Mortality Predictors for Adult Patients with Mild-to-Moderate Traumatic Brain Injury: A Literature Review

 , , and
, , and
Abstract
:1. Introduction
2. Methods
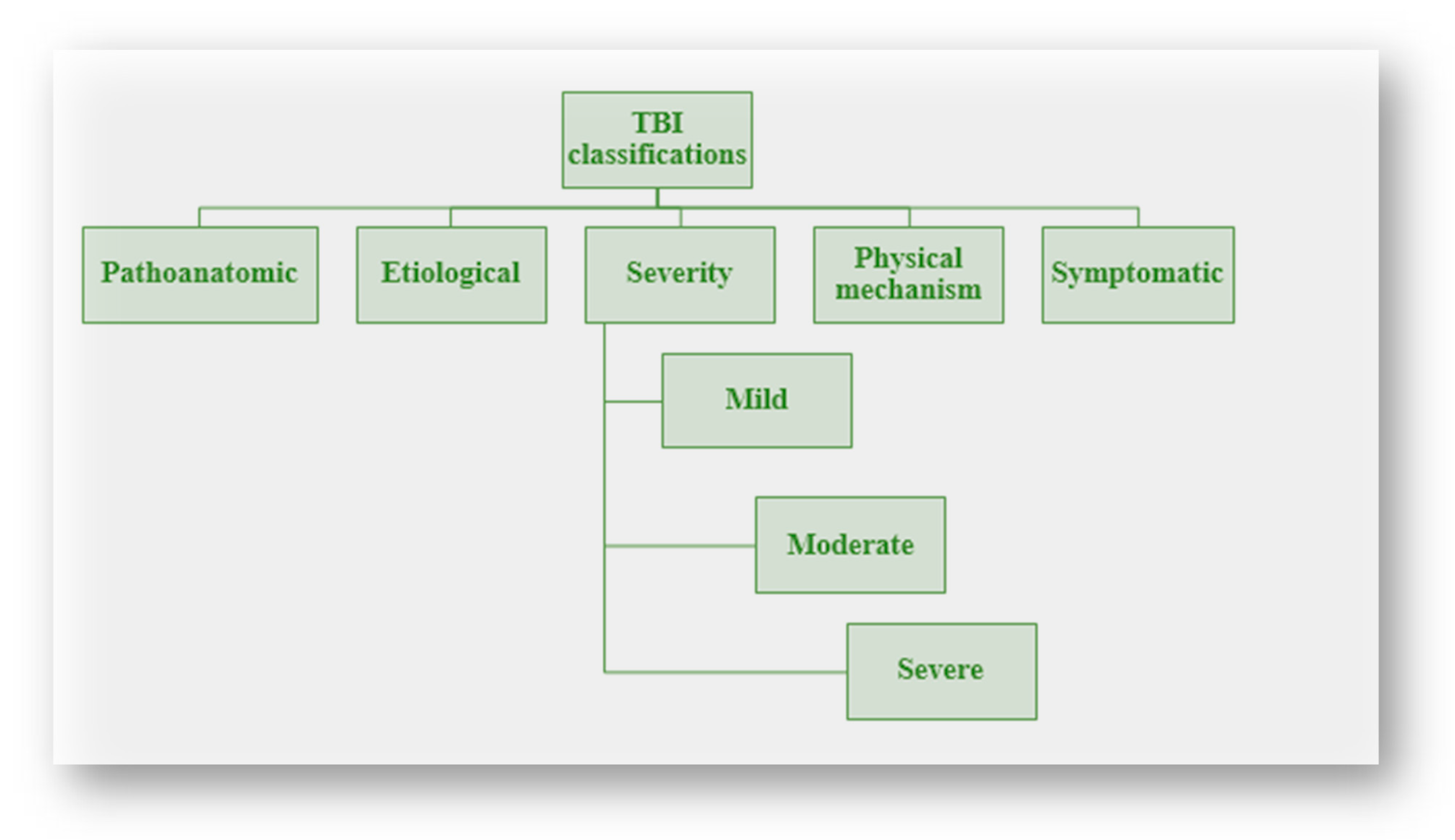
3. TBI Severity Classification
4. Mortality Predictors and Rates of Mild–Moderate TBIs
5. Biomarkers in Traumatic Brain Injury
6. Miscellaneous Factors Affect TBI Outcome
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Amare, A.T.; Tesfaye, T.D.; Ali, A.S.; Woelile, T.A.; Birlie, T.A.; Kebede, W.M.; Tassew, S.F.; Chanie, E.S.; Feleke, D.G. Survival Status and Predictors of Mortality among Traumatic Brain Injury Patients in an Ethiopian Hospital: A Retrospective Cohort Study. Afr. J. Emerg. Med. 2021, 11, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Tesfaw, A.; Eshetu, M.; Teshome, F.; Fenta, E.; Gelaw, M.; Mihret, G.; Atiklt, G.; Yosef, T. Prevalence of Head Injury Among Trauma Patients at Debre Tabor Comprehensive Specialized Hospital, North Central Ethiopia. Open Access Surgery 2021, 14, 47–54. [Google Scholar] [CrossRef]
- Gao, G.; Wu, X.; Feng, J.; Hui, J.; Mao, Q.; Lecky, F.; Lingsma, H.; Maas, A.I.R.; Jiang, J. Clinical Characteristics and Outcomes in Patients with Traumatic Brain Injury in China: A Prospective, Multicentre, Longitudinal, Observational Study. Lancet Neurol. 2020, 19, 670–677. [Google Scholar] [CrossRef] [PubMed]
- Dewan, M.C.; Rattani, A.; Gupta, S.; Baticulon, R.E.; Hung, Y.-C.; Punchak, M.; Agrawal, A.; Adeleye, A.O.; Shrime, M.G.; Rubiano, A.M.; et al. Estimating the Global Incidence of Traumatic Brain Injury. J. Neurosurg. 2019, 130, 1080–1097. [Google Scholar] [CrossRef] [PubMed]
- Najem, D.; Rennie, K.; Ribecco-Lutkiewicz, M.; Ly, D.; Haukenfrers, J.; Liu, Q.; Nzau, M.; Fraser, D.D.; Bani-Yaghoub, M. Traumatic Brain Injury: Classification, Models, and Markers. Biochem. Cell Biol. 2018, 96, 391–406. [Google Scholar] [CrossRef] [PubMed]
- Al-Shareef, A.S.; Thaqafi, M.A.; Alzahrani, M.; Samman, A.M.; AlShareef, A.; Alzahrani, A.; Alzahrani, A.; Rio, A.; Hariri, B.; Ramadan, M. Traumatic Brain Injury Cases’ Mortality Predictors, Association, and Outcomes in the Emergency Department at a Tertiary Healthcare Center in Saudi Arabia. Asian J. Neurosurg. 2022, 17, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Flaada, J.T.; Leibson, C.L.; Mandrekar, J.N.; Diehl, N.; Perkins, P.K.; Brown, A.W.; Malec, J.F. Relative Risk of Mortality after Traumatic Brain Injury: A Population-Based Study of The Role of Age And Injury Severity. J. Neurotrauma 2007, 24, 435–445. [Google Scholar] [CrossRef] [PubMed]
- Saadat, S.; Akbari, H.; Khorramirouz, R.; Mofid, R.; Rahimi-Movaghar, V. Determinants of Mortality in Patients with Traumatic Brain Injury. Ulus. Travma Acil. Cerrahi Derg. 2012, 18, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Daugherty, J.; Waltzman, D.; Sarmiento, K.; Xu, L. Traumatic Brain Injury–Related Deaths by Race/Ethnicity, Sex, Intent, and Mechanism of Injury—United States, 2000–2017. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 1050–1056. [Google Scholar] [CrossRef]
- Okidi, R.; Ogwang, D.M.; Okello, T.R.; Ezati, D.; Kyegombe, W.; Nyeko, D.; Scolding, N.J. Factors Affecting Mortality after Traumatic Brain Injury in a Resource-Poor Setting. BJS Open 2020, 4, 320–325. [Google Scholar] [CrossRef]
- Nortje, J.; Menon, D.K. Traumatic Brain Injury: Physiology, Mechanisms, and Outcome. Curr. Opin. Neurol. 2004, 17, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Yue, J.; Krishnan, N.; Kanter, J.; Deng, H.; Okonkwo, D.; Puccio, A.; Madhok, D.; Belton, P.; Lindquist, B.; Satris, G.; et al. Neuroworsening in the Emergency Department Is a Predictor of Traumatic Brain Injury Intervention and Outcome: A TRACK-TBI Pilot Study. J. Clin. Med. 2023, 12, 2024. [Google Scholar] [CrossRef] [PubMed]
- Noorbakhsh, S.; Keirsey, M.; Hess, A.; Bellu, K.; Laxton, S.; Byerly, S.; Filiberto, D.M.; Kerwin, A.J.; Stein, D.M.; Howley, I.W. Key Findings on Computed Tomography of the Head That Predict Death or the Need for Neurosurgical Intervention From Traumatic Brain Injury. Am. Surg. 2024, 90, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Tunthanathip, T.; Phuenpathom, N.; Jongjit, A. Prognostic Factors and Clinical Nomogram for In-Hospital Mortality in Traumatic Brain Injury. Am. J. Emerg. Med. 2024, 77, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Fazel, S.; Wolf, A.; Pillas, D.; Lichtenstein, P.; Långström, N. Suicide, Fatal Injuries, and Other Causes of Premature Mortality in Patients With Traumatic Brain Injury: A 41-Year Swedish Population Study. JAMA Psychiatry 2014, 71, 326. [Google Scholar] [CrossRef]
- Troeung, L.; Mann, G.; Martini, A. Patterns and Predictors of Ten-Year Mortality after Discharge from Community-Based Post-Acute Care for Acquired Brain Injury: A Retrospective Cohort Study (ABI-RESTaRT), Western Australia, 1991–2017. Disabil. Health J. 2024, 101591. [Google Scholar] [CrossRef]
- Peterson, A.B.; Zhou, H.; Thomas, K.E. Disparities in Traumatic Brain Injury-Related Deaths—United States, 2020. J. Saf. Res. 2022, 83, 419–426. [Google Scholar] [CrossRef]
- Sussman, E.S.; Pendharkar, A.V.; Ho, A.L.; Ghajar, J. Mild Traumatic Brain Injury and Concussion: Terminology and Classification. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2018; Volume 158, pp. 21–24. [Google Scholar] [CrossRef]
- McCrea, M.A.; Giacino, J.T.; Barber, J.; Temkin, N.R.; Nelson, L.D.; Levin, H.S.; Dikmen, S.; Stein, M.; Bodien, Y.G.; Boase, K.; et al. Functional Outcomes Over the First Year After Moderate to Severe Traumatic Brain Injury in the Prospective, Longitudinal TRACK-TBI Study. JAMA Neurol. 2021, 78, 982. [Google Scholar] [CrossRef]
- Cheng, P.-L.; Lin, H.-Y.; Lee, Y.-K.; Hsu, C.-Y.; Lee, C.-C.; Su, Y.-C. Higher Mortality Rates among the Elderly with Mild Traumatic Brain Injury: A Nationwide Cohort Study. Scand. J. Trauma Resusc. Emerg. Med. 2014, 22, 7. [Google Scholar] [CrossRef] [PubMed]
- Saatman, K.E.; Duhaime, A.-C.; Bullock, R.; Maas, A.I.R.; Valadka, A.; Manley, G.T. Classification of Traumatic Brain Injury for Targeted Therapies. J. Neurotrauma 2008, 25, 719–738. [Google Scholar] [CrossRef]
- Hawryluk, G.W.J.; Manley, G.T. Classification of Traumatic Brain Injury. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2015; Volume 127, pp. 15–21. [Google Scholar] [CrossRef]
- Aryan, H.E.; Jandial, R.; Bennett, R.L.; Masri, L.S.; Lavine, S.D.; Levy, M.L. Gunshot Wounds to the Head: Gang- and Non-Gang-Related Injuries and Outcomes. Brain Inj. 2005, 19, 505–510. [Google Scholar] [CrossRef]
- Mckee, A.C.; Daneshvar, D.H. The Neuropathology of Traumatic Brain Injury. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2015; Volume 127, pp. 45–66. [Google Scholar] [CrossRef]
- Demlie, T.A.; Alemu, M.T.; Messelu, M.A.; Wagnew, F.; Mekonen, E.G. Incidence and Predictors of Mortality among Traumatic Brain Injury Patients Admitted to Amhara Region Comprehensive Specialized Hospitals, Northwest Ethiopia, 2022. BMC Emerg. Med. 2023, 23, 55. [Google Scholar] [CrossRef]
- Tenovuo, O.; Diaz-Arrastia, R.; Goldstein, L.E.; Sharp, D.J.; Van Der Naalt, J.; Zasler, N.D. Assessing the Severity of Traumatic Brain Injury—Time for a Change? J. Clin. Med. 2021, 10, 148. [Google Scholar] [CrossRef] [PubMed]
- Levin, H.S.; O’donnell, V.M.; Grossman, R.G. The Galveston Orientation and Amnesia Test: A Practical Scale to Assess Cognition after Head Injury. J. Nerv. Ment. Dis. 1979, 167, 675–684. [Google Scholar] [CrossRef]
- Meares, S.; Shores, E.A.; Taylor, A.J.; Lammél, A.; Batchelor, J. Validation of the Abbreviated Westmead Post-Traumatic Amnesia Scale: A Brief Measure to Identify Acute Cognitive Impairment in Mild Traumatic Brain Injury. Brain Inj. 2011, 25, 1198–1205. [Google Scholar] [CrossRef]
- Mehta, V.; Harward, S.C.; Sankey, E.W.; Nayar, G.; Codd, P.J. Evidence Based Diagnosis and Management of Chronic Subdural Hematoma: A Review of the Literature. J. Clin. Neurosci. 2018, 50, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Baalen, B.V.; Odding, E.; Maas, A.I.R.; Ribbers, G.M.; Bergen, M.P.; Stam, H.J. Traumatic Brain Injury: Classification of Initial Severity and Determination of Functional Outcome. Disabil. Rehabil. 2003, 25, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Murray, G.D.; Teasdale, G.M.; Braakman, R.; Cohadon, F.; Dearden, M.; Iannotti, F.; Karimi, A.; Lapierre, F.; Maas, A.; Ohman, J.; et al. The European Brain Injury Consortium Survey of Head Injuries. Acta Neurochir. 1999, 141, 223–236. [Google Scholar] [CrossRef]
- Foreman, B.P.; Caesar, R.R.; Parks, J.; Madden, C.; Gentilello, L.M.; Shafi, S.; Carlile, M.C.; Harper, C.R.; Diaz-Arrastia, R.R. Usefulness of the Abbreviated Injury Score and the Injury Severity Score in Comparison to the Glasgow Coma Scale in Predicting Outcome After Traumatic Brain Injury. J. Trauma Inj. Infect. Crit. Care 2007, 62, 946–950. [Google Scholar] [CrossRef]
- Perrin, P.B.; Niemeier, J.P.; Mougeot, J.-L.; Vannoy, C.H.; Hirsch, M.A.; Watts, J.A.; Rossman, W.; Grafton, L.M.; Guerrier, T.D.; Pershad, R.; et al. Measures of Injury Severity and Prediction of Acute Traumatic Brain Injury Outcomes. J. Head Trauma Rehabil. 2015, 30, 136–142. [Google Scholar] [CrossRef]
- Königs, M.; De Kieviet, J.F.; Oosterlaan, J. Post-Traumatic Amnesia Predicts Intelligence Impairment Following Traumatic Brain Injury: A Meta-Analysis. J. Neurol. Neurosurg. Psychiatry 2012, 83, 1048–1055. [Google Scholar] [CrossRef] [PubMed]
- Friedland, D.; Swash, M. Post-Traumatic Amnesia and Confusional State: Hazards of Retrospective Assessment. J. Neurol. Neurosurg. Psychiatry 2016, 87, 1068–1074. [Google Scholar] [CrossRef] [PubMed]
- Dikmen, S.; Machamer, J.; Temkin, N. Mild Head Injury: Facts and Artifacts. J. Clin. Exp. Neuropsychol. 2001, 23, 729–738. [Google Scholar] [CrossRef] [PubMed]
- Cota, M.R.; Moses, A.D.; Jikaria, N.R.; Bittner, K.C.; Diaz-Arrastia, R.R.; Latour, L.L.; Turtzo, L.C. Discordance between Documented Criteria and Documented Diagnosis of Traumatic Brain Injury in the Emergency Department. J. Neurotrauma 2019, 36, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Dams-O’Connor, K.; Spielman, L.; Singh, A.; Gordon, W.A.; Lingsma, H.F.; Maas, A.I.R.; Manley, G.T.; Mukherjee, P.; Okonkwo, D.O.; Puccio, A.M.; et al. The Impact of Previous Traumatic Brain Injury on Health and Functioning: A TRACK-TBI Study. J. Neurotrauma 2013, 30, 2014–2020. [Google Scholar] [CrossRef] [PubMed]
- Maas, A.I.R.; Menon, D.K.; Adelson, P.D.; Andelic, N.; Bell, M.J.; Belli, A.; Bragge, P.; Brazinova, A.; Büki, A.; Chesnut, R.M.; et al. Traumatic Brain Injury: Integrated Approaches to Improve Prevention, Clinical Care, and Research. Lancet Neurol. 2017, 16, 987–1048. [Google Scholar] [CrossRef] [PubMed]
- Stein, S.C.; Spettell, C. The Head Injury Severity Scale (HISS): A Practical Classification of Closed-Head Injury. Brain Inj. 1995, 9, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Moskowitz, E.; Melendez, C.I.; Dunn, J.; Khan, A.D.; Gonzalez, R.; Liebscher, S.; Schroeppel, T.J. Long-Term Effects of Decompressive Craniectomy on Functional Outcomes after Traumatic Brain Injury: A Multicenter Study. Am. Surg. 2018, 84, 1314–1318. [Google Scholar] [CrossRef] [PubMed]
- Estraneo, A.; Loreto, V.; Masotta, O.; Pascarella, A.; Trojano, L. Do Medical Complications Impact Long-Term Outcomes in Prolonged Disorders of Consciousness? Arch. Phys. Med. Rehabil. 2018, 99, 2523–2531.e3. [Google Scholar] [CrossRef]
- Skarupa, D.J.; Khan, M.; Hsu, A.; Madbak, F.G.; Ebler, D.J.; Yorkgitis, B.; Rahmathulla, G.; Alcindor, D.; Joseph, B. Trends in Civilian Penetrating Brain Injury: A Review of 26,871 Patients. Am. J. Surg. 2019, 218, 255–260. [Google Scholar] [CrossRef]
- Gritti, P.; Zangari, R.; Carobbio, A.; Zucchi, A.; Lorini, F.L.; Ferri, F.; Agostinis, C.; Lanterna, L.A.; Brembilla, C.; Foresti, C.; et al. Acute and Subacute Outcome Predictors in Moderate and Severe Traumatic Brain Injury: A Retrospective Monocentric Study. World Neurosurg. 2019, 128, e531–e540. [Google Scholar] [CrossRef]
- El-Menyar, A.; Ramzee, A.F.; Asim, M.; Di Somma, S.; Al-Thani, H. Comparative Analysis for the Implication of Serum Cardiac Troponin Measurements by Conventional versus High-Sensitivity Assays in Patients with Traumatic Brain Injury. Minerva Cardioangiol. 2020, 68, 27–33. [Google Scholar] [CrossRef]
- Chico-Fernández, M.; Sánchez-Casado, M.; Barea-Mendoza, J.A.; García-Sáez, I.; Ballesteros-Sanz, M.Á.; Guerrero-López, F.; Quintana-Díaz, M.; Molina-Díaz, I.; Martín-Iglesias, L.; Toboso-Casado, J.M.; et al. Outcomes of Very Elderly Trauma ICU Patients. Results from the Spanish Trauma ICU Registry. Med. Intensiv. 2020, 44, 210–215. [Google Scholar] [CrossRef]
- Asim, M.; El-Menyar, A.; Parchani, A.; Nabir, S.; Ahmed, M.N.; Ahmed, Z.; Ramzee, A.F.; Al-Thani, A.; Al-Abdulmalek, A.; Al-Thani, H. Rotterdam and Marshall Scores for Prediction of In-Hospital Mortality in Patients with Traumatic Brain Injury: An Observational Study. Brain Inj. 2021, 35, 803–811. [Google Scholar] [CrossRef] [PubMed]
- Kashkoush, A.; Petitt, J.C.; Ladhani, H.; Ho, V.P.; Kelly, M.L.; Ghneim, M.; Albrecht, J.S.; Brasel, K.; Livaris, A.; Watras, J.B.; et al. Predictors of Mortality, Withdrawal of Life-Sustaining Measures, and Discharge Disposition in Octogenarians with Subdural Hematomas. World Neurosurg. 2022, 157, e179–e187. [Google Scholar] [CrossRef] [PubMed]
- Estraneo, A.; Magliacano, A.; Fiorenza, S.; Formisano, R.; Grippo, A.; Angelakis, E.; Cassol, H.; Thibaut, A.; Gosseries, O.; Lamberti, G.; et al. Risk Factors for 2-year Mortality in Patients with Prolonged Disorders of Consciousness: An International Multicentre Study. Euro J. Neurol. 2022, 29, 390–399. [Google Scholar] [CrossRef]
- Ghneim, M.; Brasel, K.; Vesselinov, R.; Albrecht, J.; Liveris, A.; Watras, J.; Michetti, C.; Haan, J.; Lightwine, K.; Winfield, R.; et al. Traumatic Brain Injury in Older Adults: Characteristics, Outcomes, and Considerations. Results From the American Association for the Surgery of Trauma Geriatric Traumatic Brain Injury (GERI-TBI) Multicenter Trial. J. Am. Med. Dir. Assoc. 2022, 23, 568–575.e1. [Google Scholar] [CrossRef]
- Réa-Neto, Á.; Bernardelli, R.S.; De Oliveira, M.C.; David-João, P.G.; Kozesinski-Nakatani, A.C.; Falcão, A.L.E.; Kurtz, P.M.P.; Teive, H.A.G.; Neurocritical Brazil Study group; Caltabeloti, F.; et al. Epidemiology and Disease Burden of Patients Requiring Neurocritical Care: A Brazilian Multicentre Cohort Study. Sci. Rep. 2023, 13, 18595. [Google Scholar] [CrossRef] [PubMed]
- Mosenthal, A.C.; Livingston, D.H.; Lavery, R.F.; Knudson, M.M.; Lee, S.; Morabito, D.; Manley, G.T.; Nathens, A.; Jurkovich, G.; Hoyt, D.B.; et al. The Effect of Age on Functional Outcome in Mild Traumatic Brain Injury: 6-Month Report of a Prospective Multicenter Trial. J. Trauma Inj. Infect. Crit. Care 2004, 56, 1042–1048. [Google Scholar] [CrossRef]
- Dell, K.C.; Grossner, E.C.; Staph, J.; Schatz, P.; Hillary, F.G. A Population-Based Study of Pre-Existing Health Conditions in Traumatic Brain Injury. Neurotrauma Rep. 2021, 2, 255–269. [Google Scholar] [CrossRef]
- Chesnut, R.M.; Marshall, L.F.; Klauber, M.R.; Blunt, B.A.; Baldwin, N.; Eisenberg, H.M.; Jane, J.A.; Marmarou, A.; Foulkes, M.A. The role of secondary brain injury in determining outcome from severe head injury. J. Trauma Inj. Infect. Crit. Care 1993, 34, 216–222. [Google Scholar] [CrossRef]
- Prabhakar, H.; Sandhu, K.; Bhagat, H.; Durga, P.; Chawla, R. Current Concepts of Optimal Cerebral Perfusion Pressure in Traumatic Brain Injury. J. Anaesthesiol. Clin. Pharmacol. 2014, 30, 318. [Google Scholar] [CrossRef] [PubMed]
- Harhangi, B.S.; Kompanje, E.J.O.; Leebeek, F.W.G.; Maas, A.I.R. Coagulation Disorders after Traumatic Brain Injury. Acta Neurochir. 2008, 150, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Mendelow, A.; Gregson, B.; Fernandes, H.; Murray, G.; Teasdale, G.; Hope, D.; Karimi, A.; Shaw, M.; Barer, D. Early Surgery versus Initial Conservative Treatment in Patients with Spontaneous Supratentorial Intracerebral Haematomas in the International Surgical Trial in Intracerebral Haemorrhage (STICH): A Randomised Trial. Lancet 2005, 365, 387–397. [Google Scholar] [CrossRef] [PubMed]
- Tsai, Y.-C.; Rau, C.-S.; Huang, J.-F.; Chang, Y.-M.; Chia, K.-J.; Hsieh, T.-M.; Chou, S.-E.; Su, W.-T.; Hsu, S.-Y.; Hsieh, C.-H. The Association between Skull Bone Fractures and the Mortality Outcomes of Patients with Traumatic Brain Injury. Emerg. Med. Int. 2022, 2022, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Rauchman, S.H.; Zubair, A.; Jacob, B.; Rauchman, D.; Pinkhasov, A.; Placantonakis, D.G.; Reiss, A.B. Traumatic Brain Injury: Mechanisms, Manifestations, and Visual Sequelae. Front. Neurosci. 2023, 17, 1090672. [Google Scholar] [CrossRef] [PubMed]
- Xiong, C.; Hanafy, S.; Chan, V.; Hu, Z.J.; Sutton, M.; Escobar, M.; Colantonio, A.; Mollayeva, T. Comorbidity in Adults with Traumatic Brain Injury and All-Cause Mortality: A Systematic Review. BMJ Open 2019, 9, e029072. [Google Scholar] [CrossRef] [PubMed]
- Zygun, D.A.; Kortbeek, J.B.; Fick, G.H.; Laupland, K.B.; Doig, C.J. Non-Neurologic Organ Dysfunction in Severe Traumatic Brain Injury. Crit. Care Med. 2005, 33, 654–660. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Ande, S.R.; Batoo, D.; Linton, J.; Shankar, J. Prognostic Value of Initial Diagnostic Imaging Findings for Patient Outcomes in Adult Patients with Traumatic Brain Injury: A Systematic Review and Meta-Analysis. Tomography 2023, 9, 509–528. [Google Scholar] [CrossRef]
- Yue, J.K.; Yuh, E.L.; Korley, F.K.; Winkler, E.A.; Sun, X.; Puffer, R.C.; Deng, H.; Choy, W.; Chandra, A.; Taylor, S.R.; et al. Association between Plasma GFAP Concentrations and MRI Abnormalities in Patients with CT-Negative Traumatic Brain Injury in the TRACK-TBI Cohort: A Prospective Multicentre Study. Lancet Neurol. 2019, 18, 953–961. [Google Scholar] [CrossRef]
- Helmrich, I.R.A.R.; Czeiter, E.; Amrein, K.; Büki, A.; Lingsma, H.F.; Menon, D.K.; Mondello, S.; Steyerberg, E.W.; Von Steinbüchel, N.; Wang, K.K.W.; et al. Incremental Prognostic Value of Acute Serum Biomarkers for Functional Outcome after Traumatic Brain Injury (CENTER-TBI): An Observational Cohort Study. Lancet Neurol. 2022, 21, 792–802. [Google Scholar] [CrossRef]
- Kulbe, J.R.; Geddes, J.W. Current Status of Fluid Biomarkers in Mild Traumatic Brain Injury. Exp. Neurol. 2016, 275, 334–352. [Google Scholar] [CrossRef] [PubMed]
- Dadas, A.; Washington, J.; Diaz-Arrastia, R.; Janigro, D. Biomarkers in Traumatic Brain Injury (TBI): A Review. Neuropsychiatr. Dis. Treat. 2018, 14, 2989–3000. [Google Scholar] [CrossRef]
- Gill, J.; Mustapic, M.; Diaz-Arrastia, R.; Lange, R.; Gulyani, S.; Diehl, T.; Motamedi, V.; Osier, N.; Stern, R.A.; Kapogiannis, D. Higher Exosomal Tau, Amyloid-Beta 42 and IL-10 Are Associated with Mild TBIs and Chronic Symptoms in Military Personnel. Brain Inj. 2018, 32, 1359–1366. [Google Scholar] [CrossRef] [PubMed]
- Zetterberg, H.; Smith, D.H.; Blennow, K. Biomarkers of Mild Traumatic Brain Injury in Cerebrospinal Fluid and Blood. Nat. Rev. Neurol. 2013, 9, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Blyth, B.J.; Farhavar, A.; Gee, C.; Hawthorn, B.; He, H.; Nayak, A.; Stöcklein, V.; Bazarian, J.J. Validation of Serum Markers for Blood-Brain Barrier Disruption in Traumatic Brain Injury. J. Neurotrauma 2009, 26, 1497–1507. [Google Scholar] [CrossRef] [PubMed]
- Pelinka, L.E.; Kroepfl, A.; Leixnering, M.; Buchinger, W.; Raabe, A.; Redl, H. GFAP Versus S100B in Serum after Traumatic Brain Injury: Relationship to Brain Damage and Outcome. J. Neurotrauma 2004, 21, 1553–1561. [Google Scholar] [CrossRef] [PubMed]
- Gabay, C.; Kushner, I. Acute-Phase Proteins and Other Systemic Responses to Inflammation. N. Engl. J. Med. 1999, 340, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Hicks, C.; Dhiman, A.; Barrymore, C.; Goswami, T. Traumatic Brain Injury Biomarkers, Simulations and Kinetics. Bioengineering 2022, 9, 612. [Google Scholar] [CrossRef]
- Gill, J.; Latour, L.; Diaz-Arrastia, R.; Motamedi, V.; Turtzo, C.; Shahim, P.; Mondello, S.; DeVoto, C.; Veras, E.; Hanlon, D.; et al. Glial Fibrillary Acidic Protein Elevations Relate to Neuroimaging Abnormalities after Mild TBI. Neurology 2018, 91, e1385–e1389. [Google Scholar] [CrossRef]
- Helmy, A.; Carpenter, K.L.; Menon, D.K.; Pickard, J.D.; Hutchinson, P.J. The Cytokine Response to Human Traumatic Brain Injury: Temporal Profiles and Evidence for Cerebral Parenchymal Production. J. Cereb. Blood Flow Metab. 2011, 31, 658–670. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.B.; Yue, J.K.; Korley, F.; Puccio, A.M.; Yuh, E.L.; Sun, X.; Rabinowitz, M.; Vassar, M.J.; Taylor, S.R.; Winkler, E.A.; et al. High-Sensitivity C-Reactive Protein Is a Prognostic Biomarker of Six-Month Disability after Traumatic Brain Injury: Results from the TRACK-TBI Study. J. Neurotrauma 2021, 38, 918–927. [Google Scholar] [CrossRef] [PubMed]
- Ramezani, F.; Bahrami-Amiri, A.; Babahajian, A.; Shahsavari Nia, K.; Yousefifard, M. Ubiquitin C-Terminal Hydrolase-L1 (UCH-L1) in Prediction of Computed Tomography Findings in Traumatic Brain Injury; a Meta-Analysis. Emergency 2018, 6, e62. [Google Scholar] [PubMed]
- Bishop, P.; Rocca, D.; Henley, J.M. Ubiquitin C-Terminal Hydrolase L1 (UCH-L1): Structure, Distribution and Roles in Brain Function and Dysfunction. Biochem. J. 2016, 473, 2453–2462. [Google Scholar] [CrossRef] [PubMed]
- Kobeissy, F.; Arja, R.D.; Munoz, J.C.; Shear, D.A.; Gilsdorf, J.; Zhu, J.; Yadikar, H.; Haskins, W.; Tyndall, J.A.; Wang, K.K. The Game Changer: UCH-L1 and GFAP-Based Blood Test as the First Marketed in Vitro Diagnostic Test for Mild Traumatic Brain Injury. Expert Rev. Mol. Diagn. 2024, 24, 67–77. [Google Scholar] [CrossRef] [PubMed]
- Mondello, S.; Linnet, A.; Buki, A.; Robicsek, S.; Gabrielli, A.; Tepas, J.; Papa, L.; Brophy, G.M.; Tortella, F.; Hayes, R.L.; et al. Clinical Utility of Serum Levels of Ubiquitin C-Terminal Hydrolase as a Biomarker for Severe Traumatic Brain Injury. Neurosurgery 2012, 70, 666–675. [Google Scholar] [CrossRef] [PubMed]
- Thelin, E.; Al Nimer, F.; Frostell, A.; Zetterberg, H.; Blennow, K.; Nyström, H.; Svensson, M.; Bellander, B.-M.; Piehl, F.; Nelson, D.W. A Serum Protein Biomarker Panel Improves Outcome Prediction in Human Traumatic Brain Injury. J. Neurotrauma 2019, 36, 2850–2862. [Google Scholar] [CrossRef] [PubMed]
- Di Pietro, V.; Ragusa, M.; Davies, D.; Su, Z.; Hazeldine, J.; Lazzarino, G.; Hill, L.J.; Crombie, N.; Foster, M.; Purrello, M.; et al. MicroRNAs as Novel Biomarkers for the Diagnosis and Prognosis of Mild and Severe Traumatic Brain Injury. J. Neurotrauma 2017, 34, 1948–1956. [Google Scholar] [CrossRef]
- CDC. Available online: https://www.cdc.gov/traumaticbraininjury/data/index.html (accessed on 29 February 2024).
- National Center for Health Statistics. Available online: https://www.cdc.gov/nchs/hus/index.htm (accessed on 29 February 2024).
- WHO. Available online: https://www.who.int/violence_injury_prevention/key_facts/VIP_key_fact_1.pdf (accessed on 29 February 2024).
- Hyder, A.A.; Wunderlich, C.A.; Puvanachandra, P.; Gururaj, G.; Kobusingye, O.C. The Impact of Traumatic Brain Injuries: A Global Perspective. NeuroRehabilitation 2007, 22, 341–353. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Paper ID | Year | Study Design | Sample Size | Key Finding |
|---|---|---|---|---|
| Moskowitz, Eliza et al. [41] | 2018 | A retrospective multi-institutional cohort study | 54 | Penetrating injury, young age, and higher GCS at admission were associated with lower mortality rates in patients undergoing decompressive craniotomy after TBI |
| Estraneo, Anna et al. [42] | 2018 | A prospective observational cohort study | 194 | In the long term, respiratory complications including infections were the most common cause of death in patients with moderate TBI |
| Skarupa, David J. et al. [43] | 2019 | A retrospective observational study | 26,871 | The incidence and mortality rates for civilian penetrating brain injury have increased over the last 5 years, with self-inflicted injury and prehospital intubation being the most significant predictors of mortality |
| Gritti, Paolo et al. [44] | 2019 | A retrospective monocentric study | 193 | Increasing age is the main acute risk factor and the Oxford Handicap Scale (OHS) is a potential subacute predictor of mortality moderate TBI patients |
| El-Menyar, Ayman et al. [45] | 2020 | A retrospective study | 654 | Any positive result of serum troponin after TBI is associated with higher mortality risk |
| Chico-Fernández, M. et al. [46] | 2020 | A retrospective study | 465 | The observed mortality rate was lower than predicted in very elderly patients admitted to the ICU based on the severity of injury |
| Gao, Guoyi et al. [3] | 2020 | A prospective, multicenter, longitudinal, observational study | 13,627 | The survival outcomes of individuals with TBI were found to be significantly correlated with age, (GCS) score, injury severity score, pupillary light reflex, (CT) findings (specifically, compressed basal cistern and midline shift ≥ 5 mm), the presence of hypoxia, systemic hypotension, altitude exceeding 500 m, and gross domestic product (GDP) per capita |
| Amare, Abraham Tsedalu et al. [1] | 2021 | A retrospective cohort study | 338 | TBI patients with high Glasgow Coma Scale score, bilateral non-reactive pupils, and elevated blood pressure have a lower survival rate |
| Asim, Mohammad et al. [47] | 2021 | A retrospective study | 1035 | GCS scores were lower in patients with TBI having higher Rotterdam or Marshall CT scores, which were associated with higher mortality rates |
| Kashkoush, Ahmed et al. [48] | 2021 | A prospective study | 695 | Hospital mortality was independently associated with GCS scores less than 13, nonreactivity of pupils, escalating Injury Severity Score (ISS), intraventricular hemorrhage, and the need for neurosurgical intervention in patients aged > 79 years old with TBI having subdural hematoma |
| Estraneo, Anna et al. [49] | 2022 | A prospective study | 143 [traumatic n = 55] | In adult patients with prolonged vegetative state/unresponsive wakefulness syndrome (VS/UWS) or minimally conscious state (MCS) after TBI, mortality rate was higher in VS/UWS than MCS especially with older age and lower CRS-R total score |
| Ghneim, Mira et al. [50] | 2022 | A prospective observational study | 2028 | In TBI patients aged ≥ 65 years old, GCS score < 9 was the main predictor of mortality, and relying solely on chronological age might be inadequate for accurately forecasting the mortality outcomes |
| Réa-Neto, Álvaro et al. [51] | 2023 | A prospective cohort study | 1194 | Advanced age, reduced GCS scores, and higher number of concurrent potential secondary injuries are independent predictors of mortality in TBI patients presenting to the ICU |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eghzawi, A.; Alsabbah, A.; Gharaibeh, S.; Alwan, I.; Gharaibeh, A.; Goyal, A.V. Mortality Predictors for Adult Patients with Mild-to-Moderate Traumatic Brain Injury: A Literature Review. Neurol. Int. 2024, 16, 406-418. https://doi.org/10.3390/neurolint16020030
Eghzawi A, Alsabbah A, Gharaibeh S, Alwan I, Gharaibeh A, Goyal AV. Mortality Predictors for Adult Patients with Mild-to-Moderate Traumatic Brain Injury: A Literature Review. Neurology International. 2024; 16(2):406-418. https://doi.org/10.3390/neurolint16020030
Chicago/Turabian StyleEghzawi, Ansam, Alameen Alsabbah, Shatha Gharaibeh, Iktimal Alwan, Abeer Gharaibeh, and Anita V. Goyal. 2024. "Mortality Predictors for Adult Patients with Mild-to-Moderate Traumatic Brain Injury: A Literature Review" Neurology International 16, no. 2: 406-418. https://doi.org/10.3390/neurolint16020030
APA StyleEghzawi, A., Alsabbah, A., Gharaibeh, S., Alwan, I., Gharaibeh, A., & Goyal, A. V. (2024). Mortality Predictors for Adult Patients with Mild-to-Moderate Traumatic Brain Injury: A Literature Review. Neurology International, 16(2), 406-418. https://doi.org/10.3390/neurolint16020030