Abstract
The aim was to examine mental health and burnout among frontline and critical care healthcare workers caring for COVID-19 patients. A cohort study was conducted among frontline and critical care healthcare workers in hospitals with COVID-19 patients. Burnout of healthcare workers was high, and mental health was median. Differences in emotional exhaustion, personal accomplishment, depersonalization, satisfaction, and mental health were found during the COVID-19 pandemic. A positive correlation between emotional exhaustion with a higher number of patients, higher workload, higher concern for health, and workplace stress was established. At the end of the third wave, the number of healthcare workers with high emotional exhaustion and depersonalization had decreased by one-third. When emotional exhaustion and occupational stress levels are high, psychologically supporting healthcare workers is essential to preserving their health and well-being.
1. Introduction
1.1. Pandemic Contextualization and Study Population
The Coronavirus SAR-CoV-2 2019 (COVID-19) pandemic was a significant global public health emergency [1]. COVID-19 spread rapidly across all continents [2]. According to statistics published by the World Health Organization [1], globally, as of 2 August 2021, there had been more than 198,234,951 confirmed cases of COVID-19 and more than 4,227,359 deaths. COVID-19 is transmitted primarily by respiratory droplets and close contact, and healthcare workers are at high risk of exposure [3,4].
Well-being is a major global concern that has become even more important in the context of the COVID-19 outbreak. In the population, the impact of economic uncertainty, also due to the epidemic and consequent financial crisis, affected the mental health of individuals. As the unemployment rate increased exponentially, individuals faced greater health problems as a result. Not all members of society have been affected to the same extent, and access to public health services has also been limited. The well-known phenomenon of intolerance of uncertainty in healthcare came to the fore [5]. The pandemic did not only affect health, it also had a major impact on small and medium-sized enterprises in the economy, which required many adjustments [6]. Employees entering the labour market for the first time had different induction conditions [7]. During the epidemic, general uncertainty resulted from the state of the economy, social relations, and health concerns. Isolation and social distancing drastically affected mental health and increased the number of mental disorders and suicidal thoughts [5]. The prevalence of anxiety and depression in the affected group have been higher than in the unaffected group [8,9], with an especially negative effect found in the mental health of frontline healthcare workers [10,11]. Maslach and Leiter [12] defined burnout as a psychological syndrome caused by a prolonged response to interpersonal stressors, mainly in the workplace. The construct of burnout includes three main dimensions: emotional exhaustion, depersonalization, and reduced personal accomplishment [13,14,15,16]. This multidimensional burnout model highlights the importance of individual stress experience within a social context and involves the conception of oneself and others [17]. Some earlier research on the possible health implications of burnout has focused on its negative impact on mental health [18,19,20]. The daily working hours among the frontline medical staff were associated with all psychological disturbances [21]. Landscape has been found to positively affect activating the restoration of psychological mediators [22], which was limited in many countries during the COVID-19 epidemic.
The care itself, with new ways of working, is potentially highly stressful for employees in nursing. When the COVID-19 pandemic occurred, nursing employees on the front line were in exceptional circumstances of healthcare and social care [14].
1.2. Identifying the Research Question
The outbreak of COVID-19 put national and global healthcare systems to the test, which can compromise critical care and frontline healthcare professionals’ well-being when overwhelmed. With many infections and deaths, COVID-19 can lead to many psychological problems, such as stress, anxiety, depression, concern, and burnout [23]. It is vital to understand the factors associated with individuals’ experiences of stress and burnout during the COVID-19 pandemic to prevent psychological problems in the future. Frontline nurses faced great challenges during the pandemic outbreak [24]. The highest rates of burnout (over 40%) were in frontline healthcare providers, in critical care, emergency medicine, and primary care [25]. Bradley and Chahar [26] noted that the COVID-19 pandemic has presented multiple stressors to employees in nursing, including social isolation, risk of infection, and economic consequences. A study of more than 9000 critical care employees indicated that median self-reported stress had increased during the pandemic. Major stressors included fear of COVID-19, fear of spreading the infection to family members, and lack of personal protective equipment [27]. The work-related stressors have been associated with depression and anxiety and reflect genuine physical and emotional risks for healthcare workers [28], especially those on the front line [11]. Simultaneously, many healthcare professionals were experiencing increased demands at home, as the closing of schools and day-care centres has made finding childcare a significant challenge [29].
In recent years, increasing workloads and work-life imbalances have led to mental distress and a high level of burnout among healthcare workers [30], which reached an extremely high level during the pandemic [31]. Frontline healthcare workers working with COVID-19-positive patients have had a moderate association with occupational burnout symptoms, increased likelihood of mental distress, increased risk of sleep problems [32,33,34], and emotional exhaustion [11]. And those working in isolation wards have felt fear of infecting family [35], experienced problematic alcohol use [36], and had higher levels of anxiety and depression than the general population [37,38]. The possibility of burnout increased with longer working hours, and the psychological distress deepened with the increased number of deaths of patients related to COVID [39]. Anxiety and stress were associated with several changes in the everyday lives of healthcare workers (long working hours, isolation after the work shift, and separation from family life) [10]. Anxiety and burnout are also associated with the hours employees work with COVID-19-positive patients [40]. The highest burnout rates were in intensive care and infectious disease units [41,42], increasing the risk of nurses leaving intensive care or the profession [43]. Burnout had the most significant effect on physical health [44]. Of the respondents, 31.1% identified themselves as having symptoms of moderate to severe depression and 44.6% of them had symptoms of anxiety [45]. The results of research in a Slovenian hospital during the restrictions due to COVID-19 showed that, according to the assessment of nursing employees, most employees rate the quality of work and life at a moderate level [46]. An important piece of information for management is that the likelihood of burnout was 40% lower for those who felt they were more valued at work [47]. During the COVID-19 epidemic, healthcare professionals also faced additional teamwork challenges. In order to control the epidemic, for emergency assistance ability and due to the need for intensive therapy units, hospitals in Slovenia rearranged rooms, and reassigned patients, nursing staff, and other medical personnel. Most of the redeployed employees lacked the experience to work in units under special conditions (isolation). Also, the consequences of the transfers were that employees had not worked together in the past, and after the epidemic were not likely to cooperate with each other, i.e., there were problems in teamwork, which was also noted in the research [48]. Considering the number of patients, adequate information, teamwork, and working positions can explain work-life quality differences, and they have effects on the well-being at the workplace and work satisfaction of employees in nursing [41].
This study examined mental health and burnout among frontline and critical care healthcare workers caring for COVID-19 patients in hospitals in Slovenia.
2. Materials and Methods
2.1. Setting and Participants
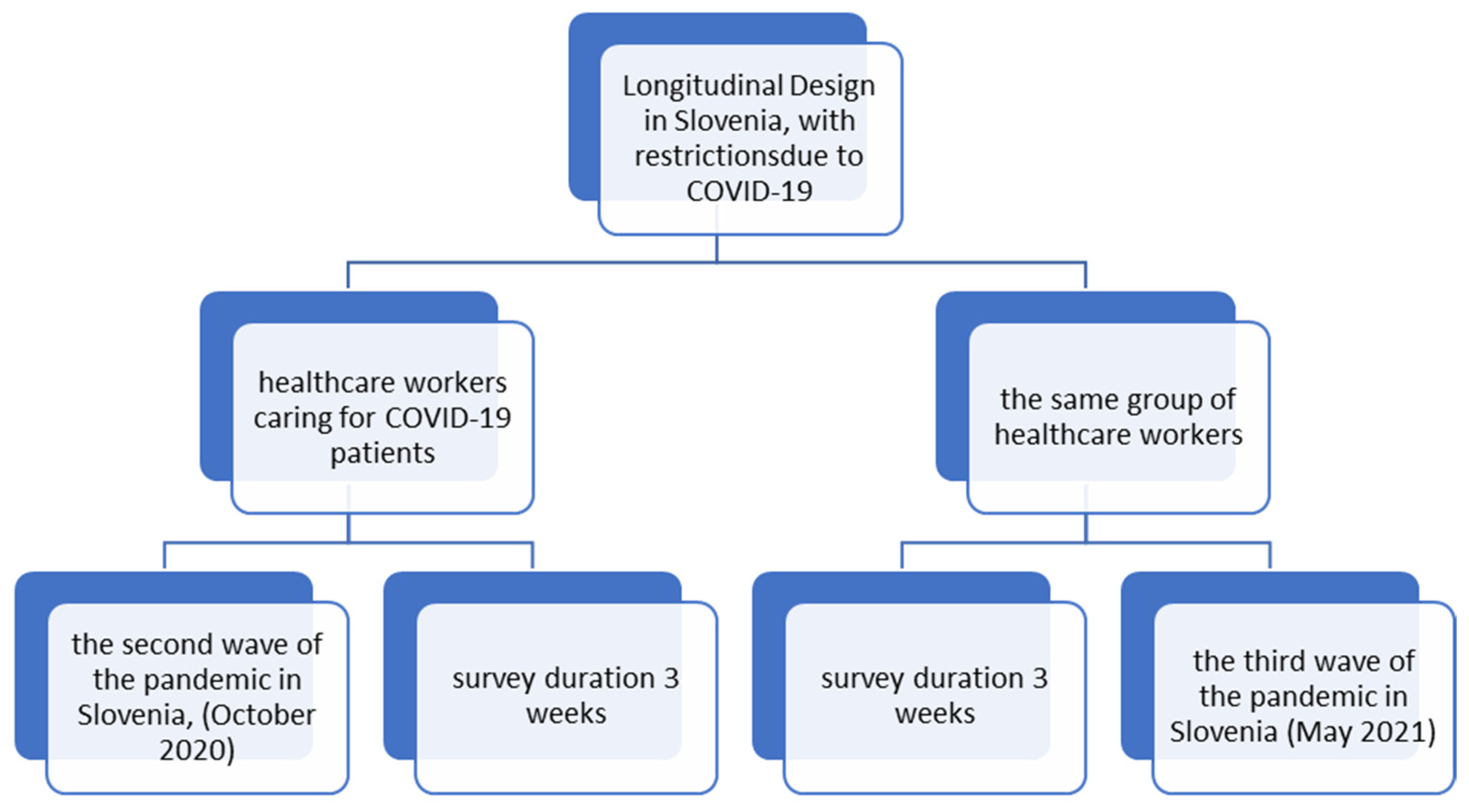
At the beginning of the second wave of the COVID-19 pandemic in Slovenia (in October 2020), all frontline and critical care healthcare workers caring for COVID-19 patients in the participating hospitals were invited to participate in the study (Figure 1).
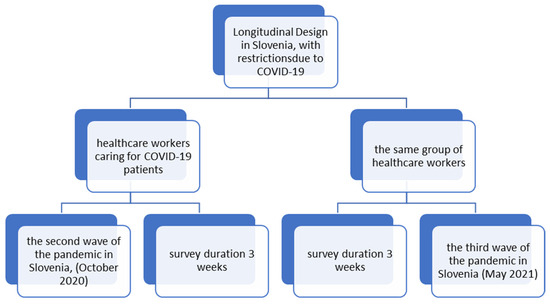
Figure 1.
The research concept of the longitudinal design in Slovenia.
The inclusion criteria for participants were that he or she is a healthcare worker working on the front line or critical care departments and caring for COVID-19 patients in a hospital, regardless of education level and length of service. A purposive sample was used. In total, 340 questionnaires were delivered in four participating hospitals, of which 184 were completed. The response rate was 54%. The same number of questionnaires were delivered to the frontline and critical care healthcare workers at the same hospitals towards the end of the third wave of the COVID-19 pandemic in Slovenia (May 2021), of which 142 were filled out. The response rate was 42%.
At the beginning of the second wave, 184 respondents participated in the study, of which 85.3% (n = 157) were female, and 14.7% (n = 27) were male. At the end of the third wave, 142 respondents participated, of which 82% (n = 116) were female, and 18% (n = 26) were male. At the beginning of the second wave, the mean age of the participants was 33.17 ± 7.45 (95%, CI = 32.08–34.26) years, and the mean professional experience was 9.07 ± 7.19 (95%, CI = 8.02–10.12) years. At the end of the third wave, the mean age was 34.76 ± 10.71 (95%, CI = 32.97–36.55), and professional experience was 10.39 ± 7.58 (95%, CI = 8.62–12.16). At the beginning of the second wave, only 26.1% (n = 45) of healthcare workers had previously worked with COVID-19 patients during the first wave. At the beginning of the second wave, 95% (n = 175) of healthcare workers had no chronic conditions, but at the end of the third wave, this number lowered to 75% (n = 131).
2.2. Data Collection
We used closed-ended questions in the survey. The questionnaire included demographic data (gender, level of education, years of work, etc.); in the following, the respondents defined themselves regarding statements about the assessment of mental health and burnout. The prevalence of burnout was determined with the Maslach Burnout Inventory—MBI-HSS (12) and the Mini-Z Survey 2.0 [45]. The MBI-HSS is a measure of job burnout defined by three subscales: emotional exhaustion (9 items); depersonalization (5 items); and personal accomplishment (8 items), each with a 7-point Likert-type frequency response scale (0 = never, 1 = a few times a year or less, 2 = once a month or less, 3 = a few times a month, 4 = once a week, 5 = a few times a week, 6 = every day) [27,49,50]. The maximum possible subscale scores were 54 for emotional exhaustion, 48 for personal accomplishment, and 30 for depersonalization. Higher scores indicate higher burnout for the emotional exhaustion and depersonalization dimensions, while lower scores indicate higher burnout for the personal accomplishment dimension. Scores of 19–26 or ≥27 on emotional exhaustion, 6–9 or ≥10 on depersonalization, and 34–39 and ≤33 on personal accomplishment are indicative of moderate or high burnout for the respective dimensions [27,28]. Internal consistency (Cronbach alpha) of the MBI-HSS was 0.86.
Self-reported burnout was also measured using the Mini Z Burnout Survey, accessible through the Institute for Professional Worklife’s website [45,51], which consists of ten questions with 5-point Likert scales. These ten items assess three outcomes (burnout, stress, and satisfaction) and seven drivers of burnout (work control, work chaos, teamwork, values alignment with leadership, documentation time pressure, electronic health record use at home, and electronic health record proficiency). A total score ≥ 20 (ranging from 10 to 40) represents a joyful work environment. The four questions on the Satisfaction Subscale focus on the positive features of a healthy work environment, including values aligned with institutional leadership and teamwork in the workplace. A higher score reflects a more supportive environment. An additional four questions on the Stress Subscale describe a lack of workplace control, pressured time for documentation, and a chaotic work environment. A higher score is considered to indicate a low-stress environment. The Mini Z Burnout Survey is an assessment tool used for evaluating burnout that was developed and statistically validated by Linzer et al. [44]. The internal consistency (Cronbach alpha) of the Mini Z Burnout Survey was 0.72.
The General Health Questionnaire (GHQ-12) [51], a closed-ended questionnaire for assessing mental health, was also used in the research. The questionnaire consists of 12 items that consider the severity of mental problems over several weeks using a 4-point Likert scale (from 0 for positive items to 3 for defining never). The maximum number of items could be 36 (from 0 to 36). A higher total indicates poorer mental health [41]. Internal consistency (Cronbach alpha) for the GHQ-12 was 0.86.
2.3. Statistical Analysis
A descriptive analysis was performed to assess the burnout and mental health of healthcare workers who worked with COVID-19 patients during the second and third waves of the COVID-19 pandemic. The results for the studied variables did not have a normal distribution (p < 0.001), which was confirmed by the Kolmogorov–Smirnov test. Therefore, non-parametric tests were used for analysis. The Mann–Whitney U-test and the Kruskal–Wallis H-test were used to find the differences between groups. Spearman’s correlation coefficient was used to find the associations between variables, and a regression analysis was used to determine the impacts of the studied independent variables on mental health (dependent variables) in the beginning and at the end of the second wave and at the end of the third wave of the COVID-19 pandemic in Slovenia. The level of statistical significance was set at p < 0.05. Statistical analysis was performed with SPSS version 27.0 (IBM Corp, Armonk, NY, USA).
3. Results
At the beginning of the second wave, 98% of participating healthcare workers (n = 180, 95%, CI = 96.2–100) were deployed in another clinical area, and 79% (n = 145, 95%, CI = 72.9–85.7) reported having received adequate information about COVID-19. The latter increased to 89% (n = 126, 95%, CI = 84.7–93.4) by the end of the third wave. During the period from the beginning of the second to the end of the third wave, the percentage of healthcare workers who assessed teamwork to be as efficient as it had been before the COVID-19 pandemic increased from 10.4% (n = 19, 95%, CI = 6.6–14.8) to 62.9% (n = 89, 95%, CI = 54.3–70.7). Healthcare workers who assessed that they had a person who provided all information about work increased from 90% (n = 166, 95%, CI = 85.0–95.0) to 96.2% (n = 137, 95%, CI = 93.5–98.9). Assessments that they had all documentation about work available increased from 87.9% (n = 162, 95%, CI = 82.1–92.9) to 95.1% (n = 135, 95%, CI = 91.8–97.8), and that they had sufficient equipment for personal safety and appropriate protection against infection increased from 87.9% (n = 162, 95%, CI = 82.1–92.9) to 98.9% (n = 140, 95%, CI = 97.3–100). Conversely, the percentage of healthcare workers who felt fearful for their loved ones’ health decreased from 94% (n = 173, 95%, CI = 90.2–97.3) to 52.9% (n = 74, 95%, CI = 44.3–60.7). We observed a similar decrease from 94% (n = 173, 95%, CI = 90.2–97.3) to 50% (n = 70, 95%, CI = 41.4–58.6) in the percentage of healthcare workers that were fearful for their health. Interestingly, the percentage of healthcare workers who assessed that the number of patients had increased fell from 97.8% (n = 180, 95%, CI = 95.7–99.5) to 77.9% (n = 81, 95%, CI = 69.3–85.7), and the percentage of those who assessed an increased workload fell from 100% 184 (n = 184, CI = 100) to 87.6% (n = 117, 95%, CI = 83.4–94.0). Table 1 presents descriptive statistics, the prevalence of burnout, and the level of mental health.

Table 1.
Prevalence of burnout and mental health assessments before the beginning of the second and at the end of the third wave of the COVID-19 pandemic.
The percentage of healthcare workers who felt uneasy about their work fell from 17.6% (n = 33, 95%, CI = 11.4–24.3) to 2.7% (n = 4, 95%, CI = 0.5–5.5); the percentage of healthcare workers who were physically active at least five times per week increased from 7.7% (n = 14, 95%, CI = 3.8–11.5) to 21.4% (n = 30, 95%, CI = 15.0–28.6) by the end of the third wave. Crucially, the percentage of healthcare workers who assessed that their quality of life was lower than before the COVID-19 pandemic decreased from 87.5% (n = 161, 95%, CI = 82.1–91.8) to 50.7% (n = 71, 955, CI = 42.1–59.3), and the percentage of healthcare workers feeling under stress due to their job fell from 64.6% (n = 119, 95%, CI = 59.8–69.1) to 36.7% (n = 52, 95%, CI = 31.3–40.8). The percentage of healthcare workers feeling a sense of job satisfaction increased from 16.4% (n = 30, 95%, CI = 26.2–34.3) to 62.6% (n = 89, 95%, CI = 57.8–67.8). Healthcare workers with one or more children were found to have had significantly higher scores for emotional exhaustion (Z = −4.295, p < 0.001) and depersonalization (Z = −3.023, p = 0.002), and lower scores for personal accomplishment (Z = 2.955, p = 0.003) and the workplace satisfaction (Z = 3.855, p < 0.001). Healthcare workers whose concern for the health of their loved ones was greater had a significantly higher score for depersonalization (Z = 2.560; p = 0.010). Table 1 shows significant differences in emotional exhaustion (Z = −6.444, p < 0.001), personal accomplishment (Z = −3.372, p < 0.001), depersonalization (Z = −4.240, p < 0.001), workplace satisfaction (Z = −7.007, p < 0.001), and mental health (Z = −7.336, p < 0.001) in a comparison between the beginning of the second and the end of the third wave of the COVID-19 pandemic.
At the beginning of the second wave of the COVID-19 pandemic, a positive correlation was found between emotional exhaustion and a higher number of patients (ρ = 0.246, p = 0.001, 95%, CI = 0.124–0.324), higher concern for health (ρ = 0.250, p = 0.001, 95%, CI = 0.089–0.390) and workload (ρ = 0.172, p = 0.006, 95%, CI = 0.038–0.310). A positive correlation was also found between depersonalization and a higher number of patients (ρ = 0.192; p = 0.009, 95%, CI = 0.050–0.301) and higher concern for health (ρ = 0.168; p = 0.023, 95%, CI = 0.092–0.327). Also, a positive correlation was found between mental health and workplace satisfaction (ρ = 0.198; p = 0.007, 95%, CI = 0.051–0.292) and physical activity (ρ = 0.160; p = 0.015, 95%, CI = 0.021–0.275) and a negative correlation between mental health and workload (ρ = −0.136; p = 0.039, 95%, CI = −0.232–0.010) (Table 2).
Table 2.
Correlation coefficient at the beginning of the second wave of the COVID-19 pandemic.
At the end of the third wave of the COVID-19 pandemic, a positive correlation was found between emotional exhaustion and workload (ρ = 0.181; p = 0.024, 95%, CI = 0.040–0.319), workplace stress (ρ = 0.551; p < 0.001, 95%, CI = 0.410–0.679), and depersonalization (ρ = 0.381; p < 0.001, 95%, CI = 0.220–0.527). A negative correlation was observed between personal accomplishment and depersonalization (ρ = −0.193; p = 0.015, 95%, CI = −0.358–0.022) and workplace stress (ρ = −0.203; p < 0.001, 95%, CI = −0.367–−0.044). A negative correlation was found between workplace satisfaction and a higher workload (ρ = −0.113, p = 0.038, 95%, CI = −0.204–0.026), and a higher number of patients (ρ = −0.256, p < 0.001, 95%, CI = −0.354–0.150). A positive correlation was found between workplace stress and a higher number of patients (ρ = 0.233; p < 0.001, 95%, CI = 0.081–0.389). A positive correlation was found between depersonalization and workplace stress (ρ = 0.176, p = 0.021, 95%, CI = 0.054–0.309) and emotional exhaustion (ρ = 0.381, p < 0.001, 95%, CI = 0.253–0.503), and a negative one with personal accomplishment (ρ = −0.193, p < 0.001, 95%, CI = 0.054, −0.312). A negative correlation was also found between mental health and workplace stress (ρ = −0.588; p = 0.003, 95%, CI = −0.698–0.312), concern for security (ρ = −0.286; p = 0.003, 95%, CI = −0.412–−0.156), emotional exhaustion (ρ = −0.403; p < 0.001, 95%, CI = −0.539–−0.256), and depersonalization (ρ = −0.240; p < 0.001, 95%, CI = −0.389–−0.103); and a positive correlation with workplace satisfaction (ρ = 0.205; p = 0.004, 95%, CI = −0.071–0.407) and physical activity (ρ = 0.312; p < 0.001, 95%, CI = 0.151–0.471) (Table 3).
Table 3.
Correlation coefficient at the end of the third wave of the COVID-19 pandemic.
We wanted to find out which studied factors affected healthcare workers’ mental health at the beginning of the second and at the end of the third wave of the COVID-19 pandemic. With the regression analysis (Table 4), we can explain 37% of the total variability of healthcare workers’ mental health at the beginning of the second wave of the COVID-19 pandemic with physical activity, concern for workplace security, and workplace satisfaction.
Table 4.
Results of the regression analysis for mental health at the beginning of the second wave of COVID-19 pandemic.
We also found that at the end of the third wave of the COVID-19 pandemic, we can explain 53% of the total variability of the mental health of healthcare workers with workload, concern for workplace security, physical activity, emotional exhaustion, personal accomplishment, and workplace stress (Table 5).
Table 5.
Results of the regression analysis for mental health at the end of the third wave of the COVID-19 pandemic.
4. Discussion
Burnout experienced by healthcare workers in this sample of frontline and critical care healthcare workers in hospitals was high. The mean scores for burnout and mental health were significantly lower at the end of the third wave, but still very high. Many researchers found that burnout among healthcare workers was moderate after experiencing a traumatic event [29,52,53]. There were significant differences in burnout according to level of education and parenthood status. Additionally, some previous studies reported that having children and living with a family [54] and demographic characteristics such as gender, age, and education level [55,56] influenced burnout.
At the beginning of the second wave of the COVID-19 pandemic, 88% of healthcare workers were deployed in a new clinical area. The mental health of many healthcare workers after the first wave already needed improvement [10]. Compared with the study in Poland [57], only 30% of medical professionals changed work locations during the outbreak of COVID-19. Healthcare workers who worked with COVID-19 patients during the first wave self-assessed personal burnout and emotional exhaustion as being slightly lower at the end of the third wave. All healthcare workers in the study said that patient numbers and workload had increased. Over 90% of healthcare workers felt concerned for the health of their loved ones and themselves at the beginning of the second wave, and this percentage was halved by the end of the third wave of the COVID-19 pandemic. Also, Hu et al. [47] found a high level of concern in frontline healthcare workers during the outbreak in Wuhan.
Regarding management, results support that they assessed that 89% of healthcare workers received all the required information; 84% assessed their teamwork as efficient, 96% had someone available who provided information about work, 95% had all work-related documentation available, 99% had sufficient equipment for personal safety and appropriate protection against infection, and 97% felt secure about their job at the end of the third wave. Compared with healthcare workers at the primary level during the COVID-19 pandemic in Australia [28], we can see the paradox that many healthcare workers were significantly concerned about their job security, and many reported lost work hours. Also, our study found that concern for workplace security was a significant predictor of healthcare workers’ mental health at the beginning of the second and at the end of the third wave of the COVID-19 pandemic. In Poland [57], only 30% of medical professionals reported appropriate protection against infection; in our study, in the beginning of the second wave of the COVID-19 pandemic, this was reported by about 87.9% of healthcare workers.
Scores for the MBI-HSS indicated high emotional exhaustion, high depersonalization, and a lower sense of personal accomplishment at the beginning of the second wave, which persisted throughout the third wave of the COVID-19 pandemic. At the end of the third wave of the COVID-19 pandemic, the percentage of healthcare workers with high emotional exhaustion and levels of depersonalization fell by 30%; conversely, 30% more healthcare workers felt a sense of increased personal accomplishment. Hu et al. [47] found that during the outbreak of COVID-19 in Wuhan, 61% of surveyed healthcare workers reported high emotional exhaustion. In our study, in the beginning of the second wave of COVID-19, 92% of healthcare workers reported high emotional exhaustion and 31% reported high levels of depersonalization. During the first wave of the COVID-19 pandemic, researchers also found, among Portuguese healthcare workers, high levels of work-related burnout, significant depression, stress, and anxiety [57].
Furthermore, our research indicates that more patients and an increased workload positively correlate with healthcare workers’ emotional exhaustion. Similarly, other researchers [56,57] found a positive correlation between high levels of emotional exhaustion among healthcare workers and an increased number of patients. Aiken et al. [58] noted that for each additional patient added to a healthcare worker’s workload, the likelihood of burnout is increased by 23%. Liu and Aungsuroch [59] found that workload represents a major stressor for healthcare workers, followed by the nature of healthcare workers’ work, healthcare workers’ expectations, family, interpersonal relationships, and contact with patients. At the beginning of the second wave of the COVID-19 pandemic, 64.6% of participating healthcare workers self-assessed that they were under stress, which fell to 36.7% by the end of the third wave. Concern for health correlated with healthcare workers’ emotional exhaustion and depersonalization in the beginning of the second wave of the COVID-19 pandemic. A study in China found that, during the first wave, women had less frequent symptoms of depression than men. Employees with shorter working years were more likely to develop depressive symptoms. Being a nurse was associated with a higher risk of mental health problems in the first wave [60]. In our study, we did not find differences in mental health between men and women, not even differences according to working experiences.
Additionally, before the coronavirus disease, some previous studies indicated that hospital healthcare workers in Slovenia were often exposed to stress [61,62]. At the beginning of the second wave of the COVID-19 pandemic, 17% of healthcare workers reported their working environment as being less stressful, and 16% of surveyed healthcare workers were satisfied with their work. This percentage increased to 63% by the end of the third wave, despite the high burnout. Furthermore, all participating healthcare workers in the second and third waves assessed their work environment as joyful. At the end of the third wave, 30% of surveyed healthcare workers assessed their work environment as less stressful, compared to 17% at the beginning of the second wave of the COVID-19 pandemic.
Scores for the GHQ-12 suggest that healthcare workers’ mental health was moderate. Crucially, our results indicate an improvement in the average levels of mental health among healthcare workers throughout the COVID-19 pandemic. The self-reported positive mental health of healthcare workers rose from 53% at the beginning of the second wave to 75% at the end of the third wave of the COVID-19 pandemic. In the study, we found that with individual and organizational studied variables (concern for workplace security, workplace satisfaction, and physical activity), we can explain 37% of the total variability of the mental health of healthcare workers at the beginning of the second wave of the COVID-19 pandemic. And it was also found that at the end of the third wave of the COVID-19 pandemic, with workload, concern for workplace security, physical activity, emotional exhaustion, personal accomplishment, and workplace stress we can explain 53% of the total variability of the mental health of healthcare workers. The results on burnout and mental health are comparable to results from Poland [55], China [33,63], and Wuhan [57]. A cross-sectional study [64] found that 80% of healthcare workers in Slovenian hospitals had positive mental health and that leadership style, leaders’ characteristics, and job satisfaction significantly correlate with healthcare workers’ mental health. These results also underpin the importance of management support for healthcare workers during the COVID-19 pandemic.
Few studies [65,66,67] identified individual and institutional risks and protective factors affecting the mental health of healthcare professionals during the pandemic. Healthcare workers should prioritize their well-being, meeting their basic needs (food, drink, time to sleep and rest) and adequate rest both during and outside work [67]. Also, Kenrick et al. [68] noted that human physiological and safety needs come to the forefront at times of crisis.
Limitations and Future Recommendations
This study can serve as a basis for taking care of healthcare employees during crises, and can contribute to a significant degree to both avoiding and preventing burnout, which harms the mental health of healthcare professionals. Our topic is central to the changes in management practices in hospitals worldwide and should be an integrated part of everyday discussion. Nonetheless, the study has its limitations. A limitation of this study is its cross-sectional design, wherein the different subgroups may differ in respects not directly attributable to the different hospitals. Further, the fact that we have data only from hospitals that were taking care of COVID-19 patients at the beginning of the second wave of the COVID-19 pandemic should be considered. The survey’s timing may limit the generalizability to frontline and critical care healthcare workers working in other fields and at different periods. Moreover, frontline healthcare workers might express less burnout, anxiety, depression, and fear than they de facto experience due to social desirability factors. In the research, factors affecting wellness levels were assessed while taking into account fears of contracting COVID-19 and the equipment and information available. Personal factors were taken into account. For future research, it is recommended that, in addition to external factors and personal influences, the organization’s policies, employee support available, and the attitudes and conduct of health policy-makers are taken into account. It makes sense that further studies be conducted on a larger number of respondents, in all healthcare institutions, to ensure the generalizability of the results. Further research and monitoring are required to determine and care for healthcare professionals’ mental health and well-being.
Decision-makers at the national and hospital management levels should take measures to strengthen workplace satisfaction, as this protects against mental health problems in the long term. Including employees in psychological support efforts, training that enhances satisfaction and effective communication strategies to reduce burnout, and promoting mechanisms for strengthening mental health are necessary. Also, management should not forget working conditions (working hours, balance between personal and professional life), as a healthy work environment can improve mental health.
Healthy workplace practices can help employees create a low-stress work environment with integrated daily working habits. As a prerequisite, they must be organized at an organizational level with supportive management, including efforts to decrease stress at work and the promotion of employees’ well-being and engagement. To prevent burnout, we recommend the following measures for both management and healthcare employees:
- Real-time and constant information and involvement of all employees in the planning and implementation of healthcare activities;
- Providing support and assistance in times of crisis and during the emergence of fear (employees must be informed about the person in charge of offering support, as well as all necessary documentation);
- Providing adequate and sufficient protective equipment;
- Promoting effective communication and cooperation between employees;
- Workload and capacity have to be in balance;
- Constant monitoring of well-being and the presence of possible burnout symptoms in employees;
- Awareness that inadequate resources and a lack of autonomy and control of feelings impact one’s ability to succeed at our present and future actions;
- A feeling of fairness at work can be improved if employees feel valued and recognized for the contributions they make;
- It is important to recognize highly demanding (cognitively, emotionally, or physically) tasks;
- Taking time for oneself is crucial for well-being and will benefit the individual’s performance;
- It is important to recognize times when someone is most stressed or anxious;
- All members of healthcare teams must be aware of the symptoms and signs of burnout among colleagues and promote early recognition.
5. Conclusions
During the COVID-19 pandemic, there was also a shortage of medical workers in Slovenia and there was a mismatch between medical needs and the qualifications and experience of employees. In the research, we tried to define employees’ reactions to establishing strategies based on best practices and the possibility of creating a new personnel model for possible emergencies. The research provided insight into the problems of nursing employees during the COVID-19 pandemic and the possibility of preparing strategies for possible emergency situations based on the lessons learned. In the event of a possible future emergency, it is necessary to carry out country-level responses with consideration of specific situations in the country. The sustainable development of the mental health of healthcare employees must be a crucial part of the strategic sustainable development of healthcare organizations. Management must encourage employees to satisfy their needs and enable them to satisfy them at the workplace. With the development of sustainable strategies in the field of mental health and the prevention of burnout, it is only necessary to include this in the work culture that affects the work environment. Employees do not only want to work for the organization, but they also want sustainable development within the organization.
These results create a foundation for interventions that aim to decrease healthcare workers’ burnout and simultaneously improve healthcare workers’ mental health. Considering that both burnout and worsening mental health are preventable, nursing employees must raise awareness of burnout and poor mental health, because of the psychologically and physically significant effects on the individuals’ health.
Psychological support for employees in nursing is essential to maintaining their well-being and mental health, especially when levels of occupational stress and emotional exhaustion are high. Ensuring psychological well-being and health requires a complex approach with different interventions, techniques, and strategies for prevention and recognition at different levels of healthcare. This study also provides some suggestions on how to take care of employees in nursing during a crisis and avoid and prevent burnout, to a significant degree.
Author Contributions
Conceptualization, M.D. and M.L.; methodology, M.L. and M.D.; software, M.L.; validation, M.L.; formal analysis, M.L.; investigation, M.D.; resources, M.L. and M.D.; data curation, M.L. and M.D.; writing—original draft preparation, M.L. and M.D; writing—review and editing, M.L. and M.D.; visualization, M.D.; supervision, M.L. and M.D.; project administration, M.L. and M.D.; funding acquisition, M.L. and M.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The research includes human data which is in accordance with the Declaration of Helsinki and has been approved by the Ethics Committee (No. 04/1R-2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic. 2019. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 30 May 2023).
- Yıldırım, M.; Geçer, E.; Akgül, Ö. The impacts of vulnerability, perceived risk, and fear on preventive behaviours against COVID-19. Psychol. Health Med. 2020, 26, 35–43. [Google Scholar] [CrossRef]
- Adams, J.G.; Walls, R.M. Supporting the health care workforce during the COVID-19 global epidemic. JAMA 2020, 323, 1439–1440. [Google Scholar] [CrossRef] [PubMed]
- Koh, D. Occupational risks for COVID-19 infection. Occup. Med. 2020, 70, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Godinic, D.; Obrenovic, B.; Khudaykulov, A. Effects of Economic Uncertainty on Mental Health in the COVID-19 Pandemic Context: Social Identity Disturbance, Job Uncertainty and Psychological Well-Being Model. Int. J. Innov. Econ. Dev. 2020, 6, 61–74. [Google Scholar] [CrossRef]
- Xie, X.; Jin, X.; Wei, G.; Chang, C.-T. Monitoring and Early Warning of SMEs’ Shutdown Risk under the Impact of Global Pandemic Shock. Systems 2023, 11, 260. [Google Scholar] [CrossRef]
- Wang, D. The influencing factors of career adaptability of newcomers: Based on multiple perspectives of individual, family and school. J. Chin. Hum. Resour. Manag. 2020, 11, 84–91. [Google Scholar] [CrossRef]
- Lei, L.; Huang, X.; Zhang, S.; Yang, J.; Yang, L.; Xu, M. Comparison of Prevalence and Associated Factors of Anxiety and Depression Among People Affected by versus People Unaffected by Quarantine During the COVID-19 Epidemic in Southwestern China. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2020, 26, e924609. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef]
- Kapetanos, K.; Mazeri, S.; Constantinou, D.; Vavlitou, A.; Karaiskakis, M.; Kourouzidou, D.; Nikolaides, C.; Savvidou, N.; Katsouris, S.; Koliou, M. Exploring the factors associated with the mental health of frontline healthcare workers during the COVID-19 pandemic. PLoS ONE 2021, 16, e0258475. [Google Scholar] [CrossRef]
- McGuinness, S.L.; Johnson, J.; Eades, O.; Cameron, P.A.; Forbes, A.; Fisher, J.; Grantham, K.; Hodgson, C.; Hunter, P.; Kasza, J.; et al. Mental Health Outcomes in Australian Healthcare and Aged-Care Workers during the Second Year of the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 4951. [Google Scholar] [CrossRef]
- Maslach, C.; Leiter, M.P. Understanding the burnout experience: Recent research and its implications for psychiatry. World Psychiatry 2016, 15, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Jackson, S.E. The measurement of experienced burnout. J. Organ. Behav. 1981, 2, 99–113. [Google Scholar] [CrossRef]
- Xiao, X.; Zhu, X.; Fu, S.; Hu, Y.; Li, X.; Xiao, J. Psychological impact of healthcare workers in China during COVID-19 pneumonia epidemic: A multi-center cross-sectional survey investigation. J. Affect. Disord. 2020, 274, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Bueno Ferrán, M.; Barrientos-Trigo, S. Caring for the caregiver: The emotional impact of the coronavirus epidemic on nurses and other health professionals. Enferm. Clin. Engl. Ed. 2021, 31, S35–S39. [Google Scholar] [CrossRef]
- Estiri, M.; Nargesian, A.; Dastpish, F.; Sharifi, S.M. The impact of psychological capital on mental health among Iranian nurses: Considering the mediating role of job burnout. SpringerPlus 2016, 5, 1377. [Google Scholar] [CrossRef]
- Arrogante, O.; Aparicio-Zaldivar, E. Burnout and health among critical care professionals: The mediational role of resilience. Intensive. Crit. Care. Nurs. 2017, 42, 110–115. [Google Scholar] [CrossRef]
- Scanlan, J.N.; Still, M. Relationships between burnout, turnover intention, job satisfaction, job demands and job resources for mental health personnel in an Australian mental health service. BMC Health Serv. Res. 2019, 19, 62. [Google Scholar] [CrossRef]
- Maben, J.; Bridges, J. Covid-19: Supporting nurses’ psychological and mental health. J. Clin. Nurs. 2020, 29, 2742–2750. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, W.; Sun, Y.; Qian, W.; Liu, Z.; Wang, R.; Qi, L.; Yang, J.; Song, X.; Zhou, X.; et al. The prevalence and risk factors of psychological disturbances of frontline medical staff in china under the COVID-19 epidemic: Workload should be concerned. J. Affect. Disord. 2020, 277, 510–514. [Google Scholar] [CrossRef]
- Linzer, M.; Smith, C.D.; Hingle, S.; Poplau, S.; Miranda, R.; Freese, R.; Palamara, K. Evaluation of Work Satisfaction, Stress, and Burnout Among US Internal Medicine Physicians and Trainees. JAMA Netw. Open 2020, 3, e2018758. [Google Scholar] [CrossRef]
- Xin, L.; Xia, Z.; Tao, J. Humanization of nature: Testing the influences of urban park characteristics and psychological factors on collegers’ perceived restoration. Urban For. Urban Green. 2023, 79, 127806. [Google Scholar]
- Arslan, G.; Yıldırım, M.; Wong, P.T.P. Meaningful living, resilience, affective balance, and psychological health problems during COVID-19. Curr. Psychol. 2020, 71, 7812–7823. [Google Scholar] [CrossRef]
- Cai, Z.; Cui, Q.; Liu, Z.; Li, J.; Gong, X.; Liu, J.; Wan, Z.; Yuan, X.; Li, X.; Chen, C.; et al. Nurses endured high risks of psychological problems under the epidemic of COVID-19 in a longitudinal study in Wuhan China. J. Psychiatr. Res. 2020, 131, 132–137. [Google Scholar] [CrossRef] [PubMed]
- West, C.P.; Dyrbye, L.N.; Shanafelt, T.D. Physician burnout: Contributors, consequences and solutions. J. Intern. Med. 2018, 283, 516–529. [Google Scholar] [CrossRef] [PubMed]
- Bradley, M.; Chahar, P. Burnout of healthcare providers during COVID-19. Clevel. Clin. J. Med. 2020. epub ahead of print. Available online: https://www.ccjm.org/content/ccjom/early/2020/07/01/ccjm.87a.ccc051.full.pdf (accessed on 21 August 2023).
- Society of Critical Care Medicine. Clinicians Report High Stress in COVID-19 Response. 2020. Available online: https://sccm.org/blog/may-2020/sccm-covid-19-rapid-cycle-survey-2-report (accessed on 21 August 2023).
- Stehman, C.R.; Testo, Z.; Gershaw, R.S.; Kellogg, A.R. Burnout, Drop Out, Suicide: Physician Loss in Emergency Medicine, Part I. West. J. Emerg. 2019, 20, 485–494. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Dyrbye, L.N.; Sinsky, C.; Hasan, O.; Satele, D.; Sloan, J.; West, C.P. Relationship Between Clerical Burden and Characteristics of the Electronic Environment with Physician Burnout and Professional Satisfaction. Mayo Clin. Proc. 2016, 91, 836–848. [Google Scholar] [CrossRef]
- Medscape. Medscape US and International Physicians’ COVID-19 Experience Report: Risk, Burnout, Loneliness. Available online: https://www.medscape.com/slideshow/2020-physician-covid-experience-6013151 (accessed on 21 August 2023).
- Du, M.; Hu, K. Frontline Health Care Workers’ Mental Workload During the COVID-19 Pandemic: A Cross-Sectional Study. Asia Pac. J. Public Health 2021, 33, 303–305. [Google Scholar] [CrossRef]
- Chen, Q.; Liang, M.; Li, Y.; Guo, J.; Fei, D.; Wang, L.; He, L.; Sheng, C.; Cai, Y.; Li, X.; et al. Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, e15–e16. [Google Scholar] [CrossRef]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Cohen, M.; Cruz, L.N.; Cardoso, R.B.; Albuquerque, M.D.F.P.M.D.; Montarroyos, U.R.; de Souza, W.V.; Ludermir, A.B.; de Carvalho, M.R.; Vicente, J.D.D.S.; Filho, M.P.V.; et al. Impact of the COVID-19 pandemic on the mental health of frontline healthcare workers in a highly affected region in Brazil. BMC Psychiatry 2023, 23, 255. [Google Scholar] [CrossRef]
- Juan, Y.; Yuanyuan, C.; Qiuxiang, Y.; Cong, L.; Xiaofeng, L.; Yundong, Z.; Jing, C.; Peifeng, Q.; Yan, L.; Xiaojiao, X.; et al. Psychological distress surveillance and related impact analysis of hospital staff during the COVID-19 epidemic in Chongqing, China. Compr. Psychiatry 2020, 103, 152198. [Google Scholar] [CrossRef] [PubMed]
- Tomaszewska, K.; Majchrowicz, B.; Snarska, K.; Guzak, B. Psychosocial Burden and Quality of Life of Surveyed Nurses during the SARS-CoV-2 Pandemic. Int. J. Environ. Res. Public Health 2023, 20, 994. [Google Scholar] [CrossRef] [PubMed]
- Cahill, A.G.; Olshavsky, M.E.; Newport, D.J.; Benzer, J.; Chambers, K.M.; Custer, J.; Rathouz, P.J.; Nutt, S.; Jwaied, S.; Leslie, R.; et al. Occupational Risk Factors and Mental Health Among Frontline Health Care Workers in a Large US Metropolitan Area During the COVID-19 Pandemic. Prim. Care Companion CNS Disord. 2022, 24, 21m03166. [Google Scholar] [CrossRef]
- Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1859–1922. [CrossRef] [PubMed]
- Guttormson, J.L.; Calkins, K.; McAndrew, N.; Fitzgerald, J.; Losurdo, H.; Loonsfoot, D. Critical Care Nurse Burnout, Moral Distress, and Mental Health During the COVID-19 Pandemic: A United States Survey. Heart Lung 2022, 55, 127–133. [Google Scholar] [CrossRef]
- Lee, Y.J.; Yun, J.; Kim, T. Stress- and Work-Related Burnout in Frontline Health-Care Professionals During the COVID-19 Pandemic. Disaster Med. Public Health Prep. 2021, 17, e38. [Google Scholar] [CrossRef]
- Lorber, M.; Dobnik, M. The Importance of Monitoring the Work-Life Quality during the COVID-19 Restrictions for Sustainable Management in Nursing. Sustainability 2023, 15, 6516. [Google Scholar] [CrossRef]
- Prasad, K.; McLoughlin, C.; Stillman, M.; Poplau, S.; Goelz, E.; Taylor, S.; Nankivil, N.; Brown, R.; Linzer, M.; Cappelucci, K.; et al. Prevalence and correlates of stress and burnout among U.S. healthcare workers during the COVID-19 pandemic: A national cross-sectional survey study. eClinicalMedicine 2021, 35, 100879. [Google Scholar] [CrossRef]
- Maslach, C.; Leiter, M.P.; Jackson, S.E. Maslach Burnout Inventory, 4th ed.; Mind Garden: Menlo Park, CA, USA, 2017. [Google Scholar]
- Linzer, M.; Poplau, S.; Babbott, S.; Collins, T.; Guzman-Corrales, L.; Menk, J.; Murphy, M.L.; Ovington, K. Worklife and Wellness in Academic General Internal Medicine: Results from a National Survey. J. Gen. Intern. Med. 2016, 31, 1004–1010. [Google Scholar] [CrossRef]
- Linzer, M. Mini Z Burnout Survey. Institute for Professional Worklife (IPS). 2015. Available online: https://www.professionalworklife.com/mini-z-survey (accessed on 30 September 2020).
- Kim, J.S.; Choi, J.S. Factors Influencing Emergency Nurses’ Burnout During an Outbreak of Middle East Respiratory Syndrome Coronavirus in Korea. Asian Nurs. Res. 2016, 10, 295–299. [Google Scholar] [CrossRef] [PubMed]
- Hu, D.; Kong, Y.; Li, W.; Han, Q.; Zhang, X.; Zhu, L.X.; Wan, S.W.; Liu, Z.; Shen, Q.; Yang, J.; et al. Frontline nurses’ burnout, anxiety, depression, and fear statuses and their associated factors during the COVID-19 outbreak in Wuhan, China: A large-scale cross-sectional study. Clin. Med. 2020, 24, 100424. [Google Scholar] [CrossRef]
- Mayo, A.T. Teamwork in a pandemic: Insights from management research. BMJ Lead. 2020, 4, 53–56. [Google Scholar] [CrossRef]
- Escribà-Agüir, V.; Martín-Baena, D.; Pérez-Hoyos, S. Psychosocial work environment and burnout among emergency medical and nursing staff. Int. Arch. Occup. Environ. Health 2006, 80, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, D.P. User’s Guide to the General Health Questionnaire; National Foundation for Educational Research Nelson: Windsor, UK, 1988. [Google Scholar]
- Adriaenssens, J.; De Gucht, V.; Maes, S. Determinants and prevalence of burnout in emergency nurses: A systematic review of 25 years of research. Int. J. Nurs. Stud. 2015, 52, 649–661. [Google Scholar] [CrossRef] [PubMed]
- Hunsaker, S.; Chen, H.-C.; Maughan, D.; Heaston, S. Factors That Influence the Development of Compassion Fatigue, Burnout, and Compassion Satisfaction in Emergency Department Nurses. J. Nurs. Sch. 2015, 47, 186–194. [Google Scholar] [CrossRef]
- Halcomb, E.; McInnes, S.; Williams, A.; Ashley, C.; James, S.; Fernandez, R.; Stephen, C.; Calma, K. The Experiences of Primary Healthcare Nurses During the COVID-19 Pandemic in Australia. J. Nurs. Sch. 2020, 52, 553–563. [Google Scholar] [CrossRef]
- Maciaszek, J.; Ciulkowicz, M.; Misiak, B.; Szczesniak, D.; Luc, D.; Wieczorek, T.; Fila-Witecka, K.; Gawlowski, P.; Rymaszewska, J. Mental Health of Medical and Non-Medical Professionals during the Peak of the COVID-19 Pandemic: A Cross-Sectional Nationwide Study. J. Clin. Med. 2020, 9, 2527. [Google Scholar] [CrossRef]
- Duarte, I.; Pinho, R.; Teixeira, A.; Martins, V.; Nunes, R.; Morgado, H.; Castro, L.; Serrão, C. Impact of COVID-19 pandemic on the mental health of healthcare workers during the first wave in Portugal: A cross-sectional and correlational study. BMJ Open 2022, 12, e064287. [Google Scholar] [CrossRef]
- Pradas-Hernández, L.; Ariza, T.; Gómez-Urquiza, J.L.; Albendín-García, L.; De la Fuente, E.I.; Canadas-De la Fuente, G.A. Prevalence of burnout in paediatric nurses: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0195039. [Google Scholar] [CrossRef]
- Sacadura-Leite, E.; Sousa-Uva, A.; Ferreira, S.; Costa, P.L.; Passos, A.M. Working conditions and high emotional ex-haustion among hospital nurses. Rev. Bras. Med. Trop. 2020, 17, 69–75. [Google Scholar] [CrossRef]
- Aiken, L.H.; Clarke, S.; Sloane, D.M.; Sochalski, J.; Silber, J.H. Hospital Nurse Staffing and Patient Mortality, Nurse Burnout, and Job Dissatisfaction. JAMA 2002, 288, 1987–1993. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Aungsuroch, Y. Work stress, perceived social support, self-efficacy and burnout among Chinese registered nurses. J. Nurs. Manag. 2019, 27, 1445–1453. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Fu, W.; Liu, X.; Luo, Z.; Wang, R.; Zhou, N.; Yan, S.; Lv, C. Mental health status of medical staff in emergency departments during the Coronavirus disease 2019 epidemic in China. Brain Behav. Immun. 2020, 88, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Dobnik, M.; Maletič, M.; Skela-Savič, B. Work-Related stress factors in nurses at Slovenian hospitals—A cross-sectional study. Zdr. Varst. 2018, 57, 192–200. [Google Scholar] [CrossRef]
- Lorber, M.; Treven, S.; Mumel, D. Well-Being and Satisfaction of Nurses in Slovenian Hospitals: A Cross-Sectional Study. Zdr. Varst. 2020, 59, 180–188. [Google Scholar] [CrossRef]
- Kang, L.; Ma, S.; Chen, M.; Yang, J.; Wang, Y.; Li, R.; Yao, L.; Bai, H.; Cai, Z.; Yang, B.X.; et al. Impact on mental health and perceptions of psychological care among medical and nursing staff in Wuhan during the 2019 novel coronavirus disease outbreak: A cross-sectional study. Brain Behav. Immun. 2020, 87, 11–17. [Google Scholar] [CrossRef]
- Lorber, M.; Treven, S.; Mumel, D. Leadership behavior predictor of employees’ job satisfaction and psychological health. In Exploring the Influence of Personal Values and Cultures in the Workplace; Nedelko, Z., Brzozowski, M., Eds.; IGI Global: Hershey, PA, USA, 2017; pp. 323–347. [Google Scholar] [CrossRef]
- Li, Z.; Ge, J.; Yang, M.; Feng, J.; Qiao, M.; Jiang, R.; Bi, J.; Zhan, G.; Xu, X.; Wang, L.; et al. Vicarious traumatization in the general public, members, and non-members of medical teams aiding in COVID-19 control. Brain Behav. Immun. 2020, 88, 916–919. [Google Scholar] [CrossRef]
- Sasangohar, F.; Jones, S.L.; Masud, F.N.; Vahidy, F.S.; Kash, B.A. Provider Burnout and Fatigue During the COVID-19 Pandemic: Lessons Learned from a High-Volume Intensive Care Unit. Anesth. Analg. 2020, 131, 106–111. [Google Scholar] [CrossRef]
- Cole-King, A.; Dykes, L. Wellbeing for HCWs during COVID-19. 2020. Available online: https://d29e30c9-ac68-433c-8256-f6f9c1d4a9ec.filesusr.com/ugd/bbd630_fc6de742af1442baada144de34343388.pdf (accessed on 21 August 2023).
- Kenrick, D.T.; Griskevicius, V.; Neuberg, S.L.; Schaller, M. Renovating the Pyramid of Needs: Contemporary extensions built upon ancient foundations. Perspect. Psychol. Sci. 2010, 5, 292–314. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).