
Prognostic Value of the Controlling Nutritional Status (CONUT) Score in Patients at Dialysis Initiation


 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Data Collection and Measurements
2.3. Follow-Up Study
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Prognostic Value of the CONUT Score
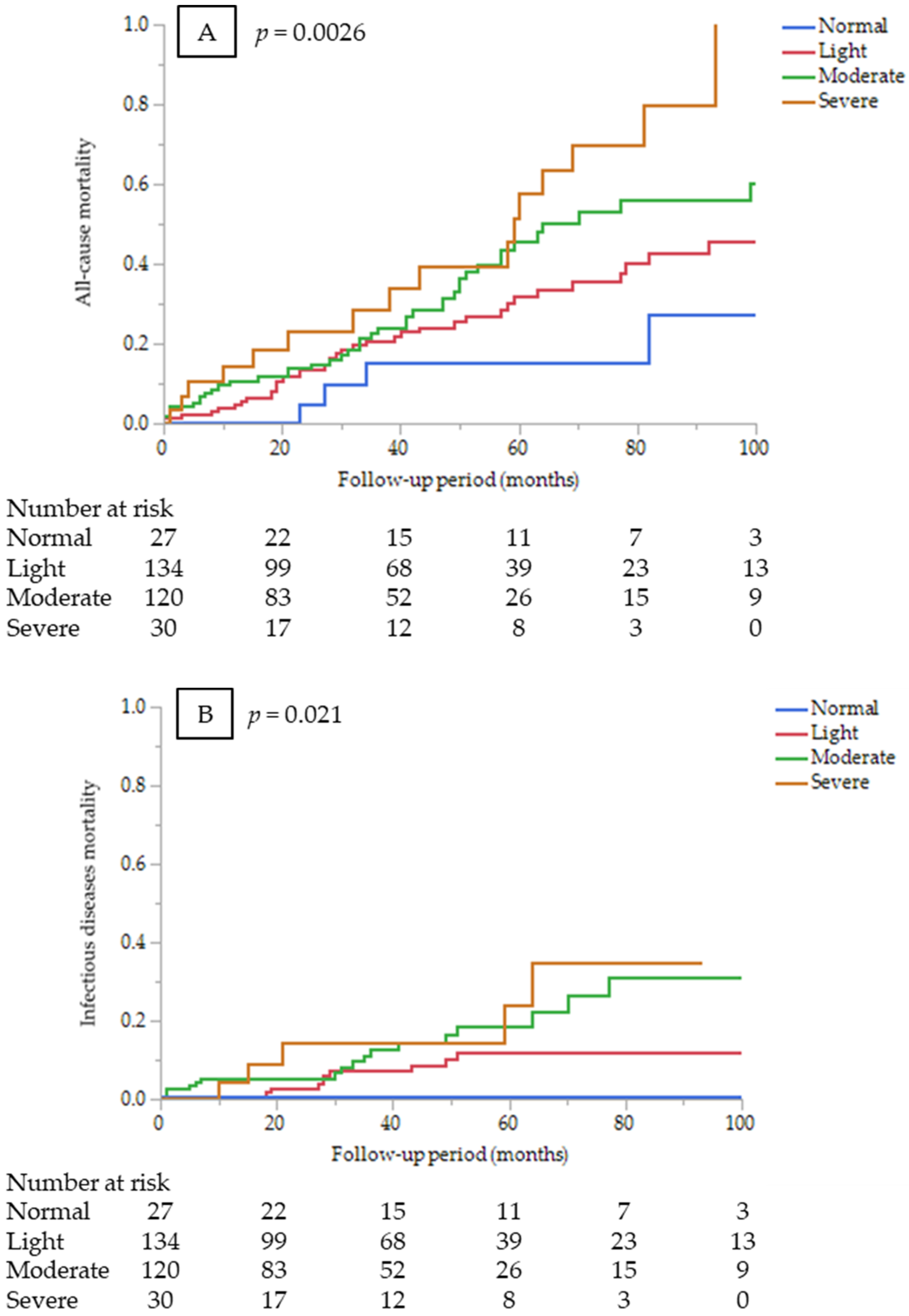
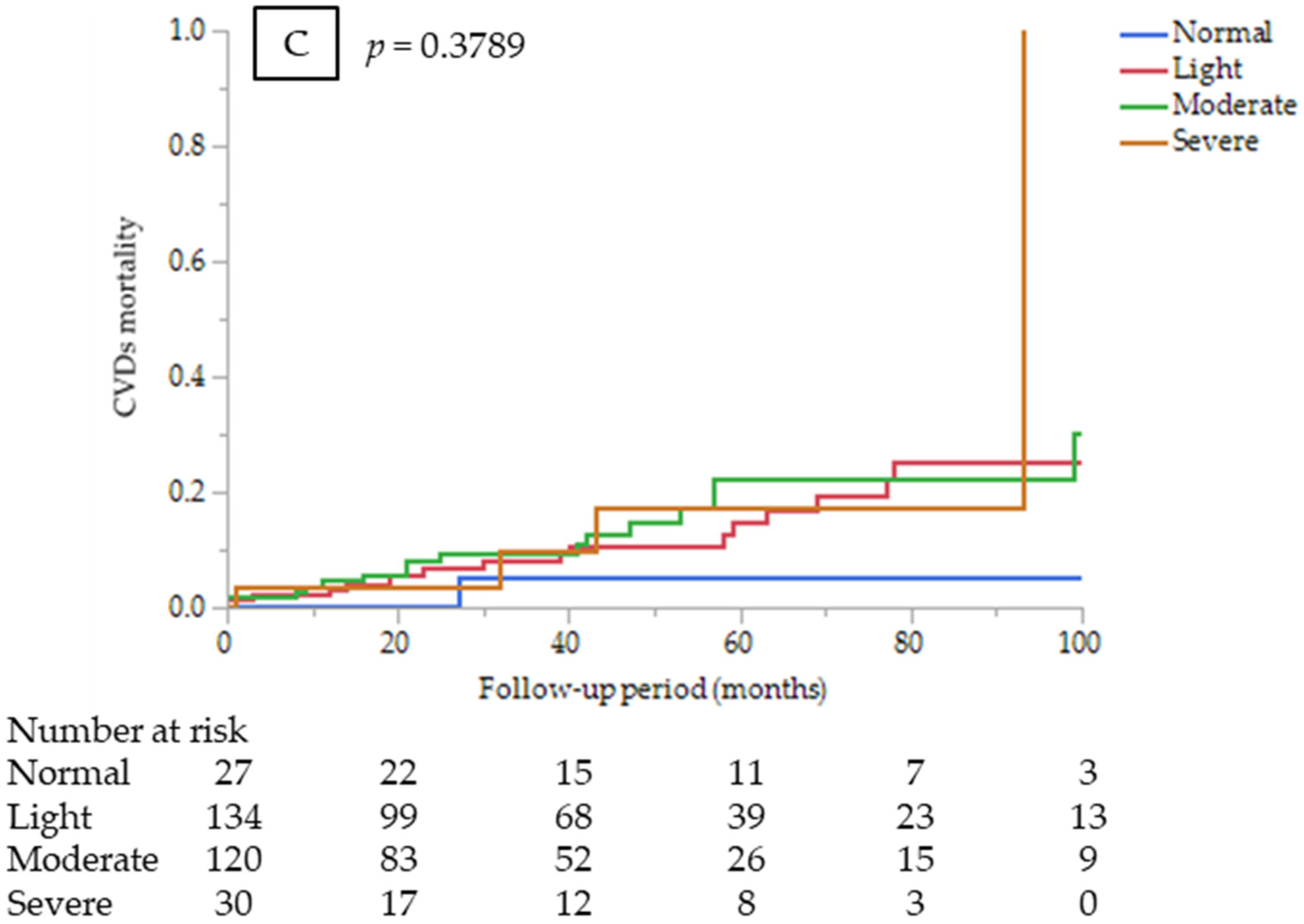
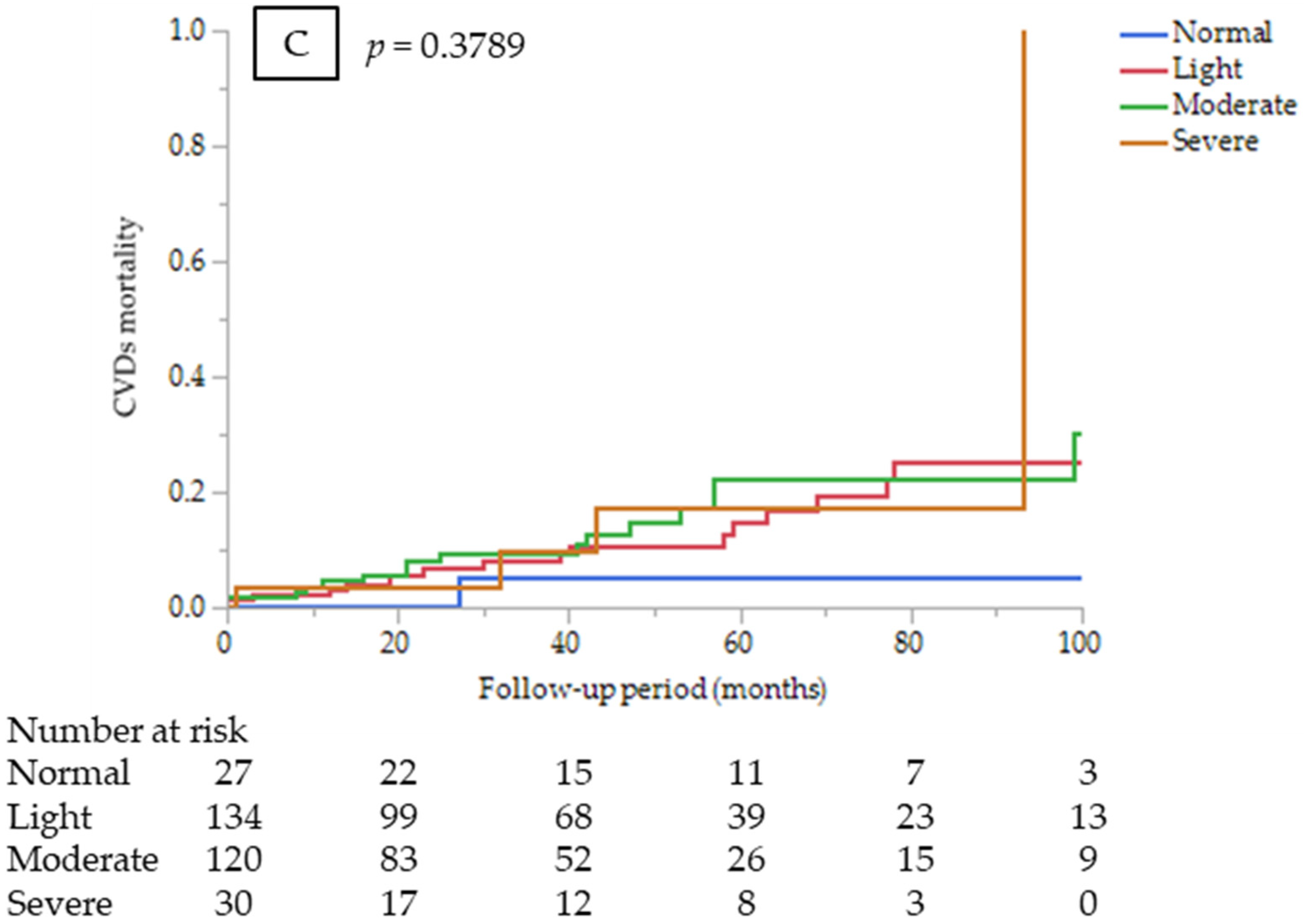
3.3. Sub-Analysis by Cause of Death
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hanna, R.M.; Ghobry, L.; Wassef, O.; Rhee, C.M.; Kalantar-Zadeh, K. A Practical Approach to nutrition, protein-energy wasting, sarcopenia, and cachexia in patients with chronic kidney disease. Blood Purif. 2020, 49, 202–211. [Google Scholar] [CrossRef] [PubMed]
- Khor, B.H.; Tiong, H.C.; Tan, S.C.; Abdul Rahman, R.; Abdul Gafor, A.H. Protein-Energy Wasting Assessment and Clinical Outcomes in Patients with Acute Kidney Injury: A Systematic Review with Meta-Analysis. Nutrients 2020, 12, 2809. [Google Scholar] [CrossRef] [PubMed]
- Obi, Y.; Qader, H.; Kovesdy, C.P.; Kalantar-Zadeh, K. Latest consensus and update on protein-energy wasting in chronic kidney disease. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Rhee, C.; Sim, J.J.; Stenvinkel, P.; Anker, S.D.; Kovesdy, C.P. Why cachexia kills: Examining the causality of poor outcomes in wasting conditions. J. Cachexia Sarcopenia Muscle 2013, 4, 89–94. [Google Scholar] [CrossRef]
- Detsky, A.S.; McLaughlin, J.R.; Baker, J.P.; Johnston, N.; Whittaker, S.; Mendelson, R.A.; Jeejeebhoy, K.N. What is subjective global assessment of nutritional status? JPEN J. Parenter. Enter. Nutr. 1987, 11, 8–13. [Google Scholar] [CrossRef] [Green Version]
- Vellas, B.; Guigoz, Y.; Garry, P.J.; Nourhashemi, F.; Bennahum, D.; Lauque, S.; Albarede, J.L. The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition 1999, 15, 116–122. [Google Scholar] [CrossRef]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef] [Green Version]
- Canaud, B.; Granger Vallée, A.; Molinari, N.; Chenine, L.; Leray-Moragues, H.; Rodriguez, A.; Chalabi, L.; Morena, M.; Cristol, J.P. Creatinine index as a surrogate of lean body mass derived from urea Kt/V, pre-dialysis serum levels and anthropometric characteristics of haemodialysis patients. PLoS ONE 2014, 9, e93286. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Kopple, J.D.; Block, G.; Humphreys, M.H. A malnutrition-inflammation score is correlated with morbidity and mortality in maintenance hemodialysis patients. Am. J. Kidney Dis. 2001, 38, 1251–1263. [Google Scholar] [CrossRef] [Green Version]
- Fouque, D.; Kalantar-Zadeh, K.; Kopple, J.; Cano, N.; Chauveau, P.; Cuppari, L.; Franch, H.; Guarnieri, G.; Ikizler, T.A.; Kaysen, G.; et al. A proposed nomenclature and diagnostic criteria for protein-energy wasting in acute and chronic kidney disease. Kidney Int. 2008, 73, 391–398. [Google Scholar] [CrossRef] [Green Version]
- Ignacio de Ulíbarri, J.; González-Madroño, A.; de Villar, N.G.; González, P.; González, B.; Mancha, A.; Rodríguez, F.; Fernández, G. CONUT: A tool for controlling nutritional status. First validation in a hospital population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar] [PubMed]
- Gul, B.; Metintas, S.; Ak, G.; Yilmaz, S.; Metintas, M. The relationship between nutritional status and prognosis in patients with locally advanced and advanced stage lung cancer. Support. Care Cancer 2021, 29, 3357–3365. [Google Scholar] [CrossRef] [PubMed]
- Takagi, K.; Buettner, S.; Ijzermans, J.N.M. Prognostic significance of the controlling nutritional status (CONUT) score in patients with colorectal cancer: A systematic review and meta-analysis. Int. J. Surg. 2020, 78, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Sze, S.; Pellicori, P.; Zhang, J.; Weston, J.; Clark, A.L. The impact of malnutrition on short-term morbidity and mortality in ambulatory patients with heart failure. Am. J. Clin. Nutr. 2021, 113, 695–705. [Google Scholar] [CrossRef]
- Iwakami, N.; Nagai, T.; Furukawa, T.A.; Sugano, Y.; Honda, S.; Okada, A.; Asaumi, Y.; Aiba, T.; Noguchi, T.; Kusano, K.; et al. Prognostic value of malnutrition assessed by Controlling Nutritional Status score for long-term mortality in patients with acute heart failure. Int. J. Cardiol. 2017, 230, 529–536. [Google Scholar] [CrossRef]
- Zhou, H.; Chao, W.; Cui, L.; Li, M.; Zou, Y.; Yang, M. Controlling Nutritional Status (CONUT) score as immune-nutritional predictor of outcomes in patients undergoing peritoneal dialysis. Clin. Nutr. 2020, 39, 2564–2570. [Google Scholar] [CrossRef]
- Alves, F.C.; Sun, J.; Qureshi, A.R.; Dai, L.; Snaedal, S.; Bárány, P.; Heimbürger, O.; Lindholm, B.; Stenvinkel, P. The higher mortality associated with low serum albumin is dependent on systemic inflammation in end-stage kidney disease. PLoS ONE 2018, 13, e0190410. [Google Scholar] [CrossRef]
- Zhang, Z.; Pereira, S.L.; Luo, M.; Matheson, E.M. Evaluation of blood biomarkers associated with risk of malnutrition in older adults: A systematic review and meta-analysis. Nutrients 2017, 9, 829. [Google Scholar] [CrossRef]
- Eckart, A.; Struja, T.; Kutz, A.; Baumgartner, A.; Baumgartner, T.; Zurfluh, S.; Neeser, O.; Huber, A.; Stanga, Z.; Mueller, B.; et al. Relationship of nutritional status, inflammation, and serum albumin levels during acute illness: A prospective study. Am. J. Med. 2020, 133, 713–722.e7. [Google Scholar] [CrossRef]
- Kaysen, G.A.; Dubin, J.A.; Müller, H.G.; Rosales, L.; Levin, N.W.; Mitch, W.E.; HEMO Study Group NIDDK. Inflammation and reduced albumin synthesis associated with stable decline in serum albumin in hemodialysis patients. Kidney Int. 2004, 65, 1408–1415. [Google Scholar] [CrossRef] [Green Version]
- den Hoedt, C.H.; Bots, M.L.; Grooteman, M.P.; van der Weerd, N.C.; Penne, E.L.; Mazairac, A.H.; Levesque, R.; Blankestijn, P.J.; Nubé, M.J.; ter Wee, P.M.; et al. Clinical predictors of decline in nutritional parameters over time in ESRD. Clin. J. Am. Soc. Nephrol. 2014, 9, 318–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nitta, K.; Goto, S.; Masakane, I.; Hanafusa, N.; Taniguchi, M.; Hasegawa, T.; Nakai, S.; Wada, A.; Hamano, T.; Hoshino, J.; et al. Annual dialysis data report for 2018, JSDT Renal Data Registry: Survey methods, facility data, incidence, prevalence, and mortality. Ren. Replace Ther. 2020, 6, 41. [Google Scholar] [CrossRef]
- Fock, R.A.; Blatt, S.L.; Beutler, B.; Pereira, J.; Tsujita, M.; de Barros, F.E.; Borelli, P. Study of lymphocyte subpopulations in bone marrow in a model of protein-energy malnutrition. Nutrition 2010, 26, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.J.; McClung, J.P. Nutrition, immune function, and infectious disease. Med. J. (Ft Sam Houst Tex). 2021, PB 8-21-01/02/03, 133–136. [Google Scholar]
- Kim, J.U.; Kim, M.; Kim, S.; Nguyen, T.T.; Kim, E.; Lee, S.; Kim, S.; Kim, H. Dendritic cell dysfunction in patients with end-stage renal disease. Immune Netw. 2017, 17, 152–162. [Google Scholar] [CrossRef] [PubMed]
- Kato, T.; Yaku, H.; Morimoto, T.; Inuzuka, Y.; Tamaki, Y.; Yamamoto, E.; Yoshikawa, Y.; Kitai, T.; Taniguchi, R.; Iguchi, M.; et al. Association with Controlling Nutritional Status (CONUT) score and in-hospital mortality and infection in acute heart failure. Sci. Rep. 2020, 10, 3320. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Block, G.; Humphreys, M.H.; Kopple, J.D. Reverse epidemiology of cardiovascular risk factors in maintenance dialysis patients. Kidney Int. 2003, 63, 793–808. [Google Scholar] [CrossRef] [Green Version]
- Lim, C.T.; Yap, X.H.; Chung, K.J.; Khalid, M.A.; Yayha, N.; Latiff, L.A.; Goh, B.L. Predictor of cardiovascular risks in end stage renal failure patients on maintenance dialysis. Pak. J. Med. Sci. 2015, 31, 1300–1305. [Google Scholar] [CrossRef]
- Canaud, B.; Garred, L.J.; Argiles, A.; Flavier, J.L.; Bouloux, C.; Mion, C. Creatinine kinetic modelling: A simple and reliable tool for the assessment of protein nutritional status in haemodialysis patients. Nephrol. Dial. Transplant. 1995, 10, 1405–1410. [Google Scholar]
- Arase, H.; Yamada, S.; Hiyamuta, H.; Taniguchi, M.; Tokumoto, M.; Tsuruya, K.; Nakano, T.; Kitazono, T. Modified creatinine index and risk for long-term infection-related mortality in hemodialysis patients: Ten-year outcomes of the Q-Cohort Study. Sci. Rep. 2020, 10, 1241. [Google Scholar] [CrossRef] [Green Version]
- Vellas, B.; Villars, H.; Abellan, G.; Soto, M.E.; Rolland, Y.; Guigoz, Y.; Morley, J.E.; Chumlea, W.; Salva, A.; Rubenstein, L.Z.; et al. Overview of the MNA—Its history and challenges. J. Nutr. Health Aging. 2006, 10, 456–463; discussion 463–465. [Google Scholar] [PubMed]
- Cereda, E.; Pedrolli, C.; Klersy, C.; Bonardi, C.; Quarleri, L.; Cappello, S.; Turri, A.; Rondanelli, M.; Caccialanza, R. Nutritional status in older persons according to healthcare setting: A systematic review and meta-analysis of prevalence data using MNA®. Clin. Nutr. 2016, 35, 1282–1290. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variables | All n = 311 | CONUT Score Groups | p Value | |||
|---|---|---|---|---|---|---|
| Normal n = 27 | Light n = 134 | Moderate n = 120 | Severe n = 30 | |||
| Age (years) | 69 ± 12 | 63 ± 14 | 69 ± 12 | 70 ± 13 | 73 ± 11 | 0.0116 |
| Sex, male (%) | 226 (73) | 16 (59) | 99 (74) | 89 (74) | 22 (73) | 0.4755 |
| Smoking, yes (%) | 148 (48) | 13 (48) | 58 (43) | 61 (51) | 16 (53) | 0.5923 |
| History of CVDs (%) | 134 (43) | 6 (22) | 55 (41) | 55 (46) | 18 (60) | 0.0264 |
| Late referral (%) | 33 (11) | 2 (7) | 12 (9) | 15 (13) | 4 (13) | 0.729 |
| Diabetes mellitus (%) | 170 (55) | 15 (56) | 64 (48) | 71 (59) | 20 (67) | 0.148 |
| Hypertension (%) | 275 (88) | 25 (93) | 122 (91) | 104 (87) | 24 (80) | 0.3097 |
| Dyslipidemia (%) | 110 (35) | 11 (41) | 44 (33) | 43 (36) | 12 (40) | 0.8007 |
| BMI | 21.9 ± 3.9 | 23.4 ± 4.8 | 21.9 ± 3.8 | 21.7 ± 3.8 | 20.8 ± 3.3 | 0.091 |
| CTR | 53.3 (48.6–58.8) | 49.3 (45.6–52.9) | 53.5 (49–59.3) | 53.3 (48.3–58.4) | 56.2 (53.4–60) | 0.0038 |
| Etiology of ESRD (%) | 0.1625 | |||||
| Diabetic nephropathy | 165 (53) | 14 (52) | 62 (46) | 70 (58) | 19 (63) | |
| Non-diabetic nephropathy | 146 (47) | 13 (48) | 72 (54) | 50 (42) | 11 (37) | |
| Dialysis modality, PD (%) | 38 (12) | 4 (15) | 25 (19) | 9 (8) | 0 (0) | 0.0015 |
| Albumin (g/dL) | 3.3 ± 0.7 | 3.8 ± 0.3 | 3.7 ± 0.4 | 2.9 ± 0.5 | 2.2 ± 0.4 | <0.0001 |
| Total cholesterol (mg/dL) | 170 ± 52 | 194 ± 39 | 174 ± 40 | 168 ± 63 | 133 ± 41 | <0.0001 |
| Lymphocyte count (/μL) | 1023 (777–1377) | 1758 (1233–4585) | 1100 (360–2350) | 881 (160–4311) | 783 (172–1942) | <0.0001 |
| CRP (mg/dL) | 0.2 (0.07–0.6) | 0.07 (0.02–0.33) | 0.12 (0.05–0.4) | 0.35 (0.09–0.92) | 0.37 (0.16–1.53) | <0.0001 |
| Hemoglobin (g/dL) | 9.2 ± 1.5 | 9.7 ± 1.3 | 9.6 ± 1.4 | 8.9 ± 1.5 | 8.3 ± 1.3 | <0.0001 |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| β | p-Value | β | p-Value | |
| Age | 0.1714 | 0.0024 | 0.0252 | 0.0305 |
| Sex, male | 0.0382 | 0.5025 | ||
| Smoking | 0.0638 | 0.2619 | ||
| History of CVD | 0.1552 | 0.0061 | 0.5112 | 0.0540 |
| Late referral | 0.0697 | 0.2204 | ||
| Diabetes mellitus | 0.1380 | 0.0149 | 0.6953 | 0.0092 |
| Hypertension | −0.1155 | 0.0419 | −0.3758 | 0.3583 |
| Dyslipidemia | 0.0306 | 0.5909 | ||
| BMI | −0.0890 | 0.1172 | −0.0465 | 0.1910 |
| CTR | 0.1400 | 0.0136 | −0.0130 | 0.4887 |
| Log CRP | 0.3463 | <0.0001 | 0.4851 | <0.0001 |
| Hemoglobin | −0.3790 | <0.0001 | −0.5776 | <0.0001 |
| Cardiovascular diseases | 21 (21%) |
| Cerebrovascular diseases | 8 (8) |
| Sudden death | 10 (10) |
| Infectious diseases | 33 (33) |
| Malignancy | 12 (12) |
| Cachexia | 4 (4) |
| Others | 7 (7) |
| Undetermined | 5 (5) |
| Variables | Univariate | Multivariate * | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| All-cause mortality | ||||
| CONUT score (continuous) | 1.18 (1.09–1.27) | <0.0001 | 1.13 (1.04–1.22) | 0.0024 |
| CONUT score groups (vs. normal) | 0.0031 ** | 0.019 ** | ||
| Light | 2.3 (0.82–6.45) | 0.11 | 2.75 (0.64–11.8) | 0.17 |
| Moderate | 3.21 (1.15–8.97) | 0.026 | 3.93 (0.92–16.8) | 0.065 |
| Severe | 5.38 (1.79–16.1) | 0.0027 | 5.47 (1.19–25.2) | 0.029 |
| CVD mortality | ||||
| CONUT score (continuous) | 1.12 (0.99–1.27) | 0.059 | 1.05 (0.92–1.2) | 0.4388 |
| CONUT score groups (vs. normal) | 0.25 ** | 0.75 ** | ||
| Light | 4.2 (0.56–31.6) | 0.16 | 2.1 (0.26–17.2) | 0.49 |
| Moderate | 4.94 (0.65–37.3) | 0.12 | 2.68 (0.33–21.9) | 0.36 |
| Severe | 5.37 (0.6–48.2) | 0.13 | 1.8 (0.17–19.6) | 0.63 |
| Infectious disease mortality | ||||
| CONUT score (continuous) | 1.30 (1.15–1.49) | <0.0001 | 1.28 (1.11–1.47) | 0.0006 |
| CONUT score groups (vs. normal) ¶ | 0.0058 ** | 0.032 ** | ||
| Variables | C-Index | p Value | NRI | p Value | IDI | P Value |
|---|---|---|---|---|---|---|
| All-cause Mortality | ||||||
| Established risk factors * | 0.676 | Reference | Reference | Reference | ||
| +CONUT | 0.712 | 0.086 | 0.285 | 0.0278 | 0.025 | 0.023 |
| Infectious diseases Mortality | ||||||
| Established risk factors * | 0.63 | Reference | Reference | Reference | ||
| +CONUT | 0.711 | 0.035 | 0.486 | 0.007 | 0.035 | 0.002 |
| Variables | C-Index | p Value | NRI | p Value | IDI | p Value |
|---|---|---|---|---|---|---|
| All-cause Mortality | ||||||
| Established risk factors * +GNRI | 0.69 | Reference | Reference | Reference | ||
| Established risk factors * +CONUT | 0.702 | 0.282 | 0.051 | 0.339 | 0.009 | 0.061 |
| Infectious diseases Mortality | ||||||
| Established risk factors * +GNRI | 0.664 | Reference | Reference | Reference | ||
| Established risk factors * +CONUT | 0.711 | 0.084 | 0.063 | 0.367 | 0.004 | 0.295 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takagi, K.; Takahashi, H.; Miura, T.; Yamagiwa, K.; Kawase, K.; Muramatsu-Maekawa, Y.; Koie, T.; Mizuno, M. Prognostic Value of the Controlling Nutritional Status (CONUT) Score in Patients at Dialysis Initiation. Nutrients 2022, 14, 2317. https://doi.org/10.3390/nu14112317
Takagi K, Takahashi H, Miura T, Yamagiwa K, Kawase K, Muramatsu-Maekawa Y, Koie T, Mizuno M. Prognostic Value of the Controlling Nutritional Status (CONUT) Score in Patients at Dialysis Initiation. Nutrients. 2022; 14(11):2317. https://doi.org/10.3390/nu14112317
Chicago/Turabian StyleTakagi, Kimiaki, Hiroshi Takahashi, Tomomi Miura, Kasumi Yamagiwa, Kota Kawase, Yuka Muramatsu-Maekawa, Takuya Koie, and Masashi Mizuno. 2022. "Prognostic Value of the Controlling Nutritional Status (CONUT) Score in Patients at Dialysis Initiation" Nutrients 14, no. 11: 2317. https://doi.org/10.3390/nu14112317
APA StyleTakagi, K., Takahashi, H., Miura, T., Yamagiwa, K., Kawase, K., Muramatsu-Maekawa, Y., Koie, T., & Mizuno, M. (2022). Prognostic Value of the Controlling Nutritional Status (CONUT) Score in Patients at Dialysis Initiation. Nutrients, 14(11), 2317. https://doi.org/10.3390/nu14112317