3.1. Standardized Texture Levels
Dysphagia rehabilitation for stroke at Seirei Mikatahara General Hospital was started in 1989. When the dysphagia team realized the importance of dysphagia diets, 5-stage Seirei Dysphagia Diets were developed using sensory evaluations, videofluoroscopic examination of swallowing (VF) findings, and clinical observations. These diets were published in 1993 [
3], and later named as the “Dysphagia Diet Pyramid” by a team member, dietitian Ms. Setsuko Kanaya, in 2004 (personal communication) (
Figure 8).
The 5-stage Seirei Dysphagia Diets (Dysphagia Diet Pyramid) consist of five categories from L0 to L4: L0 is gelatin jelly (tea or fruit juice, etc.), L1 is gelatin jelly (miso soup, milk, etc., containing protein), L2 is gelatin jelly (mixer meal with gelatin), L3 is a puréed or mixer meal, and L4 is a softened diet. Gelatin jelly was mainly used in the first stage of swallowing training due to no better alternative at the time.
We evaluated the frequency of aspiration/penetration and pharyngeal residues among the different types of food of the 5-stage Seirei Dysphagia Diets using VF [
36]. A total of 121 patients with dysphagia (85 male and 36 female; average age: 72.7 ± 10.0 years) underwent VF. The cause of dysphagia was cerebral infarction in 46 patients (37%), aspiration pneumonia in 18 patients (15%), cerebral hemorrhage in 13 patients (11%), neuromuscular disease in 13 patients (11%), gastrointestinal disease in 8 patients (7%), and other in 23 patients (19%). The severity of dysphagia was determined by using the Food Intake Level Scale [
37]. VF was performed for six different types of food containing 40% barium sulfate: sliced and crushed gelatin, mildly and extremely thickened water, crushed agar jelly, and water. A xanthan gum-based thickener was used for thickening the water. The χ2 test and Fisher’s exact test were employed for statistical analysis. The significance level was corrected by Bonferroni correction for multiple comparisons, and p < 0.0033 was considered statistically significant.
Penetration/aspiration was markedly more frequent for thin water than for all other types of food (
Table 4) and was less frequent for sliced gelatin jelly without chewing than for crushed gelatin or agar jellies. Penetration/aspiration was also less frequent for extremely thickened water than for crushed gelatin, agar jellies, or mildly thickened water. Pharyngeal residue was remarkably lower for sliced gelatin and water than for mildly or extremely thickened water or crushed agar jelly (
Table 5). These results suggested that sliced gelatin jelly was the safest type of food for dysphagia patients, followed next by extremely thickened water. Based on these findings, the Dysphagia Diet Pyramid was judged as valid and has since been widely adopted in Japan.
Figure 9 shows the tendency of aspiration and pharyngeal residue among different types of food.
Although the Dysphagia Diet Pyramid became widely known in Japan, several other kinds of dysphagia diets existed at various institutions nationwide. To avoid confusion, a standardized dysphagia diet system was needed for patients, their families, and medical staff in the patient care network. Especially, a uniform name was required. We organized a special committee for a modified dysphagia diet system in the JSDR in 2010 to categorize the levels of modified foods and thickened liquids. The special committee developed “The tentative draft of 5-stage modified dysphagia diet” in 2011 and “The standard draft of Japanese Dysphagia Diet 2012” in 2012 and published them on paper and on the website. Public and professional feedback culminated in the JDD2013 consisting of a precise explanation text and tables for food and liquid [
38].
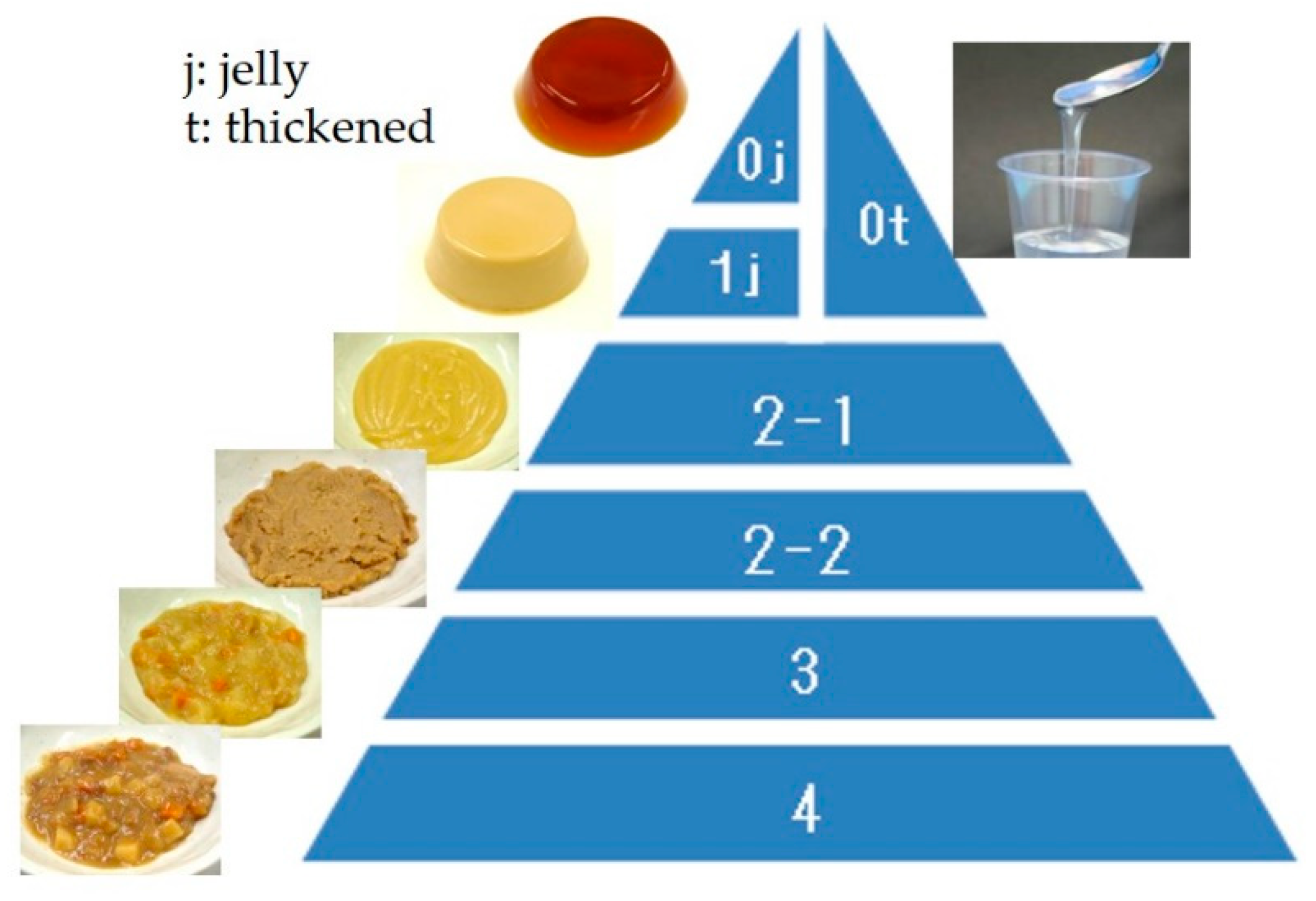
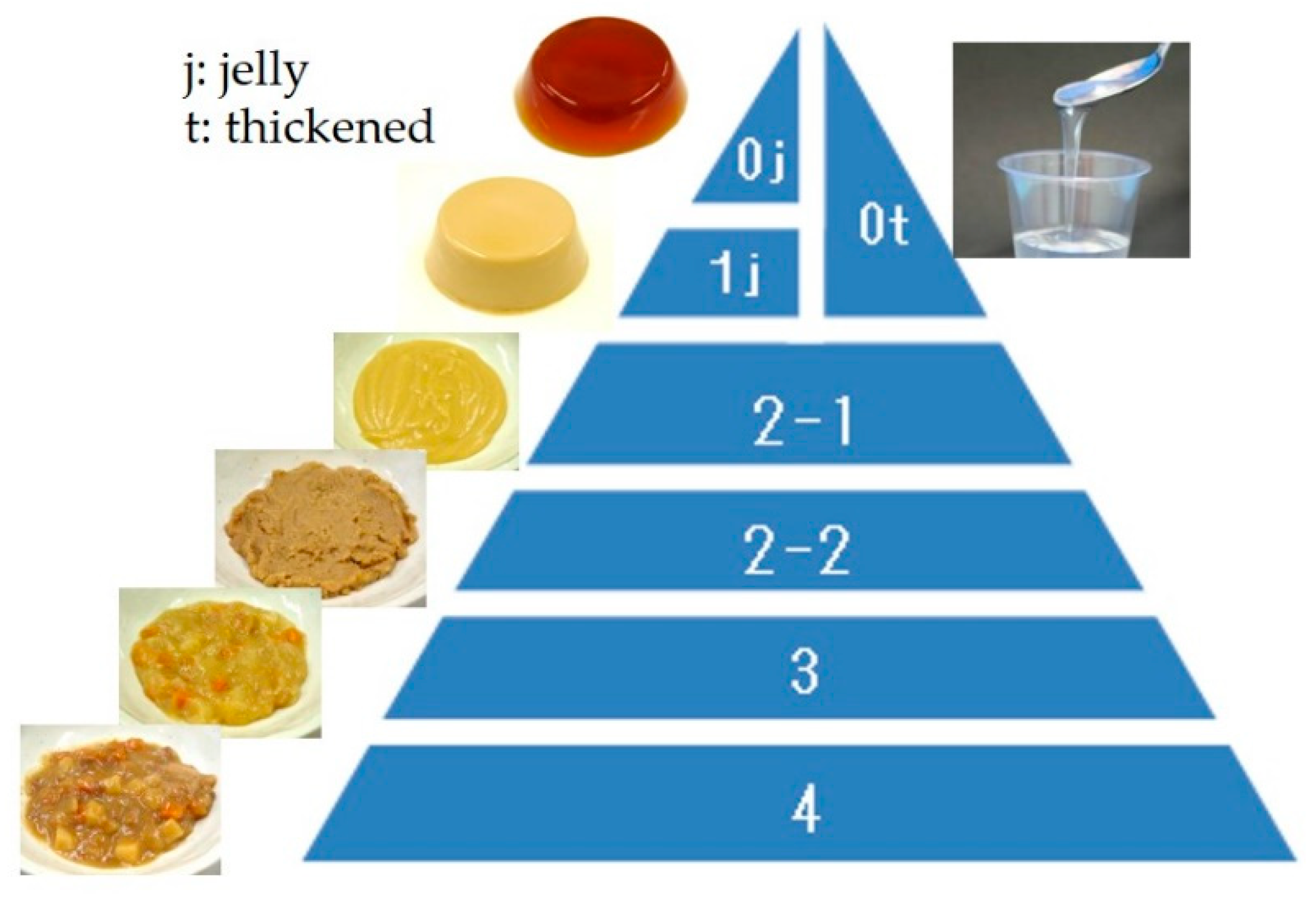
The JDD2013 consists of five categories (
Figure 10). Code 0j is swallow-training jelly, which can be placed directly in the mouth and swallowed without chewing (i.e., can be swallowed whole). Considering infection and tissue reactions to pulmonary aspiration, protein content is kept low. Code 0t is thickened liquid, which applies to tea or fruit juice thickened with a thickening-adjustment food. If the food contains protein, it is considered Code 1j. Code 1j is a jelly/pudding/mousse-like food product that does not require abilities related to chewing. It is homogeneous and soft, with little syneresis. Code 2 is food in the form of a paste that is sub-classified into 2-1 or 2-2 based on heterogeneity. Code 2-1 is food with smooth and homogeneous materials under 850 μm, while Code 2-2 is for inhomogeneous materials containing soft grains (i.e., a blender diet). Typically, Code 2 foods are considered blender, mixer, puréed, or paste foods. Code 3 food contains solid forms, which can be crushed even without teeth into a bolus. Code 4 food can be handled with teeth and is difficult to crush between the tongue and palate. Some general foods of not too hard, not too sticky, and not too crumbly are classified into this category. JDD2013 did not determine the physical property evaluation so that it can be used by general clinicians. However, since JDD2013 and Dysphagia Diet Pyramid are compatible [
38], measured variables in the Dysphagia Diet Pyramid are shown in
Table 6 as the references [
39,
40].
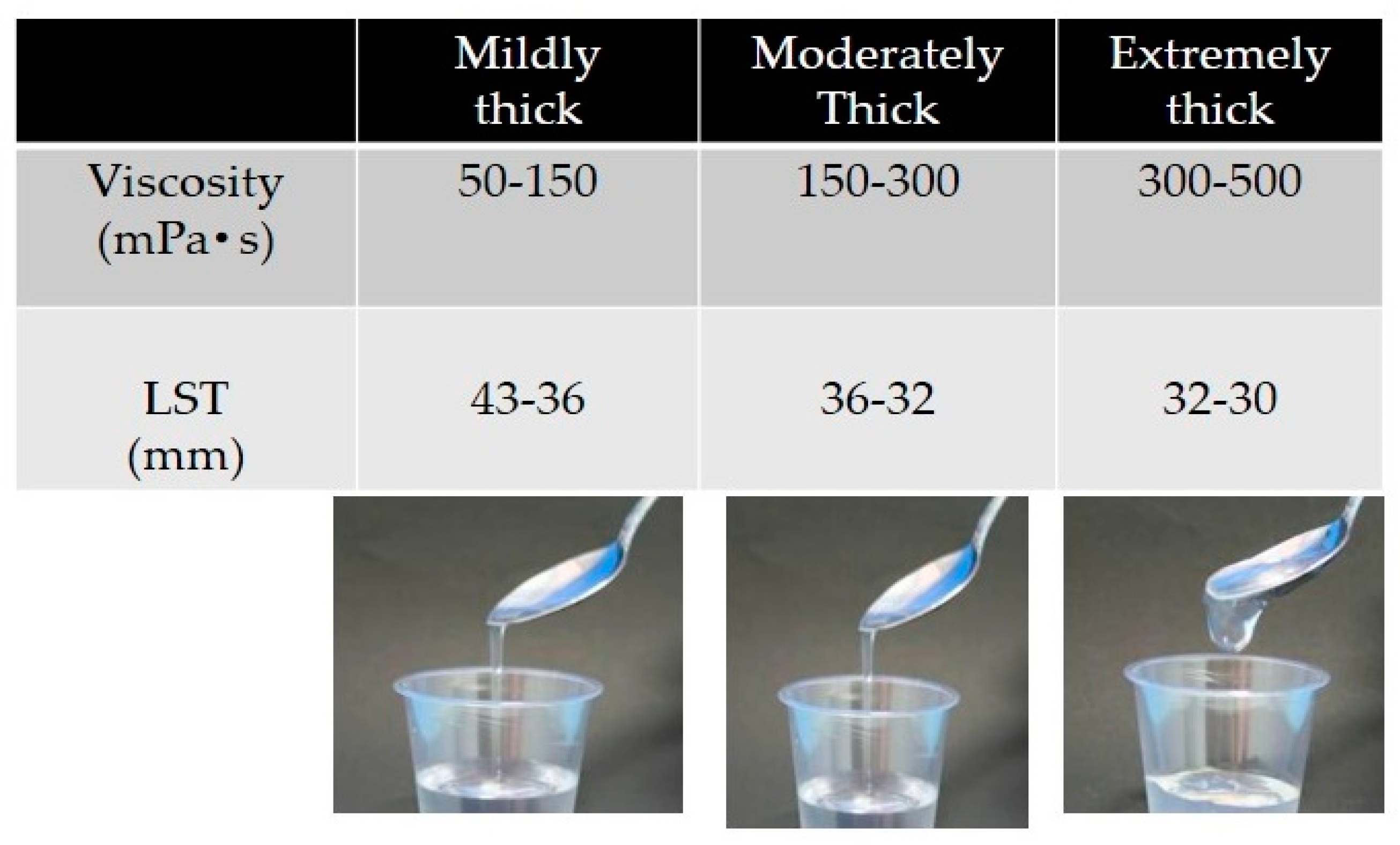
Liquids are thickened by a xanthan gum-based thickener and are divided into three categories: mildly, moderately, and extremely thick (
Figure 11) [
41]. Mildly thick liquids flow quickly by tilting the spoon and leave a thin trace of residue in the cup after poured. They are suitable for patients with mild dysphagia. Moderately thick liquids flow slowly by tilting the spoon and leave a film of residue in the cup after being poured. They are appropriate for patients with moderately severe dysphagia. Extremely thick liquids maintain most of their form after tilting the spoon and flow slowly while being poured. They are suitable for patients with more severe dysphagia who display a risk of aspiration using moderately thick liquids. Viscosity levels are 50–150 mPa·s for mildly thick, 150–300 mPa·s for moderately thick, and 300–500 mPa·s for extremely thick liquids, with a Viscometer share rate of 50 sec
−1.
3.2. Assessment of Proper Texture for Patients with Oral Dysphagia
When starting dysphagia therapy, two critical conditions require verification: patient’s conscious level is clear and his or her general condition is stable (i.e., normal vital signs and respiration, no cough or excess sputum). The oral cavity should first be cleaned. For screening, we use the 3 mL and/or 30 mL water swallow test with/without liquid thickener and the Repetitive Saliva Swallow Test (RSST) (three times or more is normal). If there are no problems, we commence meals with a normal diet. If a problem is found, we begin a dysphagia diet with close observation. Instrumental examination is performed for difficult cases. Our basis for applying direct therapy is safe swallowing and errorless training, as depicted in
Figure 12.
The key to successful dysphagia rehabilitation is the choice of proper food and body position and the use of rehabilitation techniques to enable no aspiration and residue-free eating training. The combination of these 3 elements is important (
Figure 13). We use VF and/or videoendscopic examination of swallowing (VE) to select the most suitable food for the patient’s swallowing function status, and conduct direct swallowing training in an easy-to-eat posture using rehabilitation techniques. Such step-by-step safe feeding training leads to improvements in swallowing function.
Food texture is essential in dysphagia rehabilitation. We discussed swallowing bolus texture from two key aspects: the textural change of solid food by mastication and the current standardized definition of food texture in Japan. Since mastication changes the texture of ingested food dramatically, understanding masticatory mechanism and its influencing factors is important to provide dysphagia diet. As standardized criteria for classifying the texture of food and liquid are essential as well, we introduced the Japanese Dysphagia Diet 2013 that is commonly used as the standardized index for dysphagia diets in Japan.














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}