

Influence of Metabolic Dysregulation in the Management of Depressive Disorder—Narrative Review

 , , , , , ,
, , , , , , 
Abstract
1. Introduction
2. Factors of Mental Health
3. Pathophysiology
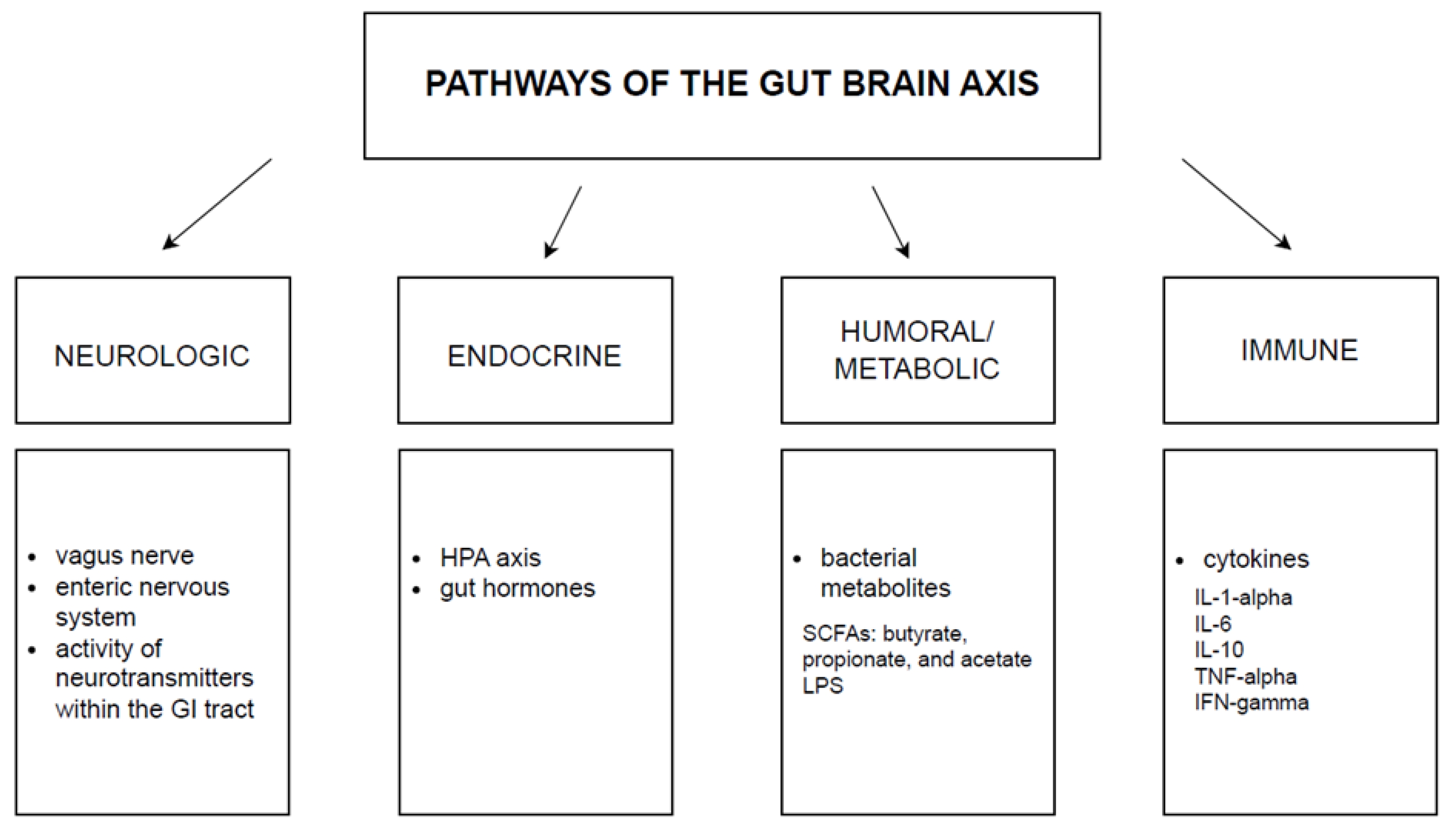
4. Gut-Brain Axis
5. Role of Diet
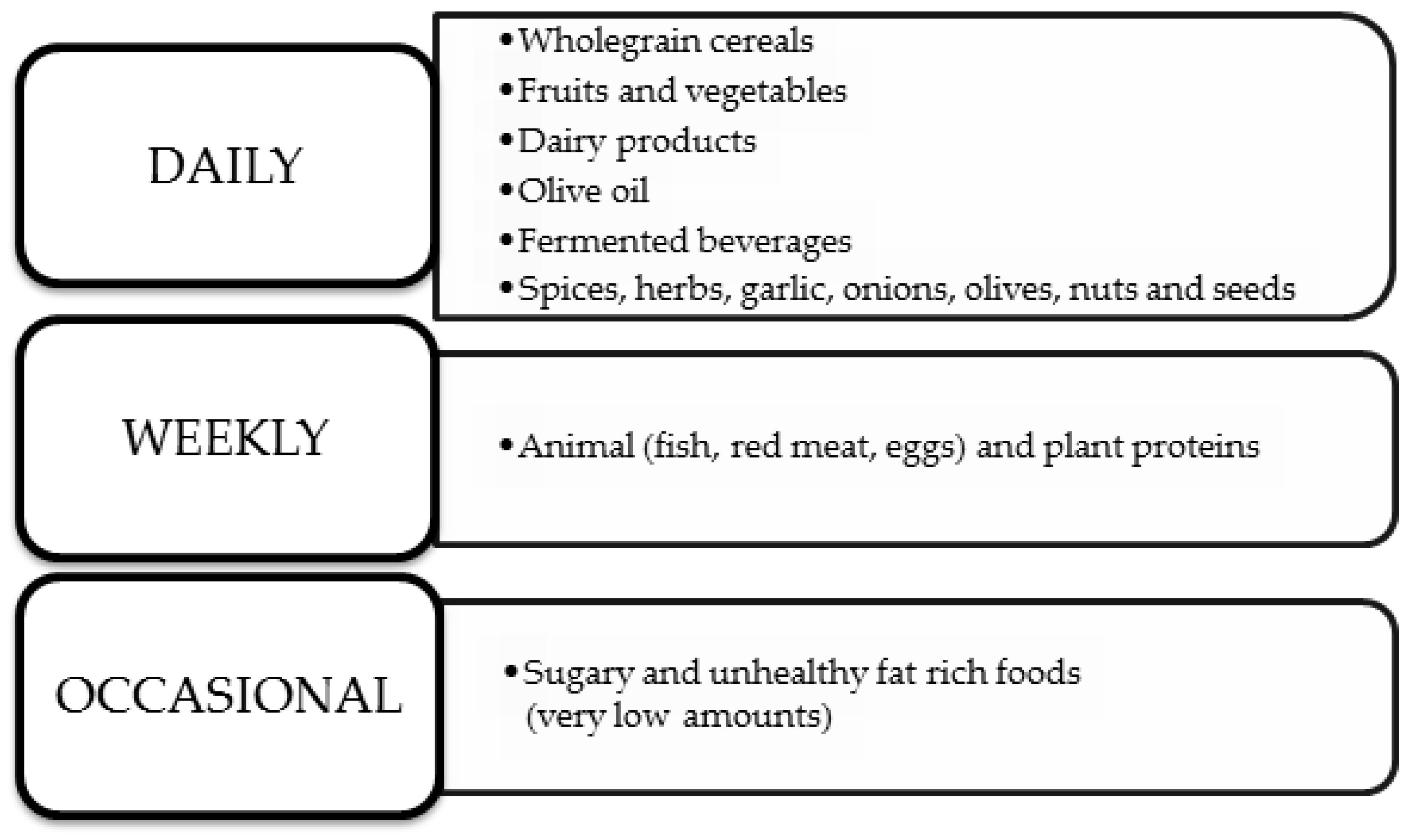
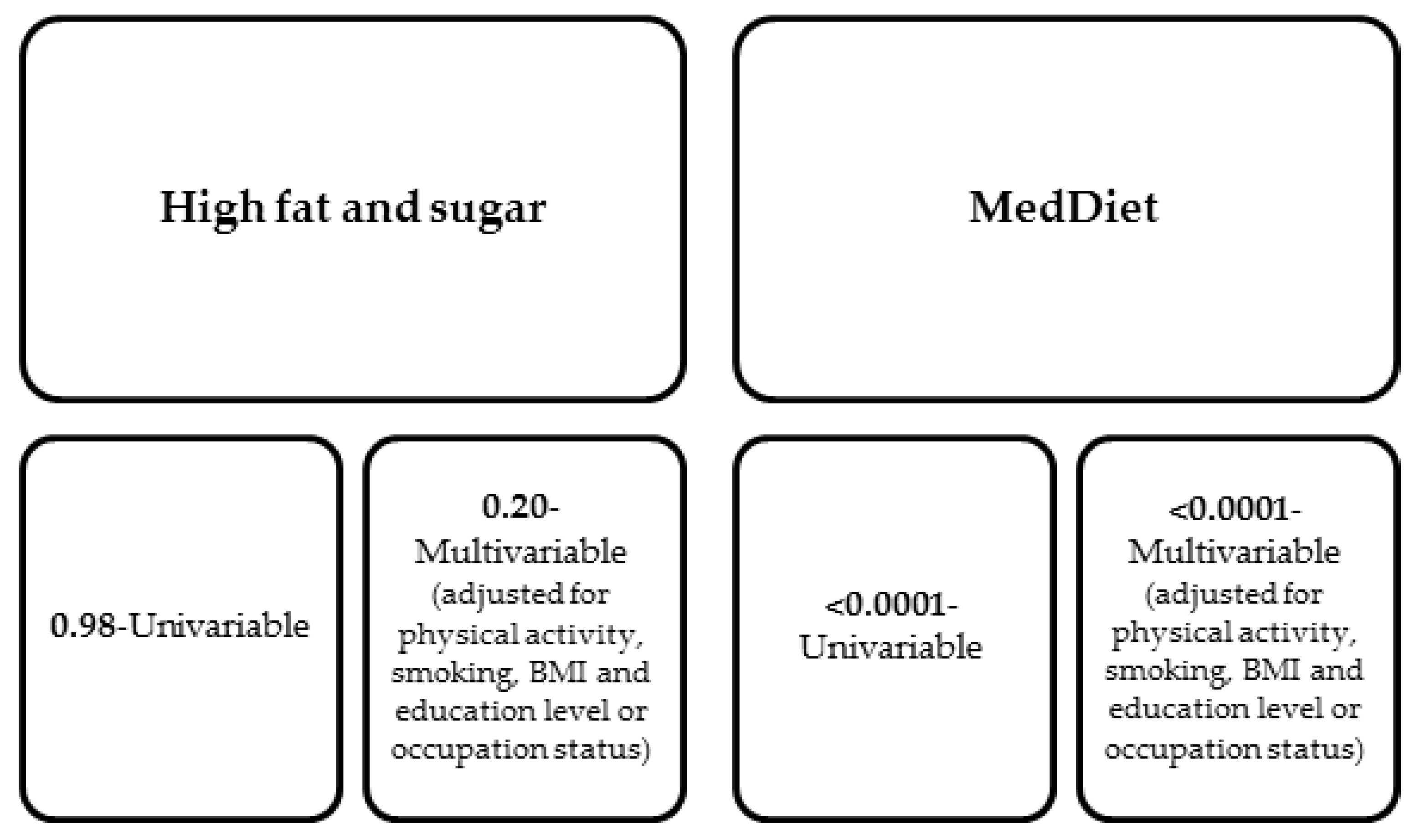
5.1. Mediterranean Diet
5.2. Anti-Inflammatory Diet
6. Physical Activity
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858, Erratum in Lancet 2019, 393, e44. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cheng, J.; Feng, Y.; Liu, Z.; Zheng, D.; Han, H.; Liu, N.; Liu, S.; Zhao, J.; Li, X.; Han, S. Knowledge, attitude, and practice of patients with major depressive disorder on exercise therapy. BMC Public Health 2024, 24, 323. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhdanava, M.; Pilon, D.; Ghelerter, I.; Chow, W.; Joshi, K.; Lefebvre, P.; Sheehan, J.J. The Prevalence and National Burden of Treatment-Resistant Depression and Major Depressive Disorder in the United States. J. Clin. Psychiatry 2021, 82, 20m13699. [Google Scholar] [CrossRef] [PubMed]
- Gartlehner, G.; Dobrescu, A.; Chapman, A.; Toromanova, A.; Emprechtinger, R.; Persad, E.; Affengruber, L.; Pieh, C.; Klerings, I.; Wagner, G. Nonpharmacologic and Pharmacologic Treatments of Adult Patients With Major Depressive Disorder: A Systematic Review and Network Meta-analysis for a Clinical Guideline by the American College of Physicians. Ann. Intern. Med. 2023, 176, 196–211. [Google Scholar] [CrossRef] [PubMed]
- Marasine, N.R.; Sankhi, S.; Lamichhane, R.; Marasini, N.R.; Dangi, N.B. Use of Antidepressants among Patients Diagnosed with Depression: A Scoping Review. Biomed Res. Int. 2021, 2021, 6699028. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Moraczewski, J.; Awosika, A.O.; Aedma, K.K. Tricyclic Antidepressants. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar] [PubMed]
- Niarchou, E.; Roberts, L.H.; Naughton, B.D. What is the impact of antidepressant side effects on medication adherence among adult patients diagnosed with depressive disorder: A systematic review. J. Psychopharmacol. 2024, 38, 127–136. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Marwaha, S.; Palmer, E.; Suppes, T.; Cons, E.; Young, A.H.; Upthegrove, R. Novel and emerging treatments for major depression. Lancet 2023, 401, 141–153. [Google Scholar] [CrossRef] [PubMed]
- Angelopoulou, E.; Bougea, A.; Hatzimanolis, A.; Stefanis, L.; Scarmeas, N.; Papageorgiou, S. Mild Behavioral Impairment in Parkinson’s Disease: An Updated Review on the Clinical, Genetic, Neuroanatomical, and Pathophysiological Aspects. Medicina 2024, 60, 115. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cui, L.; Li, S.; Wang, S.; Wu, X.; Liu, Y.; Yu, W.; Wang, Y.; Tang, Y.; Xia, M.; Li, B. Major depressive disorder: Hypothesis, mechanism, prevention and treatment. Signal Transduct. Target. Ther. 2024, 9, 30. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Caraci, F.; Spampinato, S.F.; Morgese, M.G.; Tascedda, F.; Salluzzo, M.G.; Giambirtone, M.C.; Caruso, G.; Munafò, A.; Torrisi, S.A.; Leggio, G.M.; et al. Neurobiological links between depression and AD: The role of TGF-β1 signaling as a new pharmacological target. Pharmacol. Res. 2018, 130, 374–384. [Google Scholar] [CrossRef] [PubMed]
- Benros, M.E.; Waltoft, B.L.; Nordentoft, M.; Østergaard, S.D.; Eaton, W.W.; Krogh, J.; Mortensen, P.B. Autoimmune Diseases and Severe Infections as Risk Factors for Mood Disorders: A Nationwide Study. JAMA Psychiatry 2013, 70, 812–820. [Google Scholar] [CrossRef] [PubMed]
- Clarke, D.M.; Currie, K.C. Depression, anxiety and their relationship with chronic diseases: A review of the epidemiology, risk and treatment evidence. Med. J. Aust. 2009, 190, S54–S60. [Google Scholar] [CrossRef] [PubMed]
- Piao, J.; Wang, Y.; Zhang, T.; Zhao, J.; Lv, Q.; Ruan, M.; Yu, Q.; Li, B. Antidepressant-like Effects of Representative Types of Food and Their Possible Mechanisms. Molecules 2023, 28, 6992. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Calcaterra, V.; Rossi, V.; Magenes, V.C.; Baldassarre, P.; Grazi, R.; Loiodice, M.; Fabiano, V.; Zuccotti, G. Dietary habits, depression and obesity: An intricate relationship to explore in pediatric preventive strategies. Front. Pediatr. 2024, 12, 1368283. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ross, R.E.; VanDerwerker, C.J.; Saladin, M.E.; Gregory, C.M. The role of exercise in the treatment of depression: Biological underpinnings and clinical outcomes. Mol. Psychiatry 2023, 28, 298–328. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kandola, A.; Ashdown-Franks, G.; Hendrikse, J.; Sabiston, C.M.; Stubbs, B. Physical activity and depression: Towards understanding the antidepressant mechanisms of physical activity. Neurosci. Biobehav. Rev. 2019, 107, 525–539. [Google Scholar] [CrossRef] [PubMed]
- Marazziti, D.; Avella, M.T.; Mucci, N.; Della Vecchia, A.; Ivaldi, T.; Palermo, S.; Mucci, F. Impact of economic crisis on mental health: A 10-year challenge. CNS Spectr. 2021, 26, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Pavlidi, P.; Kokras, N.; Dalla, C. Sex Differences in Depression and Anxiety. Curr. Top. Behav. Neurosci. 2023, 62, 103–132. [Google Scholar] [CrossRef] [PubMed]
- Altemus, M.; Sarvaiya, N.; Neill Epperson, C. Sex differences in anxiety and depression clinical perspectives. Front. Neuroendocrinol. 2014, 35, 320–330. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sarris, J.; O’Neil, A.; Coulson, C.E.; Schweitzer, I.; Berk, M. Lifestyle medicine for depression. BMC Psychiatry 2014, 14, 107. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ibarra-Rovillard, M.S.; Kuiper, N.A. Social support and social negativity findings in depression: Perceived responsiveness to basic psychological needs. Clin. Psychol. Rev. 2011, 31, 342–352. [Google Scholar] [CrossRef] [PubMed]
- Milaneschi, Y.; Simmons, W.K.; van Rossum, E.F.C.; Penninx, B.W. Depression and obesity: Evidence of shared biological mechanisms. Mol. Psychiatry 2019, 24, 18–33. [Google Scholar] [CrossRef] [PubMed]
- Usmani, Z.A.; Chai-Coetzer, C.L.; Antic, N.A.; McEvoy, R.D. Obstructive sleep apnoea in adults. Postgrad. Med. J. 2013, 89, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Sforza, E.; Chouchou, F.; Collet, P.; Pichot, V.; Barthélémy, J.C.; Roche, F. Sex differences in obstructive sleep apnoea in an elderly French population. Eur. Respir. J. 2011, 37, 1137–1143. [Google Scholar] [CrossRef] [PubMed]
- Kurhe, Y.; Mahesh, R. Mechanisms linking depression co-morbid with obesity: An approach for serotonergic type 3 receptor antagonist as novel therapeutic intervention. Asian J. Psychiatr. 2015, 17, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Lopresti, A.L.; Drummond, P.D. Obesity and psychiatric disorders: Commonalities in dysregulated biological pathways and their implications for treatment. Prog. Neuropsychopharmacol. Biol. Psychiatry 2013, 45, 92–99. [Google Scholar] [CrossRef] [PubMed]
- McLachlan, C.; Shelton, R.; Li, L. Obesity, inflammation, and depression in adolescents. Front. Psychiatry 2023, 14, 1221709. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Miller, G.E.; Freedland, K.E.; Carney, R.M.; Stetler, C.A.; Banks, W.A. Pathways linking depression, adiposity, and inflammatory markers in healthy young adults. Brain Behav. Immun. 2003, 17, 276–285. [Google Scholar] [CrossRef] [PubMed]
- Chaves Filho, A.J.M.; Lima, C.N.C.; Vasconcelos, S.M.M.; de Lucena, D.F.; Maes, M.; Macedo, D. IDO chronic immune activation and tryptophan metabolic pathway: A potential pathophysiological link between depression and obesity. Prog. Neuropsychopharmacol. Biol. Psychiatry 2018, 80 Pt C, 234–249. [Google Scholar] [CrossRef] [PubMed]
- André, C.; Dinel, A.L.; Ferreira, G.; Layé, S.; Castanon, N. Diet-induced obesity progressively alters cognition, anxiety-like behavior and lipopolysaccharide-induced depressive-like behavior: Focus on brain indoleamine 2,3-dioxygenase activation. Brain Behav. Immun. 2014, 41, 10–21. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.K.; Leslie, S.M.; Packer, M.M.; Zaiko, Y.V.; Phillips, O.R.; Weisman, E.F.; Wall, D.M.; Jo, B.; Rasgon, N. Brain and behavioral correlates of insulin resistance in youth with depression and obesity. Horm. Behav. 2019, 108, 73–83. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Patist, C.M.; Stapelberg, N.J.C.; Du Toit, E.F.; Headrick, J.P. The brain-adipocyte-gut network: Linking obesity and depression subtypes. Cogn. Affect. Behav. Neurosci. 2018, 18, 1121–1144. [Google Scholar] [CrossRef] [PubMed]
- Nemiary, D.; Shim, R.; Mattox, G.; Holden, K. The Relationship Between Obesity and Depression Among Adolescents. Psychiatr. Ann. 2012, 42, 305–308. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Du, F.M.; Kuang, H.Y.; Duan, B.H.; Liu, D.N.; Yu, X.Y. Effects of thyroid hormone and depression on common components of central obesity. J. Int. Med. Res. 2019, 47, 3040–3049. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sevilla-González, M.D.R.; Quintana-Mendoza, B.M.; Aguilar-Salinas, C.A. Interaction Between Depression, Obesity, and Type 2 Diabetes: A Complex Picture. Arch. Med. Res. 2017, 48, 582–591. [Google Scholar] [CrossRef] [PubMed]
- Gomes, A.P.; Soares, A.L.G.; Menezes, A.M.B.; Assunção, M.C.; Wehrmeister, F.C.; Howe, L.D.; Gonçalves, H. Adiposity, depression and anxiety: Interrelationship and possible mediators. Rev. Saude Publica 2019, 53, 103. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Vogelzangs, N.; Kritchevsky, S.B.; Beekman, A.T.; Brenes, G.A.; Newman, A.B.; Satterfield, S.; Yaffe, K.; Harris, T.B.; Penninx, B.W.; Health ABC Study. Obesity and onset of significant depressive symptoms: Results from a prospective community-based cohort study of older men and women. J. Clin. Psychiatry 2010, 71, 391–399. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wiltink, J.; Michal, M.; Wild, P.S.; Zwiener, I.; Blettner, M.; Münzel, T.; Schulz, A.; Kirschner, Y.; Beutel, M.E. Associations between depression and different measures of obesity (BMI, WC, WHtR, WHR). BMC Psychiatry 2013, 13, 223. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chang, L.; Wei, Y.; Hashimoto, K. Brain-gut-microbiota axis in depression: A historical overview and future directions. Brain Res. Bull. 2022, 182, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Generoso, J.S.; Giridharan, V.V.; Lee, J.; Macedo, D.; Barichello, T. The role of the microbiota-gut-brain axis in neuropsychiatric disorders. Braz. J. Psychiatry 2021, 43, 293–305. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Appleton, J. The Gut-Brain Axis: Influence of Microbiota on Mood and Mental Health. Integr. Med. 2018, 17, 28–32. [Google Scholar] [PubMed] [PubMed Central]
- Cryan, J.F.; O’Riordan, K.J.; Cowan, C.S.M.; Sandhu, K.V.; Bastiaanssen, T.F.S.; Boehme, M.; Codagnone, M.G.; Cussotto, S.; Fulling, C.; Golubeva, A.V.; et al. The Microbiota-Gut-Brain Axis. Physiol. Rev. 2019, 99, 1877–2013. [Google Scholar] [CrossRef] [PubMed]
- Dinan, T.G.; Stanton, C.; Cryan, J.F. Psychobiotics: A novel class of psychotropic. Biol. Psychiatry 2013, 74, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Zagórska, A.; Marcinkowska, M.; Jamrozik, M.; Wiśniowska, B.; Paśko, P. From probiotics to psychobiotics—The gut-brain axis in psychiatric disorders. Benef. Microbes 2020, 11, 717–732. [Google Scholar] [CrossRef] [PubMed]
- Chahwan, B.; Kwan, S.; Isik, A.; van Hemert, S.; Burke, C.; Roberts, L. Gut feelings: A randomised, triple-blind, placebo-controlled trial of probiotics for depressive symptoms. J. Affect. Disord. 2019, 253, 317–326. [Google Scholar] [CrossRef] [PubMed]
- Schwarcz, R.; Bruno, J.P.; Muchowski, P.J.; Wu, H.Q. Kynurenines in the mammalian brain: When physiology meets pathology. Nat. Rev. Neurosci. 2012, 13, 465–477. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Braniste, V.; Al-Asmakh, M.; Kowal, C.; Anuar, F.; Abbaspour, A.; Tóth, M.; Korecka, A.; Bakocevic, N.; Ng, L.G.; Kundu, P.; et al. The gut microbiota influences blood-brain barrier permeability in mice. Sci. Transl. Med. 2014, 6, 263ra158, Erratum in Sci. Transl. Med. 2014, 6, 266er7. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Caspani, G.; Kennedy, S.; Foster, J.A.; Swann, J. Gut microbial metabolites in depression: Understanding the biochemical mechanisms. Microb. Cell 2019, 6, 454–481. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Naseribafrouei, A.; Hestad, K.; Avershina, E.; Sekelja, M.; Linløkken, A.; Wilson, R.; Rudi, K. Correlation between the human fecal microbiota and depression. Neurogastroenterol. Motil. 2014, 26, 1155–1162. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Ling, Z.; Zhang, Y.; Mao, H.; Ma, Z.; Yin, Y.; Wang, W.; Tang, W.; Tan, Z.; Shi, J.; et al. Altered fecal microbiota composition in patients with major depressive disorder. Brain Behav. Immun. 2015, 48, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Zheng, P.; Zeng, B.; Zhou, C.; Liu, M.; Fang, Z.; Xu, X.; Zeng, L.; Chen, J.; Fan, S.; Du, X.; et al. Gut microbiome remodeling induces depressive-like behaviors through a pathway mediated by the host’s metabolism. Mol. Psychiatry 2016, 21, 786–796. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.E.; Chen, H.C.; Chou, H.L.; Chen, I.M.; Lee, M.S.; Chuang, L.C.; Liu, Y.W.; Lu, M.L.; Chen, C.H.; Wu, C.S.; et al. Exploration of microbiota targets for major depressive disorder and mood related traits. J. Psychiatr. Res. 2019, 111, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, A.; Lehto, S.M.; Harty, S.; Dinan, T.G.; Cryan, J.F.; Burnet, P.W.J. Psychobiotics and the Manipulation of Bacteria-Gut-Brain Signals. Trends Neurosci. 2016, 39, 763–781. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kelly, J.R.; Borre, Y.; O’ Brien, C.; Patterson, E.; El Aidy, S.; Deane, J.; Kennedy, P.J.; Beers, S.; Scott, K.; Moloney, G.; et al. Transferring the blues: Depression-associated gut microbiota induces neurobehavioural changes in the rat. J. Psychiatr. Res. 2016, 82, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Mörkl, S.; Butler, M.I.; Holl, A.; Cryan, J.F.; Dinan, T.G. Probiotics and the Microbiota-Gut-Brain Axis: Focus on Psychiatry. Curr. Nutr. Rep. 2020, 9, 171–182, Erratum in Curr. Nutr. Rep. 2020, 9, 183. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Burokas, A.; Arboleya, S.; Moloney, R.D.; Peterson, V.L.; Murphy, K.; Clarke, G.; Stanton, C.; Dinan, T.G.; Cryan, J.F. Targeting the Microbiota-Gut-Brain Axis: Prebiotics Have Anxiolytic and Antidepressant-like Effects and Reverse the Impact of Chronic Stress in Mice. Biol. Psychiatry 2017, 82, 472–487. [Google Scholar] [CrossRef] [PubMed]
- Savignac, H.M.; Corona, G.; Mills, H.; Chen, L.; Spencer, J.P.; Tzortzis, G.; Burnet, P.W. Prebiotic feeding elevates central brain derived neurotrophic factor, N-methyl-D-aspartate receptor subunits and D-serine. Neurochem. Int. 2013, 63, 756–764. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Berrington de Gonzalez, A.; Hartge, P.; Cerhan, J.R.; Flint, A.J.; Hannan, L.; MacInnis, R.J.; Moore, S.C.; Tobias, G.S.; Anton-Culver, H.; Freeman, L.B.; et al. Body-mass index and mortality among 1.46 million white adults. N. Engl. J. Med. 2010, 363, 2211–2219, Erratum in N. Engl. J. Med. 2011, 365, 869. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- World Health Organization. Obesity and Overweight Fact Sheet; World Health Organization: Geneva, Switzerland, 2021; Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 1 March 2024).
- Martinez, J.A. Body-weight regulation: Causes of obesity. Proc. Nutr. Soc. 2000, 59, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Paris, T.; Daly, R.M.; Abbott, G.; Sood, S.; Freer, C.L.; Ryan, M.C.; George, E.S. Diet Overall and Hypocaloric Diets Are Associated With Improvements in Depression but Not Anxiety in People With Metabolic Conditions: A Systematic Review and Meta-Analysis. Adv. Nutr. 2024, 15, 100169. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lobstein, T.; Jackson-Leach, R.; Moodie, M.L.; Hall, K.D.; Gortmaker, S.L.; Swinburn, B.A.; James, W.P.; Wang, Y.; McPherson, K. Child and adolescent obesity: Part of a bigger picture. Lancet 2015, 385, 2510–2520. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- WHO Consultation on Obesity; World Health Organization. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation; World Health Organization: Geneva, Switzerland, 2000; Available online: https://iris.who.int/handle/10665/42330 (accessed on 10 March 2024).
- Luppino, F.S.; de Wit, L.M.; Bouvy, P.F.; Stijnen, T.; Cuijpers, P.; Penninx, B.W.; Zitman, F.G. Overweight, obesity, and depression: A systematic review and meta-analysis of longitudinal studies. Arch. Gen. Psychiatry 2010, 67, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Lamers, F.; Vogelzangs, N.; Merikangas, K.R.; de Jonge, P.; Beekman, A.T.; Penninx, B.W. Evidence for a differential role of HPA-axis function, inflammation and metabolic syndrome in melancholic versus atypical depression. Mol. Psychiatry 2013, 18, 692–699. [Google Scholar] [CrossRef] [PubMed]
- Kearney, J. Food consumption trends and drivers. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2010, 365, 2793–2807. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Manore, M.M. Exercise and the Institute of Medicine recommendations for nutrition. Curr. Sports Med. Rep. 2005, 4, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Speakman, J.R. Use of high-fat diets to study rodent obesity as a model of human obesity. Int. J. Obes. 2019, 43, 1491–1492. [Google Scholar] [CrossRef] [PubMed]
- Eskelinen, M.H.; Ngandu, T.; Helkala, E.L.; Tuomilehto, J.; Nissinen, A.; Soininen, H.; Kivipelto, M. Fat intake at midlife and cognitive impairment later in life: A population-based CAIDE study. Int. J. Geriatr. Psychiatry 2008, 23, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Gibson, E.L.; Barr, S.; Jeanes, Y.M. Habitual fat intake predicts memory function in younger women. Front. Hum. Neurosci. 2013, 7, 838. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Patsalos, O.; Keeler, J.; Schmidt, U.; Penninx, B.W.J.H.; Young, A.H.; Himmerich, H. Diet, Obesity, and Depression: A Systematic Review. J. Pers Med. 2021, 11, 176. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Applewhite, B.; Penninx, B.W.J.H.; Young, A.H.; Schmidt, U.; Himmerich, H.; Keeler, J.L. The effect of a low-calorie diet on depressive symptoms in individuals with overweight or obesity: A systematic review and meta-analysis of interventional studies. Psychol. Med. 2024, 54, 1671–1683. [Google Scholar] [CrossRef] [PubMed]
- Brinkworth, G.D.; Luscombe-Marsh, N.D.; Thompson, C.H.; Noakes, M.; Buckley, J.D.; Wittert, G.; Wilson, C.J. Long-term effects of very low-carbohydrate and high-carbohydrate weight-loss diets on psychological health in obese adults with type 2 diabetes: Randomized controlled trial. J. Intern. Med. 2016, 280, 388–397. [Google Scholar] [CrossRef] [PubMed]
- Akbaraly, T.N.; Brunner, E.J.; Ferrie, J.E.; Marmot, M.G.; Kivimaki, M.; Singh-Manoux, A. Dietary pattern and depressive symptoms in middle age. Br. J. Psychiatry 2009, 195, 408–413. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Davis, C.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the Mediterranean Diet; a Literature Review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kiani, A.K.; Medori, M.C.; Bonetti, G.; Aquilanti, B.; Velluti, V.; Matera, G.; Iaconelli, A.; Stuppia, L.; Connelly, S.T.; Herbst, K.L.; et al. Modern vision of the Mediterranean diet. J. Prev. Med. Hyg. 2022, 63 (Suppl. 3), E36–E43. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Naureen, Z.; Bonetti, G.; Medori, M.C.; Aquilanti, B.; Velluti, V.; Matera, G.; Iaconelli, A.; Bertelli, M. Foods of the Mediterranean diet: Lacto-fermented food, the food pyramid and food combinations. J. Prev. Med. Hyg. 2022, 63 (Suppl. 3), E28–E35. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Widmer, R.J.; Flammer, A.J.; Lerman, L.O.; Lerman, A. The Mediterranean diet, its components, and cardiovascular disease. Am. J. Med. 2015, 128, 229–238. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yin, W.; Löf, M.; Chen, R.; Hultman, C.M.; Fang, F.; Sandin, S. Mediterranean diet and depression: A population-based cohort study. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 153. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Marx, W.; Lane, M.; Hockey, M.; Aslam, H.; Berk, M.; Walder, K.; Borsini, A.; Firth, J.; Pariante, C.M.; Berding, K.; et al. Diet and depression: Exploring the biological mechanisms of action. Mol. Psychiatry 2021, 26, 134–150. [Google Scholar] [CrossRef] [PubMed]
- Parletta, N.; Zarnowiecki, D.; Cho, J.; Wilson, A.; Bogomolova, S.; Villani, A.; Itsiopoulos, C.; Niyonsenga, T.; Blunden, S.; Meyer, B.; et al. A Mediterranean-style dietary intervention supplemented with fish oil improves diet quality and mental health in people with depression: A randomized controlled trial (HELFIMED). Nutr. Neurosci. 2019, 22, 474–487. [Google Scholar] [CrossRef] [PubMed]
- Zarnowiecki, D.; Cho, J.; Wilson, A.; Bogomolova, S.; Villani, A.; Itsiopoulos, C.; Niyonsenga, T.; O’Dea, K.; Blunden, S.; Meyer, B.; et al. A 6-month randomised controlled trial investigating effects of Mediterranean-style diet and fish oil supplementation on dietary behaviour change, mental and cardiometabolic health and health-related quality of life in adults with depression (HELFIMED): Study protocol. BMC Nutr. 2016, 2, e132. [Google Scholar] [CrossRef]
- Murphy, K.J.; Parletta, N. Implementing a Mediterranean-Style Diet Outside the Mediterranean Region. Curr. Atheroscler. Rep. 2018, 20, 28. [Google Scholar] [CrossRef] [PubMed]
- Bogomolova, S.; Zarnowiecki, D.; Wilson, A.; Fielder, A.; Procter, N.; Itsiopoulos, C.; O’Dea, K.; Strachan, J.; Ballestrin, M.; Champion, A.; et al. Dietary intervention for people with mental illness in South Australia. Health Promot. Int. 2018, 33, 71–83. [Google Scholar] [CrossRef] [PubMed]
- Rienks, J.; Dobson, A.J.; Mishra, G.D. Mediterranean dietary pattern and prevalence and incidence of depressive symptoms in mid-aged women: Results from a large community-based prospective study. Eur. J. Clin. Nutr. 2012, 67, 75–82. [Google Scholar] [CrossRef]
- Tolkien, K.; Bradburn, S.; Murgatroyd, C. An anti-inflammatory diet as a potential intervention for depressive disorders: A systematic review and meta-analysis. Clin. Nutr. 2019, 38, 2045–2052. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Shao, H.; Zhang, X.; Qin, B. Hesperidin Alleviates Lipopolysaccharide-Induced Neuroinflammation in Mice by Promoting the miRNA-132 Pathway. Inflammation 2016, 39, 1681–1689. [Google Scholar] [CrossRef] [PubMed]
- Maleki, S.J.; Crespo, J.F.; Cabanillas, B. Anti-inflammatory effects of flavonoids. Food Chem. 2019, 299, 125124. [Google Scholar] [CrossRef] [PubMed]
- Bellavite, P. Neuroprotective Potentials of Flavonoids: Experimental Studies and Mechanisms of Action. Antioxidants 2023, 12, 280. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pei, R.; Liu, X.; Bolling, B. Flavonoids and gut health. Curr. Opin. Biotechnol. 2020, 61, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Salehi, B.; Cruz-Martins, N.; Butnariu, M.; Sarac, I.; Bagiu, I.C.; Ezzat, S.M.; Wang, J.; Koay, A.; Sheridan, H.; Adetunji, C.O.; et al. Hesperetin’s health potential: Moving from preclinical to clinical evidence and bioavailability issues, to upcoming strategies to overcome current limitations. Crit. Rev. Food Sci. Nutr. 2022, 62, 4449–4464. [Google Scholar] [CrossRef] [PubMed]
- Muhammad, T.; Ikram, M.; Ullah, R.; Rehman, S.U.; Kim, M.O. Hesperetin, a Citrus Flavonoid, Attenuates LPS-Induced Neuroinflammation, Apoptosis and Memory Impairments by Modulating TLR4/NF-κB Signaling. Nutrients 2019, 11, 648. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fusar-Poli, L.; Vozza, L.; Gabbiadini, A.; Vanella, A.; Concas, I.; Tinacci, S.; Petralia, A.; Signorelli, M.S.; Aguglia, E. Curcumin for depression: A meta-analysis. Crit. Rev. Food Sci. Nutr. 2020, 60, 2643–2653. [Google Scholar] [CrossRef] [PubMed]
- Kotha, R.R.; Luthria, D.L. Curcumin: Biological, Pharmaceutical, Nutraceutical, and Analytical Aspects. Molecules 2019, 24, 2930. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar] [PubMed] [PubMed Central]
- Dishman, R.K.; O’Connor, P.J. Lessons in exercise neurobiology: The case of endorphins. Ment. Health Phys. Act. 2009, 2, 4–9. [Google Scholar] [CrossRef]
- Kleim, J.A.; Cooper, N.R.; VandenBerg, P.M. Exercise induces angiogenesis but does not alter movement representations within rat motor cortex. Brain Res. 2002, 934, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Duclos, M.; Gouarne, C.; Bonnemaison, D. Acute and chronic effects of exercise on tissue sensitivity to glucocorticoids. J. Appl. Physiol. 2003, 94, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Knapen, J.; Vancampfort, D.; Moriën, Y.; Marchal, Y. Exercise therapy improves both mental and physical health in patients with major depression. Disabil Rehabil. 2015, 37, 1490–1495. [Google Scholar] [CrossRef] [PubMed]
- Schuch, F.B.; Vancampfort, D.; Richards, J.; Rosenbaum, S.; Ward, P.B.; Stubbs, B. Exercise as a treatment for depression: A meta-analysis adjusting for publication bias. J. Psychiatr. Res. 2016, 77, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.B. Depression, heart rate related variables and cardiovascular disease. Int. J. Psychophysiol. 2010, 78, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Pearce, M.; Garcia, L.; Abbas, A.; Strain, T.; Schuch, F.B.; Golubic, R.; Kelly, P.; Khan, S.; Utukuri, M.; Laird, Y.; et al. Association Between Physical Activity and Risk of Depression: A Systematic Review and Meta-analysis. JAMA Psychiatry 2022, 79, 550–559. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Busch, A.M.; Ciccolo, J.T.; Puspitasari, A.J.; Nosrat, S.; Whitworth, J.W.; Stults-Kolehmainen, M. Preferences for Exercise as a Treatment for Depression. Ment. Health Phys. Act 2016, 10, 68–72. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Seo, E.Y.; Kim, Y.S.; Lee, Y.J.; Hur, M.H. Virtual Reality Exercise Program Effects on Body Mass Index, Depression, Exercise Fun and Exercise Immersion in Overweight Middle-Aged Women: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2023, 20, 900. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Huang, B.; Huang, Z.; Tan, J.; Xu, H.; Deng, K.; Cheng, J.; Ren, Z.; Gong, X.; Gao, Y. The mediating and interacting role of physical activity and sedentary behavior between diabetes and depression in people with obesity in United States. J. Diabetes Complicat. 2021, 35, 107764. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, J.A.; Schuch, F.B.; Tonello, L.; Meneghel Vargas, K.F.; Oliveira-Junior, S.A.; Müller, P.T.; Boullosa, D. Effectiveness of short sprint interval training in women with major depressive disorder: A proof-of-concept study. Front. Psychiatry 2024, 15, 1356559. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Verhoeven, J.E.; Han, L.K.M.; Lever-van Milligen, B.A.; Hu, M.X.; Révész, D.; Hoogendoorn, A.W.; Batelaan, N.M.; van Schaik, D.J.F.; van Balkom, A.J.L.M.; van Oppen, P.; et al. Antidepressants or running therapy: Comparing effects on mental and physical health in patients with depression and anxiety disorders. J. Affect. Disord. 2023, 329, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Migueles, J.H.; Cadenas-Sanchez, C.; Lubans, D.R.; Henriksson, P.; Torres-Lopez, L.V.; Rodriguez-Ayllon, M.; Plaza-Florido, A.; Gil-Cosano, J.J.; Henriksson, H.; Escolano-Margarit, M.V.; et al. Effects of an Exercise Program on Cardiometabolic and Mental Health in Children with Overweight or Obesity: A Secondary Analysis of a Randomized Clinical Trial. JAMA Netw. Open 2023, 6, e2324839. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Holmquist, S.; Mattsson, S.; Schele, I.; Nordström, P.; Nordström, A. Low physical activity as a key differentiating factor in the potential high-risk profile for depressive symptoms in older adults. Depress Anxiety 2017, 34, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Ayllon, M.; Cadenas-Sánchez, C.; Estévez-López, F.; Muñoz, N.E.; Mora-Gonzalez, J.; Migueles, J.H.; Molina-García, P.; Henriksson, H.; Mena-Molina, A.; Martínez-Vizcaíno, V.; et al. Role of Physical Activity and Sedentary Behavior in the Mental Health of Preschoolers, Children and Adolescents: A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 1383–1410. [Google Scholar] [CrossRef] [PubMed]
- Currie, K.D.; Thomas, S.G.; Goodman, J.M. Effects of short-term endurance exercise training on vascular function in young males. Eur. J. Appl. Physiol. 2009, 107, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, K.; Sugawara, J.; Komine, H.; Maeda, S.; Yokoi, T. Effects of aerobic exercise training on the stiffness of central and peripheral arteries in middle-aged sedentary men. Jpn J. Physiol. 2005, 55, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Farpour-Lambert, N.J.; Aggoun, Y.; Marchand, L.M.; Martin, X.E.; Herrmann, F.R.; Beghetti, M. Physical activity reduces systemic blood pressure and improves early markers of atherosclerosis in pre-pubertal obese children. J. Am. Coll. Cardiol. 2009, 54, 2396–2406. [Google Scholar] [CrossRef] [PubMed]
- Labayen, I.; Medrano, M.; Arenaza, L.; Maíz, E.; Osés, M.; Martínez-Vizcaíno, V.; Ruiz, J.R.; Ortega, F.B. Effects of Exercise in Addition to a Family-Based Lifestyle Intervention Program on Hepatic Fat in Children With Overweight. Diabetes Care 2020, 43, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Herouvi, D.; Karanasios, E.; Karayianni, C.; Karavanaki, K. Cardiovascular disease in childhood: The role of obesity. Eur. J. Pediatr. 2013, 172, 721–732. [Google Scholar] [CrossRef] [PubMed]
- Franks, P.W.; Hanson, R.L.; Knowler, W.C.; Sievers, M.L.; Bennett, P.H.; Looker, H.C. Childhood obesity, other cardiovascular risk factors, and premature death. N. Engl. J. Med. 2010, 362, 485–493. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chen, Y.; Chen, Z.; Pan, L.; Ma, Z.M.; Zhang, H.; Li, X.J.; Li, X. Effect of Moderate and Vigorous Aerobic Exercise on Incident Diabetes in Adults with Obesity: A 10-Year Follow-up of a Randomized Clinical Trial. JAMA Intern. Med. 2023, 183, 272–275. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Oliveira-Silva, I.; Medeiros, A.R.; Donato, A.N.A.; Schuch, F.B.; Donath, L.; Boullosa, D. Prediction of Depression Scores from Aerobic Fitness, Body Fatness, Physical Activity, and Vagal Indices in Non-exercising, Female Workers. Front. Psychiatry 2019, 10, 192. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Carraça, E.V.; Encantado, J.; Battista, F.; Beaulieu, K.; Blundell, J.E.; Busetto, L.; van Baak, M.; Dicker, D.; Ermolao, A.; Farpour-Lambert, N.; et al. Effect of exercise training on psychological outcomes in adults with overweight or obesity: A systematic review and meta-analysis. Obes. Rev. 2021, 22 (Suppl. 4), e13261. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Thompson, P.D.; Buchner, D.; Piña, I.L.; Balady, G.J.; Williams, M.A.; Marcus, B.H.; Berra, K.; Blair, S.N.; Costa, F.; Franklin, B.; et al. Exercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular disease: A statement from the Council on Clinical Cardiology (Subcommittee on Exercise, Rehabilitation, and Prevention) and the Council on Nutrition, Physical Activity, and Metabolism (Subcommittee on Physical Activity). Circulation 2003, 107, 3109–3116. [Google Scholar] [CrossRef] [PubMed]
- Daliri, E.B.-M.; Ofosu, F.K.; Chelliah, R.; Lee, B.H.; Oh, D.-H. Health Impact and Therapeutic Manipulation of the Gut Microbiome. High-Throughput 2020, 9, 17. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
{kind=link}
{kind=link}
| Author, Year | N (Men/Women), Mean Age | Intervention | Key Results | Methodology |
|---|---|---|---|---|
| Verhoeven JE, 2023 [108] | 58/83, 38.2 years | (1) 16-week treatment: escitalopram or sertraline (2) running therapy ≥ 2 per week | Remission rates at T16 were comparable, but the running group had greater reductions in weight loss, waist circumference, systolic and diastolic blood pressure, and heart rate. | The presence of depressive disorders and/or anxiety disorders was established at T0 and T16 using the CIDI. Severity of depression was measured using the 30-item Inventory of Depressive Symptomatology—Self Report (IDS-SR) and the severity of anxiety was measured with the 21-item Beck Anxiety Inventory (BAI). The physical health outcomes were assessed using outline standardized laboratory methods. |
| Sofie Holmquist, 2017 [110] | 2063/1021, 70 years | Explorative cluster analysis was used to group participants according to functional performance level, using measures of basic mobility skills, gait variability, and grip strength. | One potential high-risk cluster was identified, with an overrepresentation of individuals with GDS scores > 5 (15.1%) also with obese individuals (39.7%) and those with type 2 diabetes (24.7%) | Intercluster differences in depressive symptoms (measured by the Geriatric Depression Scale [GDS]-15), physical activity (PA; measured objectively with the ActiGraph GT3X+) |
| Labayen I, 2020 [115] | 52/62, 10.6 years | First group—family-based education sessions/month Second group—additionally high-intensity aerobic workouts (3 sessions/week, 90 min/session) | Percentage of hepatic fat decreased only in the II group. BMI, abdominal fat, and insulin were reduced in both groups. | Hepatic fat was measured by MRI, abdominal fat was measured by DEXA, and other outcomes were measured by standardized laboratory methods. |
| Farpour-Lambert NJ, 2009 [114] | n = 44 8.9 years | First group—trained 60 min 3 times/week during 3 months, then 2 times/week during 3 months. Control group—inactive for 3 months, then trained 2 times/week during 3 months. | Decrease in arterial blood pressure after the first 3 months in the I group. After 6 months, endothelial function, intima-media thickness, arterial stiffness, and adipose tissue were lower in the I and the control group. | The pubertal stage was assessed by clinical examination according to the method of Tanner. The DXA was used to do a total body scan. A real-time B-mode ultrasound imager was used to measure an IMT. Cardiorespiratory fitness was measured as VO2max assessed by direct gas analysis. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jakubowska, P.; Balcerczyk-Lis, M.; Fortuna, M.; Janiak, A.; Kopaczyńska, A.; Skwira, S.; Młynarska, E.; Rysz, J.; Franczyk, B. Influence of Metabolic Dysregulation in the Management of Depressive Disorder—Narrative Review. Nutrients 2024, 16, 1665. https://doi.org/10.3390/nu16111665
Jakubowska P, Balcerczyk-Lis M, Fortuna M, Janiak A, Kopaczyńska A, Skwira S, Młynarska E, Rysz J, Franczyk B. Influence of Metabolic Dysregulation in the Management of Depressive Disorder—Narrative Review. Nutrients. 2024; 16(11):1665. https://doi.org/10.3390/nu16111665
Chicago/Turabian StyleJakubowska, Paulina, Marta Balcerczyk-Lis, Milena Fortuna, Aleksandra Janiak, Adrianna Kopaczyńska, Sylwia Skwira, Ewelina Młynarska, Jacek Rysz, and Beata Franczyk. 2024. "Influence of Metabolic Dysregulation in the Management of Depressive Disorder—Narrative Review" Nutrients 16, no. 11: 1665. https://doi.org/10.3390/nu16111665
APA StyleJakubowska, P., Balcerczyk-Lis, M., Fortuna, M., Janiak, A., Kopaczyńska, A., Skwira, S., Młynarska, E., Rysz, J., & Franczyk, B. (2024). Influence of Metabolic Dysregulation in the Management of Depressive Disorder—Narrative Review. Nutrients, 16(11), 1665. https://doi.org/10.3390/nu16111665