
Intranasal Therapy in Palliative Care


1
Department of Emergency Medicine, Faculty of Health Science, Medical University of Gdansk, Mariana Smoluchowskiego Street 17, 80-214 Gdansk, Poland
2
Hospice Foundation, Kopernika Street 6, 80-208 Gdansk, Poland
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Pharmaceutics 2024, 16(4), 519; https://doi.org/10.3390/pharmaceutics16040519
Submission received: 28 February 2024
/
Revised: 28 March 2024
/
Accepted: 30 March 2024
/
Published: 9 April 2024
(This article belongs to the Special Issue Nasal Drug Delivery: Challenges and Future Opportunities)
Abstract
:In recent years, the use of the intranasal route has been actively explored as a possible drug delivery method in the palliative patient population. There are reports demonstrating the effectiveness of nasally administered medications that are routinely used in patients at the end of life. The subject of this study is the intranasal drug administration among palliative patients. The aim is to summarize currently used intranasal therapies among palliative patients, determine the benefits and difficulties, and identify potential areas for future research. A review of available medical literature published between 2013 and 2023 was performed using online scientific databases. The following descriptors were used when searching for articles: “palliative”, “intranasal”, “nasal”, “end-of-life care”, “intranasal drug delivery” and “nasal drug delivery”. Out of 774 articles, 55 directly related to the topic were finally selected and thoroughly analyzed. Based on the bibliographic analysis, it was shown that drugs administered intranasally may be a good, effective, and convenient form of treatment for patients receiving palliative care, in both children and adults. This topic requires further, high-quality clinical research.
1. Introduction
There is an increasing interest in non-invasive drug administration around the world [1]. Modern therapies are expected to be safe, non-invasive, and effective. The method of drug administration should be easy to use, well tolerated by the patient, and result in achieving the expected drug concentration in the target tissue. The above promotes satisfactory cooperation with the patient [2,3].
One of the most intensively researched methods of drug delivery is the intranasal route. It enables effective transport of substances directly to the brain and systemic circulation, provided that appropriate chemicals are used [4,5]. In recent years, the area of knowledge regarding the supply of drugs via the transmucosal route, especially intranasal, has been rapidly developing [6,7,8,9]. The intranasal route of drug administration has great potential and promising prospects for further development. Intranasal administration was studied in the treatment of a wide variety of ailments and diseases, such as depression [6], eating disorders [7], obesity [8], hormonal disorders, treatment of primary brain tumors [9], neurodegenerative processes (Parkinson’s disease [7], Alzheimer’s disease [10], Huntington’s disease [11]), coagulation disorders [12,13], treatment of infections (vaccines [14]), migraine [15], and addictions [4]. There are also reports describing the use of systemic treatment by the intranasal route among palliative care patients [16]. There is a growing demand for alternative methods of drug administration for patients at the end of life [2]. One factor behind the increased interest in alternative routes of drug administration in palliative care, especially among community-based settings, was the coronavirus (COVID-19) pandemic [17].
Palliative care patients are those receiving symptomatic treatment for a life-limiting illness [18]. The term “palliative care patient” most often refers to patients with advanced or metastatic cancer. However, it is worth distinguishing a group of non-cancer diseases that lead to a terminal condition, which include the following, among others: end-stage renal failure, severe liver failure, or progressive and incurable neurological conditions [19]. Patients at the end-of-life experience similar problems and distressing symptoms. Dyspnea, pain, and agitation are often observed [20,21]. Depression and anxiety are common. An inability to carry out daily activities, including taking scheduled medication is observed. The care of a terminally ill patient is mainly the responsibility of the family, relatives, and health care professionals [22]. Considering the wide use of intranasal route in different medical conditions, it appears that the group of palliative care patients could benefit significantly from this form of drug administration [2].
The aim of this review is to summarize currently used intranasal therapies among palliative patients. The objective of this publication is also to outline the benefits and difficulties associated with the use of intranasal medications for symptomatic treatment in a group of patients undergoing palliative treatment. Another goal is to identify potential areas for future research on intranasal therapy in terminal care patients.
2. Materials and Methods
The available bibliography on the research topic was reviewed. The study was conducted from December 2023 to February 2024. The following descriptors: “palliative” and “intranasal”, “palliative” and “nasal”, “oncology” and “intranasal”, “end-of-life care” and “intranasal drug delivery” and “nasal drug delivery” were used to search online databases such as MEDLINE Complete, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic reviews, Cochrane Methodology Register. At this stage, the following criteria were included: papers available in full-text versions, concerning children or adults and written in English. Due to the fact that we wanted to summarize the most up-to-date medical knowledge, an important criterion for selecting articles was the date of publication from the beginning of 2013 to the end of 2023.
The articles obtained during the search were initially selected based on their title and an analysis of the content of the abstract. Duplicate articles were removed. To select the final group, the remaining articles were read in their entirety and the same inclusion criteria were applied as before. This allowed us to exclude publications repeating the same conclusions as well as those that did not apply to the group of patients under study. The search and selection process were carried out by two independent researchers, and any disagreements were resolved by consensus. Out of 774 articles, 55 directly related to the topic were finally selected and thoroughly analyzed. The process of selecting articles from identification in the database to inclusion in the review is presented in Table 1.
Two independent researchers processed and synthesized the data. The included works were critically analyzed, and the results were interpreted and assessed. During this process, data were obtained to answer the research questions included in the objectives of our review.
3. The Nasal Cavity as a Promising Space for Drug Delivery
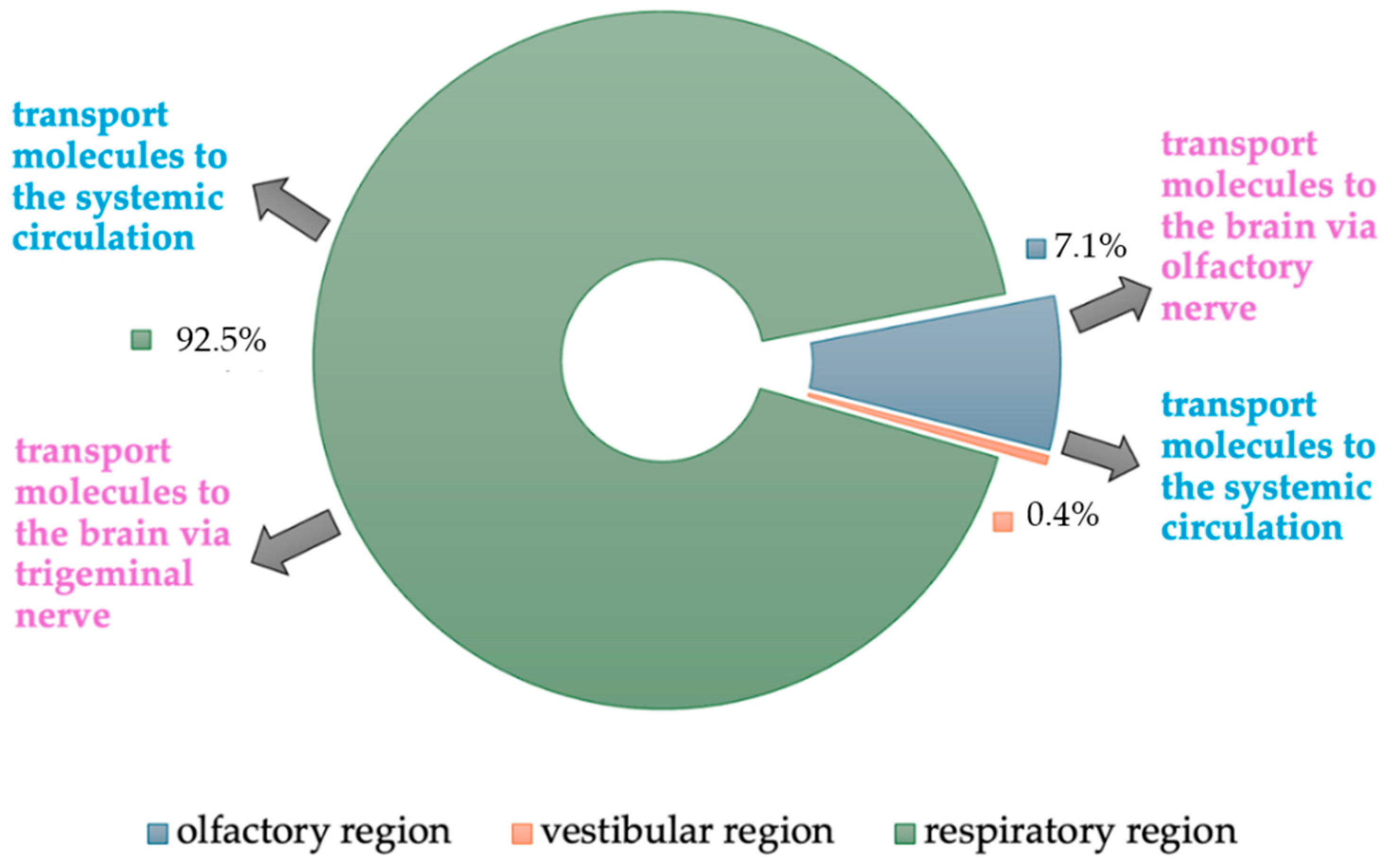
In the context of the structure and physiological diversity, the nasal cavity is perceived as a promising space for drug supply. Drug absorption through the nose occurs through several routes and mechanisms [2]. The human nasal cavity consists of the following three regions: vestibular, olfactory, and respiratory (Figure 1).
The vestibular region, which is a small anterior part of the nasal cavity, covers an area of approximately 0.6 cm2 and plays a marginal role in the absorption of drugs.
The olfactory region is located in the upper part of the nasal cavity, occupies an area of approximately 10 cm2, and is covered with the olfactory epithelium. The tissues that make up this epithelium allow molecules to be transported directly to the brain (nose-to-brain route). The penetration of molecules directly into the brain tissue through the olfactory epithelium takes place via different forms of transport: intracellular (neuronal endocytosis and exocytosis), extracellular (paracellular and through the blood and lymphatic vessels), and transcellular [2]. The transport of molecules depends on their physicochemical properties, mainly hydro- or lipophilicity, molecular weight, and degree of ionization [7]. Lipophilic substances can pass easily through cell membranes (transcellular transport). Hydrophilic molecules reach the cerebrospinal fluid thanks to a concentration gradient (paracellular transport). An important barrier to paracellular transport is the existence of a tight junction of the epithelial layer. The presence of P-glycoprotein-containing efflux pumps in the olfactory epithelium and endothelial cells surrounding the olfactory bulb hinders the penetration of molecules. The function of the efflux pumps is to limit the expansion of the xenobiotic into the central nervous system (CNS) by excreting it back into the nasal cavity [23]. Despite this phenomenon, most of the drug given intranasally is absorbed into the brain via the neuronal route and a smaller amount via the systemic route [24]. The molecules absorbed via the neuronal route are transported by axonal transport [23]. This process involves the olfactory nerve, which passes through the cribriform plate and reaches the olfactory bulb and other brain area. The involvement of trigeminal nerve fibers is also important in neuronal transport. The V1 and V2 branches of trigeminal nerve innervate the nasal cavity and transmit drug molecules to the brain stem both intracellularly and extracellularly [7]. Intranasal administration of the molecules allows them to penetrate brain tissue via the olfactory and trigeminal pathways bypassing the blood-brain-barrier (BBB) [25,26]. This is particularly important because the BBB is a very tight, selectively permeable membrane that helps maintain homeostasis in the CNS environment and protects the CNS from exposure to xenobiotics and toxic substances [13,14,27]. The BBB has been proven to resist the penetration of approximately 98% of small-molecule drugs and 100% of high-molecular-weight substances [24].
The largest part of the nasal cavity is the respiratory region, occupying an area of approximately 130 cm2. It is covered with epithelium, which contains cilia and produces mucus. The respiratory region has various functions, in particular filtering, humidifying, and warming inspired air. The function of respiratory epithelial structures is to contribute to mucociliary clearance [2]. Mucociliary cleansing is responsible for the removal of foreign substances. This process in a healthy nose takes about 12–20 min [4]. The respiratory epithelium is a highly vascularized tissue, which means that molecules can be absorbed directly into the vessels and from there into systemic circulation [14].
4. Optimizing Intranasal Drug Delivery
The intranasal administration of intravenous formulations of several drugs (fentanyl, sufentanil, ketamine, hydromorphone, midazolam, haloperidol, naloxone, glucagon) may be an effective alternative to intramuscular or intravenous administration [26]. In a paper by Lam et al. (2020), it was stated that formulations available for intravenous delivery can be used for nasal administration using appropriate devices such as a mucosal atomization device (MAD) [2]. Nevertheless, creating delivery systems that facilitate the supply of molecules to the appropriate tissue is a rapidly developing area of scientific research [1,26,27].
The intranasal systems are still being researched and improved upon to deliver the drug to the brain and achieve the most optimal effect. According to expert opinion, nanocarriers increase part of the dose delivered intranasally. Interesting conclusions are reached in a study by Emad et al. [23] in which some nanocarriers are described. Particle encapsulation was shown to protect drug molecules from precipitation and destabilization by enzymatic agents of the nasal cavity environment. Transferosomes, nanoparticles, microemulsions, nanoemulsions, and liposomes have been proven to be effective in delivering drugs from the nose to the brain. Specially designed polymer-lipid-based nanoparticle for intranasal administration facilitates bypassing the BBB, but also can reach the systemic circulation via vessels of the nasal mucosa, thus avoiding first-pass effect through the gastrointestinal tract and liver [23].
Size, charge, and organicity are important when designing nanoparticles. To illustrate: large (>900 nm in diameter), hydrophobic or highly charged particles will be difficult to diffuse through the mucosa. Pharmaceutical researchers focus on the physicochemical properties of drugs to achieve low molecular weight, high lipophilicity, and good water solubility [4].
In addition to the transport of the drug to the brain, the time rate of drug absorption is also important. There are mucoadhesive agents, ciliostatics or biogels used to prolong the residence time of the drug on the nasal mucosa for better absorption [14,25]. Some reports indicate that microemulsions are effective nanosystems for delivering hydrophobic drugs to the brain. It was observed that the addition of a mucoadhesive agent further increased the concentration of a given drug in brain tissue [28]. There are also studies that attempt to combine different systems, for example, mucoadhesive and mucopenetrating properties on the same particles [29]. Promising, although preclinical, are the results of Di Gioia et al. (2023) study of drug encapsulation in nanocarriers using chitosan and its derivatives [27]. It is believed that prolonged drug exposure to the nasal mucosa can be achieved due to the mucoadhesive properties of these carriers and their ability to temporarily open tight intercellular junctions. Another preclinical study worth highlighting is a report by Han et al. (2023) describing gold nanorods administered to the nasal cavity of laboratory mice [25]. This study, based on analytical methods, found that gold nanowires are quickly absorbed in the brain as early as 10 min after intranasal administration. The gold nanorods were observed to enter the brain via the olfactory bulb and then diffuse to higher brain areas within 1 h of exposure. A study of insulin-containing carbon quantum dots showed that their prolonged drug release on the nasal mucosa could be used to treat Alzheimer’s disease [30]. Neurodegenerative diseases (e.g., Alzheimer’s disease, Parkinson’s disease, Huntington’s disease, glioblastoma) are challenging to treat. The use of nanovesicular-mediated intranasal drug therapy to bypass the effect of first-pass metabolism and deliver the drug directly to the target site, i.e., the brain, is a rapidly developing and promising field of research [24].
Although many therapies can to some extent be achieved without the use of drug-loaded nanocarriers, optimizing intranasal drug delivery using nasal permeability agents, gelling agents, or nanocarrier formulations may be critical in the development of new therapies to meet clinical requirements. This topic was the main area of interest in 19 of the analyzed studies (Table 2).
5. Research among Adults and Children Receiving Palliative Care
There were more studies conducted in the adult palliative patient population than in the pediatric population (Table 2). Studies on adult patients were characterized by a higher statistical value, i.e., larger number of research centers involved. Detailed data on the type of paper, the number of analyzed patients, the drug tested, and palliative indications are presented in Table 3 and Table 4.
6. Problems with Administering Medications in Palliative Patients, New Hope—Intranasal Route
In the treatment of palliative patients, establishing a venous or subcutaneous access route or administering drugs intramuscularly causes suffering to patients and significantly complicates the administration of drugs by family members who are not medical professionals [2,42]. Chronic solutions such as vascular ports are available only to some patients who have a history of or are undergoing chemotherapy. Their use requires the ability to use a special port needle [65]. Complications such as catheter-related infections or accidental damage that are associated with the presence of intravascular devices in patients with permanently impaired immunity (chemotherapy, cancer itself) are additional factors limiting their widespread and trouble-free use in patients at the end of life [49]. Although drugs administered intravenously quickly reach the desired serum concentrations, this method of treatment is sometimes very difficult.
There are many clinical situations in which obtaining intravascular access is very difficult or undesirable. Apart from palliative patients receiving care at home or in a hospice, these may include the pediatric population requiring quick and effective pain treatment or short sedation [34,69] or even people traveling in difficult weather conditions suffering from symptoms of acute altitude illness [85]. In the above situations, administering the drug intranasally may be the method of choice, avoiding unnecessary suffering, and sometimes even the need for the intervention of professional medical staff while maintaining the same effectiveness of the drug as with intravascular administration [3]. In the context of palliative patients, nursing care is very important and is considered one of the strategic factors in improving patient comfort [63]. However, even simple nursing interventions can increase pain intensity and cause procedural breakthrough pain, the incidence of which reaches up to 12–20% [16]. It is very important that in such situations the pain relief or sedation is simple, easy, and convenient for everyone involved in the process [16,31]. Intranasal drug delivery seems to fulfil these requirements.
Intranasal route is widely used in emergency medicine (out of hospital and in emergency department) [86,87]. Drugs administered intranasally play a particularly important role in situations where their quick systemic action is required, and in cases when another route of administration (e.g., intravenous) is for some reason unavailable or difficult to access [2]. Such situations often occur in emergency medicine, especially among the pediatric population, due to a lack of time and technical possibilities to obtain intravenous access, as well as the invasiveness of obtaining intraosseous access [22,34,56]. An additional barrier can be the uncertainty of drug dosages, and this can affect both the pediatric population and cachectic patients at the end of life. In an emergency, intranasal drug administration is a convenient, safe, and fully acceptable alternative for patients [3,8]. Many of the acute medical problems of palliative patients are similar to the emergency patients. These include unpredictable severe pain, acute dyspnea, confusion or psychomotor agitation [20]. In these cases, in elderly cancer patients, immediate administration of rescue medication is necessary. Considering the emergency medicine experience, transmucosal drug administration (including intranasal) is a promising alternative to the currently preferred subcutaneous and intravenous routes among patients with unpredictable breakthrough pain, breathlessness or seizures. A list of doses proposed by the literature is provided in Table 5.
7. Intranasal versus Intravenous Route
Current research focuses on assessing the effectiveness of drugs administered intranasally [82,87]. Several studies compared the intranasal and intravenous route of drug administration [78]. It has been proven that the concentrations of various drugs (e.g., fentanyl, dexmedetomidine, diamorphine, ketamine, dexamethasone) in blood serum after intravenous administration do not differ significantly from those after intranasal administration [56,67]. There were some experiments in patients where serum drug concentrations following intravenous administration are compared with intranasal administration [5,67]. The systemic bioavailability of potent glucocorticoids such as dexamethasone and methylprednisolone administered intranasally was shown to be comparable to intravenous bioavailability [5]. The above suggests that intranasal use of glucocorticosteroids is a non-invasive alternative to intravenous drug administration. In a systematic review aimed at determining the dose of intranasal diamorphine in children treated for breakthrough pain, it was found that the analgesic effect ratio for intravenous morphine compared to intranasal diamorphine was 1:1 [67]. A publication on the use of desmopressin in the prevention and treatment of bleeding of various etiologies showed that desmopressin administered intranasally is as effective as that administered intravenously [12]. The use of intranasal desmopressin was described in the treatment of hemophilia A [13], certain subtypes of von Willebrand’s disease, coagulation disorders in uremia, and in palliative patients with end-stage renal and heart failure. There are also studies indicating that intranasal administration of some drugs does not produce a therapeutic effect. Such an example, according to some studies, may be glucagon in some indications. A study evaluating the efficacy of intranasal glucagon versus placebo in healthy volunteers found that adrenocorticoid, somatotropic, and antidiuretic responses were clinically insignificant [77]; however, there is an approved nasal powder formulation of glucagon available for the treatment of severe hypoglycemia [89].
Some reports compared intranasal and intravenous drug administration in animal models and tissue lines [11,26]. Animal models showed that concentrations in brain tissue may be higher after intranasal administration than after intravenous administration [72]. In the case of drugs acting mainly on the CNS, this is an extremely valuable discovery. If we add the following to the above-presented benefits: potentially lower side effects of the systemic effect of the drug, ease of self-administration by the patient or family, and the non-invasiveness (needle-free), the intranasal route of drug administration appears to be a very important alternative in various treatment options [73]. Some authors claim that the intranasal route has an advantage over intravenous route in delivering a large set of drugs to the brain [28]. However, in the context of comparing drug plasma concentrations after intranasal administration to other routes, there is still a noticeable lack of good quality experimental studies.
8. Intranasal versus Oral Route
In the population of palliative patients at the end of life, the convenience of using the drug is particularly important [3]. Taking medications orally is much more convenient for patients than intravenous, intramuscular or subcutaneous administration [16]. However, the ability to bypass the first-pass effect through the gastrointestinal tract and liver gives an advantage to molecules administered intranasally over the oral route [25]. In situations where patients cannot take medications orally due to weakness (e.g., cachexia), impaired consciousness or a disease that causes gastrointestinal failure (e.g., intestinal obstruction caused by a tumor), intranasal administration may be a much better option.
9. Intranasal Opioids
Patients receiving hospice care are often treated for both severe pain and psychomotor agitation. This treatment involves the use of opioids and benzodiazepines, which are described as substances that can be administered intranasally with good tolerance and bioavailability [42]. For many years, various intranasally administered fentanyl preparations were widely used in this group of patients to treat breakthrough pain, with very good effectiveness [3,42,48,65].
After analyzing selected articles, it was shown that among patients receiving palliative care, the group of drugs administered intranasally best represented in the bibliography are opioids (e.g., fentanyl, diamorphine) (Table 2). There is abundant evidence of their high effectiveness and feasible application, especially in breakthrough pain [65]. It was observed that morphine administered intravenously, and fentanyl administered intranasally or buccally have similarly high analgesic effectiveness, with good treatment tolerance and improved quality of life in the treatment of procedural pain in cancer patients [55]. Administration of intranasal fentanyl or buccal midazolam was accepted by dying patients and their families [51]. Additionally, several authors noticed that patients treated with intranasal and buccal fentanyl had better physical fitness and were more active [49,52].
The use of intranasal opioids is also being investigated among terminal cardiological patients with end-stage heart failure. Reports on this subject confirm the efficacy and safety, as well as the high tolerability of fentanyl and its derivatives used intranasally [39,40]. However, conclusions from reports on the use of fentanyl for the prevention of acute breathlessness among patients at the end of life from non-malignant causes are inconclusive [41]. Good tolerance of this type of treatment has been proven in both adults and children, and the long-term effects of intranasal administration are already known in the adult population [44].
Interesting reports concern the increasing use of intranasal opioids to treat vaso-occlusive pain in sickle cell disease (SCD). Publications cover both pediatric and adult populations and indicate that rapid administration of intranasal fentanyl can shorten the patient’s Emergency Department (ED) stay and reduce overall opioid consumption [36,46,47]. However, these reports require further thorough studies on larger groups of patients and with more profound methodology [90].
10. Sedative, Antidepressant, and Antianxiety Drugs
Regarding sedative, antidepressant or antianxiety drugs, ketamine and dexmedetomidine are the most studied (Table 2). There is evidence in the medical literature of the high effectiveness, efficiency, and ease of intranasal use of these drugs [32,43,46]. Interesting findings are presented in the review by Lemus et al. (2022) where, based on a series of case reports, dexmedetomidine was shown to be highly effective in palliative and hospice care [59]. Subsequent reports indicate the effective and safe effects of dexmedetomidine in refractory situations of irritability, dystonia, and insomnia among palliative children [61,83]. A prospective, randomized, doubled-blind study demonstrated that intranasal dexmedetomidine (2.5 mcg kg−1) is superior to intranasal ketamine (5 mg kg−1) to provide procedural sedation for radiotherapy in children [58]. A meta-analysis of intranasal delivery of analgesia for moderate to severe pain in children showed that intranasal ketamine has similar analgesic efficacy to intranasal fentanyl but induces deeper sedation [34]. Another study of intranasal ketamine for procedural sedation in children by Rached-d’Astous et al. (2023) showed good effects using a dose of 6 mg kg−1 in patients being treated for lacerated wounds [82]. However, limitations in methodology of this study suggest the importance of further research [91]. Although numerous studies confirm the effectiveness and safety of intranasal administration of ketamine to children [82,92], it is still formally administered off-label in many countries. Intranasal ketamine especially in combination with intranasal dexmedetomidine has a high efficacy and safety profile in dental procedural sedation in healthy children [35]. In addition, recent reports have identified intranasal ketamine as effective in the treatment of local nasal and sinus mucosal pain caused by oncological radiation treatment [80].
Less research is devoted to intranasal benzodiazepines (e.g., midazolam, lorazepam), but their high effectiveness in terminating status epilepticus in children is widely known and clinically used [56]. The randomized open-label study comparing intranasal versus intravenous lorazepam (0.1 mg kg−1) for control of acute seizures in children has shown clinical seizures remission within 10 min in 83 and 80% of patients, respectively [78]. The authors are aware of an ongoing study comparing the sedative effect of midazolam administered by the subcutaneous and intranasal route, in which the plasma concentration of the drug is being investigated [76].
11. Limitations of Intranasal Therapy
A limitation of the use of the intranasal route of drug administration is the limited volume of drug that can be administered. The volume of the drug that can be administered into one nostril in adults and children is 1 mL [16] and 0.3 mL [50], respectively. However, some articles indicate that the volume of substance sprayed or dropped into each nostril should not exceed 0.15 mL [2]. This restriction limits the intranasal use of low concentration drugs. Medications should be administered during a few seconds and divided evenly between nostrils. In addition, the presence of mucociliary clearance eliminates drugs from the nasal space quite quickly—within approximately 12–20 min in healthy nose. Additional limitations to this method of drug delivery include possible disease states of the nasal mucosa (e.g., rhinitis, local peri-infective inflammation, allergic edema) or of the vessels (e.g., diabetes) [2].
12. Future Perspectives
Issues related to the limitations of intranasal drug delivery are being actively and intensively investigated [24]. Potential solutions include various particle delivery systems. Among them, nanosystems such as liposomes, polymer nanoparticles (nanocapsules and nanospheres), lipid nanoparticles, artificial exosomes, nanometric emulsions, and nanogels are promising [14,26]. Nanosystems are small particles that facilitate the bioavailability of drugs and increase the residence time of the molecule in the nasal cavity, as well as enable their rapid penetration through the nasal mucosa. These features mean that nanosystems can facilitate the transport of drugs from the nose to the brain and peripheral circulation [27].
The number of patients qualified for palliative treatment of various diseases, especially cancer, increases every year [18,93]. Many of them suffer from disseminated disease, with the tumor process often affecting the central nervous system and, as a result, causing brain edema as the disease expands. In the event of cerebral edema, available treatment for hospice patients includes palliative brain radiotherapy and symptomatic treatment involving the administration of drugs that reduce edema of brain tissue. A commonly used drug that reduces cerebral edema is dexamethasone, a synthetic glucocorticosteroid, a fluorinated derivative of prednisone with a long-lasting and powerful effect, which includes the inhibition of capillary permeability, and thus swelling [66]. There are reports confirming good bioavailability and the achievement of similar serum concentrations of dexamethasone after intranasal administration compared to the intravenous route [5]. Studies in animal models suggest even better penetration into the CNS after intranasal administration compared to other routes (intravenous and oral) [7]. Intranasal administration of dexamethasone was discussed in only three articles, one of which concerns experiments on animal models [7], the second on patients with moderate to severe COVID-19 [17], and the third is a study conducted on healthy volunteers [5]. Based on these articles, it can be assumed that dexamethasone administered intranasally is characterized by high bioavailability, effectiveness of targeting the brain, and a high safety profile. Using dexamethasone among palliative patients should be a subject of future research.
While there is scientific evidence supporting intranasal drug administration and its effects on quality of life [42], the impact of changing the method of drug administration to the nasal route in terms of its cost-effectiveness for health care systems has not yet been thoroughly investigated [94].
The authors suggest that future research should focus on several areas. Firstly, drugs that have potential for intranasal use in palliative medicine should be thoroughly investigated for their plasma and brain tissue concentrations. An additional consideration is the need for intranasal application devices that are practical for use by a person with a disability, e.g., a chronically recumbent, physically incapacitated or confused patient. The intranasal preparation must persist long enough in the nasal mucosa, against ciliary-mucosal clearance, while not irritating it. Finally, a clinical assessment based on the examination of patients receiving end-of-life care, in terms of alleviating symptoms associated with severe condition and impending death, is important.
13. Conclusions
According to our review there is a significant interest in the intranasal treatment for patients receiving palliative care. Our main conclusions are as follows: Patients receiving palliative care benefit from the use of drugs administered intranasally. For patients in terminal stages of a disease, the supply of drugs via the intranasal route guarantees quick bioavailability and, consequently, high effectiveness, as well as comfort and safety of use.
So far, scientific studies have focused on opioids and sedatives used intranasally. The benefits of the intranasal use of fentanyl, diamorphine, ketamine or dexmedetomidine in these patients are well documented.
This topic requires further research in terms of both clinical and financial effects on the patient and health care system.
Author Contributions
Conceptualization, R.K.S.; methodology, R.K.S. and A.I.; validation, R.K.S., and A.I.; formal analysis, A.I.; investigation, R.K.S. and A.I.; writing—original draft preparation, A.I.; writing—review and editing, R.K.S.; visualization, A.I. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study did not require ethical approval.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Zhao, J.; Yang, J.; Jiao, J.; Wang, X.; Zhao, Y.; Zhang, L. Biomedical applications of artificial exosomes for intranasal drug delivery. Front. Bioeng. Biotechnol. 2023, 11, 1271489. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.K.; Cheung, C.C.; Chow, M.Y.; Harrop, E.; Lapwood, S.; Barclay, S.I.; Wong, I.C. Transmucosal drug administration as an alternative route in palliative and end-of-life care during the COVID-19 pandemic. Adv. Drug Deliv. Rev. 2020, 160, 234–243. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, L.; Harrop, E.; Liossi, C.; Boyce, K.; Mitchell, L.; Johnson, M.; Jani, Y.; Akinyooye, V.; Skene, S.S.; Wong, I.C.K.; et al. Carer preferences of route of administration of transmucosal diamorphine and willingness to take part in a randomised controlled trial: An interview study (DIPPER). BMC Palliat. Care 2022, 21, 78. [Google Scholar] [CrossRef] [PubMed]
- Keller, L.-A.; Merkel, O.; Popp, A. Intranasal drug delivery: Opportunities and toxicologic challenges during drug development. Drug Deliv. Transl. Res. 2022, 12, 735–757. [Google Scholar] [CrossRef] [PubMed]
- Cárdenas, G.; Bobes, R.J.; Fragoso, G.; Pérez-Osorio, N.I.; Hernández, M.; Espinosa, A.; Fleury, A.; Flores, J.; The Revival Project Consortium; Laclette, J.P.; et al. Pharmacokinetic Study of Intranasal Dexamethasone and Methylprednisolone Compared with Intravenous Administration: Two Open-Label, Single-Dose, Two-Period, Two-Sequence, Cross-Over Study in Healthy Volunteers. Pharmaceutics 2022, 15, 105. [Google Scholar] [CrossRef] [PubMed]
- Rosenblat, J.D.; Devries, F.E.; Doyle, Z.; McIntyre, R.S.; Rodin, G.; Zimmermann, C.; Mak, E.; Hannon, B.; Schulz-Quach, C.; Al Kindy, A.; et al. A Phase II, Open-Label Clinical Trial of Intranasal Ketamine for Depression in Patients with Cancer Receiving Palliative Care (INKeD-PC Study). Cancers 2023, 15, 400. [Google Scholar] [CrossRef] [PubMed]
- Erdő, F.; Bors, L.A.; Farkas, D.; Bajza, Á.; Gizurarson, S. Evaluation of intranasal delivery route of drug administration for brain targeting. Brain Res. Bull. 2018, 143, 155–170. [Google Scholar] [CrossRef]
- Espinoza, S.E.; Lee, J.L.; Wang, C.-P.; Ganapathy, V.; MacCarthy, D.; Pascucci, C.; Musi, N.; Volpi, E. Intranasal Oxytocin Improves Lean Muscle Mass and Lowers LDL Cholesterol in Older Adults with Sarcopenic Obesity: A Pilot Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2021, 22, 1877–1882.e2. [Google Scholar] [CrossRef] [PubMed]
- Bruinsmann, F.A.; Vaz, G.R.; Alves, A.D.C.S.; Aguirre, T.; Pohlmann, A.R.; Guterres, S.S.; Sonvico, F. Nasal Drug Delivery of Anticancer Drugs for the Treatment of Glioblastoma: Preclinical and Clinical Trials. Molecules 2019, 24, 4312. [Google Scholar] [CrossRef]
- Szabó-Révész, P. Modifying the physicochemical properties of NSAIDs for nasal and pulmonary administration. Drug Discov. Today Technol. 2018, 27, 87–93. [Google Scholar] [CrossRef]
- Passoni, A.; Favagrossa, M.; Colombo, L.; Bagnati, R.; Gobbi, M.; Diomede, L.; Birolini, G.; Di Paolo, E.; Valenza, M.; Cattaneo, E.; et al. Efficacy of Cholesterol Nose-to-Brain Delivery for Brain Targeting in Huntington’s Disease. ACS Chem. Neurosci. 2020, 11, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Mohinani, A.; Patel, S.; Tan, V.; Kartika, T.; Olson, S.; DeLoughery, T.G.; Shatzel, J. Desmopressin as a hemostatic and blood sparing agent in bleeding disorders. Eur. J. Haematol. 2023, 110, 470–479. [Google Scholar] [CrossRef] [PubMed]
- Leissinger, C.; Becton, D.; Cornell, C., Jr.; Cox Gill, J. High-dose DDAVP intranasal spray (Stimate) for the prevention and treatment of bleeding in patients with mild haemophilia A, mild or moderate type 1 von Willebrand disease and symptomatic carriers of haemophilia A. Haemophilia 2001, 7, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Duong, V.-A.; Nguyen, T.-T.-L.; Maeng, H.-J. Recent Advances in Intranasal Liposomes for Drug, Gene, and Vaccine Delivery. Pharmaceutics 2023, 15, 207. [Google Scholar] [CrossRef] [PubMed]
- Assadpour, S.; Shiran, M.R.; Asadi, P.; Akhtari, J.; Sahebkar, A. Harnessing Intranasal Delivery Systems of Sumatriptan for the Treatment of Migraine. Biomed. Res. Int. 2022, 2022, 3692065. [Google Scholar] [CrossRef] [PubMed]
- Rahm, N.D.; Zaccaria, I.; Wey, B.G.; Pautex, S.; Habre, W.; Elia, N. Intranasal Dexmedetomidine for Pain Management in Older Patients: A Cross-Over, Randomized, Double-Blinded, Active-Controlled Trial. Drugs Aging 2023, 40, 527–538. [Google Scholar] [CrossRef] [PubMed]
- Cárdenas, G.; Chávez-Canales, M.; Espinosa, A.M.; Jordán-Ríos, A.; Malagon, D.A.; Murillo, M.F.M.; Araujo, L.V.T.; Campos, R.L.B.; Wong-Chew, R.M.; González, L.E.R.; et al. dexamethasone: A new clinical trial for the control of inflammation and neuroinflammation in COVID-19 patients. Trials 2022, 23, 148. [Google Scholar] [CrossRef]
- Rothberg, B.E.G.; Quest, T.E.; Yeung, S.J.; Pelosof, L.C.; Gerber, D.E.; Seltzer, J.A.; Bischof, J.J.; Thomas, C.R.; Akhter, N.; Mamtani, M.; et al. Oncologic emergencies and urgencies: A comprehensive review. CA Cancer J. Clin. 2022, 72, 570–593. [Google Scholar] [CrossRef]
- Kirkland, S.W.; Ghalab, A.; Kruhlak, M.; Ruske, H.; Campbell, S.; Yang, E.H.; Villa-Roel, C.; Rowe, B.H. An Assessment of Emergency Department-Based Interventions for Patients with Advanced or End-Stage Illness: A Systematic Review. J. Palliat. Med. 2021, 24, 605–618. [Google Scholar] [CrossRef]
- Chan, Y.C.; Yang, M.L.C.; Ho, H.F. Characteristics and Outcomes of Patients Referred to an Emergency Department-Based End-of-Life Care Service in Hong Kong: A Retrospective Cohort Study. Am. J. Hosp. Palliat. Care 2021, 38, 25–31. [Google Scholar] [CrossRef]
- Verhoef, M.-J.; de Nijs, E.; Horeweg, N.; Fogteloo, J.; Heringhaus, C.; Jochems, A.; Fiocco, M.; van der Linden, Y. Palliative care needs of advanced cancer patients in the emergency department at the end of life: An observational cohort study. Support. Care Cancer 2020, 28, 1097–1107. [Google Scholar] [CrossRef]
- Jamieson, L.; Harrop, E.; Johnson, M.; Liossi, C.; Mott, C.; Oulton, K.; Skene, S.S.; Wong, I.C.; Howard, R.F. Healthcare professionals’ views of the use of oral morphine and transmucosal diamorphine in the management of paediatric breakthrough pain and the feasibility of a randomised controlled trial: A focus group study (DIPPER). Palliat. Med. 2021, 35, 1118–1125. [Google Scholar] [CrossRef] [PubMed]
- Emad, N.A.; Ahmed, B.; Alhalmi, A.; Alzobaidi, N.; Al-Kubati, S.S. Recent progress in nanocarriers for direct nose to brain drug delivery. J. Drug Deliv. Sci. Technol. 2021, 64, 102642. [Google Scholar] [CrossRef]
- Singh, S.; Shukla, R. Nanovesicular-Mediated Intranasal Drug Therapy for Neurodegenerative Disease. AAPS PharmSciTech 2023, 24, 179. [Google Scholar] [CrossRef]
- Han, S.; Wang, J.T.-W.; Yavuz, E.; Zam, A.; Rouatbi, N.; Utami, R.N.; Liam-Or, R.; Griffiths, A.; Dickson, W.; Sosabowski, J.; et al. Spatiotemporal tracking of gold nanorods after intranasal administration for brain targeting. J. Control. Release 2023, 357, 606–619. [Google Scholar] [CrossRef] [PubMed]
- Antunes, J.L.; Amado, J.; Veiga, F.; Paiva-Santos, A.C.; Pires, P.C. Nanosystems, Drug Molecule Functionalization and Intranasal Delivery: An Update on the Most Promising Strategies for Increasing the Therapeutic Efficacy of Antidepressant and Anxiolytic Drugs. Pharmaceutics 2023, 15, 998. [Google Scholar] [CrossRef]
- Di Gioia, S.; Fracchiolla, G.; Cometa, S.; Perna, F.M.; Quivelli, A.F.; Trapani, G.; Daniello, V.; Nobile, C.; Hossain, M.N.; Trapani, A.; et al. Carboxymethyl chitosan dopamine conjugates: Synthesis and evaluation for intranasal anti Parkinson therapy. Int. J. Biol. Macromol. 2023, 253 Pt 5, 127174. [Google Scholar] [CrossRef] [PubMed]
- Pires, P.C.; Santos, A.O. Nanosystems in nose-to-brain drug delivery: A review of non-clinical brain targeting studies. J. Control Release 2018, 270, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Netsomboon, K.; Bernkop-Schnürch, A. Mucoadhesive vs. mucopenetrating particulate drug delivery. Eur. J. Pharm. Biopharm. 2016, 98, 76–89. [Google Scholar] [CrossRef]
- Camlik, G.; Bilakaya, B.; Ozsoy, Y.; Degim, I.T. A new approach for the treatment of Alzheimer’s disease: Insulin-quantum dots. J. Microencapsul. 2024, 41, 18–26. [Google Scholar] [CrossRef]
- Perkins, P.; Parkinson, A.; Taylor, V.; Husbands, E. Nasal fentanyl and buccal midazolam carer administration “as needed” for breakthrough symptom control in a specialist palliative care unit: A nested qualitative study. BMJ Support. Palliat. Care 2021, 11, 440–443. [Google Scholar] [CrossRef]
- Mercadante, S. Breakthrough cancer pain in the radiotherapy setting: A systematic and critical review. Expert. Rev. Anticancer Ther. 2023, 23, 229–234. [Google Scholar] [CrossRef]
- Janssen, D.J.A.; van den Beuken-van Everdingen, M.H.J.; Verberkt, C.A.; Creemers, J.P.H.M.; Wouters, E.F.M. Fentanyl nasal spray in a patient with end-stage COPD and severe chronic breathlessness. Breathe 2019, 15, e122–e125. [Google Scholar] [CrossRef] [PubMed]
- Prescott, M.G.; Iakovleva, E.; Simpson, M.R.; Pedersen, S.A.; Munblit, D.; Vallersnes, O.M.; Austad, B. Intranasal analgesia for acute moderate to severe pain in children—A systematic review and meta-analysis. BMC Pediatr. 2023, 23, 405. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Alam Ansari, A.; Nath, R.; Chak, R.K.; Singh, R.K.; Khanna, R.; Singh, P.R. Comparative evaluation of intranasal midazolam-ketamine, dexmedetomidine-ketamine, midazolam-fentanyl, and dexmedetomidine-fentanyl combinations for procedural sedation and analgesia in pediatric dental patients: A randomized controlled trial. J. Dent. Anesth. Pain Med. 2023, 23, 69–81. [Google Scholar] [CrossRef] [PubMed]
- Astles, R.; Liu, Z.; Gillespie, S.E.; Lai, K.W.; Maillis, A.; Morris, C.R.; Lane, P.A.; Krishnamurti, L.; Bakshi, N. Sex and frequency of pain episodes are associated with acute pain trajectories in adolescents with sickle cell disease. Pain Rep. 2023, 8, e1084. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, T.G.; Husbands, E.L. Benefits of Intranasal Administration of Diamorphine and Midazolam in the Management of Patients Receiving Palliative Care in the Community: A Case Series. J. Pain Palliat. Care Pharmacother. 2022, 36, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Giuliani, J.; Fiorica, F.; Sacchetto, A.; Franceschini, G.; Vaccari, F.; Bonetti, A. The role of fentanyl in the treatment of breakthrough cancer pain: Different biotechnologies, different results and different drug costs. J. Oncol. Pharm. Pract. 2021, 27, 445–447. [Google Scholar] [CrossRef] [PubMed]
- Pilkey, J.; Pedersen, A.; Tam, J.W.; Malik, A.; Wong, J. The Use of Intranasal Fentanyl for the Palliation of Incident Dyspnea in Advanced Congestive Heart Failure: A Pilot Study. J. Palliat. Care 2019, 34, 96–102. [Google Scholar] [CrossRef]
- Wiens, E.J.; Pilkey, J.; Wong, J.K. Delivery of End-of-Life Care in Patients Requesting Withdrawal of a Left Ventricular Assist Device Using Intranasal Opioids and Benzodiazepines. J. Palliat. Care 2019, 34, 92–95. [Google Scholar] [CrossRef]
- Iupati, S.; Bridge, R.; Allan, S.; Hewitt, D. Intranasal Fentanyl Versus Placebo for Treatment of Episodic Breathlessness in Hospice Patients with Advanced Nonmalignant Diseases. J. Pain Symptom Manag. 2021, 61, 1035–1041. [Google Scholar] [CrossRef] [PubMed]
- Piotrowska, W.; Leppert, W.; Majkowicz, M. Comparison of analgesia, adverse effects, and quality of life in cancer patients during treatment of procedural pain with intravenous morphine, fentanyl nasal spray, and fentanyl buccal tablets. Cancer Manag. Res. 2019, 11, 1587–1600. [Google Scholar] [CrossRef] [PubMed]
- Vellucci, R.; Mediati, R.D.; Gasperoni, S.; Mammucari, M.; Marinangeli, F.; Romualdi, P. Assessment and treatment of breakthrough cancer pain: From theory to clinical practice. J. Pain Res. 2017, 10, 2147–2155. [Google Scholar] [CrossRef] [PubMed]
- Taylor, D.; Radbruch, L.; Revnic, J.; Torres, L.M.; Ellershaw, J.E.; Perelman, M. A report on the long-term use of fentanyl pectin nasal spray in patients with recurrent breakthrough pain. J. Pain Symptom Manag. 2014, 47, 1001–1007. [Google Scholar] [CrossRef] [PubMed]
- Jaiswal, N.; Singh, M.; Agarwal, A.; Chauhan, A.; Jaiswal, N. Palliative drug treatments for breathlessness in cystic fibrosis. Cochrane Database Syst. Rev. 2020, 2020, CD011855. [Google Scholar] [CrossRef] [PubMed]
- Rees, C.A.; Brousseau, D.C.; Ahmad, F.A.; Bennett, J.; Bhatt, S.; Bogie, A.; Brown, K.M.; Casper, T.C.; Chapman, L.L.; Chumpitazi, C.E.; et al. Intranasal fentanyl and discharge from the emergency department among children with sickle cell disease and vaso-occlusive pain: A multicenter pediatric emergency medicine perspective. Am. J. Hematol. 2023, 98, 620–627. [Google Scholar] [CrossRef]
- Assad, O.; Zamora, R.; Brown, K.; Melnitsky, L.; Moses, J.; Sherman, V. IF IM in a crisis: Intranasal fentanyl versus intravenous morphine in adult vaso-occlusive crisis. Am. J. Emerg. Med. 2023, 64, 86–89. [Google Scholar] [CrossRef] [PubMed]
- Hui, D.; Kilgore, K.; Park, M.; Williams, J.; Liu, D.; Bruera, E. Impact of Prophylactic Fentanyl Pectin Nasal Spray on Exercise-Induced Episodic Dyspnea in Cancer Patients: A Double-Blind, Randomized Controlled Trial. J. Pain Symptom Manag. 2016, 52, 459–468.e1. [Google Scholar] [CrossRef] [PubMed]
- Mercadante, S.; Vellucci, R.; Cuomo, A.; Adile, C.; Cortegiani, A.; Valle, A.; Villari, P.; Casuccio, A. Long-term efficacy and tolerability of intranasal fentanyl in the treatment of breakthrough cancer pain. Support. Care Cancer 2015, 23, 1349–1354. [Google Scholar] [CrossRef]
- Pansini, V.; Curatola, A.; Gatto, A.; Lazzareschi, I.; Ruggiero, A.; Chiaretti, A. Intranasal drugs for analgesia and sedation in children admitted to pediatric emergency department: A narrative review. Ann. Transl. Med. 2021, 9, 189. [Google Scholar] [CrossRef]
- Perkins, P.; Parkinson, A.; Akyea, R.K.; Husbands, E. Nasal fentanyl alone plus buccal midazolam: An open-label, randomised, controlled feasibility study in the dying. BMJ Support. Palliat. Care 2020, 10, 300–303. [Google Scholar] [CrossRef] [PubMed]
- Rogríguez, D.; Urrutia, G.; Escobar, Y.; Moya, J.; Murillo, M. Efficacy and Safety of Oral or Nasal Fentanyl for Treatment of Breakthrough Pain in Cancer Patients: A Systematic Review. J. Pain Palliat. Care Pharmacother. 2015, 29, 228–246. [Google Scholar] [CrossRef]
- Pieper, L.; Wager, J.; Zernikow, B. Intranasal fentanyl for respiratory distress in children and adolescents with life-limiting conditions. BMC Palliat. Care 2018, 17, 106. [Google Scholar] [CrossRef] [PubMed]
- Bossi, P.; Escobar, Y.; Pea, F. Rapid-Onset Opioids for Management of Breakthrough Cancer Pain: Considerations for Daily Practice. Front. Pain Res. 2022, 3, 893530. [Google Scholar] [CrossRef] [PubMed]
- Magnani, C.; Giannarelli, D.; Casale, G. Procedural Pain in Palliative Care: Is It Breakthrough Pain? A Multicenter National Prospective Study to Assess Prevalence, Intensity, and Treatment of Procedure-related Pain in Patients with Advanced Disease. Clin. J. Pain 2017, 33, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Grönheit, W.; Popkirov, S.; Wehner, T.; Schlegel, U.; Wellmer, J. Practical Management of Epileptic Seizures and Status Epilepticus in Adult Palliative Care Patients. Front. Neurol. 2018, 9, 595. [Google Scholar] [CrossRef] [PubMed]
- Goldman, N.; Frankenthaler, M.; Klepacz, L. The Efficacy of Ketamine in the Palliative Care Setting: A Comprehensive Review of the Literature | Journal of Palliative Medicine. J. Palliat. Med. 2019, 22, 1154–1161. [Google Scholar] [CrossRef]
- Suvvari, P.; Mishra, S.; Bhatnagar, S.; Garg, R.; Bharati, S.J.; Gupta, N.; Kumar, V.; Khan, M. Comparison of Intranasal Dexmedetomidine Versus Intranasal Ketamine as Premedication for Level of Sedation in Children Undergoing Radiation Therapy: A Prospective, Randomised, Double-Blind Study. Turk. J. Anaesthesiol. Reanim. 2020, 48, 215–222. [Google Scholar] [CrossRef]
- Lemus, R.; Jacobowski, N.L.; Humphrey, L.; Tobias, J.D. Applications of Dexmedetomidine in Palliative and Hospice Care. J. Pediatr. Pharmacol. Ther. 2022, 27, 587–594. [Google Scholar] [CrossRef]
- Ferguson, L.; Wilson, M. Intranasal dexmedetomidine: Procedural sedation in palliative care: A case report. Palliat. Med. 2021, 35, 1625–1628. [Google Scholar] [CrossRef]
- De Zen, L.; Della Paolera, S.; Del Rizzo, I.; Taucar, V.; Skabar, A.; Barbi, E. Home Intranasal Dexmedetomidine for Refractory Dystonia in Pediatric Palliative Care. J. Pain Symptom Manag. 2020, 59, e3–e5. [Google Scholar] [CrossRef]
- Bartoletta, K.M.; Collura, C.A.; Thorvilson, M.J. Novel Use of Intranasal Dexmedetomidine for Refractory Irritability in Pediatric Home Care. J. Palliat. Med. 2023, 26, 596–598. [Google Scholar] [CrossRef] [PubMed]
- Kestenbaum, M.G.; Vilches, A.O.; Messersmith, S.; Connor, S.R.; Fine, P.G.; Murphy, B.; Davis, M.; Muir, J.C. Alternative Routes to Oral Opioid Administration in Palliative Care: A Review and Clinical Summary. Pain Med. 2014, 15, 1129–1153. [Google Scholar] [CrossRef]
- Pautex, S.; Vogt-Ferrier, N.; Zulian, G.B. Breakthrough Pain in Elderly Patients with Cancer: Treatment Options. Drugs Aging 2014, 31, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Harris, D.G. Management of pain in advanced disease. Br. Med. Bull. 2014, 110, 117–128. [Google Scholar] [CrossRef]
- Ong, Q.; Hochberg, F.H.; Cima, M.J. Depot delivery of dexamethasone and cediranib for the treatment of brain tumor associated edema in an intracranial rat glioma model. J. Control Release 2015, 217, 183–190. [Google Scholar] [CrossRef]
- Gastine, S.; Morse, J.D.; Leung, M.T.; Wong, I.C.K.; Howard, R.F.; Harrop, E.; Liossi, C.; Standing, J.F.; Jassal, S.S.; Hain, R.D.; et al. Diamorphine pharmacokinetics and conversion factor estimates for intranasal diamorphine in paediatric breakthrough pain:systematic review. BMJ Support. Palliat. Care 2022, 13, e485–e493. [Google Scholar] [CrossRef]
- Hewitt, M.; Goldman, A.; Collins, G.S.; Childs, M.; Hain, R. Opioid use in palliative care of children and young people with cancer. J Pediatr. 2008, 152, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, A.E.; Presland, M.; Harrop, E.; Carey, M.; Miller, M.; Wong, I.C.K.C. Orodispersible and transmucosal alternative medications for symptom control in adults. BMJ Support. Palliat. Care 2022, 12, 305–315. [Google Scholar] [CrossRef]
- Haasbroek-Pheiffer, A.; Van Niekerk, S.; Van der Kooy, F.; Cloete, T.; Steenekamp, J.; Hamman, J. In vitro and ex vivo experimental models for evaluation of intranasal systemic drug delivery as well as direct nose-to-brain drug delivery. Biopharm Drug Dispos. 2023, 44, 94–112. [Google Scholar] [CrossRef]
- Wu, D.; Chen, Q.; Chen, X.; Han, F.; Chen, Z.; Wang, Y. The blood-brain barrier: Structure, regulation, and drug delivery. Signal Transduct. Target. Ther. 2023, 8, 217. [Google Scholar] [CrossRef] [PubMed]
- Maher, R.; Moreno-Borrallo, A.; Jindal, D.; Mai, B.T.; Ruiz-Hernandez, E.; Harkin, A. Intranasal Polymeric and Lipid-Based Nanocarriers for CNS Drug Delivery. Pharmaceutics 2023, 15, 746. [Google Scholar] [CrossRef] [PubMed]
- Crowe, T.P.; Hsu, W.H. Evaluation of Recent Intranasal Drug Delivery Systems to the Central Nervous System. Pharmaceutics 2022, 14, 629. [Google Scholar] [CrossRef] [PubMed]
- Crowe, T.P.; Greenlee, M.H.W.; Kanthasamy, A.G.; Hsu, W.H. Mechanism of intranasal drug delivery directly to the brain. Life Sci. 2018, 195, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Aucoin, R.; Lewthwaite, H.; Ekström, M.; von Leupoldt, A.; Jensen, D. Impact of trigeminal nerve and/or olfactory nerve stimulation on activity of human brain regions involved in the perception of breathlessness. Respir. Physiol. Neurobiol. 2023, 311, 104036. [Google Scholar] [CrossRef] [PubMed]
- Hirschinger, H.; Jaeger, E.; Nittka, S.; Hetjens, S.; Lorenz, C.; Remi, C.; Saussele, S.; Hofmann, W.-K.; Gencer, D.; Boch, T. Treatment of agitation in terminally ill patients with intranasal midazolam versus subcutaneous midazolam: Study protocol for a randomised controlled open-label monocentric trial (MinTU Study). BMC Palliat. Care 2024, 23, 8. [Google Scholar] [CrossRef] [PubMed]
- Varaldo, E.; Bioletto, F.; Cuboni, D.; Prencipe, N.; Bona, C.; Barale, M.; Ghigo, E.; Grottoli, S.; Berton, A.M.; Gasco, V. Adrenocortical, somatotropic, and antidiuretic response to nasal glucagon in healthy subjects. Eur. J. Endocrinol. 2023, 188, lvad019. [Google Scholar] [CrossRef]
- Arya, R.; Gulati, S.; Kabra, M.; Sahu, J.K.; Kalra, V. Intranasal versus intravenous lorazepam for control of acute seizures in children: A randomized open-label study. Epilepsia 2011, 52, 788–793. [Google Scholar] [CrossRef] [PubMed]
- Mercadante, S.; Aielli, F.; Adile, C.; Costanzi, A.; Casuccio, A. Fentanyl Pectin Nasal Spray Versus Oral Morphine in Doses Proportional to the Basal Opioid Regimen for the Management of Breakthrough Cancer Pain: A Comparative Study. J. Pain Symptom Manag. 2016, 52, 27–34. [Google Scholar] [CrossRef]
- Ehrman, S.; Houchard, G.; Kullgren, J. Novel Use of Atomized Intravenous Ketamine Solution for the Topical Treatment of Intranasal Mucositis Pain: A Case Report. J. Palliat. Med. 2021, 24, 954–958. [Google Scholar] [CrossRef]
- Delgado-Miguel, C.; Miguel-Ferrero, M.; Ezquerra, A.; Díaz, M.; De Ceano-Vivas, M.; López-Gutiérrez, J.C. Sedoanalgesia in the Debridement of Pediatric Burns in the Emergency Department: Is It Effective and Safe? Children 2023, 10, 1137. [Google Scholar] [CrossRef] [PubMed]
- Rached-D’Astous, S.; Finkelstein, Y.; Bailey, B.; Marquis, C.; Lebel, D.; Desjardins, M.-P.; Trottier, E.D. Intranasal ketamine for procedural sedation in children: An open-label multicenter clinical trial. Am. J. Emerg. Med. 2023, 67, 10–16. [Google Scholar] [CrossRef] [PubMed]
- De Zen, L.; Divisic, A.; Molinaro, G.; Solidoro, S.; Barbi, E. Dexmedetomidine at Home for Intractable Dystonia and Insomnia in Children with Special Needs: A Case Series. J. Pain Symptom Manag. 2023, 66, e653–e657. [Google Scholar] [CrossRef] [PubMed]
- De Zen, L.; Del Rizzo, I.; Robazza, M.; Barbieri, F.; Campagna, M.; Vaccher, S.; Barbi, E.; Dall’Amico, R. Home Use of Intranasal Dexmedetomidine in a Child with An Intractable Sleep Disorder. J. Pediatr. Pharmacol. Ther. 2020, 25, 332–335. [Google Scholar] [CrossRef] [PubMed]
- Szymczak, R.K.; Sawicka, M. Can intranasal delivery of dexamethasone facilitate the management of severe altitude disease? J. Travel. Med. 2023, 30, taad026. [Google Scholar] [CrossRef] [PubMed]
- Rech, M.A.; Barbas, B.; Chaney, W.; Greenhalgh, E.; Turck, C. When to Pick the Nose: Out-of-Hospital and Emergency Department Intranasal Administration of Medications. Ann. Emerg. Med. 2017, 70, 203–211. [Google Scholar] [CrossRef]
- Corrigan, M.; Wilson, S.S.; Hampton, J. Safety and efficacy of intranasally administered medications in the emergency department and prehospital settings. Am. J. Health Syst. Pharm. 2015, 72, 1544–1554. [Google Scholar] [CrossRef]
- Kälviäinen, R.; Reinikainen, M. Management of prolonged epileptic seizures and status epilepticus in palliative care patients. Epilepsy Behav. 2019, 101, 106288. [Google Scholar] [CrossRef]
- Pontiroli, A.E.; Tagliabue, E. Intranasal versus injectable glucagon for hypoglycemia in type 1 diabetes: Systematic review and meta-analysis. Acta Diabetol. 2020, 57, 743–749. [Google Scholar] [CrossRef]
- Oni, M.O.; Archer, N.M. Intranasal fentanyl works-Why are we not using it more to treat acute pain in sickle cell disease? Am. J. Hematol. 2023, 98, 564–565. [Google Scholar] [CrossRef]
- Pruc, M.; Navolokina, A.; Szarpak, L. Intranasal ketamine for pediatric emergency department lacerations. Am. J. Emerg. Med. 2023, 68, 206. [Google Scholar] [CrossRef] [PubMed]
- Weber, F.; Wulf, H.; el Saeidi, G. Premedication with nasal s-ketamine and midazolam provides good conditions for induction of anesthesia in preschool children. Can. J. Anaesth. 2003, 50, 470–475. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Fernández, M.R.; Ortiz-Ortiz, K.J.; Torres-Cintrón, C.R.; Tortolero-Luna, G. Patterns of End-of-Life Care as Measured by Emergency Room Visits Among Cancer Patients in Puerto Rico. Am. J. Hosp. Palliat. Care 2022, 39, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.S.-K.; Wong, C.H.-L.; Choi, H.C.-W. Cost-Effectiveness of Intranasal Live-Attenuated Influenza Vaccine for Children: A Systematic Review. Vaccines 2022, 10, 1466. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Types of epithelium in the nasal cavity and their role in drug transport.


{kind=link}
Table 1.
Decision path for selecting articles.
| Characteristic | Number of Articles |
|---|---|
| Articles identified by database search | 774 |
| Articles after removing doubles | 626 |
| Articles after title analysis | 458 |
| Articles after analysis of abstracts | 94 |
| Articles after reading the entire text | 62 |
| Articles included in the review | 55 |
Table 2.
List of publications divided according to their research topics.
| Main Research Topic | Number of Papers | Articles |
|---|---|---|
| Intranasal opioids | 27 | [3,22,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55] |
| Intranasal sedatives | 10 | [6,16,50,56,57,58,59,60,61,62] |
| Palliative adults | 20 | [2,6,9,11,16,42,43,44,48,49,51,54,56,57,58,60,63,64,65,66] |
| Palliative children | 10 | [3,22,34,53,58,59,61,62,67,68] |
| Nasal drug delivery systems | 19 | [1,4,7,10,11,14,23,24,25,26,27,28,69,70,71,72,73,74,75] |
| Comparison intranasal vs. another route | 8 | [5,35,47,67,76,77,78,79] |
Table 3.
List of articles on adult palliative patients divided by number of participants. (Ref.—reference number; No.—number of patients; IV—intravenous; IN—intranasal; PO—oral; SC—subcutaneous; CNS—central nervous system; LVAD—left ventricular assist device).
Table 3.
List of articles on adult palliative patients divided by number of participants. (Ref.—reference number; No.—number of patients; IV—intravenous; IN—intranasal; PO—oral; SC—subcutaneous; CNS—central nervous system; LVAD—left ventricular assist device).
| Adult Palliative Patients | |||||
|---|---|---|---|---|---|
| Ref. | No. | Drug Intranasal | Type of Paper | Palliative Indication | Main Finding |
| [44] | 401 | fentanyl | review | breakthrough pain | The most appropriate therapeutic choice is an intranasal opioid (fentanyl spray). |
| [57] | 376 | ketamine | review | Depression | Oral or intranasal ketamine may be the most effective for treating depression at home. |
| [67] | 113 | diamorphine | systematic review | breakthrough pain | Equianalgesic ratios of IV/PO morphine to IN diamorphine is 1:1 and 1:3, respectively. |
| [49] | 75 | fentanyl | original article | breakthrough pain | Long-term use of IN fentanyl is effective and safe (no side effects up to six months). |
| [17] | 60 | dexamethasone | study protocol | severe inflammation | Background—therapeutic doses of dexamethasone in the CNS at low IN doses. |
| [76] | 60 | midazolam | study protocol | agitation | Hypothesis—equivalent reduction in terminal agitation—IN vs. SC midazolam. |
| [47] | 31 | fentanyl | article | pain in sickle cell disease | IN fentanyl and IV morphine similarly reduce pain in vaso-occlusive crisis. |
| [16] | 24 | dexmedetomidine | original research article | procedural pain | IN dexmedetomidine—good alternative to SC opioids in procedural pain. |
| [39] | 24 | fentanyl | research article | dyspnea | Pretreatment with IN fentanyl may improve dyspnea on exertion in palliative patients with heart failure. |
| [48] | 24 | fentanyl | original article | dyspnea | IN fentanyl reduces dyspnea at rest in cancer patients. |
| [6] | 20 | ketamine | article | depression | IN ketamine is effective for depression in cancer patients receiving palliative care. |
| [51] | 20 | fentanyl | short report | agitation, pain | IN fentanyl—acceptable and well tolerated to control end-of-life symptoms at home. |
| [41] | 19 | fentanyl | brief report | dyspnea | No difference between IN fentanyl and placebo in the relief of episodic dyspnea in terminal non-malignant diseases. |
| [42] | 15 | fentanyl | original research | procedural pain | IN fentanyl and IV morphine have similarly high analgesic efficacy in procedural pain in cancer patients. |
| [59] | 14 | dexmedetomidine | review | sedation, pain | Sedation and analgesia are potential therapeutic applications of IN dexmedetomidine in palliative care. |
| [37] | 3 | diamorphine midazolam | case series | pain | IN diamorphine and IN midazolam administered by patients or lay carers at home are acceptable and efficacious. |
| [40] | 1 | midazolam sufentanil | case report | pain dyspnea | IN midazolam and sufentanil—effective strategy for palliative care in patients requesting discontinuation of LVAD. |
| [60] | 1 | dexmedetomidine | case report | procedural sedation | IN dexmedetomidine—effective in the management of complex wound dressings. |
| [80] | 1 | ketamine | case report | mucositis pain in sinonasal carcinoma | IN ketamine—a safe and effective topical treatment for mucositis pain of the sinuses. |
Table 4.
List of articles on pediatric palliative patients divided by number of participants. (Ref.—reference number; No.—number of patients; IV—intravenous; IN—intranasal; ED—emergency department).
Table 4.
List of articles on pediatric palliative patients divided by number of participants. (Ref.—reference number; No.—number of patients; IV—intravenous; IN—intranasal; ED—emergency department).
| Pediatric Palliative Patients | |||||
|---|---|---|---|---|---|
| Ref. | No. | Drug Intranasal | Type of Paper | Palliative Indication | Main Finding |
| [50] | 23,000 | dexmedetomidin, fentanyl, ketamine, midazolam | review | analgosedation | IN analgosedation is a simple, quick, and painless method of treating pain and anxiety in a pediatric emergency department. |
| [34] | 1163 | fentanyl, ketorolac, ketamine | systematic review | pain | IN analgesics may be a good alternative to IM and IV analgesics in children with acute moderate to severe pain. |
| [58] | 165 | ketamine, dexmedetomidine | original article | sedation | IN dexmedetomidine is superior to IN ketamine to provide procedural sedation for radiotherapy in children. |
| [35] | 128 | fentanyl, midazolam, ketamine, dexmedetomidine | research article | procedural dental pain | IN dexmedetomidine-ketamine and IN dexmedetomidine-fentanyl are promising drug combinations with successful anxiolytic and analgesic effects. |
| [36] | 113 | fentanyl | research article | pain in sickle cell disease | Adolescents with sickle cell disease, who frequently visit ED due to pain, were more likely to receive IV or IN opioids. |
| [81] | 111 | fentanyl midazolam | article | pain in burns | Sedoanalgesia with IN fentanyl-midazolam or IN fentanyl in treatment of childhood burns is safe and highly effective. |
| [46] | 75 | fentanyl | research article | pain in sickle cell disease | IN fentanyl is an effective analgesic used to treat episodes of vaso-occlusive pain in children with sickle cell disease. |
| [82] | 30 | ketamine | research article | procedural sedation | Single dose of 6 mg/kg of IN ketamine led to effective sedation in 60% of patients. |
| [53] | 16 | fentanyl | research article | dyspnea | IN fentanyl may be a safe and effective medication for attacks of respiratory distress in pediatric palliative patients. |
| [83] | 8 | dexmedetomidine | case series | dystonia, insomnia | IN dexmedetomidine is a promising approach for sleep disorders or dystonic states in pediatric palliative care children. |
| [62] | 1 | dexmedetomidine | case report | irritability | IN dexmedetomidine may be effective in the treatment of refractory irritability. |
| [61] | 1 | dexmedetomidine | case report | dystonia | IN dexmedetomidine should be considered for symptomatic treatment of intractable dystonia in children. |
| [84] | 1 | dexmedetomidine | case report | insomnia | IN dexmedetomidine may be a safe and effective drug for the treatment of refractory sleep disorders in pediatric palliative patients. |
Table 5.
Proposed intranasal dose of drugs used in palliative medicine.
| Intranasal Drug | Population | Proposed Single Intranasal Dose | Palliative Indications | References |
|---|---|---|---|---|
| morfine | children | 0.1 mg/kg | pain | [67] |
| adults | 0.1 mg/kg | pain | [67] | |
| diamorphine | children | 0.1 mg/kg | pain | [48] |
| adults | 1.25–2.5 mg | pain | [69] | |
| 2.5 mg | pain | [37] | ||
| fentanyl | children | 0.5–2 mcg/kg | pain | [34] |
| 1.5–2 mcg/kg | procedural dental pain, sedation | [35,50] | ||
| adults | 100–400 mcg | control symptoms in the dying | [40,51] | |
| 50–100 mcg | pain | [69] | ||
| 100 mcg | dyspnea, pain in sickle cell disease | [47,48] | ||
| 100–800 mcg | pain | [44] | ||
| 50 mcg | dyspnea | [39] | ||
| ketamine | children | 5 mg/kg | procedural sedation | [58] |
| 1–4 mg/kg | procedural dental pain | [35] | ||
| 6 mg/kg | procedural sedation | [82] | ||
| 1.0–1.5 mg/kg | pain | [34] | ||
| adults | 50–100 mg | depression | [6] | |
| 50 mg | nasal mucositis pain | [80] | ||
| ipratropium | adults | 41 mcg | respiratory secretion | [69] |
| dexmedetomidine | children | 2.5 mcg/kg | procedural sedation, dystonia | [58,59,61,83] |
| 3 mcg/kg | insomnia | [84] | ||
| 0.5–4 mcg/kg | sedation | [50] | ||
| 1 mcg/kg | procedural dental pain | [35] | ||
| adults | 1–1.5 mcg/kg | pain, sedation | [60] | |
| 1.25 mcg/kg | pain, anxiety | [16] | ||
| dexamethasone | adults | 0.12 mg/kg for 3 days, next 0.06 mg/kg for 7 days | severe inflammation in COVID-19 | [17] |
| midazolam | children | 0.2–0.5 mg/kg | sedation | [50] |
| 0.2 mg/kg | status epilepticus | [56] | ||
| adults | 5 mg | agitation | [76] | |
| 2.5–5 mg | agitation | [37] | ||
| 0.2 mg/kg | status epilepticus | [88] | ||
| lorazepam | children | 0.05 mg/kg | status epilepticus | [56] |
| ketorolac | children | 1 mg/kg | pain | [34] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ingielewicz, A.; Szymczak, R.K. Intranasal Therapy in Palliative Care. Pharmaceutics 2024, 16, 519. https://doi.org/10.3390/pharmaceutics16040519
AMA Style
Ingielewicz A, Szymczak RK. Intranasal Therapy in Palliative Care. Pharmaceutics. 2024; 16(4):519. https://doi.org/10.3390/pharmaceutics16040519
Chicago/Turabian StyleIngielewicz, Anna, and Robert K. Szymczak. 2024. "Intranasal Therapy in Palliative Care" Pharmaceutics 16, no. 4: 519. https://doi.org/10.3390/pharmaceutics16040519
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.