

Cardioprotective and Hepatoprotective Potential of Silymarin in Paracetamol-Induced Oxidative Stress
 , , , , ,
, , , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Chemicals
2.2. Animals
2.3. In Vivo Experimental Design
- First (control) group—saline solution 1 mL/kg, seven days p.o.;
- Second group—saline solution 1 mL/kg seven days p.o. + toxic unidose of paracetamol 110 mg/kg p.o.;
- Third group—silymarin 50 mg/kg, seven days p.o.;
- Fourth group—silymarin 50 mg/kg, seven days p.o. + toxic unidose of paracetamol 110 mg/kg p.o.
2.4. Antioxidant Activity
2.4.1. DPPH Assay
2.4.2. FRAP Assay
2.4.3. ABTS Assay
2.5. Liver Function Tests
2.6. Histopathology and Immunohistochemistry Assessment
2.7. Determination of In Vivo Antioxidant Activity
2.8. Statistical Analysis
3. Results
3.1. In Vitro Antioxidant Potential Examinations
3.2. Effects of Silymarin on Liver and Kidney Function Tests, Lipid Profile, and Oxidative Stress Enzyme Measurments
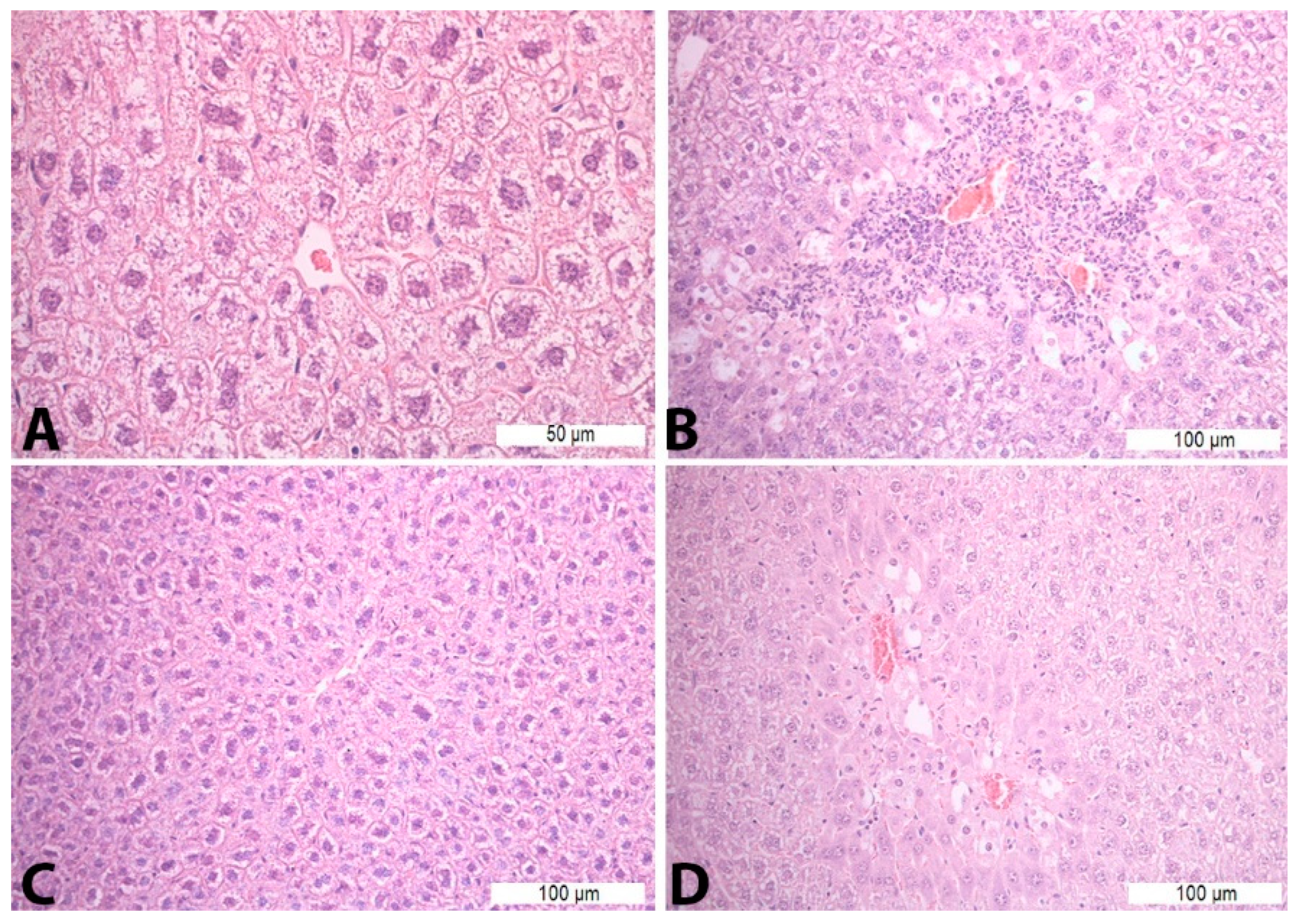
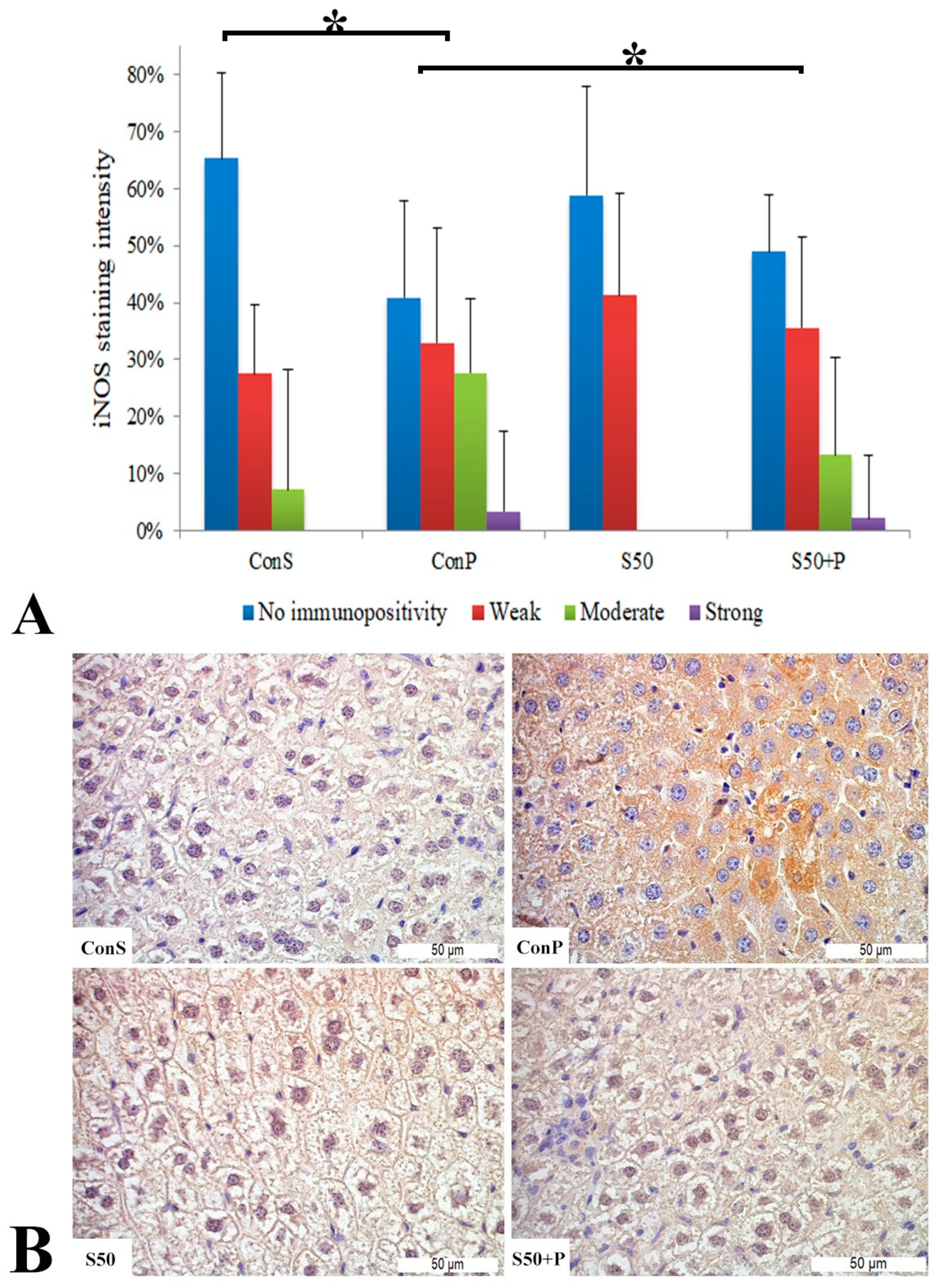
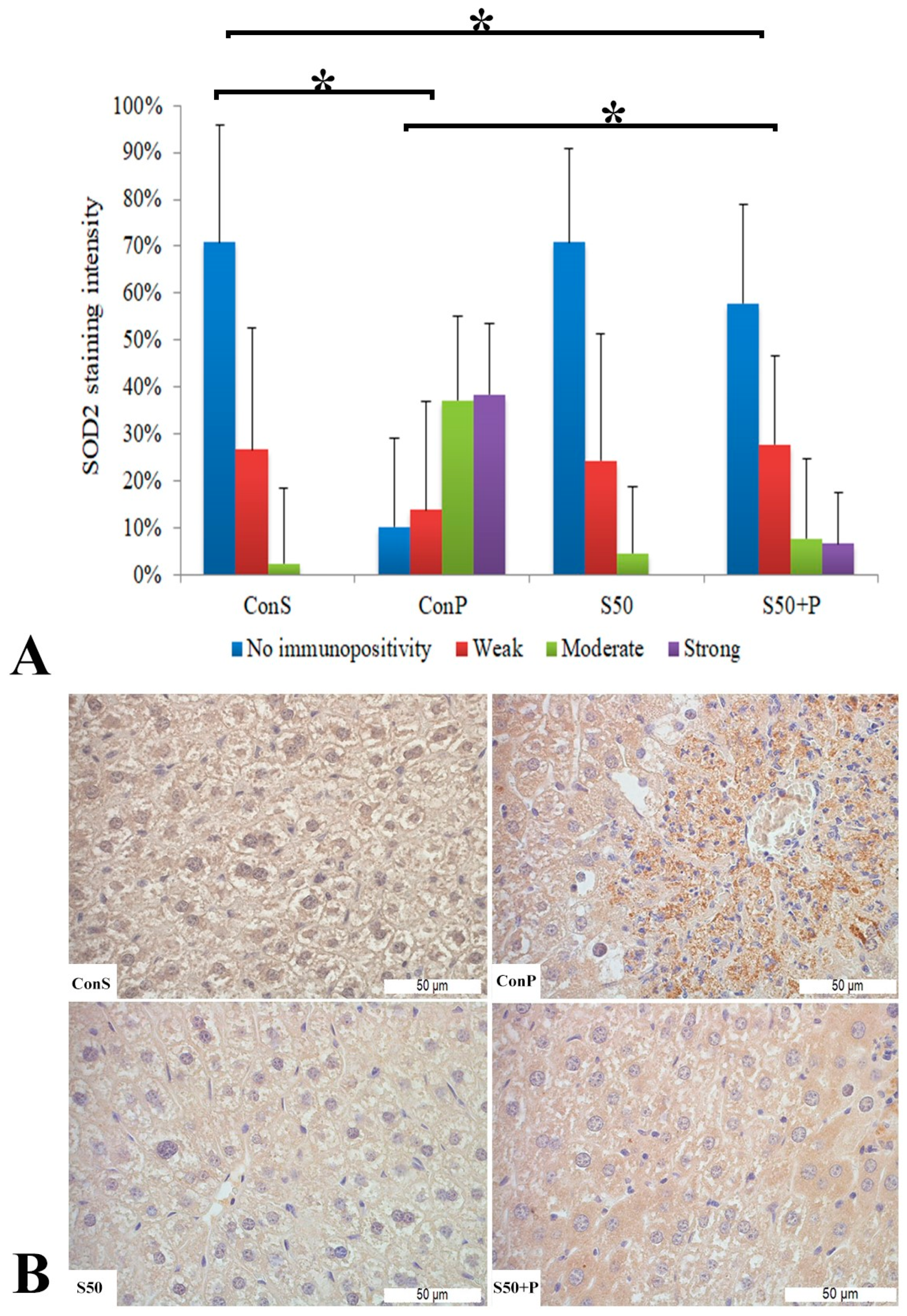
3.3. Histopathological Analysis of Liver Tissue
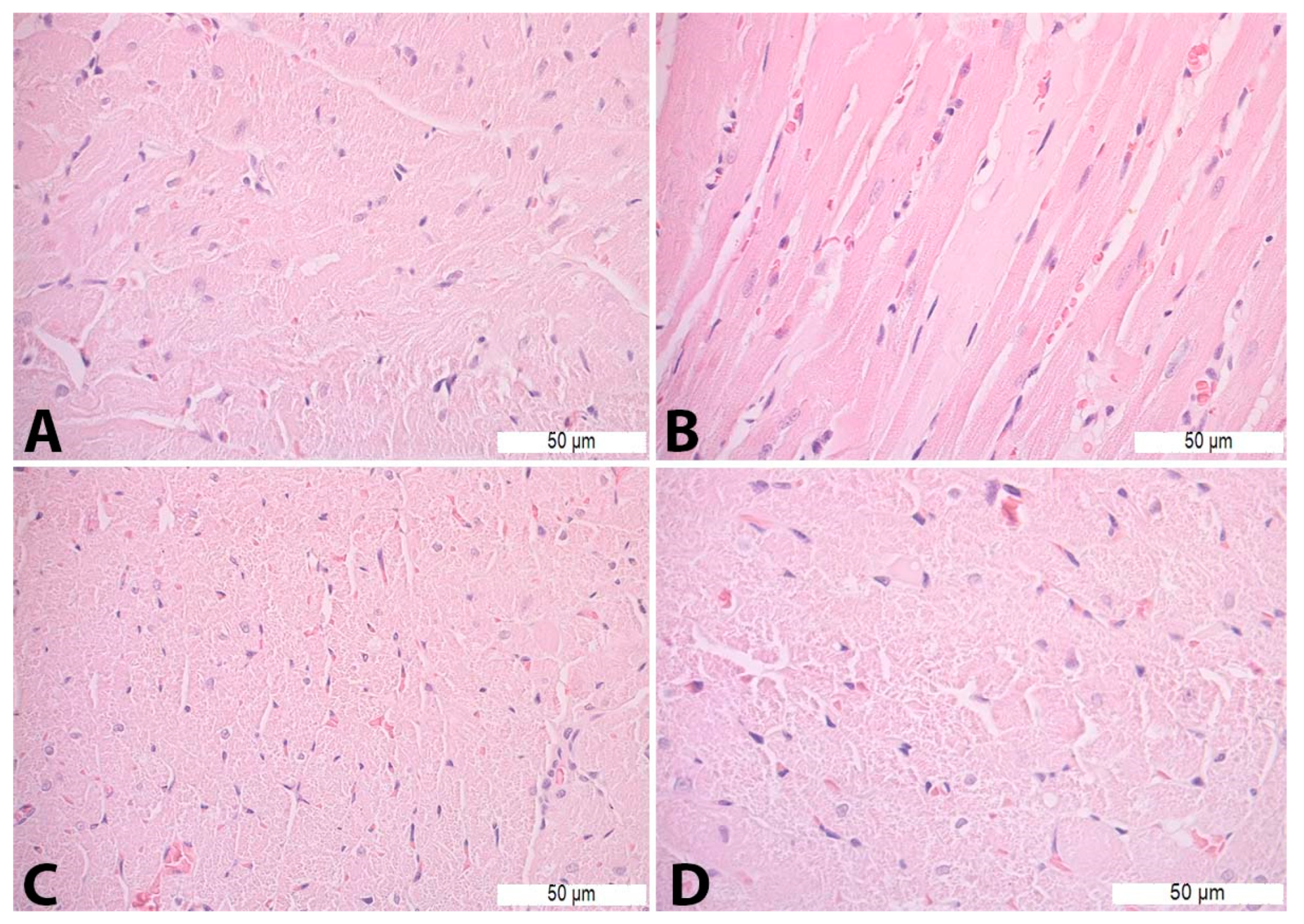
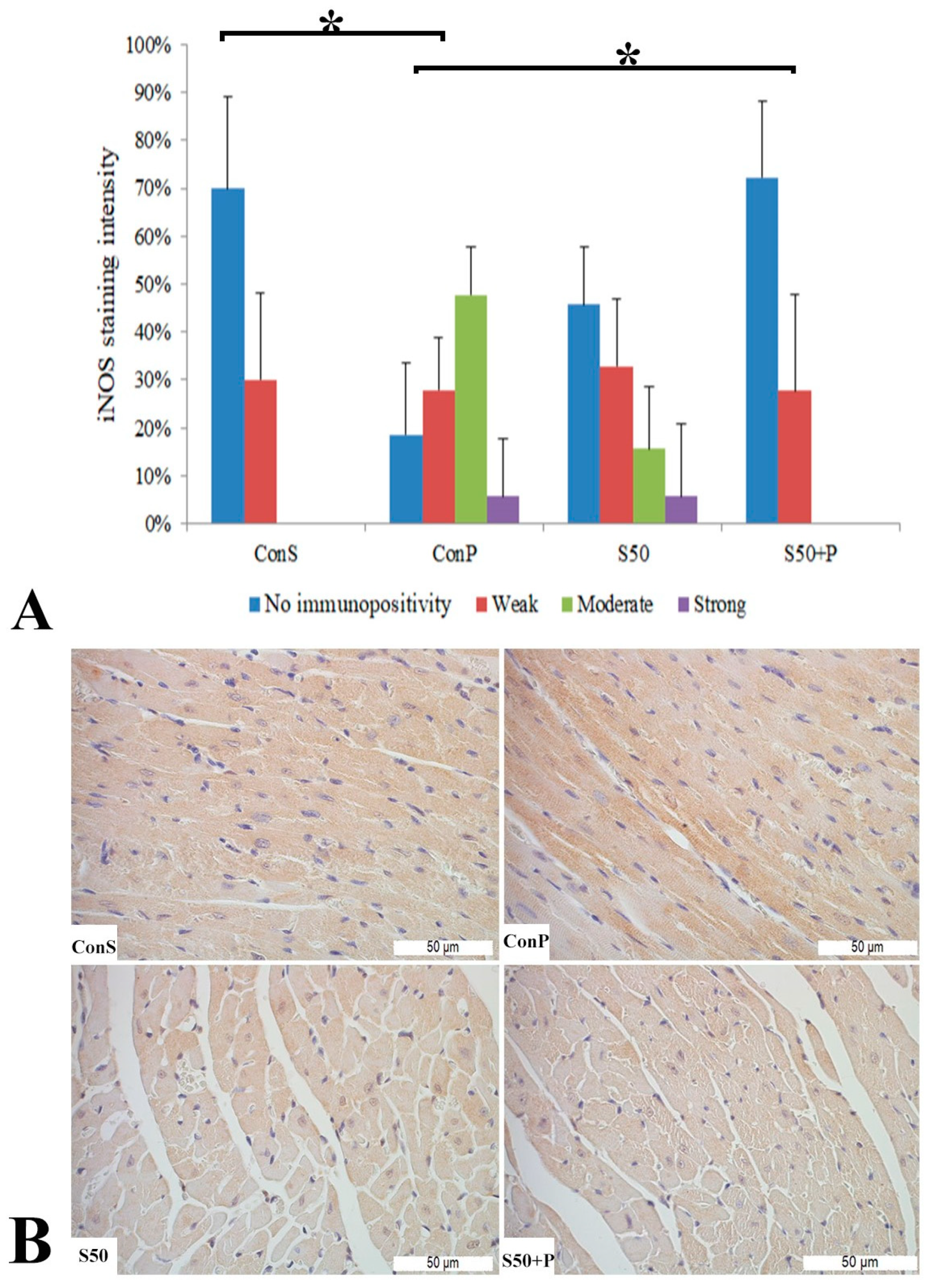
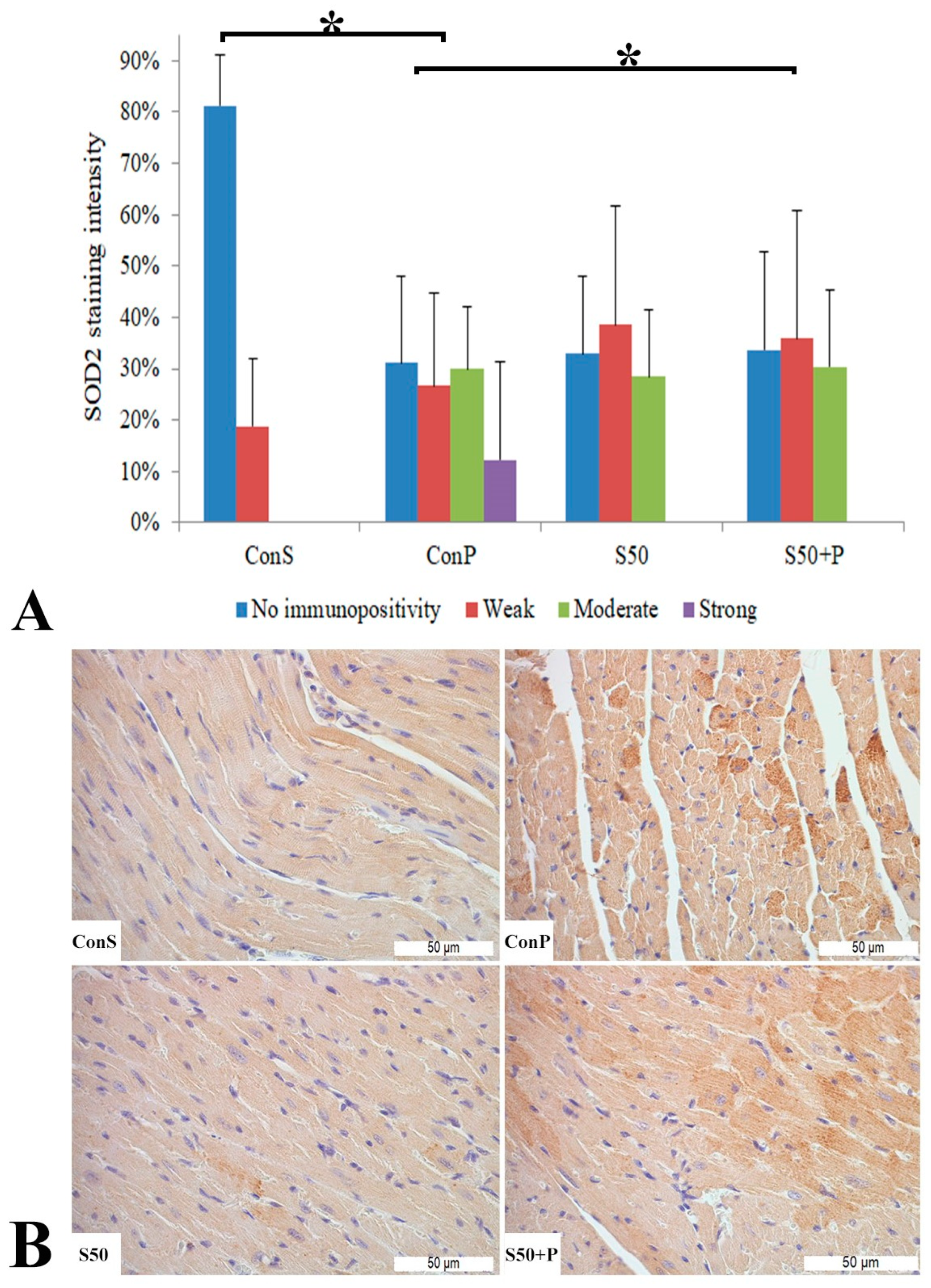
3.4. Histopathological Analysis of Heart Tissue
4. Discussion
4.1. Effects of Silymarin on Paracetamol-Induced Oxidative Stress—Serum Biochemical Parameters
4.2. Effects of Silymarin on Paracetamol-Induced Oxidative Stress—Liver Tissue
4.3. Effects of Silymarin on Paracetamol-Induced Oxidative Stress—Heart Tissue
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Javed, S.; Kohli, K.; Ali, M. Reassessing bioavailability of silymarin. Altern. Med. Rev. 2011, 16, 239. [Google Scholar] [PubMed]
- Kvasnička, F.; Bıba, B.; Ševčık, R.; Voldřich, M.; Kratka, J. Analysis of the active components of silymarin. J. Chromatogr. A 2003, 990, 239–245. [Google Scholar] [CrossRef]
- Křen, V.; Walterová, D. Silybin and silymarin-new effects and applications. Biomed. Pap. 2005, 149, 29–41. [Google Scholar] [CrossRef]
- Wu, J.W.; Lin, L.C.; Tsai, T.H. Drug–drug interactions of silymarin on the perspective of pharmacokinetics. J. Ethnopharmacol. 2009, 121, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Fraschini, F.; Demartini, G.; Esposti, D. Pharmacology of silymarin. Clin. Drug Investig. 2002, 22, 51–65. [Google Scholar] [CrossRef]
- Valenzuela, A.L.; Garrido, A.R. Biochemical bases of the pharmacological action of the flavonoid silymarin and of its structural isomer silibinin. Biol. Res. 1994, 27, 105–112. [Google Scholar] [PubMed]
- Halliwell, B. Free radicals, antioxidants, and human disease: Curiosity, cause, or consequence? Lancet 1994, 344, 721–724. [Google Scholar] [CrossRef]
- Singal, P.K.; Khaper, N.; Palace, V.; Kumar, D. The role of oxidative stress in the genesis of heart disease. Cardiovasc. Res. 1998, 40, 426–432. [Google Scholar] [CrossRef]
- Deavall, D.G.; Martin, E.A.; Horner, J.M.; Roberts, R. Drug-induced oxidative stress and toxicity. J. Toxicol. 2012, 2012, 645460. [Google Scholar] [CrossRef]
- Li, S.; Tan, H.Y.; Wang, N.; Zhang, Z.J.; Lao, L.; Wong, C.W.; Feng, Y. The role of oxidative stress and antioxidants in liver diseases. Int. J. Mol. Sci. 2015, 16, 26087–26124. [Google Scholar] [CrossRef]
- Costa, V.M.; Carvalho, F.; Duarte, J.A.; Bastos, M.D.; Remião, F. The heart as a target for xenobiotic toxicity: The cardiac susceptibility to oxidative stress. Chem. Res. Toxicol. 2013, 26, 1285–1311. [Google Scholar] [CrossRef]
- McGill, M.R.; Williams, C.D.; Xie, Y.; Ramachandran, A.; Jaeschke, H. Acetaminophen-induced liver injury in rats and mice: Comparison of protein adducts, mitochondrial dysfunction, and oxidative stress in the mechanism of toxicity. Toxicol. Appl. Pharmacol. 2012, 264, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wu, Q.; Liu, A.; Anadón, A.; Rodríguez, J.L.; Martínez-Larrañaga, M.R.; Zonghui, Y.; Martínez, M.A. Paracetamol: Overdose-induced oxidative stress toxicity, metabolism, and protective effects of various compounds in vivo and in vitro. Drug Metab. Rev. 2017, 49, 395–437. [Google Scholar] [CrossRef]
- Gomaa, S. Adverse effects induced by diclofenac, ibuprofen, and paracetamol toxicity on immunological and biochemical parameters in Swiss albino mice. JOBAZ 2018, 79, 5. [Google Scholar] [CrossRef]
- Safarpour, S.; Safarpour, S.; Moghadamnia, A.A.; Kazemi, S.; Ebrahimpour, A.; Shirafkan, F.; Mansoori, R.; Golchoobian, R. Cardioprotective effect of silymarin nanoemulsion on 5-fluorouracil-induced cardiotoxicity in rats. Arch. Pharm. 2022, 355, 2200060. [Google Scholar] [CrossRef] [PubMed]
- Rašković, A.; Stilinović, N.; Kolarović, J.; Vasović, V.; Vukmirović, S.; Mikov, M. The protective effects of silymarin against doxorubicin-induced cardiotoxicity and hepatotoxicity in rats. Molecules 2011, 16, 8601–8613. [Google Scholar] [CrossRef] [PubMed]
- Afsar, T.; Razak, S.; Almajwal, A.; Shabbir, M.; Khan, M.R. Evaluating the protective potency of Acacia hydaspica R. Parker on histological and biochemical changes induced by Cisplatin in the cardiac tissue of rats. BMC Complement. Altern. Med. 2019, 19, 182. [Google Scholar] [CrossRef]
- Rao, P.R.; Viswanath, R.K. Cardioprotective activity of silymarin in ischemia-reperfusion-induced myocardial infarction in albino rats. Exp. Clin. Cardiol. 2007, 12, 179. [Google Scholar]
- Brand-Williams, W.; Cuvelier, M.E.; Berset, C. Use of a free radical method to evaluate antioxidant activity. LWT-Food Sci. Technol. 1995, 28, 25–30. [Google Scholar] [CrossRef]
- Benzie, I.F.; Strain, J.J. The ferric reducing ability of plasma (FRAP) as a measure of “antioxidant power”: The FRAP assay. Anal. Biochem. 1996, 239, 70–76. [Google Scholar] [CrossRef]
- Re, R.; Pellegrini, N.; Proteggente, A.; Pannala, A.; Yang, M.; Rice-Evans, C. Antioxidant activity applying an improved ABTS radical cation decolorization assay. Free Radic. Biol. Med. 1999, 26, 1231–1237. [Google Scholar] [CrossRef] [PubMed]
- Rašković, A.; Ćućuz, V.; Torović, L.; Tomas, A.; Gojković-Bukarica, L.; Ćebović, T.; Milijašević, B.; Stilinović, N.; Hogervorst, J.C. Resveratrol supplementation improves metabolic control in rats with induced hyperlipidemia and type 2 diabetes. Saudi Pharm. J. 2019, 27, 1036–1043. [Google Scholar] [CrossRef] [PubMed]
- Buege, J.A.; Aust, S.D. Microsomal lipid peroxidation. Meth Enzymol. 1978, 52, 302–310. [Google Scholar]
- McCord, J.M.; Fridovich, I. Superoxide dismutase: An enzymic function for erythrocuprein (hemocuprein). J. Biol. Chem. 1969, 244, 6049–6055. [Google Scholar] [CrossRef] [PubMed]
- Liyana-Pathirana, C.; Shahidi, F. Optimization of extraction of phenolic compounds from wheat using response surface methodology. Food Chem. 2005, 93, 47–56. [Google Scholar] [CrossRef]
- Beers, R.F.; Sizer, I.W. A spectrophotometric method for measuring the breakdown of hydrogen peroxide by catalase. J. Biol. Chem. 1952, 195, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Beutler, E. Red Cell Metabolism: A Manual of Biochemical Methods, 3rd ed.; Grune & Stratton Inc.: New York, NY, USA, 1984. [Google Scholar]
- Khatri, D.; Chhetri, S.B.B.; Devkota, H.P. Silybum marianum (L.) Gaertn.: Traditional Uses, Phytochemistry, and Pharmacological Activities. In Medicinal Plants of the Asteraceae Family: Traditional Uses, Phytochemistry and Pharmacological Activities; Springer Nature: Singapore, 2022; pp. 213–230. [Google Scholar]
- Magalhães, L.M.; Segundo, M.A.; Reis, S.; Lima, J.L. Methodological aspects about in vitro evaluation of antioxidant properties. Anal. Chim. Acta 2008, 613, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Villegas-Aguilar, M.D.C.; Sánchez-Marzo, N.; Fernández-Ochoa, Á.; Del Río, C.; Montaner, J.; Micol, V.; Segura-Carretero, A. Evaluation of Bioactive Effects of Five Plant Extracts with Different Phenolic Compositions against Different Therapeutic Targets. Antioxidants 2024, 13, 217. [Google Scholar] [CrossRef] [PubMed]
- Razavi, B.M.; Karimi, G. Protective effect of silymarin against chemical-induced cardiotoxicity. Iran. J. Basic. Med. Sci. 2016, 19, 916. [Google Scholar]
- Vargas-Mendoza, N.; Madrigal-Santillán, E.; Morales-González, Á.; Esquivel-Soto, J.; Esquivel-Chirino, C.; y González-Rubio, M.G.; A Gayosso-de-Lucio, J.; A Morales-González, J. Hepatoprotective effect of silymarin. World J. Hepatol. 2014, 6, 144. [Google Scholar] [CrossRef]
- Mossanen, J.C.; Tacke, F. Acetaminophen-induced acute liver injury in mice. Lab. Anim. 2015, 49, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Aktas, I.; Ozgocmen, M. The treatment effect of silymarin on heart damage in rats. Ann. Med. Res. 2020, 27, 948–954. [Google Scholar] [CrossRef]
- Gabrielová, E.; Bartošíková, L.; Nečas, J.; Modrianský, M. Cardioprotective effect of 2, 3-dehydrosilybin preconditioning in isolated rat heart. Fitoterapia 2019, 132, 12–21. [Google Scholar] [CrossRef] [PubMed]
- KhabazianZadeh, F.; Kazemi, T.; Nakhaee, S.; Ng, P.C.; Mehrpour, O. Acetaminophen poisoning-induced heart injury: A case-based review. Daru 2019, 27, 839–851. [Google Scholar] [CrossRef]
- Nelson, S.D. Molecular mechanisms of the hepatotoxicity caused by acetaminophen. Sem. Liver Dis. 1990, 10, 267–278. [Google Scholar] [CrossRef] [PubMed]
- Mladenović, D.; Radosavljević, T.; Ninković, M.; Vučević, D.; Ješić-Vukićević, R.; Todorović, V. Liver antioxidant capacity in the early phase of acute paracetamol-induced liver injury in mice. Food Chem. Toxicol. 2009, 47, 866–870. [Google Scholar] [CrossRef] [PubMed]
- Hamza, R.Z.; Al-Harbi, M.S. Amelioration of paracetamol hepatotoxicity and oxidative stress on mice liver with silymarin and Nigella sativa extract supplements. Asian Pac. J. Trop. Biomed. 2015, 5, 521–531. [Google Scholar] [CrossRef]
- Hau, D.K.; Wong, R.S.; Cheng, G.Y.; Wong, W.Y.; Tong, S.W.; Chan, K.W.; Leung, A.K.; Zhu, G.Y.; Lai, P.B.; Lau, F.Y.; et al. Novel use of silymarin as delayed therapy for acetaminophen-induced acute hepatic injury. Complement. Med. Res. 2010, 17, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Bektur, N.E.; Sahin, E.; Baycu, C.; Unver, G. Protective effects of silymarin against acetaminophen-induced hepatotoxicity and nephrotoxicity in mice. Toxicol. Ind. Health 2016, 32, 589–600. [Google Scholar] [CrossRef]
- Gopi, K.S.; Reddy, A.G.; Jyothi, K.; Kumar, B.A. Acetaminophen-induced Hepato-and Nephrotoxicity and Amelioration by Silymarin and Terminalia chebula in Rats. Toxicol. Int. 2010, 17, 64. [Google Scholar]
- Papackova, Z.; Heczkova, M.; Dankova, H.; Sticova, E.; Lodererova, A.; Bartonova, L.; Poruba, M.; Cahova, M. Silymarin prevents acetaminophen-induced hepatotoxicity in mice. PLoS ONE 2018, 13, e0191353. [Google Scholar] [CrossRef] [PubMed]
- Taghiabadi, E.; Imenshahidi, M.; Abnous, K.; Mosafa, F.; Sankian, M.; Memar, B.; Karimi, G. Protective effect of silymarin against acrolein-induced cardiotoxicity in mice. eCAM 2012, 2012, 352091. [Google Scholar] [CrossRef] [PubMed]
- Simeonova, R.; Vitcheva, V.; Kondeva-Burdina, M.; Krasteva, I.; Manov, V.; Mitcheva, M. Hepatoprotective and antioxidant effects of saponarin, isolated from Gypsophila trichotoma Wend. on paracetamol-induced liver damage in rats. Biomed. Res. Int. 2013, 2013, 757126. [Google Scholar] [CrossRef] [PubMed]
- Soliman, A.M.; Rizk, H.A.; Shalaby, M.A.; Elkomy, A.A. Mechanisms of hepato-renal protective activity of Ocimum basilicum leaf extract against paracetamol toxicity in rat model. Adv. Anim. Vet. Sci. 2020, 8, 385–391. [Google Scholar] [CrossRef]
- Basol, N.; Ozmen, C.; Ocakli, S.; Cetin, S. Evaluation of the effects of curcumin, erdosteine, vitamin E and vitamin C on paracetamol toxicity. Medicine 2022, 11, 465–470. [Google Scholar] [CrossRef]
- Pawar, S.S.; Velhal, A.B.; Chaware, V.J.; Redasani, V.K. Evaluation of hepatoprotective activity of amalgamation of kutkuti (tridax procumbens) and ginger juice against paracetamol induced hepatotoxicity in rats. J. Popul. Ther. Clin. Pharmacol. 2023, 30, 2039–2048. [Google Scholar] [CrossRef]
- Yousef, M.I.; Omar, S.A.; El-Guendi, M.I.; Abdelmegid, L.A. Potential protective effects of quercetin and curcumin on paracetamol-induced histological changes, oxidative stress, impaired liver and kidney functions and haematotoxicity in rat. Food Chem. Toxicol. 2010, 48, 3246–3261. [Google Scholar] [CrossRef]
- Ralapanawa, U.; Jayawickreme, K.P.; Ekanayake, E.M.; Dissanayake, A.D. A study on paracetamol cardiotoxicity. BMC Pharmacol. Toxicol. 2016, 17, 30. [Google Scholar] [CrossRef]
- Talaat, A.; Elgendy, Y.A.; Mohamed, H.F.; Saed, N.M.; Abd Elrouf, N.A.; Elgendy, H.A.; Elbalakousy, H.H.; Elmezaien, M.S.; Sayed, Y.M.; Hekal, Y.E.; et al. Ameliorative effects of frankincense oil on rats treated with a minimum toxic dose of paracetamol. J. Med. Life Sci. 2023, 5, 155–175. [Google Scholar]
- Di Lisi, D.; Bonura, F.; Macaione, F.; Peritore, A.; Meschisi, M.; Cuttitta, F.; Novo, G.; Novo, S. Chemotherapy-induced cardiotoxicity: Role of the tissue Doppler in the early diagnosis of left ventricular dysfunction. Anti-Cancer Drugs 2011, 22, 468–472. [Google Scholar] [CrossRef]
- Ratterree, W.; Gieger, T.; Pariaut, R.; Saelinger, C.; Strickland, K. Value of echocardiography and electrocardiography as screening tools prior to doxorubicin administration. J. Am. Anim. Hosp. Assoc. 2012, 48, 89–96. [Google Scholar] [CrossRef]
- Graham, G.G.; Scott, K.F. Mechanisms of action of paracetamol and related analgesics. Inflammopharmacology 2003, 11, 401–413. [Google Scholar] [CrossRef]
- Reilly, T.P.; Brady, J.N.; Marchick, M.R.; Bourdi, M.; George, J.W.; Radonovich, M.F.; Pise-Masison, C.A.; Pohl, L.R. A protective role for cyclooxygenase-2 in drug-induced liver injury in mice. Chem. Res. Toxicol. 2001, 14, 1620–1628. [Google Scholar] [CrossRef] [PubMed]
- Oz, H.S.; Chen, T.S. Green-tea polyphenols downregulate cyclooxygenase and Bcl-2 activity in acetaminophen-induced hepatotoxicity. Dig. Dis. Sci. 2008, 53, 2980–2988. [Google Scholar] [CrossRef]
- Eltahir, H.M.; Fawzy, M.A.; Mohamed, E.M.; Alrehany, M.A.; Shehata, A.M.; Abouzied, M.M. Antioxidant, anti-inflammatory and anti-fibrotic effects of Boswellia serrate gum resin in CCl4-induced hepatotoxicity. Exp. Ther. Med. 2020, 19, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Du, K.; Ramachandran, A.; Jaeschke, H. Oxidative stress during acetaminophen hepatotoxicity: Sources, pathophysiological role and therapeutic potential. Redox Biol. 2016, 10, 148–156. [Google Scholar] [CrossRef]
- Hussein, R.M.; Kandeil, M.A.; Mohammed, N.A.; Khallaf, R.A. Evaluation of the hepatoprotective effect of curcumin-loaded solid lipid nanoparticles against paracetamol overdose toxicity: Role of inducible nitric oxide synthase. J. Liposome Res. 2022, 32, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Aksun, S.; Gökcimen, A.; Kahyaoglu, F.; Demirci, B. The effect of Paracetamol exposure on hepatic and renal tissues during statin usage. Turk. J. Biochem. 2019, 44, 113–120. [Google Scholar] [CrossRef]
- Attia, G.M.; Elmansy, R.A.; Algaidi, S.A. Silymarin decreases the expression of VEGF-A, iNOS and caspase-3 and preserves the ultrastructure of cardiac cells in doxorubicin induced cardiotoxicity in rats: A possible protective role. Int. J. Clin. Exp. Med. 2017, 10, 4158–4173. [Google Scholar]
- Guo, H.; Sun, J.; Li, D.; Hu, Y.; Yu, X.; Hua, H.; Jing, X.; Chen, F.; Jia, Z.; Xu, J. Shikonin attenuates acetaminophen-induced acute liver injury via inhibition of oxidative stress and inflammation. Biomed. Pharmacother. 2019, 112, 108704. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DPPH (mM TE/g) | FRAP (mM Fe2+/g) | ABTS (mM TE/g) | |
|---|---|---|---|
| Silymarin | 0.7148 ± 0.0064 | 4.6759 ± 0.0208 | 5.0478 ± 0.0283 |
| Con S | Con P | S50 | S50+P | |
|---|---|---|---|---|
| ALT (U/L) | 49.83 ± 5.34 | 72.75 ± 12.45 a | 53.80 ± 6.01 b | 56.00 ± 8.29 b |
| AST (U/L) | 127.80 ± 33.34 | 257.00 ± 46.94 a | 147.50 ± 13.82 b | 151.29 ± 39.38 b |
| Total bilirubin (µmol/L) | 2.06 ± 0.25 | 2.50 ± 0.54 | 2.30 ± 0.24 | 2.62 ± 0.28 |
| Urea (mmol/L) | 6.50 ± 0.45 | 7.68 ± 1.03 | 6.01 ± 0.17 | 6.70 ± 0.28 |
| Creatinine (μmol/L) | 29.78 ± 1.08 | 33.04 ± 5.30 | 29.64 ± 0.85 | 31.44 ± 1.95 |
| Uric acid (μmol/L) | 265.00 ± 5.48 | 256.67 ± 27.33 | 218.33 ± 19.41 | 180.00 ± 17.32 a,b |
| Triglycerides (mmol/L) | 1.31 ± 0.23 | 2.25 ± 0.12 a | 1.27 ± 0.10 b | 1.69 ± 0.45 b |
| Cholesterol (mmol/L) | 3.81 ± 0.36 | 3.93 ± 0.99 | 3.51 ± 0.27 | 3.85 ± 0.33 |
| HDL (mmol/L) | 2.11 ± 0.14 | 1.88 ± 0.48 | 2.01 ± 0.13 | 1.98 ± 0.29 |
| LDL (mmol/L) | 0.98 ± 0.29 | 1.25 ± 0.66 | 0.92 ± 0.15 | 1.12 ± 0.22 |
| Con S | Con P | S50 | S50+P | |
|---|---|---|---|---|
| LP (nmol MDA/mg proteins) | 0.116 ± 0.021 | 0.177 ± 0.036 a | 0.092 ± 0.023 | 0.131 ± 0.014 b |
| SOD (U/mg proteins) | 26.25 ± 1.91 | 13.57 ± 2.81 a | 27.22 ± 3.70 | 20.89 ± 1.82 b |
| CAT (U/mg proteins) | 82.03 ± 9.46 | 46.19 ± 4.50 a | 80.41 ± 5.16 | 75.72 ± 3.78 b |
| GPx (nmol/mg proteins) | 45.94 ± 3.93 | 29.87 ± 4.59 a | 46.10 ± 2.74 b | 38.99 ± 4.60 b |
| GR (nmol/mg proteins) | 16.85 ± 3.55 | 13.40 ± 3.23 | 14.26 ± 2.69 | 15.48 ± 3.65 |
| GST (nmol/mg proteins) | 40.52 ± 4.94 | 17.89 ± 2.97 a | 38.47 ± 5.34 a,b | 31.93 ± 4.38 b |
| Con S | Con P | S50 | S50+P | |
|---|---|---|---|---|
| LP (nmol MDA/mg proteins) | 0.82 ± 0.010 | 0.138 ± 0.019 a | 0.076 ± 0.017 b | 0.098 ± 0.012 b |
| SOD (U/mg proteins) | 16.47 ± 1.73 | 11.25 ± 1.80 a | 15.57 ± 1.51 | 15.12 ± 1.61 b |
| CAT (U/mg proteins) | 56.19 ± 4.50 | 44.03 ± 3.72 a | 53.38 ± 4.38 | 51.74 ± 2.87 b |
| GPx (nmol/mg proteins) | 39.87 ± 4.59 | 36.05 ± 3.93 | 43.10 ± 5.74 | 38.99 ± 4.60 |
| GR (nmol/mg proteins) | 13.40 ± 2.01 | 10.85 ± 2.49 | 14.48 ± 3.65 | 12.26 ± 2.69 |
| GST (nmol/mg proteins) | 27.89 ± 2.97 | 23.52 ± 1.94 | 29.47 ± 2.34 | 25.93 ± 1.38 |
| Con S | Con P | S50 | S50+P | |
|---|---|---|---|---|
| Necrosis | 0% | 7.8% a | 0% | 3.3% b |
| Inflamatory infiltrate | 0% | 15.9% a | 1.2% | 8.2% b |
| Con S | Con P | S50 | S50+P | |
|---|---|---|---|---|
| COX2 | 2% | 19.7% a | 5.4% | 10.58% b |
| iNOS | 4.5% | 27.3% a | 16.78% | 5.94% b |
| SOD2 | 1.4% | 15.2% a | 10.6% | 8.8% b |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okiljević, B.; Martić, N.; Govedarica, S.; Andrejić Višnjić, B.; Bosanac, M.; Baljak, J.; Pavlić, B.; Milanović, I.; Rašković, A. Cardioprotective and Hepatoprotective Potential of Silymarin in Paracetamol-Induced Oxidative Stress. Pharmaceutics 2024, 16, 520. https://doi.org/10.3390/pharmaceutics16040520
Okiljević B, Martić N, Govedarica S, Andrejić Višnjić B, Bosanac M, Baljak J, Pavlić B, Milanović I, Rašković A. Cardioprotective and Hepatoprotective Potential of Silymarin in Paracetamol-Induced Oxidative Stress. Pharmaceutics. 2024; 16(4):520. https://doi.org/10.3390/pharmaceutics16040520
Chicago/Turabian StyleOkiljević, Bogdan, Nikola Martić, Srđan Govedarica, Bojana Andrejić Višnjić, Milana Bosanac, Jovan Baljak, Branimir Pavlić, Isidora Milanović, and Aleksandar Rašković. 2024. "Cardioprotective and Hepatoprotective Potential of Silymarin in Paracetamol-Induced Oxidative Stress" Pharmaceutics 16, no. 4: 520. https://doi.org/10.3390/pharmaceutics16040520