
Standards for the Use of Enteral Nutrition in Patients with Diabetes or Stress Hyperglycaemia: Expert Consensus

 ,
,  , , , , ,
, , , , ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Review
2.2. Preparation of the Clinical Scenarios or Indicatios
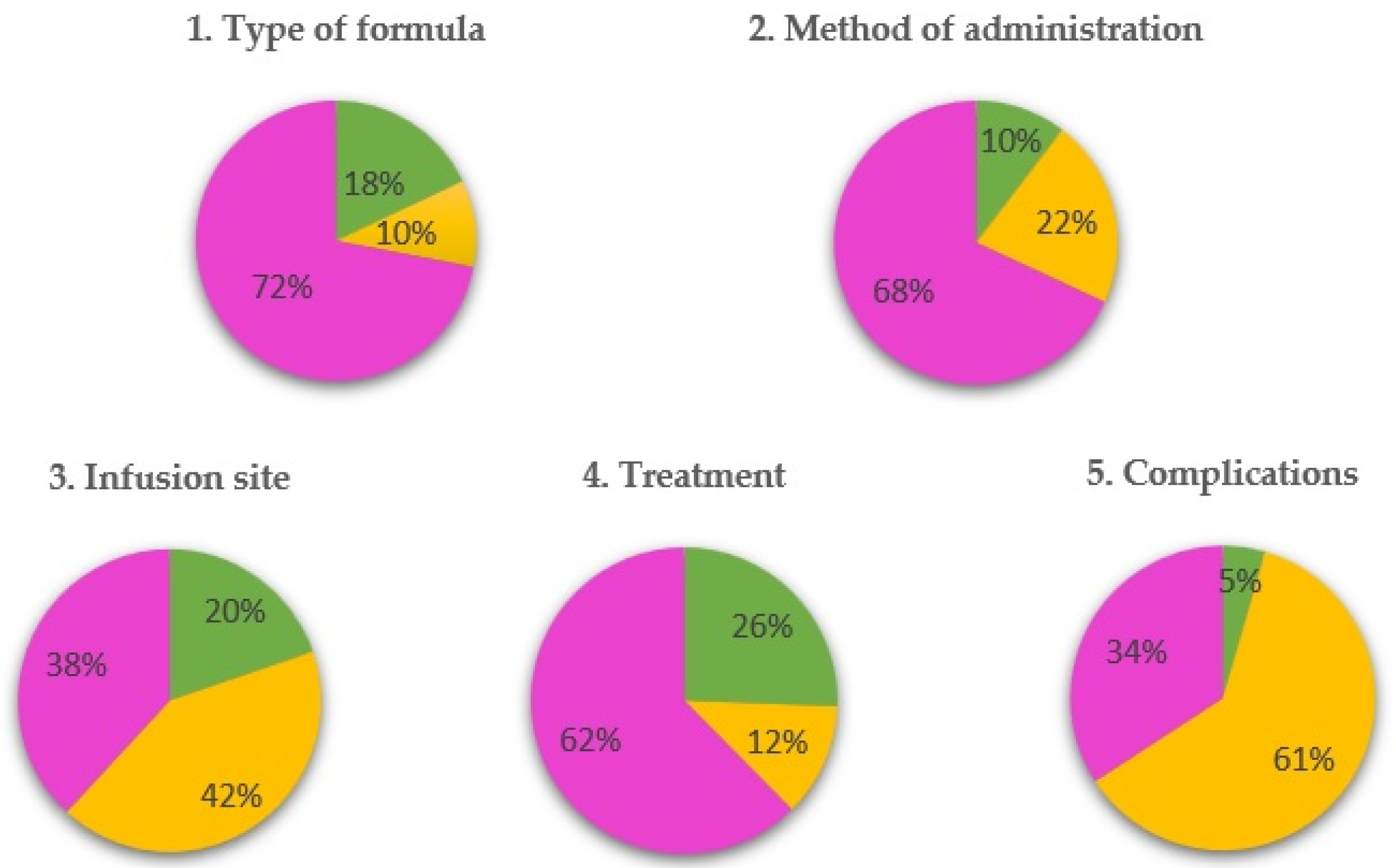
- Chapter 1: types of formulas used (768 clinical scenarios);
- Chapter 2: method of administration (288 clinical scenarios);
- Chapter 3: infusion site (192 clinical scenarios);
- Chapter 4: treatment of diabetes (1104 clinical scenarios);
- Chapter 5: management of complications (640 clinical scenarios).
2.3. Selection of the Members of the Panel of Experts
2.4. Rounds to Score Indications
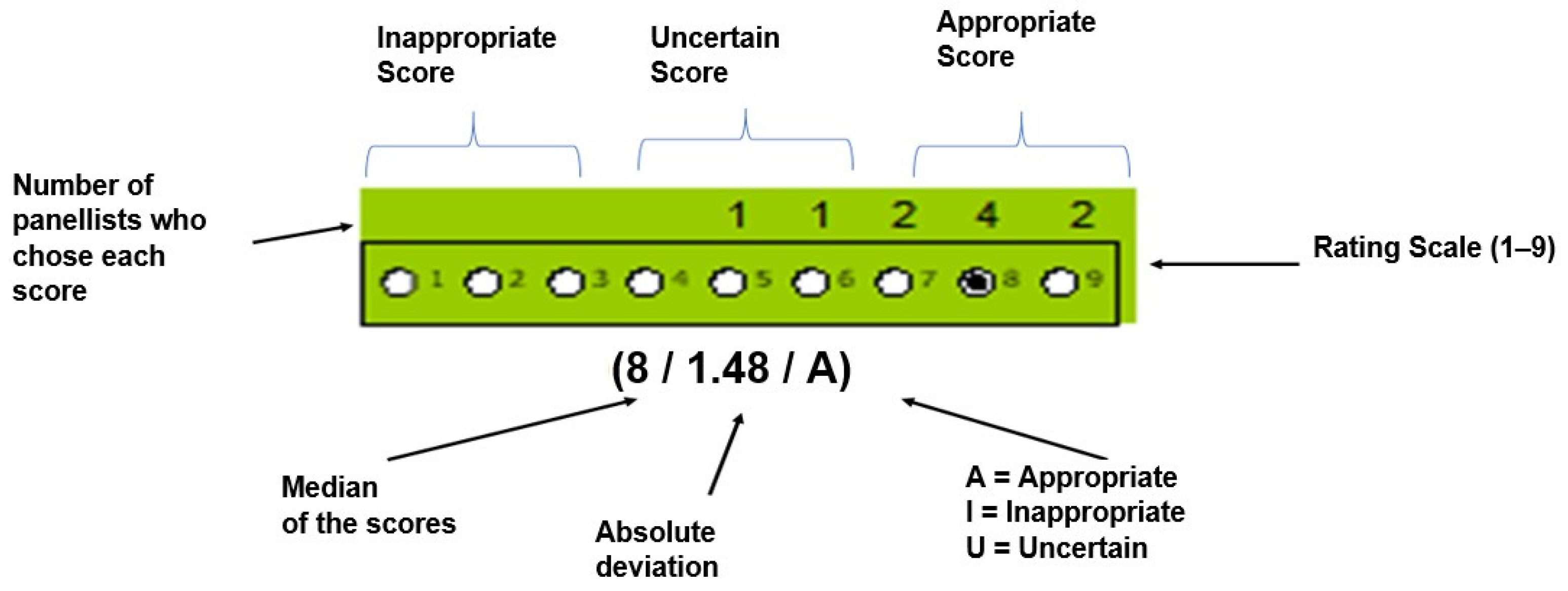
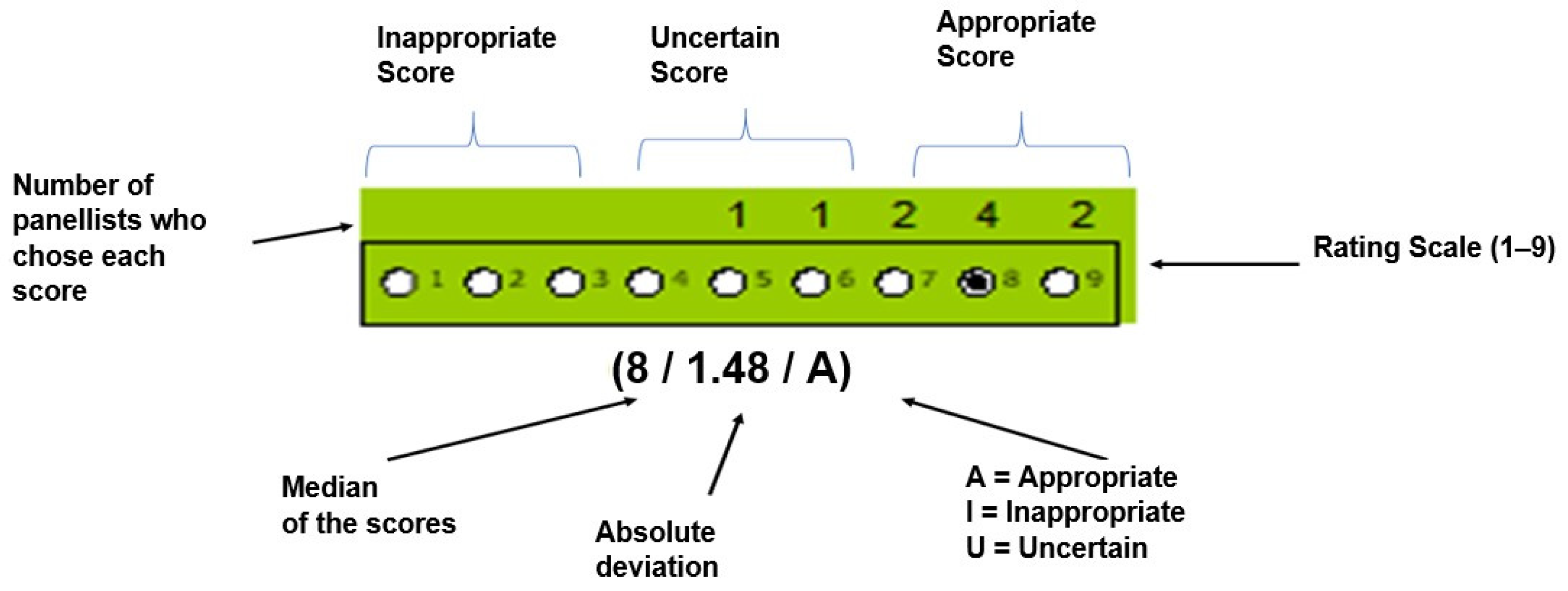
2.4.1. Definition of Appropriateness
2.4.2. First Round
2.4.3. Second Round
2.5. Statistical Criteria for Consensus
- Appropriate indication if the median was in the interval from seven to nine, without disagreement.
- Uncertain indication if the median was in the interval from four to six, or when there was disagreement among the panellists, independent of the median;
- Inappropriate indication if the median was in the interval of one to three, without disagreement.
3. Results
4. Discussion
4.1. Types of Formulas Used
4.2. Method of Administration
4.3. Infusion Site
4.4. Treatment of Diabetes
4.5. Management of Gastrointestinal Complications
5. Limitations and Strengths
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- Calorie-protein and vitamin-mineral targets:
- Do your patients with diabetes mellitus (DM) receive different calorie and/or protein intake through enteral nutrition (EN) than those without DM? If the answer is yes, state why;
- What type of formula (or formulas) would you use to prescribe a low-calorie EN?/high-protein for patients with DM and body mass index (BMI) > 40 kg/m2?
- Administration regimen:
- Regarding the starting administration regimen (not the type of formula). Does the fact that the patient has DM change anything? Respond yes or no and justify the answer;
- Regarding subsequent regimens, does the fact that the patient has DM change anything? Respond yes or no and justify the answer;
- Which method of administration would you prefer to use in patients with DM? Continuous 24 h, continuous day/night or gravity/bolus. Justify the answer.
- Specific formulas for diabetes or stress hyperglycaemia:
- Do you always use “specific formulas for diabetes” as the first option in people with DM or stress hyperglycaemia? Respond yes or no and justify the answer;
- Would you use specific formulas for DM in prediabetes? Respond yes or no and justify the answer;
- In a patient with DM and home enteral nutrition (HEN), do you consider HbA1c to be useful data for deciding to prescribe standard or specific formulas? Respond yes or no and justify the answer;
- In an inpatient with stress hyperglycaemia or DM with overt hyperglycaemia (mean glycaemia around 180 mg/dl), would you prescribe a specific enteral formula for DM? Respond yes or no and justify the answer;
- Do you think that standard formulas with fibre can be used in home nutrition in people with DM? Respond yes or no and justify the answer;
- In inpatients with DM who are discharged home with HEN, do you maintain the same formula? Why?
- Would you use other specific formulas for patients with DM (oligopeptide/low-fat, immunomodulatory, with Omega-3, beta-hydroxy-beta-methylbutyrate (HMB), etc.)? Specify in which clinical situations you would prescribe them;
- Regarding the composition of the formulas in people with DM:
- Regarding the concept of “formula for people with diabetes or stress hyperglycaemia”, what is the aim with its chemical formulation?
- What do you think is the ideal distribution of macronutrients?
- Would you use fructose?
- What proteins would you use?
- Would you supplement with “extra” doses of micronutrients (above the Dietary Reference Intakes (DRIs)). If yes, which?
- Is a fibre-free formula beneficial in people with DM? Justify each answer;
- The price of formulas for people with DM is higher than the standard equivalents:
- Do you know by approximately how much?
- Do you think it is justified to use formulas for diabetes, despite the increased cost for public health? Would it be cost-effective?
- Do you take price into account when prescribing? Respond yes or no and justify the answer.
- Specific formulas in various clinical situations:
- Person with DM with HEN with a specific formula for diabetes and constipation. What would you do? Justify the answer;
- Neurological patient, with DM, bedridden and malnourished with HEN with a specific formula that presents abdominal distension and meteorism, do you think it is appropriate to maintain the same formula? Justify the answer;
- Bedridden DM patient with HEN and high risk of pressure ulcers. Should they be treated preventively with arginine supplements or with a higher protein content than current formulas for DM? Justify the answer;
- For patients with DM and gastrointestinal cancer, what type of enteral formula would you use in the perioperative period? Justify the answer;
- For patients with DM and head and neck cancer, what type of enteral formula would you use in the perioperative period? Justify the answer;
- For patients with DM and predialysis or dialysis chronic kidney disease (CKD) requiring EN by tube, what kind of formula would you use? Justify the answer;
- For patients with DM who presents diarrhoea attributable to EN itself, what type of formula would you use? Justify the answer;
- For patients with DM and hypertriglyceridemia over 400 mg/dl, what kind of formula would you use? Justify the answer;
- For patients with DM and EN by nasogastric tube presenting gastroparesis, what formula would you use? Justify the answer;
- In case of severe gastroparesis that requires infusion of nutrition into the jejunum; what formula would you use? Justify the answer;
- In what situations do you consider it necessary to use micronutrient supplementation in people with DM? Justify the answer.
- Treatment of diabetes in EN:
- What would be the ideal oral hypoglycaemic agents (OHAs) treatment in patients with DM2 and HEN?
- Do the new drugs (GLP-1-1 analogues; SGLT-2) have a role in the management of patients with EN and DM2?
- Do you use the glycaemic load calculation and the sensitivity index to calculate bolus insulin in people with a bolus or who are critically ill? Respond yes or no and justify the answer;
- Which insulin do you consider most appropriate as basal insulin? As night-time or daytime EN, as continuous 24-h EN and as EN in bolus or by gravity. Justify the answer;
- Which insulin do you consider most appropriate as bolus insulin? As night-time or daytime EN, as continuous 24-h EN and as EN in bolus or by gravity. Justify the answer;
- Which insulin do you consider most appropriate as a correction or rescue insulin? As night-time or daytime EN, as continuous 24-h EN and as EN in bolus or by gravity. Justify the answer;
- What do you think influences you the most when prescribing EN to a patient (select the top three):
- Type of formula: macronutrient composition;
- Formula type: calorie density;
- Formula Type: flavouring;
- Price;
- Characteristics of the container (size, weight, grip, opening and closing, etc.) and connections;
- Patient preferences;
- Marketing of the manufacturing company;
- Clinical studies of the formula.
Appendix B
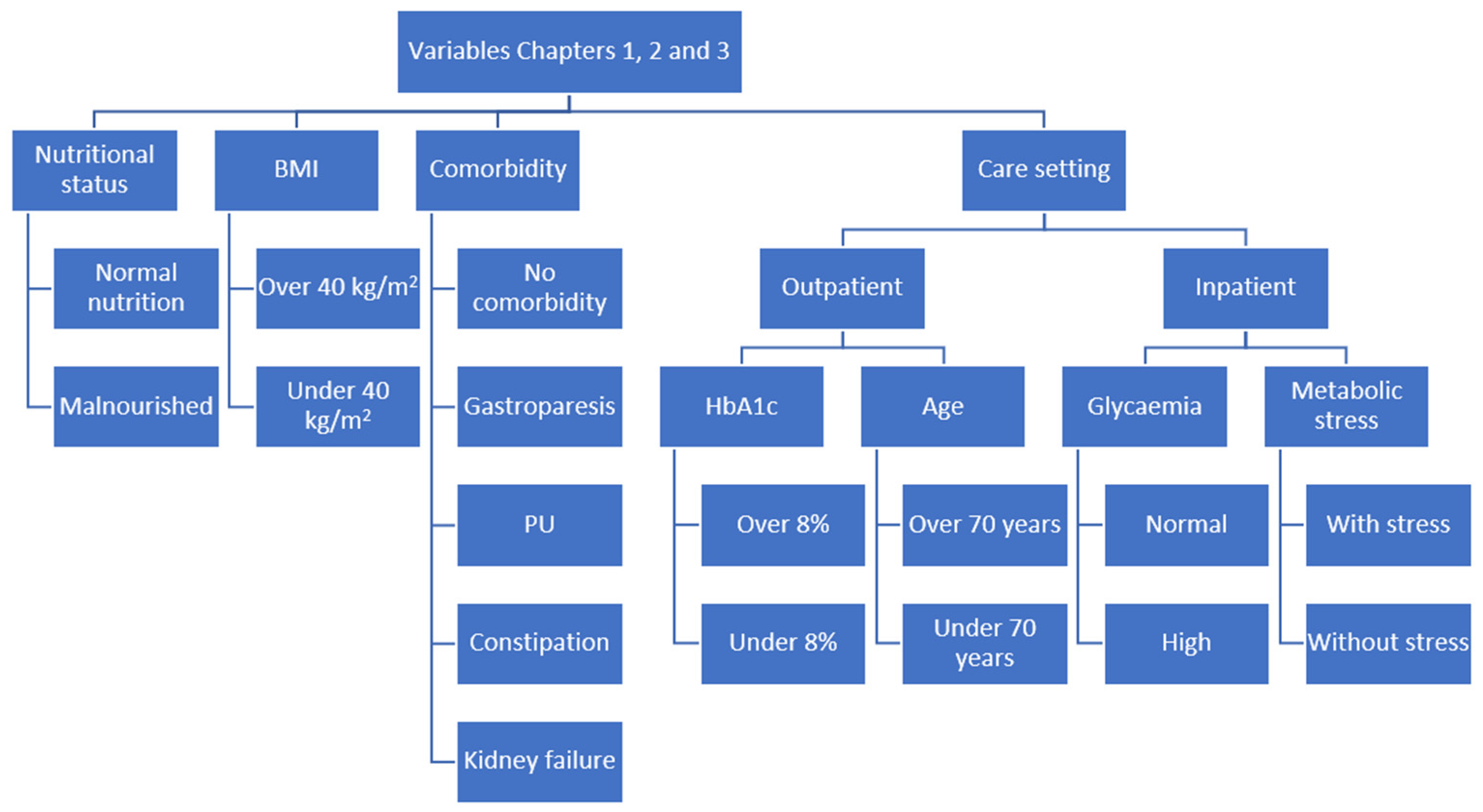
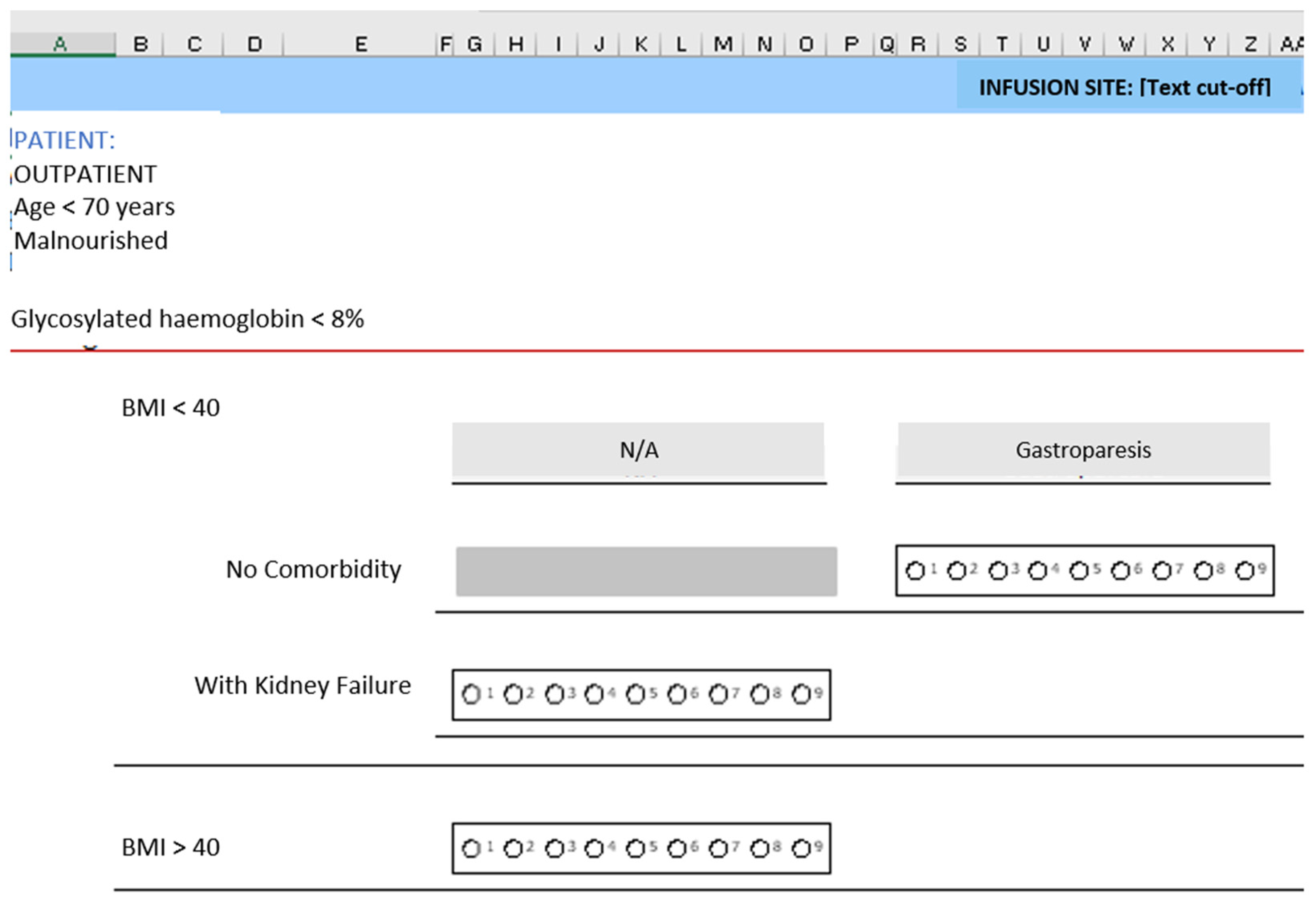
- Variables used to create the scenarios in chapters 1, 2 and 3:
- Patient point of care: outpatient or inpatient;
- Age (only in outpatients): under 70 years or 70 years or older;
- Glycaemia (only in inpatients): controlled or high;
- Metabolic stress (only in inpatients): without stress or with stress;
- Glycaemia (only in outpatients): glycosylated haemoglobin greater than 8% or glycosylated haemoglobin under 8%;
- Nutritional status: malnourished or normonourished;
- Body Mass Index (BMI): BMI < 40 kg/m2 or BMI > 40 kg/m2;
- Kidney failure (KF) (only in patients with BMI < 40): without kidney failure (KF) or with KF;
- Comorbidity (only in patients with BMI < 40 and without KF): no comorbidities, gastroparesis, pressure ulcer or constipation.
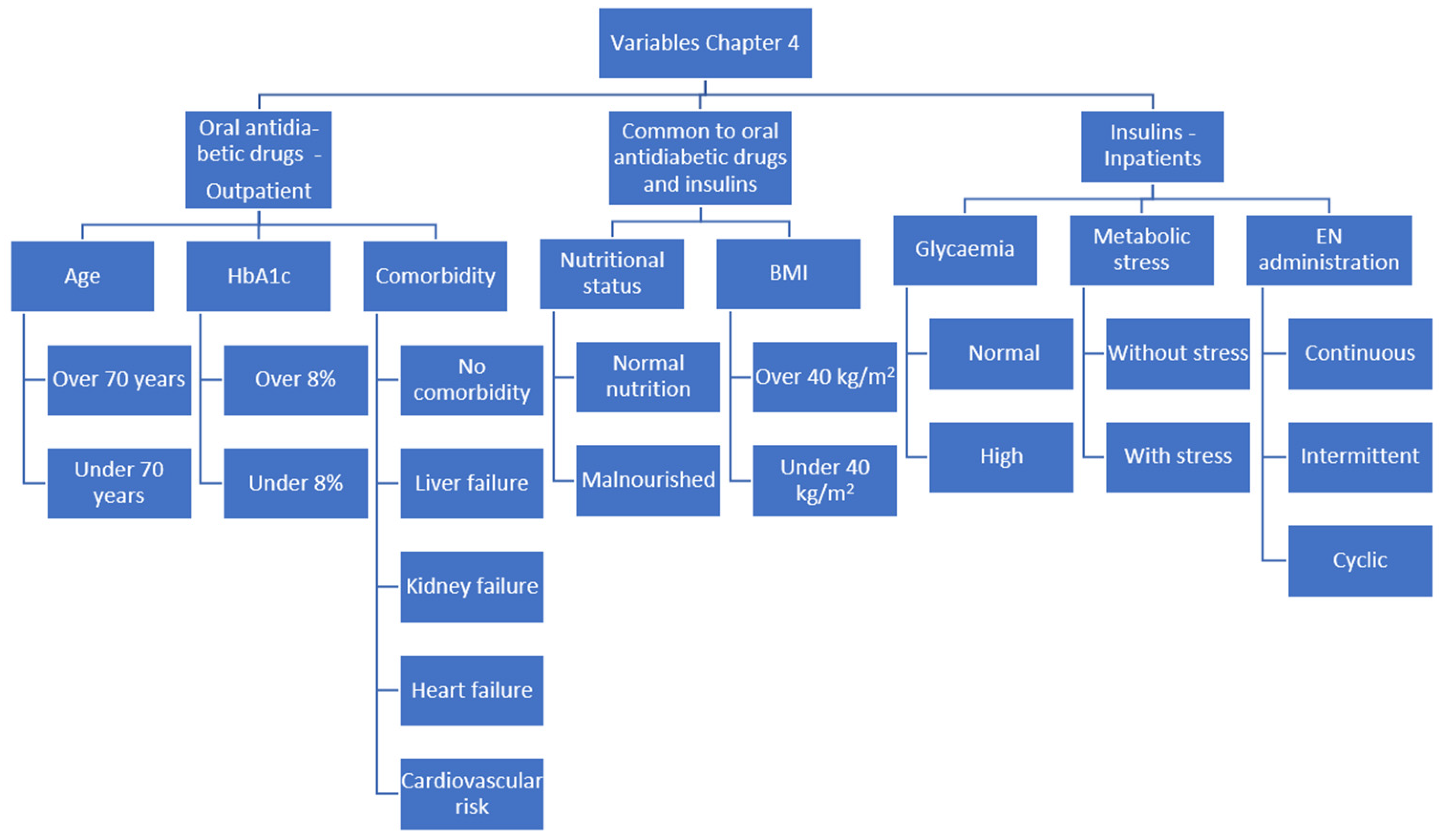
- Variables used to build the scenarios in chapter 4 (for antidiabetic drugs):
- Patient point of care: outpatient;
- Age: under 70 years or 70 years or older;
- Glycaemia: glycosylated haemoglobin greater than 8% or glycosylated haemoglobin under 8%;
- Nutritional status: malnourished or normonourished;
- Body Mass Index (BMI): BMI < 40 kg/m2 or BMI > 40 kg/m2;
- Comorbidity: No comorbidities, kidney failure, liver failure, heart failure or cardiovascular risk.
- Variables used to create the scenarios in chapter 4 (for insulins):
- Patient point of care: inpatients;
- Glycaemia: controlled or high;
- Metabolic stress: without stress or with stress;
- Nutritional status: malnourished or normonourished;
- Body Mass Index (BMI): BMI < 40 kg/m2 or BMI > 40 kg/m2;
- Enteral nutrition form of administration: continuous or bolus/intermittent or cyclic administration.
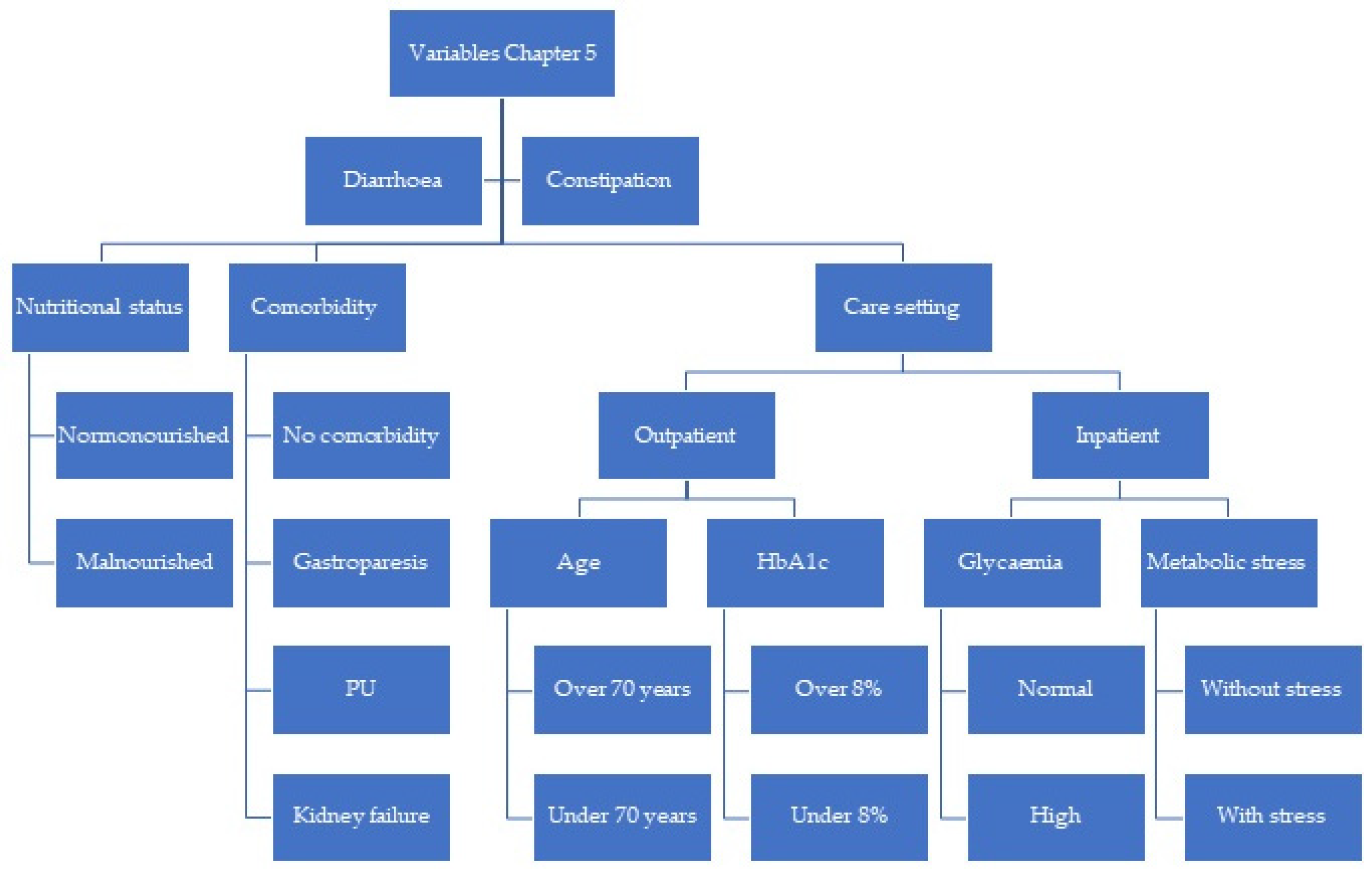
- Variables used to build the scenarios in chapter 5:
- Patient point of care: outpatient or inpatient;
- Age (only in outpatients): under 70 years or 70 years or older;
- Glycaemia (only in inpatients): controlled or high;
- Metabolic stress (only in inpatients): without stress or with stress;
- Glycaemia (only in outpatients): glycosylated haemoglobin greater than 8% or glycosylated haemoglobin under 8%;
- Nutritional status: malnourished or normonourished;
- Side effects: no comorbidities, gastroparesis, pressure ulcer or kidney failure.
Appendix C
| Term | Definition |
|---|---|
| Cyclic administration | Administration at a constant rate of enteral nutrition (EN) with a pump for a period of 8–12 h. (it can be during the day with a break at night or vice versa) |
| Continuous administration | Administration at a constant rate of EN with a pump, without interruption over 24 h. (also acceptable if there is a 1–2 h break) |
| Bolus/intermittent administration | Bolus administration of EN in 3–6 doses per day. It can be with a syringe or by gravity, with a duration of 30 to 120 min per dose. |
| Degludec | Insulin analogue over more than 24 h. |
| Malnutrition | Clinical situation caused by a nutrient deficit (due to inadequate intake, increased losses, increased requirements, altered absorption and/or inflammation) that entails a change in body composition and that decreases physical and mental functions and has a negative impact on the clinical evolution of the patient. |
| Disease-related malnutrition | Malnutrition caused directly or indirectly by suffering from an acute, subacute or chronic disease. |
| Detemir | Long-acting insulin analogue (16–24 h) |
| Diarrhoea | Producing loose or liquid stools, three or more times a day (or with a greater than normal frequency for the person). |
| Distension | Feeling of fullness, nausea, bloating or abdominal pain, due to the accumulation of gas in the stomach and intestine, or accumulation of abdominal fluid. |
| Constipation/equivalent to chronic constipation | less than 3 bowel movements a week and/or hard stools in more than 25% of bowel movements, or a feeling of incomplete or very difficult defecations. |
| Low-fat formula | Enteral formula with fat content 5–20% of the total energy (TE). |
| High-calorie/high-protein diabetic formula | Complete polymeric enteral formula with density >1.2 Kcal/mL, protein content >18% of TE, which contains fermentable fibre in a high or exclusive proportion, low glycaemic index carbohydrates, and/or prebiotics (fructooligosaccharides (FOS), Inulin) and, frequently, a high content of monounsaturated fatty acids. |
| Normal-calorie/high-protein diabetic formula | Complete polymeric enteral formula with density >0.9 and <1.2 Kcal/mL, protein content ≥18% of TE, which contains fermentable fibre in a high or exclusive proportion, carbohydrates, which contain soluble fibre in a high or exclusive proportion. Low glycaemic index carbohydrates, and/or prebiotics (FOS, Inulin) and, frequently, a high content of monounsaturated fatty acids. |
| Normal-calorie/normal-protein diabetic formula | Complete polymeric enteral formula with density >0.9 and <1.2 Kcal/mL, protein content 11–18% of TE, which contains fermentable fibre in a high or exclusive proportion, low glycaemic index carbohydrates, and/or prebiotics (FOS, Inulin) and, frequently, a high content of monounsaturated fatty acids. |
| Standard formula | Complete polymeric enteral formula with density >0.9 and <1.2 Kcal/mL, protein content 11–18% of TE, which do not contain fibre. |
| Standard formula with fibre | Complete polymeric enteral formula with density >0.9 and <1.2 Kcal/mL, protein content 11–18% of TE, which contain fermentable, non-fermentable fibre or a mixture of fibres. |
| Immunomodulatory formula | Complete enteral formula, protein content >18% of TE, enriched to varying degrees with: glutamine, Omega-3 fatty acids, arginine, nucleotides, micronutrients. |
| Peptide formula | Complete oligomeric enteral formula, which contains hydrolysed proteins (peptides), in addition to carbohydrates, fats with high medium chain triglycerides (MCT) and micronutrient content. |
| VLCD(very low calorie diet) formulas | Omega-3 fatty acids, arginine, nucleotides, micronutrients. |
| Specific formulas | Complete enteral formula with a nutrient profile appropriate to metabolic situations or requirements of a specific pathology (diabetes and stress hyperglycaemia, nephropathy, liver disease, stress or immunosuppression, oncology, respiratory failure, cystic fibrosis). |
| Gastroparesis | Delayed gastric emptying observed in the absence of gastric obstruction, and accompanied by early satiety, nausea or vomiting, or abdominal pain. |
| Glargine U100 and U300 | Long-acting insulin analogue (U100 20–24 h U300 over 24 h). |
| Glinides or meglitinides | Group of oral hypoglycaemic drugs that increase insulin secretion. |
| HbA1c | Glycosylated haemoglobin. |
| Hyperglycaemia | Glycaemia ≥ 126 mg/dL. |
| Body Mass Index (BMI) | Degree of adiposity calculated according to the formula body weight (Kg)/height (m2). |
| Gastric infusion | EN infusion through a tube whose distal end is placed in the stomach. |
| Postpyloric infusion | Infusion of EN through a tube whose distal end is placed in the duodenum or jejunum. |
| Bolus and rescue insulin | Insulin administration in preset doses with established intervals (every 6–8 h, or prandial), adding a higher dose to the preset dose if glycaemia exceeds a preset limit. |
| Rapid-acting insulin | Regular insulin duration (5–7 h). |
| Ultra-rapid-acting insulin | Insulin analogues (Lispro, aspart, glulisine) duration (2–4 h). |
| Malabsorption | Signs and symptoms derived from a deficit in the intestinal absorption of nutrients. |
| Metformin | Oral hypoglycaemic drug from the biguanide group that reduces postprandial and basal glycaemia. |
| Normal nutrition | Normal nutritional status according to assessment scales such as subjective global assessment (SGA) or clinical and analytical assessment methods. |
| NPH | Intermediate-acting insulin (12–16 h). |
| Obesity | BMI ≥ 30 k/m2. |
| Outpatient | Patient who receives health care while living in the community (care home or private residence) and who comes to the medical or nursing appointment in person or virtually. |
| Inpatients | Patient who remains admitted to hospital for diagnosis or treatment. |
| Metabolic stress | Metabolic response to trauma, sepsis, surgery that is associated with increased energy expenditure and muscle catabolism manifested by hyperglycaemia increased urinary nitrogen losses and oxygen consumption. |
| Sulfonylurea | Group of oral hypoglycaemic drugs that increase insulin secretion and boost the action of insulin in extrapancreatic tissues. |
| Pressure ulcer | Localised area of damage to the skin and underlying tissues caused by pressure, friction, or a combination of both. |
Appendix D

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Appropriate Indication |
|---|
|
|
|
|
|
| Inappropriate Indication |
|
|
|
|
|
| Appropriate Indication |
|---|
|
|
| Inappropriate Indication |
|
|
| Appropriate Indication |
|---|
|
|
| Inappropriate Indication |
|
|
| Appropriate Indication |
|---|
|
|
|
|
| Inappropriate Indication |
|
|
|
|
|
|
| Appropriate Indication |
|---|
|
|
|
| Inappropriate Indication |
|
|
|
|
Appendix E
| Item | Result |
|---|---|
| Median (average) | 4.3 |
| Median absolute deviation | 1.0 |
| % Scenarios with agreement (n) | 90.4 (2706) |
| % Scenarios with disagreement (n) | 0.5 (14) |
| % Appropriate scenarios (n) | 23.7 (708) |
| % Inappropriate scenarios (n) | 12.7 (381) |
| % Uncertain scenarios (n) | 63.6 (1903) |
| Item | Result |
|---|---|
| Median (average) | 4.4 |
| Median absolute deviation | 1.0 |
| % Scenarios with agreement (n) | 83.7 (643) |
| % Scenarios with disagreement (n) | 1.0 (8) |
| % Appropriate scenarios (n) | 18.0 (138) |
| % Inappropriate scenarios (n) | 10.0 (77) |
| % Uncertain scenarios (n) | 72.0 (553) |
| Item | Result |
|---|---|
| Median (average) | 5.1 |
| Median absolute deviation | 0.5 |
| % Scenarios with agreement (n) | 69.1 (199) |
| % Scenarios with disagreement (n) | 0.0 (0) |
| % Appropriate scenarios (n) | 10.4 (30) |
| % Inappropriate scenarios (n) | 21.5 (62) |
| % Uncertain scenarios (n) | 68.1 (196) |
| Item | Result |
|---|---|
| Median (average) | 5.4 |
| Median absolute deviation | 3.0 |
| % Scenarios with agreement (n) | 84.9 (163) |
| % Scenarios with disagreement (n) | 3.1 (6) |
| % Appropriate scenarios (n) | 19.8 (38) |
| % Inappropriate scenarios (n) | 42.2 (73) |
| % Uncertain scenarios (n) | 38.2 (73) |
| Item | Result |
|---|---|
| Median (average) | 4.3 |
| Median absolute deviation | 1.5 |
| % Scenarios with agreement (n) | 98.1 (1083) |
| % Scenarios with disagreement (n) | 1.9 (21) |
| % Appropriate scenarios (n) | 25.6 (283) |
| % Inappropriate scenarios (n) | 12.0 (132) |
| % Uncertain scenarios (n) | 62.4 (689) |
| Item | Result |
|---|---|
| Median (average) | 3.7 |
| Median absolute deviation | 1.5 |
| % Scenarios with agreement (n) | 96.6 (618) |
| % Scenarios with disagreement (n) | 3.4 (22) |
| % Appropriate scenarios (n) | 4.5 (29) |
| % Inappropriate scenarios (n) | 61.3 (392) |
| % Uncertain scenarios (n) | 34.2 (219) |
References
- Marik, P.E.; Bellomo, R. Stress Hyperglycemia: An Essential Survival Response! Crit. Care Med. 2013, 41, e93–e94. [Google Scholar] [CrossRef] [PubMed]
- Cakir, M.; Altunbas, H.; Karayalcin, U.; Umpierrez, G.E.; Kitabchi, A.E. Hyperglycemia: An Independent Marker of in-Hospital Mortality in Patients with Undiagnosed Diabetes. J. Clin. Endocrinol. Metab. 2003, 88, 1402. [Google Scholar] [CrossRef] [PubMed]
- Olveira, G.; García-Luna, P.P.; Pereira, J.L.; Rebollo, I.; García-Almeida, J.M.; Serrano, P.; Irles, J.A.; Muñoz-Aguilar, A.; Molina, M.J.; Tapia, M.J. Recomendaciones Del Grupo GARIN Para El Manejo de Pacientes No Críticos Con Diabetes o Hiperglucemia de Estrés y Nutrición Artificial. Nutr. Hosp. 2012, 27, 1837–1849. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Paris, A.; Álvarez Hernández, J.; Ballesteros-Pomar, M.D.; Botella-Romero, F.; León-Sanz, M.; Martín-Palmero, Á.; Martínez Olmos, M.Á.; Olveira, G. Evidence-Based Recommendations and Expert Consensus on Enteral Nutrition in the Adult Patient with Diabetes Mellitus or Hyperglycemia. Nutrition 2017, 41, 58–67. [Google Scholar] [CrossRef]
- Abuín-Fernández, J.; Doulatram-Gamgaram, V.; Sánchez-Torralvo, F.; Contreras-Bolívar, V.; Padín, S.; Gonzalo-Marín, M.; Olveira, G. Prevalence of Diabetes Mellitus in Patients with Home Enteral Nutrition. Endocrinol. Diabetes Nutr. 2020, 67, 650–657. [Google Scholar] [CrossRef] [PubMed]
- González Infantino, C.A.; González, C.D.; Sánchez, R.; Presner, N. Hyperglycemia and Hypoalbuminemia as Prognostic Mortality Factors in Patients with Enteral Feeding. Nutrition 2013, 29, 497–501. [Google Scholar] [CrossRef] [PubMed]
- Laesser, C.I.; Cumming, P.; Reber, E.; Stanga, Z.; Muka, T.; Bally, L. Management of Glucose Control in Noncritically Ill, Hospitalized Patients Receiving Parenteral and/or Enteral Nutrition: A Systematic Review. J. Clin. Med. 2019, 8, 935. [Google Scholar] [CrossRef]
- Ojo, O.; Brooke, J. Evaluation of the Role of Enteral Nutrition in Managing Patients with Diabetes: A Systematic Review. Nutrients 2014, 6, 5142–5152. [Google Scholar] [CrossRef]
- Elia, M.; Ceriello, A.; Laube, H.; Sinclair, A.J.; Engfer, M.; Statton, R.J.; Stratton, R.J. Enteral Nutritional Support and Use of Diabetes-Specific Formulas for Patients. Diabetes Care 2005, 28, 2267–2279. [Google Scholar] [CrossRef]
- Brook, R.H. The RAND/UCLA Appropriateness Method. In Methodology Perspectives; AHCPR Pub. No. 95-0009; McCormick, K.A., Moore, S.R., Siegel, R.A., Eds.; Public Health Service, U.S. Department of Health and Human Services: Rockville, MD, USA, 1994; pp. 59–70. [Google Scholar]
- Fitch, K.; Bernstein, S.J.; Mcdonnell, J.; Kahan, J.P. The RAND/UCLA Appropriateness Method User’s Manual; RAND: Santa Mónica, CA, USA, 2001; ISBN 0833029185. Available online: http://www.rand.org (accessed on 17 October 2022).
- Olveira-Fuster, G.; Gonzalo-Marín, M. Fórmulas de Nutrición Enteral Para Personas Con Diabetes Mellitus. Endocrinol. Nutr. 2005, 52, 516–524. [Google Scholar] [CrossRef]
- Sanz-París, A.; Matía-Martín, P.; Martín-Palmero, Á.; Gómez-Candela, C.; Camprubi Robles, M. Diabetes-Specific Formulas High in Monounsaturated Fatty Acids and Metabolic Outcomes in Patients with Diabetes or Hyperglycaemia. A Systematic Review and Meta-Analysis. Clin. Nutr. 2020, 39, 3273–3282. [Google Scholar] [CrossRef]
- Fiaccadori, E.; Sabatino, A.; Barazzoni, R.; Carrero, J.J.; Cupisti, A.; De Waele, E.; Jonckheer, J.; Singer, P.; Cuerda, C. ESPEN Guideline on Clinical Nutrition in Hospitalized Patients with Acute or Chronic Kidney Disease. Clin. Nutr. 2021, 40, 1644–1668. [Google Scholar] [CrossRef]
- American Diabetes Association. 11. Microvascular Complications and Foot Care: Standards of Medical Care in Diabete-2020. Diabetes Care 2020, 43, S135–S151. [Google Scholar] [CrossRef] [PubMed]
- Mesejo, A.; Sánchez Álvarez, C.; Arboleda Sánchez, J.A. Recomendaciones Para El Soporte Nutricional y Metabólico Especializado Del Paciente Crítico. Actualización. Consenso SEMICYUC-SENPE: Paciente Obeso. Med. Intensiva 2011, 35, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Pohl, M.; Mayr, P.; Mertl-Roetzer, M.; Lauster, F.; Haslbeck, M.; Hipper, B.; Steube, D.; Tietjen, M.; Eriksen, J.; Rahlfs, V.W. Glycemic Control in Patients with Type 2 Diabetes Mellitus with a Disease-Specific Enteral Formula: Stage II of a Randomized, Controlled Multicenter Trial. J. Parenter. Enter. Nutr. 2009, 33, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Ojo, O.; Weldon, S.M.; Thompson, T.; Crockett, R.; Wang, X.H. The Effect of Diabetes-Specific Enteral Nutrition Formula on Cardiometabolic Parameters in Patients with Type 2 Diabetes: A Systematic Review and Meta–Analysis of Randomised Controlled Trials. Nutrients 2019, 11, 1905. [Google Scholar] [CrossRef]
- Maldonado, C.G.S. Nutrición Enteral: Concepto, Indicaciones, Vías, Formas de Administración, Material Necesario y Cuidados. In Manuel de Nutrición Clínica y Dietética; Gabriel Olveira Fuster; Diaz de Santos: Madrid, Spain, 2016; pp. 261–282. [Google Scholar]
- Davidson, P.; Kwiatkowski, C.A.; Wien, M. Management of Hyperglycemia and Enteral Nutrition in the Hospitalized Patient. Nutr. Clin. Pract. 2015, 30, 652–659. [Google Scholar] [CrossRef]
- Camilleri, M.; Parkman, H.P.; Shafi, M.A.; Abell, T.L.; Gerson, L. Clinical Guideline: Management of Gastroparesis. Am. J. Gastroenterol. 2013, 108, 18–37. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes—2022. Diabetes Care 2022, 45, S125–S143. [Google Scholar] [CrossRef]
- Peña, J.; Arenaza, A.; Benítez, M.; Gómez, C.; Borrego, M.; Fernández, A.; González, M.; Hernández, S. Guia de Administración de Medicamentos Por Sondas de Alimentación Enteral; Salud Madrid: Madrid, Spain, 2012; ISBN 9788469551141. [Google Scholar]
- American Diabetes Association Professional Practice Committee. 15. Diabetes Care in the Hospital: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 43, S193–S202. [Google Scholar] [CrossRef]
- Fatati, G.; Di Donato, A.; Grandone, I.; Menicocci, P.; Mirri, E.; Prosperini, G.; Scardapane, M.; Rossi, M.C.; Palazzi, M. Impact of Insulin Degludec in Hospitalized Patients with and without Type 2 Diabetes Requiring Parenteral/Enteral Nutrition: An Observational Study. Adv. Ther. 2018, 35, 809–816. [Google Scholar] [CrossRef] [PubMed]
- Wanden-Berghe, C.; Patino-Alonso, M.C.; Galindo-Villardón, P.; Sanz-Valero, J. Complications Associated with Enteral Nutrition: CAFANE Study. Nutrients 2019, 11, 2041. [Google Scholar] [CrossRef] [PubMed]
- Moraga-Mardones, F. Complicaciones De La Alimentación Enteral. Gastrohnup 2005, 7, 4–8. [Google Scholar]




| Appropriate | Inappropriate |
|---|---|
|
|
| Appropriate | Inappropriate |
|---|---|
|
|
| Appropriate | Inappropriate |
|---|---|
| The indications and routes of access for enteral nutrition in patients with hyperglycaemia are similar to those in patients without hyperglycaemia * | |
|
|
| Appropriate | Inappropriate | |
|---|---|---|
| Oral Antidiabetic Drugs |
|
|
| Insulin |
|
|
| Appropriate | Inappropriate | |
|---|---|---|
| Diarrhoea |
|
|
| Constipation |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rebollo-Pérez, M.I.; Florencio Ojeda, L.; García-Luna, P.P.; Irles Rocamora, J.A.; Olveira, G.; Lacalle Remigio, J.R.; Arraiza Irigoyen, C.; Calañas Continente, A.; Campos Martín, C.; Fernández Soto, M.L.; et al. Standards for the Use of Enteral Nutrition in Patients with Diabetes or Stress Hyperglycaemia: Expert Consensus. Nutrients 2023, 15, 4976. https://doi.org/10.3390/nu15234976
Rebollo-Pérez MI, Florencio Ojeda L, García-Luna PP, Irles Rocamora JA, Olveira G, Lacalle Remigio JR, Arraiza Irigoyen C, Calañas Continente A, Campos Martín C, Fernández Soto ML, et al. Standards for the Use of Enteral Nutrition in Patients with Diabetes or Stress Hyperglycaemia: Expert Consensus. Nutrients. 2023; 15(23):4976. https://doi.org/10.3390/nu15234976
Chicago/Turabian StyleRebollo-Pérez, María I., Luna Florencio Ojeda, Pedro P. García-Luna, José A. Irles Rocamora, Gabriel Olveira, Juan Ramón Lacalle Remigio, Carmen Arraiza Irigoyen, Alfonso Calañas Continente, Cristina Campos Martín, María Luisa Fernández Soto, and et al. 2023. "Standards for the Use of Enteral Nutrition in Patients with Diabetes or Stress Hyperglycaemia: Expert Consensus" Nutrients 15, no. 23: 4976. https://doi.org/10.3390/nu15234976