
Longitudinal Correlations between Molecular Compositions of Stratum Corneum and Breast Milk Factors during Infancy: A Prospective Birth Cohort Study
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measurement of the Molecular Composition of the Infants’ SC
2.3. Measurement of Mothers’ Breast Milk
2.4. Statistical Analysis
3. Results
3.1. Patients’ Demographics
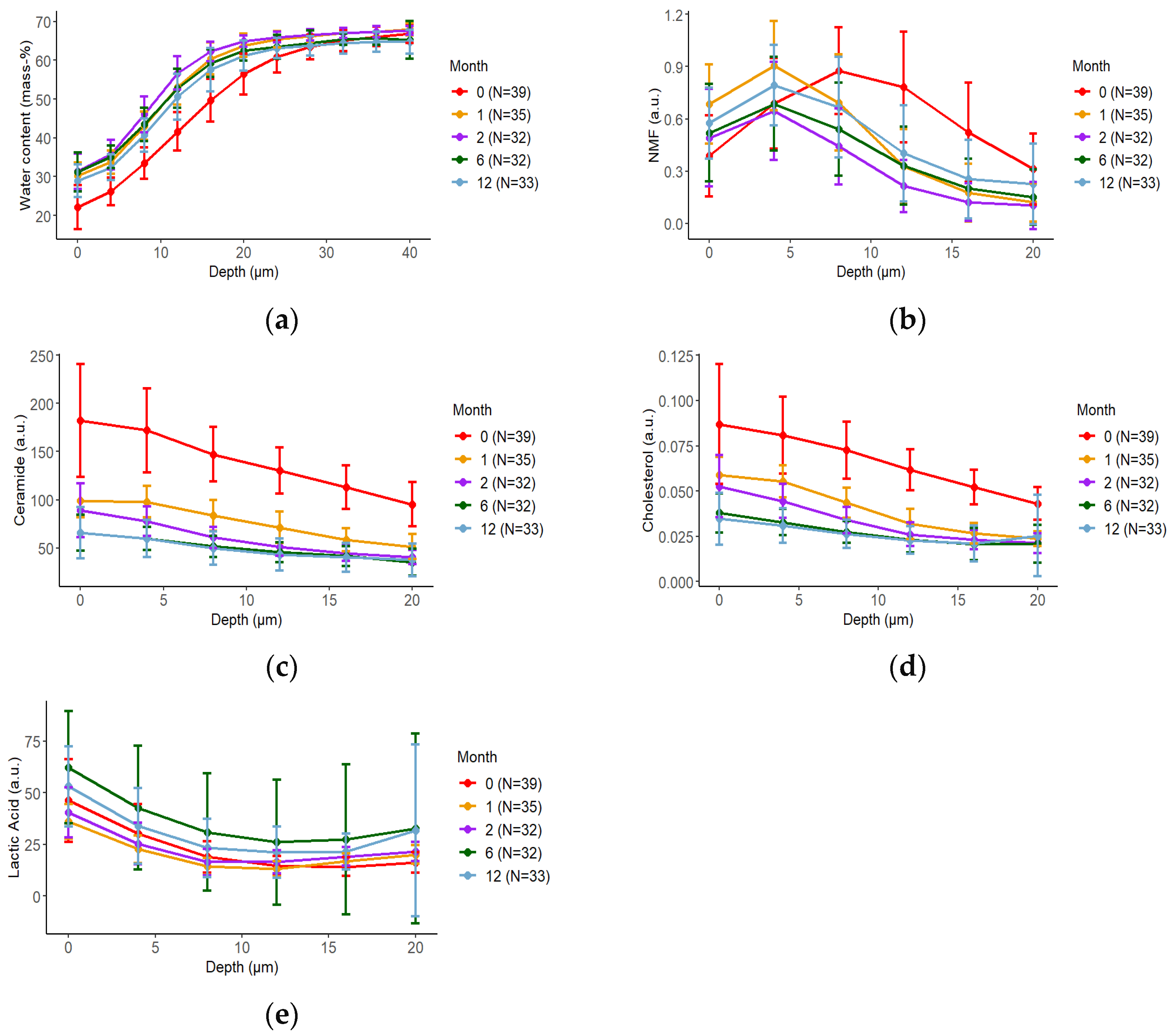
3.2. Longitudinal Molecular Changes in the Infants’ SC
3.3. Longitudinal Changes of Breast Milk Factors
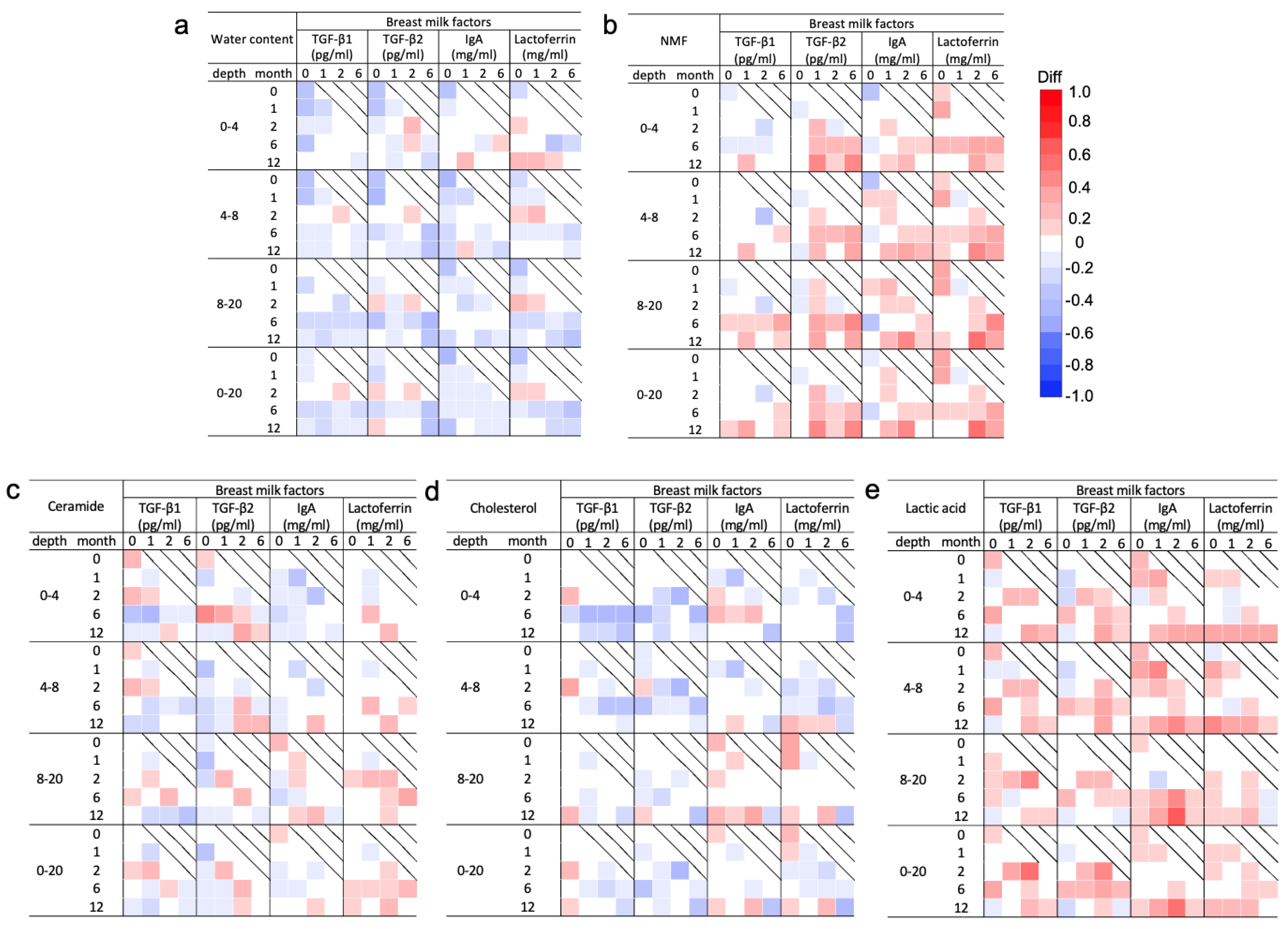
3.4. Spearman’s Correlation Analysis of the Molecular Components in the SC and Breast Milk Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Iyengar, S.R.; Walker, W.A. Immune factors in breast milk and the development of atopic disease. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 641–647. [Google Scholar] [CrossRef] [PubMed]
- Czosnykowska-Łukacka, M.; Lis-Kuberka, J.; Królak-Olejnik, B.; Orczyk-Pawiłowicz, M. Changes in human milk immunoglobulin profile during prolonged lactation. Front. Pediatr. 2020, 8, 428. [Google Scholar] [CrossRef] [PubMed]
- Ballard, O.; Morrow, A.L. Human milk composition: Nutrients and bioactive factors. Pediatr. Clin. N. Am. 2013, 60, 49–74. [Google Scholar] [CrossRef] [PubMed]
- Hirata, N.; Kiuchi, M.; Pak, K.; Fukuda, R.; Mochimaru, N.; Mitsui, M.; Yoshida, K. Association between maternal characteristics and immune factors TGF-β1, TGF-β2, and IgA in colostrum: An exploratory study in japan. Nutrients 2022, 14, 3255. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Lochhead, P.; Ko, Y.; Claggett, B.; Leong, R.W.; Ananthakrishnan, A.N. Systematic review with meta-analysis: Breastfeeding and the risk of Crohn’s disease and ulcerative colitis. Aliment. Pharmacol. Ther. 2017, 46, 780–789. [Google Scholar] [CrossRef] [PubMed]
- Morita, Y.; Campos-Alberto, E.; Yamaide, F.; Nakano, T.; Ohnisi, H.; Kawamoto, M.; Kawamoto, N.; Matsui, E.; Kondo, N.; Kohno, Y.; et al. TGF-β concentration in breast milk is associated with the development of eczema in infants. Front. Pediatr. 2018, 6, 162. [Google Scholar] [CrossRef]
- Dogaru, C.M.; Nyffenegger, D.; Pescatore, A.M.; Spycher, B.D.; Kuehni, C.E. Breastfeeding and childhood asthma: Systematic review and meta-analysis. Am. J. Epidemiol. 2014, 179, 1153–1167. [Google Scholar] [CrossRef] [PubMed]
- Horta, B.L.; Loret de Mola, C.; Victora, C.G. Long-term consequences of breastfeeding on cholesterol, obesity, systolic blood pressure and type 2 diabetes: A systematic review and meta-analysis. Acta. Paediatr. 2015, 104, 30–37. [Google Scholar] [CrossRef]
- Klopp, A.; Vehling, L.; Becker, A.B.; Subbarao, P.; Mandhane, P.J.; Turvey, S.E.; Lefebvre, D.L.; Sears, M.R.; Azad, M.B. Modes of infant feeding and the risk of childhood asthma: A prospective birth cohort study. J. Pediatr. 2017, 190, 192–199.e192. [Google Scholar] [CrossRef]
- Parikh, N.I.; Hwang, S.J.; Ingelsson, E.; Benjamin, E.J.; Fox, C.S.; Vasan, R.S.; Murabito, J.M. Breastfeeding in infancy and adult cardiovascular disease risk factors. Am. J. Med. 2009, 122, 656–663.e651. [Google Scholar] [CrossRef]
- Munblit, D.; Abrol, P.; Sheth, S.; Chow, L.Y.; Khaleva, E.; Asmanov, A.; Lauriola, S.; Padovani, E.M.; Comberiati, P.; Boner, A.L.; et al. Levels of growth factors and IgA in the colostrum of women from Burundi and Italy. Nutrients 2018, 10, 1216. [Google Scholar] [CrossRef] [PubMed]
- Böttcher, M.F.; Jenmalm, M.C.; Garofalo, R.P.; Björkstén, B. Cytokines in breast milk from allergic and nonallergic mothers. Pediatr. Res. 2000, 47, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Casas, R.; Böttcher, M.F.; Duchén, K.; Björkstén, B. Detection of IgA antibodies to cat, β-lactoglobulin, and ovalbumin allergens in human milk. J. Allergy Clin. Immunol. 2000, 105, 1236–1240. [Google Scholar] [CrossRef] [PubMed]
- Rogier, E.W.; Frantz, A.L.; Bruno, M.E.; Wedlund, L.; Cohen, D.A.; Stromberg, A.J.; Kaetzel, C.S. Secretory antibodies in breast milk promote long-term intestinal homeostasis by regulating the gut microbiota and host gene expression. Proc. Natl. Acad. Sci. USA 2014, 111, 3074–3079. [Google Scholar] [CrossRef] [PubMed]
- Brock, J.H. The physiology of lactoferrin. Biochem. Cell. Biol. 2002, 80, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Walker, V.P.; Akinbi, H.T.; Meinzen-Derr, J.; Narendran, V.; Visscher, M.; Hoath, S.B. Host defense proteins on the surface of neonatal skin: Implications for innate immunity. J. Pediatr. 2008, 152, 777–781. [Google Scholar] [CrossRef] [PubMed]
- Bezirtzoglou, E.; Tsiotsias, A.; Welling, G.W. Microbiota profile in feces of breast- and formula-fed newborns by using fluorescence in situ hybridization (FISH). Anaerobe 2011, 17, 478–482. [Google Scholar] [CrossRef] [PubMed]
- Pannaraj, P.S.; Li, F.; Cerini, C.; Bender, J.M.; Yang, S.; Rollie, A.; Adisetiyo, H.; Zabih, S.; Lincez, P.J.; Bittinger, K.; et al. Association between breast milk bacterial communities and establishment and development of the infant gut microbiome. JAMA Pediatr. 2017, 171, 647–654. [Google Scholar] [CrossRef] [PubMed]
- Donovan, S.M.; Wang, M.; Monaco, M.H.; Martin, C.R.; Davidson, L.A.; Ivanov, I.; Chapkin, R.S. Noninvasive molecular fingerprinting of host-microbiome interactions in neonates. FEBS Lett. 2014, 588, 4112–4119. [Google Scholar] [CrossRef]
- Ando, T.; Hatsushika, K.; Wako, M.; Ohba, T.; Koyama, K.; Ohnuma, Y.; Katoh, R.; Ogawa, H.; Okumura, K.; Luo, J.; et al. Orally administered TGF-β is biologically active in the intestinal mucosa and enhances oral tolerance. J. Allergy Clin. Immunol. 2007, 120, 916–923. [Google Scholar] [CrossRef]
- Murata, M.; Satoh, T.; Wakabayashi, H.; Yamauchi, K.; Abe, F.; Nomura, Y. Oral administration of bovine lactoferrin attenuates ultraviolet B-induced skin photodamage in hairless mice. J. Dairy Sci. 2014, 97, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Fluhr, J.W.; Darlenski, R.; Lachmann, N.; Baudouin, C.; Msika, P.; De Belilovsky, C.; Hachem, J.P. Infant epidermal skin physiology: Adaptation after birth. Br. J. Dermatol. 2012, 166, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, D.; Cardinali, G.; Aspite, N.; Picardo, M. Bovine colostrum promotes growth and migration of the human keratinocyte HaCaT cell line. Growth Factors 2009, 27, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, D.; Maresca, V.; Flori, E.; Mastrofrancesco, A.; Picardo, M.; Cardinali, G. Bovine colostrum induces the differentiation of human primary keratinocytes. FASEB J. 2020, 34, 6302–6321. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, Y.; Mochimaru, N.; Yasuda, H.; Pak, K.; Kobayashi, T.; Yamamoto-Hanada, K.; Ohya, Y.; Kiuchi, M.; Kurokawa, M.; Yoshida, K. In vivo analysis of the stratum corneum of Japanese neonates and infants using confocal Raman spectroscopy: A pilot study. Skin Res. Technol. 2023, 29, e13276. [Google Scholar] [CrossRef] [PubMed]
- Miyauchi, Y.; Shimaoka, Y.; Fujimura, T.; Koike, Y.; Yatabe, M.; Nishikawa, M.; Hayashi, M.; Sugata, K.; Moriwaki, S.; Hatamochi, A. Developmental changes in neonatal and infant skin structures during the first 6 months: In vivo observation. Pediatr. Dermatol. 2016, 33, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Stamatas, G.N.; Roux, P.F.; Boireau-Adamezyk, E.; Lboukili, I.; Oddos, T. Skin maturation from birth to 10 years of age: Structure, function, composition and microbiome. Exp. Dermatol. 2023, 32, 1420–1429. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Ko, Y.; Park, Y.K.; Kim, N.I.; Ha, W.K.; Cho, Y. Dietary effect of lactoferrin-enriched fermented milk on skin surface lipid and clinical improvement of acne vulgaris. Nutrition 2010, 26, 902–909. [Google Scholar] [CrossRef] [PubMed]
- Ling, C.J.; Min, Q.Q.; Yang, J.R.; Zhang, Z.; Yang, H.H.; Xu, J.Y.; Qin, L.Q. Lactoferrin alleviates the progression of atherosclerosis in ApoE−/− mice fed with high-fat/cholesterol diet through cholesterol homeostasis. J. Med. Food. 2019, 22, 1000–1008. [Google Scholar] [CrossRef]
- Takeuchi, T.; Shimizu, H.; Ando, K.; Harada, E. Bovine lactoferrin reduces plasma triacylglycerol and NEFA accompanied by decreased hepatic cholesterol and triacylglycerol contents in rodents. Br. J. Nutr. 2004, 91, 533–538. [Google Scholar] [CrossRef]
- Mueller, E.A.; Trapp, S.; Frentzel, A.; Kirch, W.; Brantl, V. Efficacy and tolerability of oral lactoferrin supplementation in mild to moderate acne vulgaris: An exploratory study. Curr. Med. Res. Opin. 2011, 27, 793–797. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.; Chan, G.; Santos, J.; Dee, K.; Co, J.K. A randomized, double-blind, placebo-controlled trial to determine the efficacy and safety of lactoferrin with vitamin E and zinc as an oral therapy for mild to moderate acne vulgaris. Int. J. Dermatol. 2017, 56, 686–690. [Google Scholar] [CrossRef] [PubMed]
- Subbiah, M.T.; Yunker, R.L.; Yamamoto, M.; Kottke, B.A.; Bale, L.K. Human breast milk stimulates prostaglandin synthesis in cultured human skin fibroblasts. Biochem. Biophys. Res. Commun. 1985, 129, 972–976. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Ren, C.; Han, X.; Huang, W.; You, Y.; Zhan, J. Role of IgA in the early-life establishment of the gut microbiota and immunity: Implications for constructing a healthy start. Gut Microbes 2021, 13, 1908101. [Google Scholar] [CrossRef] [PubMed]
- Kordy, K.; Gaufin, T.; Mwangi, M.; Li, F.; Cerini, C.; Lee, D.J.; Adisetiyo, H.; Woodward, C.; Pannaraj, P.S.; Tobin, N.H.; et al. Contributions to human breast milk microbiome and enteromammary transfer of Bifidobacterium breve. PLoS ONE 2020, 15, e0219633. [Google Scholar] [CrossRef] [PubMed]
- Duranti, S.; Lugli, G.A.; Mancabelli, L.; Armanini, F.; Turroni, F.; James, K.; Ferretti, P.; Gorfer, V.; Ferrario, C.; Milani, C.; et al. Maternal inheritance of bifidobacterial communities and bifidophages in infants through vertical transmission. Microbiome 2017, 5, 66. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Nakayama, J. Development of the gut microbiota in infancy and its impact on health in later life. Allergol. Int. 2017, 66, 515–522. [Google Scholar] [CrossRef]
- Zeng, M.Y.; Inohara, N.; Nuñez, G. Mechanisms of inflammation-driven bacterial dysbiosis in the gut. Mucosal Immunol. 2017, 10, 18–26. [Google Scholar] [CrossRef]
- Shamash, M.; Maurice, C.F. Phages in the infant gut: A framework for virome development during early life. ISME J. 2022, 16, 323–330. [Google Scholar] [CrossRef]
- Makino, H.; Kushiro, A.; Ishikawa, E.; Kubota, H.; Gawad, A.; Sakai, T.; Oishi, K.; Martin, R.; Ben-Amor, K.; Knol, J.; et al. Mother-to-infant transmission of intestinal bifidobacterial strains has an impact on the early development of vaginally delivered infant’s microbiota. PLoS ONE 2013, 8, e78331. [Google Scholar] [CrossRef]
- Polkowska-Pruszyńska, B.; Gerkowicz, A.; Krasowska, D. The gut microbiome alterations in allergic and inflammatory skin diseases—An update. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Sugawara, T.; Kikuchi, K.; Tagami, H.; Aiba, S.; Sakai, S. Decreased lactate and potassium levels in natural moisturizing factor from the stratum corneum of mild atopic dermatitis patients are involved with the reduced hydration state. J. Dermatol. Sci. 2012, 66, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Egawa, M.; Tagami, H. Comparison of the depth profiles of water and water-binding substances in the stratum corneum determined in vivo by Raman spectroscopy between the cheek and volar forearm skin: Effects of age, seasonal changes and artificial forced hydration. Br. J. Dermatol. 2008, 158, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Bielfeldt, S.; Schoder, V.; Ely, U.; Van Der Pol, A.; De Sterke, J.; Wilhelm, K.-P. Assessment of human stratum corneum thickness and its barrier properties by in-vivo confocal Raman spectroscopy. Int. J. Cosmet. Sci. 2009, 31, 479–480. [Google Scholar] [CrossRef]
- Hoeger, P.H.; Schreiner, V.; Klaassen, I.A.; Enzmann, C.C.; Friedrichs, K.; Bleck, O. Epidermal barrier lipids in human vernix caseosa: Corresponding ceramide pattern in vernix and fetal skin. Br. J. Dermatol. 2002, 146, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Al, S.; Asilsoy, S.; Atay, O.; Kangallı, O.; Atakul, G.; Tezcan, D.; Uzuner, N. Transepidermal water loss in allergic diseases. Allergy Asthma. Proc. 2023, 44, 186–192. [Google Scholar] [CrossRef]
- Sloin, H.E.; Ruggiero, G.; Rubinstein, A.; Smadja Storz, S.; Foulkes, N.S.; Gothilf, Y. Interactions between the circadian clock and TGF-β signaling pathway in zebrafish. PLoS ONE 2018, 13, e0199777. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factors | Classes | Total (N = 39) N (%) |
|---|---|---|
| Infants’ sex | Male | 21 (53.8%) |
| Female | 18 (46.2%) | |
| Birth weight | <2500 g | 0 (0.0%) |
| 2500−4000 g | 39 (100.0%) | |
| ≥4000 g | 0 (0.0%) | |
| Family history of allergies | Yes | 37 (94.9%) |
| No | 2 (5.1%) | |
| Mother’s smoking status | Yes | 9 (23.1%) |
| No | 30 (76.9%) | |
| Parity | Primipara | 29 (74.4%) |
| Multipara | 10 (25.6%) | |
| Gestational age | <37 weeks | 0 (0.0%) |
| 37 to 41 weeks | 39 (100.0%) | |
| ≥42 weeks | 0 (0.0%) | |
| Age at delivery | 20 s | 4 (10.3%) |
| 30 s | 21 (53.8%) | |
| 40 s | 14 (35.9%) | |
| Delivery mode | Vaginal birth | 26 (66.7%) |
| Cesarean section | 13 (33.3%) | |
| Colostrum secretion | Before birth | 7 (17.9%) |
| After birth | 32 (82.1%) | |
| Colostrum collection day | ≤3 days | 15 (38.5%) |
| 4 days | 9 (23.1%) | |
| ≥5 days | 15 (38.5%) |
| Factors | Classes | Months | ||||
|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 6 | 12 | ||
| Total (N = 39) N (%) | Total (N = 35) N (%) | Total (N = 32) N (%) | Total (N = 32) N (%) | Total (N= 33) N (%) | ||
| Nutrition source | Breast | 3 (7.7%) | 5 (14.3%) | 4 (12.5%) | 5 (15.6%) | 4 (12.1%) |
| Formula | 1 (2.6%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (3.0%) | |
| Mix | 35 (89.7%) | 30 (85.7%) | 28 (87.5%) | 23 (71.9%) | 11 (33.3%) | |
| Bath frequency | No bath | 28 (71.8%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Every few days | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| Once daily | 7 (17.9%) | 34 (97.1%) | 30 (93.8%) | 26 (81.2%) | 28 (84.8%) | |
| Twice or more daily | 0 (0.0%) | 1 (2.9%) | 2 (6.2%) | 6 (18.8%) | 4 (12.1%) | |
| Frequency unknown | 4 (10.3%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (3.0%) | |
| Wash with soap in bath | Yes | 6 (15.4%) | 34 (97.1%) | 32 (100.0%) | 32 (100.0%) | 33 (100.0%) |
| No | 33 (84.6%) | 1 (2.9%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| Moisturizer use (face) | No use | 8 (20.5%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Less than once daily | 3 (7.7%) | 0 (0.0%) | 0 (0.0%) | 1 (3.1%) | 1 (3.0%) | |
| Once daily | 13 (33.3%) | 23 (65.7%) | 16 (50.0%) | 11 (34.4%) | 12 (36.4%) | |
| Twice or more daily | 6 (15.4%) | 11 (31.4%) | 16 (50.0%) | 19 (59.4%) | 17 (51.5%) | |
| Frequency unknown | 9 (23.1%) | 1 (2.9%) | 0 (0.0%) | 1 (3.1%) | 3 (9.1%) | |
| Moisturizer use (legs) | No use | 15 (38.5%) | 1 (2.9%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Less than once daily | 1 (2.6%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (3.0%) | |
| Once daily | 10 (25.6%) | 27 (77.1%) | 17 (53.1%) | 11 (34.4%) | 14 (42.4%) | |
| Twice or more daily | 6 (15.4%) | 6 (17.1%) | 13 (40.6%) | 15 (46.9%) | 15 (45.5%) | |
| Frequency unknown | 7 (17.9%) | 1 (2.9%) | 2 (6.2%) | 6 (18.8%) | 3 (9.1%) | |
| Breast or nipple problem | Yes | 27 (69.2%) | 16 (45.7%) | 7 (21.9%) | 7 (21.9%) | 1 (3.0%) |
| No | 12 (30.8%) | 19 (54.3%) | 25 (78.1%) | 25 (78.1%) | 31 (93.9%) | |
| Nipple care | Yes | 20 (51.3%) | 19 (54.3%) | 10 (31.2%) | 5 (15.6%) | 2 (6.1%) |
| No | 19 (48.7%) | 16 (45.7%) | 22 (68.8%) | 27 (84.4%) | 29 (87.9%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fukuda, R.; Pak, K.; Kiuchi, M.; Hirata, N.; Mochimaru, N.; Tanaka, R.; Mitsui, M.; Ohya, Y.; Yoshida, K. Longitudinal Correlations between Molecular Compositions of Stratum Corneum and Breast Milk Factors during Infancy: A Prospective Birth Cohort Study. Nutrients 2024, 16, 1897. https://doi.org/10.3390/nu16121897
Fukuda R, Pak K, Kiuchi M, Hirata N, Mochimaru N, Tanaka R, Mitsui M, Ohya Y, Yoshida K. Longitudinal Correlations between Molecular Compositions of Stratum Corneum and Breast Milk Factors during Infancy: A Prospective Birth Cohort Study. Nutrients. 2024; 16(12):1897. https://doi.org/10.3390/nu16121897
Chicago/Turabian StyleFukuda, Risa, Kyongsun Pak, Megumi Kiuchi, Naoko Hirata, Naoko Mochimaru, Ryo Tanaka, Mari Mitsui, Yukihiro Ohya, and Kazue Yoshida. 2024. "Longitudinal Correlations between Molecular Compositions of Stratum Corneum and Breast Milk Factors during Infancy: A Prospective Birth Cohort Study" Nutrients 16, no. 12: 1897. https://doi.org/10.3390/nu16121897