Abstract
Background: Cardiometabolic comorbidities are common in multiple sclerosis (MS), and lifestyle interventions are effective in managing these conditions in the general population, though evidence in the MS patient population is limited. Objective: To evaluate the effect of a multimodal lifestyle intervention on serum apolipoproteins (Apo), creatine kinase (CK), glucose, and insulin in people with progressive MS (PwPMS). Methods: This study included n = 19 PwPMS who participated in a 12-month multimodal lifestyle intervention (including a modified Paleolithic diet, exercise, neuromuscular electrical stimulation, supplements, and stress reduction). Lipid profile (ApoA1, B, and E), CK, glucose, and insulin were obtained at baseline and after 12 months under fasting conditions. Results: At 12 months, there was a marginally significant decrease in ApoB (mean change: −7.17 mg/dL; 95% CI: −14.4, 0.12; p = 0.06), while no significant changes were observed for ApoA1 (mean change: −1.28 mg/dL; 95% CI: 12.33, 9.76; p = 0.80), ApoE (mean change: +0.12 mg/dL; 95% CI: −0.27, 0.52; p = 0.51), CK (mean change: +13.19 U/L; 95% CI: −32.72, 59.11; p = 0.55), Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) (mean change: −0.44; 95% CI: −1.11, 0.22; p = 0.17), and HOMA-β (mean change: +45.62; 95% CI: −95.6, 186.9; p = 0.50). A positive association was observed between changes in HOMA-IR and fatigue changes at 12 months (β = 0.81, p = 0.02), suggesting that an increase in HOMA-IR was linked to increased fatigue, which was no longer significant following the exclusion of outliers (β = 0.71, p = 0.16). Conclusions: A multimodal lifestyle intervention did not negatively impact glycemic and lipid profiles. While improvements were observed in serum biomarkers, these changes were not statistically significant, highlighting the need for stronger evidence from larger, controlled studies to confirm the cardiometabolic health benefits in PwPMS.
1. Introduction
Multiple sclerosis (MS) is a chronic, immune-mediated neuroinflammatory disease with increasing prevalence both nationally and globally [1]. People with progressive MS (PwPMS) are characterized by pronounced neurodegeneration, brain and spinal cord atrophy, and steadily worsening disability [2]. The quality of life (QoL) of PwPMS is significantly diminished as disability advances [3,4]. In addition to MS-specific symptoms, comorbidities, including cardiometabolic conditions, are highly prevalent throughout the disease course [5] and are linked to greater severity of MS [6,7,8], brain volume loss [9,10], and death [11,12]. Emerging evidence suggests that adopting healthy lifestyle behaviors, including dietary modifications, regular physical activity, and mindfulness practices, either separately or in combination, is desirable among people with MS [13,14]. Several surveys have reported that over half of individuals with MS report implementing dietary modification [15,16,17,18]. Additionally, health behavior changes have shown promise in optimizing disease outcomes [19,20,21] and managing comorbid conditions [22,23].
In MS, comorbidities refer to the presence of additional health conditions that coexist alongside MS and require medical care [24]. Cardiometabolic comorbidities are common among PwMS, and their management and prevention are suggested to be a pressing clinical concern [25]. For instance, impairments in lipid and glucose profiles can lead to poor MS disease prognosis [26], specifically with increased total cholesterol (TC), low-density lipoprotein (LDL), triglyceride (TG), and insulin levels being associated with increased MS disability progression [27]. Notably, cardiometabolic comorbidities are often considered modifiable conditions, which could be prevented or improved by lifestyle modifications [28]. While the current evidence preliminarily indicates the promising impact of individual lifestyle factors, including adopting a healthy diet [29,30,31,32,33], exercise training [34,35], and mindfulness therapies [36,37], on clinical and patient-reported outcomes, only sparse evidence exists for how multimodal lifestyle modification interventions impact MS symptoms, as well as cardiometabolic risk factors among PwMS [38,39].
Evidence indicates a link between TC and other lipid biomarkers and disease progression in MS [40,41]. Biomarkers related to the cholesterol pathway, including HDL-C and LDL-C levels, apolipoproteins (ApoA1, ApoAII, ApoB, and ApoE), and other cholesterol metabolites, have been linked to the disruption of the blood–brain barrier [42] and neurodegeneration in MS [9]. In this regard, apolipoproteins, proteins that mediate carriage of cholesterol and other lipids in the serum, are important factors in cholesterol homeostasis and have been shown to be associated with neuroaxonal injury, contributing to MS progression [43,44]. For instance, ApoE is the dominant apolipoprotein in the brain, and its role in MS has been extensively studied [45,46]. Additionally, ApoA1 is involved in HDL biosynthesis and transport, and has a neuroprotective effect on the immune and central nervous systems [47], while ApoB, the major component of LDL, is independently associated with higher Expanded Disability Status Scale (EDSS) scores [26].
Several previous studies have demonstrated the beneficial impact of lifestyle interventions, including diet and exercise, on lipid and glycemic profile biomarkers among people with cardiometabolic conditions [48,49,50]. However, limited research has investigated these effects within the MS community [31,51,52,53]. Notably, our prior work using the data from the same trial [39] showed that this 12-month multimodal intervention including diet, exercise, neuromuscular electrical stimulation, and stress reduction significantly decreased LDL and TG levels as well as increasing HDL levels, which were associated with improvements in fatigue [52]. Additionally, evidence suggests that disruptions in insulin signaling could contribute to the development of neurodegenerative disorders like MS. A recent meta-analysis found that individuals with MS have significantly higher insulin resistance (IR) compared to healthy people, which was more pronounced among individuals with progressive MS, likely due to increased oxidative stress [54]. Building on previous findings regarding the contribution of improvements in lipid markers due to a change in diet and reductions in fatigue [31,52,53,54,55] and the established link between IR and MS [56,57,58], this secondary analysis seeks to further explore the impact of diet-based lifestyle interventions on cardiometabolic health and explore their potential associations with fatigue. We hypothesize that a multimodal lifestyle intervention combining diet, physical activity, stress management, and neuromuscular electrical stimulation will lead to improvements in glycemic and lipid biomarkers. The results of this study could contribute to new practices by promoting the integration of lifestyle modification interventions into MS clinical care. By linking improvements in lipid and glycemic profiles with better clinical outcomes, this study may inform personalized, interdisciplinary strategies for PwPMS.
2. Materials and Methods
2.1. Study Population and Design
The study data of this secondary analysis were obtained from a previously conducted pilot trial studying the impact of a multimodal lifestyle intervention on fatigue over a 12-month period in a sample of 20 PwPMS [39]. The intervention included a modified Paleolithic diet, neuromuscular electrical stimulation, exercise, supplements, and stress reduction. In the present secondary analysis among (n = 19) participants, apolipoprotein and glycemic profile samples were analyzed at baseline and 12-month follow-up.
2.2. Inclusion and Exclusion Criteria
The inclusion criteria for the study were as follows: (1) a diagnosis of progressive MS confirmed by a neurologist specializing in MS, (2) the presence of gait impairment while still being able to walk 25 feet independently or with an assistive device, (3) age 18–65 years old, and an adult companion willing to assist with home exercises and neuromuscular electrical stimulation. The exclusion criteria for the study included the following: (1) a change in the MS diagnosis within the previous 3 months, (2) an active cancer diagnosis (excluding non-melanoma skin cancer), (3) significant cognitive dysfunction, seizure disorders, psychotic disorders, abnormal hepatic or renal functions, (4) abnormal heart rhythm or heart block, (5) unstable heart disease, antiplatelet or anticoagulant medication, (6) lung disease, diabetes requiring changes in medication in the prior three months, (7) an implanted electronic device, and vitamin D levels exceeding 150 ng/mL (or levels above 100 ng/mL accompanied by elevated blood calcium levels over 10.2 mg/dL). Notably, fatigue status was not included in the eligibility criteria for this study [52].
2.3. Study Protocol
The University of Iowa Human Subjects Institutional Review Board provided ethical approval (IRB#201611800) of the study and its protocol on 25 May 2010. All participants provided written informed consent. This study is registered under ClinicalTrials.gov identifier NCT01381354 [39]. Before the intervention began, participants completed a two-week run-in phase focused on educating them about the study’s dietary protocol. During the run-in period, participants were asked to follow the study diet, perform exercise stretches from a stretching exercise program designed for each of them, and keep records of their food intake and physical activity. A trial electrical stimulation session was performed during the second visit. Those who were able to tolerate the electrical stimulation and adhered to the diet for seven consecutive days during the run-in phase were eligible for inclusion in the 12-month study [39].
2.4. Study Diet
The diet component was the foundation of the multimodal intervention, outlining specific foods to prioritize (recommended), avoid (excluded), and incorporate in moderation (encouraged). Participants were guided to consume three daily cup-equivalent servings of sulfur-rich vegetables, leafy greens, and vibrantly colored vegetables and fruits. Foods to avoid included gluten-containing grains, dairy, and eggs. The diet also promoted daily consumption of animal protein (at least 4 ounces), plant-based protein sources (at least 4 ounces), omega-3-rich oils (2 tablespoons), and non-dairy milk alternatives such as soy, almond, rice, or coconut milk. Additionally, participants were encouraged to include nutritional yeast, kelp, and algae supplements like spirulina and chlorella. Intake of gluten-free grains and starchy foods was limited to two servings per week. Participants were advised to eat to fullness.
Weight loss or fasting behaviors were not the goal of this study. If a participant lost 10% of their body weight or more while part of the study, their primary care physician was notified, and the study team worked with the participant to increase higher-calorie foods in their daily intake [35]. Participants were advised to take dietary supplements believed to benefit MS and fatigue but were free to refuse or discontinue them at any time [39].
2.5. Exercise, Neuromuscular Electrical Stimulation, and Stress Reduction
Each participant was provided with a personalized home-based exercise program targeting leg and trunk muscles, which included both stretching and strengthening exercises. The majority of strengthening exercises were combined with neuromuscular electrical stimulation (NMES) to enhance muscle contraction and movement. Initially, participants performed 10–20 repetitions of each exercise within 10 min of electrical stimulation. As participants’ tolerance improved, the number of repetitions and duration of both exercises and electrical stimulation were gradually increased. Participants were instructed to engage in stretching and exercise–NMES at least five days a week. Detailed descriptions of the exercise types and electrical stimulation protocols have been provided in prior publications [52]. For stress reduction, participants were instructed to practice mantra-based meditation and self-massage their hands, feet, and face for a recommended duration of 20 min daily [39].
2.6. Biochemical Marker Assessment
Serum biochemistry analytes, including glucose and creatine kinase, were measured using diagnostic reagent kits, calibrators, and quality control materials from Sekisui Diagnostics (Burlington, MA, USA). Apolipoproteins (ApoA1, B, and E) and insulin were measured using diagnostic immunoturbidometric reagent kits, calibrators, and quality control materials from Kamiya Biomedical Co. (Seattle, WA, USA). All assays were adapted to the ABX Pentra 400 automated chemistry analyzer (Horiba Medical, Irvine, CA, USA). Additionally, Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) was calculated as fasting glucose (mg/dL) multiplied by fasting insulin (μU/mL) divided by 405 [59], where a value of <2 is considered to be insulin-sensitive and a value ≥ 2 is considered to be insulin-resistant. HOMA-β, which assesses beta cell function from fasting glucose and insulin concentrations, was calculated as 360 × fasting insulin (µU/mL)/[fasting glucose (mg/dL) − 63]. All samples were collected in a fasting state in the morning before breakfast.
2.7. Statistical Analysis
A paired t-test was conducted to evaluate changes in creatine kinase (CK), apolipoprotein (ApoA1, ApoB, and ApoE) and glucose (glucose and insulin) profile variables between baseline and 12 months. The association of change in Fatigue Severity Score (FSS) with changes in cardiometabolic variables (ApoA1, ApoB, ApoE, glucose, insulin, and CK) from baseline to 12 months was assessed using general linear models, adjusting for baseline values. The change in FSS from baseline to 12 months served as the dependent variable, while the change in the selected cardiometabolic variable over the same period was treated as the independent variable. No corrections for multiple comparisons were applied, as this analysis is exploratory in nature, aiming to explore potential relationships for future investigations.
3. Results
3.1. Demographic Characteristics
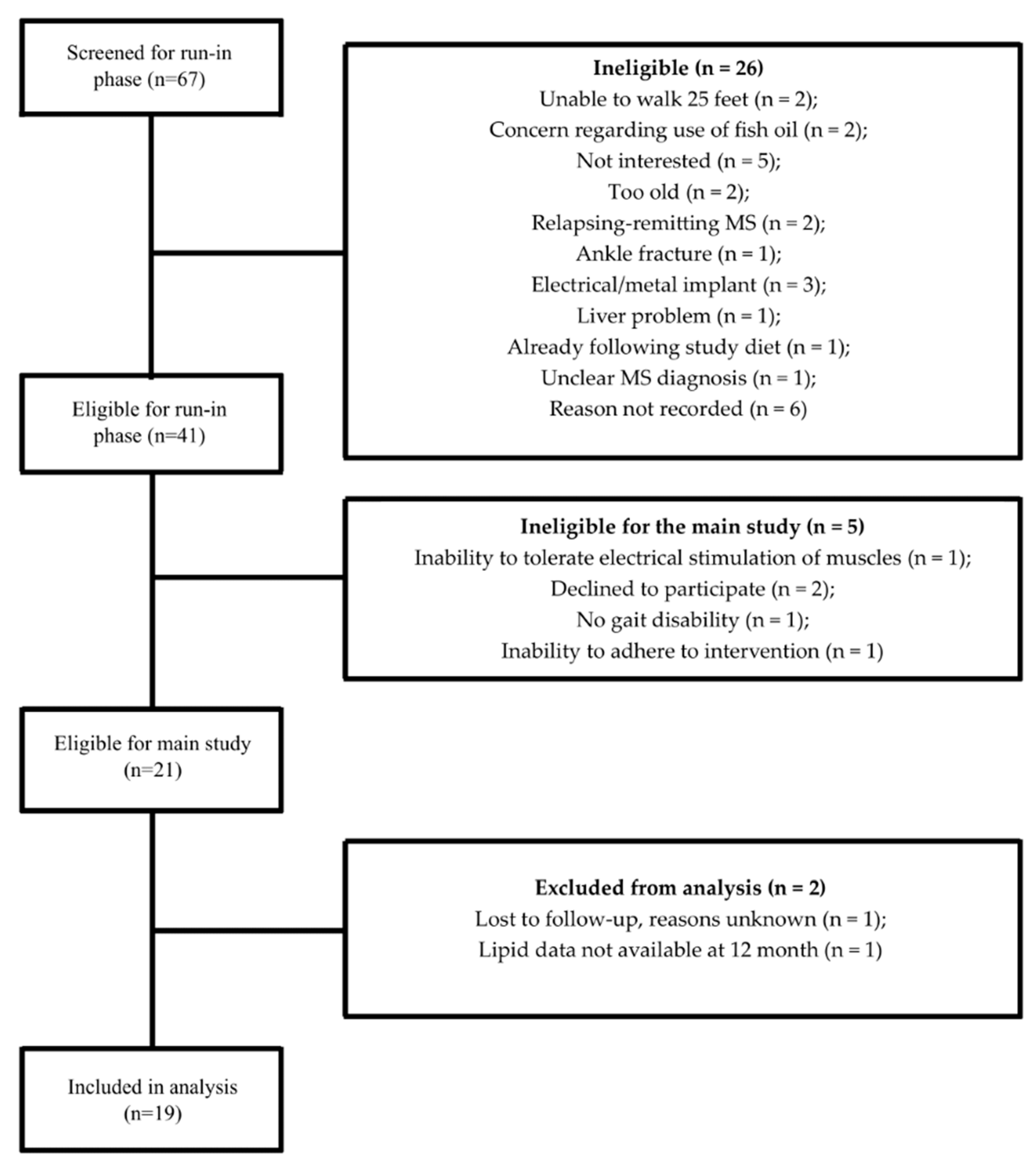
The detailed information of the study participants has been explained in detail elsewhere [39]. Briefly, 19 progressive MS patients were included in the present secondary analysis. Figure 1 shows the CONSORT diagram for the present sub-study.
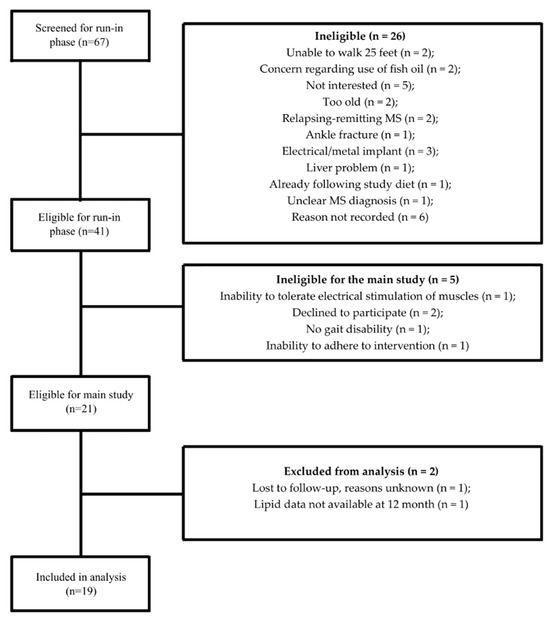
Figure 1.
CONSORT diagram for the cardiometabolic marker sub-study.
Table 1 displays the baseline clinical and demographic characteristics of the participants. As this was a cohort of PwPMS, the majority (n = 14, 73.7%) used a walking aid. Sixteen participants had a baseline FSS score ≥ 4.0. Nine of the nineteen subjects (47.4%) were taking approved disease-modifying therapies (DMTs). Treatment choices were determined by the patients’ attending neurologists, and no adjustments to their DMTs were introduced as part of the study.

Table 1.
Characteristics of study participants a.
3.2. Cardiometabolic Marker Change
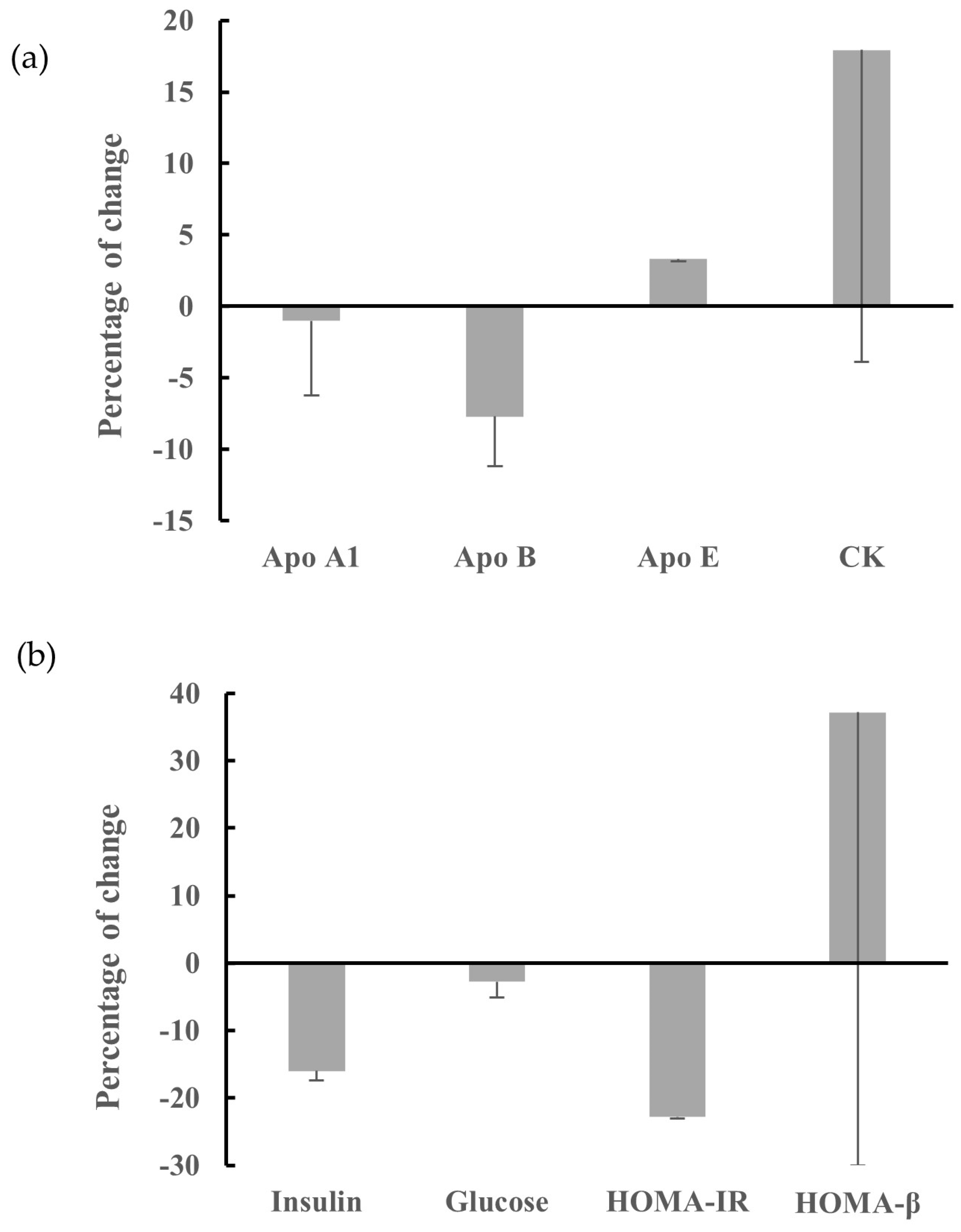
As shown in Figure 2, ApoB showed a marginally significant decrease at 12 months compared to baseline (mean change: −7.17 mg/dL; 95% CI: −14.4 0.12; p = 0.06), while no changes were observed for ApoA1 (mean change: −1.28 mg/dL; 95% CI: −12.33, 9.76; p = 0.80), ApoE (mean change: +0.12 mg/dL; 95% CI: −0.27, 0.52; p = 0.51), CK (mean change: +13.19 U/L; 95% CI: −32.72, 59.11; p = 0.55), glucose (mean change: −2.51 mg/dL; 95% CI: −7.42, 2.39; p = 0.29), HOMA-IR (mean change: −0.44; 95% CI: −1.11, 0.22; p = 0.17), HOMA-β (mean change: +45.62; 95% CI: −95.6, 186.9; p = 0.50), or insulin (mean change: −1.34 μIU/mL; 95% CI: −4.30, 1.60; p = 0.34). We also performed analyses excluding subject IDs 5 and 18 as outliers. Subject ID 5, diagnosed with chronic lymphocytic leukemia (CLL) (a consequence of prior mitoxantrone use for SPMS), exhibited an unexpected sharp rise in serum insulin (Figure S1). Subject ID 18 had the highest disability level at baseline (EDSS = 8) and demonstrated a high rate of progressive decline after diagnosis [39]. However, the exclusion of these two subjects did not alter any of the findings. Additionally, mean changes from baseline at 6 months showed no significant differences in any biomarkers or their associations with fatigue (Tables S1 and S2).
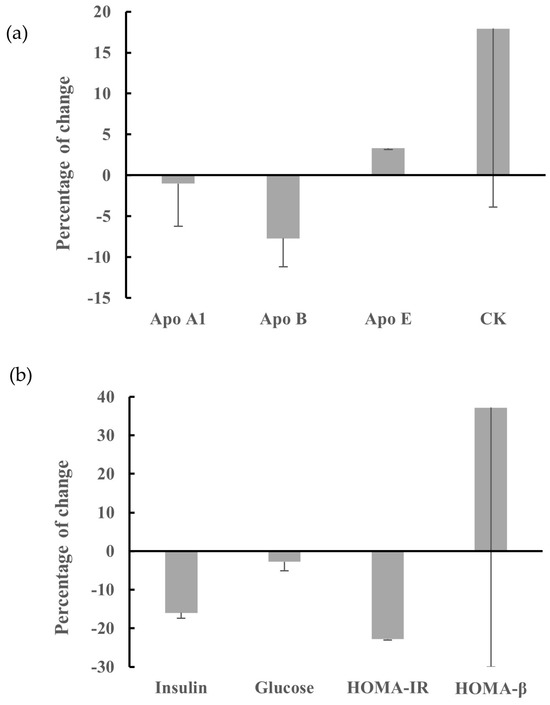
Figure 2.
Percentage of change from baseline for serum cardiometabolic markers including: (a) ApoA1, B, E, and CK; and (b) insulin, glucose, HOMA-IR, and HOMA-β, following multimodal intervention among n = 19 participants.
Changes in HOMA-IR were significantly associated with changes in FSS at 12 months among n = 19 (including subject IDs 5 and 18), with β-coefficients (95% CI) of 0.81 (0.12, 1.5; p = 0.02; Table 2). However, after excluding subject IDs 5 and 18, the association was no longer significant (β = 0.71 (−0.33, 1.75; p = 0.16); Figure S2). No significant associations were observed between changes in apolipoproteins and CK and changes in FSS (Table 2).
Table 2.
Association of 12-month changes in fatigue with cardiometabolic marker change among n = 19 participants with progressive MS following a multimodal intervention.
4. Discussion
The findings of the current secondary analysis of a previous pilot study suggest that a multimodal lifestyle intervention including a modified Paleolithic diet, exercises, neuromuscular electrical stimulation, stress management techniques, and supplementation may lead to a modest reduction in ApoB levels. Furthermore, ApoE, CK, and HOMA-β demonstrated a non-significant upward trend, while HOMA-IR exhibited a downward trend. Additionally, a positive association was found between the change in insulin resistance and the change in fatigue, suggesting that improvements or worsening in insulin resistance may be correspondingly linked to improvements or worsening in fatigue; however, after excluding outliers from the analyses, the association between insulin resistance and fatigue was no longer statistically significant.
Comorbidities are increasingly prevalent in MS [5]. Growing evidence suggests that unhealthy lifestyle habits, including poor diet quality, stress, and physical inactivity, negatively affect disability in PwMS [60,61] and are associated with greater risk of comorbidities, such as cardiovascular diseases [62]. Previous studies have shown that PwMS who had one or more cardiovascular risk factors had an increased lesion burden and more advanced brain atrophy [63]. In addition to their clinical impact, the presence of comorbid conditions in individuals with MS has been associated with diagnostic delays and increased hospitalizations [64]. Adopting health behaviors, including a healthy diet and moderate exercise, have been shown to be associated with a decreased risk of comorbidities and increased likelihood of higher QoL [65].
Increasing research has focused on the impact of lifestyle modification interventions, whether implemented individually or in combination, on clinical and patient-reported outcomes, along with lipid and glucose profiles, yielding encouraging results [23,38,66]. Findings from the original pilot study, which included the population analyzed in this sub-study, showed that adopting a diet-based multimodal intervention over 12 months led to significant improvements in fatigue, QoL [39], mood, and cognition [67]. Additionally, reductions in fatigue were linked to elevation in HDL-C and changes in TC over the 12-month period [52]. In the present study, both insulin and glucose exhibited a decreasing trend at 12 months, though the changes were not statistically significant. Furthermore, a positive association was observed between insulin resistance (calculated as HOMA-IR, which incorporates both fasting insulin and glucose) and changes in fatigue (measured as FSS score). Specifically, for every one-unit increase in HOMA-IR (worsening insulin resistance), fatigue (FSS score) is predicted to increase by 0.81 units. This suggests that higher insulin resistance is associated with higher fatigue. A positive slope was observed both with all data included and after excluding two subjects, indicating a positive association between changes in insulin resistance and fatigue in both cases. However, after excluding these two subjects—who appeared to be the primary drivers of the relationship—the association was no longer significant. Similarly, when all participants were included, HOMA-β (β-cell function) increased from 123% to 168%, remaining within the normal range. However, after excluding IDs 5 and 18, HOMA-β showed a slight decrease (from 104% at baseline to 90% after the 12-month intervention).
The finding of improved insulin levels observed in the present study is consistent with prior research from the Wahls research team, which demonstrated that a modified Paleolithic elimination (Wahls) diet resulted in statistically and clinically significant reductions in insulin levels at 12 and 24 weeks compared to a low-saturated fat (Swank) diet group [53]. However, no association was found between changes in insulin and changes in fatigue status in that study. These findings also align with other studies indicating that a Paleolithic diet significantly lowers plasma insulin and enhances insulin sensitivity in obese participants without MS [68].
In the present study, the apolipoprotein profile showed non-significant improvements, a decrease in ApoB and an increase in ApoE, and no associations with changes in fatigue. Based on the significant improvements found in HDL-c and LDL-c in a previous secondary analysis of the same sub-population [52], we had expected to potentially observe similar significant improvements in their corresponding apolipoproteins. However, these results might be attributed to the fact that changes in apolipoprotein levels may take longer to manifest due to differences in regulatory mechanisms, slower turnover rates of apolipoproteins, and the distinct effects of diet on lipids compared to proteins. Consistent with our findings, a study examining the effects of the Mediterranean–DASH Intervention for Neurodegenerative Delay (MIND) diet, promoting the intake of healthy fats, particularly monounsaturated fats and omega-3s, on biochemical markers and clinical outcomes in PwMS also observed significant reductions in LDL-c and TG, along with improvements in clinical outcomes. However, similar to our study, no significant changes in ApoA1 and ApoB levels were observed [69]. Additionally, in another four-month pilot study analyzing the relationship between lipid profile, functional disability, and fat consumption in individuals with MS following intervention with epigallocatechin gallate and coconut oil, it was found that TG levels decreased in the intervention group compared to the control group, which was positively correlated with an improvement in functional disability, as assessed by the EDSS, and negatively correlated with HDL and ApoA1 levels [70].
In another study by Niesten et al., the cardiometabolic health effects of replacing sitting with light-intensity physical activity throughout the day were compared to a single bout of vigorous-intensity exercise in PwMS [71]. This randomized cross-over study found that both light-intensity physical activity and vigorous-intensity exercise led to significant improvements in insulin sensitivity, blood lipids, and inflammatory markers compared to prolonged sitting. Notably, there was no significant change in ApoA1 compared to the control, while similarly to our results, ApoB decreased following light-intensity physical activity compared to sitting [71].
Investigating changes in apolipoproteins in the context of MS holds great importance due to their association with disease outcomes and progression, as well as their potential role as an accurate biomarker for assessing cardiovascular disease [72,73]. A systematic review, examining the relationship between levels of cholesterol and markers of cholesterol turnover and MS disease outcomes, suggests that elevated levels of circulating LDL-C, TC, and particularly ApoB are associated with adverse clinical and MRI outcomes in MS [73]. Greater ApoB levels have been shown to be associated with an increased number of new or enlarging T2 lesions over a two-year period in clinically isolated syndrome [74]. Additionally, ApoB, the key structural protein of atherogenic lipoproteins, may serve as a reliable marker for assessing vascular injury. The findings of this study are significant, as they emphasize the role of lifestyle modifications in improving not only MS-specific outcomes but also a few markers of vascular comorbidities, underscoring the need for further investigation.
In the present study, a non-significant increase in serum CK levels was observed following multimodal intervention. However, evidence regarding the impact of lifestyle behavior changes on serum CK levels in the context of MS is limited. Previous research has shown that CK activity is significantly lower in individuals with MS compared to healthy controls [69,75]. Our findings align with a study investigating the biochemical effects of the MIND diet in people with MS, which also reported a non-significant increase in serum CK levels following a 12-week dietary intervention [69]. Reduced CK activity in MS may be attributed to decreased muscle activity, as physical activity often declines due to factors such as weakness, fatigue, medication, or disability related to the disease itself [75].
The present secondary analysis was limited by the pilot trial’s unblinded single-arm design, which involved a small sample size of 19 participants with progressive MS. It should be emphasized that all participants were instructed to take up to two tablespoons of omega-3 fats in addition to the study diet. The observed improvements in the lipid profile may be attributed to the omega-3 supplementation. Additionally, another limitation of this study is the difficulty in obtaining reliable measurements of CK. CK levels can exhibit significant individual variability due to factors such as physical activity, type of exercise, underlying muscle mass, and other physiological conditions. This variability can affect the interpretation of CK data and may obscure potential effects of the intervention. Future studies should consider strategies to account for this variability, such as standardizing physical activity levels, volitional and neuromuscular electrical-stimulation-augmented exercise duration and intensity, body composition assessments prior to measurements, or using additional biomarkers to corroborate CK findings.
Overall, this study suggests improvement in cardiometabolic markers following a 12-month intervention. While we acknowledge that the clinical impact of these findings is limited, there are several factors which could explain the lack of significant effects: (1) the small sample size of 19 participants may have limited the statistical power to detect significant changes; (2) the 12-month duration of the intervention may not have been sufficient to observe significant changes in some cardiometabolic markers, which may require longer intervention periods to show measurable effects; (3) the participants’ baseline health status, for example the presence or development of new comorbidities (e.g., CLL), may have influenced their response to the intervention; and (4) the sensitivity of the biomarkers used to assess cardiometabolic health may vary. Some markers may not be as responsive to lifestyle changes as others, and more sensitive or additional biomarkers could be considered in future research. Thus, while the data observed in our study are promising, the limited clinical impact underscores the need for future research with larger sample sizes, extended follow-up periods, inclusion of a control group, and a more comprehensive set of biomarkers to fully evaluate the potential benefits of multimodal lifestyle interventions in PwPMS.
5. Conclusions
In conclusion, the current study demonstrated a marginally significant reduction in ApoB levels. Additionally, ApoE, CK, and HOMA-β exhibited a non-significant favorable upward trend, while HOMA-IR showed a decreasing trend, suggesting a potentially beneficial response. Furthermore, a positive association was observed between changes in insulin resistance and changes in fatigue, highlighting the potential role of lifestyle interventions in improving glycemic control and lipid profiles in individuals with MS. Although we did not observe significant mean changes in cardiometabolic markers from baseline, it is worth noting that no significant negative changes were observed over the 12-month period either. Future controlled clinical trials are warranted to confirm and validate these findings.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/nu17071163/s1. Figure S1: Serum insulin levels for individual participants (identified by ID) before and following 12-month multimodal intervention. Participant ID 5 was undergoing treatment for CLL. Figure S2: Scatter plot depicting the relationship between changes in fatigue and HOMA-IR among n = 19 (blue line and circles; β = 0.81, p = 0.02) and n = 17 (red dashed line and triangles; β = 0.71, p = 0.16), excluding subject IDs 5 and 18. Table S1: Mean changes from baseline for serum cardiometabolic markers following multimodal intervention at 6 months and 12 months. Table S2: Association of 6-month changes in fatigue with cardiometabolic markers change among individuals with progressive MS following a multimodal intervention.
Author Contributions
Conceptualization, F.S., T.J.T., M.R. and T.L.W.; formal analysis, F.S.; investigation, F.S., A.S.M., A.J.B. and M.S.; writing—original draft preparation, A.S.M., A.J.B. and F.S.; writing—review and editing, F.S., T.J.T., M.R., M.S., B.B., W.G.D., C.M.G., L.G.S. and T.L.W.; visualization, F.S.; supervision, T.L.W.; funding acquisition, T.L.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by Direct-MS, with additional in-kind contributions from the University of Iowa Institute for Clinical and Translational Sciences, funded through a Clinical and Translational Science Award (CTSA, Grant: U54TR001356) from the National Center for Advancing Translational Sciences. Other in-kind support was provided by DJO Inc., Pinnaclife Inc., TZ Press LLC, and the Iowa City Veterans Administration Healthcare System in Iowa City, IA. The views expressed in this publication are those of the authors and do not necessarily reflect the official opinions of the National Institutes of Health (NIH) or the Veterans Administration. Dr. Murali Ramanathan and his team at the University at Buffalo, State University of New York, did not receive any financial support for their involvement in this research. The funding organizations had no influence over the study’s design, data collection or analysis, publication decision, or manuscript preparation.
Institutional Review Board Statement
The study was reviewed and approved by the Institutional Review Board (IRB Identifier 201611800, 25 May 2010).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All relevant data are within the manuscript, the tables, and figures.
Conflicts of Interest
T.L.W. personally follows and promotes the Wahls™ diet. She has equity interest in the following companies: Terry Wahls LLC; TZ Press LLC; The Wahls Institute, PLC; FBB Biomed Inc.; Levels Health Inc.; Foogal Inc.; and the website http://www.terrywahls.com. She also owns the copyright to the books Minding My Mitochondria (second edition), The Wahls Protocol, and The Wahls Protocol Cooking for Life, and the trademarks The Wahls Protocol®, Wahls™ diet, Wahls Paleo™ diet, Wahls Paleo Plus™ diet, and Wahls Behavior Change™. She has received grant funding from the National Multiple Sclerosis Society for the Dietary Approaches to Treating Multiple Sclerosis Related Fatigue Study. She receives royalty payments from Penguin Random House. T.L.W. has conflict-of-interest management plans in place with the University of Iowa and the Iowa City Veteran’s Affairs Medical Center. All other co-authors have no conflicts to disclose.
Abbreviations
The following abbreviations are used in this manuscript:
| BMI | Body Mass Index |
| CIS | Clinically isolated syndrome |
| CK | Creatine kinase |
| CLL | Chronic lymphocytic leukemia |
| CNS | Central nervous system |
| CPB | Cholesterol pathway biomarkers |
| DMT | Disease-modifying treatment |
| EDSS | Expanded Disability Status Scale |
| EGCG | Epigallocatechin gallate |
| EX | Vigorous-intensity exercise |
| FSS | Fatigue Severity Scale |
| HDL | High-density lipoprotein |
| HOMA-IR | Homeostasis Model Assessment of Insulin Resistance |
| IR | Insulin resistance |
| LDL | Low-density lipoprotein |
| LIPA | Light-intensity physical activity |
| MIND | Mediterranean–DASH Intervention for Neurodegenerative Delay |
| MRI | Magnetic resonance imaging |
| NMES | Neuromuscular electrical stimulation |
| PP-MS | Primary progressive multiple sclerosis |
| PwMS | People with multiple sclerosis |
| SP-MS | Secondary progressive multiple sclerosis |
| TC | Total cholesterol |
| TG | Triglyceride |
References
- Walton, C.; King, R.; Rechtman, L.; Kaye, W.; Leray, E.; Marrie, R.A.; Robertson, N.; La Rocca, N.; Uitdehaag, B.; van der Mei, I.; et al. Rising prevalence of multiple sclerosis worldwide: Insights from the Atlas of MS, third edition. Mult. Scler. J. 2020, 26, 1816–1821. [Google Scholar]
- McGinley, M.P.; Goldschmidt, C.H.; Rae-Grant, A.D. Diagnosis and Treatment of Multiple Sclerosis: A Review. JAMA 2021, 325, 765–779. [Google Scholar] [PubMed]
- Hadjimichael, O.; Vollmer, T.; Oleen-Burkey, M. Fatigue characteristics in multiple sclerosis: The North American Research Committee on Multiple Sclerosis (NARCOMS) survey. Health Qual Life Outcomes 2008, 6, 100. [Google Scholar] [PubMed]
- Krupp, L.B.; Serafin, D.J.; Christodoulou, C. Multiple sclerosis-associated fatigue. Expert Rev. Neurother. 2010, 10, 1437–1447. [Google Scholar] [CrossRef]
- Marrie, R.A.; Cohen, J.; Stuve, O.; Trojano, M.; Sørensen, P.S.; Reingold, S.; Cutter, G.; Reider, N. A systematic review of the incidence and prevalence of comorbidity in multiple sclerosis: Overview. Mult. Scler. J. 2015, 21, 263–281. [Google Scholar]
- Marrie, R.A.; Rudick, R.; Horwitz, R.; Cutter, G.; Tyry, T.; Campagnolo, D.; Vollmer, T. Vascular comorbidity is associated with more rapid disability progression in multiple sclerosis. Neurology 2010, 74, 1041–1047. [Google Scholar]
- Marrie, R.A.; Elliott, L.; Marriott, J.; Cossoy, M.; Tennakoon, A.; Yu, N. Comorbidity increases the risk of hospitalizations in multiple sclerosis. Neurology 2015, 84, 350–358. [Google Scholar]
- Kowalec, K.; McKay, K.A.; Patten, S.B.; Fisk, J.D.; Evans, C.; Tremlett, H.; Marrie, R.A.; CIHR Team in Epidemiology and Impact of Comorbidity on Multiple Sclerosis (ECoMS). Comorbidity increases the risk of relapse in multiple sclerosis: A prospective study. Neurology 2017, 89, 2455–2461. [Google Scholar] [CrossRef]
- Murali, N.; Browne, R.W.; Maxwell, K.F.; Bodziak, M.L.; Jakimovski, D.; Hagemeier, J.; Bergsland, N.; Weinstock-Guttman, B.; Zivadinov, R.; Ramanathan, M. Cholesterol and neurodegeneration: Longitudinal changes in serum cholesterol biomarkers are associated with new lesions and gray matter atrophy in multiple sclerosis over 5 years of follow-up. Eur. J. Neurol. 2020, 27, 188-e4. [Google Scholar]
- Jakimovski, D.; Gandhi, S.; Paunkoski, I.; Bergsland, N.; Hagemeier, J.; Ramasamy, D.P.; Hojnacki, D.; Kolb, C.; Benedict, R.H.B.; Weinstock-Guttman, B.; et al. Hypertension and heart disease are associated with development of brain atrophy in multiple sclerosis: A 5-year longitudinal study. Eur. J. Neurol. 2019, 26, 87-e8. [Google Scholar]
- Chou, I.J.; Kuo, C.F.; Tanasescu, R.; Tench, C.R.; Tiley, C.G.; Constantinescu, C.S.; Whitehouse, W.P. Comorbidity in multiple sclerosis: Its temporal relationships with disease onset and dose effect on mortality. Eur. J. Neurol. 2020, 27, 105–112. [Google Scholar] [PubMed]
- Marrie, R.A.; Elliott, L.; Marriott, J.; Cossoy, M.; Blanchard, J.; Leung, S.; Yu, N. Effect of comorbidity on mortality in multiple sclerosis. Neurology 2015, 85, 240–247. [Google Scholar] [PubMed]
- Silveira, S.L.; Richardson, E.V.; Motl, R.W. Desired Resources for Changing Diet Among Persons with Multiple Sclerosis: Qualitative Inquiry Informing Future Dietary Interventions. Int. J. MS Care 2022, 24, 175–183. [Google Scholar] [CrossRef]
- Elkhalii-Wilhelm, S.; Sippel, A.; Riemann-Lorenz, K.; Kofahl, C.; Scheiderbauer, J.; Arnade, S.; Kleiter, I.; Schmidt, S.; Heesen, C. Experiences of persons with Multiple Sclerosis with lifestyle adjustment-A qualitative interview study. PLoS ONE 2022, 17, e0268988. [Google Scholar]
- Anderson, H.D.; Leister, N.R.; Biely, S.A. The perceptions of persons with multiple sclerosis (MS) on the impact of diet and supplements on MS symptoms. J. Altern. Complement Med. 2022, 8, 221. [Google Scholar]
- Marck, C.H.; Probst, Y.; Chen, J.; Taylor, B.; van der Mei, I. Dietary patterns and associations with health outcomes in Australian people with multiple sclerosis. Eur. J. Clin. Nutr. 2021, 75, 1506–1514. [Google Scholar]
- Fitzgerald, K.C.; Tyry, T.; Salter, A.; Cofield, S.S.; Cutter, G.; Fox, R.J.; Marrie, R.A. A survey of dietary characteristics in a large population of people with multiple sclerosis. Mult. Scler. Relat. Disord. 2018, 22, 12–18. [Google Scholar]
- Russell, R.D.; Lucas, R.M.; Brennan, V.; Sherriff, J.L.; Begley, A.; Investigator, G.A.; Black, L.J. Reported Changes in Dietary Behavior Following a First Clinical Diagnosis of Central Nervous System Demyelination. Front. Neurol. 2018, 9, 161. [Google Scholar]
- Fidao, A.; Jelinek, G.; Simpson-Yap, S.; Neate, S.; Nag, N. Engagement with three or more healthy lifestyle behaviours is associated with improved quality of life over 7.5 years in people with multiple sclerosis. Eur. J. Neurol. 2023, 30, 3190–3199. [Google Scholar]
- Giovannoni, G.; Ford, H.L.; Schmierer, K.; Middleton, R.; Stennett, A.M.; Pomeroy, I.; Fisniku, L.; Scalfari, A.; Bannon, C.; Stross, R.; et al. MS care: Integrating advanced therapies and holistic management. Front. Neurol. 2023, 14, 1286122. [Google Scholar] [CrossRef]
- Reece, J.; Jelinek, G.A.; Milanzi, E.; Simpson-Yap, S.; Neate, S.L.; Taylor, K.L.; Jelinek, P.L.; Davenport, R.; Bevens, W.; Yu, M. Lifestyle changes and patient-reported outcomes over five years in a sample of people with multiple sclerosis after a single multimodal intensive lifestyle education workshop. Neurol. Sci. 2024, 46, 835–844. [Google Scholar]
- Moss, B.P.; Rensel, M.R.; Hersh, C.M. Wellness and the Role of Comorbidities in Multiple Sclerosis. Neurotherapeutics 2017, 14, 999–1017. [Google Scholar] [PubMed]
- Allogmanny, S.; Probst, Y. Dietary Modification Combined with Nutrition Education and Counseling for Metabolic Comorbidities in Multiple Sclerosis: Implications for Clinical Practice and Research. Curr. Nutr. Rep. 2024, 13, 106–112. [Google Scholar]
- Marrie, R.A.; Fisk, J.D.; Fitzgerald, K.; Kowalec, K.; Maxwell, C.; Rotstein, D.; Salter, A.; Tremlett, H. Etiology, effects and management of comorbidities in multiple sclerosis: Recent advances. Front. Immunol. 2023, 14, 1197195. [Google Scholar]
- Salter, A.; Lancia, S.; Kowalec, K.; Fitzgerald, K.C.; Marrie, R.A. Comorbidity and Disease Activity in Multiple Sclerosis. JAMA Neurol. 2024, 81, 1170–1177. [Google Scholar] [PubMed]
- Tettey, P.; Simpson, S., Jr.; Taylor, B.; Blizzard, L.; Ponsonby, A.L.; Dwyer, T.; Kostner, K.; van der Mei, I. An adverse lipid profile is associated with disability and progression in disability, in people with MS. Mult. Scler. J. 2014, 20, 1737–1744. [Google Scholar]
- Weinstock-Guttman, B.; Zivadinov, R.; Mahfooz, N.; Carl, E.; Drake, A.; Schneider, J.; Teter, B.; Hussein, S.; Mehta, B.; Weiskopf, M.; et al. Serum lipid profiles are associated with disability and MRI outcomes in multiple sclerosis. J. Neuroinflamm. 2011, 8, 127. [Google Scholar]
- Nociti, V.; Romozzi, M. The Importance of Managing Modifiable Comorbidities in People with Multiple Sclerosis: A Narrative Review. J. Pers. Med. 2023, 13, 1524. [Google Scholar] [CrossRef]
- Wahls, T.L.; Titcomb, T.J.; Bisht, B.; Eyck, P.T.; Rubenstein, L.M.; Carr, L.J.; Darling, W.G.; Hoth, K.F.; Kamholz, J.; Snetselaar, L.G. Impact of the Swank and Wahls elimination dietary interventions on fatigue and quality of life in relapsing-remitting multiple sclerosis: The WAVES randomized parallel-arm clinical trial. Mult. Scler. J. Exp. Transl. Clin. 2021, 7, 20552173211035399. [Google Scholar]
- Irish, A.K.; Erickson, C.M.; Wahls, T.L.; Snetselaar, L.G.; Darling, W.G. Randomized control trial evaluation of a modified Paleolithic dietary intervention in the treatment of relapsing-remitting multiple sclerosis: A pilot study. Degener. Neurol. Neuromuscul. Dis. 2017, 7, 1–18. [Google Scholar]
- Lee, J.E.; Titcomb, T.J.; Bisht, B.; Rubenstein, L.M.; Louison, R.; Wahls, T.L. A Modified MCT-Based Ketogenic Diet Increases Plasma β-Hydroxybutyrate but Has Less Effect on Fatigue and Quality of Life in People with Multiple Sclerosis Compared to a Modified Paleolithic Diet: A Waitlist-Controlled, Randomized Pilot Study. J. Am. Coll. Nutr. 2021, 40, 13–25. [Google Scholar] [PubMed]
- Parks, N.E.; Jackson-Tarlton, C.S.; Vacchi, L.; Merdad, R.; Johnston, B.C. Dietary interventions for multiple sclerosis-related outcomes. Cochrane Database Syst. Rev. 2020, 5, Cd004192. [Google Scholar]
- Katz Sand, I.; Benn, E.K.T.; Fabian, M.; Fitzgerald, K.C.; Digga, E.; Deshpande, R.; Miller, A.; Gallo, S.; Arab, L. Randomized-controlled trial of a modified Mediterranean dietary program for multiple sclerosis: A pilot study. Mult. Scler. Relat. Disord. 2019, 36, 101403. [Google Scholar] [CrossRef] [PubMed]
- Hortobágyi, T.; Ács, P.; Baumann, P.; Borbély, G.; Áfra, G.; Reichardt-Varga, E.; Sántha, G.; Tollár, J. Comparative Effectiveness of 4 Exercise Interventions Followed by 2 Years of Exercise Maintenance in Multiple Sclerosis: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2022, 103, 1908–1916. [Google Scholar] [CrossRef]
- Beratto, L.; Bressy, L.; Agostino, S.; Malandrone, F.; Brichetto, G.; Ponzano, M. The effect of exercise on mental health and health-related quality of life in individuals with multiple sclerosis: A Systematic review and meta-analysis. Mult. Scler. Relat. Disord. 2024, 83, 105473. [Google Scholar] [CrossRef]
- Morrow, S.A.; Riccio, P.; Vording, N.; Rosehart, H.; Casserly, C.; MacDougall, A. A mindfulness group intervention in newly diagnosed persons with multiple sclerosis: A pilot study. Mult. Scler. Relat. Disord. 2021, 52, 103016. [Google Scholar]
- Senders, A.; Hanes, D.; Bourdette, D.; Carson, K.; Marshall, L.M.; Shinto, L. Impact of mindfulness-based stress reduction for people with multiple sclerosis at 8 weeks and 12 months: A randomized clinical trial. Mult. Scler. J. 2018, 25, 1178–1188. [Google Scholar] [CrossRef]
- Marck, C.H.; De Livera, A.M.; Brown, C.R.; Neate, S.L.; Taylor, K.L.; Weiland, T.J.; Hadgkiss, E.J.; Jelinek, G.A. Health outcomes and adherence to a healthy lifestyle after a multimodal intervention in people with multiple sclerosis: Three year follow-up. PLoS ONE 2018, 13, e0197759. [Google Scholar] [CrossRef] [PubMed]
- Bisht, B.; Darling, W.G.; Shivapour, E.T.; Lutgendorf, S.K.; Snetselaar, L.G.; Chenard, C.A.; Wahls, T.L. Multimodal intervention improves fatigue and quality of life in subjects with progressive multiple sclerosis: A pilot study. Degener. Neurol. Neuromuscul. Dis. 2015, 5, 19–35. [Google Scholar]
- Podbielska, M.; O’Keeffe, J.; Pokryszko-Dragan, A. New Insights into Multiple Sclerosis Mechanisms: Lipids on the Track to Control Inflammation and Neurodegeneration. Int. J. Mol. Sci. 2021, 22, 7319. [Google Scholar] [CrossRef]
- Gafson, A.R.; Thorne, T.; McKechnie, C.I.J.; Jimenez, B.; Nicholas, R.; Matthews, P.M. Lipoprotein markers associated with disability from multiple sclerosis. Sci. Rep. 2018, 8, 17026. [Google Scholar]
- Fellows, K.; Uher, T.; Browne, R.W.; Weinstock-Guttman, B.; Horakova, D.; Posova, H.; Vaneckova, M.; Seidl, Z.; Krasensky, J.; Tyblova, M.; et al. Protective associations of HDL with blood-brain barrier injury in multiple sclerosis patients. J. Lipid Res. 2015, 56, 2010–2018. [Google Scholar]
- McComb, M.; Parambi, R.; Browne, R.W.; Bodziak, M.L.; Jakimovski, D.; Bergsland, N.; Maceski, A.; Weinstock-Guttman, B.; Kuhle, J.; Zivadinov, R.; et al. Apolipoproteins AI and E are associated with neuroaxonal injury to gray matter in multiple sclerosis. Mult. Scler. Relat. Disord. 2020, 45, 102389. [Google Scholar]
- Pinholt, M.; Frederiksen, J.L.; Christiansen, M. The association between apolipoprotein E and multiple sclerosis. Eur. J. Neurol. 2006, 13, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Chapman, J.; Vinokurov, S.; Achiron, A.; Karussis, D.M.; Mitosek–Szewczyk, K.; Birnbaum, M.; Michaelson, D.M.; Korczyn, A.D. APOE genotype is a major predictor of long-term progression of disability in MS. Neurology 2001, 56, 312–316. [Google Scholar] [CrossRef]
- Zhang, H.-L.; Wu, J.; Zhu, J. The Immune-Modulatory Role of Apolipoprotein E with Emphasis on Multiple Sclerosis and Experimental Autoimmune Encephalomyelitis. J. Immunol. Res. 2010, 2010, 186813. [Google Scholar]
- McComb, M.; Krikheli, M.; Uher, T.; Browne, R.W.; Srpova, B.; Oechtering, J.; Maceski, A.M.; Tyblova, M.; Jakimovski, D.; Ramasamy, D.P.; et al. Neuroprotective associations of apolipoproteins A-I and A-II with neurofilament levels in early multiple sclerosis. J. Clin. Lipidol. 2020, 14, 675–684.e2. [Google Scholar] [PubMed]
- Höchsmann, C.; Dorling, J.L.; Martin, C.K.; Newton, R.L.; Apolzan, J.W.; Myers, C.A.; Denstel, K.D.; Mire, E.F.; Johnson, W.D.; Zhang, D.; et al. Effects of a 2-Year Primary Care Lifestyle Intervention on Cardiometabolic Risk Factors. Circulation 2021, 143, 1202–1214. [Google Scholar]
- Villareal, D.T.; Miller, B.V.; Banks, M.; Fontana, L.; Sinacore, D.R.; Klein, S. Effect of lifestyle intervention on metabolic coronary heart disease risk factors in obese older adults2. Am. J. Clin. Nutr. 2006, 84, 1317–1323. [Google Scholar]
- Keshani, M.; Feizi, A.; Askari, G.; Sharma, M.; Bagherniya, M. Effects of therapeutic lifestyle change diets on blood lipids, lipoproteins, glycemic parameters, and blood pressure: A systematic review and meta-analysis of clinical trials. Nutr. Rev. 2024, 82, 176–192. [Google Scholar] [CrossRef]
- Monazamnezhad, A.; Habibi, A.; Shakeriyan, S.; Majdinasab, N.; Ghalvand, A. The Effects of Aerobic Exercise on Lipid Profile and Body Composition in Women with Multiple Sclerosis. Jundishapur J. Chronic Dis. Care 2015, 4, e26619. [Google Scholar] [CrossRef]
- Fellows Maxwell, K.; Wahls, T.; Browne, R.W.; Rubenstein, L.; Bisht, B.; Chenard, C.A.; Snetselaar, L.; Weinstock-Guttman, B.; Ramanathan, M. Lipid profile is associated with decreased fatigue in individuals with progressive multiple sclerosis following a diet-based intervention: Results from a pilot study. PLoS ONE 2019, 14, e0218075. [Google Scholar] [CrossRef] [PubMed]
- Villa, A.T.; Tu, B.H.; Titcomb, T.J.; Saxby, S.M.; Shemirani, F.; Eyck, P.T.; Rubenstein, L.M.; Snetselaar, L.G.; Wahls, T.L. Association between improved metabolic risk factors and perceived fatigue during dietary intervention trial in relapsing-remitting multiple sclerosis: A secondary analysis of the WAVES trial. Front. Neurol. 2023, 13, 1022728. [Google Scholar] [CrossRef]
- Sepidarkish, M.; Kalantari, N.; Gorgani-Firouzjaee, T.; Rostami-Mansoor, S.; Shirafkan, H. Association between insulin resistance and multiple sclerosis: A systematic review and meta-analysis. Metab. Brain Dis. 2024, 39, 1015–1026. [Google Scholar] [CrossRef]
- Browne, R.W.; Jakimovski, D.; Ziliotto, N.; Kuhle, J.; Bernardi, F.; Weinstock-Guttman, B.; Zivadinov, R.; Ramanathan, M. High-density lipoprotein cholesterol is associated with multiple sclerosis fatigue: A fatigue-metabolism nexus? J. Clin. Lipidol. 2019, 13, 654–663.e1. [Google Scholar] [CrossRef]
- Ruiz-Argüelles, A.; Méndez-Huerta, M.A.; Lozano, C.D.; Ruiz-Argüelles, G.J. Metabolomic profile of insulin resistance in patients with multiple sclerosis is associated to the severity of the disease. Mult. Scler. Relat. Disord. 2018, 25, 316–321. [Google Scholar] [CrossRef]
- Penesova, A.; Vlcek, M.; Imrich, R.; Vernerova, L.; Marko, A.; Meskova, M.; Grunnerova, L.; Turcani, P.; Jezova, D.; Kollar, B. Hyperinsulinemia in newly diagnosed patients with multiple sclerosis. Metab. Brain Dis. 2015, 30, 895–901. [Google Scholar] [CrossRef]
- Ayromlou, H.; Hosseini, S.; Khalili, M.; Ayromlou, S.; Khamudchiyan, S.; Farajdokht, F.; Hassannezhad, S.; Moghadam, S.A. Insulin resistance is associated with cognitive dysfunction in multiple sclerosis patients: A cross-sectional study. J. Neuroendocrinol. 2023, 35, e13288. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Silveira, S.L.; Jeng, B.; Cutter, G.; Motl, R.W. Diet, Physical Activity, and Stress Among Wheelchair Users with Multiple Sclerosis: Examining Individual and Co-Occurring Behavioral Risk Factors. Arch. Phys. Med. Rehabil. 2023, 104, 590–596.e1. [Google Scholar] [CrossRef]
- Fitzgerald, K.; Tyry, T.; Salter, A.; Cofield, S.; Cutter, G.; Fox, R.; Marrie, R. Diet quality is associated with disability and symptom severity in multiple sclerosis. Neurology 2017, 90, e1–e11. [Google Scholar] [CrossRef] [PubMed]
- AJMC. Comorbidities Management and Lifestyle Modification in MS. Perspect. MS 2019, 10–14. [Google Scholar]
- Kappus, N.; Weinstock-Guttman, B.; Hagemeier, J.; Kennedy, C.; Melia, R.; Carl, E.; Ramasamy, D.P.; Cherneva, M.; Durfee, J.; Bergsland, N.; et al. Cardiovascular risk factors are associated with increased lesion burden and brain atrophy in multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2016, 87, 181–187. [Google Scholar]
- Giovannoni, G.; Butzkueven, H.; Dhib-Jalbut, S.; Hobart, J.; Kobelt, G.; Pepper, G.; Sormani, M.P.; Thalheim, C.; Traboulsee, A.; Vollmer, T. Brain health: Time matters in multiple sclerosis. Mult. Scler. Relat. Disord. 2016, 9 (Suppl. 1), S5–S48. [Google Scholar] [PubMed]
- Marck, C.H.; Neate, S.L.; Taylor, K.L.; Weiland, T.J.; Jelinek, G.A. Prevalence of Comorbidities, Overweight and Obesity in an International Sample of People with Multiple Sclerosis and Associations with Modifiable Lifestyle Factors. PLoS ONE 2016, 11, e0148573. [Google Scholar]
- Jakimovski, D.; Guan, Y.; Ramanathan, M.; Weinstock-Guttman, B.; Zivadinov, R. Lifestyle-based Modifiable Risk Factors in Multiple Sclerosis: Review of Experimental and Clinical Findings. Neurodegener. Dis. Manag. 2019, 9, 149–172. [Google Scholar]
- Lee, J.E.; Bisht, B.; Hall, M.J.; Rubenstein, L.M.; Louison, R.; Klein, D.T.; Wahls, T.L. A Multimodal, Nonpharmacologic Intervention Improves Mood and Cognitive Function in People with Multiple Sclerosis. J. Am. Coll. Nutr. 2017, 36, 150–168. [Google Scholar]
- Frassetto, L.A.; Schloetter, M.; Mietus-Synder, M.; Morris, R.C.; Sebastian, A. Metabolic and physiologic improvements from consuming a paleolithic, hunter-gatherer type diet. Eur. J. Clin. Nutr. 2009, 63, 947–955. [Google Scholar]
- Navarrete-Pérez, A.; Gómez-Melero, S.; Escribano, B.M.; Galvao-Carmona, A.; Conde-Gavilán, C.; Peña-Toledo, M.Á.; Villarrubia, N.; Villar, L.M.; Túnez, I.; Agüera-Morales, E.; et al. MIND Diet Impact on Multiple Sclerosis Patients: Biochemical Changes after Nutritional Intervention. Int. J. Mol. Sci. 2024, 25, 10009. [Google Scholar] [CrossRef]
- de la Rubia Ortí, J.E.; Armero, J.L.P.; Cuerda-Ballester, M.; Sanchis-Sanchis, C.E.; Navarro-Illana, E.; Lajara-Romance, J.M.; Benlloch, M.; Ceron, J.J.; Tvarijonaviciute, A.; Proaño, B. Lipid Profile in Multiple Sclerosis: Functional Capacity and Therapeutic Potential of Its Regulation after Intervention with Epigallocatechin Gallate and Coconut Oil. Foods 2023, 12, 3730. [Google Scholar] [CrossRef]
- Nieste, I.; Franssen, W.M.A.; Duvivier, B.M.F.M.; Spaas, J.; Savelberg, H.H.C.M.; Eijnde, B.O. Replacing sitting with light-intensity physical activity throughout the day versus 1 bout of vigorous-intensity exercise: Similar cardiometabolic health effects in multiple sclerosis. A randomised cross-over study. Disabil. Rehabil. 2023, 45, 3293–3302. [Google Scholar] [CrossRef] [PubMed]
- Glavinovic, T.; Thanassoulis, G.; de Graaf, J.; Couture, P.; Hegele, R.A.; Sniderman, A.D. Physiological Bases for the Superiority of Apolipoprotein B Over Low-Density Lipoprotein Cholesterol and Non–High-Density Lipoprotein Cholesterol as a Marker of Cardiovascular Risk. J. Am. Heart Assoc. 2022, 11, e025858. [Google Scholar] [CrossRef] [PubMed]
- Zhornitsky, S.; McKay, K.A.; Metz, L.M.; Teunissen, C.E.; Rangachari, M. Cholesterol and markers of cholesterol turnover in multiple sclerosis: Relationship with disease outcomes. Mult. Scler. Relat. Disord. 2016, 5, 53–65. [Google Scholar] [CrossRef]
- Browne, R.W.; Weinstock-Guttman, B.; Horakova, D.; Zivadinov, R.; Bodziak, M.L.; Tamaño-Blanco, M.; Badgett, D.; Tyblova, M.; Vaneckova, M.; Seidl, Z.; et al. Apolipoproteins are associated with new MRI lesions and deep grey matter atrophy in clinically isolated syndromes. J. Neurol. Neurosurg. Psychiatry 2014, 85, 859–864. [Google Scholar] [PubMed]
- Vassilopoulos, D.; Jockers-Wretou, E. Serum Creatine Kinase B Levels in Diseases of the Central Nervous System. Eur. Neurol. 2008, 27, 78–81. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).