
An Overview of the Pharmacokinetics and Pharmacodynamics of Landiolol (an Ultra-Short Acting β1 Selective Antagonist) in Atrial Fibrillation

 ,
,  ,
, 
 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Overview of Pharmacodynamics and Pharmacokinetics in Comparison with Other β-Blockers
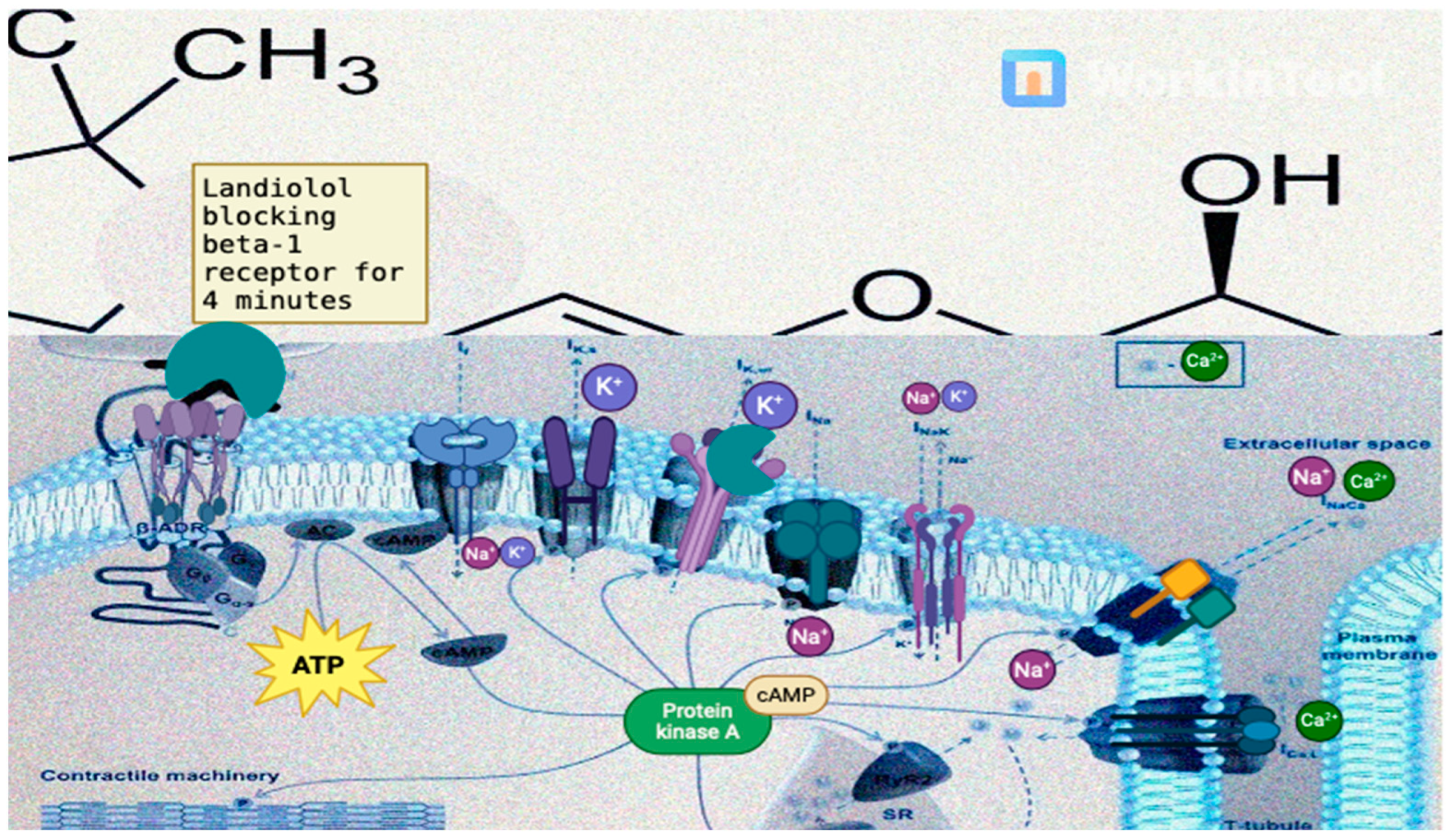
- G protein-coupled receptor signaling: β-1 adrenergic receptors are G protein-coupled receptors, meaning that their activation leads to the activation of intracellular signaling pathways through G proteins. When catecholamines (e.g., epinephrine and norepinephrine) bind to β-1 receptors, they activate stimulatory G proteins, leading to the production of cyclic adenosine monophosphate (cAMP) from adenosine triphosphate by the enzyme adenylyl cyclase;
- cAMP production: Cyclic AMP, a second messenger, plays a central role in mediating the effects of β-adrenergic receptor activation. Increased levels of cAMP lead to the activation of protein kinase A (PKA), a key enzyme involved in regulating cellular function. PKA phosphorylates a variety of target proteins, leading to changes in cellular function and gene expression, one of the major intracellular effects of β-1 receptor activation being the regulation of intracellular calcium levels in cardiac myocytes. The activation of β-1 receptors leads to an increase in intracellular calcium levels through several mechanisms, including enhanced calcium release from the sarcoplasmic reticulum and increased calcium entry through L-type calcium channels in the cell membrane. The increase in intracellular calcium levels and the subsequent activation of PKA through the ryanodine receptor 2, sarcoplasmic/endoplasmic reticulum calcium ATPase 2 and phospholamban lead to enhanced contractility and increased HR in cardiac myocytes [3,13,17,23].

- A negative bathmotropic effect—decreased cellular excitability (by inhibiting the effects of catecholamines on beta adrenergic receptors, which reduces the concentration of Ca2+ ions in the cytoplasm);
- A negative dromotropic effect (it decreases the speed of impulse conduction through the atrioventricular node by blocking IKs channels most notably);
- A negative chronotropic effect (blocking the β-1 receptors leading to a decrease in Ca2+ influx into cardiomyocytes during action potential, which is thus responsible for the negative inotropic effect);
- A negative inotropic effect—Due to its blockade of the β-1 receptors in the myocardium and in this way blocking the release of calcium, necessary for cardiomyocyte contraction;
- An antiarrhythmic effect—Due to its suppression of triggered activity and the prolongation of a refractory period by blocking IKs channels. In this way, it may help prevent the re-entry of electrical impulses that can lead to certain types of arrhythmias such as AF, AFL, atrioventricular re-entry tachycardia, or atrioventricular nodal reentry tachycardia [25].

{kind=link}
| Current Channel | If | IKs | INa | INaK |
|---|---|---|---|---|
| Role | A mixed cation current is carried by both Na+ and K+. It is mainly involved in the pacemaker activity of the sinoatrial node, contributing to the diastolic depolarization and spontaneous firing of action potentials. | A delayed rectifier potassium current plays a role in repolarizing the cardiac action potential. It contributes to the plateau phase of the action potential in cardiac myocytes. | The fast inward sodium current is responsible for the rapid depolarization phase of the cardiac action potential. It plays a critical role in initiating and propagating action potentials in cardiac myocytes. | The sodium–potassium pump (Na+/K+-ATPase) plays a crucial role in maintaining the resting membrane potential of cardiac myocytes by actively transporting 3 atoms of sodium out of the cell and 2 atoms of potassium into the cell. |
| The influence of landiolol 1 | Indirect—by blocking β-1 receptors, landiolol reduces the stimulatory effects of endogenous catecholamines, leading to a decrease in If activity and a subsequent decrease in heart rate. | May have minor effects on IKs, primarily through downstream signaling pathways influenced by the blockade of β-1 adrenergic receptors. | Indirect—by blocking β-1 receptors, landiolol reduces the stimulatory effects of catecholamines on INa, leading to a decrease in the rate of rise of the action potential and a reduction in myocardial excitability. | Not well-documented, its effects on intracellular calcium levels and ion handling in cardiac myocytes, mediated through β-1 receptor blockade, may indirectly influence the activity of the sodium–potassium pump. |
3. The Use of Landiolol in Clinical Practice
3.1. Postoperative Atrial Fibrillation Prevention and Treatment in Cardiac Surgery
3.2. Postoperative Atrial Fibrillation Prevention and Treatment in Non-Cardiac Surgery
3.3. Treatment of Atrial Fibrillation in Patients with Cardiac Dysfunction
3.4. Treatment of Sepsis-Related Atrial Fibrillation
4. Challenges and Perspectives
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Oancea, A.F.; Jigoranu, R.A.; Morariu, P.C.; Miftode, R.-S.; Trandabat, B.A.; Iov, D.E.; Cojocaru, E.; Costache, I.I.; Baroi, L.G.; Timofte, D.V.; et al. Atrial Fibrillation and Chronic Coronary Ischemia: A Challenging Vicious Circle. Life 2023, 13, 1370. [Google Scholar] [CrossRef]
- Kawakami, A.; Kobayashi, Y.; Katsube, T. Effect of Landiolol for Atrial Fibrillation after Open Heart Surgery. Jpn. J. Thorac. Surg. 2023, 75, 339–342. [Google Scholar]
- Atarashi, H. Pharmacokinetics of Landiolol Hydrochloride, a New Ultra-Short-Acting β-Blocker, in Patients with Cardiac Arrhythmias. Clin. Pharmacol. Ther. 2000, 68, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Krumpl, G.; Ulc, I.; Trebs, M.; Kadlecová, P.; Hodisch, J. Bolus Application of Landiolol and Esmolol: Comparison of the Pharmacokinetic and Pharmacodynamic Profiles in a Healthy Caucasian Group. Eur. J. Clin. Pharmacol. 2017, 73, 417–428. [Google Scholar] [CrossRef]
- Sugiura, S.; Seki, S.; Hidaka, K.; Masuoka, M.; Tsuchida, H. The Hemodynamic Effects of Landiolol, an Ultra-Short-Acting β1-Selective Blocker, on Endotracheal Intubation in Patients with and without Hypertension. Anesth. Analg. 2007, 104, 124–129. [Google Scholar] [CrossRef]
- Kinugawa, K.; Nagai, R.; Inoue, H.; Atarashi, H.; Seino, Y.; Yamashita, T.; Shimizu, W.; Aiba, T.; Kitakaze, M.; Sakamoto, A.; et al. Impacts of patient characteristics on the effectiveness of landiolol in AF/AFL patients complicated with LV dysfunction: Subgroup analysis of the J-Land study. Adv. Ther. 2014, 31, 426–439. [Google Scholar] [CrossRef]
- Tsuchiya, H.; Mizogami, M. Characteristic Interactivity of Landiolol, an Ultra-Short-Acting Highly Selective Β1-Blocker, with Biomimetic Membranes: Comparisons with Β1-Selective Esmolol and Non-Selective Propranolol and Alprenolol. Front. Pharmacol. 2013, 4, 150. [Google Scholar] [CrossRef]
- Kinjo, T.; Kimura, M.; Kaname, N.; Horiuchi, D.; Itoh, T.; Ishida, Y.; Nishizaki, K.; Toyama, Y.; Sasaki, S.; Tomita, H. Landiolol, an Intravenous Β1-selective Blocker, Is Useful for Dissociating a Fusion of Atrial Activation via Accessory Pathway and Atrioventricular Node. J. Arrhythm. 2023, 39, 937–946. [Google Scholar] [CrossRef] [PubMed]
- Nasrollahi-Shirazi, S.; Sucic, S.; Yang, Q.; Freissmuth, M.; Nanoff, C. Comparison of the -Adrenergic Receptor Antagonists Landiolol and Esmolol: Receptor Selectivity, Partial Agonism, and Pharmacochaperoning Actions. J. Pharmacol. Exp. Ther. 2016, 359, 73–81. [Google Scholar] [CrossRef]
- Matsumoto, S.; Tokumaru, O.; Ogata, K.; Kuribayashi, Y.; Oyama, Y.; Shingu, C.; Yokoi, I.; Kitano, T. Dose-Dependent Scavenging Activity of the Ultra-Short-Acting Β1-Blocker Landiolol against Specific Free Radicals. J. Clin. Biochem. Nutr. 2022, 71, 21–157. [Google Scholar] [CrossRef]
- Plosker, G.L. Landiolol: A review of its use in intraoperative and postoperative tachyarrhythmias. Drugs 2013, 73, 959–977. [Google Scholar] [CrossRef] [PubMed]
- Ikeshita, K.; Nishikawa, K.; Toriyama, S.; Yamashita, T.; Tani, Y.; Yamada, T.; Asada, A. Landiolol Has a Less Potent Negative Inotropic Effect than Esmolol in Isolated Rabbit Hearts. J. Anesth. 2008, 22, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Matsuishi, Y.; Mathis, B.J.; Shimojo, N.; Kawano, S.; Inoue, Y. Evaluating the Therapeutic Efficacy and Safety of Landiolol Hydrochloride for Management of Arrhythmia in Critical Settings: Review of the Literature. Vasc. Health Risk Manag. 2020, 16, 111–123. [Google Scholar] [CrossRef]
- Ojima, T.; Iwahashi, M.; Nakamori, M.; Nakamura, M.; Katsuda, M.; Iida, T.; Hayata, K.; Yamaue, H. Atrial Fibrillation after Esophageal Cancer Surgery: An Analysis of 207 Consecutive Patients. Surg. Today 2014, 44, 839–847. [Google Scholar] [CrossRef]
- Kimura-Kurosawa, S.; Kanaya, N.; Kamada, N.; Hirata, N.; Nakayama, M.; Namiki, A. Cardioprotective Effect and Mechanism of Action of Landiolol on the Ischemic Reperfused Heart. J. Anesth. 2007, 21, 480–489. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, A.; Hamasaki, T.; Kitakaze, M. Perioperative Landiolol Administration Reduces Atrial Fibrillation after Cardiac Surgery: A Meta-Analysis of Randomized Controlled Trials. Adv. Ther. 2014, 31, 440–450. [Google Scholar] [CrossRef] [PubMed]
- Murakami, M.; Furuie, H.; Matsuguma, K.; Wanibuchi, A.; Kikawa, S.; Irie, S. Pharmacokinetics and Pharmacodynamics of Landiolol Hydrochloride, an Ultra Short-Acting Β1-Selective Blocker, in a Dose Escalation Regimen in Healthy Male Volunteers. Drug Metab. Pharmacokinet. 2005, 20, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Kiyokuni, M.; Konishi, M.; Sakamaki, K.; Kawashima, C.; Narikawa, M.; Doi, H.; Iwata, K.; Tomari, S.; Nakayama, N.; Komura, N.; et al. Beneficial Effect of Early Infusion of Landiolol, a Very Short-Acting Beta-1 Adrenergic Receptor Blocker, on Reperfusion Status in Acute Myocardial Infarction. Int. J. Cardiol. 2016, 221, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Hoshi, T.; Sato, A.; Nishina, H.; Kakefuda, Y.; Wang, Z.; Noguchi, Y.; Aonuma, K. Acute Hemodynamic Effects of Landiolol, an Ultra-Short-Acting Beta-Blocker, in Patients with Acute Coronary Syndrome: Preliminary Study. J. Cardiol. 2012, 60, 252–256. [Google Scholar] [CrossRef]
- Morelli, A.; Ertmer, C.; Westphal, M.; Rehberg, S.; Kampmeier, T.; Ligges, S.; Orecchioni, A.; D’Egidio, A.; D’Ippoliti, F.; Raffone, C.; et al. Effect of Heart Rate Control with Esmolol on Hemodynamic and Clinical Outcomes in Patients with Septic Shock. JAMA 2013, 310, 1683. [Google Scholar] [CrossRef]
- Seki, Y.; Jesmin, S.; Shimojo, N.; Islam, M.M.; Rahman, M.A.; Khatun, T.; Sakuramoto, H.; Oki, M.; Sonobe, A.; Kamiyama, J.; et al. Significant Reversal of Cardiac Upregulated Endothelin-1 System in a Rat Model of Sepsis by Landiolol Hydrochloride. Life Sci. 2014, 118, 357–363. [Google Scholar] [CrossRef]
- Schroeder, L.; Monno, P.; Unger, M.; Ackerl, J.; Shatilova, O.; Schmitt, J.; Dresbach, T.; Mueller, A.; Kipfmueller, F. Heart Rate Control with Landiolol Hydrochloride in Infants with Ventricular Dysfunction and Pulmonary Hypertension. ESC Heart Fail. 2023, 10, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Chalkias, A.; O’Donnell, E.P. Mechanisms of Landiolol-Mediated Positive Inotropy in Critical Care Settings. Eur. J. Clin. Pharmacol. 2023, 79, 1607–1612. [Google Scholar] [CrossRef]
- Oliver, E.; Mayor, F., Jr.; D’Ocon, P. Beta-Blockers: Historical Perspective and Mechanisms of Action. Rev. Española Cardiol. (Engl. Ed.) 2019, 72, 853–862. [Google Scholar] [CrossRef]
- Grandi, E.; Ripplinger, C.M. Antiarrhythmic Mechanisms of Beta Blocker Therapy. Pharmacol. Res. 2019, 146, 104274. [Google Scholar] [CrossRef] [PubMed]
- Poveda-Jaramillo, R.; Monaco, F.; Zangrillo, A.; Landoni, G. Ultra-Short–Acting β-Blockers (Esmolol and Landiolol) in the Perioperative Period and in Critically Ill Patients. J. Cardiothorac. Vasc. Anesth. 2018, 32, 1415–1425. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.; Awosika, A.O.; Dunham, A. Metoprolol. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- AlHabeeb, W.; Mrabeti, S.; Abdelsalam, A.A.I. Therapeutic Properties of Highly Selective β-Blockers with or without Additional Vasodilator Properties: Focus on Bisoprolol and Nebivolol in Patients with Cardiovascular Disease. Cardiovasc. Drugs Ther. 2022, 36, 959–971. [Google Scholar] [CrossRef] [PubMed]
- Kirch, W.; Görg, K.G. Clinical Pharmacokinetics of Atenolol—A Review. Eur. J. Drug Metab. Pharmacokinet. 1982, 7, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Wisler, J.W.; DeWire, S.M.; Whalen, E.J.; Violin, J.D.; Drake, M.T.; Ahn, S.; Shenoy, S.K.; Lefkowitz, R.J. A Unique Mechanism of β-Blocker Action: Carvedilol Stimulates β-Arrestin Signaling. Proc. Natl. Acad. Sci. USA 2007, 104, 16657–16662. [Google Scholar] [CrossRef]
- Lewis, P. The Essential Action of Propranolol in Hypertension. Am. J. Med. 1976, 60, 837–852. [Google Scholar] [CrossRef]
- Sezai, A.; Osaka, S.; Yaoita, H.; Ishii, Y.; Arimoto, M.; Hata, H.; Shiono, M. Safety and Efficacy of Landiolol Hydrochloride for Prevention of Atrial Fibrillation after Cardiac Surgery in Patients with Left Ventricular Dysfunction: Prevention of Atrial Fibrillation after Cardiac Surgery with Landiolol Hydrochloride for Left Ventricular Dysfunction (PLATON) Trial. J. Thorac. Cardiovasc. Surg. 2015, 150, 957–964. [Google Scholar] [CrossRef] [PubMed]
- Sezai, A.; Minami, K.; Nakai, T.; Hata, M.; Yoshitake, I.; Wakui, S.; Shiono, M.; Hirayama, A. Landiolol Hydrochloride for Prevention of Atrial Fibrillation after Coronary Artery Bypass Grafting: New Evidence from the PASCAL Trial. J. Thorac. Cardiovasc. Surg. 2011, 141, 1478–1487. [Google Scholar] [CrossRef]
- Sezai, A.; Nakai, T.; Hata, M.; Yoshitake, I.; Shiono, M.; Kunimoto, S.; Hirayama, A. Feasibility of Landiolol and Bisoprolol for Prevention of Atrial Fibrillation after Coronary Artery Bypass Grafting: A Pilot Study. J. Thorac. Cardiovasc. Surg. 2012, 144, 1241–1248. [Google Scholar] [CrossRef] [PubMed]
- Hagiwara, S.; Iwasaka, H.; Maeda, H.; Noguchi, T. Landiolol, an Ultrashort-Acting β1-Adrenoceptor Antagonist, Has Protective Effects in an Lps-Induced Systemic Inflammation Model. Shock 2009, 31, 515–520. [Google Scholar] [CrossRef]
- Oprea, A.D.; Lombard, F.W.; Kertai, M.D. Perioperative β-Adrenergic Blockade in Noncardiac and Cardiac Surgery: A Clinical Update. J. Cardiothorac. Vasc. Anesth. 2019, 33, 817–832. [Google Scholar] [CrossRef]
- January, C.T.; Wann, L.S.; Alpert, J.S.; Calkins, H.; Cigarroa, J.E.; Cleveland, J.C.; Conti, J.B.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; et al. 2014 AHA/ACC/HRS Guideline for the Management of Patients with Atrial Fibrillation: Executive Summary. Circulation 2014, 130, 2071–2104. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation Developed in Collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Arsenault, K.A.; Yusuf, A.M.; Crystal, E.; Healey, J.S.; Morillo, C.A.; Nair, G.M.; Whitlock, R.P. Interventions for Preventing Post-Operative Atrial Fibrillation in Patients Undergoing Heart Surgery. Cochrane Database Syst. Rev. 2013, 2013, CD003611. [Google Scholar] [CrossRef] [PubMed]
- Thein, P.M.; White, K.; Banker, K.; Lunny, C.; Mirzaee, S.; Nasis, A. Preoperative Use of Oral Beta-Adrenergic Blocking Agents and the Incidence of New-Onset Atrial Fibrillation After Cardiac Surgery. A Systematic Review and Meta-Analysis. Heart Lung Circ. 2018, 27, 310–321. [Google Scholar] [CrossRef]
- Fellahi, J.-L.; Heringlake, M.; Knotzer, J.; Fornier, W.; Cazenave, L.; Guarracino, F. Landiolol for Managing Atrial Fibrillation in Post-Cardiac Surgery. Eur. Heart J. Suppl. 2018, 20, A4–A9. [Google Scholar] [CrossRef]
- Sasaki, K.; Kumagai, K.; Maeda, K.; Akiyama, M.; Ito, K.; Matsuo, S.; Katahira, S.; Suzuki, T.; Suzuki, Y.; Kaiho, Y.; et al. Preventive Effect of Low-Dose Landiolol on Postoperative Atrial Fibrillation Study (PELTA Study). Gen. Thorac. Cardiovasc. Surg. 2020, 68, 1240–1251. [Google Scholar] [CrossRef] [PubMed]
- Hao, J.; Zhou, J.; Xu, W.; Chen, C.; Zhang, J.; Peng, H.; Liu, L. Beta-Blocker Landiolol Hydrochloride in Preventing Atrial Fibrillation Following Cardiothoracic Surgery: A Systematic Review and Meta-Analysis. Ann. Thorac. Cardiovasc. Surg. 2022, 28, 18–31. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, A.; Kitakaze, M.; Takamoto, S.; Namiki, A.; Kasanuki, H.; Hosoda, S. Landiolol, an Ultra-Short-Acting Β1-Blocker, More Effectively Terminates Atrial Fibrillation than Diltiazem after Open Heart Surgery: Prospective, Multicenter, Randomized, Open-Label Study (JL-KNIGHT Study). Circ. J. 2012, 76, 1097–1101. [Google Scholar] [CrossRef] [PubMed]
- Ji, T.; Feng, C.; Sun, L.; Ye, X.; Bai, Y.; Chen, Q.; Qin, Y.; Zhu, J.; Zhao, X. Are Beta-Blockers Effective for Preventing Post-Coronary Artery Bypass Grafting Atrial Fibrillation? Direct and Network Meta-Analyses. Ir. J. Med. Sci. 2016, 185, 503–511. [Google Scholar] [CrossRef]
- Yoshioka, I.; Sakurai, M.; Namai, A.; Kawamura, T. Postoperative Treatment of Carvedilol Following Low Dose Landiolol Has Preventive Effect for Atrial Fibrillation after Coronary Artery Bypass Grafting. Thorac. Cardiovasc. Surg. 2009, 57, 464–467. [Google Scholar] [CrossRef]
- Balik, M.; Sander, M.; Trimmel, H.; Heinz, G. Landiolol for Managing Post-Operative Atrial Fibrillation. Eur. Heart J. Suppl. 2018, 20, A10–A14. [Google Scholar] [CrossRef]
- Nakano, T.; Shimizu, K.; Kawashima, O.; Kamiyoshihara, M.; Nagashima, T.; Ibe, T.; Takeyoshi, I. Effect of Landiolol Hydrochloride, an Ultra-Short-Acting Beta 1-Selective Blocker, on Supraventricular Tachycardia, Atrial Fibrillation and Flutter after Pulmonary Resection. J. Clin. Pharm. Ther. 2012, 37, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Nojiri, T.; Yamamoto, K.; Maeda, H.; Takeuchi, Y.; Funakoshi, Y.; Maekura, R.; Okumura, M. Efficacy of Low-Dose Landiolol, an Ultrashort-Acting β-Blocker, on Postoperative Atrial Fibrillation in Patients Undergoing Pulmonary Resection for Lung Cancer. Gen. Thorac. Cardiovasc. Surg. 2011, 59, 799–805. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Nozaki, M.; Sakamoto, R.; Suzuki, T.; Masuda, R.; Iwazaki, M. Safety of Landiolol Infusion in Patients Undergoing Lung Resection. Open J. Anesthesiol. 2014, 4, 183–190. [Google Scholar] [CrossRef]
- Aoyama, H.; Otsuka, Y.; Aoyama, Y. Landiolol Infusion during General Anesthesia Does Not Prevent Postoperative Atrial Fibrillation in Patients Undergoing Lung Resection. Gen. Thorac. Cardiovasc. Surg. 2016, 64, 735–741. [Google Scholar] [CrossRef]
- Yoshida, T.; Furukita, Y.; Yamamoto, Y.; Nishino, T.; Inoue, S.; Morimoto, M.; Okumura, K.; Toba, H.; Yoshida, M.; Takizawa, H.; et al. A Randomized, Open Label Study of the Efficacy of Prophylactic 24-h Low-Dose Landiolol for Atrial Fibrillation in Transthoracic Esophagectomy. Esophagus 2017, 14, 97–103. [Google Scholar] [CrossRef]
- Okita, T.; Uji, M.; Shinjo, T.; Morioka, M.; Kumano, H.; Ishimura, N.; Nishiwada, M. Use of Landiolol Hydrochloride for the Prevention of Atrial Fibrillation after Lung Resection. Masui 2008, 57, 953–958. [Google Scholar] [PubMed]
- Mori, K.; Yamada, K.; Fukuda, T.; Mitsui, T.; Kitamura, T.; Yamaguchi, D.; Ando, J.; Wada, I.; Nomura, S.; Shimizu, N.; et al. Landiolol Hydrochloride for Early Postoperative Tachycardia after Transthoracic Esophagectomy. Surg. Today 2014, 44, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Niwa, Y.; Koike, M.; Iwata, N.; Kobayashi, D.; Tanaka, C.; Fujii, T.; Nakayama, G.; Sugimoto, H.; Fujiwara, M.; Kodera, Y. Effect of Landiolol Hydrochloride on Tachyarrhythmia after Esophagectomy. Hepatogastroenterology 2014, 61, 1546–1551. [Google Scholar]
- Wariishi, S.; Yamashita, K.; Nishimori, H.; Fukutomi, T.; Yamamoto, M.; Radhakrishnan, G.; Sasaguri, S. Postoperative Administration of Landiolol Hydrochloride for Patients with Supraventricular Arrhythmia: The Efficacy of Sustained Intravenous Infusion at a Low Dose. Interact. Cardiovasc. Thorac. Surg. 2009, 9, 811–813. [Google Scholar] [CrossRef] [PubMed]
- Ojima, T.; Nakamori, M.; Nakamura, M.; Katsuda, M.; Hayata, K.; Kato, T.; Kitadani, J.; Tabata, H.; Takeuchi, A.; Yamaue, H. Randomized Clinical Trial of Landiolol Hydrochloride for the Prevention of Atrial Fibrillation and Postoperative Complications after Oesophagectomy for Cancer. Br. J. Surg. 2017, 104, 1003–1009. [Google Scholar] [CrossRef] [PubMed]
- Bezati, S.; Velliou, M.; Polyzogopoulou, E.; Boultadakis, A.; Parissis, J. The Role of Landiolol in the Management of Atrial Tachyarrhythmias in Patients with Acute Heart Failure and Cardiogenic Shock: Case Reports and Review of Literature. Eur. Heart J. Suppl. 2022, 24, D22–D33. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Okajima, M.; Takamura, M.; Taniguchi, T. Landiolol, an Ultra-Short-Acting Β1-Blocker, Is Useful for Managing Supraventricular Tachyarrhythmias in Sepsis. World J. Crit. Care Med. 2015, 4, 251. [Google Scholar] [CrossRef]
- Rehberg, S.; Joannidis, M.; Whitehouse, T.; Morelli, A. Landiolol for Managing Atrial Fibrillation in Intensive Care. Eur. Heart J. Suppl. 2018, 20, A15–A18. [Google Scholar] [CrossRef]
- Nagai, R.; Kinugawa, K.; Inoue, H.; Atarashi, H.; Seino, Y.; Yamashita, T.; Shimizu, W.; Aiba, T.; Kitakaze, M.; Sakamoto, A.; et al. Urgent Management of Rapid Heart Rate in Patients with Atrial Fibrillation/Flutter and Left Ventricular Dysfunction—Comparison of the Ultra-Short-Acting Β1-Selective Blocker Landiolol with Digoxin (J-Land Study). Circ. J. 2013, 77, 908–916. [Google Scholar] [CrossRef] [PubMed]
- Wada, Y.; Aiba, T.; Tsujita, Y.; Itoh, H.; Wada, M.; Nakajima, I.; Ishibashi, K.; Okamura, H.; Miyamoto, K.; Noda, T.; et al. Practical Applicability of Landiolol, an Ultra-Short-Acting Β1-Selective Blocker, for Rapid Atrial and Ventricular Tachyarrhythmias with Left Ventricular Dysfunction. J. Arrhythm. 2016, 32, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Iwahashi, N.; Takahashi, H.; Abe, T.; Okada, K.; Akiyama, E.; Matsuzawa, Y.; Konishi, M.; Maejima, N.; Hibi, K.; Kosuge, M.; et al. Urgent Control of Rapid Atrial Fibrillation by Landiolol in Patients with Acute Decompensated Heart Failure with Severely Reduced Ejection Fraction. Circ. Rep. 2019, 1, 422–430. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Myoren, T.; Kajii, T.; Kohno, M.; Nanno, T.; Ishiguchi, H.; Nishimura, S.; Fukuda, M.; Hino, A.; Fujimura, T.; et al. Addition of a Β1-Blocker to Milrinone Treatment Improves Cardiac Function in Patients with Acute Heart Failure and Rapid Atrial Fibrillation. Cardiology 2019, 142, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Kakihana, Y.; Nishida, O.; Taniguchi, T.; Okajima, M.; Morimatsu, H.; Ogura, H.; Yamada, Y.; Nagano, T.; Morishima, E.; Matsuda, N. Efficacy and Safety of Landiolol, an Ultra-Short-Acting Β1-Selective Antagonist, for Treatment of Sepsis-Related Tachyarrhythmia (J-Land 3S): A Multicentre, Open-Label, Randomised Controlled Trial. Lancet Respir. Med. 2020, 8, 863–872. [Google Scholar] [CrossRef]
- Matsuda, N.; Nishida, O.; Taniguchi, T.; Okajima, M.; Morimatsu, H.; Ogura, H.; Yamada, Y.; Nagano, T.; Ichikawa, A.; Kakihana, Y. Impact of Patient Characteristics on the Efficacy and Safety of Landiolol in Patients with Sepsis-Related Tachyarrhythmia: Subanalysis of the J-Land 3S Randomised Controlled Study. eClinicalMedicine 2020, 28, 100571. [Google Scholar] [CrossRef] [PubMed]
- Unger, M.; Morelli, A.; Singer, M.; Radermacher, P.; Rehberg, S.; Trimmel, H.; Joannidis, M.; Heinz, G.; Cerny, V.; Dostál, P.; et al. Landiolol in Patients with Septic Shock Resident in an Intensive Care Unit (LANDI-SEP): Study Protocol for a Randomized Controlled Trial. Trials 2018, 19, 637. [Google Scholar] [CrossRef]
- Lescroart, M.; Pequignot, B.; Kimmoun, A.; Klein, T.; Levy, B. Beta-Blockers in Septic Shock: What Is New? J. Intensive Med. 2022, 2, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Morisaki, H.; Serita, R.; Yamamoto, M.; Kotake, Y.; Ishizaka, A.; Takeda, J. Infusion of the β-Adrenergic Blocker Esmolol Attenuates Myocardial Dysfunction in Septic Rats. Crit. Care Med. 2005, 33, 2294–2301. [Google Scholar] [CrossRef]
- Aboab, J.; Sebille, V.; Jourdain, M.; Mangalaboyi, J.; Gharbi, M.; Mansart, A.; Annane, D. Effects of Esmolol on Systemic and Pulmonary Hemodynamics and on Oxygenation in Pigs with Hypodynamic Endotoxin Shock. Intensive Care Med. 2011, 37, 1344–1351. [Google Scholar] [CrossRef]
- Kimmoun, A.; Louis, H.; Al Kattani, N.; Delemazure, J.; Dessales, N.; Wei, C.; Marie, P.Y.; Issa, K.; Levy, B. Β1-Adrenergic Inhibition Improves Cardiac and Vascular Function in Experimental Septic Shock. Crit. Care Med. 2015, 43, e332–e340. [Google Scholar] [CrossRef] [PubMed]
- Syed, Y.Y. Landiolol: A Review in Tachyarrhythmias. Drugs 2018, 78, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, T.; Nakasu, Y.; Mizutani, H.; Sumitani, K. A Prospective Observational Survey on Landiolol in Atrial Fibrillation/Atrial Flutter Patients with Chronic Heart Failure—AF-CHF Landiolol Survey. J. Cardiol. 2019, 74, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, T.; Saitoh, T.; Matsushita, M. Design of a Prospective Observational Survey on Landiolol in Atrial Fibrillation/Atrial Flutter Patients with Chronic Heart Failure—AF-CHF Landiolol Survey. J. Cardiol. 2015, 66, 69–72. [Google Scholar] [CrossRef] [PubMed]
- Stix, G.; Wolzt, M.; Domanovits, H.; Kadlecová, P.; Husch, B.; Trebs, M.; Hodisch, J.; Unger, M.; Krumpl, G. Open-Label Two-Dose Pilot Study of Landiolol for the Treatment of Atrial Fibrillation/Atrial Flutter in Caucasian Patients. Circ. J. 2019, 84, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Shibata, S.C.; Uchiyama, A.; Ohta, N.; Fujino, Y. Efficacy and Safety of Landiolol Compared to Amiodarone for the Management of Postoperative Atrial Fibrillation in Intensive Care Patients. J. Cardiothorac. Vasc. Anesth. 2016, 30, 418–422. [Google Scholar] [CrossRef] [PubMed]
- Horikoshi, Y.; Goyagi, T.; Kudo, R.; Kodama, S.; Horiguchi, T.; Nishikawa, T. The Suppressive Effects of Landiolol Administration on the Occurrence of Postoperative Atrial Fibrillation and Tachycardia, and Plasma IL-6 Elevation in Patients Undergoing Esophageal Surgery: A Randomized Controlled Clinical Trial. J. Clin. Anesth. 2017, 38, 111–116. [Google Scholar] [CrossRef]
- Schnaubelt, S.; Eibensteiner, F.; Oppenauer, J.; Tihanyi, D.; Neymayer, M.; Brock, R.; Kornfehl, A.; Veigl, C.; Al Jalali, V.; Anders, S.; et al. Hemodynamic and Rhythmologic Effects of Push-Dose Landiolol in Critical Care—A Retrospective Cross-Sectional Study. Pharmaceuticals 2023, 16, 134. [Google Scholar] [CrossRef]
- Matsuishi, Y.; Jesmin, S.; Kawano, S.; Hideaki, S.; Shimojo, N.; Mowa, C.N.; Akhtar, S.; Zaedi, S.; Khatun, T.; Tsunoda, Y.; et al. Landiolol Hydrochloride Ameliorates Acute Lung Injury in a Rat Model of Early Sepsis through the Suppression of Elevated Levels of Pulmonary Endothelin-1. Life Sci. 2016, 166, 27–33. [Google Scholar] [CrossRef]
| Property | Landiolol [26] | Esmolol [26] | Metoprolol [27] | Nebivolol [28] | Bisoprolol [28] | Atenolol [29] | Carvedilol [30] | Propranolol [31] |
|---|---|---|---|---|---|---|---|---|
| Drug class | Ultra-short-acting selective β-1 blocker | Short-acting selective β-1 blocker | Selective β-1 blocker | Highly cardio selective β-1 blocker with vasodilator properties | Highly cardio-selective β-1 blocker | Cardio selective β-1 blocker | Non-selective β blocker with alpha-1 blocking activity | Non-selective β blocker |
| Half-life | Very short (about 4 min) | Very short (about 9 min) | 3–7 h | 10–12 h | 10–12 h | 6–7 h | 7–10 h | 4–6 h |
| Pharmacokinetics | Rapid onset and offset of action | Rapid onset and offset of action | Rapidly and completely absorbed | Absorbed rapidly and extensively metabolized | Slowly and completely absorbed | Absorbed slowly but almost completely | Extensive l y metabolized | Rapidly and completely absorbed |
| Pharmacodynamics | Selective β1-blocker, short-acting | Selective β1-blocker, short-acting | Selective β1-blocker, long-acting | β1-blocker with vasodilator effects | Selective β1-blocker, long-acting | Selective β1-blocker, long-acting | Non-selective β-blocker with β1-blockade | Non-selective β-blocker, membrane-stabilizing activity |
| Cardio selectivity | Highly | Highly | Highly | Highly with vasodilator properties | Highly | Highly | Non-selective | Non-selective |
| Dose Range | 1–40 μg/kg/min | 50–300 μg/kg/min | 25–200 mg/day | 2.5–10 mg/day | 2.5–10 mg/day | 25–100 mg/day | 6.25–25 mg/day | 20–320 mg/day |
| Vasodilator effects | Minimal | Minimal | Minimal | Significant | Minimal | Minimal | Strong | Minimal |
| Indications | Rapid heart rate control in critical care settings | Acute heart rate control, intraoperative and postoperative tachycardia | Hypertension, angina, heart failure, post-myocardial infarction | Hypertension, angina, heart failure | Hypertension, angina, heart failure | Hypertension, angina, arrhythmias | Hypertension, angina, heart failure | Hypertension, angina, arrhythmias |
| Adverse effects | Rarely hypotension, bradycardia | Hypotension, bradycardia, bronchospasm | Hypotension, bradycardia, fatigue, dizziness | Hypotension, bradycardia, fatigue, dizziness, headache | Hypotension, bradycardia, fatigue, dizziness | Hypotension, bradycardia, fatigue, dizziness | Hypotension, bradycardia, fatigue, dizziness, heart block | Hypotension, bradycardia, fatigue, dizziness, bronchospasm |
| Contraindication | Severe bradycardia, heart block | Heart block, severe bradycardia, heart failure, asthma | Bradycardia, heart block, heart failure, hypotension | Severe bradycardia, heart block, hepatic impairment | Heart block, severe bradycardia, heart failure, asthma | Bradycar dia, heart block, heart failure, asthma | Asthma, heart block, severe bradycard ia | Asthma, heart block, bradycardia |
| Study Name | Type of Surgery | Number of Patients | Design Study | Outcomes |
|---|---|---|---|---|
| Nojiri et al. [49] | Lung surgery | 30 | Study group (n = 15)—landiolol 5 mcg/kg/min or 10 mcg/kg/min Control group (n = 15)—0.25 mg digoxin and 5 mg verapamil | Rate of conversion to SR Study group: at 2 h 8/15 (53%) at 12 h 11/15 (73%) Control group: at 2 h 3/15 (20%) at 12 h 8/15 (53%) Time of conversion to SR Study group: 8.1 ± 11.0 h Control group: 23.0 ± 26.0 h |
| Niwa et al. [55] | Esophagectomy | 24 | Study group (n = 11)—landiolol 6.5 ± 3.4 mcg/kg/min, increased to 7.7 ± 4.4 mcg/kg/min Control group (n = 13)—digoxin and calcium channel blockers. | Rate of conversion to SR Study group: at 2 h 5/8 (62.5%) at 12 h 8/8 (100%) Control group: at 2 h at 2 h 1/13 (7.7%) at 12 h 7/13 (53.8%) Time of conversion to SR Study group: 3.6 6 ± 6.6 h Control group: 23.3 ± 5.2 h |
| Mori et al. [54] | Esophagectomy | 74 | Study group (n = 13)—landiolol 0.01 mg/kg/min increased to 0.04 mg/kg/min | Rate of conversion to SR: 10/13 (77%) |
| Nakano et al. [48] | Pulmonary resection | 25 | Study group (n = 25)—landiolol 5–10 mcg/kg/min or o 1–5 mcg/kg/min | Rate of conversion to SR: 14/25 (56%)—at 1 h 4/14 (28.6%) and at 12 h 5/14 (35.7%) HR control: from 135 ± 24 bpm to 85 ± 19 bpm |
| Hypotension [32,42,63,64,75,76] | Dyspnea [75] |
| Bradycardia [64,75,77] | Asthma [62] |
| Aggravation of cardiac failure [64,66,75] | Hypokalemia [74] |
| Ventricular tachycardia [75] | Hypoglycemia [74] |
| Complete atrioventricular block [64,73] | Hepatic enzyme increased [73,74] |
| Cardiorespiratory arrest [66,75] | Gamma-glutamyl transferase [74] |
| Cardiogenic shock [73,75] | Blood uric acid increased [74] |
| Embolic stroke [62] | Blood alkaline phosphatase increased [74] |
| Pneumonia [49,75] | Increased serum creatinine [64,76] |
| Respiratory failure [49,75] | Vomiting and nausea [62] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Floria, M.; Oancea, A.F.; Morariu, P.C.; Burlacu, A.; Iov, D.E.; Chiriac, C.P.; Baroi, G.L.; Stafie, C.S.; Cuciureanu, M.; Scripcariu, V.; et al. An Overview of the Pharmacokinetics and Pharmacodynamics of Landiolol (an Ultra-Short Acting β1 Selective Antagonist) in Atrial Fibrillation. Pharmaceutics 2024, 16, 517. https://doi.org/10.3390/pharmaceutics16040517
Floria M, Oancea AF, Morariu PC, Burlacu A, Iov DE, Chiriac CP, Baroi GL, Stafie CS, Cuciureanu M, Scripcariu V, et al. An Overview of the Pharmacokinetics and Pharmacodynamics of Landiolol (an Ultra-Short Acting β1 Selective Antagonist) in Atrial Fibrillation. Pharmaceutics. 2024; 16(4):517. https://doi.org/10.3390/pharmaceutics16040517
Chicago/Turabian StyleFloria, Mariana, Alexandru Florinel Oancea, Paula Cristina Morariu, Alexandru Burlacu, Diana Elena Iov, Cristina Petronela Chiriac, Genoveva Livia Baroi, Celina Silvia Stafie, Magdalena Cuciureanu, Viorel Scripcariu, and et al. 2024. "An Overview of the Pharmacokinetics and Pharmacodynamics of Landiolol (an Ultra-Short Acting β1 Selective Antagonist) in Atrial Fibrillation" Pharmaceutics 16, no. 4: 517. https://doi.org/10.3390/pharmaceutics16040517