
Sexual Dimorphism in Body Weight Loss, Improvements in Cardiometabolic Risk Factors and Maintenance of Beneficial Effects 6 Months after a Low-Calorie Diet: Results from the Randomized Controlled DiOGenes Trial

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
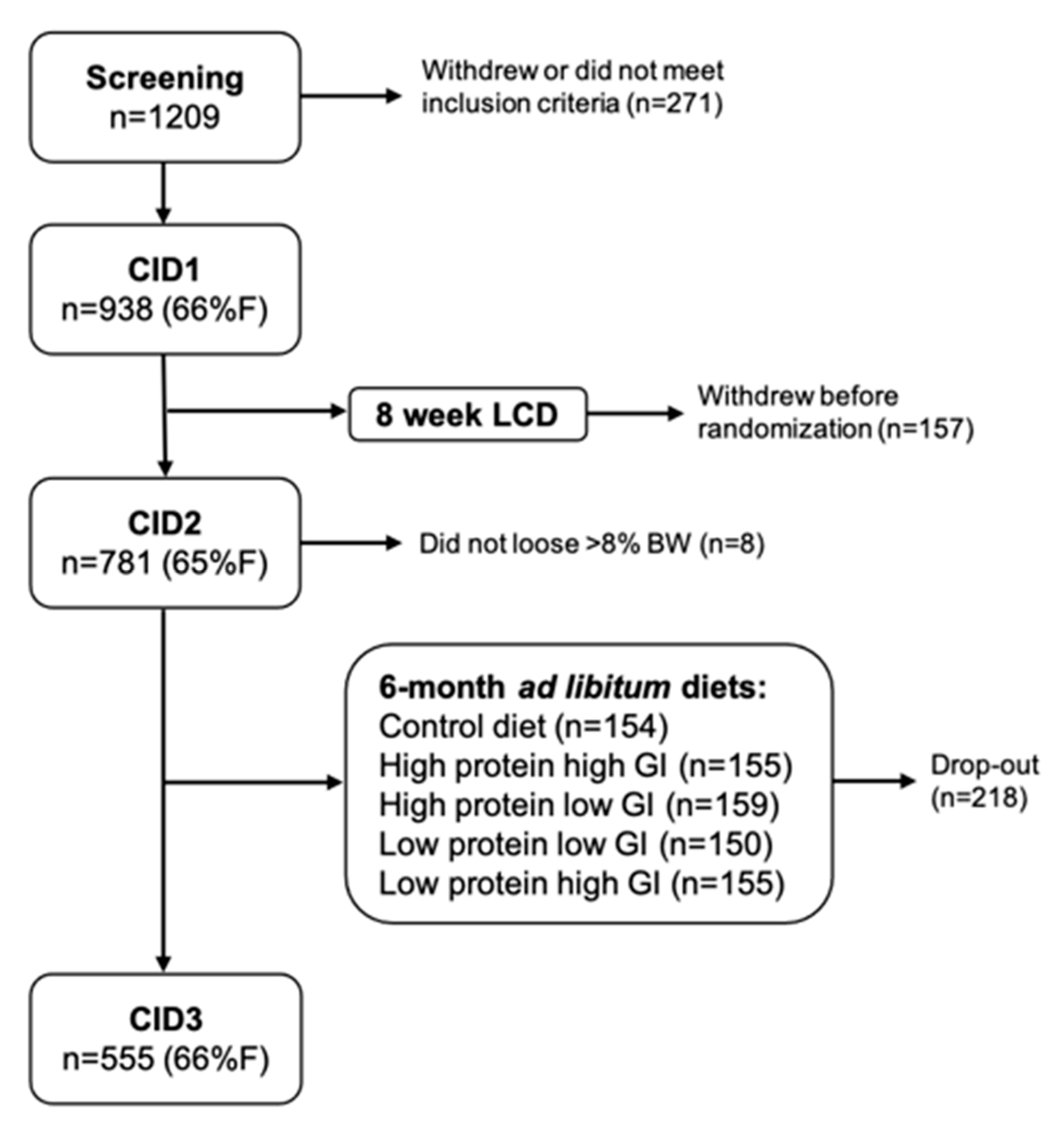
2.1. Study Design and Population
2.2. Clinical Visits
2.3. Biochemical Analysis
2.4. Insulin Sensitivity
2.5. Plasma Lipidomics
2.6. Statistical Analysis
3. Results
3.1. Clinical Characteristics of the Study Population
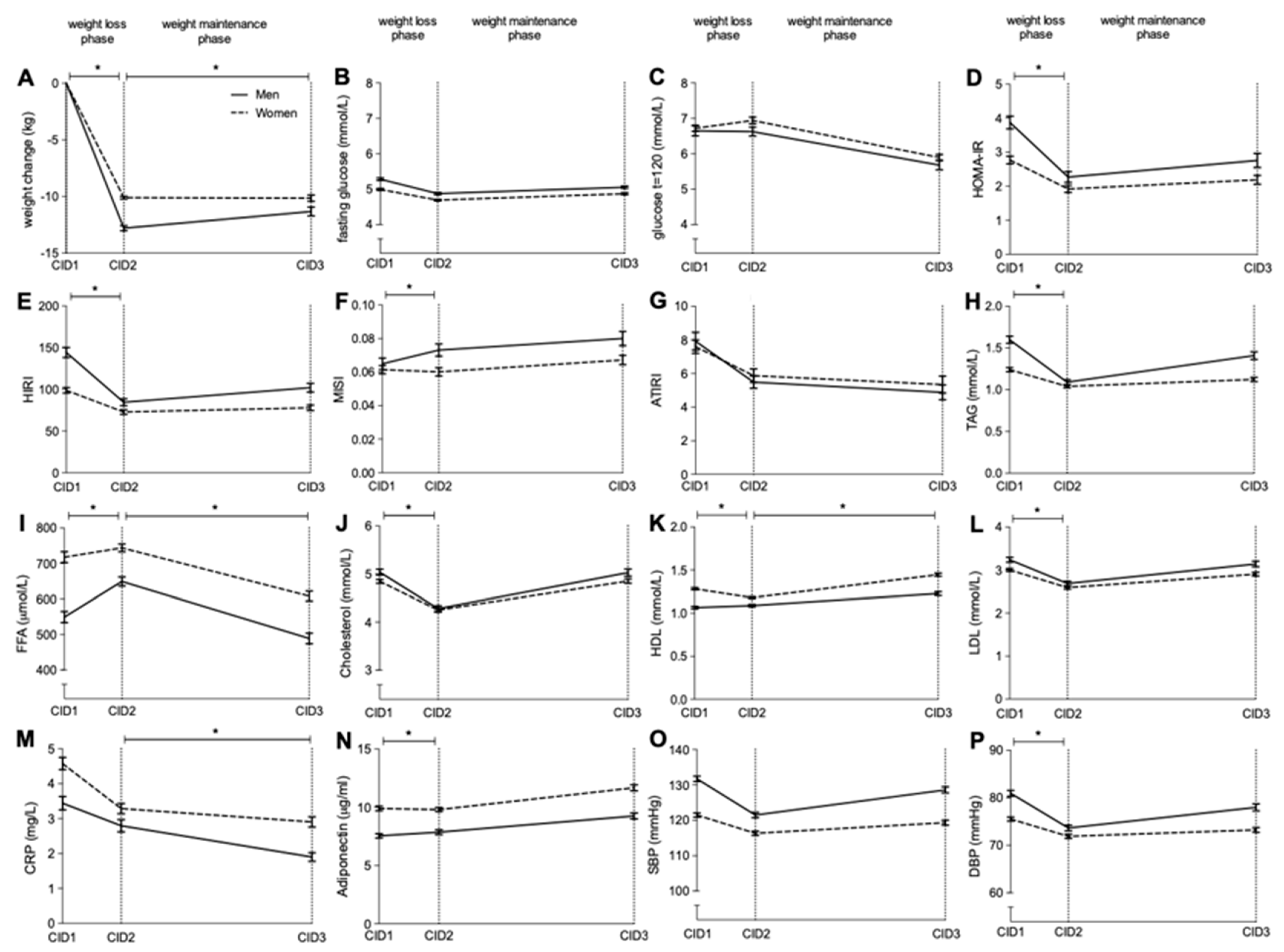
3.2. Weight Change Following LCD
3.3. Changes in Insulin Sensitivity Following Weight Loss
3.4. Changes in Lipid Profile and Blood Pressure Following Weight Loss
3.5. Changes in Plasma Lipidome Profile Following Weight Loss
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jastreboff, A.M.; Kotz, C.M.; Kahan, S.; Kelly, A.S.; Heymsfield, S.B. Obesity as a Disease: The Obesity Society 2018 Position Statement. Obesity 2019, 27, 7–9. [Google Scholar] [CrossRef]
- Bray, G.; Frühbeck, G.; Ryan, D.H.; Wilding, J.P.H. Management of obesity. Lancet 2016, 387, 1947–1956. [Google Scholar] [CrossRef]
- Anderson, J.W.; Konz, E.C.; Frederich, R.C.; Wood, C.L. Long-term weight-loss maintenance: A meta-analysis of US studies. Am. J. Clin. Nutr. 2001, 74, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Goossens, G.H.; Jocken, J.W.E.; Blaak, E.E. Sexual dimorphism in cardiometabolic health: The role of adipose tissue, muscle and liver. Nat. Rev. Endocrinol. 2021, 17, 47–66. [Google Scholar] [CrossRef]
- Meyer, A.; Montastier, E.; Hager, J.; Saris, W.H.M.; Astrup, A.; Viguerie, N.; Valsesia, A. Plasma metabolites and lipids predict insulin sensitivity improvement in obese, nondiabetic individuals after a 2-phase dietary intervention. Am. J. Clin. Nutr. 2018, 108, 13–23. [Google Scholar] [CrossRef]
- Geer, E.B.; Shen, W. Gender differences in insulin resistance, body composition, and energy balance. Gend. Med. 2009, 6, 60–75. [Google Scholar] [CrossRef]
- Goossens, G.H. The Metabolic Phenotype in Obesity: Fat Mass, Body Fat Distribution, and Adipose Tissue Function. Obes. Facts 2017, 10, 207–215. [Google Scholar] [CrossRef]
- Karpe, F.; Pinnick, K.E. Biology of upper-body and lower-body adipose tissue—link to whole-body phenotypes. Nat. Rev. Endocrinol. 2015, 11, 90–100. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Magkos, F.; Mittendorfer, B. Sex differences in lipid and lipoprotein metabolism: It’s not just about sex hormones. J. Clin. Endocrinol. Metab. 2011, 96, 885–893. [Google Scholar] [CrossRef] [PubMed]
- van der Kolk, B.W.; Vogelzangs, N.; Jocken, J.W.E.; Valsesia, A.; Hankemeier, T.; Astrup, A.; Saris, W.H.M.; Arts, I.C.W.; van Greevenbroek, M.M.J.; Blaak, E.E.; et al. Plasma lipid profiling of tissue-specific insulin resistance in human obesity. Int. J. Obes. 2019, 43, 989–998. [Google Scholar] [CrossRef]
- Valsesia, A.; Saris, W.H.; Astrup, A.; Hager, J.; Masoodi, M. Distinct lipid profiles predict improved glycemic control in obese, nondiabetic patients after a low-caloric diet intervention: The Diet, Obesity and Genes randomized trial. Am. J. Clin. Nutr. 2016, 104, 566–575. [Google Scholar] [CrossRef]
- Wadden, T.A.; Neiberg, R.H.; Wing, R.R.; Clark, J.M.; Delahanty, L.M.; Hill, J.O.; Krakoff, J.; Otto, A.; Ryan, D.H.; Vitolins, M.Z.; et al. Four-Year Weight Losses in the Look AHEAD Study: Factors Associated with Long-Term Success. Obesity 2011, 19, 1987–1998. [Google Scholar] [CrossRef]
- Christensen, P.; Larsen, T.M.; Westerterp-Plantenga, M.; Macdonald, I.; Martinez, J.A.; Handjiev, S.; Poppitt, S.; Hansen, S.; Ritz, C.; Astrup, A.; et al. Men and women respond differently to rapid weight loss: Metabolic outcomes of a multi-centre intervention study after a low-energy diet in 2500 overweight, individuals with pre-diabetes (PREVIEW). Diabetes Obes. Metab. 2018, 20, 2840–2851. [Google Scholar] [CrossRef] [PubMed]
- Navas-Carretero, S.; Holst, C.; Saris, W.H.; Van Baak, M.A.; Jebb, S.A.; Kafatos, A.; Papadaki, A.; Pfeiffer, A.F.H.; Handjieva-Darlenska, T.; Hlavaty, P.; et al. The Impact of Gender and Protein Intake on the Success of Weight Maintenance and Associated Cardiovascular Risk Benefits, Independent of the Mode of Food Provision: The DiOGenes Randomized Trial. J. Am. Coll. Nutr. 2016, 35, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Trouwborst, I.; Bowser, S.M.; Goossens, G.H.; Blaak, E.E. Ectopic Fat Accumulation in Distinct Insulin Resistant Phenotypes; Targets for Personalized Nutritional Interventions. Front. Nutr. 2018, 5, 77. [Google Scholar] [CrossRef] [PubMed]
- Larsen, T.M.; Dalskov, S.; Van Baak, M.; Jebb, S.; Kafatos, A.; Pfeiffer, A.; Martinez, J.A.; Handjieva-Darlenska, T.; Kuneå¡ovã¡, M.; Holst, C.; et al. The Diet, Obesity and Genes (Diogenes) Dietary Study in eight European countries a comprehensive design for long-term intervention. Obes. Rev. 2009, 11, 76–91. [Google Scholar] [CrossRef] [PubMed]
- Larsen, T.M.; Dalskov, S.-M.; Van Baak, M.; Jebb, S.A.; Papadaki, A.; Pfeiffer, A.F.; Martinez, J.A.; Handjieva-Darlenska, T.; Kunešová, M.; Pihlsgård, M.; et al. Diets with High or Low Protein Content and Glycemic Index for Weight-Loss Maintenance. N. Engl. J. Med. 2010, 363, 2102–2113. [Google Scholar] [CrossRef]
- Baecke, J.; Burema, J.; Frijters, J.E. A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am. J. Clin. Nutr. 1982, 36, 936–942. [Google Scholar] [CrossRef]
- Abdul-Ghani, M.A.; Matsuda, M.; Balas, B.; DeFronzo, R.A. Muscle and Liver Insulin Resistance Indexes Derived from the Oral Glucose Tolerance Test. Diabetes Care 2006, 30, 89–94. [Google Scholar] [CrossRef]
- Vogelzangs, N.; The Diogenes Consortium; Van Der Kallen, C.J.H.; Van Greevenbroek, M.M.J.; Van Der Kolk, B.W.; Jocken, J.W.E.; Goossens, G.H.; Schaper, N.C.; Henry, R.M.A.; Eussen, S.J.P.M.; et al. Metabolic profiling of tissue-specific insulin resistance in human obesity: Results from the Diogenes study and the Maastricht Study. Int. J. Obes. 2020, 44, 1376–1386. [Google Scholar] [CrossRef] [PubMed]
- Gastaldelli, A.; Gaggini, M.; DeFronzo, R.A. Role of Adipose Tissue Insulin Resistance in the Natural History of Type 2 Diabetes: Results from the San Antonio Metabolism Study. Diabetes 2017, 66, 815–822. [Google Scholar] [CrossRef]
- Valsesia, A.; Chakrabarti, A.; Hager, J.; Langin, D.; Saris, W.H.M.; Astrup, A.; Blaak, E.E.; Viguerie, N.; Masoodi, M. Integrative phenotyping of glycemic responders upon clinical weight loss using multi-omics. Sci. Rep. 2020, 10, 1–14. [Google Scholar] [CrossRef]
- Hu, C.; van Dommelen, J.; van der Heijden, R.; Spijksma, G.; Reijmers, T.H.; Wang, M.; Slee, E.; Lu, X.; Xu, G.; van der Greef, J.; et al. RPLC-Ion-Trap-FTMS Method for Lipid Profiling of Plasma: Method Validation and Application to p53 Mutant Mouse Model. J. Proteome Res. 2008, 7, 4982–4991. [Google Scholar] [CrossRef] [PubMed]
- Szymańska, E.; van Dorsten, F.A.; Troost, J.; Paliukhovich, I.; van Velzen, E.J.J.; Hendriks, M.M.W.B.; Trautwein, E.A.; van Duynhoven, J.P.M.; Vreeken, R.J.; Smilde, A.K. A lipidomic analysis approach to evaluate the response to cholesterol-lowering food intake. Metabolomics 2012, 8, 894–906. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hjorth, M.F.; Ritz, C.; Blaak, E.; Saris, W.H.; Langin, D.; Poulsen, S.K.; Larsen, T.M.; Sørensen, T.I.; Zohar, Y.; Astrup, A. Pretreatment fasting plasma glucose and insulin modify dietary weight loss success: Results from 3 randomized clinical trials. Am. J. Clin. Nutr. 2017, 106, 499–505. [Google Scholar] [CrossRef]
- Berger, S.E.; Huggins, G.S.; McCaffery, J.M.; Jacques, P.F.; Lichtenstein, A.H. Change in Cardiometabolic Risk Factors Associated with Magnitude of Weight Regain 3 Years After a 1-Year Intensive Lifestyle Intervention in Type 2 Diabetes Mellitus: The Look AHEAD Trial. J. Am. Hear. Assoc. 2019, 8, e010951. [Google Scholar] [CrossRef]
- Vistisen, B.; Hellgren, L.; Vadset, T.; Scheede-Bergdahl, C.; Helge, J.W.; Dela, F.; Stallknecht, B.M. Effect of gender on lipid-induced insulin resistance in obese subjects. Eur. J. Endocrinol. 2008, 158, 61–68. [Google Scholar] [CrossRef]
- Frias, J.P.; Macaraeg, G.B.; Ofrecio, J.; Yu, J.G.; Olefsky, J.M.; Kruszynska, Y.T. Decreased Susceptibility to Fatty Acid–Induced Peripheral Tissue Insulin Resistance in Women. Diabetes 2001, 50, 1344–1350. [Google Scholar] [CrossRef]
- Schorr, M.; Dichtel, L.E.; Gerweck, A.V.; Valera, R.D.; Torriani, M.; Miller, K.K.; Bredella, M.A. Sex differences in body composition and association with cardiometabolic risk. Biol. Sex Differ. 2018, 9, 28. [Google Scholar] [CrossRef]
- Gasteyger, C.; Larsen, T.M.; Vercruysse, F.; Pedersen, D.; Toubro, S.; Astrup, A. Visceral fat loss induced by a low-calorie diet: A direct comparison between women and men. Diabetes, Obes. Metab. 2009, 11, 596–602. [Google Scholar] [CrossRef] [PubMed]
- Wirth, A.; Steinmetz, B. Gender Differences in Changes in Subcutaneous and Intra-abdominal Fat during Weight Reduction: An Ultrasound Study. Obes. Res. 1998, 6, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Machann, J.; Thamer, C.; Stefan, N.; Schwenzer, N.F.; Kantartzis, K.; Häring, H.-U.; Claussen, C.D.; Fritsche, A.; Schick, F. Follow-up Whole-Body Assessment of Adipose Tissue Compartments during a Lifestyle Intervention in a Large Cohort at Increased Risk for Type 2 Diabetes. Radiology 2010, 257, 353–363. [Google Scholar] [CrossRef]
- Bosy-Westphal, A.; Schautz, B.; Lagerpusch, M.; Pourhassan, M.; Braun, W.; Goele, K.; Heller, M.; Glüer, C.-C.; Müller, M.J. Effect of weight loss and regain on adipose tissue distribution, composition of lean mass and resting energy expenditure in young overweight and obese adults. Int. J. Obes. 2013, 37, 1371–1377. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.; Kim, D.; Kim, J.S. Body Fat Distribution and the Risk of Incident Metabolic Syndrome: A Longitudinal Cohort Study. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef]
- Lee, M.-J.; Wu, Y.; Fried, S.K. Adipose tissue heterogeneity: Implication of depot differences in adipose tissue for obesity complications. Mol. Asp. Med. 2013, 34, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Virtue, S.; Vidal-Puig, A. Adipose tissue expandability, lipotoxicity and the Metabolic SyndromeߞAn allostatic perspective. Biochim. Biophys. Acta 2010, 1801, 338–349. [Google Scholar] [CrossRef]
- Ibrahim, M.M. Subcutaneous and visceral adipose tissue: Structural and functional differences. Obes. Rev. 2010, 11, 11–18. [Google Scholar] [CrossRef]
- Jensen, M.D. Is Visceral Fat Involved in the Pathogenesis of the Metabolic Syndrome? Human Model. Obesity 2006, 14, 20S–24S. [Google Scholar] [CrossRef]
- Barber, M.N.; Risis, S.; Yang, C.; Meikle, P.J.; Staples, M.; Febbraio, M.A.; Bruce, C.R. Plasma Lysophosphatidylcholine Levels Are Reduced in Obesity and Type 2 Diabetes. PLoS ONE 2012, 7, e41456. [Google Scholar] [CrossRef]
- Rauschert, S.; Uhl, O.; Koletzko, B.; Mori, T.A.; Beilin, L.J.; Oddy, W.H.; Hellmuth, C. Sex differences in the association of phospholipids with components of the metabolic syndrome in young adults. Biol. Sex Differ. 2017, 8, 1–13. [Google Scholar] [CrossRef]
- Hannun, Y.A.; Obeid, L.M. Sphingolipids and their metabolism in physiology and disease. Nat. Rev. Mol. Cell Biol. 2018, 19, 175–191. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| n | Men | Women | Total Group | p-Value | |
|---|---|---|---|---|---|
| Sex (%) | 782 | 35.3 | 64.7 * | 100 | <0.001 |
| Age (years) | 782 | 42.5 ± 6.0 | 41.0 ± 6.3 * | 41.5 ± 6.26 | 0.001 |
| BMI (kg/m2) | 782 | 34.3 ± 0.5 | 34.5 ± 5.0 | 34.4 ± 4.9 | 0.108 |
| Body weight (kg) | |||||
| CID1 | 782 | 109.3 ± 17.4 | 95.0 ± 15.6 * | 100.1 ± 17.6 | <0.001 |
| Weight loss CID2-CID1 | 782 | −12.8 ± 3.9 | −10.1 ± 2.8 * | −11.0 ± 3.50 | <0.001 |
| Weight maintenance CID3-CID2 | 555 | 1.6 ± 5.3 | −0.5 ± 5.5 * | 0.5 ± 5.48 | <0.001 |
| Physical activity (Baecke) | 718 | 7.9 ± 0.9 | 8.0 ± 0.9 | 8.0 ± 0.9 | 0.090 |
| Waist:hip ratio | 769 | 1.01 ± 0.05 | 0.88 ± 0.07 * | 0.92 ± 0.09 | <0.001 |
| Systolic BP (mmHg) | 758 | 132.0 ± 12.8 | 121.9 ± 14.4 * | 118.2 ± 13.3 | <0.001 |
| Diastolic BP (mmHg) | 758 | 81.4 ± 10.6 | 75.9 ± 10.6 * | 72.49 ± 9.72 | <0.001 |
| Fasting glucose (mmol/L) | 749 | 5.27 ± 0.62 | 5.00 ± 0.66 * | 5.10 ± 0.66 | <0.001 |
| 2 hr glucose (mmol/L) | 741 | 6.58 ± 2.37 | 6.74 ± 2.02 | 6.68 ± 2.16 | 0.333 |
| Fasting insulin (μIU/mL) | 723 | 13.9 ± 11.3 | 10.5 ± 9.4 * | 11.7 ± 10.3 | <0.001 |
| HOMA-IR (A.U.) | 733 | 3.87 ± 3.23 | 2.77 ± 2.64 * | 3.16 ± 2.91 | <0.001 |
| MISI (A.U.) | 649 | 0.063 ± 0.052 | 0.060 ± 0.052 | 0.061 ± 0.052 | 0.488 |
| HIRI (A.U.) | 686 | 144.8 ± 101.8 | 98.9 ± 76.0 * | 115.9 ± 89.1 | <0.001 |
| ATIRI (A.U.) | 720 | 7.92 ± 8.95 | 7.69 ± 8.38 | 7.72 ± 8.61 | 0.625 |
| Total cholesterol (mmol/L) | 768 | 5.05 ± 1.08 | 4.84 ± 0.96 * | 4.92 ± 1.01 | 0.008 |
| HDL cholesterol (mmol/L) | 770 | 1.07 ± 0.28 | 1.29 ± 0.33 * | 1.21 ± 0.33 | <0.001 |
| LDL cholesterol (mmol/L) | 764 | 3.24 ± 0.93 | 3.00 ± 0.84 * | 3.08 ± 0.88 | <0.001 |
| TAG (mmol/L) | 759 | 1.60 ± 0.70 | 1.23 ± 0.57 * | 1.36 ± 0.64 | <0.001 |
| FFA (μmol/L) | 672 | 552.3 ± 281.6 | 711.54 ± 326.7 * | 646.8 ± 318.7 | <0.001 |
| C-reactive protein (mg/L) | 747 | 3.78 ± 3.18 | 4.54 ± 4.13 * | 4.12 ± 3.86 | <0.001 |
| Adiponectin (μg/mL) | 768 | 7.46 ± 3.17 | 9.96 ± 4.71 * | 9.08 ± 4.40 | <0.001 |
| Men (n = 258) | Women (n = 474) | Total Group (n = 732) | p-Value | |
|---|---|---|---|---|
| TAG | 50.9 ± 8.2 | 44.8 ± 8.9 * | 47.0 ± 9.2 | <0.001 |
| Odd | 5.7 ± 1.1 | 6.4 ± 1.3 * | 6.2 ± 1.3 | <0.001 |
| even | 94.3 ± 1.1 | 93.6 ± 1.3 * | 93.8 ± 1.3 | <0.001 |
| Sat | 2.5 ± 1.1 | 2.3 ± 1.0 * | 2.4 ± 1.07 | 0.022 |
| Usat | 76.0 ± 5.2 | 76.2 ± 5.6 | 76.1 ± 5.4 | 0.649 |
| Psat | 21.5 ± 5.7 | 21.5 ± 6.0 | 21.5 ± 5.9 | 0.992 |
| Long | 95.6 ± 1.2 | 95.9 ± 1.3 * | 95.8 ± 1.3 | 0.004 |
| very long | 4.4 ± 1.2 | 4.1 ± 1.3 * | 4.2 ± 1.3 | 0.004 |
| DAG | 0.040 ± 0.014 | 0.037 ± 0.015 * | 0.038 ± 0.015 | 0.047 |
| CholE | 0.13 ± 0.04 | 0.15 ± 0.04 * | 0.14 ± 0.04 | <0.001 |
| LPC | 5.7 ± 1.5 | 5.8 ± 1.8 | 5.8 ± 1.7 | 0.758 |
| LPCO | 0.035 ± 0.011 | 0.037 ± 0.014 | 0.036 ± 0.013 | 0.098 |
| LPE | 0.033 ± 0.014 | 0.037 ± 0.018 * | 0.036 ± 0.013 | 0.003 |
| PC | 34.1 ± 5.4 | 38.6 ± 5.9 * | 37.0 ± 6.1 | <0.001 |
| PCO | 1.33 ± 0.42 | 1.45 ± 0.43 * | 1.40 ± 0.43 | <0.001 |
| PE | 1.73 ± 0.43 | 2.08 ± 0.50 * | 1.95 ± 0.51 | <0.001 |
| PEO | 0.37 ± 0.15 | 0.34 ± 0.12 * | 0.35 ± 0.13 | 0.047 |
| SM | 5.6 ± 1.4 | 6.6 ± 1.7 * | 6.3 ± 1.6 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trouwborst, I.; Goossens, G.H.; Astrup, A.; Saris, W.H.M.; Blaak, E.E. Sexual Dimorphism in Body Weight Loss, Improvements in Cardiometabolic Risk Factors and Maintenance of Beneficial Effects 6 Months after a Low-Calorie Diet: Results from the Randomized Controlled DiOGenes Trial. Nutrients 2021, 13, 1588. https://doi.org/10.3390/nu13051588
Trouwborst I, Goossens GH, Astrup A, Saris WHM, Blaak EE. Sexual Dimorphism in Body Weight Loss, Improvements in Cardiometabolic Risk Factors and Maintenance of Beneficial Effects 6 Months after a Low-Calorie Diet: Results from the Randomized Controlled DiOGenes Trial. Nutrients. 2021; 13(5):1588. https://doi.org/10.3390/nu13051588
Chicago/Turabian StyleTrouwborst, Inez, Gijs H. Goossens, Arne Astrup, Wim H. M. Saris, and Ellen E. Blaak. 2021. "Sexual Dimorphism in Body Weight Loss, Improvements in Cardiometabolic Risk Factors and Maintenance of Beneficial Effects 6 Months after a Low-Calorie Diet: Results from the Randomized Controlled DiOGenes Trial" Nutrients 13, no. 5: 1588. https://doi.org/10.3390/nu13051588
APA StyleTrouwborst, I., Goossens, G. H., Astrup, A., Saris, W. H. M., & Blaak, E. E. (2021). Sexual Dimorphism in Body Weight Loss, Improvements in Cardiometabolic Risk Factors and Maintenance of Beneficial Effects 6 Months after a Low-Calorie Diet: Results from the Randomized Controlled DiOGenes Trial. Nutrients, 13(5), 1588. https://doi.org/10.3390/nu13051588