Abstract
Aim: The aim of this study was to identify the effectiveness of Family Group Conferencing (FGC), a decision-making model that is not only family-centered but also takes the form of a family-driven or social network, and to consider the challenges to FGC implementation. Methods: A scoping review was conducted using the Arksey and O’Malley framework. A systematic search was conducted of such electronic databases as PsycInfo, CINAHL, Google Scholar, and Web of Science. Criteria were set utilizing the search terms “family group conferencing” or “family group conference”, with the search refined to studies published between January 2015 and July 2020. The data extracted by the review team were inductively analyzed, and the findings were classified into categories. Results: This review included a total of 26 studies. The categories underscoring the effectiveness of FGC included “sense of ownership”, “restoring belongingness”, “reduction of coercion”, and “learning platform”. Categories presenting challenges to FGC implementation included “severe situations of main actor”, “severe situations of the family”, “the complex role of the FGC coordinator”, and “the cost-ineffectiveness of FGC”. Conclusions: The effectiveness in the capacity of decision-makers was determined by the interaction between the main actor and social network of the FGC, with the challenges to FGC reducing the likelihood of completing the FGC process. It will be necessary therefore to identify the skills and qualifications of FGC coordinators, who must take into account group dynamics, so as to enable the main actor and their social network to develop a positive reciprocal interaction.
1. Introduction
Family Group Conferencing (FGC) is a decision-making model that was developed in New Zealand in the 1980s. In 1989, it was incorporated into that country’s Children, Young Persons, and Their Families Act [1] as an effective method for solving problems involving children. FGC is based on the idea that families themselves, rather than professionals, are the experts on their family’s situation and problems, and postulates that most families have sufficient abilities and resources to make competent decisions concerning their own welfare. This differs, therefore, from the general idea of decision-making.
FGC’s principles and values are based on New Zealand Māori culture. In traditional Māori culture, whānau was the place where family members and extended family members would meet, as well as where initial teaching and socialization took place. Nowadays, whānau has come to mean an environment within which certain responsibilities and obligations are taught to the younger generation [2]. According to Barn and Das (2016) [3], while the roots of the FGC model come from Māori cultural traditions, and the concept of family in FGC was broadly defined to include immediate family members and wider kinship systems, little actual discussion or research on FGC focuses on the system’s cultural and ethnic background.
FGC had been presented at local workshops throughout New Zealand, and it was shared and further developed in Great Britain, as well as in Hawaii and in other US states [4]. FGC studies were conducted across Europe, North America, and Oceania, mostly focused on child welfare and restorative justice [5]. De Jong and Schout (2011) [6] note that studies on the application of FGC in mental health practices are uncommon, but from around 2015, the number of studies using FGC in mental health practices began increasing [7,8,9,10,11,12]. Furthermore, the FGC has been widely implemented in numerous other areas, such as homelessness [13], work disability [14], care for older adults with dementia and their families [15], and so on. FGC has also been evaluated using a variety of strategies, such as qualitative interviews, observations of clients and families, social networks, practitioners, and analysis of administrative data and impact analysis of outcome.
The FGC process consists of five phases: (1) preparation phase, (2) information phase, (3) private time phase, (4) presentation of the plan phase, and (5) carrying out the plan and evaluation phase [16,17]. In the preparation phase, the coordinator helps the main actor to explore his/her social network, and the main actor decides who to invite for the conference. In the information phase, the meeting starts, and professionals can provide the information needed to help answer the main actor’s questions. In the private time phase, the main actor and his/her social network deliberate together, but the professionals and the coordinator are not present. In the presentation of the plan phase, the participants present their plan to the coordinator and the professionals involved. Having professionals involved with families at this stage is different from the general method of decision-making. In the final phase, all those involved carry out the plan and evaluate its effectiveness and results, and then they adjust the plan accordingly.
FGC might have numerous participants, including patients, children, their families, members of their social network, professionals (caseworkers, nurses, and so on), and FGC coordinators. In the field of public mental health nursing, the person suffering from or causing the problem(s) in question is referred to as the main actor, and family or people close to them are referred to as their social network. In the field of FGC for older adults, those who are suffering from health or financial problems, such as caring for a spouse who had suffered a stroke, are referred to as cases and their family (siblings, children, and so on) are referred to as their social network. In this study, “main actor(s)” refers to the primary party(s) in FGC, while “social network” refers to their family, relatives, and friends.
The theory underlying FGC is that people have the right to make their own decisions, and that the main actor and their social network bear the primary responsibility for that person’s problems and for finding solutions to these problems [16]. In this way, FGC is not only family-centered but also family-driven (or social network-driven). The key concepts of FGC are resilience and relational autonomy [18], which are central to the FGC process of interaction between the main actor and social network. Resilience is the ability to adapt to difficult or threatening situations, and it includes the ability to adapt and develop through social and environmental interactions [18,19]. Relational autonomy is defined as an approach to autonomy that emphasizes interaction and growth through one’s relationships [20,21].
Regarding the interaction between the main actor and the social network in FGC, the aim of the interaction is to optimize family decision-making, as it is a process with alternating phases of sharing knowledge and skills, coaching, shared decision-making (SDM), and, eventually, of fully empowering the participants [22]. Metze et al. (2015) [16] suggest that the main actor’s interaction during FGC with a social network helps them validate and gain respect for their own decisions and actions, leading to a changed perspective, while building self-respect and self-esteem, and creating a stronger sense of self-worth.
The SDM model, typically seen in the medical field, also emphasizes the interaction of people in a manner similar to FGC. SDM supports patient/family autonomy through informed consent, and through communication among clinicians, patients, and family members. SDM is defined as an approach where clinicians and patients communicate using the best available evidence when faced with a task [23]. Decision-making, in this view, is important for people’s own values and identity, as well as for the amount of communication between clinicians and patients it provides. Hence, healthcare providers play a key role when informed consent is involved, promoting patients’ autonomy through relational approaches. Specifically, in clinical nursing practice, FGC provides nurses with an effective framework to foster patient and family engagement; enhance communication among care teams; and support holistic, patient-centered care through empowerment and relational autonomy. Moreover, nurses, who typically work closely with patients and their families, are ideally positioned to facilitate FGC, thereby improving care coordination, adherence to treatment plans, and overall health outcomes by leveraging families’ inherent strengths and social networks.
While interactions between people in decision-making support are important, the effects on the lives of patients and their families through those decisions have not been adequately examined. FGC resulted in improvements in the quality of social support, resilience, and living conditions [7]. However, a meta-analysis examining the effectiveness of FGC in youth care indicated FGC to be no more effective than regular care [24]. The mechanisms of FGC are complex and difficult to quantify. Arguments have been raised that randomized trials are not the most appropriate research methods to examine the efficacy of FGC, and that it would be more effective to employ a variety of both qualitative and quantitative research methods to analyze the FGC process [25,26]. It is also believed that, in order to identify the effectiveness of FGC and the challenges to its implementation, it is important to consider the process from multiple perspectives, using qualitative and quantitative research, and that scoping reviews are useful for summarizing research findings and identifying multiple research gaps. As research into FGC progresses, new methods of family decision-making may be developed.
The purpose of this study was to identify the efficacy of FGC and the challenges it faces regarding its implementation by addressing two questions: (1) In what ways has FGC shown to have been effective? (2) What are the key challenges that FGC faces?
2. Methods
2.1. Study Design
Scoping reviews are useful for summarizing research findings and identifying research gaps [27]. Because the purpose of this study was to identify the areas in which FGC is effective and examine the challenges faced in implementing FGC, a scoping review was employed.
A scoping review was conducted using the method steps outlined in Arksey and O’Malley (2005) [27] and reported in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis Extension for Scoping Reviews (PRISMA-ScR) [28]. As this is the first systematic review on this topic, the review protocol has not been registered.
2.2. Definition of FGC
FGC is defined as “an intervention in which a plan is not made by a professional, but by the person who needs help and support himself/herself, together with his/her social network” [18].
2.3. Information Sources and Strategies
A systematic search was conducted through the electronic databases in PsycInfo, CINAHL (Cumulative Index to Nursing and Allied Health Literature), Google Scholar, and Web of Science. The search keywords were set to “family group conferencing” or “family group conference”. The range of publication was set from January 2015 to July 2020, the reason being that 2015 marks the point from which FGC began to be widely implemented in numerous fields and in various forms.
2.4. Exclusion Criteria
Publication exclusion criteria were articles not published in English and articles that made no reference to any kind of intervention process, outcome, and effect or problem of FGC. This review did not assess the methodological quality of the included studies.
2.5. Charting the Data
A descriptive–analytical method was used for data extraction from the included studies. The following information was extracted: study characteristics (author, date of publication, country, aims, and study design); participant demographics; study settings; description of the FGC intervention (e.g., coordinator role and length of time for FGC intervention); outcomes and outcome measures; and key findings, including the efficacy and challenges of FGC intervention.
An inductive thematic approach was used for identifying and coding contributing factors. Through this analysis, the areas in which FGC is effective and the challenges faced in implementing FGC were extracted.
Descriptive data from individual studies were collated, and the effectiveness and challenges to FGC were identified for each context. Next, each description was divided into codes, which are small meaning units. Code classification was performed by focusing on similarities and differences, with codes found to be conceptually similar being grouped into more abstract concepts, termed subcategories. The subcategories were then grouped to create categories, and their abstraction levels were refined and checked by the review team. Specifically, the trustworthiness of all analyses underwent independent analysis by two family health nursing researchers and was reviewed until a consensus was reached. If there was no consensus between the two researchers, both researchers re-evaluated the paper. If no consensus was reached between the two researchers, opinions were exchanged repeatedly with 11 collaborating researchers until a final decision was reached.
3. Results
3.1. Study Selection
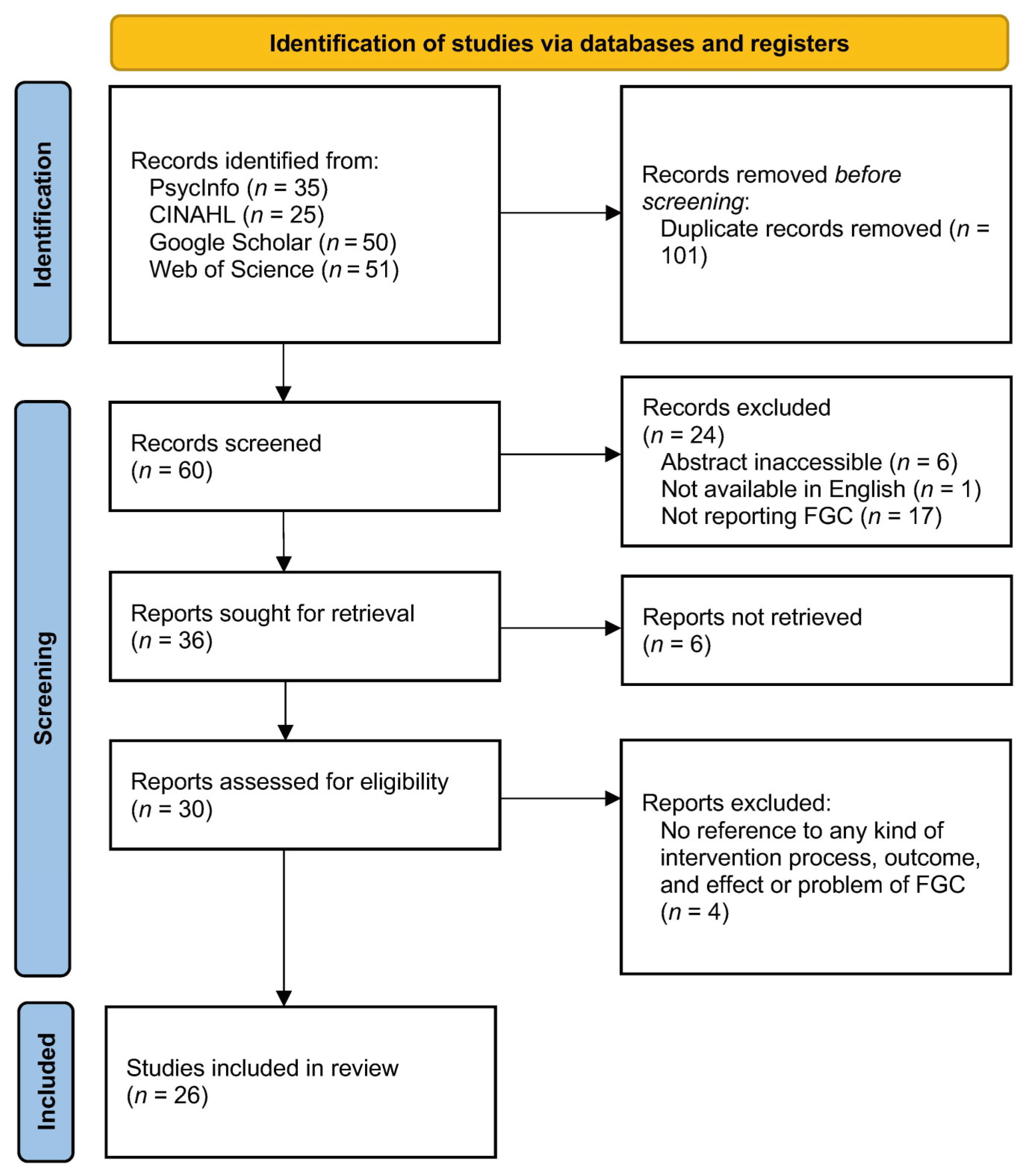
The flow of study identification and selection is shown in Figure 1. The search identified 161 articles: PsycInfo (n = 35); CINAHL (n = 25), Google Scholar (n = 50), and Web of Science (n = 51). After removing 101 duplicate articles, 60 abstracts were screened, and then those papers which were abstract inaccessible (n = 6), not available in English (n = 1), and not reporting FGC (n = 17) were excluded. Thirty full papers were accessed for further evaluation based on the exclusion criteria (no reference to any kind of intervention process, outcome, and effect or problem of FGC), resulting in the final review of 26 full-text articles (43.3% of identified citations).
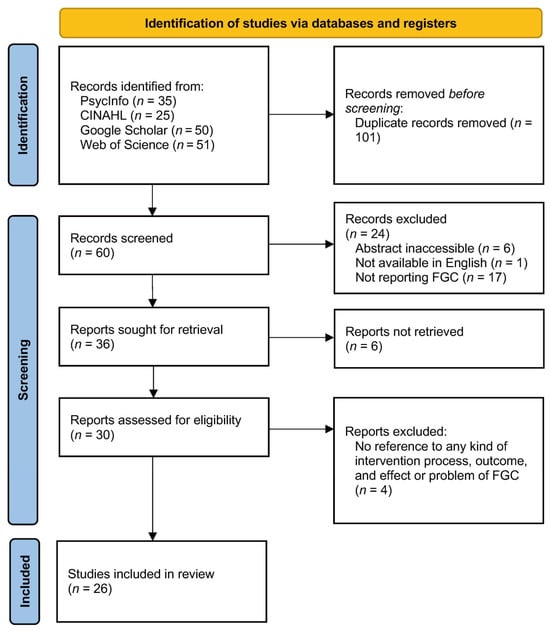
Figure 1.
The flow of study identification and selection.
3.2. Description of Included Studies
Major characteristics of the included studies are shown in Table 1 and Table 2. Studies employed a qualitative design (n = 13), mixed-method design (n = 1), and quantitative design (n = 12). Quantitative studies included quantitative randomized studies (n = 4), meta-analysis study (n = 1), longitudinal quantitative study (n = 1), quantitative non-randomized study (n = 1), and others (n = 5). Studies were conducted across three of the seven continents, with most studies conducted in the Netherlands (n = 14, 53.8%) and the US (n = 4, 15.4%).

Table 1.
Characteristics of included qualitative publications (n = 13).
Table 2.
Characteristics of included quantitative and mixed-method publications (n = 13).
The included studies focused on child welfare (n = 10, 38.5%), mental health care (n = 8, 30.8%), youth justice (n = 2, 7.7%), disability care (n = 2, 7.7%), older adult healthcare (n = 2, 7.7%), homeless care (n = 1, 3.8%), and BME (Black and minority ethnic) immigrant background issues (n = 1, 3.8%).
Participants included the main actor and social network (families and community members), professionals, and coordinators. The qualitative studies comprised the main actor (n = 8, 61.5%), social-network members (n = 8, 61.5%), professionals (n = 10, 76.9%), and coordinators (n = 8, 61.5%). The quantitative and mixed-method studies comprised the patient, family members (n = 9, 69.2%), social-network members (n = 3, 23.1%), professionals (n = 9, 69.2%), and coordinators (n = 4, 30.8%).
3.3. The Effectiveness of FGC
The effectiveness of FGC was extracted across 16 studies. The frequency of identification of each category of effectiveness is summarized in Table 3. The effectiveness of FGC included such categories as “sense of ownership” (n = 14), “restoring belongingness” (n = 10), “reduction of coercion” (n = 4), and “learning platform” (n = 4). One example of each subcategory is also shown in Table 3.
Table 3.
Summary of findings on effectiveness of Family Group Conferencing.
“Sense of ownership” refers to the idea of the main actor and their family making improvements and taking control of their situation through self-reflection during interactions with their social network in the FGC. This category includes the following subcategories: “self-reflection through FGC”, “users taking control of their situation”, and “improvement of users’ situations”.
“Restoring belongingness” refers to the idea of the main actor feeling safe and supported in their social network during the process of self-disclosure in FGC. This category includes the following subcategories: “self-disclosure during FGC process”, “feeling safe and accepted”, and “feeling supported”. “Sense of ownership” focuses on the initiative of the main actor and family to proactively reflect on their own situation and seek to improve it, while “restoring belongingness” refers to the emotional aspect of feeling a sense of security, acceptance, and support within a social network through self-disclosure in FGC, and restoring a sense of belonging.
“Reduction of coercion” refers to the process of the main actor’s self-respect and self-confidence improving through being connected or related to a social network, and also not feeling pressure exerted on them to accept treatment. This category includes the following subcategories: “improvement in self-respect” and “improvement in self-confidence”.
“Learning platform” refers to the partnership between the main actor and their social network, wherein the main actor can learn relational autonomy as a person from working in partnership with their social network. This category includes the following subcategories: “learning relational autonomy” and “learning to work with professionals”.
3.4. The Challenges to FGC Implementation
The challenges to FGC implementation were extracted across 18 studies. The frequency of identification of each category of the problems is summarized in Table 4. The challenges to FGC implementation included such categories as “severe situations of main actor” (n = 4), “severe situations of the family” (n = 6), “the complex role of the FGC coordinator” (n = 9), and “the cost-ineffectiveness of FGC” (n = 11). One example of each subcategory is shown in Table 4.
Table 4.
Summary of findings on challenges to Family Group Conferencing implementation.
“Severe situations of main actor” refers to emergency situations where time is a critical factor, such as when a child requires immediate care, and situations in which the main actor is unable to make decision because of a serious illness. Both of these situations can pose difficulties in organizing and conducting FGC. This category includes the following subcategories: “emergency situations” and “severe problems of the main actor”.
“Severe situations of the family” refers to situations where relationships within family or community are broken or strained, such as poor inter-familial communication or dissolving network relationships. Such situations can reduce the likelihood of completing FGC. This category includes the following subcategories: “broken family” and “broken relationships within the network”.
“The complex role of the FGC coordinator” refers to the difficulties of the role of the FGC coordinator. FGC coordinators have to organize FGC and carry out FGC, and they need to consider the dynamics and unique situations of all of the participants. This category includes the following subcategories: “FGC coordinator complex role” and “difficulties encountered by coordinators”.
“The cost-ineffectiveness of FGC” refers to situations where FGC coordinators with experience or knowledge about the FGC process are insufficient, or where FGC spending is cost inefficient when compared to other models. This category includes the following subcategories: “lack of experience and knowledge of FGC implementation”, and “inefficient spending”.
4. Discussion
FGC differs from general decision-making models in that it places more emphasis on the interaction between participants and the reconstruction of social relationships than it places on the decision itself. While general models focus on the analysis and evaluation of clear options, in FGC, the process in which participants develop self-esteem and a sense of belonging and become independent decision-makers is considered important. Here, the ways in which interaction between the main actor and their social network can impact the implementation of FGC, both positively and negatively, will be discussed.
4.1. The Effectiveness of FGC and the FGC Process
FGC was effective in four aspects, but the literature works on “sense of ownership” and “restoring belongingness” were more numerous, suggesting these two aspects, in particular, may be more effective. The interaction between the main actor and social network in the FGC process appears to be a key factor in the effectiveness of FGC. According to Anderson and Parkinson (2018) [43], the interaction between these two key elements in FGC has a therapeutic effect, because they are able to discuss problems, issues, and difficulties. The relationship is not a one-way process that considers the perspective of the main actor alone but rather a two-way process that includes multiple perspectives from the social network as well, forming a reciprocal interaction [16]. In this way, the interactions between participants in FGC create the conditions for planning meetings [44], which enable the participants to solve their problems mutually, thereby forming the therapeutic foundation.
The interaction in FGC can improve the ability of participants to understand their situation, build relationships, and collaborate with others to change and improve their situation over time. Four categories of effects of FGC cannot be produced in isolation, but rather must be created through interpersonal social interaction. Therefore, the interaction of the two key elements does not facilitate decision-making in FGC per se but rather works on the participants to assist them in becoming decision-makers themselves.
4.2. Challenges to the Implementation of FGC and the FGC Process
The challenges facing the implementation of FGC can hinder the prospects for the FGC process to be successfully completed. In the course of research, it came to be understood that challenges to FGC implementation include both those that impede the successful completion of the FGC process itself and those that impede the very possibility of implementing FGC in the first place.
Regarding challenges that hinder the possibility of implementing FGC, De Jong et al. (2015) [31] analyzed the factors that block FGC preparations and the ability to plan FGC and implement it fully, such as sense of shame and sense of pride of the main actor, and a lack of initiative and care paralysis. The authors also noted that if the parties feel shame over their problems, this may lead to the fear that their social network will ascribe blame, ultimately hindering their participation in FGC. They also stated that, in these cases, the FGC preparation phase bogs down. These findings brought to light obstructions that may hinder the implementation of FGC, as well as the establishing of balanced relationships among participants.
On the other hand, according to Mitchell and Ambrose (2007) [45], numerous studies on reciprocal relationships focus on positive reciprocity, namely reciprocity that promotes stability in relationships through considerate, valued, and balanced exchanges. However, negative reciprocity can also affect relationships. For example, when a parent puts undue pressure on a child with depression, the child may react toward the parent with hostility, thus rendering meetings to resolve this problem unsuccessful. In this way, relationships with negative reciprocity can result in negative behavior. Negative reciprocity must be taken into account in the interaction between the main actor and their social network, and activities must also take into account the group dynamics of the participants.
This study focused mainly on the challenges faced during the FGC process. However, the challenges to effective FGC implementation involve not only FGC management that addresses the FGC process but also the time period leading up to the introduction of FGC. It is also necessary to identify the skills and qualifications of the coordinators who must take into account group dynamics, enabling the building of positive reciprocal interaction.
4.3. Strengths and Limitations
The first limitation of this review relates to the very small number of studies that give clear information about the time period of the FGC process and the method by which coordinators were selected. For this reason, the study’s findings may be frustrated by some shortcomings. The second limitation concerns the fact that more than half the authors were based in the Netherlands. However, this review included time-series analysis studies, and the Dutch authors’ studies were conducted in a variety of fields, including child abuse, community mental health, and disability. Therefore, despite the abovementioned limitations, the use of a scoping review method to provide a broad overview of FGC in numerous fields and in various forms, thereby enabling clarification of the effectiveness of FGC and the challenges in implementing FGC, works in this study’s favor. Future research should focus on the duration of FGC implementation and the method of selecting coordinators. In addition, in this study, the literature search was limited to the years 2015 to 2020, but ideally it would be desirable to review the literature from a wider range of search years. Moreover, the number of papers covered in this study was small (26), of which 14 were from the Netherlands. Taking these factors into consideration, the number of papers that can be discussed is limited, and it will be advisable to increase the number of papers referenced in the future.
4.4. Implications for Nursing Practice
It is difficult to implement FGC in all types of family nursing because many cases of decision-making support in the healthcare field require an emergency response. In this respect, it may be difficult to introduce FGC to all areas of nursing, particularly in acute or emergency care. However, it is believed that the effectiveness of the interaction between the main actor and social network, as revealed in this study, which focused on their abilities as decision-makers, can be practically utilized in nursing. Nurses have become involved in communication with healthcare providers, patients, and families in SDM. Inagaki (2020) [46] observed that this was limited to confirming the family’s understanding of information supplied by the healthcare provider and noted that the nursing professionals were hesitant to express their thoughts. In response to this, the following two recommendations are proposed:
Firstly, in FGC, the interaction between the main actor and the social network does not facilitate decision-making per se, but it works on the participants to assist them in becoming decision-makers themselves. Similarly, it is important to examine the effects of communication between healthcare providers, patients, and families in SDM on decision-making abilities, such as relational autonomy, rather than viewing it as simply a process of understanding information from healthcare providers, making choices, and agreeing. In addition to the participation by patients and their families, participation of those belonging to social networks, such as a friend or member of a kinship group, should also be considered.
Secondly, the coordinator in FGC plays an important role in shaping the interaction between the main actor and social network. In particular, the coordinator must plan and manage the FGC and take into account the dynamics of all participants. Similarly, in SDM, nursing professionals must take into account the dynamics of the participants and play the role of coordinator toward positive reciprocal relationships.
5. Conclusions
The effectiveness of FGC is exhibited by “sense of ownership”, “restoring belongingness”, “reduction of coercion”, and “learning platform”, which are created by the interaction between the main actor and social network, and this interaction impacts on the effectiveness of the capacity of decision-makers. The challenges to FGC implementation are “severe situations of main actor”, “severe situations of the family”, “the complex role of the FGC coordinator”, and “the cost-ineffectiveness of FGC”, all of which hinder the FGC process. However, the challenges to effective FGC implementation involve the FGC process and the time prior to the introduction of FGC, as well as the development of positive interactions between the main actors and their social networks. Because it has become clear that interactions between main actors and social networks are effective in decision-making in FGCs, we recommend that, after understanding the characteristics of FGCs, FGCs be utilized in clinical nursing to support decision-making for various families.
Author Contributions
N.H., conceptualization, methodology, investigation, formal analysis, drafting the work, final approval of the version to be publish, funding acquisition, and project administration; Q.Y., methodology, investigation, and drafting the work. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported in part by a Grant-in-Aid for Scientific Research (B) from the Japan Society for the Promotion of Science (JSPS) in Japan (Grant Number: JP22H03400).
Institutional Review Board Statement
Not required.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author.
Public Involvement Statement
There was no public involvement in any aspect of this research.
Guidelines and Standards Statement
This manuscript was drafted against the PRISMA extension for Scoping Reviews (https://www.equator-network.org/reporting-guidelines/prisma-scr/ accessed on 18 September 2024).
Use of Artificial Intelligence
AI or AI-assisted tools were not used in drafting any aspect of this manuscript.
Acknowledgments
We would like to thank Yasuko Irie for her assistance in data collection and analysis. Our laboratory members’ discussions in the data analysis were effective in ensuring its trustworthiness.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- New Zealand Government. Children, Young Persons, and Their Families Act. 1989. Available online: https://www.legislation.govt.nz/act/public/1989/0024/65.0/DLM147088.html (accessed on 18 September 2024).
- Moeke-Pickering, T.M. Maori Identity Within Whanau: A Review of Literature. [Working Paper]. 1996. Available online: https://hdl.handle.net/10289/464 (accessed on 18 September 2024).
- Barn, R.; Das, C. Family group conferences and cultural competence in social work. Br. J. Soc. Work 2016, 46, 942–959. [Google Scholar] [CrossRef] [PubMed]
- Smith, D. The Family Group Conference Aotearoa/New Zealand: Reflections and Where We Are Thirty Years on; Independently Published: Paekakariki, New Zealand, 2019. [Google Scholar]
- Sen, R.; Webb, C. Exploring the declining rates of state social work intervention in an English local authority using family group conferences. Child. Youth Serv. Rev. 2019, 106, 1–8. [Google Scholar] [CrossRef]
- De Jong, G.; Schout, G. Family group conferences in public mental health care: An exploration of opportunities. Int. J. Ment. Health Nurs. 2011, 20, 63–74. [Google Scholar] [CrossRef] [PubMed]
- De Jong, G.; Schout, G.; Meijer, E.; Mulder, C.L.; Abma, T. Enabling social support and resilience: Outcomes of family group conferencing in public mental health care. Eur. J. Soc. Work 2016, 19, 731–748. [Google Scholar] [CrossRef]
- Schout, G.; De Jong, G. Collecting feedback as a tool to reduce care paralysis: Something for family group conferencing coordinators? Child Fam. Soc. Work 2017, 22, 1197–1206. [Google Scholar] [CrossRef]
- Schout, G.; Van Dijk, M.; Meijer, E.; Landeweer, E.; De Jong, G. The use of family group conferences in mental health: Barriers for implementation. J. Soc. Work 2017, 17, 52–70. [Google Scholar] [CrossRef]
- De Jong, G.; Schout, G.; Abma, T. Understanding the process of family group conferencing in public mental health care: A multiple case study. Br. J. Soc. Work 2018, 48, 353–370. [Google Scholar] [CrossRef]
- Meijer, E.; Schout, G.; De Jong, G.; Abma, T. Regaining ownership and restoring belongingness: Impact of family group conferences in coercive psychiatry. J. Adv. Nurs. 2017, 73, 1862–1872. [Google Scholar] [CrossRef]
- Johansen, S. Therapeutic features of the family group conference model when applied for long-term social assistance recipients. J. Fam. Soc. Work 2020, 23, 277–292. [Google Scholar] [CrossRef]
- Miklosko, J.; Bezakova, E.; Herak, J. Family group conference and its role in addressing homelessness worldwide. Clin. Soc. Work Health Interv. 2017, 8, 30–38. [Google Scholar] [CrossRef]
- Brongers, K.A.; Cornelius, B.; Roelofs, P.D.D.M.; Van Der Klink, J.J.L.; Brouwer, S. Feasibility of family group conference to promote return-to-work of persons receiving work disability benefit. Disabil Rehabil. 2020, 42, 3227–3236. [Google Scholar] [CrossRef] [PubMed]
- Górska, S.; Forsyth, K.; Prior, S.; Irvine, L.; Haughey, P. Family group conferencing in dementia care: An exploration of opportunities and challenges. Int. Psychogeriatr. 2016, 28, 233–246. [Google Scholar] [CrossRef] [PubMed]
- Metze, R.N.; Kwekkeboom, R.H.; Abma, T.A. The potential of family group conferencing for the resilience and relational autonomy of older adults. J. Aging Stud. 2015, 34, 68–81. [Google Scholar] [CrossRef] [PubMed]
- Sundell, K.; Vinnerljung, B.; Ryburn, M. Social workers’ attitudes towards family group conferences in Sweden and the UK. Child Fam. Soc. Work 2001, 6, 327–336. [Google Scholar] [CrossRef]
- Metze, R.N.; Abma, T.A.; Kwekkeboom, R.H. Family group conferencing: A theoretical underpinning. Health Care Anal. 2015, 23, 165–180. [Google Scholar] [CrossRef]
- Egeland, B.; Carlson, E.; Sroufe, L.A. Resilience as process. Dev. Psychopathol. 1993, 5, 517–528. [Google Scholar] [CrossRef]
- Schipper, K.; Widdershoven, G.A.M.; Abma, T.A. Citizenship and autonomy in acquired brain injury. Nurs. Ethics 2011, 18, 526–536. [Google Scholar] [CrossRef]
- Jennings, B. Reconceptualizing autonomy: A relational turn in bioethics. Hastings Cent. Rep. 2016, 46, 11–16. [Google Scholar] [CrossRef]
- Hillebregt, C.F.; Cholten, E.W.M.; Ketelaar, M.; Post, M.W.M.; Visser-Meily, J.M.A. Effects of family group conferences among high-risk patients of chronic disability and their significant others: Study protocol for a multicentre controlled trial. BMJ Open. 2018, 8, e018883. [Google Scholar] [CrossRef]
- Scholl, I.; Koelewijn-van Loon, M.; Sepucha, K.; Elwyn, G.; Légaré, F.; Härter, M.; Dirmaier, J. Measurement of shared decision making: A review of instruments. Zeitschrift für Evidenz Fortbildung und Qualität im Gesundheitswesen 2011, 105, 313–324. [Google Scholar] [CrossRef]
- Dijkstra, S.; Creemers, H.E.; Asscher, J.J.; Dekovic, M.; Stams, G.J.J.M. The effectiveness of family group conferencing in youth care: A meta-analysis. Child Abus. Negl. 2016, 62, 100–110. [Google Scholar] [CrossRef]
- Creemers, H.E.; Sundell, K.; Dekovic, M.; Dijkstra, S.; Stams, G.J.J.M.; Asscher, J.J. When the ‘golden’ standard should be the general standard: Response to a commentary on the use of randomised controlled trials to examine the effectiveness of family group conferencing. Br. J. Soc. Work 2017, 47, 1262–1267. [Google Scholar] [CrossRef]
- De Jong, G.; Schout, G.; Abma, T. Examining the effects of family group conferencing with randomised controlled trials: The golden standard? Br. J. Soc. Work 2015, 45, 1623–1629. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. Prisma extension for scoping reviews (Prisma-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Mitchell, M. Reimagining child welfare outcomes: Learning from family group conferencing. Child Fam. Soc. Work 2020, 25, 211–220. [Google Scholar] [CrossRef]
- Schmid, J.; Morgenshtern, M. Successful, sustainable? Facilitating the growth of family group conferencing in Canada. J. Fam. Soc. Work 2017, 20, 322–339. [Google Scholar] [CrossRef]
- De Jong, G.; Schout, G.; Pennell, J.; Abma, T. Family Group Conferencing in public mental health and social capital theory. J. Soc. Work 2015, 15, 277–296. [Google Scholar] [CrossRef]
- Meijer, E.; Schout, G.; Abma, T. Family group conferencing in coercive psychiatry: On forming partnership between the client, social networks and professionals. Issues Ment. Health Nurs. 2019, 40, 459–465. [Google Scholar] [CrossRef]
- Slater, C.; Lambie, I.; McDowell, H. Youth justice co-ordinators’ perspectives on New Zealand’s youth justice family group conference process. J. Soc. Work 2015, 15, 621–643. [Google Scholar] [CrossRef]
- Valenti, K. Family group conferencing with BME families in Scotland. Pract Soc. Work Action 2017, 29, 121–136. [Google Scholar] [CrossRef]
- Corwin, T.W.; Maher, E.J.; Merkel-Holguin, L.; Allan, H.; Hollinshead, D.M.; Fluke, J.D. Increasing social support for child welfare-involved families through family group conferencing. Br. J. Soc. Work 2020, 50, 137–156. [Google Scholar] [CrossRef]
- Dijkstra, S.; Creemers, H.E.; Asscher, J.J.; Dekovic, M.; Stams, G.J.J.M. Family group conferencing in Dutch child welfare: Which families are most likely to organize a family group conference? Child. Youth Serv. Rev. 2017, 83, 255–263. [Google Scholar] [CrossRef]
- Dijkstra, S.; Creemers, H.E.; Van Steensel, F.J.A.; Dekovic, M.; Stams, G.J.J.M.; Asscher, J.J. Cost-effectiveness of family group conferencing in child welfare: A controlled study. BMC Public Health 2018, 18, 848. [Google Scholar] [CrossRef]
- Dijkstra, S.; Asscher, J.J.; Deković, M.; Stams, G.J.J.M.; Creemers, H.E. A randomised controlled trial on the effectiveness of family group conferencing in child welfare: Effectiveness, moderators, and level of FGC completion. Child Maltreat. 2019, 24, 137–151. [Google Scholar] [CrossRef]
- Hollinshead, D.M.; Corwin, T.W.; Maher, E.J.; Merkel-Holguin, L.; Allan, H.; Fluke, J.D. Effectiveness of family group conferencing in preventing repeat referrals to child protective services and out-of-home placements. Child Abus. Negl. 2017, 69, 285–294. [Google Scholar] [CrossRef]
- Merkel-Holguin, L.; Schwab-Reese, L.; Drury, I.; Allan, H. Nothing about me without me: Children and young people’s experiences with family group conferences. Child Fam. Soc. Work 2020, 25, 27–36. [Google Scholar] [CrossRef]
- Onrust, S.A.; Romijn, G.; De Beer, Y. Family group conferences within the integrated care system for young people with ID: A controlled study of effects and costs. BMC Health Serv. Res. 2015, 15, 392. [Google Scholar] [CrossRef]
- Hipple, N.K.; Gruenewald, J.; McGarrell, E.F. Restorativeness, procedural justice, and defiance as long-term predictors of reoffending of participants in family group conferences. Crim. Justice Behav. 2015, 42, 1110–1127. [Google Scholar] [CrossRef]
- Anderson, M.; Parkinson, K. Balancing justice and welfare needs in family group conferences for children with harmful sexual behavior: The HSB-FGC framework. J. Child Sex Abus. 2018, 27, 490–509. [Google Scholar] [CrossRef]
- Holland, S.; Rivett, M. Everyone started shouting: Making connections between the process of family group conferences and family therapy practice. Br. J. Soc. Work 2008, 38, 21–38. [Google Scholar] [CrossRef]
- Mitchell, M.S.; Ambrose, M.L. Abusive supervision and workplace deviance and the moderating effects of negative reciprocity beliefs. J. Appl. Psychol. 2007, 92, 1159–1168. [Google Scholar] [CrossRef] [PubMed]
- Inagaki, N. Nurse participation in the shared decision-making process for patients with advanced heart failure: Perceptions of the certified nurse specialists in critical care nursing. J. Jpn. Acad. Nurs. Sci. 2020, 40, 544–552. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).