
Body Mass Index Mediates the Relationship between the Frequency of Eating Away from Home and Hypertension in Rural Adults: A Large-Scale Cross-Sectional Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. The Measurement of Blood Pressure and the Definition of Hypertension
2.3. Definition and Assessment of EAFH
2.4. Assessment of Covariates
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Study Populations
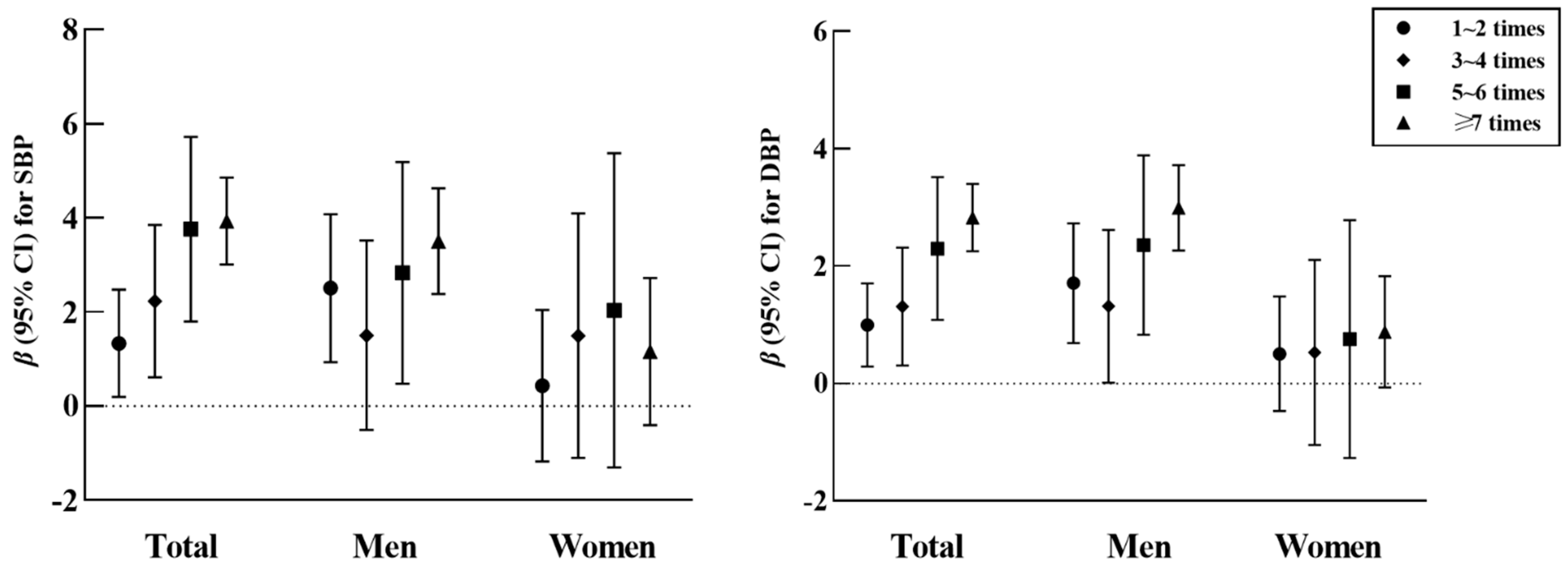
3.2. Association between the Frequency of EAFH and Blood Pressure and Hypertension
3.3. Association between the Frequency of EAFH Breakfasts, Lunches, and Dinners and Hypertension
3.4. Mediation Effects
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhou, B.; Carrillo-Larco, R.M.; Danaei, G.; Riley, L.M.; Paciorek, C.J.; Stevens, G.A.; Gregg, E.W.; Bennett, J.E.; Solomon, B.; Singleton, R.K.; et al. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef]
- Lu, J.; Lu, Y.; Wang, X.; Li, X.; Linderman, G.C.; Wu, C.; Cheng, X.; Mu, L.; Zhang, H.; Liu, J.; et al. Prevalence, awareness, treatment, and control of hypertension in China: Data from 1·7 million adults in a population-based screening study (China PEACE Million Persons Project). Lancet 2017, 390, 2549–2558. [Google Scholar] [CrossRef]
- Doyle, A.E. Hypertension and vascular disease. Am. J. Hypertens. 1991, 4, 103s–106s. [Google Scholar] [CrossRef]
- Buonacera, A.; Stancanelli, B.; Malatino, L. Stroke and Hypertension: An Appraisal from Pathophysiology to Clinical Practice. Curr. Vasc. Pharmacol. 2019, 17, 72–84. [Google Scholar] [CrossRef] [PubMed]
- Bartges, J.W.; Willis, A.M.; Polzin, D.J. Hypertension and renal disease. Vet. Clin. N. Am. Small Anim. Pract. 1996, 26, 1331–1345. [Google Scholar] [CrossRef]
- Ondimu, D.O.; Kikuvi, G.M.; Otieno, W.N. Risk factors for hypertension among young adults (18-35) years attending in Tenwek Mission Hospital, Bomet County, Kenya in 2018. Pan Afr. Med. J. 2019, 33, 210. [Google Scholar] [CrossRef]
- Erem, C.; Hacihasanoglu, A.; Kocak, M.; Deger, O.; Topbas, M. Prevalence of prehypertension and hypertension and associated risk factors among Turkish adults: Trabzon Hypertension Study. J. Public Health (Oxf) 2009, 31, 47–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sitthi-Amorn, C.; Chandraprasert, S.; Bunnag, S.C.; Plengvidhya, C.S. The prevalence and risk factors of hypertension in Klong Toey slum and Klong Toey government apartment houses. Int. J. Epidemiol. 1989, 18, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Glew, G. European trends in conviviality and eating out. Bibl. Nutr. Dieta 1990, 45, 92–103. [Google Scholar] [CrossRef]
- Zhao, Y.; Wang, L.; Xue, H.; Wang, H.; Wang, Y. Fast food consumption and its associations with obesity and hypertension among children: Results from the baseline data of the Childhood Obesity Study in China Mega-cities. BMC Public Health 2017, 17, 933. [Google Scholar] [CrossRef] [Green Version]
- Robson, S.M.; Crosby, L.E.; Stark, L.J. Eating dinner away from home: Perspectives of middle-to high-income parents. Appetite 2016, 96, 147–153. [Google Scholar] [CrossRef] [Green Version]
- Taillie, L.S.; Afeiche, M.C.; Eldridge, A.L.; Popkin, B.M. The contribution of at-home and away-from-home food to dietary intake among 2-13-year-old Mexican children. Public Health Nutr. 2017, 20, 2559–2568. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M.; Wu, J.; Zhang, X.; Hu, C.H.; Zhao, Z.P.; Li, C.; Huang, Z.J.; Zhou, M.G.; Wang, L.M. Prevalence and control of hypertension in adults in China, 2018. Chin. J. Epidemiol. 2021, 42, 1780–1789. [Google Scholar] [CrossRef]
- Liu, X.; Mao, Z.; Li, Y.; Wu, W.; Zhang, X.; Huo, W.; Yu, S.; Shen, L.; Li, L.; Tu, R.; et al. Cohort Profile: The Henan Rural Cohort: A prospective study of chronic non-communicable diseases. Int. J. Epidemiol. 2019, 48, 1756–1756j. [Google Scholar] [CrossRef]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L., Jr.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.T., Jr.; et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: The JNC 7 report. JAMA 2003, 289, 2560–2572. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Liu, L.; Qiao, D.; Xue, Y.; Liu, X.; Zhang, D.; Liu, C.; Mao, Z.; Yu, S.; Shen, F.; et al. The association between frequency of away-from home meals and type 2 diabetes mellitus in rural Chinese adults: The Henan Rural Cohort Study. Eur. J. Nutr. 2020, 59, 3815–3825. [Google Scholar] [CrossRef] [PubMed]
- Cui, N.; Dong, X.; Liao, W.; Xue, Y.; Liu, X.; Li, X.; Hou, J.; Huo, W.; Li, L.; Mao, Z.; et al. Association of eating out frequency and other factors with serum uric acid levels and hyperuricemia in Chinese population. Eur. J. Nutr. 2021, 61, 243–254. [Google Scholar] [CrossRef] [PubMed]
- Fan, M.; Lyu, J.; He, P. Chinese guidelines for data processing and analysis concerning the International Physical Activity Questionnaire. Chin. J. Epidemiol. 2014, 35, 961–964. [Google Scholar]
- Yang, Y.X.; Wang, X.L.; Leong, P.M.; Zhang, H.M.; Yang, X.G.; Kong, L.Z.; Zhai, F.Y.; Cheng, Y.Y.; Guo, J.S.; Su, Y.X. New Chinese dietary guidelines: Healthy eating patterns and food-based dietary recommendations. Asia Pac. J. Clin. Nutr. 2018, 27, 908–913. [Google Scholar] [CrossRef] [PubMed]
- Preacher, K.J.; Hayes, A.F. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav. Res. Methods Instrum. Comput. 2004, 36, 717–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, Y.; Zhang, M.; Liu, Y.; Sun, X.; Wang, B.; Zhao, Y.; Liu, D.; Liu, X.; Zhang, D.; Liu, F.; et al. Association of menopause and type 2 diabetes mellitus. Menopause 2019, 26, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhang, L.; Wang, F.; Liu, L.; Wang, H. Prevalence, awareness, treatment, and control of hypertension in China: Results from a national survey. Am. J. Hypertens. 2014, 27, 1355–1361. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Gu, H.; Teo, K.K.; Bo, J.; Wang, Y.; Yang, J.; Wang, X.; Zhang, H.; Sun, Y.; Jia, X.; et al. Hypertension prevalence, awareness, treatment, and control in 115 rural and urban communities involving 47,000 people from China. J. Hypertens. 2016, 34, 39–46. [Google Scholar] [CrossRef]
- Xing, L.; Jing, L.; Tian, Y.; Lin, M.; Du, Z.; Yan, H.; Ren, G.; Dong, Y.; Sun, Q.; Liu, S. Urban-Rural disparities in status of hypertension in northeast China: A population-based study, 2017–2019. Clin. Epidemiol. 2019, 11, 801–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Yu, Y.; Tian, X. Does Eating-Away-from-Home Increase the Risk of a Metabolic Syndrome Diagnosis? Int. J. Environ. Res. Public Health 2019, 16, 575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seow, D.Y.; Haaland, B.; Jafar, T.H. The Association of Prehypertension With Meals Eaten Away From Home in Young Adults in Singapore. Am. J. Hypertens. 2015, 28, 1197–1200. [Google Scholar] [CrossRef] [PubMed]
- Kar, S.; Khandelwal, B. Fast foods and physical inactivity are risk factors for obesity and hypertension among adolescent school children in east district of Sikkim, India. J. Nat. Sci. Biol. Med. 2015, 6, 356–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Provido, S.M.P.; Abris, G.P.; Hong, S.; Yu, S.H.; Lee, C.B.; Lee, J.E. Association of fried food intake with prehypertension and hypertension: The Filipino women s diet and health study. Nutr. Res. Pract. 2020, 14, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Qin, P.; Liu, D.; Wu, X.; Zeng, Y.; Sun, X.; Zhang, Y.; Li, Y.; Wu, Y.; Han, M.; Qie, R.; et al. Fried-food consumption and risk of overweight/obesity, type 2 diabetes mellitus, and hypertension in adults: A meta-analysis of observational studies. Crit. Rev. Food Sci. Nutr. 2021, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, M.; Saito, A.; Okada, C.; Okada, E.; Tajima, R.; Takimoto, H. Consumption of meals prepared away from home is associated with inadequacy of dietary fiber, vitamin C and mineral intake among Japanese adults: Analysis from the 2015 National Health and Nutrition Survey. Nutr. J. 2021, 20, 40. [Google Scholar] [CrossRef] [PubMed]
- Byrd, K.; Almanza, B.; Ghiselli, R.F.; Behnke, C.; Eicher-Miller, H.A. Reported Action to Decrease Sodium Intake Is Associated with Dining Out Frequency and Use of Menu Nutrition Information among US Adults. J. Acad. Nutr. Diet. 2018, 118, 824–835. [Google Scholar] [CrossRef] [PubMed]
- Kornitzer, M.; Dramaix, M.; De Backer, G. Epidemiology of risk factors for hypertension: Implications for prevention and therapy. Drugs 1999, 57, 695–712. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Knüppel, S.; Iqbal, K.; Andriolo, V.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food Groups and Risk of Hypertension: A Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Adv. Nutr. 2017, 8, 793–803. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A.; Cannon, G.; Moubarac, J.C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The UN Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutr. 2018, 21, 5–17. [Google Scholar] [CrossRef] [Green Version]
- Rezende-Alves, K.; Hermsdorff, H.H.M.; Miranda, A.; Lopes, A.C.S.; Bressan, J.; Pimenta, A.M. Food processing and risk of hypertension: Cohort of Universities of Minas Gerais, Brazil (CUME Project). Public Health Nutr. 2021, 24, 4071–4079. [Google Scholar] [CrossRef]
- Nardocci, M.; Polsky, J.Y.; Moubarac, J.C. Consumption of ultra-processed foods is associated with obesity, diabetes and hypertension in Canadian adults. Can. J. Public Health 2021, 112, 421–429. [Google Scholar] [CrossRef]
- Cohen, D.A.; Story, M. Mitigating the health risks of dining out: The need for standardized portion sizes in restaurants. Am. J. Public Health 2014, 104, 586–590. [Google Scholar] [CrossRef]
- Seravalle, G.; Grassi, G. Obesity and hypertension. Pharmacol. Res. 2017, 122, 1–7. [Google Scholar] [CrossRef]
- Shen, Y.; Chang, C.; Zhang, J.; Jiang, Y.; Ni, B.; Wang, Y. Prevalence and risk factors associated with hypertension and prehypertension in a working population at high altitude in China: A cross-sectional study. Environ. Health Prev. Med. 2017, 22, 19. [Google Scholar] [CrossRef] [Green Version]
- Orshal, J.M.; Khalil, R.A. Gender, sex hormones, and vascular tone. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2004, 286, R233–R249. [Google Scholar] [CrossRef] [Green Version]
- Doumas, M.; Papademetriou, V.; Faselis, C.; Kokkinos, P. Gender differences in hypertension: Myths and reality. Curr. Hypertens. Rep. 2013, 15, 321–330. [Google Scholar] [CrossRef]
- Wang, L.; Szklo, M.; Folsom, A.R.; Cook, N.R.; Gapstur, S.M.; Ouyang, P. Endogenous sex hormones, blood pressure change, and risk of hypertension in postmenopausal women: The Multi-Ethnic Study of Atherosclerosis. Atherosclerosis 2012, 224, 228–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clemons, M.; Goss, P. Estrogen and the risk of breast cancer. N. Engl. J. Med. 2001, 344, 276–285. [Google Scholar] [CrossRef]
- Di Giosia, P.; Giorgini, P.; Stamerra, C.A.; Petrarca, M.; Ferri, C.; Sahebkar, A. Gender Differences in Epidemiology, Pathophysiology, and Treatment of Hypertension. Curr. Atheroscler. Rep. 2018, 20, 13. [Google Scholar] [CrossRef] [PubMed]
- Song, J.J.; Ma, Z.; Wang, J.; Chen, L.X.; Zhong, J.C. Gender Differences in Hypertension. J. Cardiovasc. Transl. Res. 2020, 13, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, N.H.; Lloyd, L.E.; Bernstein, V.R. Sex and age differences in lifestyle risk: Implications for health promotion programming. Am. J. Prev. Med. 1987, 3, 192–199. [Google Scholar] [CrossRef]
- Ikehara, S.; Iso, H. Alcohol consumption and risks of hypertension and cardiovascular disease in Japanese men and women. Hypertens. Res. 2020, 43, 477–481. [Google Scholar] [CrossRef] [PubMed]
- Bezerra, I.N.; Sichieri, R. Eating out of home and obesity: A Brazilian nationwide survey. Public Health Nutr. 2009, 12, 2037–2043. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ju, L.; Yu, D.; Guo, Q.; Fang, H.; Xu, X.; Li, S.; Cheng, X.; Piao, W.; Cai, S.; Zhao, L. Eating out behavior and its impact on obesity among Chinese residents aged 18-59 in 2015. J. Hyg. Res. 2021, 50, 395–400. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total (N = 29,611) | Men (N = 12,098) | Women (N = 17,513) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Normotensive | Hypertension | p | Normotensive | Hypertension | p | Normotensive | Hypertension | p | |
| Age (years), mean ± SD | 53.0 ± 12.6 | 60.5 ± 10.2 | <0.001 | 54.9 ± 12.7 | 59.6 ± 11.1 | <0.001 | 51.7 ± 12.4 | 61.2 ± 9.4 | <0.001 |
| Marital status, n (%) | <0.001 | 0.978 | <0.001 | ||||||
| Married/cohabitation | 18,372 (91.3) | 8314 (87.7) | 7404 (90.2) | 3511 (90.2) | 10,968 (92.0) | 4803 (85.9) | |||
| Unmarried/divorced/widowed | 1754 (8.7) | 1171 (12.3) | 802 (9.8) | 381 (9.8) | 952 (8.0) | 790 (14.1) | |||
| Education level, n (%) | <0.001 | 0.002 | <0.001 | ||||||
| Junior high school or below | 16,426 (81.6) | 8191 (86.4) | 6440 (78.5) | 3052 (78.4) | 9986 (83.8) | 5139 (91.9) | |||
| High school | 2831 (14.1) | 1147 (12.1) | 1423 (17.3) | 724 (18.6) | 1408 (11.8) | 423 (7.5) | |||
| High school above | 869 (4.3) | 147 (1.5) | 343 (4.2) | 116 (3.0) | 526 (4.4) | 31 (0.6) | |||
| Average income per month, n (%) | <0.001 | 0.005 | <0.001 | ||||||
| <500 CNY | 6882 (34.2) | 3791 (40.0) | 2941 (35.8) | 1474 (37.9) | 3941 (33.0) | 2317 (41.4) | |||
| 500–1000 CNY | 6296 (31.3) | 3032 (32.0) | 2486 (30.3) | 1213 (31.2) | 3810 (32.0) | 1819 (32.5) | |||
| ≥1000 CNY | 6948 (34.5) | 2662 (28.0) | 2779 (33.9) | 1205 (31.0) | 4169 (35.0) | 1457 (26.1) | |||
| Smoking status, n (%) | <0.001 | <0.001 | 0.944 | ||||||
| Never | 14,394 (71.5) | 6898 (72.7) | 2519 (30.7) | 1328 (34.2) | 11,875 (99.6) | 5570 (99.6) | |||
| Former | 1386 (6.9) | 949 (10.0) | 1374 (16.7) | 943 (24.2) | 12 (0.1) | 6 (0.1) | |||
| Current | 4346 (21.6) | 1638 (17.3) | 4313 (52.6) | 1621 (41.6) | 33 (0.3) | 17 (0.3) | |||
| Alcohol consumption, n (%) | <0.001 | <0.001 | <0.001 | ||||||
| Never | 15,698 (78.0) | 7272 (76.7) | 4078 (49.7) | 1756 (45.1) | 11,620 (97.5) | 5516 (98.6) | |||
| Former | 913 (4.5) | 543 (5.7) | 886 (10.8) | 531 (13.6) | 27 (0.2) | 12 (0.2) | |||
| Current | 3515 (17.5) | 1670 (17.6) | 3242 (39.5) | 1605 (41.3) | 273 (2.3) | 65 (1.2) | |||
| Physical activity, n (%) | <0.001 | <0.001 | <0.001 | ||||||
| Low | 5920 (29.4) | 3507 (37.0) | 2592 (31.6) | 1595 (41.0) | 3328 (27.9) | 1912 (34.2) | |||
| Moderate | 7774 (38.6) | 3108 (32.7) | 2403 (29.3) | 996 (25.6) | 5371 (45.1) | 2112 (37.8) | |||
| High | 6432 (32.0) | 2870 (30.3) | 3211 (39.1) | 1301 (33.4) | 3221 (27.0) | 1569 (28.0) | |||
| Abundant vegetable and fruit intake, n (%) | 10,239 (50.9) | 3929 (41.4) | <0.001 | 4171 (50.8) | 1624 (41.7) | <0.001 | 6068 (50.9) | 2305 (41.2) | <0.001 |
| High-fat diet, n (%) | 4028 (20.0) | 1362 (14.4) | <0.001 | 2075 (25.3) | 802 (20.6) | <0.001 | 1953 (16.4) | 560 (10.0) | <0.001 |
| Family history of hypertension, n (%) | 2966 (14.7) | 2607 (27.5) | <0.001 | 1027 (12.5) | 1051 (27.0) | <0.001 | 1939 (16.3) | 1556 (27.8) | <0.001 |
| BMI (kg/m2), mean ± SD | 24.1 ± 3.4 | 26.0 ± 3.6 | <0.001 | 23.9 ± 3.3 | 25.8 ± 3.5 | <0.001 | 24.3 ± 3.4 | 26.1 ± 3.7 | <0.001 |
| Frequency of EAFH (times/week), n (%) | <0.001 | 0.492 | <0.001 | ||||||
| 0 | 17,423 (86.6) | 8512 (89.7) | 6656 (81.1) | 3169 (81.4) | 10,767 (90.3) | 5343 (95.5) | |||
| 1–2 | 794 (3.9) | 257 (2.7) | 361 (4.4) | 162 (4.2) | 433 (3.6) | 95 (1.7) | |||
| 3–4 | 397 (2.0) | 116 (1.2) | 224 (2.7) | 93 (2.4) | 173 (1.5) | 23 (0.4) | |||
| 5–6 | 261 (1.3) | 84 (0.9) | 162 (2.0) | 66 (1.7) | 99 (0.8) | 18 (0.3) | |||
| ≥7 | 1251 (6.2) | 516 (5.5) | 803 (9.8) | 402 (10.3) | 448 (3.8) | 114 (2.1) | |||
| SBP (mmHg), mean ± SD | 115.7 ± 11.9 | 146.9 ± 16.9 | <0.001 | 117.2 ± 11.2 | 145.6 ± 16.1 | <0.001 | 114.6 ± 12.3 | 147.8 ± 17.4 | <0.001 |
| DBP (mmHg), mean ± SD | 72.4 ± 8.2 | 88.1 ± 10.7 | <0.001 | 73.3 ± 8.3 | 89.5 ± 10.9 | <0.001 | 71.8 ± 8.0 | 87.1 ± 10.4 | <0.001 |
| Weekly Frequency of EAFH | Prevalence, % (95% CI) | OR (95% CI) | P trend | |||
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | * Per Level Risk | |||
| Total (n = 29,611) | 1.031 (1.022–1.040) | <0.001 | ||||
| 0 time (n = 25,935) | 32.82 (32.25–33.39) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | ||
| 1–2 times (n = 1051) | 24.45 (21.85–27.06) | 1.147 (0.986–1.334) | 1.173 (1.007–1.366) | 1.115 (0.953–1.305) | ||
| 3–4 times (n = 513) | 22.61 (18.98–26.24) | 1.310 (1.051–1.632) | 1.366 (1.094–1.704) | 1.341 (1.067–1.684) | ||
| 5–6 times (n = 345) | 24.35 (19.80–28.90) | 1.545 (1.190–2.005) | 1.625 (1.250–2.112) | 1.576 (1.202–2.065) | ||
| ≥7 times (n = 1767) | 29.20 (27.08–31.32) | 1.645 (1.468–1.844) | 1.723 (1.533–1.935) | 1.673 (1.482–1.889) | ||
| Men (n = 12,098) | 1.026 (1.016–1.037) | <0.001 | ||||
| 0 time (n = 9825) | 32.25 (31.33–33.18) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | ||
| 1–2 times (n = 523) | 30.98 (27.00–34.95) | 1.307 (1.074–1.591) | 1.291 (1.061–1.573) | 1.190 (0.969–1.462) | ||
| 3–4 times (n = 317) | 29.34 (24.30–34.38) | 1.437 (1.114–1.855) | 1.411 (1.093–1.823) | 1.405 (1.077–1.833) | ||
| 5–6 times (n = 228) | 28.95 (23.02–34.88) | 1.514 (1.122–2.044) | 1.475 (1.092–1.993) | 1.419 (1.037–1.941) | ||
| ≥7 times (n = 1205) | 33.36 (30.70–36.03) | 1.693 (1.475–1.943) | 1.653 (1.439–1.898) | 1.634 (1.413–1.890) | ||
| Women (n = 17,513) | 1.010 (0.993–1.027) | 0.245 | ||||
| 0 time (n = 16,110) | 33.17 (32.44–33.89) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | ||
| 1–2 times (n = 528) | 17.99 (14.71–21.28) | 0.976 (0.766–1.244) | 0.992 (0.777–1.265) | 1.006 (0.783–1.293) | ||
| 3–4 times (n = 196) | 11.73 (7.19–16.28) | 0.854 (0.540–1.353) | 0.891 (0.561–1.417) | 0.885 (0.551–1.422) | ||
| 5–6 times (n = 117) | 15.38 (8.75–22.02) | 1.183 (0.691–2.025) | 1.274 (0.740–2.195) | 1.393 (0.800–2.426) | ||
| ≥7 times (n = 562) | 20.28 (16.95–23.62) | 1.172 (0.936–1.467) | 1.199 (0.956–1.503) | 1.170 (0.926–1.478) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, B.; Liu, X.; Wang, Y.; Dong, X.; Liao, W.; Huo, W.; Hou, J.; Li, L.; Wang, C. Body Mass Index Mediates the Relationship between the Frequency of Eating Away from Home and Hypertension in Rural Adults: A Large-Scale Cross-Sectional Study. Nutrients 2022, 14, 1832. https://doi.org/10.3390/nu14091832
Liu B, Liu X, Wang Y, Dong X, Liao W, Huo W, Hou J, Li L, Wang C. Body Mass Index Mediates the Relationship between the Frequency of Eating Away from Home and Hypertension in Rural Adults: A Large-Scale Cross-Sectional Study. Nutrients. 2022; 14(9):1832. https://doi.org/10.3390/nu14091832
Chicago/Turabian StyleLiu, Beibei, Xiaotian Liu, Yuyang Wang, Xiaokang Dong, Wei Liao, Wenqian Huo, Jian Hou, Linlin Li, and Chongjian Wang. 2022. "Body Mass Index Mediates the Relationship between the Frequency of Eating Away from Home and Hypertension in Rural Adults: A Large-Scale Cross-Sectional Study" Nutrients 14, no. 9: 1832. https://doi.org/10.3390/nu14091832