Abstract
This systematic review investigates the effect of botulinum neurotoxin (BoNT) therapy on cancer-related disorders. A major bulk of the literature is focused on BoNT’s effect on pain at the site of surgery or radiation. All 13 published studies on this issue indicated reduction or cessation of pain at these sites after local injection of BoNTs. Twelve studies addressed the effect of BoNT injection into the pylorus (sphincter between the stomach and the first part of the gut) for the prevention of gastroparesis after local resection of esophageal cancer. In eight studies, BoNT injection was superior to no intervention; three studies found no difference between the two approaches. One study compared the result of intra-pyloric BoNT injection with preventive pyloromyotomy (resection of pyloric muscle fibers). Both approaches reduced gastroparesis, but the surgical approach had more serious side effects. BoNT injection was superior to saline injection in the prevention of esophageal stricture after surgery (34% versus 6%, respectively, p = 0.02) and produced better results (30% versus 40% stricture) compared to steroid (triamcinolone) injection close to the surgical region. All 12 reported studies on the effect of BoNT injection into the parotid region for the reduction in facial sweating during eating (gustatory hyperhidrosis) found that BoNT injections stopped or significantly reduced facial sweating that developed after parotid gland surgery. Six studies showed that BoNT injection into the parotid region prevented the development of or healed the fistulas that developed after parotid gland resection—parotidectomy gustatory hyperhidrosis (Frey syndrome), post-surgical parotid fistula, and sialocele. Eight studies suggested that BoNT injection into masseter muscle reduced or stopped severe jaw pain after the first bite (first bite syndrome) that may develop as a complication of parotidectomy.
Keywords:
botulinum toxin; botulinum neurotoxin; cancer; radiation; pain; gastroparesis; esophageal stricture; parotid gland; parotid fistula; sialocele; gustatory hyperhidrosis; first bite syndrome Key Contribution:
In cancer patients, botulinum toxins can reduce pain after surgery or radiation, improve gastroparesis by relaxing the pylorus, and prevent the development of esophageal structures following esophagectomy. They have the potential to slow the growth of cancer cells both in vitro and in vivo.
1. Introduction
Botulinum neurotoxins (BoNTs) are now major therapeutic agents for a large number of medical disorders based on their ability to inhibit the release of acetylcholine and pain neurotransmitters from presynaptic vesicles [1,2]. They are considered the treatment of choice for several movement disorders, such as cervical dystonia, blepharospasm, and hemifacial spasm [3]. The same anticholinergic mechanism makes BoNTs very useful for the treatment of spasticity, a common symptom associated with conditions such as stroke, cerebral palsy, and brain or spinal cord trauma [4].
Both type A and type B toxins have the potential to inhibit or reduce the action of pain transmitters such as calcitonin gene-related peptide (CGRP), substance P, or glutamate, both in the peripheral and the central nervous system [5,6,7]. OnabotulinumtoxinnA has been approved for the treatment of migraines in the US and European federations since 2010. There is strong evidence that both type A and type B are effective against several other disabling pain disorders [8,9,10,11,12].
Over the past 25 years, BoNT therapy has been studied and used for the treatment of a variety of issues associated with cancer. These include treatment of different types of pain associated with cancer, as well as other cancer-related disorders such as gastroparesis secondary to surgical treatment of local esophageal cancer, post-surgical esophageal stricture, and parotid fistula and gustatory hyperhidrosis that may develop following parotid cancer surgery and radiation. The purpose of this review is to provide up-to-date information regarding the abovementioned potential indications of botulinum toxin therapy for cancer-related disorders. The most important gain from conducting this review will be if any of the published literature has reached the level where it can confidently recommend this treatment for cancer-related disorders or justify conducting phase II or phase III clinical trials in this area.
2. Search Design and Search Results
We have searched articles published in Pub Med, Ovid Embrace, and Google Scholar from January 1970 to 1 October 2023, crossing the words cancer (or neoplasm), cancer surgery, radiation with botulinum toxin, or botulinum neurotoxin. Articles not in English were excluded unless the article’s abstract in English provided the minimum information for this review, i.e., number of patients, type of study (double-blind, prospective, retrospective), type and dose of the toxin used, type and location of cancer, location of botulinum toxin injection results, and side effects.
3. Results
Of 957 articles found, 47 met the search criteria and underwent final analysis (Figure 1—Prisma). There were four major clinical categories comprising the effect of botulinum neurotoxins (BoNTs) on cancer-associated symptoms: 1—cancer-related pain; 2—gastroparesis caused by esophagectomy for esophageal cancer; 3—esophageal stricture after focal esophagectomy; 4—complications of parotidectomy or parotid radiation (gustatory hyperhidrosis, fistula, sialocele).
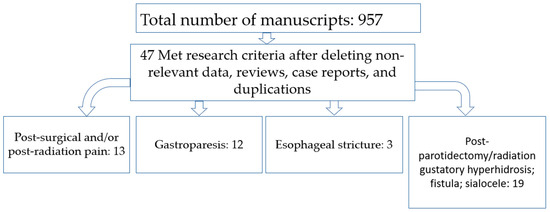
Figure 1.
Total number of articles found as well as numbers in different clinical categories.
4. Cancer-Related Pain
Pain related to cancer can be due to direct pressure from cancer upon pain-sensitive structures, remote effect of cancer upon muscles, or post-radiation/post-surgical pain at the region of scarred tissue.
Direct effect: A malignant tumor (primary or metastatic) can directly press against adjacent structures and cause pain. There are reports that injection of BoNTs into the tumorous tissue can significantly reduce such pains. The existing literature, however, is limited to two case reports [13,14].
The authors have successfully treated severe jaw pain and locked jaw due to metastasis from lung cancer with BoNT in a patient who had developed the inability to fully open her mouth and severe pain in the area of the right masseter when attempting to open the mouth. The problem gradually reached a point where she refrained from eating. Medications, including oxycodone and fentanyl, provided moderate and temporary pain relief but did not alleviate her trismus. A magnetic resonance imaging (MRI) of the jaws demonstrated enlargement of the right masseter muscle due to involvement by metastatic carcinoma (Figure 2). Injection of 50 units of onabotulinumtoxinA into the right masseter and 20 units into the right temporalis muscles decreased the right masseter pain substantially and improved the jaw opening for a period of 6 weeks. Subsequent injections of a larger dose of onaA into the right masseter (70 units) with an additional injection into the left masseter (30 units) enabled her to eat and improved her quality of life (pain relief, less eating difficulty) over the next 18 months before her demise from complications of cancer.
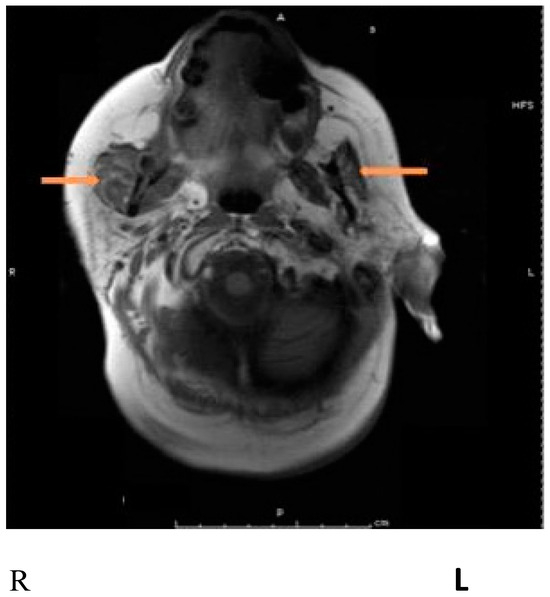
Figure 2.
Magnetic resonance imaging (MRI) showing an enlarged masseter on the right side, probably due to metastatic involvement. Arrows pointing to the masseter muscles bilaterally. From Jabbari B. Botulinum toxin treatment of pain disorders. 2nd edition. Courtesy of publisher. Springer. Berlin, Germany [13].
Another report [14] describes two patients suffering from severe local pain due to the involvement of the psoas muscle by metastatic carcinoma and pressure by adjacent enlarged lymph nodes. Injection of 75 to 100 units of OnaA within two weeks resulted in a marked improvement in pain that lasted for 12 weeks. The main mechanism of pain relief in our patient and the other two reported cases [14] is probably similar (i.e., reducing pressure upon the adjacent nerve(s) due to relaxation of nearby muscles). However, the inhibitory effect of the botulinum toxin upon pain transmitters, as described earlier, can be another contributory factor.
Remote Effect: Malignant tumors, when located inside the brain or spinal cord through affecting motor or sensory fibers, can cause remote effects. These effects are usually in the form of muscle spasms. Two case reports on the remote effects of such cancers are described below. The literature on the remote analgesic effect of botulinum toxin on cancer pain is also limited to two case reports.
The authors have used BoNT for the treatment of disabling, deep neck and shoulder pain associated with extensive ponto-medullary astrocytoma (Figure 3) in a young patient who suffered from spasms of the neck and shoulder muscles. The patient had failed treatments with non-steroidal anti-inflammatory analgesics and tizanidine, and treatment with opioids had minimal analgesic effect. The following muscles were injected with onabotulinum toxinA: left and right splenius capitis (40 units each), left and right trapezius (40 units each), left and right levator scapulae (40 units each), and left and right sternocleidomastoid (20 units each). The total dose was 280 units. The patient reported significant pain relief following these injections. His initial pain score on the Visual Analogue Scale (VAS) was between 8 and 9. It dropped to 3 to 4 a week following injections. The analgesic effect of the injected toxin lasted between 2.5 and 3 months. Injections were repeated every three months for two years until the patient passed away from complications of cancer.
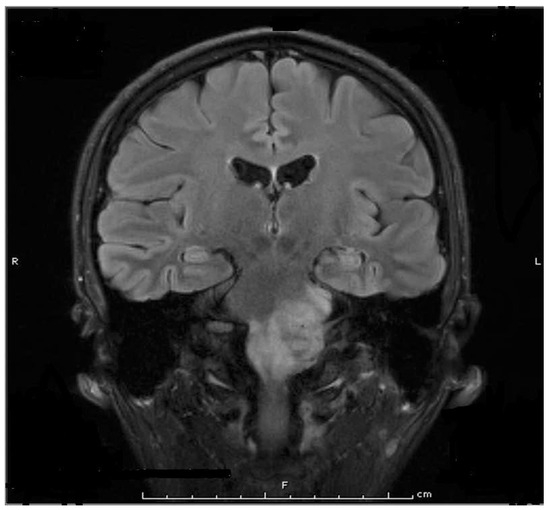
Figure 3.
Magnetic resonance scan (MRI) shows a large ponto-medullary tumor. From Jabbari B. Botulinum toxin treatment of pain disorders. 2nd edition. Courtesy of publisher. Springer, Berlin Germany [13].
Nam and co-workers [15] have reported a 62-year-old male with intracranial chondrosarcoma who suffered from neuropathic pain (burning) in a large area involving the back of the left thigh. Injection of 100 units of onabotulinumtoxinA distributed into 16 regions of the posterior thigh reduced the pain significantly (the pain level on the Visual Analogue Scale dropped from 6 to 2). The mechanism of pain relief in our case and the one reported by Nam and co-worker seems to be different. While in our case, the pain relief seems to be related to toxin-induced relaxation of painful neck muscles, the pain relief in the patient of other reports most likely resulted from the inhibitory effect of onabotulinumtoxinA upon pain transmitters.
5. Pain Following Surgery and/or Radiation
Pain at the site of surgery and radiation is common among cancer patients. Most reported patients have had throat, tongue, and neck cancer. Table 1 represents the search results up to 1 October 2023.

Table 1.
Published studies on the effect of BoNT on local pain resulting from radiation and/or surgery. Revised and updated from Mittal and Jabbari [16].
These positive results are supported by several individual case reports, including one in a patient with Raynaud syndrome secondary to lung cancer in whom severe palm pain improved significantly (3 grades in VAS) after injection of onabotulinumtoxinA at multiple points into the palm [30] (Figure 4).
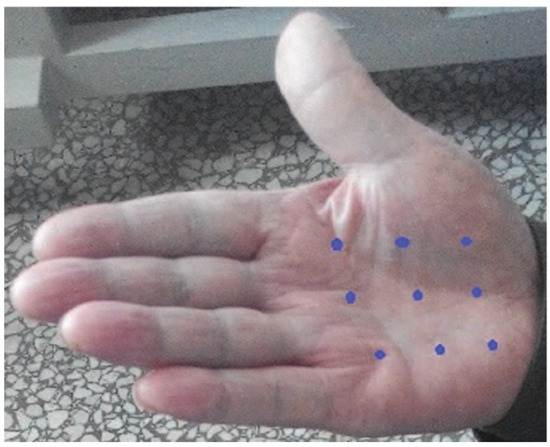
Figure 4.
The blue dots point to the site of BoNT-A injection for treatment of severe palm pain in Raynaud syndrome. From Wang et al., 2016 [30]—reproduced under the Creative Commons Attribution License 4.0. Courtesy of the publisher (Wolters-Kluwer, Amsterdam, Holland).
6. Botulinum Toxin Therapy after Esophagectomy and for Gastroparesis
Esophagectomy may lead to gastroparesis and esophageal stricture. Delayed gastric emptying (DGE) is believed to occur in up to 50% of the patients after esophagectomy for cancer [31]. Delayed gastric emptying following esophagectomy can increase the risk of aspiration, leading to prolonged hospital stays and decreasing the patient’s satisfaction after surgery. The searched literature suggests the utility of local injection of botulinum toxins in these disorders (Table 2).
Table 2.
Botulinum toxin treatment in cancer-related esophagectomy and gastroparesis (excluding single case reports).
Table 2 shows 12 studies, prospective and retrospective but no blinded investigation, describing the effect of botulinum toxin injections on DGE or preventing the development of DGE after esophagectomy. In seven studies, BoNT was injected during and in four studies after esophagectomy. One study evaluated the effect of combined BoNT injection and ballooning on post-esophagectomy DGE. In three of these studies, the dose of BoNT is not mentioned [38,39,41], and in one of the three [39], the authors did not mention which type of A toxin was used. Since the efficacy of the BoNT is highly dose-dependent, the results of these three studies cannot be compared with the rest; hence, they are not included in the final analysis. Unfortunately, these three studies are included in a recently published meta-analysis of this subject, making the authors’ conclusions debatable [44]. Among the remaining studies, six found that intra or postoperative injection of BoNTs into pyrolus led to the development of DGE in fewer patients, while three did not. In one study [43], intrapyloric injection of onabotulinumtoxinA combined with balloon dilatation in 85% of the patients improved the severity of DGE by 50% or more.
7. Esophageal Stricture (ES)
Esophageal stricture is common after esophagectomy and, depending on the esophageal pathology, affects 4–46% of the patients after esophageal surgery [45]. Dysphagia is a common symptom of ES. Severe cases may require tube feeding. Milder cases of ES are treated with balloon dilation, which may be repeated if necessary. More severe cases may require intralesional steroid injection or reconstructive surgery [46].
Wen et al. [47], in a double-blind, placebo-controlled study, investigated the effect of BoNT injections in 72 patients affected by ES caused by esophagectomy for squamous cell carcinoma with esophageal stent (ESD). Patients were divided into two groups: one group received an injection of BoNT-A (Lanzhou Institute of Biological Products, Lanzhou, China) immediately after dissection and ESD, while the other group served as a control and received no BoNT-A. One hundred units of the BoNT-A were divided into 10-unit portions and injected into ten points around the area of resection. A follow-up endoscopy defined the stricture formation when the esophageal lumen was less than 9.8 mm, not allowing the passage of a standard endoscope through the stenotic area. The secondary outcome measure was the number of esophageal balloon dilations required after surgery. The BoNT group demonstrated less development of stenosis compared to the control group: 6.1% versus 32.4% (p = 0.02). The BoNT group also required fewer esophageal dilations than the control group (p = 0.002). Dysphagia grading using the Mellow–Pinkas dysphagia score was also lower in the BoNT-treated group.
In another study, Zhou et al. [48] prospectively compared the preventive action of BoNT injection against development of strictures with steroid (triamcinolone) and no intervention (control group) in 80 patients who underwent submucosal resection of esophageal cancer. The BoNT group received 100 units of BoNT-A (Lanzhou Institute of Biological Products, Lanzhou, China) injected along the junction of the defect and normal tissue at 10 points (10 units/point). The total dose of triamcinolone was 40mg and injected deeper, close to the edge of the ulcer. The proportion of patients developing stricture (primary outcome) was 30% in the BoNT group, 40.9% in the triamcinolone group, and 82.4% in the control group (p < 0.001 and p < 004).
In a recent retrospective study of 204 patients [49], the authors compared the effect of oral statins, BoNT injection, oral and topical steroids, and non-intervention with each other in reducing the risk of stricture development after esophagectomy. The authors found that the effect of statins and BoNT injections in preventing the development of strictures were comparable with each other, and the stricture occurrence rates in the statins and BoNT group were significantly lower than both the steroid treatment and the non-intervention approach (Table 3).
Table 3.
Reports of botulinum toxin treatment of esophageal stricture esophagectomy (Search results up to 1 October 2023).
The positive results of the abovementioned studies in humans are supported by several animal studies that show injection of BoNTs close to the site of esophagectomy can reduce the development of esophageal strictures [50,51].
8. Parotidectomy and Parotid Radiation
Parotidectomy for the removal of a cancerous parotid gland or radiation of an affected parotid gland can lead to several medical disorders. Gustatory hyperhidrosis (GH-facial sweating during eating) or Frey syndrome (named after a Polish pathologist) is encountered in 20–60% of the patients after parotidectomy [52]. It impairs the quality of life in 15–30% of the patients. Parotid gland radiation can lead to fistula and sialocele formation. First bite syndrome (severe jaw pain at first bite), though uncommon, is another side effect of parotidectomy. Our literature search found 18 articles regarding BoNT therapy for GH, fistula, and sialocele formation (Table 4).
Table 4.
Reports on botulinum toxin treatment of gustatory hyperhidrosis after parotidectomy and post-parotidectomy sialorrhea, prevention of fistula and sialocele formation after parotid radiation (Search results up to 1 October 2023).
The normal flow of saliva interferes with the healing of fistulas caused by surgery or radiation. Injection of BoNTs into parotid glands reduces the flow of saliva through the inhibitory effect of the toxin-blocking acetylcholine release from parasympathetic fibers that innervate the salivary glands. It has been shown that a significant decrease in the flow of saliva occurs approximately 4 days after intra-parotid BoNT injection [61].
9. First Bite Syndrome
First bite syndrome (FBS) is an uncommon complication of parotidectomy caused by damage to the sympathetic branches innervating the parotid gland and the development of denervation hypersensitivity from unopposed parasympathetic stimulation of the salivary gland’s myoepithelial cells causing pain at the onset of gustatory salivation [71]. Sheik et al. [72] recently reviewed the literature (eight manuscripts, 22 patients) on BoNT therapy in first bite syndrome following parotidectomy; there were no blinded studies, and most reports were retrospective observations. Symptom improvement occurred in all eight patients injected with 40 units of onabotulinumtoxinA. In total, 7 of the 22 patients (38.1%) had complete resolution of FBS after BoNT injection. No side effects were reported.
10. Discussion
Botulinum neurotoxin’s molecule contains a sophisticated machinery that allows the toxin to exert its function within the nerve cell after intramuscular or subcutaneous injection. Each molecule of the toxin consists of a light chain and a heavy chain bound together by a disulfide bond. The heavy chain of the toxin attaches the toxin to the nerve cell surface and initiates the process of entry into the cell (receptor binding and internalization), while the light chain (a protease) exerts the toxin’s function inside the cell by attaching itself to and deactivating specific intracellular proteins (SNARE proteins). SNARE proteins are essential for the rupture of presynaptic vesicles and the release of neurotransmitters cleft (acetylcholine in case of neuromuscular junction) into the synaptic [73]. Of eight recognized toxin serotypes (A–G), types A and B are currently in clinical use due to their long duration of action. Most of the literature on the role of BoNTs in the treatment of cancer-related disorders relates to the action of BoNTs upon post-surgical or post-radiation pain (Table 1). The pain experienced in these conditions is often neuropathic in type, i.e., having a searing or burning quality. In a recent review of the literature, Matak and co-workers [74] presented convincing evidence that BoNTs can reduce the function of pain transmitters (substance P, calcitonin gene-related peptide, glutamate, and others) at cellular, peripheral nerve, and central nervous system levels.
Adding BoNT to the cell culture (trigeminal or dorsal root ganglia neurons) blocks the KCL-evoked release of two major pain neurotransmitters, namely calcitonin gene-related peptide (CGRP) and substance P (SP) [75,76]. A similar effect has been observed in ex-vivo bladder preparations [77,78]. Exposure to BoNTs reduces glutamate release from dorsal horn neurons of the spinal cord [79].
At the peripheral nerve level, injection of onabotulinumtoxinA into the rat’s paw, prior to injection of formalin, reduced the release of glutamate from peripheral nerves into the tissue and alleviated formalin-induced pain [80]. In rat bladders exposed to hydrochloric acid, the release of SP and CGRP was partially inhibited after exposure of the bladder tissue to BoNT-A [78]. BoNT-A decreases the function of sodium channels substantially [81]. Sodium channels are abundantly present on the peripheral nerves and on the central sensory fibers. They are believed to be essential in conducting peripheral sensations (including pain) in the brain [82]. Double-blind, placebo-controlled studies have shown that subcutaneous injection of BoNTs (A or B) can significantly reduce several neuropathic types of pain in humans [7,9,10,11,12].
There is now ample evidence that the analgesic effect of BoNT is also exerted at the central level [7]. Several studies have shown that in animals with experimental bilateral painful peripheral neuropathy, unilateral injection of BoNT into a limb improves the neuropathic pain bilaterally [83,84,85]. In another pain model, when injected into the spinal canal, botulinum toxin was more effective against pain and in lower doses compared to peripheral injection [86]. In cancer patients, when pain appears to have a major muscular component (contraction, spasm), the pain relief after BoNT injection may be all or partly due to inhibition of acetylcholine release leading to muscle relaxation (example: case 2, Figure 3). Inhibition of acetylcholine release also explains the prevention of post-parotidectomy fistula and sialocele development, as well as the improvement in gustatory hyperhidrosis after parotid surgery. Emerging data indicate that botulinum toxin injections may interfere with cancer development, an important subject that was recently reviewed by Grenda and co-workers [87]. In in vitro studies, several authors assessed the effect of BoNT application on different cancer cell lines. Exposure to BoNTs slowed the progression and development of breast, prostate, colon cancer cells, and neuroblastoma cells through different molecular mechanisms [88,89,90,91,92]. In in vivo studies, mostly conducted in mice, investigators have shown that exposure to BoNTs slowed down the progression and development of glioblastoma, prostate, fibrosarcoma, and pancreatic cancers and promoted apoptosis in some of these cancers [92,93,94,95].
11. Conclusions
The inhibitory effect of BoNTs on the synaptic release of acetylcholine and pain neuromediators makes these agents useful for the treatment of several clinical disorders associated with cancer. These consist of pain associated with cancer, treatment of gastroparesis after esophagectomy, prevention of esophageal stricture, and prevention and treatment of fistula and sialocele following parotidectomy. The data on pain associated with cancer overwhelmingly support the analgesic effect of botulinum toxin injections for cancer-associated pain. The data on gastroparesis is mixed, although a majority of the publications suggest its effectiveness for this indication (Table 2). Results of three studies, including a double-blind, placebo-controlled study, attest to the effectiveness of local BoNT injections in the prevention of esophageal stricture development after esophagectomy. Data regarding the prevention or healing of fistula and sialocele is also promising and suggests the effectiveness of BoNTs in promoting the healing of these lesions via the reduction in saliva secretion. Confirmation of the positive effects of these observations awaits the results of well-designed, controlled, and blinded studies, preferably in a large group of patients. The data from basic scientists on the effect of BoNTs slowing showing growth and development of different cancer cells both in vitro and in vivo is important and promising and deserves further evaluation.
Author Contributions
B.J. participated in investigation, writing, review and editing, as well as supervision and project administration. D.S. participated in writing and review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rossetto, O.; Pirazzini, M.; Fabris, F.; Montecucco, C. Botulinum Neurotoxins: Mechanism of Action. Handb. Exp. Pharmacol. 2021, 263, 35–47. [Google Scholar] [CrossRef] [PubMed]
- Pirazzini, M.; Montecucco, C.; Rossetto, O. Toxicology and pharmacology of botulinum and tetanus neurotoxins: An update. Arch. Toxicol. 2022, 96, 1521–1539. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J. Botulinum toxin: State of the art. Mov. Disord. 2017, 32, 1131–1138. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.A.; Schütz, S.G.; Simpson, D.M. Botulinum toxin for neuropathic pain and spasticity: An overview. Pain Manag. 2014, 4, 129–151. [Google Scholar] [CrossRef] [PubMed]
- Matak, I.; Tékus, V.; Bölcskei, K.; Lacković, Z.; Helyes, Z. Involvement of substance P in the antinociceptive effect of botulinum toxin type A: Evidence from knockout mice. Neuroscience 2017, 358, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Lian, Y.; Zhang, H.; Xie, N.; Chen, Y. CGRP Plasma Levels Decrease in Classical Trigeminal Neuralgia Patients Treated with Botulinum Toxin Type A: A Pilot Study. Pain Med. 2020, 21, 1611–1615. [Google Scholar] [CrossRef]
- Lacković, Z. Botulinum Toxin and Pain. Handb. Exp. Pharmacol. 2021, 263, 251–264. [Google Scholar] [CrossRef]
- Dodick, D.W.; Turkel, C.C.; DeGryse, R.E.; Aurora, S.K.; Silberstein, S.D.; Lipton, R.B.; Diener, H.C.; Brin, M.F. OnabotulinumtoxinA for treatment of chronic migraine: Pooled results from the double-blind, randomized, placebo-controlled phases of the PREEMPT clinical program. Headache 2010, 50, 921–936. [Google Scholar] [CrossRef]
- Babcock, M.S.; Foster, L.; Pasquina, P.; Jabbari, B. Treatment of pain attributed to plantar fasciitis with botulinum toxin a: A short-term, randomized, placebo-controlled, double-blind study. Am. J. Phys. Med. Rehabil. 2005, 84, 649–654. [Google Scholar] [CrossRef]
- Yuan, R.Y.; Sheu, J.J.; Yu, J.M.; Chen, W.T.; Tseng, I.J.; Chang, H.H.; Hu, C.J. Botulinum toxin for diabetic neuropathic pain: A randomized double-blind crossover trial. Neurology 2009, 72, 1473–1478. [Google Scholar] [CrossRef]
- Xiao, L.; Mackey, S.; Hui, H.; Xong, D.; Zhang, Q.; Zhang, D. Subcutaneous injection of botulinum toxin a is beneficial in postherpetic neuralgia. Pain Med. 2010, 11, 1827–1833. [Google Scholar] [CrossRef] [PubMed]
- Attal, N.; de Andrade, D.C.; Adam, F.; Ranoux, D.; Teixeira, M.J.; Galhardoni, R.; Raicher, I.; Üçeyler, N.; Sommer, C.; Bouhassira, D. Safety and efficacy of repeated injections of botulinum toxin A in peripheral neuropathic pain (BOTNEP): A randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2016, 15, 555–565. [Google Scholar] [CrossRef] [PubMed]
- Jabbari, B. Botulinum Toxin Treatment of Pain Disorders, 2nd ed.; Springer Nature: Berlin/Heidelberg, Germany, 2022. [Google Scholar]
- Kim, S.I.; Choi, Y. Botulinum Toxin Injection for Intractable Pain in Cancer Patients With Psoas Muscle Invasion. J. Pain Symptom Manag. 2022, 63, e441–e444. [Google Scholar] [CrossRef]
- Nam, K.E.; Kim, J.S.; Hong, B.Y.; Sul, B.; Choi, H.; Jun, S.Y.; Lim, S.H. Botulinum Toxin Type A Injection for Neuropathic Pain in a Patient With a Brain Tumor: A Case Report. Ann. Rehabil. Med. 2017, 41, 1088–1092. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Mittal, S.O.; Jabbari, B. Botulinum Neurotoxins and Cancer-A Review of the Literature. Toxins 2020, 12, 32. [Google Scholar] [CrossRef] [PubMed]
- Van Daele, D.J.; Finnegan, E.M.; Rodnitzky, R.L.; Zhen, W.; McCulloch, T.M.; Hoffman, H.T. Head and neck muscle spasm after radiotherapy: Management with botulinum toxin A injection. Arch. Otolaryngol. Head Neck Surg. 2002, 128, 956–959. [Google Scholar] [CrossRef] [PubMed]
- Vasan, C.W.; Liu, W.C.; Klussmann, J.P.; Guntinas-Lichius, O. Botulinum toxin type A for the treatment of chronic neck pain after neck dissection. Head Neck 2004, 26, 39–45. [Google Scholar] [CrossRef]
- Wittekindt, C.; Liu, W.C.; Preuss, S.F.; Guntinas-Lichius, O. Botulinum toxin A for neuropathic pain after neck dissection: A dose-finding study. Laryngoscope 2006, 116, 1168–1171. [Google Scholar] [CrossRef]
- Hartl, D.M.; Cohen, M.; Juliéron, M.; Marandas, P.; Janot, F.; Bourhis, J. Botulinum toxin for radiation-induced facial pain and trismus. Otolaryngol. Head Neck Surg. 2008, 138, 459–463. [Google Scholar] [CrossRef]
- Stubblefield, M.D.; Levine, A.; Custodio, C.M.; Fitzpatrick, T. The role of botulinum toxin type A in the radiation fibrosis syndrome: A preliminary report. Arch. Phys. Med. Rehabil. 2008, 89, 417–421. [Google Scholar] [CrossRef]
- Chuang, Y.C.; Kim, D.K.; Chiang, P.H.; Chancellor, M.B. Bladder botulinum toxin A injection can benefit patients with radiation and chemical cystitis. BJU Int. 2008, 102, 704–706. [Google Scholar] [CrossRef] [PubMed]
- Vuong, T.; Waschke, K.; Niazi, T.; Richard, C.; Parent, J.; Liberman, S.; Mayrand, S.; Loungnarath, R.; Stein, B.; Devic, S. The value of Botox-A in acute radiation proctitis: Results from a phase I/II study using a three-dimensional scoring system. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 1505–1511. [Google Scholar] [CrossRef] [PubMed]
- Mittal, S.; Machado, D.G.; Jabbari, B. OnabotulinumtoxinA for treatment of focal cancer pain after surgery and/or radiation. Pain Med. 2012, 13, 1029–1033. [Google Scholar] [CrossRef] [PubMed]
- Bach, C.A.; Wagner, I.; Lachiver, X.; Baujat, B.; Chabolle, F. Botulinum toxin in the treatment of post-radiosurgical neck contracture in head and neck cancer: A novel approach. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2012, 129, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Rostami, R.; Mittal, S.O.; Radmand, R.; Jabbari, B. Incobotulinum Toxin-A Improves Post-Surgical and Post-Radiation Pain in Cancer Patients. Toxins 2016, 8, 22. [Google Scholar] [CrossRef] [PubMed]
- De Groef, A.; Devoogdt, N.; Van Kampen, M.; Nevelsteen, I.; Smeets, A.; Neven, P.; Geraerts, I.; Dams, L.; Van der Gucht, E.; Debeer, P. Effectiveness of Botulinum Toxin A for Persistent Upper Limb Pain after Breast Cancer Treatment: A Double-Blinded Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2018, 99, 1342–1351. [Google Scholar] [CrossRef] [PubMed]
- Mailly, M.; Benzakin, S.; Chauvin, A.; Brasnu, D.; Ayache, D. Douleurs post-radiques après radiothérapie pour cancer des voies aérodigestives superieures: Traitement par injections de toxine botulique A Radiation-induced head and neck pain: Management with botulinum toxin a injections. Cancer Radiother. 2019, 23, 312–315. [Google Scholar] [CrossRef] [PubMed]
- Dang, S.; Shinn, J.R.; Sowder, J.; Ries, W.R.; Stephan, S.J. Peri-Incisional Botulinum Toxin Therapy for Treatment of Intractable Head Pain After Lateral Skull Base Surgery: A Case Series. Headache 2019, 59, 1624–1630. [Google Scholar] [CrossRef]
- Wang, L.; Lei, Q.S.; Liu, Y.Y.; Song, G.J.; Song, C.L. A case report of the beneficial effects of botulinum toxin type A on Raynaud phenomenon in a patient with lung cancer. Medicine 2016, 95, e5092. [Google Scholar] [CrossRef]
- Konradsson, M.; Nilsson, M. Delayed emptying of the gastric conduit after esophagectomy. J. Thorac. Dis. 2019, 11, S835–S844. [Google Scholar] [CrossRef]
- Kent, M.S.; Pennathur, A.; Fabian, T.; McKelvey, A.; Schuchert, M.J.; Luketich, J.D.; Landreneau, R.J. A pilot study of botulinum toxin injection for the treatment of delayed gastric emptying following esophagectomy. Surg. Endosc. 2007, 21, 754–757. [Google Scholar] [CrossRef] [PubMed]
- Cerfolio, R.J.; Bryant, A.S.; Canon, C.L.; Dhawan, R.; Eloubeidi, M.A. Is botulinum toxin injection of the pylorus during Ivor Lewis [corrected] esophagogastrectomy the optimal drainage strategy? J. Thorac. Cardiovasc. Surg. 2009, 137, 565–572. [Google Scholar] [CrossRef]
- Martin, J.T.; Federico, J.A.; McKelvey, A.A.; Kent, M.S.; Fabian, T. Prevention of delayed gastric emptying after esophagectomy: A single center’s experience with botulinum toxin. Ann. Thorac. Surg. 2009, 87, 1708–1713; discussion 1713–1714. [Google Scholar] [CrossRef]
- Bagheri, R.; Fattahi, S.H.; Haghi, S.Z.; Aryana, K.; Aryanniya, A.; Akhlaghi, S.; Riyabi, F.N.; Sheibani, S. Botulinum toxin for prevention of delayed gastric emptying after esophagectomy. Asian Cardiovasc. Thorac. Ann. 2013, 21, 689–692. [Google Scholar] [CrossRef] [PubMed]
- Antonoff, M.B.; Puri, V.; Meyers, B.F.; Baumgartner, K.; Bell, J.M.; Broderick, S.; Krupnick, A.S.; Kreisel, D.; Patterson, G.A.; Crabtree, T.D. Comparison of pyloric intervention strategies at the time of esophagectomy: Is more better? Ann. Thorac. Surg. 2014, 97, 1950–1957; discussion 1957–1958. [Google Scholar] [CrossRef] [PubMed]
- Eldaif, S.M.; Lee, R.; Adams, K.N.; Kilgo, P.D.; Gruszynski, M.A.; Force, S.D.; Pickens, A.; Fernandez, F.G.; Luu, T.D.; Miller, D.L. Intrapyloric botulinum injection increases postoperative esophagectomy complications. Ann. Thorac. Surg. 2014, 97, 1959–1964; discussion 1964–1965. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, H.F.; Broderick, R.C.; Harnsberger, C.R.; Divo, F.A.; Coker, A.M.; Jacobsen, G.R.; Sandler, B.J.; Bouvet, M.; Horgan, S. Intraoperative Endoscopic Botox Injection During Total Esophagectomy Prevents the Need for Pyloromyotomy or Dilatation. J. Laparoendosc. Adv. Surg. Tech. A 2016, 26, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.L.; Wilson, L.; Hamm, A.; Bartsch, C.; Boniface, M.; Gleisner, A.; Mitchell, J.D.; Weyant, M.J.; Meguid, R.; Gajdos, C.; et al. Is Chemical Pyloroplasty Necessary for Minimally Invasive Esophagectomy? Ann. Surg. Oncol. 2017, 24, 1414–1418. [Google Scholar] [CrossRef]
- Giugliano, D.N.; Berger, A.C.; Meidl, H.; Pucci, M.J.; Rosato, E.L.; Keith, S.W.; Evans, N.R.; Palazzo, F. Do intraoperative pyloric interventions predict the need for postoperative endoscopic interventions after minimally invasive esophagectomy? Dis. Esophagus 2017, 30, 1–8. [Google Scholar] [CrossRef]
- Marchese, S.; Qureshi, Y.A.; Hafiz, S.P.; Dawas, K.; Turner, P.; Mughal, M.M.; Mohammadi, B. Intraoperative Pyloric Interventions during Oesophagectomy: A Multicentre Study. J. Gastrointest. Surg. 2018, 22, 1319–1324. [Google Scholar] [CrossRef]
- Tham, J.C.; Nixon, M.; Ariyarathenam, A.V.; Humphreys, L.; Berrisford, R.; Wheatley, T.; Sanders, G. Intraoperative pyloric botulinum toxin injection during Ivor-Lewis gastroesophagectomy to prevent delayed gastric emptying. Dis. Esophagus 2019, 32, doy112. [Google Scholar] [CrossRef] [PubMed]
- Bhutani, M.S.; Ejaz, S.; Cazacu, I.M.; Singh, B.S.; Shafi, M.; Stroehlein, J.R.; Mehran, R.J.; Walsh, G.; Vaporciyan, A.; Swisher, S.G.; et al. Endoscopic Intrapyloric Botulinum Toxin Injection with Pyloric Balloon Dilation for Symptoms of Delayed Gastric Emptying after Distal Esophagectomy for Esophageal Cancer: A 10-Year Experience. Cancers 2022, 14, 5743. [Google Scholar] [CrossRef] [PubMed]
- Urschel, J.D.; Blewett, C.J.; Young, J.E.; Miller, J.D.; Bennett, W.F. Pyloric drainage (pyloroplasty) or no drainage in gastric reconstruction after esophagectomy: A meta-analysis of randomized controlled trials. Dig. Surg. 2002, 19, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Lew, R.J.; Kochman, M.L. A review of endoscopic methods of esophageal dilation. J. Clin. Gastroenterol. 2002, 35, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Hordijk, M.L.; Siersema, P.D.; Tilanus, H.W.; Kuipers, E.J. Electrocautery therapy for refractory anastomotic strictures of the esophagus. Gastrointest. Endosc. 2006, 63, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Wen, J.; Lu, Z.; Linghu, E.; Yang, Y.; Yang, J.; Wang, S.; Yan, B.; Song, J.; Zhou, X.; Wang, X.; et al. Prevention of esophageal strictures after endoscopic submucosal dissection with the injection of botulinum toxin type A. Gastrointest. Endosc. 2016, 84, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Chen, H.; Chen, M.; Ding, C.; Zhang, G.; Si, X. Comparison of endoscopic injection of botulinum toxin and steroids immediately after endoscopic submucosal dissection to prevent esophageal stricture: A prospective cohort study. J. Cancer 2021, 12, 5789–5796. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Xia, W.; Tian, L.; Zhu, B.; Chen, M.; Si, X.; Lin, S.; Gong, Y. Comparison of statins with steroids and botulinum toxin A in the prevention of benign strictures after esophageal endoscopic submucosal dissection: A retrospective cohort study. Surg. Endosc. 2023, 37, 4328–4337. [Google Scholar] [CrossRef]
- Svensson, E.; Zvara, P.; Qvist, N.; Hagander, L.; Möller, S.; Rasmussen, L.; Schrøder, H.D.; Hejbøl, E.K.; Bjørn, N.; Petersen, S.; et al. The Effect of Botulinum Toxin Type A Injections on Stricture Formation, Leakage Rates, Esophageal Elongation, and Anastomotic Healing Following Primary Anastomosis in a Long- and Short-Gap Esophageal Atresia Model—A Protocol for a Randomized, Controlled, Blinded Trial in Pigs. Int. J. Surg. Protoc. 2021, 25, 171–177. [Google Scholar] [CrossRef]
- Usui, Y.; Ono, S. Impact of botulinum toxin A injection on esophageal anastomosis in a rabbit model. Pediatr. Surg. Int. 2016, 32, 881–886. [Google Scholar] [CrossRef]
- Linder, T.E.; Huber, A.; Schmid, S. Frey’s syndrome after parotidectomy: A retrospective and prospective analysis. Laryngoscope 1997, 107, 1496–1501. [Google Scholar] [CrossRef] [PubMed]
- Bjerkhoel, A.; Trobbe, O. Frey’s syndrome: Treatment with botulinum toxin. J. Laryngol. Otol. 1997, 111, 839–844. [Google Scholar] [CrossRef] [PubMed]
- Laccourreye, O.; Muscatelo, L.; Naude, C.; Bonan, B.; Brasnu, D. Botulinum toxin type A for Frey’s syndrome: A preliminary prospective study. Ann. Otol. Rhinol. Laryngol. 1998, 107, 52–55. [Google Scholar] [CrossRef] [PubMed]
- von Lindern, J.J.; Niederhagen, B.; Bergé, S.; Hägler, G.; Reich, R.H. Frey syndrome: Treatment with type A botulinum toxin. Cancer 2000, 89, 1659–1663. [Google Scholar] [CrossRef] [PubMed]
- Cavalot, A.L.; Palonta, F.; Preti, G.; Nazionale, G.; Ricci, E.; Staffieri, A.; Di Girolamo, S.; Cortesina, G. [Post-parotidectomy Frey’s syndrome. Treatment with botulinum toxin type A]. Acta Otorhinolaryngol. Ital. 2000, 20, 187–191. [Google Scholar]
- Vargas, H.; Galati, L.T.; Parnes, S.M. A pilot study evaluating the treatment of postparotidectomy sialoceles with botulinum toxin type A. Arch. Otolaryngol. Head Neck Surg. 2000, 126, 421–424. [Google Scholar] [CrossRef][Green Version]
- Küttner, C.; Tröger, M.; Dempf, R.; Eckardt, A. [Effectiveness of botulinum toxin A in the treatment of gustatory sweating]. Nervenarzt 2001, 72, 787–790. [Google Scholar] [CrossRef]
- Eckardt, A.; Kuettner, C. Treatment of gustatory sweating (Frey’s syndrome) with botulinum toxin A. Head Neck 2003, 25, 624–628. [Google Scholar] [CrossRef]
- Nolte, D.; Gollmitzer, I.; Loeffelbein, D.J.; Hölzle, F.; Wolff, K.D. [Botulinum toxin for treatment of gustatory sweating. A prospective randomized study]. Mund. Kiefer Gesichtschir 2004, 8, 369–375. [Google Scholar] [CrossRef]
- Marchese-Ragona, R.; Marioni, G.; Restivo, D.A.; Staffieri, A. The role of botulinum toxin in postparotidectomy fistula treatment. A technical note. Am. J. Otolaryngol. 2006, 27, 221–224. [Google Scholar] [CrossRef]
- Pomprasit, M.; Chintrakarn, C. Treatment of Frey’s syndrome with botulinum toxin. J. Med. Assoc. Thai 2007, 90, 2397–2402. [Google Scholar] [PubMed]
- Marchese, M.R.; Almadori, G.; Giorgio, A.; Paludetti, G. Post-surgical role of botulinum toxin-A injection in patients with head and neck cancer: Personal experience. Acta Otorhinolaryngol. Ital. 2008, 28, 13–16. [Google Scholar] [PubMed]
- Martos Díaz, P.; Bances del Castillo, R.; Mancha de la Plata, M.; Naval Gías, L.; Martínez Nieto, C.; Lee, G.Y.; Muñoz Guerra, M. Clinical results in the management of Frey’s syndrome with injections of Botulinum toxin. Med. Oral Patol. Oral Cir. Bucal 2008, 13, E248–E252. [Google Scholar] [PubMed]
- Cantarella, G.; Berlusconi, A.; Mele, V.; Cogiamanian, F.; Barbieri, S. Treatment of Frey’s syndrome with botulinum toxin type B. Otolaryngol. Head Neck Surg. 2010, 143, 214–218. [Google Scholar] [CrossRef] [PubMed]
- Laskawi, R.; Winterhoff, J.; Köhler, S.; Kottwitz, L.; Matthias, C. Botulinum toxin treatment of salivary fistulas following parotidectomy: Follow-up results. Oral Maxillofac. Surg. 2013, 17, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Steffen, A.; Hasselbacher, K.; Heinrichs, S.; Wollenberg, B. Botulinum toxin for salivary disorders in the treatment of head and neck cancer. Anticancer. Res. 2014, 34, 6627–6632. [Google Scholar] [PubMed]
- Melville, J.C.; Stackowicz, D.J.; Jundt, J.S.; Shum, J.W. Use of Botox (OnabotulinumtoxinA) for the Treatment of Parotid Sialocele and Fistula After Extirpation of Buccal Squamous Cell Carcinoma with Immediate Reconstruction Using Microvascular Free Flap: A Report of 3 Cases. J. Oral Maxillofac. Surg. 2016, 74, 1678–1686. [Google Scholar] [CrossRef]
- Marchese, M.R.; Di Cesare, T.; De Corso, E.; Petracca, M.; Oliveto, G.; Almadori, G. Botulinum Neurotoxin A in the Treatment of Pharyngocutaneous Fistula after Salvage Surgery in Head and Neck Cancer Patients: Our Preliminary Results. Curr. Oncol. 2022, 29, 7099–7105. [Google Scholar] [CrossRef]
- Mueller, J.; Langbein, T.; Mishra, A.; Baum, R.P. Safety of High-Dose Botulinum Toxin Injections for Parotid and Submandibular Gland Radioprotection. Toxins 2022, 14, 64. [Google Scholar] [CrossRef]
- Laccourreye, O.; Werner, A.; Garcia, D.; Malinvaud, D.; Tran Ba Huy, P.; Bonfils, P. First bite syndrome. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2013, 130, 269–273. [Google Scholar] [CrossRef]
- Shaikh, N.E.; Jafary, H.A.; Behnke, J.W.; Turner, M.T. Botulinum toxin A for the treatment of first bite syndrome-a systematic review. Gland Surg. 2022, 11, 1251–1263. [Google Scholar] [CrossRef] [PubMed]
- Tighe, A.P.; Schiavo, G. Botulinum neurotoxins: Mechanism of action. Toxicon 2013, 67, 87–93. [Google Scholar] [CrossRef]
- Matak, I.; Bölcskei, K.; Bach-Rojecky, L.; Helyes, Z. Mechanisms of Botulinum Toxin Type A Action on Pain. Toxins 2019, 11, 459. [Google Scholar] [CrossRef] [PubMed]
- Durham, P.L.; Cady, R.; Cady, R. Regulation of calcitonin gene-related peptide secretion from trigeminal nerve cells by botulinum toxin type A: Implications for migraine therapy. Headache 2004, 44, 35–42; discussion 42–43. [Google Scholar] [CrossRef] [PubMed]
- Purkiss, J.; Welch, M.; Doward, S.; Foster, K. Capsaicin-stimulated release of substance P from cultured dorsal root ganglion neurons: Involvement of two distinct mechanisms. Biochem. Pharmacol. 2000, 59, 1403–1406. [Google Scholar] [CrossRef] [PubMed]
- Rapp, D.E.; Turk, K.W.; Bales, G.T.; Cook, S.P. Botulinum toxin type a inhibits calcitonin gene-related peptide release from isolated rat bladder. J. Urol. 2006, 175, 1138–1142. [Google Scholar] [CrossRef] [PubMed]
- Lucioni, A.; Bales, G.T.; Lotan, T.L.; McGehee, D.S.; Cook, S.P.; Rapp, D.E. Botulinum toxin type A inhibits sensory neuropeptide release in rat bladder models of acute injury and chronic inflammation. BJU Int. 2008, 101, 366–370. [Google Scholar] [CrossRef]
- Hong, B.; Yao, L.; Ni, L.; Wang, L.; Hu, X. Antinociceptive effect of botulinum toxin A involves alterations in AMPA receptor expression and glutamate release in spinal dorsal horn neurons. Neuroscience 2017, 357, 197–207. [Google Scholar] [CrossRef]
- Cui, M.; Khanijou, S.; Rubino, J.; Aoki, K.R. Subcutaneous administration of botulinum toxin A reduces formalin-induced Pain. Pain 2004, 107, 125–133. [Google Scholar] [CrossRef]
- Shin, M.C.; Wakita, M.; Xie, D.J.; Yamaga, T.; Iwata, S.; Torii, Y.; Harakawa, T.; Ginnaga, A.; Kozaki, S.; Akaike, N. Inhibition of Membrane Na(+) Channels by A Type Botulinum Toxin at Femtomolar Concentrations in Central and Peripheral Neurons. J. Pharmacol. Sci. 2012, 118, 33–42. [Google Scholar] [CrossRef]
- Waxman, S.G.; Cummins, T.R.; Dib-Hajj, S.D.; Black, J.A. Voltage-gated sodium channels and the molecular pathogenesis of pain: A review. J. Rehabil. Res. Dev. 2000, 37, 517–528. [Google Scholar] [PubMed]
- Filipović, B.; Matak, I.; Bach-Rojecky, L.; Lacković, Z. Central action of peripherally applied botulinum toxin type A on pain and dural protein extravasation in rat model of trigeminal neuropathy. PLoS ONE 2012, 7, e29803. [Google Scholar] [CrossRef] [PubMed]
- Favre-Guilmard, C.; Auguet, M.; Chabrier, P.E. Different antinociceptive effects of botulinum toxin type A in inflammatory and peripheral polyneuropathic rat models. Eur. J. Pharmacol. 2009, 617, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Bach-Rojecky, L.; Salković-Petrisić, M.; Lacković, Z. Botulinum toxin type A reduces pain supersensitivity in experimental diabetic neuropathy: Bilateral effect after unilateral injection. Eur. J. Pharmacol. 2010, 633, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Drinovac Vlah, V.; Bach-Rojecky, L.; Lacković, Z. Antinociceptive action of botulinum toxin type A in carrageenan-induced mirror Pain. J. Neural Transm. 2016, 123, 1403–1413. [Google Scholar] [CrossRef]
- Grenda, T.; Grenda, A.; Krawczyk, P.; Kwiatek, K. Botulinum toxin in cancer therapy-current perspectives and limitations. Appl. Microbiol. Biotechnol. 2022, 106, 485–495. [Google Scholar] [CrossRef]
- Karsenty, G.; Rocha, J.; Chevalier, S.; Scarlata, E.; Andrieu, C.; Zouanat, F.Z.; Rocchi, P.; Giusiano, S.; Elzayat, E.A.; Corcos, J. Botulinum toxin type A inhibits the growth of LNCaP human prostate cancer cells in vitro and in vivo. Prostate 2009, 69, 1143–1150. [Google Scholar] [CrossRef]
- Bandala, C.; Cortés-Algara, A.L.; Mejía-Barradas, C.M.; Ilizaliturri-Flores, I.; Dominguez-Rubio, R.; Bazán-Méndez, C.I.; Floriano-Sánchez, E.; Luna-Arias, J.P.; Anaya-Ruiz, M.; Lara-Padilla, E. Botulinum neurotoxin type A inhibits synaptic vesicle 2 expression in breast cancer cell lines. Int. J. Clin. Exp. Pathol. 2015, 8, 8411–8418. [Google Scholar]
- Rust, A.; Leese, C.; Binz, T.; Davletov, B. Botulinum neurotoxin type C protease induces apoptosis in differentiated human neuroblastoma cells. Oncotarget 2016, 7, 33220–33228. [Google Scholar] [CrossRef]
- Shebl, R.I. Anti-cancer Potential of Captopril and Botulinum Toxin Type-A and Associated p53 Gene Apototic Stimulating Activity. Iran. J. Pharm. Res. 2019, 18, 1967–1977. [Google Scholar] [CrossRef]
- Ulloa, F.; Gonzàlez-Juncà, A.; Meffre, D.; Barrecheguren, P.J.; Martínez-Mármol, R.; Pazos, I.; Olivé, N.; Cotrufo, T.; Seoane, J.; Soriano, E. Blockade of the SNARE protein syntaxin 1 inhibits glioblastoma tumor growth. PLoS ONE 2015, 10, e0119707. [Google Scholar] [CrossRef] [PubMed]
- He, D.; Manzoni, A.; Florentin, D.; Fisher, W.; Ding, Y.; Lee, M.; Ayala, G. Biologic effect of neurogenesis in pancreatic cancer. Hum. Pathol. 2016, 52, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Coarfa, C.; Florentin, D.; Putluri, N.; Ding, Y.; Au, J.; He, D.; Ragheb, A.; Frolov, A.; Michailidis, G.; Lee, M.; et al. Influence of the neural microenvironment on prostate cancer. Prostate 2018, 78, 128–139. [Google Scholar] [CrossRef] [PubMed]
- Ansiaux, R.; Baudelet, C.; Cron, G.O.; Segers, J.; Dessy, C.; Martinive, P.; De Wever, J.; Verrax, J.; Wauthier, V.; Beghein, N.; et al. Botulinum toxin potentiates cancer radiotherapy and chemotherapy. Clin. Cancer Res. 2006, 12, 1276–1283. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).