
Association of Prenatal Healthy and Unhealthy Plant-Based Diets with Behavioral Outcomes in Preschool Children

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
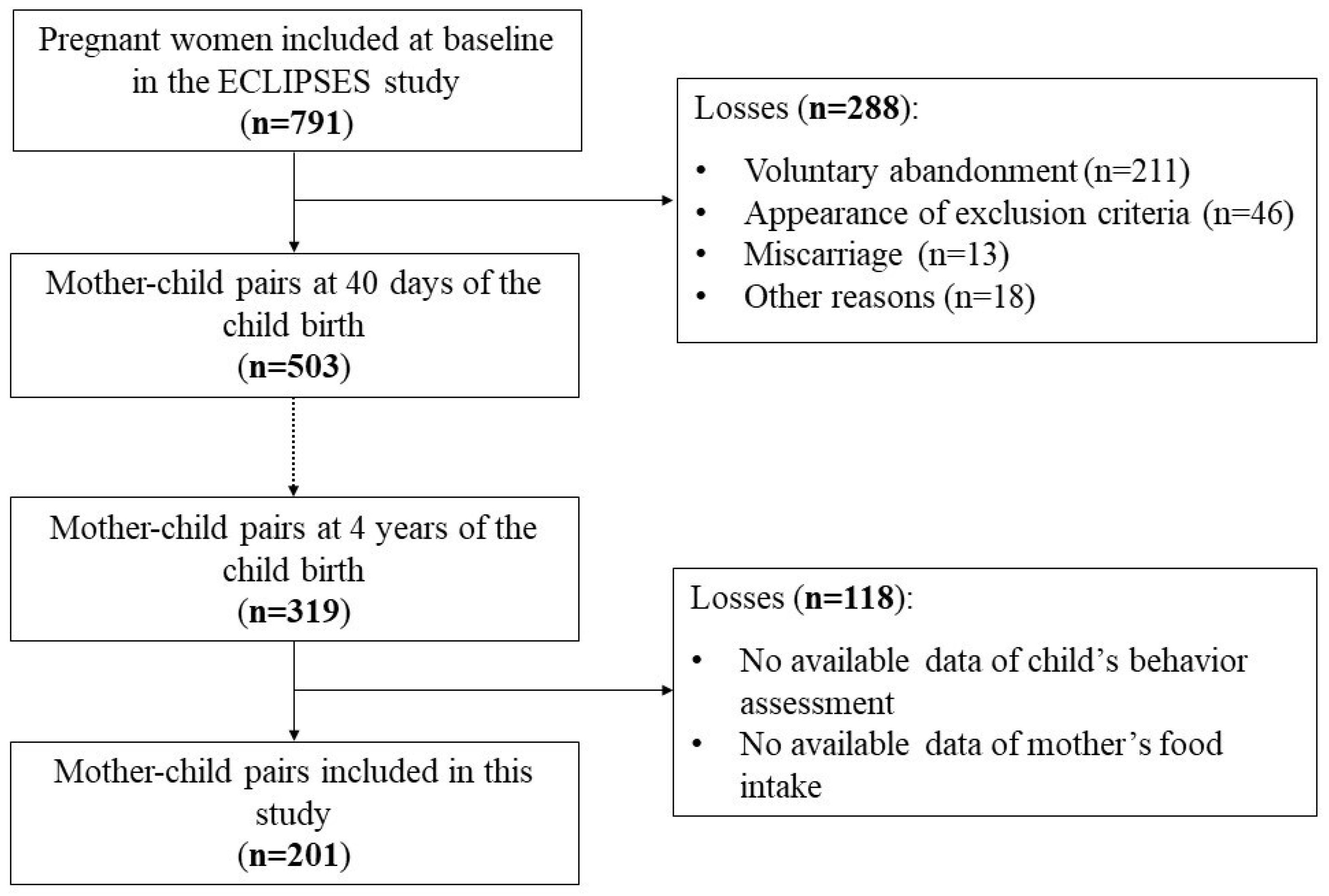
2.1. Study Population
2.2. Assessment of Dietary Intake and Plant-Based Diet Indices
2.3. Child Behavioral Problems
2.4. Assessment of Other Variables
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ADHD | Attention-Deficit/Hyperactivity Disorder |
| BMI | Body Mass Index |
| DSM | Diagnostic and Statistical Manual of Mental Disorders |
| CBCL 1.5-5 | Child Behavior Checklist 1.5-5 |
| FFQ | Food Frequency Questionnaire |
| hPDI | Healthy Plant-based Diet Index |
| uPDI | Unhealthy Plant-based Diet Index |
| ODD | Oppositional Defiant Disorder |
| OR | Odds Ratios |
| CI | Confidence Intervals |
References
- de Matos Reis, Á.E.; Teixeira, I.S.; Maia, J.M.; Luciano, L.A.A.; Brandião, L.M.; Silva, M.L.S.; Branco, L.G.S.; Soriano, R.N. Maternal Nutrition and Its Effects on Fetal Neurodevelopment. Nutrition 2024, 125, 112483. [Google Scholar] [CrossRef] [PubMed]
- Bordeleau, M.; Fernández de Cossío, L.; Chakravarty, M.M.; Tremblay, M.È. From Maternal Diet to Neurodevelopmental Disorders: A Story of Neuroinflammation. Front. Cell. Neurosci. 2021, 14, 612705. [Google Scholar] [CrossRef]
- ProVeg International; University of Copenhagen; Ghent University. Evolving Appetites: An In-Depth Look at European Attitudes Towards Plant-Based Eating. A Follow-Up to the 2021 Survey Report ‘What Consumers Want’; ProVeg International: Berlin, Germany, 2023. [Google Scholar]
- Yisahak, S.F.; Hinkle, S.N.; Mumford, S.L.; Li, M.; Andriessen, V.C.; Grantz, K.L.; Zhang, C.; Grewal, J. Vegetarian Diets during Pregnancy, and Maternal and Neonatal Outcomes. Int. J. Epidemiol. 2020, 50, 165. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Martínez-González, M.A.; Tong, T.Y.N.; Forouhi, N.G.; Khandelwal, S.; Prabhakaran, D.; Mozaffarian, D.; de Lorgeril, M. Definitions and Potential Health Benefits of the Mediterranean Diet: Views from Experts around the World. BMC Med. 2014, 12, 112. [Google Scholar] [CrossRef] [PubMed]
- Tuso, P.J.; Ismail, M.H.; Ha, B.P.; Bartolotto, C. Nutritional Update for Physicians: Plant-Based Diets. Perm. J. 2013, 17, 61. [Google Scholar] [CrossRef] [PubMed]
- Crovetto, F.; Nakaki, A.; Arranz, A.; Borras, R.; Vellvé, K.; Paules, C.; Boutet, M.L.; Castro-Barquero, S.; Freitas, T.; Casas, R.; et al. Effect of a Mediterranean Diet or Mindfulness-Based Stress Reduction During Pregnancy on Child Neurodevelopment: A Prespecified Analysis of the IMPACT BCN Randomized Clinical Trial. JAMA Netw. Open 2023, 6, e2330255. [Google Scholar] [CrossRef]
- Cendra-Duarte, E.; Canals, J.; Iglesias-Vázquez, L.; Jardí, C.; Martín-Luján, F.; Arija, V. Adherence to the Mediterranean Diet during Pregnancy and Behavioural Problems at 4 Years of Age. Matern. Child Nutr. 2024, 20, e13700. [Google Scholar] [CrossRef]
- Meulenbroeks, D.; Otten, E.; Smeets, S.; Groeneveld, L.; Jonkers, D.; Eussen, S.; Scheepers, H.; Gubbels, J. The Association of a Vegan Diet during Pregnancy with Maternal and Child Outcomes: A Systematic Review. Nutrients 2024, 16, 3329. [Google Scholar] [CrossRef]
- Avnon, T.; Paz Dubinsky, E.; Lavie, I.; Ben-Mayor Bashi, T.; Anbar, R.; Yogev, Y. The Impact of a Vegan Diet on Pregnancy Outcomes. J. Perinatol. 2021, 41, 1129–1133. [Google Scholar] [CrossRef]
- Crozier, S.R.; Godfrey, K.M.; Calder, P.C.; Robinson, S.M.; Inskip, H.M.; Baird, J.; Gale, C.R.; Cooper, C.; Sibbons, C.M.; Fisk, H.L.; et al. Vegetarian Diet during Pregnancy Is Not Associated with Poorer Cognitive Performance in Children at Age 6–7 Years. Nutrients 2019, 11, 3029. [Google Scholar] [CrossRef]
- Wang, T.; Masedunskas, A.; Willett, W.C.; Fontana, L. Vegetarian and Vegan Diets: Benefits and Drawbacks. Eur. Heart J. 2023, 44, 3423. [Google Scholar] [CrossRef] [PubMed]
- Gehring, J.; Touvier, M.; Baudry, J.; Julia, C.; Buscail, C.; Srour, B.; Hercberg, S.; Péneau, S.; Kesse-Guyot, E.; Allès, B. Consumption of Ultra-Processed Foods by Pesco-Vegetarians, Vegetarians, and Vegans: Associations with Duration and Age at Diet Initiation. J. Nutr. 2021, 151, 120–131. [Google Scholar] [CrossRef]
- Gastaldello, A.; Giampieri, F.; De Giuseppe, R.; Grosso, G.; Baroni, L.; Battino, M. The Rise of Processed Meat Alternatives: A Narrative Review of the Manufacturing, Composition, Nutritional Profile and Health Effects of Newer Sources of Protein, and Their Place in Healthier Diets. Trends Food Sci. Technol. 2022, 127, 263–271. [Google Scholar] [CrossRef]
- Peña-Jorquera, H.; Cid-Jofré, V.; Landaeta-Díaz, L.; Petermann-Rocha, F.; Martorell, M.; Zbinden-Foncea, H.; Ferrari, G.; Jorquera-Aguilera, C.; Cristi-Montero, C. Plant-Based Nutrition: Exploring Health Benefits for Atherosclerosis, Chronic Diseases, and Metabolic Syndrome—A Comprehensive Review. Nutrients 2023, 15, 3244. [Google Scholar] [CrossRef] [PubMed]
- Satija, A.; Bhupathiraju, S.N.; Rimm, E.B.; Spiegelman, D.; Chiuve, S.E.; Borgi, L.; Willett, W.C.; Manson, J.A.E.; Sun, Q.; Hu, F.B. Plant-Based Dietary Patterns and Incidence of Type 2 Diabetes in US Men and Women: Results from Three Prospective Cohort Studies. PLoS Med. 2016, 13, e1002039. [Google Scholar] [CrossRef]
- Arija, V.; Fargas, F.; March, G.; Abajo, S.; Basora, J.; Canals, J.; Ribot, B.; Aparicio, E.; Serrat, N.; Hernández-Martínez, C.; et al. Adapting Iron Dose Supplementation in Pregnancy for Greater Effectiveness on Mother and Child Health: Protocol of the ECLIPSES Randomized Clinical Trial. BMC Pregnancy Childbirth 2014, 14, 33. [Google Scholar] [CrossRef] [PubMed]
- Trinidad Rodríguez, I.; Fernández Ballart, J.; Cucó, G.; Biarnés Jordà, E.; Arija Val, V. Validación de Un Cuestionario de Frecuencia de Consumo Alimentario Corto: Reproducibilidad y Validez [Validation of a Short Questionnaire on Frequency of Dietary Intake: Reproducibility and Validity]. Nutr. Hosp. 2008, 23, 242–252. [Google Scholar]
- Arija, V.; Salas-Salvadó, J.; Fernández-Ballart, J.; Cuco, G.; Marti-Henneberg, C. Consumo, Hábitos Alimentarios y Estado Nutricional de La Población de Reus (IX). Evolución Del Consumo Alimentario, La Ingesta de Energía y Nutrientes y Su Relación Con El Nivel Socioeconómico y Cultural, 1983–1993. Med. Clin. 1996, 106, 174–179. [Google Scholar]
- Favier, J.C.; Ireland-Ripert, J.; Toque, C.; Feinberg, M. Répertoire Général des Aliments: Tables de Composition; Technique & Documentation; INRA: Paris, France, 1995. [Google Scholar]
- Mataix, J.; García-Diz, L.; Mañas, M.; Martinez de Vitoria, E.; Llopis, J. Tablas de Composición de Alimentos, 5th ed.; Editorial Universidad de Granada: Granada, Spain, 2009. [Google Scholar]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA Preschool Forms & Profiles; University of Vermont, Research Center for Children, Youth, & Families: Burlington, VT, USA, 2000. [Google Scholar]
- de la Osa, N.; Granero, R.; Trepat, E.; Domenech, J.M.; Ezpeleta, L. The Discriminative Capacity of CBCL/1½-5-DSM5 Scales to Identify Disruptive and Internalizing Disorders in Preschool Children. Eur. Child. Adolesc. Psychiatry 2016, 25, 17–23. [Google Scholar] [CrossRef]
- Generalitat de Catalunya Institut d’Estadística de Catalunya. Classificació Catalana d’Ocupacions 2011 (CCO-2011). Adaptació de la CNO-2011; Generalitat de Catalunya Institut d’Estadística de Catalunya: Barcelona, Spain, 2013. [Google Scholar]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerström, K.O. The Fagerström Test for Nicotine Dependence: A Revision of the Fagerström Tolerance Questionnaire. Br. J. Addict. 1991, 86, 1119–1127. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.E. STAI. Cuestionario de Ansiedad Estado-Rasgo. (Adaptación Española: Nicolás Seisdedos Cubero); TEA Ediciones: Madrid, Spain, 1994. [Google Scholar]
- Abidin, R.R. Parenting Stress Index (PSI) Manual, 3rd ed.; Pediatric Psychology Press: Charlottesville, VA, USA, 1995. [Google Scholar]
- Díaz-Herrero, A.; Brito de la Nuez, A.G.; López Pina, J.A.; Pérez-López, J.; Martínez-Fuentes, M.T. Factor Structure and Internal Consistency of the Spanish Version of the Parenting Stress Index-Short Form. Psicothema 2010, 22, 1033–1038. [Google Scholar] [PubMed]
- Norte Navarro, A.I.; Ortiz Moncada, R. Calidad de La Dieta Española Según El Índice de Alimentación Saludable. Nutr. Hosp. 2011, 26, 330–336. [Google Scholar] [CrossRef] [PubMed]
- Esteban-Figuerola, P.; Jardí, C.; Canals, J.; Arija, V. Validation of a Short Food Frequency Questionnaire in Small Children. Nutr. Hosp. 2020, 37, 101–113. [Google Scholar] [CrossRef]
- Montón, C.; Pérez Echeverría, M.J.; Campos, R.; García Campayo, J.; Lobo, A. Anxiety Scales and Goldberg’s Depression: An Efficient Interview Guide for the Detection of Psychologic Distress. Aten. Primaria 1993, 12, 345–349. [Google Scholar]
- Goldberg, D.; Bridges, K.; Duncan-Jones, P.; Grayson, D. Detecting Anxiety and Depression in General Medical Settings. BMJ Br. Med. J. 1988, 297, 897. [Google Scholar] [CrossRef]
- Willett, W. Nutritional Epidemiology; Oxford University Press: New York, NY, USA, 2012; ISBN 9780199979448. [Google Scholar]
- de Waal, T.; Pannekoek, J.; Scholtus, S. Handbook of Statistical Data Editing and Imputation; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar] [CrossRef]
- Xue, L.; Chen, X.; Sun, J.; Fan, M.; Qian, H.; Li, Y.; Wang, L. Maternal Dietary Carbohydrate and Pregnancy Outcomes: Quality over Quantity. Nutrients 2024, 16, 2269. [Google Scholar] [CrossRef]
- Witek, K.; Wydra, K.; Filip, M. A High-Sugar Diet Consumption, Metabolism and Health Impacts with a Focus on the Development of Substance Use Disorder: A Narrative Review. Nutrients 2022, 14, 2940. [Google Scholar] [CrossRef]
- Gao, R.; Liu, X.; Li, X.; Zhang, Y.; Wei, M.; Sun, P.; Zhang, J.; Cai, L. Association between Maternal Sugar-Sweetened Beverage Consumption and the Social-Emotional Development of Child before 1 Year Old: A Prospective Cohort Study. Front. Nutr. 2022, 9, 966271. [Google Scholar] [CrossRef]
- Kvalvik, L.G.; Klungsøyr, K.; Igland, J.; Caspersen, I.H.; Brantsæter, A.L.; Solberg, B.S.; Hartman, C.; Schweren, L.J.S.; Larsson, H.; Li, L.; et al. Association of Sweetened Carbonated Beverage Consumption during Pregnancy and ADHD Symptoms in the Offspring: A Study from the Norwegian Mother, Father and Child Cohort Study (MoBa). Eur. J. Nutr. 2022, 61, 2153. [Google Scholar] [CrossRef]
- Cendra-Duarte, E.; Canals, J.; Becerra-Tomás, N.; Jardí, C.; Martín-Luján, F.; Arija, V. Maternal Dietary Patterns and Offspring Behavioral Problems. Pediatr. Res. 2024. ahead of print. [Google Scholar] [CrossRef]
- Choi, C.S.; Kim, P.; Park, J.H.; Gonzales, E.L.T.; Kim, K.C.; Cho, K.S.; Ko, M.J.; Yang, S.M.; Seung, H.; Han, S.H.; et al. High Sucrose Consumption during Pregnancy Induced ADHD-like Behavioral Phenotypes in Mice Offspring. J. Nutr. Biochem. 2015, 26, 1520–1526. [Google Scholar] [CrossRef]
- Faleschini, S.; Doyon, M.; Arguin, M.; Lepage, J.F.; Tiemeier, H.; Van Lieshout, R.J.; Perron, P.; Bouchard, L.; Hivert, M.F. Maternal Hyperglycemia in Pregnancy and Offspring Internalizing and Externalizing Behaviors. Matern. Child Health J. 2023, 27, 1765–1773. [Google Scholar] [CrossRef] [PubMed]
- Daraki, V.; Roumeliotaki, T.; Koutra, K.; Georgiou, V.; Kampouri, M.; Kyriklaki, A.; Vafeiadi, M.; Papavasiliou, S.; Kogevinas, M.; Chatzi, L. Effect of Parental Obesity and Gestational Diabetes on Child Neuropsychological and Behavioral Development at 4 Years of Age: The Rhea Mother-Child Cohort, Crete, Greece. Eur. Child. Adolesc. Psychiatry 2017, 26, 703–714. [Google Scholar] [CrossRef]
- Rodolaki, K.; Pergialiotis, V.; Iakovidou, N.; Boutsikou, T.; Iliodromiti, Z.; Kanaka-Gantenbein, C. The Impact of Maternal Diabetes on the Future Health and Neurodevelopment of the Offspring: A Review of the Evidence. Front. Endocrinol. 2023, 14, 1125628. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Ochoa, E.; Hernández-Ortega, K.; Ferrera, P.; Morimoto, S.; Arias, C. Short-Term High-Fat-and-Fructose Feeding Produces Insulin Signaling Alterations Accompanied by Neurite and Synaptic Reduction and Astroglial Activation in the Rat Hippocampus. J. Cereb. Blood Flow Metab. 2014, 34, 1001–1008. [Google Scholar] [CrossRef]
- Piazza, F.V.; Segabinazi, E.; de Meireles, A.L.F.; Mega, F.; Spindler, C.d.F.; Augustin, O.A.; Salvalaggio, G.d.S.; Achaval, M.; Kruse, M.S.; Coirini, H.; et al. Severe Uncontrolled Maternal Hyperglycemia Induces Microsomia and Neurodevelopment Delay Accompanied by Apoptosis, Cellular Survival, and Neuroinflammatory Deregulation in Rat Offspring Hippocampus. Cell Mol. Neurobiol. 2019, 39, 401–414. [Google Scholar] [CrossRef]
- Goran, M.I.; Plows, J.F.; Ventura, E.E. Effects of Consuming Sugars and Alternative Sweeteners during Pregnancy on Maternal and Child Health: Evidence for a Secondhand Sugar Effect. Proc. Nutr. Soc. 2019, 78, 262–271. [Google Scholar] [CrossRef] [PubMed]
- Vickers, M.H.; Clayton, Z.E.; Yap, C.; Sloboda, D.M. Maternal Fructose Intake during Pregnancy and Lactation Alters Placental Growth and Leads to Sex-Specific Changes in Fetal and Neonatal Endocrine Function. Endocrinology 2011, 152, 1378–1387. [Google Scholar] [CrossRef]
- Tobiansky, D.J.; Kachkovski, G.V.; Enos, R.T.; Schmidt, K.L.; Murphy, E.A.; Floresco, S.B.; Soma, K.K. Maternal Sucrose Consumption Alters Behaviour and Steroids in Adult Rat Offspring. J. Endocrinol. 2021, 251, 161–180. [Google Scholar] [CrossRef]
- Mukai, Y.; Ozaki, H.; Serita, Y.; Sato, S. Maternal Fructose Intake during Pregnancy Modulates Hepatic and Hypothalamic AMP-Activated Protein Kinase Signalling in a Sex-Specific Manner in Offspring. Clin. Exp. Pharmacol. Physiol. 2014, 41, 331–337. [Google Scholar] [CrossRef]
- Dearden, L.; Balthasar, N. Sexual Dimorphism in Offspring Glucose-Sensitive Hypothalamic Gene Expression and Physiological Responses to Maternal High-Fat Diet Feeding. Endocrinology 2014, 155, 2144. [Google Scholar] [CrossRef] [PubMed]
- Samuelsson, A.M.; Matthews, P.A.; Jansen, E.; Taylor, P.D.; Poston, L. Sucrose Feeding in Mouse Pregnancy Leads to Hypertension, and Sex-Linked Obesity and Insulin Resistance in Female Offspring. Front. Physiol. 2013, 4, 14. [Google Scholar] [CrossRef] [PubMed]
- Solberg, B.S.; Kvalvik, L.G.; Instanes, J.T.; Hartman, C.A.; Klungsøyr, K.; Li, L.; Larsson, H.; Magnus, P.; Njølstad, P.R.; Johansson, S.; et al. Maternal Fiber Intake During Pregnancy and Development of Attention-Deficit/Hyperactivity Disorder Symptoms Across Childhood: The Norwegian Mother, Father, and Child Cohort Study. Biol. Psychiatry 2024, 95, 839–848. [Google Scholar] [CrossRef]
- Jessen, H.M.; Auger, A.P. Sex Differences in Epigenetic Mechanisms May Underlie Risk and Resilience for Mental Health Disorders. Epigenetics 2011, 6, 857–861. [Google Scholar] [CrossRef] [PubMed]
- Czamara, D.; Dieckmann, L.; Lahti-Pulkkinen, M.; Cruceanu, C.; Henrich, W.; Plagemann, A.; Räikkönen, K.; Braun, T.; Binder, E.B.; Lahti, J.; et al. Sex Differences in DNA Methylation across Gestation: A Large Scale, Cross-Cohort, Multi-Tissue Analysis. Cell. Mol. Life Sci. 2024, 81, 1–16. [Google Scholar] [CrossRef]
- Pistollato, F.; Cano, S.S.; Elio, I.; Vergara, M.M.; Giampieri, F.; Battino, M. Plant-Based and Plant-Rich Diet Patterns during Gestation: Beneficial Effects and Possible Shortcomings. Adv. Nutr. 2015, 6, 581. [Google Scholar] [CrossRef]
- Miedziaszczyk, M.; Ciabach, P.; Grześkowiak, E.; Szałek, E. The Safety of a Vegan Diet during Pregnancy. Postepy Hig. Med. Dosw. 2021, 75, 91–100. [Google Scholar] [CrossRef]
- Sebastiani, G.; Barbero, A.H.; Borrás-Novel, C.; Casanova, M.A.; Aldecoa-Bilbao, V.; Andreu-Fernández, V.; Tutusaus, M.P.; Martínez, S.F.; Roig, M.D.G.; García-Algar, O. The Effects of Vegetarian and Vegan Diet during Pregnancy on the Health of Mothers and Offspring. Nutrients 2019, 11, 557. [Google Scholar] [CrossRef]
- Melina, V.; Craig, W.; Levin, S. Position of the Academy of Nutrition and Dietetics: Vegetarian Diets. J. Acad. Nutr. Diet. 2016, 116, 1970–1980. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Food Groups | Foods Included | Scoring Criteria | |
|---|---|---|---|
| Healthy Plant Foods | hPDI | uPDI | |
| Fruits | Fresh and preserved fruits | Q1 = 1 Q2 = 2 Q3 = 3 Q4 = 4 Q5 = 5 | Q1 = 5 Q2 = 4 Q3 = 3 Q4 = 2 Q5 = 1 |
| Vegetables | Lettuce, tomato, green beans, chard, spinach, eggplant, mushrooms, etc. | ||
| Nuts | All types of nuts | ||
| Legumes | Lentils, chickpeas, beans, etc. | ||
| Unhealthy Plant Foods | |||
| Juices | All types of fruit juices | Q1 = 5 Q2 = 4 Q3 = 3 Q4 = 2 Q5 = 1 | Q1 = 1 Q2 = 2 Q3 = 3 Q4 = 4 Q5 = 5 |
| Refined grains | Breakfast cereals, rice, pasta, bread, muffins, biscuit. | ||
| Potatoes | Baked, fried or boiled potatoes and chips. | ||
| Sugar-sweetened beverages | All types of sugar-sweetened beverages | ||
| Sweets and desserts | Chocolate, chocolate bars, candies, cookies, doughnuts, croissants, cakes. | ||
| Animal Foods | |||
| Dairy products | Milk, yogurt, all types of cheese, custard, flan, ice cream. | Q1 = 5 Q2 = 4 Q3 = 3 Q4 = 2 Q5 = 1 | Q1 = 5 Q2 = 4 Q3 = 3 Q4 = 2 Q5 = 1 |
| Eggs | Eggs | ||
| Fish and seafood | White fish (hake, grouper, sole, cod, etc.), oily fish (sardines, tuna, salmon, etc.) and other seafood (mussels, shrimp, prawns, squid, etc.) | ||
| Meat | Chicken, turkey, beef, pork, lamb, minced beef, ham, sausage, hamburger. | ||
| Other animal-based foods | Soup, croquettes, pizza. | ||
| Sample size, n = 201 | ||
| Maternal Characteristics | ||
| Age (years) | 31.8 ± 4.4 | |
| First trimester BMI (kg/m2) | 25.0 ± 4.6 | |
| Socioeconomic status | ||
| Low-middle | 151 (75.1) | |
| High | 50 (24.9) | |
| Smoke during gestation (yes) | 33 (16.4) | |
| Alcohol during gestation (yes) | 3 (1.5) | |
| Physical activity during gestation (METs/min/week) | 2204.6 ± 2472.8 | |
| Energy intake during gestation (kcal/day) | 1747.5 ± 294.2 | |
| Anxiety during gestation (score) | 14.0 ± 8.1 | |
| Anxiety and depression at 4-year visit (yes) | 126 (62.7) | |
| hPDI (score) | 42.0 ± 4.6 | |
| Low adherence | 59 (29.4) | |
| Middle adherence | 81 (40.3) | |
| High adherence | 61 (30.3) | |
| uPDI (score) | 42.0 ± 6.4 | |
| Low adherence | 68 (33.8) | |
| Middle adherence | 60 (29.9) | |
| High adherence | 73 (36.3) | |
| Children Characteristics | ||
| Age (years) | 4.3 ± 0.3 | |
| Sex (girl) | 102 (50.7) | |
| Birth weight (grams) | 3308.2 ± 434.9 | |
| Gestational age (weeks) | 39.5 ± 1.6 | |
| Breastfeeding duration (months) | 11.0 ± 12.5 | |
| Maternal and child attachment (score) | 51.8 ± 5.3 | |
| Diet quality (score) | 61.5 ± 10.7 | |
| Behavioral Assessment (CBCL 1.5-5) (score) | ||
| Girls (n = 102) | Boys (n = 99) | |
| Emotionally reactive | 56.7 ± 8.3 | 58.0 ± 9.6 |
| Anxious/depressed | 56.0 ± 7.6 | 56.3 ± 7.4 |
| Somatic complaints | 55.7 ± 6.9 | 55.2 ± 6.9 |
| Withdrawn | 56.9 ± 6.7 | 59.4 ± 8.6 |
| Attention problems | 55.7 ± 6.6 | 60.0 ± 7.2 |
| Aggressive behavior | 53.9 ± 5.6 | 57.3 ± 8.6 |
| Internalizing problems | 54.2 ± 12.0 | 55.9 ± 12.0 |
| Externalizing problems | 50.9 ± 9.6 | 56.4 ± 11.8 |
| Total problems | 52.8 ± 11.3 | 56.8 ± 12.9 |
| Depressive problems | 55.8 ± 6.3 | 57.6 ± 8.2 |
| Anxiety problems | 57.7 ± 8.3 | 57.3 ± 8.3 |
| Autism spectrum problems | 56.5 ± 6.6 | 58.8 ± 8.2 |
| Attention deficit/hyperactivity problems | 55.7 ± 7.0 | 59.1 ± 8.3 |
| Oppositional defiant problems | 53.8 ± 5.7 | 56.1 ± 7.7 |
| Girls (n = 102) | Boys (n = 99) | |||||||
|---|---|---|---|---|---|---|---|---|
| hPDI | uPDI | hPDI | uPDI | |||||
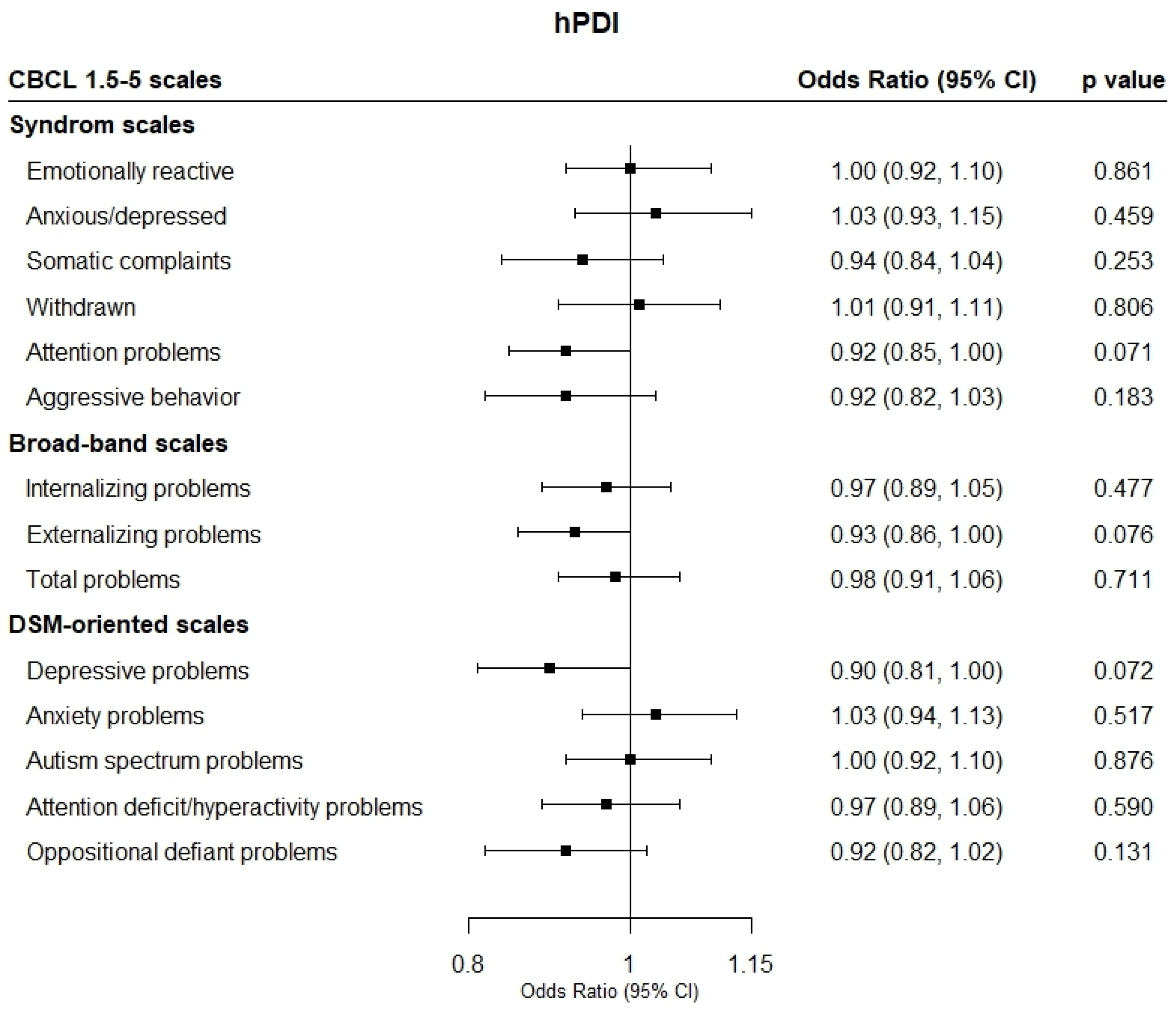
| CBCL 1.5-5 Scales | OR (95% CI) | p Value | OR (95% CI) | p Value | OR (95% CI) | p Value | OR (95% CI) | p Value |
| Syndrome Scales | ||||||||
| Emotionally reactive | 0.98 (0.84, 1.15) | 0.879 | 1.03 (0.92, 1.15) | 0.537 | 1.03 (0.91, 1.17) | 0.589 | 0.98 (0.88, 1.09) | 0.750 |
| Anxious/depressed | 1.04 (0.89, 1.22) | 0.577 | 1.02 (0.92, 1.14) | 0.641 | 1.05 (0.90, 1.23) | 0.464 | 0.91 (0.81, 1.03) | 0.160 |
| Somatic complaints | 0.99 (0.83, 1.18) | 0.956 | 1.10 (0.96, 1.26) | 0.141 | 0.91 (0.76, 1.09) | 0.335 | 0.97 (0.85, 1.10) | 0.640 |
| Withdrawn | 1.04 (0.79, 1.37) | 0.756 | 1.16 (0.95, 1.43) | 0.134 | 0.99 (0.86, 1.13) | 0.909 | 0.98 (0.89, 1.09) | 0.814 |
| Attention problems | 0.86 (0.72, 1.03) | 0.113 | 1.06 (0.95, 1.18) | 0.263 | 0.91 (0.82, 1.03) | 0.146 | 1.04 (0.95, 1.14) | 0.358 |
| Aggressive behavior | NE | NE | NE | NE | 0.92 (0.79, 1.07) | 0.322 | 1.07 (0.94, 1.22) | 0.290 |
| Broad-band Scales | ||||||||
| Internalizing problems | 0.96 (0.84, 1.10) | 0.632 | 1.02 (0.93, 1.11) | 0.667 | 1.01 (0.90, 1.13) | 0.820 | 1.02 (0.93, 1.12) | 0.549 |
| Externalizing problems | 0.88 (0.76, 1.02) | 0.104 | 1.18 (1.04, 1.33) | 0.006 * | 0.96 (0.86, 1.07) | 0.483 | 1.04 (0.96, 1.14) | 0.303 |
| Total problems | 0.96 (0.85, 1.09) | 0.582 | 1.07 (0.97, 1.17) | 0.136 | 1.00 (0.90, 1.12) | 0.917 | 0.99 (0.90, 1.08) | 0.875 |
| DSM-Oriented Scales | ||||||||
| Depressive problems | 0.80 (0.60, 1.06) | 0.127 | 1.51 (0.98, 2.33) | 0.060 | 0.91 (0.79, 1.05) | 0.242 | 1.01 (0.91, 1.12) | 0.761 |
| Anxiety problems | 0.99 (0.87, 1.13) | 0.941 | 0.99 (0.91, 1.09) | 0.959 | 1.17 (0.99, 1.39) | 0.062 | 0.82 (0.72, 0.94) | 0.007 * |
| Autism spectrum problems | 0.96 (0.82, 1.12) | 0.629 | 1.05 (0.95, 1.17) | 0.304 | 1.04 (0.90, 1.19) | 0.570 | 1.00 (0.89, 1.12) | 0.981 |
| Attention deficit/hyperactivity problems | 0.99 (0.84, 1.16) | 0.930 | 1.20 (1.02, 1.40) | 0.022 * | 0.96 (0.85, 1.08) | 0.567 | 1.05 (0.95, 1.17) | 0.268 |
| Oppositional defiant problems | 0.82 (0.63, 1.05) | 0.128 | 1.24 (0.98, 1.56) | 0.062 | 0.95 (0.82, 1.10) | 0.507 | 1.06 (0.95, 1.19) | 0.265 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cendra-Duarte, E.; Becerra-Tomás, N.; Canals, J.; Jardí, C.; Arija, V. Association of Prenatal Healthy and Unhealthy Plant-Based Diets with Behavioral Outcomes in Preschool Children. Nutrients 2025, 17, 1372. https://doi.org/10.3390/nu17081372
Cendra-Duarte E, Becerra-Tomás N, Canals J, Jardí C, Arija V. Association of Prenatal Healthy and Unhealthy Plant-Based Diets with Behavioral Outcomes in Preschool Children. Nutrients. 2025; 17(8):1372. https://doi.org/10.3390/nu17081372
Chicago/Turabian StyleCendra-Duarte, Esther, Nerea Becerra-Tomás, Josefa Canals, Cristina Jardí, and Victoria Arija. 2025. "Association of Prenatal Healthy and Unhealthy Plant-Based Diets with Behavioral Outcomes in Preschool Children" Nutrients 17, no. 8: 1372. https://doi.org/10.3390/nu17081372
APA StyleCendra-Duarte, E., Becerra-Tomás, N., Canals, J., Jardí, C., & Arija, V. (2025). Association of Prenatal Healthy and Unhealthy Plant-Based Diets with Behavioral Outcomes in Preschool Children. Nutrients, 17(8), 1372. https://doi.org/10.3390/nu17081372