
Dietary Patterns and Brain Health in Middle-Aged and Older Adults: A Narrative Review

 ,
, 
 ,
, Highlights
- This narrative review synthesizes findings from 18 studies (2013–2023) assessing the impact of dietary patterns—such as the Mediterranean (MedDiet), DASH, MIND, and Western diets—on brain health in middle-aged and older adults.
- The MedDiet demonstrated the most consistent cognitive benefits, including improved memory and processing speed, and likely has the potential for delaying cognitive aging by up to 3.5 years.
- Practical and cost-effective strategies to support brain health include increasing omega-3 intake from canned fish and seeds, consuming more fruits, vegetables, and whole grains, and reducing ultra-processed foods and refined grains.
- This review contributes to the ABCDS brain health framework by focusing on “D” for Diet—highlighting nutrition as a modifiable lifestyle factor that directly and indirectly supports brain, cardiovascular, and mental health.
- The review emphasizes culturally sensitive, equitable, and scalable approaches—adapting dietary guidance to local food preferences, leveraging technology for personalized nutrition, and integrating strategies into national health policies.
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
- Population: Humans (adults, older adults);
- Intervention/Exposure: Diet;
- Comparator and Outcomes: Dementia/cognitive impairment, brain/mental/social health;
- Study Design: Observational and experimental studies, systematic reviews, and meta-analyses.
2.2. Conceptual Framework
3. Results
3.1. The Role of Nutrition in Brain Function
3.2. Dietary Patterns and Brain Health
3.2.1. Mediterranean Diet
3.2.2. DASH Diet
3.2.3. MIND Diet
3.2.4. Western Diet
4. Discussion
5. Implications for Practice and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ABCDS | Activity, Blood Pressure Control, Connecting, Diet, Sleep |
| MedDiet | Mediterranean Diet |
| DASH | Dietary Approaches to Stop Hypertension |
| MIND | Mediterranean-DASH Intervention for Neurodegenerative Delay |
Appendix A
| Full PubMed Search Strategy Organized by PICOS Framework |
| P—Population |
| (“Persons”[Mesh] OR “Humans”[Mesh] OR human*[tw] OR people*[tw] OR patient*[tw] OR out-patient*[tw] OR child*[tw] OR adult*[tw] OR aged[tw] OR elderl*[tw] OR age group*[tw] OR individual*[tw] OR adolescent*[tw] OR men[tw] OR women[tw] OR boy[tw] OR boys[tw] OR girl*[tw] OR super-ager*[tw] OR “Aged, 80 and over”[Mesh] OR “Centenarians”[Mesh] OR “Nonagenarians”[Mesh] OR “Octogenarians”[Mesh] OR octogenarian*[tw] OR nonagenarian*[tw] OR semisupercentenarian*[tw] OR semi-supercentenarian*[tw] OR supercentenarian*[tw] OR super-centenarian*[tw] OR oldest old[tw]) |
| I—Intervention/Exposure (Diet) |
| (“Diet, Healthy”[Mesh] OR healthy diet*[tw] OR healthy eating[tw] OR eating health[tw] OR healthy nutrition[tw] OR prudent diet*[tw] OR “Diet Therapy”[Mesh] OR diet therap*[tw] OR dietary modification*[tw] OR restrictive diet[tw] OR restriction diet therapy[tw] OR restrictive diet therapy[tw] OR dietary restriction*[tw] OR “Dietary Approaches To Stop Hypertension”[Mesh] OR hypertension diet*[tw] OR DASH diet*[tw] OR mediterranean[tw] OR MIND[tw] OR nordic[tw]) |
| C—Comparator (Implicit/General Health Comparisons) |
| Comparator terms were not explicitly defined in this search due to variability in dietary exposures and health outcomes across studies. Studies with various comparator groups (e.g., low vs. high adherence, different diet types) were included. |
| O—Outcomes (Brain, Mental, Cognitive, Social Health) |
| (brain health[tw] OR brain wellbeing[tw] OR brain well-being[tw] OR healthy brain[tw] OR “Healthy Aging”[Mesh] OR healthy aging[tw] OR healthy ageing[tw] OR aging well[tw] OR ageing well[tw] OR well aging[tw] OR well ageing[tw] OR cognitive health[tw] OR healthy cognition[tw] OR mindfulness[tw] OR relaxation[tw] OR peace-of-mind[tw] OR mental health[tw] OR social health[tw] OR mental wellbeing[tw] OR social wellbeing[tw] OR emotional wellbeing[tw] OR mental well-being[tw] OR social well-being[tw] OR emotional well-being[tw] OR mental abuse[tw] OR functional disorder*[tw] OR physical abuse[tw]) |
| OR |
| (“Dementia”[Mesh] OR dementia*[tw] OR amentia*[tw] OR Alzheimer syndrome[tw] OR Alzheimer-Type Dementia[tw] OR Alzheimer’s disease*[tw] OR Alzheimers disease*[tw] OR Alzheimer dementia*[tw] OR senile dementia[tw] OR senile degenerative dementia[tw] OR Alzheimer sclerosis[tw] OR presenile dementia[tw] OR binswanger disease[tw] OR progressive subcortical encephalopathy[tw] OR binswanger encephalopathy[tw] OR leukoaraiosis[tw] OR subcortical leukoencephalopathy*[tw] OR leukoencephalopathies*[tw] OR binswanger’s encephalopathy[tw] OR binswanger’s disease[tw] OR subcortical vascular dementia[tw] OR progressive aphasia*[tw] OR mesulam’s syndrome[tw] OR “Cognitive Dysfunction”[Majr] OR cognitive dysfunction*[tw] OR cognitive disorder*[tw] OR cognitive impairment*[tw] OR cognitive decline*[tw] OR mental deterioration*[tw]) |
| AND |
| (“Stroke”[Mesh] OR stroke*[tw] OR cerebrovascular accident*[tw] OR cerebrovascular event*[tw] OR brain attack*[tw] OR cerebrovascular apoplexy[tw] OR brain vascular accident*[tw] OR “CVA”[tw] OR “CVAs”[tw] OR brain infarct*[tw] OR brain venous infarction*[tw] OR venous brain infarction*[tw] OR cerebral circulation infarct*[tw] OR brain circulation infarct*[tw] OR cerebral infarct*[tw] OR choroidal artery infarct*[tw] OR subcortical infarct*[tw] OR multi-infarct dementia*[tw] OR multiinfarct dementia*[tw] OR dementia multi-infarct*[tw] OR lacunar dementia*[tw] OR subarachnoid hemorrhagic[tw] OR brain failure*[tw] OR “Myocardial Ischemia”[Mesh] OR ischemic heart disease*[tw] OR ischaemic heart disease*[tw] OR myocardial ischemia*[tw] OR myocardial ischaemia*[tw] OR coronary heart disease*[tw] OR coronary thrombosis[tw] OR coronary artery disease*[tw] OR coronary atheroscleros*[tw] OR coronary disease*[tw] OR myocardial infarct*[tw] OR heart attack*[tw] OR cardiovascular stroke*[tw] OR “Heart Failure”[Mesh] OR myocardial failure[tw] OR cardiac failure[tw] OR heart decompensation[tw] OR heart failure[tw] OR “Atrial Fibrillation”[Mesh] OR atrial fibrillation*[tw] OR auricular fibrillation*[tw]) |
| S—Study Design |
| (“Follow-Up Studies”[Mesh] OR follow up stud*[tw] OR followup stud*[tw] OR “Longitudinal Studies”[Mesh] OR longitudinal stud*[tw] OR “Cross-Sectional Studies”[Mesh] OR Cross Sectional Studi*[tw] OR birth cohort*[tw] OR Framingham Heart Stud*[tw] OR Jackson Heart Stud*[tw] OR California Teachers Stud*[tw] OR Bogalusa Heart Stud*[tw] OR Longitudinal Survey*[tw] OR add health study[tw] OR “Prospective Studies”[Mesh] OR “Randomized Controlled Trial”[Publication Type] OR randomized controlled trial*[tw] OR randomised controlled trial*[tw] OR RCT[tw] OR RCTs[tw] OR “Community Health Planning”[mh] OR population based[tw] OR community based[tw] OR community health[tw] OR community dwelling*[tw] OR “Home Care Services, Hospital-Based”[mh] OR hospital based[tw] OR hospital-based[tw] OR clinic based[tw] OR clinic-based[tw] |
| OR |
| (meta-analysis[pt] OR meta-analy*[tw] OR metaanaly*[tw] OR meta-synthesis[tw] OR metasynthesis[tw] OR meta-study[tw] OR metastudy[tw] OR metaethnograph*[tw] OR meta-ethnograph*[tw] OR sensitivity analys*[tw] OR systematic review[pt] OR systematic review[tw] OR systematic literature[tw] OR integrative review[tw] OR integrative literature[tw] OR evidence-based review[tw] OR evidence-based overview[tw] OR evidence-based literature[tw] OR evidence-based survey[tw] OR literature search[tw]) |
| OR |
| ((systemat*[ti] OR evidence-based[ti]) AND (review*[ti] OR literature[ti] OR overview[ti] OR survey[ti])) |
| OR |
| data synthesis[tw] OR evidence synthesis[tw] OR data extraction[tw] OR data source[tw] OR data sources[tw] OR study selection[tw] OR methodological quality[tw] OR methodologic quality[tw] OR cochrane database syst rev[ta] OR umbrella review[pt] OR “Comparative Effectiveness Research”[mh] |
| OR |
| (“Life Change Events”[Mesh] OR life change event*[tw] OR life crisis[tw] OR life course*[tw] OR life experience*[tw])) |
References
- Hachinski, V. Brain Health-Curbing Stroke, Heart Disease, and Dementia: The 2020 Wartenberg Lecture. Neurology 2021, 97, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Avan, A.; Hachinski, V. Brain Health Learn and Act Group. Brain health: Key to health, productivity, and well-being. Alzheimer’s Dement. 2022, 18, 1396–1407. [Google Scholar] [CrossRef]
- Bassetti, C.L.A.; Endres, M.; Sander, A.; Crean, M.; Subramaniam, S.; Carvalho, V.; Di Liberto, G.; Franco, O.H.; Pijnenburg, Y.; Leonardi, M.; et al. The European Academy of Neurology Brain Health Strategy: One brain, one life, one approach. Eur. J. Neurol. 2022, 29, 2559–2566. [Google Scholar] [CrossRef]
- Gorelick, P.B.; Sorond, F.A. What is brain health? Cereb. Circ. Cogn. Behav. 2023, 6, 100190. [Google Scholar] [CrossRef]
- Hachinski, V. Brain health: The time has come. Eur. J. Neurol. 2022, 29, 2553–2554. [Google Scholar] [CrossRef] [PubMed]
- Owolabi, M.O. Improving brain and vascular health at the population level: Lessons from the Norwegian success story. Eur. J. Neurol. 2023, 30, 2141–2143. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Demnitz, N.; Yamamoto, S.; Yaffe, K.; Lawlor, B.; Leroi, I. Defining brain health: A concept analysis. Int. J. Geriatr. Psychiatry 2021, 37. [Google Scholar] [CrossRef]
- Avan, A.; Hachinski, V. Stroke and dementia, leading causes of neurological disability and death, potential for prevention. Alzheimer’s Dement. 2021, 17, 1072–1076. [Google Scholar] [CrossRef]
- Hendriks, S.; Ranson, J.M.; Peetoom, K.; Lourida, I.; Tai, X.Y.; de Vugt, M.; Llewellyn, D.J.; Köhler, S. Risk Factors for Young-Onset Dementia in the UK Biobank. JAMA Neurol. 2024, 81, 134–142. [Google Scholar] [CrossRef]
- Kuźma, E.; Lourida, I.; Moore, S.F.; Levine, D.A.; Ukoumunne, O.C.; Llewellyn, D.J. Stroke and dementia risk: A systematic review and meta-analysis. Alzheimer’s Dement. 2018, 14, 1416–1426. [Google Scholar] [CrossRef]
- Francis, H.M.; Stevenson, R.J. Potential for diet to prevent and remediate cognitive deficits in neurological disorders. Nutr. Rev. 2018, 76, 204–217. [Google Scholar] [CrossRef]
- Gauci, S.; Young, L.M.; Arnoldy, L.; Lassemillante, A.C.; Scholey, A.; Pipingas, A. Dietary patterns in middle age: Effects on concurrent neurocognition and risk of age-related cognitive decline. Nutr. Rev. 2022, 80, 1129–1159. [Google Scholar] [CrossRef] [PubMed]
- Marchand, N.E.; Jensen, M.K. The Role of Dietary and Lifestyle Factors in Maintaining Cognitive Health. Am. J. Lifestyle Med. 2017, 12, 268–285. [Google Scholar] [CrossRef]
- Solfrizzi, V.; Custodero, C.; Lozupone, M.; Imbimbo, B.P.; Valiani, V.; Agosti, P.; Schilardi, A.; D’Introno, A.; La Montagna, M.; Calvani, M.; et al. Relationships of Dietary Patterns, Foods, and Micro- and Macronutrients with Alzheimer’s Disease and Late-Life Cognitive Disorders: A Systematic Review. J. Alzheimer’s Dis. 2017, 59, 815–849. [Google Scholar] [CrossRef] [PubMed]
- Allès, B.; Samieri, C.; Féart, C.; Jutand, M.A.; Laurin, D.; Barberger-Gateau, P. Dietary patterns: A novel approach to examine the link between nutrition and cognitive function in older individuals. Nutr. Res. Rev. 2012, 25, 207–222. [Google Scholar] [CrossRef]
- Chen, X.; Liu, Z.; Sachdev, P.S.; Kochan, N.A.; O’Leary, F.; Brodaty, H. Dietary Patterns and Cognitive Health in Older Adults: Findings from the Sydney Memory and Ageing Study. J. Nutr. Health Aging 2021, 25, 255–262. [Google Scholar] [CrossRef]
- Corley, J.; Cox, S.R.; Taylor, A.M.; Hernandez, M.V.; Maniega, S.M.; Ballerini, L.; Wiseman, S.; Meijboom, R.; Backhouse, E.V.; Bastin, M.E.; et al. Dietary patterns, cognitive function, and structural neuroimaging measures of brain aging. Exp. Gerontol. 2020, 142, 111117. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Barbagallo, M.; Muñoz-Garcia, M.; Godos, J.; Martinez-Gonzalez, M.A. Dietary Patterns and Cognitive Decline: Key features for prevention. Curr. Pharm. Des. 2019, 25, 2428–2442. [Google Scholar] [CrossRef] [PubMed]
- Gardener, S.L.; Rainey-Smith, S.R.; Barnes, M.B.; Sohrabi, H.R.; Weinborn, M.; Lim, Y.Y.; Harrington, K.; Taddei, K.; Gu, Y.; Rembach, A.; et al. Dietary patterns and cognitive decline in an Australian study of ageing. Mol. Psychiatry 2015, 20, 860–866. [Google Scholar] [CrossRef]
- Wu, J.; Song, X.; Chen, G.C.; Neelakantan, N.; van Dam, R.M.; Feng, L.; Yuan, J.M.; Pan, A.; Koh, W.P. Dietary pattern in midlife and cognitive impairment in late life: A prospective study in Chinese adults. Am. J. Clin. Nutr. 2019, 110, 912–920. [Google Scholar] [CrossRef]
- Jacka, F.N.; Cherbuin, N.; Anstey, K.J.; Sachdev, P.; Butterworth, P. Western diet is associated with a smaller hippocampus: A longitudinal investigation. BMC Med. 2015, 13, 215. [Google Scholar] [CrossRef] [PubMed]
- Shakersain, B.; Santoni, G.; Larsson, S.C.; Faxén-Irving, G.; Fastbom, J.; Fratiglioni, L.; Xu, W. Prudent diet may attenuate the adverse effects of Western diet on cognitive decline. Alzheimer’s Dement. 2016, 12, 100–109. [Google Scholar] [CrossRef]
- Torres, S.J.; Lautenschlager, N.T.; Wattanapenpaiboon, N.; Greenop, K.R.; Beer, C.; Flicker, L.; Alfonso, H.; Nowson, C.A. Dietary patterns are associated with cognition among older people with mild cognitive impairment. Nutrients 2012, 4, 1542–1551. [Google Scholar] [CrossRef] [PubMed]
- Kedar, N.P. Can we prevent Parkinson’s and Alzheimer’s disease? J. Postgrad. Med. 2003, 49, 236–245. [Google Scholar]
- Prasad, K.N.; Hovland, A.R.; Cole, W.C.; Prasad, K.C.; Nahreini, P.; Edwards-Prasad, J.; Andreatta, C.P. Multiple antioxidants in the prevention and treatment of Alzheimer disease: Analysis of biologic rationale. Clin. Neuropharmacol. 2000, 23, 2–13. [Google Scholar] [CrossRef] [PubMed]
- Food and Nutrition Board; Health and Medicine Division; National Academies of Sciences, Engineering, and Medicine. Meeting the Dietary Needs of Older Adults: Exploring the Impact of the Physical, Social, and Cultural Environment: Workshop Summary; National Academies Press: Washington, DC, USA, 2016. [Google Scholar]
- Russell, R.M. The aging process as a modifier of metabolism. Am. J. Clin. Nutr. 2000, 72, 529S–532S. [Google Scholar] [CrossRef]
- Flanagan, E.; Lamport, D.; Brennan, L.; Burnet, P.; Calabrese, V.; Cunnane, S.C.; de Wilde, M.C.; Dye, L.; Farrimond, J.A.; Emerson Lombardo, N.; et al. Nutrition and the ageing brain: Moving towards clinical applications. Ageing Res. Rev. 2020, 62, 101079. [Google Scholar] [CrossRef]
- Moore, K.; Hughes, C.F.; Ward, M.; Hoey, L.; McNulty, H. Diet, nutrition and the ageing brain: Current evidence and new directions. Proc. Nutr. Soc. 2018, 77, 152–163. [Google Scholar] [CrossRef]
- Pettigrew, S.; Pescud, M.; Donovan, R.J. Older people’s diet-related beliefs and behaviours: Intervention implications. Nutr. Diet. 2012, 69, 260–264. [Google Scholar] [CrossRef]
- Schaafsma, H.; Laasanen, H.; Twynstra, J.; Seabrook, J.A. A Review of Statistical Reporting in Dietetics Research (2010-2019): How is a Canadian Journal Doing? Can. J. Diet. Pract. Res. 2021, 82, 59–67. [Google Scholar] [CrossRef]
- Adjibade, M.; Assmann, K.E.; Julia, C.; Galan, P.; Hercberg, S.; Kesse-Guyot, E. Prospective association between adherence to the MIND diet and subjective memory complaints in the French NutriNet-Santé cohort. J. Neurol. 2019, 266, 942–952. [Google Scholar] [CrossRef] [PubMed]
- Akbaraly, T.N.; Singh-Manoux, A.; Dugravot, A.; Brunner, E.J.; Kivimäki, M.; Sabia, S. Association of Midlife Diet With Subsequent Risk for Dementia. JAMA 2019, 321, 957–968. [Google Scholar] [CrossRef] [PubMed]
- Barnes, L.L.; Dhana, K.; Liu, X.; Carey, V.J.; Ventrelle, J.; Johnson, K.; Hollings, C.S.; Bishop, L.; Laranjo, N.; Stubbs, B.J.; et al. Trial of the MIND Diet for Prevention of Cognitive Decline in Older Persons. N. Engl. J. Med. 2023, 389, 602–611. [Google Scholar] [CrossRef] [PubMed]
- Berti, V.; Walters, M.; Sterling, J.; Quinn, C.G.; Logue, M.; Andrews, R.; Matthews, D.C.; Osorio, R.S.; Pupi, A.; Vallabhajosula, S.; et al. Mediterranean diet and 3-year Alzheimer brain biomarker changes in middle-aged adults. Neurology 2018, 90, e1789–e1798. [Google Scholar] [CrossRef]
- Bhushan, A.; Fondell, E.; Ascherio, A.; Yuan, C.; Grodstein, F.; Willett, W. Adherence to Mediterranean diet and subjective cognitive function in men. Eur. J. Epidemiol. 2018, 33, 223–234. [Google Scholar] [CrossRef]
- Dearborn-Tomazos, J.L.; Wu, A.; Steffen, L.M.; Anderson, C.A.M.; Hu, E.A.; Knopman, D.; Mosley, T.H.; Gottesman, R.F. Association of Dietary Patterns in Midlife and Cognitive Function in Later Life in US Adults Without Dementia. JAMA Netw. Open 2019, 2, e1916641. [Google Scholar] [CrossRef]
- Hosking, D.E.; Eramudugolla, R.; Cherbuin, N.; Anstey, K.J. MIND not Mediterranean diet related to 12-year incidence of cognitive impairment in an Australian longitudinal cohort study. Alzheimer’s Dement. 2019, 15, 581–589. [Google Scholar] [CrossRef]
- Lassale, C.; Batty, G.D.; Baghdadli, A.; Jacka, F.; Sánchez-Villegas, A.; Kivimäki, M.; Akbaraly, T. Healthy dietary indices and risk of depressive outcomes: A systematic review and meta-analysis of observational studies. Mol. Psychiatry 2019, 24, 965–986, Erratum in Mol. Psychiatry 2021, 26, 3657. https://doi.org/10.1038/s41380-021-01056-7. [Google Scholar] [CrossRef]
- Mattei, J.; Bigornia, S.J.; Sotos-Prieto, M.; Scott, T.; Gao, X.; Tucker, K.L. The Mediterranean Diet and 2-Year Change in Cognitive Function by Status of Type 2 Diabetes and Glycemic Control. Diabetes Care 2019, 42, 1372–1379. [Google Scholar] [CrossRef]
- Muñoz García, M.I.; Toledo, E.; Razquin, C.; Dominguez, L.J.; Maragarone, D.; Martinez-Gonzalez, J.; Martinez-Gonzalez, M.A. “A priori” Dietary Patterns and Cognitive Function in the SUN Project. Neuroepidemiology 2020, 54, 45–57. [Google Scholar] [CrossRef]
- Pearson, K.E.; Wadley, V.G.; McClure, L.A.; Shikany, J.M.; Unverzagt, F.W.; Judd, S.E. Dietary patterns are associated with cognitive function in the REasons for Geographic And Racial Differences in Stroke (REGARDS) cohort. J. Nutr. Sci. 2016, 5, e38. [Google Scholar] [CrossRef] [PubMed]
- Samieri, C.; Sun, Q.; Townsend, M.K.; Chiuve, S.E.; Okereke, O.I.; Willett, W.C.; Stampfer, M.; Grodstein, F. The association between dietary patterns at midlife and health in aging: An observational study. Ann. Intern. Med. 2013, 159, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Shannon, O.M.; Stephan, B.C.M.; Granic, A.; Lentjes, M.; Hayat, S.; Mulligan, A.; Brayne, C.; Khaw, K.T.; Bundy, R.; Aldred, S.; et al. Mediterranean diet adherence and cognitive function in older UK adults: The European Prospective Investigation into Cancer and Nutrition-Norfolk (EPIC-Norfolk) Study. Am. J. Clin. Nutr. 2019, 110, 938–948. [Google Scholar] [CrossRef]
- Shi, Z.; El-Obeid, T.; Li, M.; Xu, X.; Liu, J. Iron-related dietary pattern increases the risk of poor cognition. Nutr. J. 2019, 18, 48. [Google Scholar] [CrossRef]
- Sohouli, M.H.; Rohani, P.; Nasehi, M.M.; Hekmatdoost, A. Changes in serum brain-derived neurotrophic factor following supplementation of omega 3 fatty acids: A systematic review and Meta-Regression analysis. Clin. Nutr. ESPEN 2023, 56, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Wade, A.T.; Davis, C.R.; Dyer, K.A.; Hodgson, J.M.; Woodman, R.J.; Keage, H.A.D.; Murphy, K.J. A Mediterranean Diet with Fresh, Lean Pork Improves Processing Speed and Mood: Cognitive Findings from the MedPork Randomised Controlled Trial. Nutrients 2019, 11, 1521. [Google Scholar] [CrossRef]
- Wade, A.T.; Davis, C.R.; Dyer, K.A.; Hodgson, J.M.; Woodman, R.J.; Keage, H.A.D.; Murphy, K.J. A Mediterranean diet supplemented with dairy foods improves mood and processing speed in an Australian sample: Results from the MedDairy randomized controlled trial. Nutr. Neurosci. 2020, 23, 646–658. [Google Scholar] [CrossRef]
- Xu, X.; Parker, D.; Shi, Z.; Byles, J.; Hall, J.; Hickman, L. Dietary Pattern, Hypertension and Cognitive Function in an Older Population: 10-Year Longitudinal Survey. Front. Public Health 2018, 6, 201. [Google Scholar] [CrossRef]
- Firth, J.; Gangwisch, J.E.; Borisini, A.; Wootton, R.E.; Mayer, E.A. Food and mood: How do diet and nutrition affect mental wellbeing? BMJ 2020, 369, m2382. [Google Scholar] [CrossRef]
- Morley, J.E. Cognition and nutrition. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 1–4. [Google Scholar] [CrossRef]
- Smith, M.A.; Scholey, A.B. Nutritional influences on human neurocognitive functioning. Front. Hum. Neurosci. 2014, 8, 358. [Google Scholar] [CrossRef]
- Miquel, S.; Champ, C.; Day, J.; Aarts, E.; Bahr, B.A.; Bakker, M.; Bánáti, D.; Calabrese, V.; Cederholm, T.; Cryan, J.; et al. Poor cognitive ageing: Vulnerabilities, mechanisms and the impact of nutritional interventions. Ageing Res. Rev. 2018, 42, 40–55. [Google Scholar] [CrossRef] [PubMed]
- Crupi, R.; Marino, A.; Cuzzocrea, S. n-3 fatty acids: Role in neurogenesis and neuroplasticity. Curr. Med. Chem. 2013, 20, 2953–2963. [Google Scholar] [CrossRef]
- Pocernich, C.B.; Lange, M.L.; Sultana, R.; Butterfield, D.A. Nutritional approaches to modulate oxidative stress in Alzheimer’s disease. Curr. Alzheimer Res. 2011, 8, 452–469. [Google Scholar] [CrossRef]
- Griffiths, K.; Aggarwal, B.B.; Singh, R.B.; Buttar, H.S.; Wilson, D.; De Meester, F. Food Antioxidants and Their Anti-Inflammatory Properties: A Potential Role in Cardiovascular Diseases and Cancer Prevention. Diseases 2016, 4, 28. [Google Scholar] [CrossRef] [PubMed]
- Poulose, S.M.; Miller, M.G.; Scott, T.; Shukitt-Hale, B. Nutritional Factors Affecting Adult Neurogenesis and Cognitive Function. Adv. Nutr. 2017, 8, 804–811. [Google Scholar] [CrossRef]
- Kennedy, D.O. B Vitamins and the Brain: Mechanisms, Dose and Efficacy—A Review. Nutrients 2016, 8, 68. [Google Scholar] [CrossRef]
- Rudzki, L.; Stone, T.W.; Maes, M.; Misiak, B.; Samochowiec, J.; Szulc, A. Gut microbiota-derived vitamins-underrated powers of a multipotent ally in psychiatric health and disease. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 107, 110240. [Google Scholar] [CrossRef]
- Harms, L.R.; Burne, T.H.; Eyles, D.W.; McGrath, J.J. Vitamin D and the brain. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 657–669. [Google Scholar] [CrossRef]
- Kesby, J.P.; Eyles, D.W.; Burne, T.H.; McGrath, J.J. The effects of vitamin D on brain development and adult brain function. Mol. Cell Endocrinol. 2011, 347, 121–127. [Google Scholar] [CrossRef]
- Barbagallo, M.; Dominguez, L.J. Magnesium and health. Intern. Med. 2019, 9, e105. [Google Scholar] [CrossRef]
- Schwalfenberg, G.K.; Genuis, S.J. The Importance of Magnesium in Clinical Healthcare. Scientifica 2017, 2017, 4179326. [Google Scholar] [CrossRef]
- Gower-Winter, S.D.; Levenson, C.W. Zinc in the central nervous system: From molecules to behavior. Biofactors 2012, 38, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, A.S.; Dyck, R.H. Zinc and cortical plasticity. Brain Res. Rev. 2009, 59, 347–373. [Google Scholar] [CrossRef]
- Prakash, A.; Bharti, K.; Majeed, A.B. Zinc: Indications in brain disorders. Fundam. Clin. Pharmacol. 2015, 29, 131–149. [Google Scholar] [CrossRef]
- Travaglia, A.; La Mendola, D. Zinc Interactions With Brain-Derived Neurotrophic Factor and Related Peptide Fragments. Vitam. Horm. 2017, 104, 29–56. [Google Scholar] [CrossRef]
- Natsume, M. Polyphenols: Inflammation. Curr. Pharm. Des. 2018, 24, 191–202. [Google Scholar] [CrossRef]
- Yoon, J.H.; Baek, S.J. Molecular targets of dietary polyphenols with anti-inflammatory properties. Yonsei Med. J. 2005, 46, 585–596. [Google Scholar] [CrossRef]
- Ghosh, D.; Scheepens, A. Vascular action of polyphenols. Mol. Nutr. Food Res. 2009, 53, 322–331. [Google Scholar] [CrossRef]
- Ramassamy, C. Emerging role of polyphenolic compounds in the treatment of neurodegenerative diseases: A review of their intracellular targets. Eur. J. Pharmacol. 2006, 545, 51–64. [Google Scholar] [CrossRef]
- Charisis, S.; Yannakoulia, M.; Scarmeas, N. Diets to promote healthy brain ageing. Nat. Rev. Neurol. 2024, 21, 5–16. [Google Scholar] [CrossRef] [PubMed]
- Clemente-Suárez, V.J.; Beltrán-Velasco, A.I.; Redondo-Flórez, L.; Martín-Rodríguez, A.; Tornero-Aguilera, J.F. Global Impacts of Western Diet and Its Effects on Metabolism and Health: A Narrative Review. Nutrients 2023, 15, 2749. [Google Scholar] [CrossRef] [PubMed]
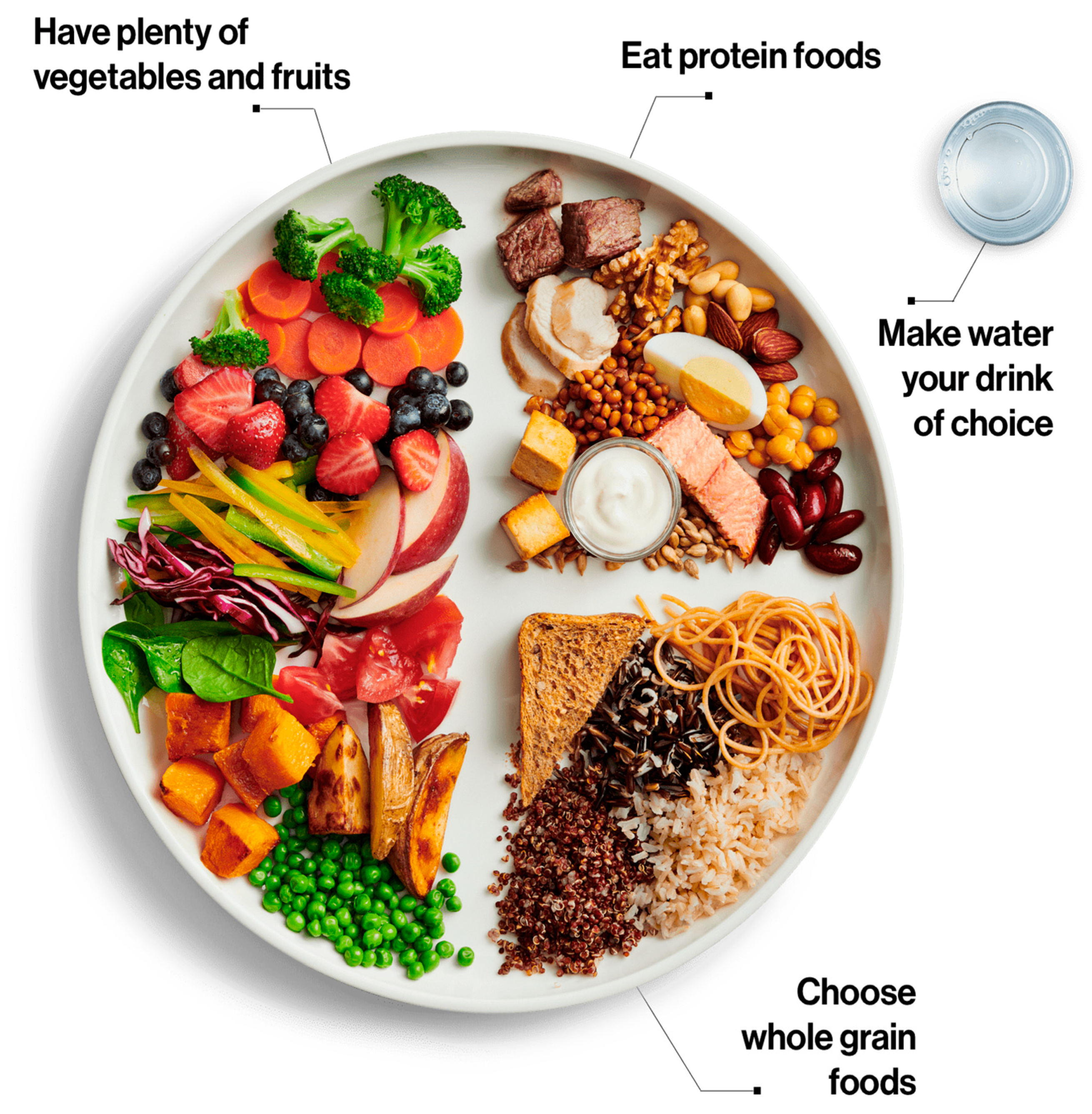
- Health Canada. Canada’s Food Guide; Health Canada: Ottawa, ON, Canada, 2019. [Google Scholar]

{kind=link}
{kind=link}
| Author(s), Year | Objective | Study Design | Sample Size | Key Findings |
|---|---|---|---|---|
| Adjibade et al., 2019 [32] | To examine whether adherence to the MIND diet is associated with subjective memory complaints (SMC) in older adults. | Prospective Cohort. | 6011 participants aged ≥ 60 years without SMC at baseline. | No significant association in full sample or ages 60–69. In adults ≥ 70 years, higher MIND adherence was associated with lower risk of SMC, especially after excluding those with depressive symptoms. |
| Akbaraly et al., 2019 [33] | To examine whether midlife diet quality is associated with later risk of dementia. | Population-based prospective cohort study with up to 25 years of follow-up. | 8225 participants without dementia at baseline (mean age ~50). | No significant association between diet quality in midlife and incident dementia over long-term follow-up. |
| Barnes et al., 2023 [34] | To test whether the MIND diet with mild caloric restriction improves cognition compared to a control diet in older adults at risk of dementia. | Two-site, randomized controlled trial over 3 years. | 604 participants (301 MIND diet, 303 control). | No significant difference in cognitive outcomes or brain MRI measures between MIND and control diet groups after 3 years. Both groups showed modest cognitive improvements. |
| Berti et al., 2018 [35] | To examine the effects of higher vs. lower adherence to a Mediterranean-style diet (MeDi) on Alzheimer’s disease (AD) biomarkers over 3 years. | Longitudinal study with clinical, neuropsychological, and imaging assessments at least 2 years apart. | 70 cognitively normal adults (34 MeDi+ and 36 MeDi-), aged 30–60. | MeDi- group had lower glucose metabolism (FDG-PET) and higher β-amyloid load (PiB-PET) at baseline. Longitudinally, MeDi- showed greater declines in CMRglc and increases in PiB. No MRI effects. Higher MeDi adherence was associated with 1.5 to 3.5 years of AD protection. |
| Bhushan et al., 2018 [36] | To assess the association between long-term adherence to a Mediterranean diet and self-reported subjective cognitive function (SCF). | Prospective observational study. | 27,842 men from the Health Professionals’ Follow-up Study, aged 40–75 at enrollment. | Men in the highest Mediterranean diet quintile had 36% lower odds of poor SCF and 24% lower odds of moderate SCF compared to those in the lowest quintile. Associations were consistent over time, with both past and recent diet contributing. |
| Dearborn-Tomazos et al., 2019 [37] | To examine the association of dietary patterns in midlife with cognitive function and dementia risk in later life. | Observational cohort study using data from the ARIC study (1987–2017). | 13,588 participants (55.8% women), mean age 54.6 at baseline. | No association between midlife dietary patterns (Western or prudent) and cognitive function change over 20 years or risk of incident dementia. Participants with a Western diet had lower cognitive scores at baseline, but no significant long-term differences in cognitive change or dementia risk. |
| Hosking et al., 2019 [38] | To evaluate the relationship between the MIND and Mediterranean diets and the 12-year incidence of Alzheimer’s disease, vascular dementia, and mild cognitive impairment in Australia. | Longitudinal cohort study (PATH Through Life). | 1220 participants (Canberra, Australia). | In adjusted models, the MIND diet was associated with reduced odds of cognitive impairment (OR = 0.47, 95% CI 0.24, 0.91) over 12 years, but the Mediterranean diet was not. The MIND diet’s protective effects appear geographically generalizable, though further studies are needed. |
| Lassale et al., 2019 [39] | To synthesize evidence on the link between diet quality and depression outcomes to guide future psychiatric healthcare. | Systematic review and meta-analysis of longitudinal and cross-sectional studies. | 41 studies (20 longitudinal, 21 cross-sectional). | The Mediterranean diet showed the strongest association with a lower incidence of depression (relative risk 0.67). A lower Dietary Inflammatory Index was also linked to reduced depression incidence (relative risk 0.76). Other dietary indices (e.g., HEI, AHEI) showed similar trends. Adherence to a healthy diet, particularly the Mediterranean diet, appears to offer protection against depression. |
| Mattei et al., 2019 [40] | To examine associations between Mediterranean diet score (MeDS) and 2-year change in cognitive function based on type 2 diabetes and glycemic control status. | Longitudinal study (Boston Puerto Rican Health Study). | 913 (42.6% with type 2 diabetes at baseline). | Higher MeDS was associated with greater improvement in global cognitive function in adults with type 2 diabetes (p = 0.016). This effect was significant for those with controlled glycemic levels and stable/improved control over 2 years, but not for those with uncontrolled or declined glycemic control. Healthy diets supported memory function in adults without type 2 diabetes. |
| Muñoz García et al., 2020 [41] | To study and compare associations of 5 dietary patterns (MDP, DASH, MIND, AHEI-2010, and PVD) with cognitive function. | Cohort Study. | 806 participants. | The MIND diet and AHEI-2010 were beneficially associated with cognitive function. MDP, DASH, and PVD showed positive trends, but results were not statistically significant. The MIND diet appeared to modify cognitive function changes over time. |
| Pearson et al., 2016 [42] | To evaluate associations between dietary patterns and cognitive function in older adults. | Cohort study using data from the REasons for Geographic And Racial Differences in Stroke (REGARDS) cohort. | 18,080 participants aged 45 and older. | Five dietary patterns were identified: convenience, plant-based, sweets/fats, Southern, and alcohol/salads. Greater consumption of the alcohol/salads pattern was associated with lower odds of cognitive impairment and higher cognitive function scores. The plant-based pattern was linked to better learning and memory scores. The Southern pattern, characterized by fried food and processed meats, was associated with lower cognitive scores. |
| Samieri et al., 2013 [43] | To examine the association between dietary patterns in midlife and the prevalence of healthy aging. | Cross-sectional observational study. | 10,670 women. | Greater adherence to the Alternative Healthy Eating Index-2010 (AHEI-2010) and Alternate Mediterranean diet in midlife was associated with significantly higher odds of healthy aging (34% and 46%, respectively). This was particularly linked to better physical function and mental health. The study suggests that better diet quality in midlife is strongly linked to health and well-being in older age. |
| Shannon et al., 2019 [44] | To examine associations between MedDiet adherence and cognitive function in older UK adults. To investigate whether associations differ between individuals with high and low cardiovascular disease (CVD) risk. | Cross-sectional observational study. | 8009 participants. | Higher adherence to MedDiet associated with better cognitive function. MedDiet adherence linked to lower risk of poor cognitive performance. A 1-point increase in Pyramid MedDiet score = 1.7 fewer years of cognitive aging. Stronger associations found in individuals at higher CVD risk. |
| Shi et al., 2019 [45] | To examine the association between iron-related dietary pattern (IDP) and cognitive function in Chinese adults. | Longitudinal study using data from the China Health and Nutrition Survey (CHNS) (1991–2006). | N = 4852, ≥55 years old. | High IDP intake was associated with poor cognition. The odds ratio for poor cognitive function across IDP quartiles was 1.00, 1.06, 1.24, and 1.50. The association was significant only among those with low or no meat intake. IDP was also positively associated with lead intake, mediating the relationship. |
| Sohouli et al., 2023 [46] | To investigate the effects of omega-3 supplementation on BDNF levels. | Random-effects meta-analysis of controlled trials. | Data from multiple trials. | Omega-3 supplementation significantly increased BDNF levels (pooled WMD 1.01 μmol/L, 95% CI 0.35–1.67, p = 0.003). The increase was more pronounced for interventions > 10 weeks and doses ≤ 1500 mg/day, especially in individuals under 50 years. |
| Wade et al., 2019 [47] | To assess the cognitive effects of a Mediterranean diet, including fresh, lean pork, in older adults. | 24-week parallel cross-over trial comparing MedPork vs. low-fat control diet. | N = 35, aged 45–80, at cardiovascular risk. | MedPork led to improved processing speed (p = 0.01) and emotional role functioning (p = 0.03) compared to control. Diet was well tolerated. |
| Wade et al., 2020 [48] | To examine the cognitive and psychological effects of a Mediterranean diet with adequate calcium in an aging population. | Randomized controlled cross-over trial comparing MedDairy and low-fat control diet. | N = 41, aged ≥ 45, at cardiovascular risk. | MedDairy improved processing speed (p = 0.04) and several mood measures (Total Mood Disturbance, Tension, Depression, Anger, Confusion). No significant effects on memory, planning, or dementia risk scores. |
| Xu et al., 2018 [49] | To examine the association between dietary patterns, hypertension, and cognitive function in older adults. | Longitudinal study of CHNS data (1997–2006). | N = 4847 (10,658 observations), aged ≥ 55 years. | A protein-rich diet was linked to better cognitive scores; a starch-rich diet was linked to poorer scores. Hypertension was independently associated with lower cognitive function. Diet and hypertension both play roles in cognitive aging. |
Overview of Dietary Patterns
|
Common Recommendations Across Brain-Healthy Diets
|
Unique Recommendations
|
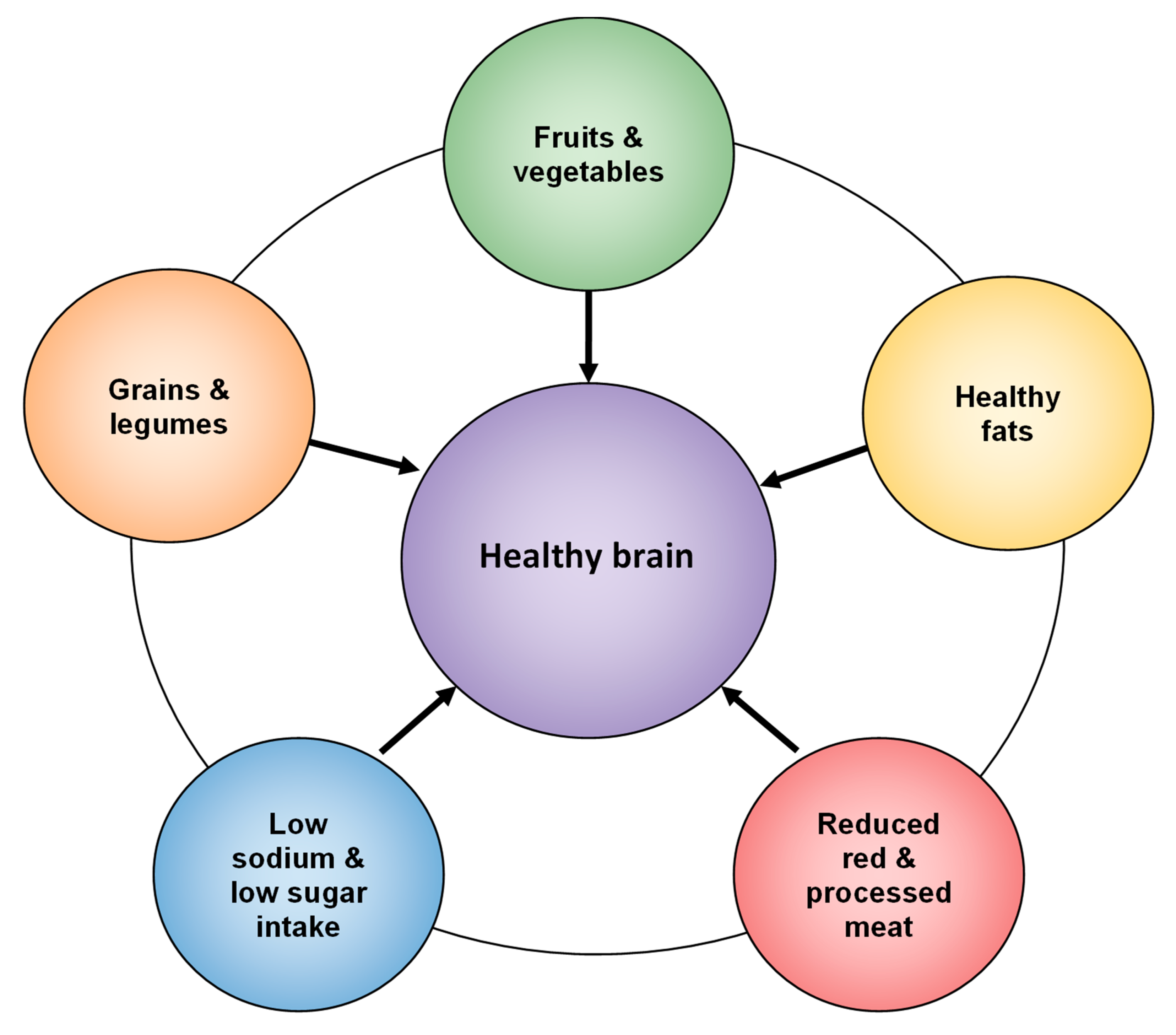
| Interpretation The MedDiet, DASH, and MIND diets converge on recommendations for consuming plant-based foods, healthy fats, and whole grains, while limiting processed foods, unhealthy fats, and red meat. The MIND diet uniquely targets neurodegenerative prevention by emphasizing foods like berries and leafy greens. Conversely, the Western diet’s high intake of processed and inflammatory foods poses significant risks to brain health. Implementing elements from MedDiet, DASH, or MIND can provide a synergistic approach to promoting cognitive health and reducing the risk of dementia. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seabrook, J.A.; Avan, A.; O’Connor, C.; Prapavessis, H.; Nagamatsu, L.; Twynstra, J.; Stranges, S.; MacDougall, A.; Hachinski, V. Dietary Patterns and Brain Health in Middle-Aged and Older Adults: A Narrative Review. Nutrients 2025, 17, 1436. https://doi.org/10.3390/nu17091436
Seabrook JA, Avan A, O’Connor C, Prapavessis H, Nagamatsu L, Twynstra J, Stranges S, MacDougall A, Hachinski V. Dietary Patterns and Brain Health in Middle-Aged and Older Adults: A Narrative Review. Nutrients. 2025; 17(9):1436. https://doi.org/10.3390/nu17091436
Chicago/Turabian StyleSeabrook, Jamie A., Abolfazl Avan, Colleen O’Connor, Harry Prapavessis, Lindsay Nagamatsu, Jasna Twynstra, Saverio Stranges, Arlene MacDougall, and Vladimir Hachinski. 2025. "Dietary Patterns and Brain Health in Middle-Aged and Older Adults: A Narrative Review" Nutrients 17, no. 9: 1436. https://doi.org/10.3390/nu17091436
APA StyleSeabrook, J. A., Avan, A., O’Connor, C., Prapavessis, H., Nagamatsu, L., Twynstra, J., Stranges, S., MacDougall, A., & Hachinski, V. (2025). Dietary Patterns and Brain Health in Middle-Aged and Older Adults: A Narrative Review. Nutrients, 17(9), 1436. https://doi.org/10.3390/nu17091436