Abstract
The restrictions due to COVID-19 have left their mark on the education of children with disabilities. Conducting physical therapy classes online was a necessity and at the same time a challenge for both teachers and parents. The purpose of this paper was to investigate spatio-temporal orientation, followed by the design and implementation of stimulation programs for education, by applying multisensory intervention programs conducted online. The study included 27 students with DS and associated conditions. The groups were established according to the kinetic diagnosis, motor and psychomotor disorders of each child. The statistical analysis was quantitative, with a significance level of 95%. The dependent test was used to highlight the significance of the rate of progress achieved by the children. Results obtained for the psychomotor component—spatial orientation registered an increase of 1.81 units, between the initial and the final test. The value of the Student-t test calculated t between the two tests is 6.20 so 6.20 > 2.056 (Table Fischer) and as a result the differences are significant (p < 0.05). Regarding the psychomotor component, for temporal orientation, the results registered an increase of 1.37 units between the initial and the final test. The value of the Student t test calculated between the two tests is 7.68 so 7.68 > 2.056 (Table Fischer), and as a result the differences are significant between the averages of the two tests (p < 0.05). Following the experiment, the results obtained by the subjects, at the final test, were superior to the initial ones, with differences between statistically significant arithmetic averages for all components of the investigated psychomotor ability: spatial orientation and temporal orientation.
1. Introduction
The impact of COVID-19 has also left its mark on the education of children with disabilities. Like all education systems, special education has been conducted online, through various educational programs. [1,2,3]. The application of online learning in the educational system has allowed a learning framework centered on the student [4,5].
Global policies on the rights of persons with disabilities (Article 24 of the UN Convention) stipulate that Member States must take measures to ensure that persons with disabilities have access to primary and secondary education, including quality and free education [6,7,8]. Special education will enable people with Down Syndrome to achieve and maintain maximum independence and full physical, mental, social and professional capacity [9,10].
Continuing online studies for children with Down Syndrome (DS) is all the more important as it ensures mental balance and physical well-being, materialized in health, physical mobility, and adequate nutrition [11,12,13]. Through the online platforms, it was possible to continue the training and kinetic stimulation (supported by the attendant) of children with DS, given that the problems they may have are multiple: muscle hypotonia (low muscle tone), heart problems, respiratory disorders, hearing or vision problems, etc. [14,15,16]. The construction of the holistic image of a child’s world and the surrounding space is revealed in many psychological and pedagogical problems. The ability to move in space is one of the means towards harmonious personal development [17].
Young people with intellectual disabilities (ID) have significant limitations in the functioning of both intellectual and adaptive behavior, which leads to disabilities in terms of conceptual, social and practical adaptation skills [18,19,20,21,22].
Special education can be understood as a mode of education adapted and intended for children who fail to meet the requirements of the school curriculum and to reach a level of education appropriate to the age and requirements of society. The child’s relationship with the world will determine his level of organization and spatial orientation, information on the external environment and knowledge of body parts condition the control of body movements [23,24,25,26,27]. Spatial structure “involves awareness of the situation of one’s body in relation to the external environment, awareness of objects between them and the ability to organize activity, to place objects according to the desired spatial landmarks” [28,29]. The specialized literature specifies that spatial structure appears in the preschool period: spatial orientation is highlighted at the age of 4 and lasts about 1 year, emphasizing knowledge of the right-left concept; spatial organization from the age of 5 until the age of 6 is characterized by the ability to orient and combine certain elements, knowing the inclined position, occupying a predetermined space and following a path; understanding of spatial relations takes place after the age of 5–6 years when the individual depends on the criteria according to which a sequence is composed. The structuring of time is achieved starting from perception, through the interaction of the visual, auditory, kinesthetic analyzers and with the help of thinking [30,31]. Specialists in the field believe that “temporal organization allows us to realize a sequence of events, in relation to each other, to define the present in relation to the past and the future, evaluating the duration and speed of execution to achieve in the end of the rhythmic structure”. Understanding the regular alternation over time of certain groups of stimuli and their accentuation leads to the perception of rhythm. Movements are performed with the help of two connecting elements, space and time; these elements are learned and acquired through a differentiated and individualized psychomotor education [32,33,34].
Complex programs developed and applied for kinetic stimulation capitalize on sensory learning based on component modification, by internalizing and integrating sensory stimuli that lead to perceptions and perceptual-motor responses: body awareness, spatial awareness, direction awareness and temporal awareness. The formation of new movement skills of a child with Down Syndrome is effective when he has his own body consciousness, has stability and can coordinate his motor gestures, given that each child has its own pace of evolution and a unique pattern of growth and development.
The purpose of the study is to investigate spatio-temporal orientation followed by the design and implementation of a stimulation program for education, by applying a multisensory intervention program, conducted online, whose ultimate goal is orientation (organization), structuring (spatial) and temporal (reporting of time to one’s own person, discrimination of chronological succession, discrimination of the duration of facts, actions, processes, events; discrimination of the rhythm of the interval, transposition of space in time and vice versa). The research hypothesis can be formulated as follows: “The education of the components of psychomotor skills, especially of spatiotemporal orientation, in a pandemic context, ensures a better efficiency of the activity of the child with Down Syndrome”.
2. Materials and Methods
Objectives:
- Outlining the perceptual-motor profile of space and time of the child with DS;
- Carrying out complex intervention programs and ways to individualize them, depending on the particularities of each subject and their use in online physiotherapy lessons in special secondary schools.
2.1. Participants
The research was conducted on a sample of 27 students with DS and associated conditions. The groups were established according to the kinetic diagnosis, motor and psychomotor disorders of each child. The experimental group was formed by randomization (using the random selection technique) and included 27 students aged 12 to 15 years, with the same psychomotor characteristics (Down Syndrome, IQ = 30–65) (Appendix A, Table A1 and Table A2).
In psycho-pedagogical/methodological research where participants cannot be selected without the risk of rendering incomplete the numbers of students in the class-rooms, the “classroom” is also taken as an experimental group, considering that the “chance” factor has acted in the initial establishment of the classroom [35]. In special schools in Romania, children with Down Syndrome are randomly assigned to classes with a maximum number of 3 children with Down Syndrome per class.
All students with Down Syndrome whose parents gave their consent participated. There were no criteria for excluding subjects from participating in the research. The research respected the ethical and medical conditions of the subjects’ participation. The study was conducted in accordance with the Helsinki Declaration on Research Involving Human Subjects.
The children subjected to the experiment accomplished the psychomotor therapy program, during kineto-therapy classes, through the Microsoft Teams platform, the psychomotor therapy being associated with the kinetic therapy. The motor stimulation program was created by the teachers who initiated this research and who distributed this program to physical therapy teachers in special schools to be implemented in lessons, using the specified means. The evaluation tests were carried out online by each teacher.
It is specified that students with severe intellectual disability (Down Syndrome) benefit from 1–2 h per week of psychomotor therapy in specific therapies, but this therapy is performed individually, online. The therapeutic group includes a single child, who will be supervised by a family companion. Due to the diversity of diagnosis, the specific characteristics of children in therapeutic groups are represented by poor posture, reduced ability to control muscle, disorders of static and dynamic balance, inefficient coordination of movements in space, disorders of breathing rhythm, crawling and walking away; unclear laterality, motor slowness, disturbances in movement accuracy, poor evolution of complicated movements.
2.2. Procedure
The research is of the ameliorative ascertainment type in which only one experimental independent variable (the motor stimulation program) was used.
The applied research was carried out through educational platforms (Microsoft Teams, Google Classroom) in the Special Gymnasium Schools of the Municipality of Bucharest, in the form of a longitudinal, challenging, ascertaining and comparative experiment.
The aim of this study is to investigate, design and implement a multisensory stimulation program (one curriculum) to educate the components of perceptual-motor capacity, as well as to correct existing physical deficiencies in children with Down Syndrome included in special education (12–15 years), who benefit from 1–2 h of physical therapy, regulated by the school curriculum. The experiment took place in the kineto-therapy lessons as follows: a kineto-therapy lesson for each child/30 min, between 01 October 2020–10 June 2021, respectively 28 lessons (Table 1).

Table 1.
Stages of experimental research.
The therapy took place online, at the home of each child who was part of the research group. During the therapy classes, melo-therapy was used; the songs were slow throughout the therapy, aiming to facilitate communication, thus giving the child confidence in his own strength, making gradual progress; the children’s clothing was light to allow them to move during class.
Individual psychomotor progress assessment sheets were used, in which the results of the initial and final tests were noted, aiming to achieve all the objectives. Each teacher was able to choose the order of the exercises used in the lesson, taking into account the time allocated to the lesson and the conscious and active participation of the subject (Table 2).
Table 2.
The multisensory stimulation program.
The evaluation was carried out according to the pretest–independent variable–final test scheme [36,37]; between the two tests the independent variable was applied to the subjects (Table 3):
Table 3.
The evaluation of the spatio-temporal orientation.
Pretest–Independent variable (motor program stimulation)–Final test.
2.3. Statistics
The data obtained as a result of the measurements were recorded in collective files in order to centralize, process, compare and establish the relationships between them (Appendix B, Table A3).
Data processing and interpretation was carried out with the help of statistical programs:
- the computer product WORD version 2007, from the Microsoft company;
- computer product EXCEL version 2007, from the Microsoft company and then analyzed through IBM SPSS software.
As part of our research, the data obtained through measurements and tests were processed statistically, recording the following indicators:
- Upper limit (Maximum) = the highest value in the data string;
- Lower limit (Minimum) = the smallest value in the data string;
- The arithmetic mean denotes the central tendency of the research group and results from the sum of the variables, related to the total number of cases (n).
- Standard deviation (S)—represents the square root of the dispersion and allows us to evaluate the degree of homogeneity of the group. Thus, the smaller the standard deviation, the more homogeneous the data obtained.
- The coefficient of variability (CV)—shows us the degree of importance of the data;
- T test dependent—A dependent t-test is an example of a “within-subjects” or “repeated-measures” statistical test. This indicates that the same participants are tested more than once. In our research, we used a significance threshold of p = 0.05, in order to see the confidence level of the arithmetic mean, at a risk of 5%. Thus, within the limits determined by the confidence level, with a certain possibility of risk, it is assumed that the value of the statistical index of the general community will also be found. The higher the value of t, the greater the difference between the means and the smaller the standard deviations of the respective series. In the case of the 5% confidence level, we will have a 95% chance that the true mean of the general population will be within the determined confidence limits [38].
3. Results
The highlighting of the level of motor development and the rate of progress was achieved through the indicators of the central tendency and the T dependent significance test.
The results obtained for the psychomotor component – spatial orientation registered an increase of 1.81 units between the initial and the final test (Table 4, Figure 1).
Table 4.
Statistical indicators for spatial orientation, initial and final testing.
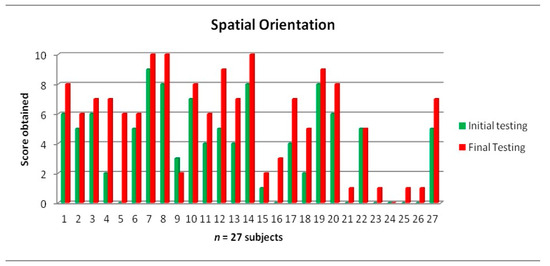
Figure 1.
The results obtained by the children, at the initial and final tests applied, for the spatial orientation.
The coefficient of variability “Cv”, in the case of the initial test, has a value of 77.64% and a value of 62.07% for the final test. In both tests, the value of the coefficient of variation indicates heterogeneity of the group.
The degree of scattering of the string values represented by the standard deviation “σ” has values of 2.96 for the initial test and 3.15 for the final test.
The value of the Student t test calculated between the two tests is 6.20, so 6.20 > 2.056 (Table Fischer), and as a result the differences are significant (p < 0.05).
The data obtained at the initial test show that students have problems with spatial orientation (seven subjects obtained a score of 0 points). Following the applied program, only one child did not make progress; he had a complex diagnosis and his comprehension was quite low. The subjects also obtained low scores in spatial orientation, although there is an improvement in the final results.
The final test showed an improvement in the results, in terms of spatial orientation, in the final tests three subjects obtaining the maximum score.
Regarding the psychomotor component–temporal orientation, the results registered an increase between the initial and the final test (Table 5, Figure 2).
Table 5.
Statistical indicators for time orientation initial and final testing.
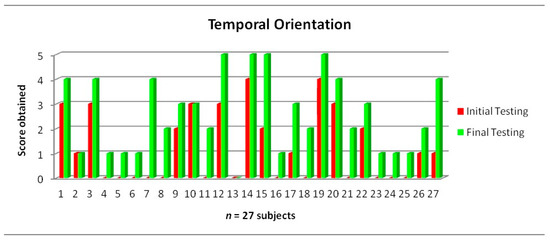
Figure 2.
The results obtained by the children at the initial and final tests applied for the temporal orientation.
The coefficient of variability “Cv” in the case of the initial test has a value of 116.44% and a value of 59.81% for the final test. In both tests, the value of the coefficient of variation indicates heterogeneity of the group.
The degree of scattering of the string values represented by the standard deviation “σ” has values of 1.43 for the initial test and 1.55 for the final test.
The value of the Student t test calculated between the two tests is 7.68, so 7.68 > 2.056 (Table Fischer) and as a result the differences are significant between the averages of the two tests (p < 0.05).
Initial testing for temporal orientation shows that students have major temporal orientation problems (13 subjects scored 0 points).
The final test showed an improvement of the results: three subjects obtained the maximum score in the temporal orientation test, which was more difficult for children with intellectual disabilities.
Following the applied program, only one child did not make progress, but obtained satisfactory results in other tests, though this test proved to be a very difficult one for him.
4. Discussion
Most studies have identified the effectiveness of using online lessons in improving the psychomotor potential of children with Down Syndrome, compared to traditional teaching [39,40,41].
The positive effects of motor programs are consistent with empirical research on the effects of motor interventions on balance and spatio-temporal orientation skills in children and young people with Down Syndrome [42,43,44].
Eloquent results were obtained when subjects were assigned general motor skills programs (e.g., a training program adapted to play and physical development), balance and strength exercises, computer games, physical therapy program, vestibular or sensori-motor exercises or specific sports techniques (handball) [45,46]. In the analysis by [47,48], it is specified that the most effective interventions lasted from 6 weeks to one year and a half, with three to five sessions of 45 to 60 min per week and the importance of keeping children with physical and mental disability not only physically safe, but also looking after their psychological and emotional wellbeing [49]. The family plays an important role in the psycho-physical development of children with Down Syndrome [50,51,52].
Impact
This paper provides an important scientific contribution, as there are no studies on the link between motor education, psychomotor education and physical therapy programs.
The design of adequate stimulation programs for motor and psychomotor education of children with intellectual disabilities aimed at the multifunctional development of psycho-motor skills, improving the physical condition of students and their social integration.
The strategy applied focused in a first phase on the development of psychomotor components through newly created and diversified exercises, followed by specific exercises for physical therapy. These were special means for educating psychomotor skills, all of which were conducted online.
The present results indicate that the improvement of spatial and temporal orientation skills in children with Down Syndrome should be targeted by professionals through general motor skills programs, physical therapy programs and vestibular sensorimotor exercises. The satisfactory results obtained from this study are clear evidence for a potential further study that will benefit the e-learning system for children with Down Syndrome.
5. Conclusions
The results obtained in psychomotor tests applied to the research subjects, who bene-fitted from complex kinetic programs of individualized stimulation, showed that the spatio-temporal orientation is the component of psycho-motority that poses the biggest problem for children with Down Syndrome, which is why the use of many exercises meant to form a sense of rhythm and tempo. We highlight the fact that the heterogeneity of the group also left its mark on the rate of progress registered by the children during the months of training, but nevertheless all of them registered a positive evolution, not only at the motor level, but also emotionally.
Improving intellectual ability is closely linked to motor activity and, as a result, educational programs should focus on the use of sensorimotor skills, basic skills, basic movement patterns and movement components.
Achieving the objectives stipulated in the multisensory stimulation programs re-quires rethinking the physiotherapy lessons, meant to ensure the individualization of the demands from a motor and functional point of view, in relation to the mental age of each subject.
The adaptation of kinetic programs for the online environment is based on the use of individual sensory information (their perception, interpretation and integration) obtained from the organism environment interaction, in order to form an organized and coordinated motor behavior.
Children who worked online and were supported by parents were able to achieve remarkable results, unlike those who did not benefit from the involvement of an adult, who were unable to carry out the program, which led to unfavorable results.
Author Contributions
Conceptualization, O.P. and N.L.; methodology, O.P.; software, N.L.; validation, N.L. and O.P.; formal analysis, O.P. and N.L.; investigation, O.P.; resources, N.L. and O.P.; data curation, O.P. and N.L.; writing—original draft preparation, O.P.; writing—review and editing, N.L.; visualization, O.P. and N.L.; supervision, N.L.; project administration, O.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki. In the field of Sports Science and Physical Education, research is conducted on human subjects. The article for which approval is requested is not in the medical field, the subjects of this research being students with various disabilities, who perform motor programs with means specific to Physical Education. Ethical review and approval were waived for this study because Politehnica University of Bucharest has an engineering profile and Politehnica University of Bucharest Ethics Committee (https://upb.ro/en/ethics-committee/, accessed on 11 December 2022), has no procedures (https://upb.ro/wp-content/uploads/2017/11/regulament-comisie-de-etica.pdf, accessed on 11 December 2022) for articles with scientific subjects that involves human subjects, human material, human tissues, or human data, all certified by UPB Register 2022/XII/15. Written informed consent for publication was obtained from participating subjects.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the parents to publish this paper.
Data Availability Statement
Not applicable.
Acknowledgments
Authors express thanks to all children and their parents involved in this research.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Table A1.
Subjects participating in the research.
Table A1.
Subjects participating in the research.
| No. Crt. | Class | Name Surname | Birthday | Q.I. | Anthropometric Measurements | |
|---|---|---|---|---|---|---|
| Weight | Height | |||||
| 1 | IV A | I.N. | 25 July 2008 | 36 | 36 | 143 |
| 2 | IV A | J.M. | 26 December 2008 | 32 | 23 | 125 |
| 3 | IV B | F.Ș. | 10 July 2008 | 51 | 34 | 139 |
| 4 | IV B | P.R. | 17 November 2008 | 30 | 25 | 135 |
| 5 | IV A | I.S. | 20 September2008 | 45 | 32 | 130 |
| 6 | V A | P.T. | 7 August2006 | 34 | 39 | 151 |
| 7 | V A | B.D. | 13 April 2007 | 34 | 43 | 163 |
| 8 | V A | F.M. | 28 November 2006 | 65 | 33 | 156 |
| 9 | V A | B.R. | 4 October 2008 | 40 | 46 | 159 |
| 10 | V A | G.A. | 19 September 2007 | 64 | 45 | 147 |
| 11 | V A | L.E. | 8 July 2005 | 77 | 39 | 143 |
| 12 | V B | V.A. | 31 October 2006 | 48 | 42 | 147 |
| 13 | V B | S.V. | 12 September 2007 | 64 | 30 | 140 |
| 14 | V B | Z.A. | 19 February 2005 | 40 | 31 | 139 |
| 15 | VI A | B.L. | 1 November 2007 | 50 | 54 | 146 |
| 16 | VI B | G.A.M. | 8 March 2005 | 47 | 58 | 169 |
| 17 | VI B | O.G. | 27 March 2006 | 50 | 58 | 148 |
| 18 | VI A | M.R. | 6 September 2007 | 65 | 54 | 153 |
| 19 | VII A | I.C. | 1 April 2005 | 38 | 47 | 160 |
| 20 | VII A | P.A. | 5 April 2005 | 45 | 66 | 158 |
| 21 | VIII B | I.C.A. | 16 January2005 | 35 | 70 | 165 |
| 22 | VIII B | C.Ș. | 4 October 2005 | 47 | 82 | 184 |
| 23 | VIII A | C.D. | 08 August 2005 | 30 | 35 | 140 |
| 24 | VIII A | G.A. | 13 December2005 | 65 | 53 | 173 |
| 25 | VIII A | P.D. | 12 March 2005 | 39 | 35 | 160 |
| 26 | VIII A | M.Ș. | 19 March 2005 | 50 | 39 | 170 |
| 27 | VIII A | B.A. | 17 May 2005 | 55 | 49 | 166 |
Table A2.
Diagnosis of students participating in the research.
Table A2.
Diagnosis of students participating in the research.
| No. Crt. | Class | Name Surname | Birthday | Diagnosis | Therapeutic Pregnancies | Entries | ||
|---|---|---|---|---|---|---|---|---|
| Medical | Kinetic | Q.I. | ||||||
| 1 | IV A | I.N. | 25 July 2008 | Down Syndrome medium psychic retardation psychomotor deficiency | -muscular hypotonia -psychomotor deficiency | 36 | -spatio-temporal deficiency -multisensory psychomotor stimulation | 1/week. |
| 2 | IV A | J. M. | 26 December 2008 | sdr. down severe mental and language delay psychomotor deficiency | -muscular hypotonia -psychomotor deficiency -lumbar lordosis | 32 | -correction of lordosis -stimulation Psychomotor -muscle toning | 1/week. |
| 3 | IV B | F.Ș. | 10 July 2008 | Down Syndrome moderate/severe mental delay | -muscular hypotonia, -psychomotor delay -cyfolordosis | 51 | -muscle toning -psychomotor stimulation -correction of cyfolordosis | 1/week. |
| 4 | IV B | P.R. | 17 November 2008 | Down Syndrome infantile autism severe mental retardation | -muscular hypotonia, -psychomotor delay, -kyphosis | 30 | -muscle toning, -psychomotor stimulation -correction of kyphosis | 1/week. |
| 5 | IV A | I.S. | 20 September2008 | Down Syndrome moderate mental delay. marked psychomotor instability psychomotor disorders | -kyphosis -psychomotor disorders | 45 | -correction of kyphosis -psychomotor stimulation. | 1/week. |
| 6 | V A | P.T. | 7 August2006 | Down Syndrome severe retardation in psychic development predominantly of language congenital heart malformation pulmonary hypertension—pulmonary stasis psychomotor delay | -muscular hypotonia -psychomotor delay -Lumbar lordosis | 34 | -muscle toning; -re-education of fine motor skills. -psychomotor stimulation -correction of lordosis | 1/week. |
| 7 | V A | B.D. | 13 April 2007 | Down Syndrome obesity gr.ii attention deficit attentional peculiarities psychomotor deficiency | -balance disturbances -lumbar lordosis -psychomotor deficits | 34 | -educating the balance -psychomotor optimization. -correction of lordosis -education of fine motor skills | 1/week. |
| 8 | V A | F.M. | 28 November 2006 | Down Syndrome easy delay in mental development hyperkinetic syndrome | -kyphosis -hypotonia muscle | 65 | -correction of kyphosis -muscle toning | 1/week. |
| 9 | V A | B.R. | 4 October 2008 | Down Syndrome slight delay in mental development extrapyramidal syndrome of neuromuscular etiology dyslalie | -kyphoscoliosis. -muscular hyportonia | 40 | -psychomotor optimization; -correction of kyphoscoliosis | 1/week. |
| 10 | V A | G.A. | 19 September 2007 | Down Syndrome infantile cerebral palsy—spastic paraparesis without independent gait slight psychic delay | -gait disturbances; -spastic paraparesis -balance disorders; | 64 | -correction of gait -improvement of spasticity. -stimulating balance | 1/week. |
| 11 | V A | L.E. | 8 July 2005 | Down Syndrome -cerebral palsy with spastic tetraparesis -symptomatic focal epilepsy -parencephaly | -scoliosis balance disturbances; poor gait. | 77 | -correction of scoliosis; -correction of gait; -psychomotor optimization. | 1/week. |
| 12 | V B | V.A. | 31 October 2006 | Down Syndrome infantile cerebral palsy-right spastic hemiparesis, partial sentient epilepsy average mental retardation hypoprosexy, hypomnesia | mowing gait dr scoliosis psychomotor deficiency | 48 | -correction of gait, -correction of scoliosis, -psychomotor stimulation. | 1/week. |
| 13 | V B | S.V. | 12 September 2007 | Down Syndrome disorders with autistic spectrum moderate mental retardation hyperkinetic disorder with attention deficit disorder. | muscular hypotonia; psychomotor delay. | 64 | -muscle toning; -stimulation psychomotor. -correction of scoliosis | 1/week. |
| 14 | V B | Z.A. | 19 February 2005 | Down Syndrome infantile cerebral palsy spastic paraparesis by postnatal factors symptomatic epilepsy average mental delay | bilateral mowing gait psychomotor delay, kyphosis | 40 | muscle toning, -psychomotor stimulation, -correction of kyphosis. | 1/week. |
| 15 | VI A | B.L. | 1 November 2007 | Down Syndrome spastic tetraparesis (predominantly paraparetic form by prematurity and gemenaryity mild mental retardation enuresis and diurnal ecopresis | bilateral mowing gait scolosis c dr. psychomotor delay | 50 | -psychomotor optimization; -muscle toning -correction of scoliosis | 1/week. |
| 16 | VI B | G.A.M. | 08 March 2005 | Down Syndrome moderate pshic delay | thoracic kyphosis muscular hypotonia; psychomotor delay | 47 | -correction of kyphosis; -motor optimization; -stimulation of cardio-respiratory function. | 1/week. |
| 17 | VI B | O.G. | 27 March 2006 | Down Syndrome easy psychic delay polymorphic dyslalie behavioral disorders obesity | muscular hypotonia, lumbar lordosis, psychomotor delay overweight | 50 | -muscle toning, -correction of lordosis, -psychomotor optimization. | 1/week. |
| 18 | VI A | M.R. | 6 September 2007 | Down Syndrome easy psychic delay. behavioral affective immaturity. disorders of ocular refraction, bilateral horizontal nystagmus. psychomotor disorders | orientation disorders kyphosis; psychomotor disorders | 65 | -correction of postural deficiencies kyphosis -education of fine motor skills. | 1/week. |
| 19 | VII A | I.C. | 1 April 2005 | Down Syndrome severe mental retardation psychomotor instability immature behavior dependent on the adult | scoliosis; deficient body attitude; psychomotor delay | 30 | -correction of scoliosis; -psychomotor stimulation. | 1/week. |
| 20 | VII A | P.A. | 5 April 2005 | Down Syndrome autistic elements moderate mental retardation | psychomotor retardation thoracic kyphosis muscular hypotonia | 38 | muscuular toning. -correction of kyphosis -psychomotor stimulation | 1/week. |
| 21 | VIII B | I.C.A. | 16 January2005 | Down Syndrome school difficulties through educational deficiencies and attention deficit night paver spasm of the crying roar in the antecedent easy mental delay behavioral affective immaturity serious attention deficit. | scoliosis c dr muscular hypotonia | 45 | -correction of scoliosis -muscle toning | 1/week. |
| 22 | VIII B | C.Ș. | 4 October 2005 | Down Syndrome mental retardation and severe language behavioral disorders on the background of retardation | psychomotor retardation kyphosis muscular hypotonia | 35 | -psychomotor stimulation -correction of kyphosis -muscle toning | 1/week. |
| 23 | VIII A | C.D. | 08 August 2005 | Down Syndrome neorganic enuresis average mental retardation other craniosynostoses | kyphosis psychomotor retardation improvement of stereotypes | 47 | -psychomotor stimulation -correction of kyphosis | 1/week. |
| 24 | VIII A | G.A. | 13 December2005 | Down Syndrome genetic oligophrenia average mental retardation very weak expressive language develop very difficult cooperation dyslexia, dysgraphia, dyscalculia hyperkinetic sdr. behavioral affective immaturity | psychomotor retardation thoracic kyphosis | 65 | -correction of kyphosis -stimulation psychomotor | 1/week. |
| 25 | VIII A | P.D. | 12 March 2005 | Down Syndrome interatrial septal defect delay in severe form psychic development myopia | psychomotor retardation, muscular hypotonia overweight lumbar lordosis | 39 | -psychomotor optimization, correction of lordosis -muscle toning | 1/week. |
| 26 | VIII A | M.Ș. | 19 March 2005 | Down Syndrome; mild mental delay in development psychomotor deficiency | muscular hypotonia; overweight lumbar lordosis | 50 | -muscle toning; -correction of lordosis; -psychomotor stimulation. | 1/week. |
| 27 | VIII A | B.A. | 17 May 2005 | Down Syndrome; retardation in mental and language development, polymorphic dyslalie, attention deficit psychomotor instability. psychomotor delay | muscular hypotonia psychomotor delay. kyphosis | 55 | -muscle toning; -correction of kyphosis -psychomotor stimulation | 1/week. |
Appendix B
Table A3.
The scores obtained in the tests.
Table A3.
The scores obtained in the tests.
| No. Crt. | Initial Testing | Final Testing | Initial Testing | Final Testing |
|---|---|---|---|---|
| Spatial Orientation | Temporal Orientation | |||
| 1 | 6 | 8 | 3 | 4 |
| 2 | 5 | 6 | 1 | 1 |
| 3 | 6 | 7 | 3 | 4 |
| 4 | 2 | 7 | 0 | 1 |
| 5 | 0 | 6 | 0 | 1 |
| 6 | 5 | 6 | 0 | 1 |
| 7 | 9 | 10 | 0 | 4 |
| 8 | 8 | 10 | 0 | 2 |
| 9 | 3 | 2 | 2 | 3 |
| 10 | 7 | 8 | 3 | 3 |
| 11 | 4 | 6 | 0 | 2 |
| 12 | 5 | 9 | 3 | 5 |
| 13 | 4 | 7 | 0 | 0 |
| 14 | 8 | 10 | 4 | 5 |
| 15 | 1 | 2 | 2 | 5 |
| 16 | 0 | 3 | 0 | 1 |
| 17 | 4 | 7 | 1 | 3 |
| 18 | 2 | 5 | 0 | 2 |
| 19 | 8 | 9 | 4 | 5 |
| 20 | 6 | 8 | 3 | 4 |
| 21 | 0 | 1 | 0 | 2 |
| 22 | 5 | 5 | 2 | 3 |
| 23 | 0 | 1 | 0 | 1 |
| 24 | 0 | 0 | 0 | 1 |
| 25 | 0 | 1 | 0 | 1 |
| 26 | 0 | 1 | 1 | 2 |
| 27 | 5 | 7 | 1 | 4 |
References
- Bartlett, J.D.; Griffin, J.; Thomson, D. Resources for supporting children’s emotional well-being during the COVID-19 pandemic. Child Trends 2020, 12, 1. [Google Scholar]
- Bateman, B.D. Individual Education Programs for Children with Disabilities. In Handbook of Special Education; Routledge: London, UK, 2017; pp. 87–104. [Google Scholar]
- Chaabane, S.; Doraiswamy, S.; Chaabna, K.; Mamtani, R.; Cheema, S. The Impact of COVID-19 School Closure on Child and Adolescent Health: A Rapid Systematic Review. Children 2021, 8, 415. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, W.K.; McTigue, E.M.; Matsuda, N. Development and validation of the teachers’ digital learning identity survey. Int. J. Educ. Res. 2021, 105, 101717. [Google Scholar] [CrossRef]
- Chandolias, K.; Besios, T.; Tsigaras, G.; Chalkia, A.; Trevlaki, E. The Impact of the COVID-19 Pandemic on the Rehabilitation of Children with Chronic Diseases and Disabilities. Education 2020, 5, 190–196. [Google Scholar]
- Tindle, K.; East, B.; Mellard, D. Online Learning for Students with Disabilities: Considerations for LEA Policies, Practices, and Procedures. Center for Online Learning and Students with Disabilities. 2017. Available online: https://centerononlinelearning.ku.edu/wp-content/uploads/2017/05/LEA_ResourceDoc_April2017.pdf (accessed on 17 September 2022).
- Barnett, L.M.; Stodden, D.; Cohen, K.E.; Smith, J.J.; Lubans, D.R.; Lenoir, M.; Iivonen, S.; Miller, A.; Laukkanen, A.; Dudley, D.A.; et al. Fundamental movement skills: An important focus. J. Teach. Phys. Educ. 2016, 35, 219–225. [Google Scholar] [CrossRef]
- Kim, J.Y.; Fienup, D.M.; Daniel, M. Increasing Access to Online Learning for Students With Disabilities During the COVID-19 Pandemic. J. Spéc. Educ. 2021, 55, 213–221. [Google Scholar] [CrossRef]
- Available online: https://en.unesco.org/themes/inclusion-in-education/disabilities (accessed on 13 July 2021).
- Available online: https://www.ohchr.org/EN/HRBodies/CRPD/Pages/ConventionRightsPersonsWithDisabilities.aspx (accessed on 24 September 2021).
- Smith, S.J.; Basham, J.D.; Rice, M.; Carter, R.A., Jr. Preparing special education teachers for online learning: Findings from a surve of teacher educators. J. Spec. Educ. Technol. 2016, 31, 170–178. [Google Scholar] [CrossRef]
- Cook, K.C.; Grant-Davis, K. Online Education: Global Questions, Local Answers; Routledge: London, UK, 2020. [Google Scholar]
- Tandy, C.; Meacham, M. Removing the Barriers for Students with Disabilities: Accessible Online and Web-Enhanced Courses. J. Teach. Soc. Work 2009, 29, 313–328. [Google Scholar] [CrossRef]
- Ali, A.M. E-learning for Students With Disabilities During COVID-19: Faculty Attitude and Perception. SAGE Open 2021, 11. [Google Scholar] [CrossRef]
- Nair, A.; Nair, D.; Girdhar, M.; Gugnani, A. Optimizing developmental outcomes by setting smart goals individualized home program for children with disabilities during COVID-19. Int. J. Physiother. Res. 2021, 9, 4028–4034. [Google Scholar] [CrossRef]
- Yazcayir, G.; Gurgur, H. Students with Special Needs in Digital Classrooms during the COVID-19 Pandemic in Turkey. Pedagog. Res. 2021, 6, em0088. [Google Scholar] [CrossRef]
- Wauters-Krings, F. (Psiho)Motricitate: Sprijin, Prevenție Și Compensare; Editura ASCR Cluj Napoca: Cluj, Romania, 2014. [Google Scholar]
- Logan, S.W.; Ross, S.M.; Chee, K.; Stodden, D.F.; Robinson, L.E. Fundamental motor skills: A systematic review of terminology. J. Sport. Sci. 2018, 36, 781–796. [Google Scholar] [CrossRef] [PubMed]
- Gherghuț, A. Psihopedagogia Persoanelor cu Cerințe Speciale; Editura Polirom: București, Romania, 2006; pp. 248–249. [Google Scholar]
- Schalock, R.L.; Luckasson, R.A.; Shogren, K.A. The renaming of mental retardation: Understanding the change to the term intellectual disability. Intellect. Dev. Disabil. 2007, 45, 116–124. [Google Scholar] [CrossRef]
- Bota, A.; Teodorescu, S.; Şerbănoiu, S. Unified Sports–a social inclusion factor in school communities for young people with intellectual disabilities. Procedia-Soc. Behav. Sci. 2014, 117, 21–26. [Google Scholar] [CrossRef]
- Bota, A.; Teodorescu, S. Teaching and Coaching Young People With Intellectual Disabilities: A Challenge for Mainstream Specialists. In Sport, Coaching and Intellectual Disability; Routledge: London, UK, 2014; pp. 80–105. [Google Scholar]
- Wellala, S.; Thathsarani, S.A.; Senaratne, D.; Samaranayake, P.; Jayakody, A. Assistive Learning Platform for Children with Down Syndrome. In Proceedings of the 2020 20th International Conference on Advances in ICT for Emerging Regions (ICTer), Colombo, Sri Lanka, 4–7 November 2020; pp. 294–295. [Google Scholar]
- Toquero, C.M.D. Inclusion of People with Disabilities amid COVID-19: Laws, Interventions, Recommendations. Multidiscip. J. Educ. Res. 2020, 10, 158–177. [Google Scholar] [CrossRef]
- Zare, S.; Rahnama, N.; Movahedi, A.R. The effect of balance exercises on static and dynamic balance of the mentally retarded female students. J. Exerc. Sci. Med. 2016, 8, 143–158. [Google Scholar]
- Carter, K.; Sunderman, S.; Burnett, S.W. The effect of vestibular stimulation exercises on balance, coordination, and agility in children with Down syndrome. Am. J. Psychiatry Neurosci. 2018, 6, 28–32. [Google Scholar] [CrossRef]
- Potop, V.; Jurat, V.; Buftea, V. Dezvoltarea Orientării Spațio-Temporale cu Ajutorul Mijloacelor din Gimnastică la Elevii Treptei Gimnaziale. In Sport. Olimpism. Sănătate, 2nd ed.; Print-Caro: Chișinău, Moldova, 2018; ISBN 978-9975-131-65-0. [Google Scholar]
- Verza, E.; Verza, F. Tratat De Psihopedagogie Specială; Editura Universității Din București: Bucharest, Romania, 2011; p. 671. [Google Scholar]
- Epuran, M. Psihologia Educaţiei Fizice; Universitatea Ecologică Bucureşti: Bucharest, Romania, 1994; pp. 104–105. [Google Scholar]
- Epuran, M. Psihologia Educaţie Fizice; Editura Sport Turism: Bucharest, Romania, 1976; p. 135. [Google Scholar]
- Maïano, C.; Hue, O.; April, J. Effects of motor skill interventions on fundamental movement skills in children and adolescents with intellectual disabilities: A systematic review. J. Intellect. Disabil. Res. 2019, 63, 1163–1179. [Google Scholar] [CrossRef]
- Rigal, R.; Nader, L.; Bolduc, G.; Chevaler, N. L’education Motrice et L’education Psychomotrice au Prescolaireet au Primaire; Presses De L’Universite Du Quebec: Québec, Canada, 2010; p. 329. [Google Scholar]
- McGuire, M.; Long, J.; Esbensen, A.J.; Bailes, A.F. Adapted dance improves motor abilities and participation in children with Down syndrome: A pilot study. Pediatr. Phys. Ther. 2019, 31, 76–82. [Google Scholar] [CrossRef]
- Popa, C.E.; Dobrescu, T. The effectiveness of therapeutic physical exercises in improving balance and coordination in children with Down syndrome. Rom. J. Multidimens. Educ. /Rev. Rom. Pentru Educ. Multidimens. 2017, 9, 89–102. [Google Scholar] [CrossRef]
- Epuran, M. Metodologia Cercetarii Activitatilor Corporale. Exercitii Fizice. Sport. Fitness, 2nd ed; Editura FEST: Bucharest, Romania, 2005. [Google Scholar]
- Mânzat, B. Terapia Psihomotricităţii şi Abilitare Manuală. In Terapia Educaţională Integrată; Muşu, I., Taflan, A., Eds.; Pro Humanitate: Bucharest, Romania, 1997; p. 268. [Google Scholar]
- Moţet, D. Psihopedagogia Recuperării Handicapurilor Neuromotorii; Fundaţiei Humanitas: Bucharest, Romania, 2021; p. 193. [Google Scholar]
- Available online: https://statistics.laerd.com/statistical-guides/dependent-t-test-statistical-guide.php (accessed on 30 October 2021).
- Venegas, C.; Cevallos, R.; Córdova, R.; De La Cruz, D.; Tobar, J.; Mejıa, P. Educational platform for children with Down syndrome manageable by the educator. In Proceedings of the World Congress on Engineering and Computer Science, San Francisco, CA, USA, 19–21 October 2016; Volume 1. [Google Scholar]
- Ayda, N.K.; Bastas, M.; Altınay, F.; Altinay, Z.; Dagli, G. Distance education for students with special needs in primary schools in the period of COVID-19 epidemic. Propósitos Represent. 2020, 8, 43. [Google Scholar]
- Torres-Carrión, P.V.; González-González, C.S.; Toledo-Delgado, P.A.; Muñoz-Cruz, V.; Gil-Iranzo, R.; Reyes-Alonso, N.; Hernández-Morales, S. Improving Cognitive Visual-Motor Abilities in Individuals with Down Syndrome. Sensors 2019, 19, 3984. [Google Scholar] [CrossRef] [PubMed]
- Hoseini, S.A.; Zar, A.; Khodadoust, M.; Hejazi, E. The Effect of Eight Weeks Posture and Balance Trainings on Physical Fitness Factors of Mental Retardation Children. J. Ped. Nurs. 2017, 3, 26–31. [Google Scholar] [CrossRef][Green Version]
- Logan, S.W.; Robinson, L.E.; Wilson, A.E.; Lucas, W.A. Getting the fundamentals of movement: A meta-analysis of the effectiveness of motor skill interventions in children. Child Care Health Dev. 2012, 38, 305–315. [Google Scholar] [CrossRef] [PubMed]
- John, F.M.; Bromham, N.R.; Woodhouse, J.M.; Candy, T.R. Spatial vision deficits in infants and children with Down syndrome. Investig. Ophthalmol. Vis. Sci. 2004, 45, 1566–1572. [Google Scholar] [CrossRef]
- Feng, J.; Lazar, J.; Kumin, L.; Ozok, A. Computer usage by children with down syndrome: Challenges and future research. ACM Trans. Access. Comput. (TACCESS) 2010, 2, 1–44. [Google Scholar] [CrossRef]
- Hargreaves, S.; Holton, S.; Baxter, R.; Burgoyne, K. Educational experiences of pupils with Down syndrome in the UK. Res. Dev. Disabil. 2021, 119, 104115. [Google Scholar] [CrossRef]
- Lewis, C.L.; Fragala-Pinkham, M.A. Effects of Aerobic Conditioning and Strength Training on a Child with Down Syndrome: A Case Study. Pediatr. Phys. Ther. 2005, 17, 30–36. [Google Scholar] [CrossRef]
- Hardee, J.P.; Fetters, L. The effect of exercise intervention on daily life activities and social participation in individuals with Down syndrome: A systematic review. Res. Dev. Disabil. 2017, 62, 81–103. [Google Scholar] [CrossRef]
- Patel, K. Mental health implications of COVID-19 on children with disabilities. Asian J. Psychiatry 2020, 54, 102273. [Google Scholar] [CrossRef]
- Toseeb, U.; Asbury, K.; Code, A.; Fox, L.; Deniz, E. Supporting Families with Children with Special Educational Needs and Disabilities during COVID-19. PsyArXiv. Available online: https://psyarxiv.com/tm69k?fbclid=IwAR2Ryk8XavUyWwDUGCi9hGIIBdt3FUZMxFLKwVmSQAMhK99qD8WLnA2_JAE (accessed on 21 April 2020).
- Çelik, S.; Tomris, G.; Tuna, D. The COVID-19 pandemic: The evaluation of the emergency remote parent training program based on at-home support for children with down syndrome. Child. Youth Serv. Rev. 2022, 133, 106325. [Google Scholar] [CrossRef] [PubMed]
- Rababah, A.; Khlaifat, D.; Abdelfattah, F.; Busaad, Y.; Alqaryouti, I.; AlAwamleh, A. The Impact of Covid-19 on Parents of Children with Disability: Educational Needs and Challenges. Int. J. Instr. 2022, 15, 701–722. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).