
Evaluating Double-Duty Actions in Rwanda’s Secondary Cities
 , , , ,
, , , ,
Abstract
:1. Introduction
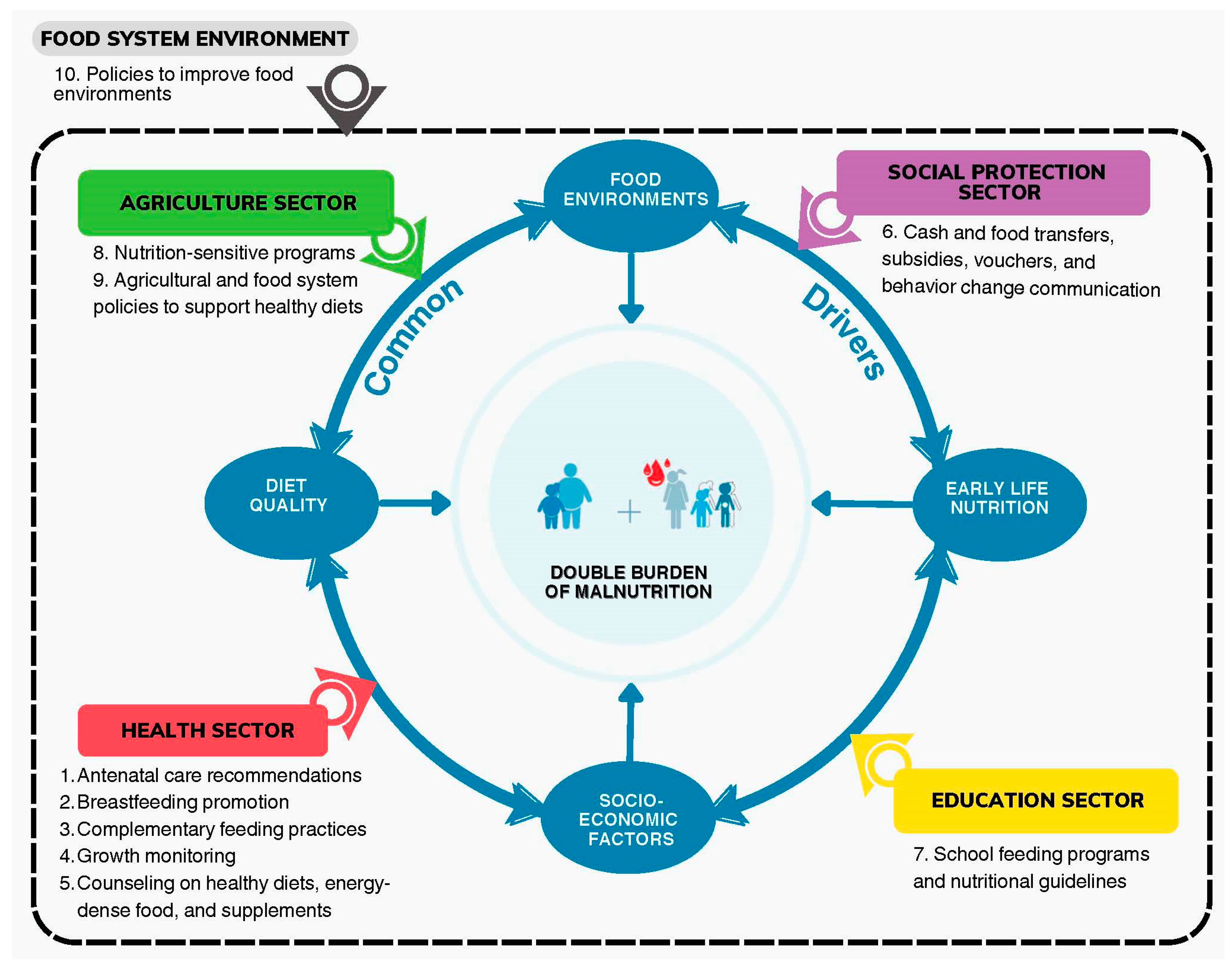
1.1. DDA Conceptual Framework
- Early life nutrition: Nutrition for pregnant and lactating mothers and children under 2 years has a profound influence on physical development for both mother and child and food-related behavior later in life;
- Diet quality: Poor diet quality can lead to micronutrient deficiencies and/or excess consumption of nutrients-to-limit (e.g., salt, sugar, fat), both of which are associated with a higher risk of non-communicable diseases (NCDs);
- Food environments: The way food is priced, marketed, and made available to a population all shape the food environment and influence food choices in a positive or negative way;
- Socio-economic factors: Increased income is associated with lower rates of stunting and anemia but is simultaneously associated with a higher risk of overweight and obesity. Higher education is associated with lower rates of both.
1.2. Case Study: DBM and DDAs in Rwanda
1.3. Objectives of the Paper
2. Methods
2.1. Data Collection
2.2. Data Analysis
2.3. Ethical Approvals and Considerations
2.4. Focus Group Discussion and Validation
3. Results
3.1. Final DDA Interventions
3.2. SWOT Analysis Results
- Program 1 (P1). Early Childhood Development (ECD) centers (Health Sector)
- P1-Recommendation 1. We recommend consulting with caregivers on which skills or topics they want training on and providing them with incentives to attend trainings, especially given that they are not compensated for their work at the ECD. Possible incentives could include transport allowances or free manuals and educational materials to take home.
- Relevant S, W, O, and Ts: S3; W2; O2, O4, O6, O7; T4
- P1-Recommendation 2. We recommend assigning specific responsibilities to parents, especially fathers, at ECDs to increase their involvement and thereby encourage them to adopt ECD services at home and motivate them to contribute. These responsibilities could include gardening, cooking, or cleaning tasks. We also recommend assisting parent groups to set up parent-led SILCs (Saving and Internal Lending Communities) through which they can collectively pool money to purchase materials for ECDs during stock-outs (e.g., porridge and milk).
- Relevant S, W, O, and Ts: S1, S2; W1, W2, W3, W4; O1, O3; T1, T2, T3, T5, T6, T7, T8
- P1-Recommendation 3. We recommend ensuring that all centers engage in at-home follow-up with households to ensure that parents are adopting ECD lessons on healthy diets and lifestyle practices at home.
- Relevant S, W, O, and Ts: S2; O5; T8, T9
- Program 2 (P2). Farmer Field Schools (Agriculture Sector)
- P2-Recommendation 1. We recommend investing in establishing a local feed supplier and distributor in or accessible to Rubavu and Rusizi districts with the capacity to supply high-quality feed in sufficient quantities to surrounding farming households. We also recommend incentivizing or supporting research and education on sustainable feed alternatives as some FFS facilitators have already accomplished with black soldier flies.
- Relevant S, W, O, and Ts: W2; O1; T3, T4, T6
- P2-Recommendation 2. We recommend increasing the number and frequency of trainings and providing regular refresher sessions for FFS facilitators to sustain their motivation and encourage continuous learning.
- Relevant S, W, O, and Ts: S2, S3; W3; O3
- P2-Recommendation 3. Given that in-person follow-up to all farmers by facilitators is often infeasible, especially in rural areas, we recommend scaling up SMS reminders for farmers to ensure they are implementing the lessons they learned at appropriate times (e.g., weeding, harvesting, and cover-cropping) and encourage them to not sell their production.
- Relevant S, W, O, and Ts: S1; W1, W3; O2; T1, T2, T5
- Program 3 (P3). School feeding program (Education Sector)
- P3-Recommendation 1. We recommend investing in building or finding designated eating spaces at schools and in acquiring sufficient kitchen and cooking materials to meet demand.
- Relevant S, W, O, and Ts: O4; T3, T5
- P3-Recommendation 2. We recommend increasing collaboration between parents, local leaders, and schoolteachers to help cultivate trust and, as with the ECD program (see program 1), establishing SILCs to help parents purchase fruits, vegetables, and animal products for school meals and allow them to gain transparency on how and where their contribution is spent.
- Relevant S, W, O, and Ts: S1, S2; W1, W2; O1, O2; T1, T2, T4
- P3-Recommendation 3. We recommend establishing links between schools and FFSs for local procurement and as a resource for agricultural education sessions. By linking the two programs, FFS facilitators could use school gardens as “model plots” for their farmer trainings and the resulting production could be used to improve the quality and diversity of school meals. We also recommend extending the option for parents and teachers to attend some of the trainings when possible to encourage their involvement at schools.
- Relevant S, W, O, and Ts: W1, W2; O3; T1, T4
- Program 4 (P4). Nutrition-Sensitive Direct Support and Shisha Kibondo (Social Protection Sector)
- P4-Recommendation 1. To address the concerns surrounding NSDS about incentivizing women to become pregnant, we recommend complementing any monetary support to beneficiaries with targeted education about family planning. We also recommend extending the support until the child reaches three years of age instead of two, at which point children are generally eligible to attend ECDs.
- Relevant S, W, O, and Ts: S1; W1; O2; T1, T4
- P4-Recommendation 2. Currently, Shisha Kibondo is distributed at community health centers at regular growth monitoring sessions for women to take home and administer themselves. We recommend linking the Shisha Kibondo program to ECD centers by training caregivers to administer Shisha Kibondo at ECDs. This could both ensure that mothers and children receive adequate quantities of the product and additionally incentivize pregnant and lactating women to attend ECDs where they could receive other antenatal and postnatal services and counseling. After the first initiation at ECDs, beneficiaries could begin to receive it again for at-home administration but with close and regular follow-up.
- Relevant S, W, O, and Ts: S1; W1, O1, O2, O3; T2, T3
- P4-Recommendation 3. Currently, the quantity of Shisha Kibondo provided to beneficiary households is based on the estimated quantity needed for only one child. We recommend calculating the quantity of Shisha Kibondo provided based on household size (i.e., number of children or household members) instead. This could reduce the likelihood of beneficiaries diluting the product to meet the needs of all family members.
- Relevant S, W, O, and Ts: W1, O2, T3
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. The Double Burden of Malnutrition: Policy Brief; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Alem, A.Z.; Yeshaw, Y.; Liyew, A.M.; Tessema, Z.T.; Worku, M.G.; Tesema, G.A.; Alamneh, T.S.; Teshale, A.B.; Chilot, D.; Ayalew, H.G. Double Burden of Malnutrition and Its Associated Factors among Women in Low and Middle Income Countries: Findings from 52 Nationally Representative Data. BMC Public Health 2023, 23, 1479. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health; Rwanda Biomedical Centre. National Strategy and Costed Action Plan for the Prevention and Control of Non-Communicable Diseases in Rwanda 2020–2025; Ministry of Health; Rwanda Biomedical Centre: Kigali, Rwanda, 2020. [Google Scholar]
- Kang, S.; Kang, M.; Lim, H. Global and Regional Patterns in Noncommunicable Diseases and Dietary Factors across National Income Levels. Nutrients 2021, 13, 3595. [Google Scholar] [CrossRef] [PubMed]
- Thow, A.M.; Kadiyala, S.; Khandelwal, S.; Menon, P.; Downs, S.; Reddy, K.S. Toward Food Policy for the Dual Burden of Malnutrition: An Exploratory Policy Space Analysis in India. Food Nutr. Bull. 2016, 37, 261–274. [Google Scholar] [CrossRef] [PubMed]
- Hawkes, C.; Ruel, M.T.; Salm, L.; Sinclair, B.; Branca, F. Double-Duty Actions: Seizing Programme and Policy Opportunities to Address Malnutrition in All Its Forms. Lancet 2020, 395, 142–155. [Google Scholar] [CrossRef] [PubMed]
- Kate Kennedy-Wood; Silvia Holschneider. From Double Burden to Double Duty: Policy Implications of Double-Duty Actions to Address the Full Spectrum of Malnutrition; Summary of Technical Consultation; World Bank Group: Washington, DC, USA, 2021. [Google Scholar]
- National Policies and Plans to Address the Dual Burden of Malnutrition: A Multi-Country Policy Review; Spring: Naperville, IL, USA, 2018.
- Batal, M.; Deaconu, A.; Steinhouse, L. The Nutrition Transition and the Double Burden of Malnutrition. In Nutritional Health: Strategies for Disease Prevention; Temple, N.J., Wilson, T., Jacobs, D.R., Jr., Bray, G.A., Eds.; Springer International Publishing: Cham, Switzerland, 2023; pp. 33–44. [Google Scholar] [CrossRef]
- Erzse, A.; Goldstein, S.; Norris, S.A.; Watson, D.; Kehoe, S.H.; Barker, M.; Cohen, E.; Hofman, K.J. Double-Duty Solutions for Optimising Maternal and Child Nutrition in Urban South Africa: A Qualitative Study. Public Health Nutr. 2021, 24, 3674–3684. [Google Scholar] [CrossRef] [PubMed]
- The World Factbook. Rwanda, 2023. Available online: https://www.cia.gov/the-world-factbook/countries/rwanda/ (accessed on 8 September 2023).
- Britannica. The Information Architects of Enyclopaedia. Rwanda, 2023. Available online: https://www.britannica.com/facts/Rwanda (accessed on 14 September 2023).
- World Food Programme. Rwanda Annual Country Report: Country Strategic Plan 2019–2024; World Food Programme: Rome, Italy, 2022. [Google Scholar]
- Iruhiriy, E.; Olney, D.K.; Ramani, G.V.; Heckert, J.; Niyongira, E.; Frongillo, E.A. Stories of Change: Rwanda: Understanding How Rwanda Created an Enabling Environment for Improvements in Nutrition and the Challenges That Remain; International Food Policy Research Institute: Washington, DC, USA, 2019. [Google Scholar]
- Committee on World Food Security (CFS). New HLPE-FSN Drafting Team on Uran and Per-Urban Food Systems; HLPE: Rome, Italy, 2023; Available online: https://www.fao.org/cfs/cfs-hlpe/insights/news-insights/news-detail/new-hlpe-fsn-drafting-team-on-urban-and-peri-urban-food-systems/en (accessed on 1 April 2024).
- MINECOFIN, 2020. Vision 2050. Republic of Rwanda, Kigali. Available online: https://www.minecofin.gov.rw/fileadmin/user_upload/Minecofin/Publications/REPORTS/National_Development_Planning_and_Research/Vision_2050/English-Vision_2050_Abridged_version_WEB_Final.pdf (accessed on 8 September 2023).
- Swiss Development and Cooperation Center (SDC). Nutrition in City Ecosystems: The Project Factsheet; 2022. Available online: https://nice.ethz.ch/wp-content/uploads/2024/02/NICE_Project_Factsheet_27_February-2024.pdf (accessed on 8 June 2023).
- Barth-Jaeggi, T.; Speich, C.; Havugimana, C.; Bayisenge, F.; Kimenju, S.; Omondi, W.; Pasha, S.F.; Islam, S.; van Zutphen-Küffer, K.G.; van den Berg, S.; et al. Nutrition Transition, Double Burden of Malnutrition, and Urbanization Patterns in Secondary Cities of Bangladesh, Kenya and Rwanda. BMC Nutr. 2023, 9, 125. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Statistics of Rwanda (NISR); Ministry of Health (MOH); ICF. Rwanda Demographic and Health Survey 2019-20 Final Report; 2021. Available online: https://dhsprogram.com/publications/publication-FR370-DHS-Final-Reports.cfm (accessed on 31 March 2023).
- United Nations World Food Programme; National Institute of Statistics of Rwanda (NISR) [Rwanda]; Ministry of Health (MOH) [Rwanda]; ICF; Ministry of Agriculture and Animal Resources. Comprehensive Food Security and Vulnerability Analysis 2021, 2021. Available online: https://www.statistics.gov.rw/publication/comprehensive-food-security-and-vulnerability-analysis2022 (accessed on 3 April 2023).
- World Health Organization. Global Nutrition Policy Review 2016–2017: Country Progress in Creating Enabling Policy Environments for Promoting Healthy Diets and Nutrition; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Harris, J.E.; Gleason, P.M.; Sheean, P.M.; Boushey, C.; Beto, J.A.; Bruemmer, B. An Introduction to Qualitative Research for Food and Nutrition Professionals. J. Am. Diet. Assoc. 2009, 109, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Horton, J.; Macve, R.; Struyven, G. Chapter 20-Qualitative Research: Experiences in Using Semi-Structured Interviews1. In The Real Life Guide to Accounting Research; Humphrey, C., Lee, B., Eds.; Elsevier: Oxford, UK, 2004; pp. 339–357. [Google Scholar] [CrossRef]
- Dhakal, K. NVivo. J. Med. Libr. Assoc. JMLA 2022, 110, 270–272. [Google Scholar] [CrossRef] [PubMed]
- Skinner, K.; Hanning, R.M.; Sutherland, C.; Edwards-Wheesk, R.; Tsuji, L.J.S. Using a SWOT Analysis to Inform Healthy Eating and Physical Activity Strategies for a Remote First Nations Community in Canada. Am. J. Health Promot. AJHP 2012, 26, e159-170. [Google Scholar] [CrossRef] [PubMed]
- Guthiga, P.M.; Kirui, L. A Synthesis on Status of Food Fortification in Rwanda. 2019. Available online: https://cgspace.cgiar.org/server/api/core/bitstreams/5642dc9b-3adf-4b9f-a5e6-efdaba39db81/content (accessed on 24 May 2024).
- Ezezika, O.; Gong, J.; Abdirahman, H.; Sellen, D. Barriers and Facilitators to the Implementation of Large-Scale Nutrition Interventions in Africa: A Scoping Review. Glob. Implement. Res. Appl. 2021, 1, 38–52. [Google Scholar] [CrossRef]
- Williams, P.A.; Schnefke, C.H.; Flax, V.L.; Nyirampeta, S.; Stobaugh, H.; Routte, J.; Musanabaganwa, C.; Ndayisaba, G.; Sayinzoga, F.; Muth, M.K. Using Trials of Improved Practices to Identify Practices to Address the Double Burden of Malnutrition among Rwandan Children. Public Health Nutr. 2019, 22, 3175–3186. [Google Scholar] [CrossRef] [PubMed]
- Flax, V.L.; Ouma, E.; Izerimana, L.; Schreiner, M.A.; Brower, A.O.; Niyonzima, E.; Nyilimana, C.; Ufitinema, A.; Uwineza, A. Animal Source Food Social and Behavior Change Communication Intervention Among Girinka Livestock Transfer Beneficiaries in Rwanda: A Cluster Randomized Evaluation. Glob. Health Sci. Pract. 2021, 9, 640. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, E.; Stickland, J.; Kershaw, M.; Biadgilign, S. Impact of Social and Behavior Change Communication in Nutrition Specific Interventions on Selected Indicators of Nutritional Status. J. Human Nutr. 2018, 2, 34–46. [Google Scholar]
- Condo, J.; Mugeni, C.; Naughton, B.; Hall, K.; Tuazon, M.A.; Omwega, A.; Nwaigwe, F.; Drobac, P.; Hyder, Z.; Ngabo, F.; et al. Rwanda’s Evolving Community Health Worker System: A Qualitative Assessment of Client and Provider Perspectives. Human Resour. Health 2014, 12, 71. [Google Scholar] [CrossRef] [PubMed]
- Ayeni Solomon Ayodele. An Impact Evaluation of Early Childhood Development Centres in Rwanda (A Case Study of Huye District, Southern Province), 2019. Available online: https://dr.ur.ac.rw/handle/123456789/756 (accessed on 23 October 2023).
- Moon, S.; Lee, S. A Strategy for Sustainable Development of Cooperatives in Developing Countries: The Success and Failure Case of Agricultural Cooperatives in Musambira Sector, Rwanda. Sustainability 2020, 12, 8632. [Google Scholar] [CrossRef]
- Lee, H.E.; Veliz, P.T.; Maffioli, E.M.; Munro-Kramer, M.L.; Sakala, I.; Chiboola, N.M.; Ngoma, T.; Kaiser, J.L.; Rockers, P.C.; Scott, N.A.; et al. The Role of Savings and Internal Lending Communities (SILCs) in Improving Community-Level Household Wealth, Financial Preparedness for Birth, and Utilization of Reproductive Health Services in Rural Zambia: A Secondary Analysis. BMC Public Health 2022, 22, 1724. [Google Scholar] [CrossRef] [PubMed]
- Mbiro, K.A.; Ndlovu, T. Impact of Women’s Participation on Village Savings and Loan on Children’s Nutritional Diversity in Rural Chimanimani in Zimbabwe. Jamba Potchefstroom S. Afr. 2021, 13, 1043. [Google Scholar] [CrossRef] [PubMed]
- Jensen, S.K.G.; Placencio-Castro, M.; Murray, S.M.; Brennan, R.T.; Goshev, S.; Farrar, J.; Yousafzai, A.; Rawlings, L.B.; Wilson, B.; Habyarimana, E.; et al. Effect of a Home-Visiting Parenting Program to Promote Early Childhood Development and Prevent Violence: A Cluster-Randomized Trial in Rwanda. BMJ Glob. Health 2021, 6, e003508. [Google Scholar] [CrossRef] [PubMed]
- Farnworth, C.R.; Jumba, H.; Otieno, P.E.; Galiè, A.; Ouma, E.; Flax, V.L.; Schreiner, M.-A.; Colverson, K. Gender Roles and Masculinities in Leveraging Milk for Household Nutrition: Evidence from Two Districts in Rwanda. Food Policy 2023, 118, 102486. [Google Scholar] [CrossRef]
- Menon, S.; Peñalvo, J.L. Actions Targeting the Double Burden of Malnutrition: A Scoping Review. Nutrients 2019, 12, 81. [Google Scholar] [CrossRef] [PubMed]
- van Zutphen, K.G.; Barjolle, D.; van den Berg, S.; Gavin-Smith, B.; Kramer, K.; Musard, C.; Prytherch, H.; Six, J.; Winter, S.; Woltering, K. Secondary Cities as Catalysts for Nutritious Diets in Low- and Middle-Income Countries; Center for Development Research (ZEF) in Cooperation with the Scientific Group for the UN Food System Summit 2021: Bonn, Germany, 2021. [Google Scholar]

{kind=link}
| Sector | Position | Rusizi (17) | Rubavu (20) |
|---|---|---|---|
| Health | District Directors of Health | 1 | 1 |
| Nutritionists in district hospitals | 1 | 1 | |
| Antenatal care (ANC) providers and nurses | 1 | 1 | |
| Community health workers (CHWs) | 1 | 1 | |
| Early Childhood Development (ECD) center workers: leaders, caregivers, and volunteers | 2 | 3 | |
| Education | District Directors of Education | 1 | 1 |
| Schoolteachers (Heads of Nutrition and Environment clubs) | 3 | 2 | |
| Social Protection | ECD District Focal Points | 1 | 1 |
| National Women’s Council representatives | 1 | 1 | |
| Members of non-governmental organizations (NGOs) | 2 | 2 | |
| Representatives of faith-based organizations (FBOs) | 0 | 2 | |
| Agriculture | District Directors of Agriculture | 1 | 0 |
| Farmer Field School (FFS) facilitators | 1 | 2 | |
| One Acre Fund officers | 1 | 1 | |
| Veterinarians | 0 | 1 |
| Sector | DDA Program |
|---|---|
| Health Sector | 1. Antenatal care (ANC) visits |
| 2. Early Childhood Development (ECD) centers | |
| 3. Exclusive breastfeeding promotion | |
| Education | 4. School feeding program |
| 5. Trainings (teachers, caregivers, and community health workers) | |
| Social Protection | 6. Social behavior change campaigns |
| 7. Non-communicable disease (NCD) prevention and physical activity promotion | |
| 8. Nutrition-Sensitive Direct Support (NSDS) and Shisha Kibondo | |
| Agriculture | 9. Farmer Field Schools (FFS) |
| 10. Small stock distribution | |
| 11. Fruit tree program | |
| 12. Kitchen garden program |
| Strengths | Weaknesses |
| S1. Parents see changes in children and are motivated to follow the ECD model at home S2. Home visits show that parents start implementing kitchen gardens after seeing them at ECDs S3. Training of ECD caregivers improves quality of services and trainings | W1. Low parent monetary contribution W2. Inconsistent and unequal support across ECDs (meals, materials, and caregiver support) W3. Not enough food at ECDs for all children W4. Lack of fruits and animal products in meals provided at ECDs |
| Opportunities | Threats |
| O1. Option for parents to make non-monetary contributions (food; firewood and charcoal; cooking; cleaning; and gardening services) O2. Increased trainings for caregivers (ensuring continuous education) O3. Increased parent involvement (e.g., parents form groups to raise money to improve ECDs) O4. Income or non-monetary compensation for caregivers (money is best incentive even if small amount) O5. Close follow-up (home visits to monitor changes or adoption of practices) O6. Incentives for caregivers to attend trainings O7. Introduce attractive new topics for trainings based on what caregivers want to learn | T1. Shared mindset that ECDs are a government program and responsibility T2. High cost of healthy food at market and high price volatility T3. Lack of sufficient funding T4. Caregivers not compensated or incentivized to attend trainings and many do not have the time T5. Stock-outs (porridge stock-outs lead to drop-outs or ECD closures) T6. Lack of long-term program sustainability without partner or government support T7. Inconsistent government budget (leads to stock-outs) T8. Lack of knowledge (parents do not know or value proper ECD services) T9. Parents do not have the time to attend ECD trainings or education sessions |
| Strengths | Weaknesses |
| S1. SMS reminders for farmers (when to top dress, weed, and harvest) work well when in-person follow-up is impossible S2. Model plot hands-on demonstrations are effective at engaging farmers S3. Farmers reached through the program are motivated to learn new methods | W1. Animal products are the first thing farmers sell on the market (not kept for at-home consumption) W2. Lack of feed industry in many districts results in high costs and long wait times to acquire feed W3. Often there are not enough trained FFS facilitators to cover all farmers |
| Opportunities | Threats |
| O1. Improved quality of feed for small stock (alternative methods, e.g., black soldier flies) O2. Continuous education for farmers and follow-up from FFS facilitators O3. More frequent and recurring trainings for FFS facilitators on best practices and on facilitation | T1. Farmers prioritize selling production to buy land or other inputs rather than consuming it T2. Farmers who do not receive follow-up become disincentivized to continue implementing best practices T3. Inputs and feed are expensive on the market (organic fertilizers especially) T4. Shared mindset to value quantity of production over quality T5. Belief that nutritious food is for wealthy people T6. Small stock often fall ill (due to bad practices or poor quality of feed) |
| Strengths | Weaknesses |
| S1. Non-monetary contributions by parents can help subsidize school meals (e.g., small fish, peanuts, and sweet potatoes) S2. Parent meetings and mobilization increase awareness, motivation, and contributions S3. Daily school meals have improved school attendance and focus in class | W1. Low parent contribution W2. Lack of animal products or vegetables or fruits in the menu (always maize, beans, rice, potatoes, and soya) |
| Opportunities | Threats |
| O1. Increase collaboration between parents and school to increase contribution and involvement O2. Increase collaboration with local government or leaders to encourage parents O3. Run trainings at schools for parents on starting and maintaining vegetable gardens O4. Increased kitchen and eating materials to meet demand (e.g., “muvero”, plates, utensils, and cooking needs) | T1. Parents, especially those with many children, are unwilling or cannot afford to contribute to the program (contribution is per child) T2. Mindset that school feeding is government’s responsibility T3. No specific room for eating (refectory) T4. Lack of trust or respect for teachers or school feeding committee T5. Lack of kitchen materials (makes food preparation time consuming) |
| Strengths | Weaknesses |
| S1. Stunting prevention measures taken before birth and continued into childhood | W1. Big families with many children rarely see effects of Shisha Kibondo as they are often distributing the Shisha Kibondo among all children in the household rather than only serving to the malnourished child |
| Opportunities | Threats |
| O1. Close monitoring through home visits to ensure Shisha Kibondo is properly prepared and consumed O2. More holistic support to vulnerable family instead of to just one child O3. Administer Shisha Kibondo outside the home, e.g., directly in health facilities or ECDs | T1. Provides contradictory messaging to family planning interventions T2. Beneficiaries sell Shisha Kibondo rather than consuming it T3. Beneficiaries dilute and share Shisha Kibondo among many children at home T4. Forgotten age group (support lasts only until 2 years) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Demekas, S.; Prytherch, H.; Bayisenge, F.; Habumugisha, S.; Kraemer, K.; Monroy-Gomez, J.; Nabacu, I.; Speich, C.; Turinimigisha, I.; Barjolle, D. Evaluating Double-Duty Actions in Rwanda’s Secondary Cities. Nutrients 2024, 16, 1998. https://doi.org/10.3390/nu16131998
Demekas S, Prytherch H, Bayisenge F, Habumugisha S, Kraemer K, Monroy-Gomez J, Nabacu I, Speich C, Turinimigisha I, Barjolle D. Evaluating Double-Duty Actions in Rwanda’s Secondary Cities. Nutrients. 2024; 16(13):1998. https://doi.org/10.3390/nu16131998
Chicago/Turabian StyleDemekas, Sophia, Helen Prytherch, Francine Bayisenge, Straton Habumugisha, Klaus Kraemer, Jimena Monroy-Gomez, Immaculée Nabacu, Cornelia Speich, Innocente Turinimigisha, and Dominique Barjolle. 2024. "Evaluating Double-Duty Actions in Rwanda’s Secondary Cities" Nutrients 16, no. 13: 1998. https://doi.org/10.3390/nu16131998