H.B.; Nunes, F.D.D.; Granjeiro, P.A.; Santos, L.L.D.; Machado, R.M. Prevalence of polymorphisms in the ANKK1, DRD2, DRD3 genes and metabolic syndrome in refractory schizophrenia. Rev. Lat. Am. Enferm. 2018, 26, e2983. [Google Scholar] [CrossRef] [Green Version]
- Popp, J.; Leucht, S.; Heres, S.; Steimer, W. DRD4 48 Bp VNTR but Not 5-HT 2C Cys23Ser Receptor Polymorphism Is Related to Antipsychotic-Induced Weight Gain. Pharm. J. 2009, 9, 71–77. [Google Scholar] [CrossRef] [Green Version]
- Alladi, C.G.; Mohan, A.; Shewade, D.G.; Rajkumar, R.P.; Adithan, S.; Subramanian, K. Risperidone-Induced Adverse Drug Reactions and Role of DRD2 (-141 C Ins/Del) and 5HTR2C (-759 C>T) Genetic Polymorphisms in Patients with Schizophrenia. J. Pharmacol. Pharmacother. 2017, 8, 28–32. [Google Scholar] [CrossRef] [Green Version]
- De Luca, V.; Souza, R.P.; Viggiano, E.; Sickert, L.; Teo, C.; Zai, C.; Tiwari, A.K.; Müller, D.J.; Lieberman, J.A.; Volavka, J.; et al. Genetic Interactions in the Adrenergic System Genes: Analysis of Antipsychotic-Induced Weight Gain. Hum. Psychopharmacol. 2011, 26, 386–391. [Google Scholar] [CrossRef]
- Gassó, P.; Arnaiz, J.A.; Mas, S.; Lafuente, A.; Bioque, M.; Cuesta, M.J.; Díaz-Caneja, C.M.; García, C.; Lobo, A.; González-Pinto, A.; et al. Association Study of Candidate Genes with Obesity and Metabolic Traits in Antipsychotic-Treated Patients with First-Episode Psychosis over a 2-Year Period. J. Psychopharmacol. Oxf. Engl. 2020, 34, 514–523. [Google Scholar] [CrossRef] [PubMed]
- Lane, H.-Y.; Liu, Y.-C.; Huang, C.-L.; Chang, Y.-C.; Wu, P.-L.; Lu, C.-T.; Chang, W.-H. Risperidone-Related Weight Gain: Genetic and Nongenetic Predictors. J. Clin. Psychopharmacol. 2006, 26, 128–134. [Google Scholar] [CrossRef]
- Thomas, P.; Srivastava, V.; Singh, A.; Mathur, P.; Nimgaonkar, V.L.; Lerer, B.; Thelma, B.K.; Deshpande, S.N. Correlates of Response to Olanzapine in a North Indian Schizophrenia Sample. Psychiatry Res. 2008, 161, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Tybura, P.; Trześniowska-Drukała, B.; Bienkowski, P.; Beszlej, A.; Frydecka, D.; Mierzejewski, P.; Samochowiec, A.; Grzywacz, A.; Samochowiec, J. Pharmacogenetics of Adverse Events in Schizophrenia Treatment: Comparison Study of Ziprasidone, Olanzapine and Perazine. Psychiatry Res. 2014, 219, 261–267. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, M.; Chen, J.; Wu, Z.; Yu, S.; Fang, Y.; Zhang, C. Metabolic Syndrome in Patients Taking Clozapine: Prevalence and Influence of Catechol-O-Methyltransferase Genotype. Psychopharmacology 2014, 231, 2211–2218. [Google Scholar] [CrossRef]
- Comings, D.E.; Blum, K. Reward Deficiency Syndrome: Genetic Aspects of Behavioral Disorders. Prog. Brain Res. 2000, 126, 325–341. [Google Scholar] [CrossRef]
- Davis, C.; Loxton, N.J.; Levitan, R.D.; Kaplan, A.S.; Carter, J.C.; Kennedy, J.L. “Food Addiction” and Its Association with a Dopaminergic Multilocus Genetic Profile. Physiol. Behav. 2013, 118, 63–69. [Google Scholar] [CrossRef]
- Nikolova, Y.S.; Ferrell, R.E.; Manuck, S.B.; Hariri, A.R. Multilocus Genetic Profile for Dopamine Signaling Predicts Ventral Striatum Reactivity. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 2011, 36, 1940–1947. [Google Scholar] [CrossRef] [Green Version]
- Stice, E.; Yokum, S.; Burger, K.; Epstein, L.; Smolen, A. Multilocus Genetic Composite Reflecting Dopamine Signaling Capacity Predicts Reward Circuitry Responsivity. J. Neurosci. Off. J. Soc. Neurosci. 2012, 32, 10093–10100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardner, D.M.; Murphy, A.L.; O’Donnell, H.; Centorrino, F.; Baldessarini, R.J. International Consensus Study of Antipsychotic Dosing. Am. J. Psychiatry 2010, 167, 686–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bursac, Z.; Gauss, C.H.; Williams, D.K.; Hosmer, D.W. Purposeful Selection of Variables in Logistic Regression. Source Code Biol. Med. 2008, 3, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houston, J.P.; Kohler, J.; Bishop, J.R.; Ellingrod, V.L.; Ostbye, K.M.; Zhao, F.; Conley, R.R.; Poole Hoffmann, V.; Fijal, B.A. Pharmacogenomic Associations with Weight Gain in Olanzapine Treatment of Patients without Schizophrenia. J. Clin. Psychiatry 2012, 73, 1077–1086. [Google Scholar] [CrossRef]
- Silveira, P.P.; Portella, A.K.; Kennedy, J.L.; Gaudreau, H.; Davis, C.; Steiner, M.; Soares, C.N.; Matthews, S.G.; Sokolowski, M.B.; Dubé, L.; et al. Association between the Seven-Repeat Allele of the Dopamine-4 Receptor Gene (DRD4) and Spontaneous Food Intake in Pre-School Children. Appetite 2014, 73, 15–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sobik, L.; Hutchison, K.; Craighead, L. Cue-Elicited Craving for Food: A Fresh Approach to the Study of Binge Eating. Appetite 2005, 44, 253–261. [Google Scholar] [CrossRef]
- Wang, G.-J.; Volkow, N.D.; Thanos, P.K.; Fowler, J.S. Similarity between Obesity and Drug Addiction as Assessed by Neurofunctional Imaging: A Concept Review. J. Addict. Dis. 2004, 23, 39–53. [Google Scholar] [CrossRef]
- Appel, L.; Bergström, M.; Buus Lassen, J.; Långström, B. Tesofensine, a Novel Triple Monoamine Re-Uptake Inhibitor with Anti-Obesity Effects: Dopamine Transporter Occupancy as Measured by PET. Eur. Neuropsychopharmacol. J. Eur. Coll. Neuropsychopharmacol. 2014, 24, 251–261. [Google Scholar] [CrossRef]
- Sasaki, T.; Ito, H.; Kimura, Y.; Arakawa, R.; Takano, H.; Seki, C.; Kodaka, F.; Fujie, S.; Takahata, K.; Nogami, T.; et al. Quantification of Dopamine Transporter in Human Brain Using PET with 18F-FE-PE2I. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2012, 53, 1065–1073. [Google Scholar] [CrossRef] [Green Version]
- Dreher, J.-C.; Kohn, P.; Kolachana, B.; Weinberger, D.R.; Berman, K.F. Variation in Dopamine Genes Influences Responsivity of the Human Reward System. Proc. Natl. Acad. Sci. USA. 2009, 106, 617–622. [Google Scholar] [CrossRef]
- Brody, A.L.; Mandelkern, M.A.; Olmstead, R.E.; Allen-Martinez, Z.; Scheibal, D.; Abrams, A.L.; Costello, M.R.; Farahi, J.; Saxena, S.; Monterosso, J.; et al. Ventral Striatal Dopamine Release in Response to Smoking a Regular vs a Denicotinized Cigarette. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 2009, 34, 282–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellingrod, V.L.; Taylor, S.F.; Dalack, G.; Grove, T.B.; Bly, M.J.; Brook, R.D.; Zöllner, S.K.; Pop-Busui, R. Risk Factors Associated with Metabolic Syndrome in Bipolar and Schizophrenia Subjects Treated with Antipsychotics: The Role of Folate Pharmacogenetics. J. Clin. Psychopharmacol. 2012, 32, 261–265. [Google Scholar] [CrossRef]
- Balt, S.L.; Galloway, G.P.; Baggott, M.J.; Schwartz, Z.; Mendelson, J. Mechanisms and Genetics of Antipsychotic-Associated Weight Gain. Clin. Pharmacol. Ther. 2011, 90, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Vehof, J.; Risselada, A.J.; Al Hadithy, A.F.Y.; Burger, H.; Snieder, H.; Wilffert, B.; Arends, J.; Wunderink, L.; Knegtering, H.; Wiersma, D.; et al. Association of Genetic Variants of the Histamine H1 and Muscarinic M3 Receptors with BMI and HbA1c Values in Patients on Antipsychotic Medication. Psychopharmacology 2011, 216, 257–265. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.F.; Huang, A.S.; Snowman, A.M.; Teuscher, C.; Snyder, S.H. From the Cover: Antipsychotic Drug-Induced Weight Gain Mediated by Histamine H1 Receptor-Linked Activation of Hypothalamic AMP-Kinase. Proc. Natl. Acad. Sci. USA 2007, 104, 3456–3459. [Google Scholar] [CrossRef] [PubMed]
- Han, M.; Deng, C.; Burne, T.H.J.; Newell, K.A.; Huang, X.-F. Short- and Long-Term Effects of Antipsychotic Drug Treatment on Weight Gain and H1 Receptor Expression. Psychoneuroendocrinology 2008, 33, 569–580. [Google Scholar] [CrossRef]
- Lian, J.; Huang, X.-F.; Pai, N.; Deng, C. Preventing Olanzapine-Induced Weight Gain Using Betahistine: A Study in a Rat Model with Chronic Olanzapine Treatment. PLoS ONE 2014, 9, e104160. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.H.; Jakubovski, E.; Gabriel, D.; Bloch, M.H. Predictors and Moderators of Antipsychotic-Related Weight Gain in the Treatment of Early-Onset Schizophrenia Spectrum Disorders Study. J. Child Adolesc. Psychopharmacol. 2018, 28, 474–484. [Google Scholar] [CrossRef]
- Vázquez-Bourgon, J.; Ibáñez Alario, M.; Mayoral-van Son, J.; Gómez Revuelta, M.; Ayesa Arriola, R.; Juncal Ruiz, M.; Ortiz-García de la Foz, V.; Crespo Facorro, B. A 3-Year Prospective Study on the Metabolic Effect of Aripiprazole, Quetiapine and Ziprasidone: A Pragmatic Clinical Trial in First Episode Psychosis Patients. Eur. Neuropsychopharmacol. J. Eur. Coll. Neuropsychopharmacol. 2020, 39, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Wysokiński, A.; Kowman, M.; Kłoszewska, I. The Prevalence of Metabolic Syndrome and Framingham Cardiovascular Risk Scores in Adult Inpatients Taking Antipsychotics—A Retrospective Medical Records Review. Psychiatr. Danub. 2012, 24, 314–322. [Google Scholar] [PubMed]
- Eriksen, B.O.; Stefansson, V.T.N.; Jenssen, T.G.; Mathisen, U.D.; Schei, J.; Solbu, M.D.; Wilsgaard, T.; Melsom, T. Blood Pressure and Age-Related GFR Decline in the General Population. BMC Nephrol. 2017, 18, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aly El-Gabry, D.M.; Abdel Aziz, K.; Okasha, T.; Azzam, H.; Okasha, A. Antipsychotic Polypharmacy and Its Relation to Metabolic Syndrome in Patients With Schizophrenia: An Egyptian Study. J. Clin. Psychopharmacol. 2018, 38, 27–33. [Google Scholar] [CrossRef]
- Edinoff, A.N.; Ellis, E.D.; Nussdorf, L.M.; Hill, T.W.; Cornett, E.M.; Kaye, A.M.; Kaye, A.D. Antipsychotic Polypharmacy-Related Cardiovascular Morbidity and Mortality: A Comprehensive Review. Neurol. Int. 2022, 14, 294–309. [Google Scholar] [CrossRef]
- Fleischhacker, W.W.; Heikkinen, M.E.; Olié, J.-P.; Landsberg, W.; Dewaele, P.; McQuade, R.D.; Loze, J.-Y.; Hennicken, D.; Kerselaers, W. Effects of Adjunctive Treatment with Aripiprazole on Body Weight and Clinical Efficacy in Schizophrenia Patients Treated with Clozapine: A Randomized, Double-Blind, Placebo-Controlled Trial. Int. J. Neuropsychopharmacol. 2010, 13, 1115–1125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Potkin, S.G.; Cohen, M.; Panagides, J. Efficacy and Tolerability of Asenapine in Acute Schizophrenia: A Placebo- and Risperidone-Controlled Trial. J. Clin. Psychiatry 2007, 68, 1492–1500. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | N | Mean | |
|---|---|---|---|
| Age (years) | 284 | 43.8 ±10.7 | |
| Onset (years) | 268 | 23.0 ± 8.2 | |
| Illness duration (years) | 268 | 20.7 ± 11.1 | |
| Sex (men) | 188 | 66.0 | |
| Educational level | Without studies | 15 | 5.3 |
| Primary | 139 | 48.8 | |
| High school | 98 | 34.4 | |
| University | 32 | 11.6 | |
| Marital status | Single | 229 | 80.9 |
| Married, couple | 23 | 8.1 | |
| Widowed, divorced | 31 | 11.0 | |
| Tobacco use | User | 190 | 66.9 |
| Not user | 83 | 29.2 | |
| Former user | 11 | 3.9 | |
| Alcohol use | Ocassional user | 45 | 15.9 |
| Not user | 231 | 81.6 | |
| Former user | 7 | 2.5 | |
| Cannabis use | Ocassional user | 40 | 14.1 |
| Not user | 235 | 82.7 | |
| Former user | 9 | 3.2 | |
| Diagnosis | Schizophrenia | 209 | 73.6 |
| Bipolar disorder | 48 | 16.9 | |
| Psychotic disorder | 16 | 5.6 | |
| Personality disorder | 7 | 2.5 | |
| Others | 4 | 1.5 | |
| AP treatment | Monotherapy n (%) | 169 | 59.3 |
| Polytherapy n (%) | 115 | 40.4 | |
| Daily doses (mg/day) | 281 | 669.8 ± 445.7 | |
| Treatment time (months) | 284 | 27.9 ± 41.4 | |
| Concomitant treatment | Mood stabilizers | 69 | 24.2 |
| Antidepressants | 51 | 17.9 | |
| Anxiolytics | 185 | 65.1 | |
| Obesity, cardiometabolic disorders parameters | Obesity, BMI a | 204 | 71.8 |
| Abdominal obesity, W b | 160 | 56.5 | |
| High SBP b | 105 | 37.1 | |
| High DBP b | 118 | 41.7 | |
| HTG b | 120 | 42.4 | |
| L-HDL b | 152 | 53.7 | |
| Hyperglycemia b | 81 | 28.7 |
| Antipsychotic Treatment (AP) | N | % | 1AP | 2AP | 3AP | |
|---|---|---|---|---|---|---|
| 284 | 100 | 169 (59.5%) | 102 (35.9%) | 13 (4.6%) | ||
| SGA | Clozapine | 87 | 30.6 | 38 | 43 | 6 |
| Olanzapine | 75 | 26.4 | 45 | 25 | 5 | |
| Quetiapine | 44 | 15.5 | 20 | 18 | 6 | |
| Risperidone | 45 | 15.8 | 21 | 21 | 3 | |
| Paliperidone | 48 | 21.1 | 30 | 24 | 4 | |
| Amisulpride | 12 | 4.2 | 1 | 9 | 2 | |
| Aripiprazole | 51 | 17.3 | 12 | 32 | 7 | |
| Asenapide | 6 | 2.1 | 2 | 4 | 0 | |
| Lurasidone | 1 | 0.4 | 0 | 0 | 1 | |
| Fluphenacin | 1 | 0.4 | 0 | 1 | 0 | |
| FGA combined with SGA | Haloperidol | 9 | 3.2 | 0 | 7 | 2 |
| Clotiapine | 14 | 4.9 | 0 | 11 | 3 | |
| Zuclophentyxol | 7 | 2.5 | 0 | 7 | 0 | |
| Levopromycin | 2 | 0.7 | 0 | 2 | 0 |
| MLR | X2 | Nag R2 | OR | 95% CI | p | ||
|---|---|---|---|---|---|---|---|
| BMI | DRD2rs1799732 | ref InsDel | 15.91 | 0.084 | |||
| InsIns | 2.91 | 1.42–5.94 | 0.003 | ||||
| Illness duration | 0.97 | 0.94–0.99 | 0.010 | ||||
| DAT1-VNTR | ref 10R10R | 12.61 | 0.067 | ||||
| 9R9R | 3.23 | 1.04–10.01 | 0.042 | ||||
| 9R10R | 1.13 | 0.64–2.01 | 0.671 | ||||
| Illness duration | 0.97 | 0.94–0.99 | 0.006 | ||||
| W | DAT1-VNTR | ref 10R10R | 22.12 | 0.101 | |||
| 9R9R | 2.73 | 1.16–6.40 | 0.021 | ||||
| 9R10R | 1.22 | 0.73–2.04 | 0.447 | ||||
| Sex (Wo/M) | 2.88 | 1.68–4.95 | <0.001 | ||||
| DRD4-VNTR | ref DRD4-S | 20.89 | 0.095 | ||||
| DRD4-L 1 or 2 | 1.73 | 1.04–2.87 | 0.035 | ||||
| Sex (Wo/M) | 2.95 | 1.72–5.06 | <0.001 |
| MLR | X2 | Nag R2 | OR | 95% CI | p | ||
|---|---|---|---|---|---|---|---|
| DBP | DAT1-VNTR | ref 10R10R | 15.88 | 0.075 | |||
| 9R9R | 3.33 | 1.54–7.31 | 0.003 | ||||
| 9R10R | 1.36 | 0.81–2.28 | 0.252 | ||||
| Age | 1.03 | 1.01–1.05 | 0.015 | ||||
| TG | DAT1-VNTR | ref 10R10R | 20.26 | 0.099 | |||
| 9R9R | 4.38 | 1.85–10.36 | 0.001 | ||||
| 9R10R | 1.05 | 0.61–1.79 | 0.867 | ||||
| Onset | 1.04 | 1.01–1.07 | 0.014 |
| Variable | Univariant Analysis | MLR | |||||
|---|---|---|---|---|---|---|---|
| p | X2 | Nag R2 | OR | 95% CI | p | ||
| BMI | 14.38 | 0.076 | |||||
| MLGP 1 score | 0.011 | 0.81 | 0.69–0.95 | 0.010 | |||
| Onset | 0.066 | ||||||
| Illness duration | 0.008 | 0.97 | 0.94–0.99 | 0.007 | |||
| W | 21.80 | 0.099 | |||||
| MLGP score | 0.016 | 0.852 | 0.74–0.97 | 0.021 | |||
| Sex (Wo/M) | <0.001 | 2.92 | 1.70–4.99 | <0.001 | |||
| Age | 0.101 | ||||||
| Onset | 0.086 | ||||||
| Treatment time | 0.124 | ||||||
| DBP | 14.18 | 0.066 | |||||
| MLGP score | 0.012 | 0.82 | 0.71–0.94 | 0.006 | |||
| Age | 0.002 | 1.03 | 1.01–1.05 | 0.014 | |||
| Illness duration | 0.038 | ||||||
| Treatment time | 0.013 | ||||||
| AP daily doses | 0.070 | ||||||
| TG | 12.77 | 0.063 | |||||
| MLGP score | 0.002 | 0.83 | 0.72–0.96 | 0.014 | |||
| Onset | 0.028 | 1.04 | 1.01–1.07 | 0.015 | |||
| Tobacco use | 0.141 | ||||||
| Treatment time | 0.056 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arrue, A.; Olivas, O.; Erkoreka, L.; Alvarez, F.J.; Arnaiz, A.; Varela, N.; Bilbao, A.; Rodríguez, J.-J.; Moreno-Calle, M.T.; Gordo, E.; et al. Multilocus Genetic Profile Reflecting Low Dopaminergic Signaling Is Directly Associated with Obesity and Cardiometabolic Disorders Due to Antipsychotic Treatment. Pharmaceutics 2023, 15, 2134. https://doi.org/10.3390/pharmaceutics15082134
Arrue A, Olivas O, Erkoreka L, Alvarez FJ, Arnaiz A, Varela N, Bilbao A, Rodríguez J-J, Moreno-Calle MT, Gordo E, et al. Multilocus Genetic Profile Reflecting Low Dopaminergic Signaling Is Directly Associated with Obesity and Cardiometabolic Disorders Due to Antipsychotic Treatment. Pharmaceutics. 2023; 15(8):2134. https://doi.org/10.3390/pharmaceutics15082134
Chicago/Turabian StyleArrue, Aurora, Olga Olivas, Leire Erkoreka, Francisco Jose Alvarez, Ainara Arnaiz, Noemi Varela, Ainhoa Bilbao, Jose-Julio Rodríguez, María Teresa Moreno-Calle, Estibaliz Gordo, and et al. 2023. "Multilocus Genetic Profile Reflecting Low Dopaminergic Signaling Is Directly Associated with Obesity and Cardiometabolic Disorders Due to Antipsychotic Treatment" Pharmaceutics 15, no. 8: 2134. https://doi.org/10.3390/pharmaceutics15082134
APA StyleArrue, A., Olivas, O., Erkoreka, L., Alvarez, F. J., Arnaiz, A., Varela, N., Bilbao, A., Rodríguez, J.-J., Moreno-Calle, M. T., Gordo, E., Marín, E., Garcia-Cano, J., Saez, E., Gonzalez-Torres, M. Á., Zumárraga, M., & Basterreche, N. (2023). Multilocus Genetic Profile Reflecting Low Dopaminergic Signaling Is Directly Associated with Obesity and Cardiometabolic Disorders Due to Antipsychotic Treatment. Pharmaceutics, 15(8), 2134. https://doi.org/10.3390/pharmaceutics15082134