Alleviating Pancreatic Cancer-Associated Pain Using Endoscopic Ultrasound-Guided Neurolysis

 ,
,  ,
, 
Abstract
:1. Introduction
2. Literature Review Methodology
3. Indications for EUS-Guided Neurolysis
4. Anatomy Relevant to Pancreatic Cancer Pain
5. Endoscopic Procedures in EUS-Guided Neurolysis
5.1. Pretreatment Procedure
5.2. Endoscopic Procedure
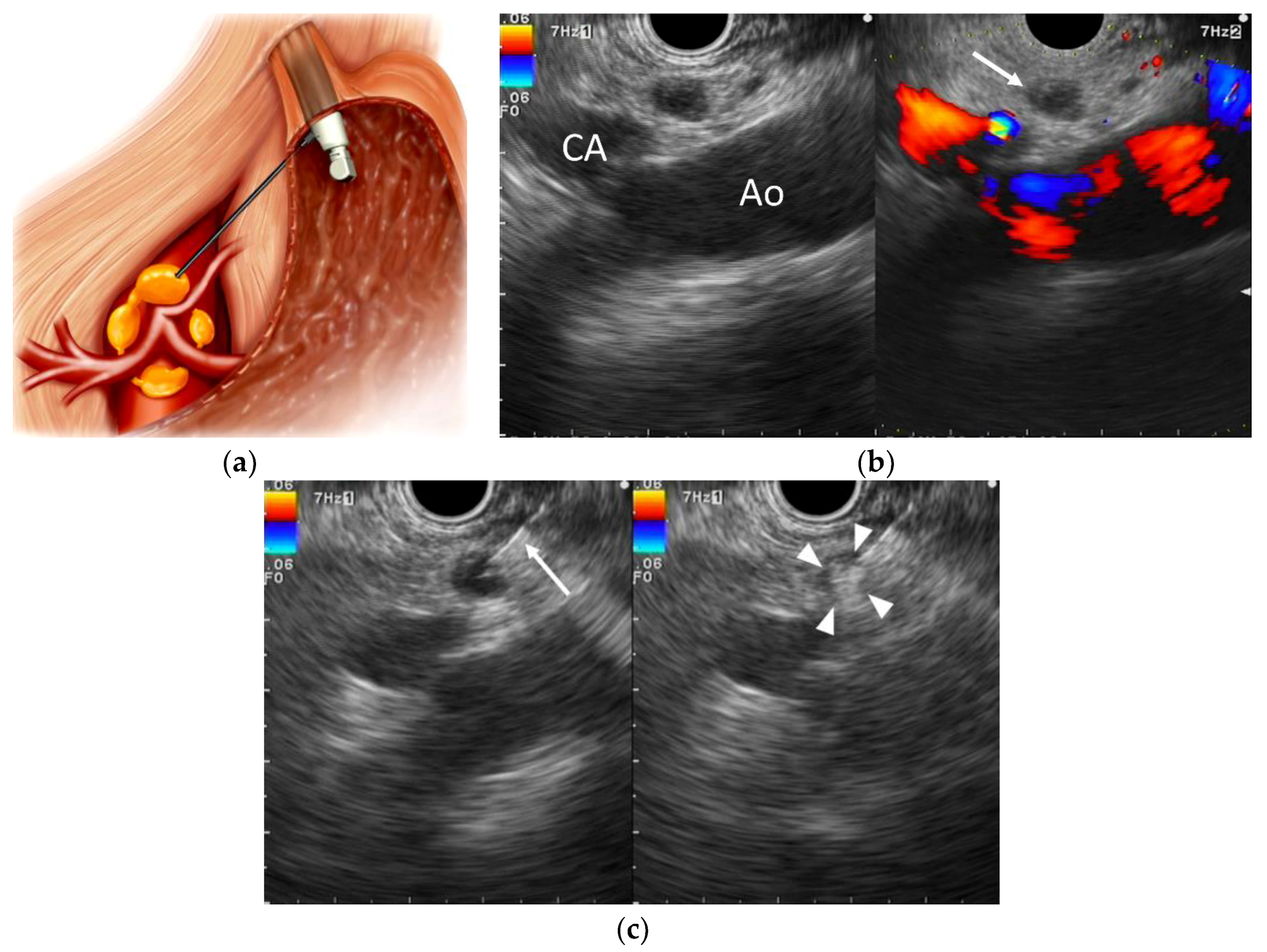
5.2.1. EUS-Guided Celiac Plexus Neurolysis (EUS-CPN)
5.2.2. EUS-Guided Celiac Ganglia Neurolysis (EUS-CGN)
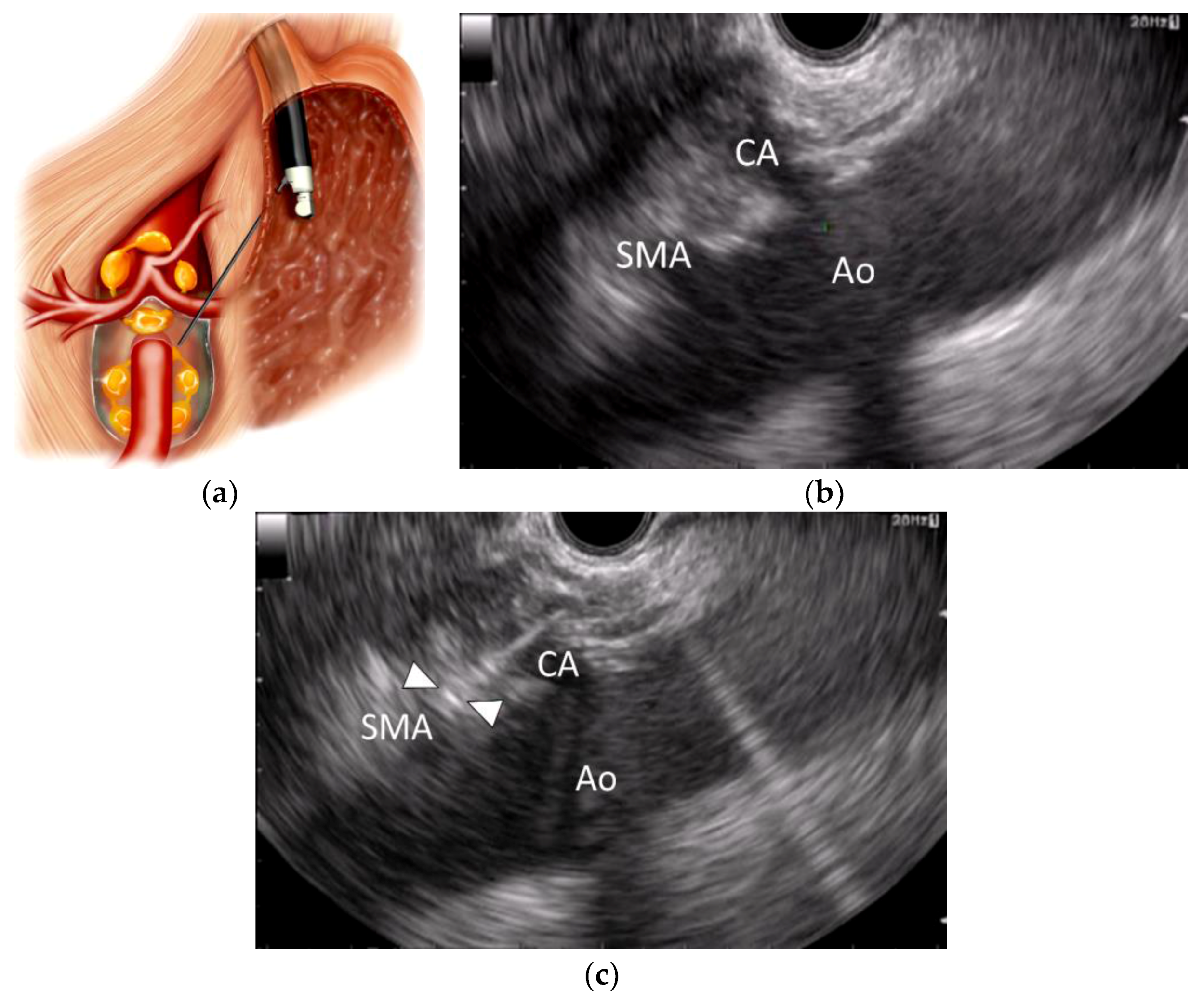
5.2.3. EUS-Guided Broad Plexus Neurolysis (EUS-BPN)
6. Efficacy of EUS-Guided Neurolysis
6.1. EUS-CPN
6.2. EUS-CGN
6.3. EUS-BPN
7. Complications of EUS-Guided Neurolysis
8. Determinants of Pain-Relief Response
9. Conclusions and Future Directions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Bilimoria, K.Y.; Bentrem, D.J.; Ko, C.Y.; Ritchey, J.; Stewart, A.K.; Winchester, D.P.; Talamonti, M.S. Validation of the 6th edition AJCC Pancreatic Cancer Staging System: Report from the National Cancer Database. Cancer 2007, 110, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Sirri, E.; Castro, F.A.; Kieschke, J.; Jansen, L.; Emrich, K.; Gondos, A.; Holleczek, B.; Katalinic, A.; Urbschat, I.; Vohmann, C.; et al. Recent trends in survival of patients with pancreatic cancer in Germany and the United States. Pancreas 2016, 45, 908–914. [Google Scholar] [CrossRef] [PubMed]
- Mekaroonkamol, P.; Willingham, F.F.; Chawla, S. Endoscopic management of pain in pancreatic cancer. J. Oncol. Pract. 2015, 16, 33–40. [Google Scholar]
- Caraceni, A.; Portenoy, R.K. Pain management in patients with pancreatic carcinoma. Cancer 1996, 78, 639–653. [Google Scholar] [CrossRef]
- Arcidiacono, P.G.; Calori, G.; Carrara, S.; McNicol, E.D.; Testoni, P.A. Celiac plexus block for pancreatic cancer pain in adults. Cochrane Database Syst. Rev. 2011, CD007519. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Cancer Pain Relief, 2nd ed.; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Nagels, W.; Pease, N.; Bekkering, G.; Cools, F.; Dobbels, P. Celiac plexus neurolysis for abdominal cancer pain: A systematic review. Pain Med. 2013, 14, 1140–1163. [Google Scholar] [CrossRef] [PubMed]
- Wiersema, M.J.; Wiersema, L.M. Endosonography-guided celiac plexus neurolysis. Gastrointest. Endosc. 1996, 44, 656–662. [Google Scholar] [CrossRef]
- NCCN guidelines for pancreatic adenocarcinoma. Version 3. 2017. Available online: http://jaxelection.altervista.org/pancreatic/NCCN3.2017Pancreatic.pdf (accessed on 21 December 2017).
- Levy, M.J.; Topazian, M.D.; Wiersema, M.J.; Clain, J.E.; Rajan, E.; Wang, K.K.; de la Mora, J.G.; Gleeson, F.C.; Pearson, R.K.; Pelaez, M.C.; et al. Initial evaluation of the efficacy and safety of endoscopic ultrasound-guided direct ganglia neurolysis and block. Am. J. Gastroenterol. 2008, 103, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, H.; Kitano, M.; Kamata, K.; Komaki, T.; Imai, H.; Chikugo, T.; Takeyama, Y.; Kudo, M. EUS-guided broad plexus neurolysis over the superior mesenteric artery using a 25-gauge needle. Am. J. Gastroenterol. 2010, 105, 2599–2606. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, I.; Wang, H.P. Endoscopic ultrasound-guided celiac plexus block and neurolysis. Dig. Endosc. 2017, 29, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Gohil, V.B.; Klapman, J.B. Endoscopic palliation of pancreatic cancer. Curr. Treat. Options Gastroenterol. 2017, 15, 333–348. [Google Scholar] [CrossRef] [PubMed]
- Bhutani, M.S.; Hoffman, B.J.; Hawes, R.H. A swine model for teaching endoscopic ultrasound (EUS) imaging and intervention under EUS guidance. Endoscopy 1998, 30, 605–609. [Google Scholar] [CrossRef] [PubMed]
- Gunaratnam, N.T.; Sarma, A.V.; Norton, I.D.; Wiersema, M.J. A prospective study of EUS-guided celiac plexus neurolysis for pancreatic cancer pain. Gastrointest. Endosc. 2001, 54, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Tran, Q.N.; Urayama, S.; Meyers, F.J. Endoscopic ultrasound-guided celiac plexus neurolysis for pancreatic cancer pain: A single-institution experience and review of the literature. J. Support. Oncol. 2006, 4, 460–464. [Google Scholar] [PubMed]
- Sakamoto, H.; Kitano, M.; Nishio, T.; Takeyama, Y.; Yasuda, C.; Kudo, M. Value of computed tomography for evaluating the injection site in endosonography-guided celiac plexus neurolysis for pancreatic cancer pain. Dig. Endosc. 2006, 18, 206–211. [Google Scholar] [CrossRef]
- Ramirez-Luna, M.A.; Chavez-Tapia, N.C.; Franco-Guzman, A.M.; Garcia-Saenz-de-Sicilia, M.; Tellez-Avila, F.I. Endoscopic ultrasound-guided celiac plexus neurolysis in patients with unresectable pancreatic cancer. Rev. Gastroenterol. Mex. 2008, 73, 63–67. [Google Scholar] [PubMed]
- Sahai, A.V.; Lemelin, V.; Lam, E.; Paquin, S.C. Central vs. bilateral endoscopic ultrasound-guided celiac plexus block or neurolysis: A comparative study of short-term effectiveness. Am. J. Gastroenterol. 2009, 104, 326–329. [Google Scholar] [CrossRef] [PubMed]
- O’Toole, T.M.; Schmulewitz, N. Complication rates of EUS-guided celiac plexus blockade and neurolysis: Results of a large case series. Endoscopy 2009, 41, 593–597. [Google Scholar] [CrossRef] [PubMed]
- Obstein, K.L.; Martins, F.P.; Fernández-Esparrach, G.; Thompson, C.C. Endoscopic ultrasound-guided celiac plexus neurolysis using a reverse phase polymer. World J. Gastroenterol. 2010, 16, 728–731. [Google Scholar] [CrossRef] [PubMed]
- Soweid, A.M.; Azar, C. Endoscopic ultrasound-guided celiac plexus neurolysis. World J. Gastrointest. Endosc. 2010, 2, 228–231. [Google Scholar] [CrossRef] [PubMed]
- Eloubeidi, M.A. Initial evaluation of the forward-viewing echoendoscope prototype for performing fine-needle aspiration, Tru-cut biopsy and celiac plexus neurolysis. J. Gastroenterol. Hepatol. 2011, 26, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Kida, M.; Araki, M.; Miyazawa, S.; Ikeda, H.; Kikuchi, H.; Watanabe, M.; Imaizumi, H.; Koizumi, W. Fine needle aspiration using forward-viewing endoscopic ultrasonography. Endoscopy 2011, 43, 796–801. [Google Scholar] [CrossRef] [PubMed]
- Ascunce, G.; Ribeiro, A.; Reis, I.; Rocha-Lima, C.; Sleeman, D.; Merchan, J.; Levi, J. EUS visualization and direct celiac ganglia neurolysis predicts better pain relief in patients with pancreatic malignancy (with video). Gastrointest. Endosc. 2011, 73, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Iwata, K.; Yasuda, I.; Enya, M.; Mukai, T.; Nakashima, M.; Doi, S.; Iwashita, T.; Tomita, E.; Moriwaki, H. Predictive factors for pain relief after endoscopic ultrasound-guided celiac plexus neurolysis. Dig. Endosc. 2011, 23, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Wyse, J.M.; Carone, M.; Paquin, S.C.; Usatii, M.; Sahai, A.V. Randomized, double-blind, controlled trial of early endoscopic ultrasound-guided celiac plexus neurolysis to prevent pain progression in patients with newly diagnosed, painful, inoperable pancreatic cancer. J. Clin. Oncol. 2011, 29, 3541–3546. [Google Scholar] [CrossRef] [PubMed]
- LeBlanc, J.K.; Al-Haddad, M.; McHenry, L.; Sherman, S.; Juan, M.; McGreevy, K.; Johnson, C.; Howard, T.J.; Lillemoe, K.D.; DeWitt, J. A prospective, randomized study of EUS-guided celiac plexus neurolysis for pancreatic cancer: one injection or two? Gastrointest. Endosc. 2011, 74, 1300–1307. [Google Scholar] [CrossRef] [PubMed]
- Wiechowska-Kozłowska, A.; Boer, K.; Wójcicki, M.; Milkiewicz, P. The efficacy and safety of endoscopic ultrasound-guided celiac plexus neurolysis for treatment of pain in patients with pancreatic cancer. Gastroenterol. Res. Pract. 2012, 2012, 503098. [Google Scholar] [CrossRef] [PubMed]
- Zou, X.P.; Chen, S.Y.; Lv, Y.; Li, W.; Zhang, X.Q. Endoscopic ultrasound-guided celiac plexus neurolysis for pain management in patients with pancreatic carcinoma reasons to fight a losing battle. Pancreas 2012, 41, 655–657. [Google Scholar] [CrossRef] [PubMed]
- Varadarajulu, S.; Bang, J.Y.; Hebert-Magee, S. Assessment of the technical performance of the flexible 19-gauge EUS-FNA needle. Gastrointest. Endosc. 2012, 76, 336–343. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.X.; Jin, Z.D.; Du, Y.Q.; Zhan, X.B.; Zou, D.W.; Liu, Y.; Wang, D.; Chen, J.; Xu, C.; Li, Z.S. EUS-guided celiac ganglion irradiation with iodine-125 seeds for pain control in pancreatic carcinoma: A prospective pilot study. Gastrointest. Endosc. 2012, 76, 945–952. [Google Scholar] [CrossRef] [PubMed]
- Leblanc, J.K.; Rawl, S.; Juan, M.; Johnson, C.; Kroenke, K.; McHenry, L.; Sherman, S.; McGreevy, K.; Al-Haddad, M.; Dewitt, J. Endoscopic ultrasound-guided celiac plexus neurolysis in pancreatic cancer: A prospective pilot study of safety using 10 mL versus 20 mL alcohol. Diagn. Ther. Endosc. 2013, 2013, 327036. [Google Scholar] [CrossRef] [PubMed]
- Seicean, A.; Cainap, C.; Gulei, I.; Tantau, M.; Seicean, R. Pain palliation by endoscopic ultrasound-guided celiac plexus neurolysis in patients with unresectable pancreatic cancer. J. Gastrointestin. Liver Dis. 2013, 22, 59–64. [Google Scholar] [PubMed]
- Doi, S.; Yasuda, I.; Kawakami, H.; Hayashi, T.; Hisai, H.; Irisawa, A.; Mukai, T.; Katanuma, A.; Kubota, K.; Ohnishi, T.; et al. Endoscopic ultrasound-guided celiac ganglia neurolysis vs. celiac plexus neurolysis: A randomized multicenter trial. Endoscopy 2013, 45, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Si-Jie, H.; Wei-Jia, X.; Yang, D.; Lie, Y.; Feng, Y.; Yong-Jian, J.; Ji, L.; Chen, J.; Liang, Z.; De-Liang, F. How to improve the efficacy of endoscopic ultrasound-guided celiac plexus neurolysis in pain management in patients with pancreatic cancer: Analysis in a single center. Surg. Laparosc. Endosc. Percutan. Tech. 2014, 24, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Téllez-Ávila, F.I.; Romano-Munive, A.F.; Herrera-Esquivel, J.J.; Ramírez-Luna, M.A. Central is as effective as bilateral endoscopic ultrasound-guided celiac plexus neurolysis in patients with unresectable pancreatic cancer. Endosc. Ultrasound 2013, 2, 153–156. [Google Scholar] [CrossRef] [PubMed]
- Ishiwatari, H.; Hayashi, T.; Yoshida, M.; Ono, M.; Masuko, H.; Sato, T.; Miyanishi, K.; Sato, Y.; Takimoto, R.; Kobune, M.; et al. Phenol-based endoscopic ultrasound-guided celiac plexus neurolysis for East Asian alcohol-intolerant upper gastrointestinal cancer patients: A pilot study. World J. Gastroenterol. 2014, 20, 10512–10517. [Google Scholar] [CrossRef] [PubMed]
- Ishiwatari, H.; Hayashi, T.; Yoshida, M.; Ono, M.; Sato, T.; Miyanishi, K.; Sato, Y.; Takimoto, R.; Kobune, M.; Masuko, H.; et al. EUS-guided celiac plexus neurolysis by using highly viscous phenol-glycerol as a neurolytic agent (with video). Gastrointest. Endosc. 2015, 81, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Fujii-Lau, L.L.; Bamlet, W.R.; Eldrige, J.S.; Chari, S.T.; Gleeson, F.C.; Abu Dayyeh, B.K.; Clain, J.E.; Pearson, R.K.; Petersen, B.T.; Rajan, E.; et al. Impact of celiac neurolysis on survival in patients with pancreatic cancer. Gastrointest. Endosc. 2015, 82, 46–56. [Google Scholar] [CrossRef] [PubMed]
- Bang, J.Y.; Hasan, M.K.; Sutton, B.; Holt, B.A.; Navaneethan, U.; Hawes, R.; Varadarajulu, S. Intraprocedural increase in heart rate during EUS-guided celiac plexus neurolysis: Clinically relevant or just a physiologic change? Gastrointest. Endosc. 2016, 84, 773–779. [Google Scholar] [CrossRef] [PubMed]
- Facciorusso, A.; Di Maso, M.; Serviddio, G.; Larghi, A.; Costamagna, G.; Muscatiello, N. Echoendoscopic ethanol ablation of tumor combined with celiac plexus neurolysis in patients with pancreatic adenocarcinoma. J. Gastroenterol. Hepatol. 2017, 32, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Minaga, K.; Kitano, M.; Sakamoto, H.; Miyata, T.; Imai, H.; Yamao, K.; Kamata, K.; Omoto, S.; Kadosaka, K.; Sakurai, T.; et al. Predictors of pain response in patients undergoing endoscopic ultrasound-guided neurolysis for abdominal pain caused by pancreatic cancer. Therap. Adv. Gastroenterol. 2016, 9, 483–494. [Google Scholar] [CrossRef] [PubMed]
- Kappelle, W.F.W.; Bleys, R.L.A.W.; van Wijck, A.J.M.; Siersema, P.D.; Vleggaar, F.P. EUS-guided celiac ganglia neurolysis: A clinical and human cadaver study (with video). Gastrointest. Endosc. 2017, 86, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Soetikno, R.M.; Nguyen, P.T.; Chang, K.J. EUS in combination with fine-needle injection celiac plexus neurolysis from within a Wallstent stent. Gastrointest. Endosc. 2002, 56, 136–139. [Google Scholar] [CrossRef] [PubMed]
- Muscatiello, N.; Panella, C.; Pietrini, L.; Tonti, P.; Ierardi, E. Complication of endoscopic ultrasound-guided celiac plexus neurolysis. Endoscopy 2006, 38, 858. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, H.M.; Friedman, S.E.; Henriques, H.F.; Berk, B.S. End-organ ischemia as an unforeseen complication of endoscopic-ultrasound-guided celiac plexus neurolysis. Endoscopy 2009, 41, E218–E219. [Google Scholar] [CrossRef] [PubMed]
- Mittal, M.K.; Rabinstein, A.A.; Wijdicks, E.F. Acute spinal cord infarction following endoscopic ultrasound-guided celiac plexus neurolysis. Neurology 2012, 78, e57–e59. [Google Scholar] [CrossRef] [PubMed]
- Fujii, L.; Clain, J.E.; Morris, J.M.; Levy, M.J. Anterior spinal cord infarction with permanent paralysis following endoscopic ultrasound celiac plexus neurolysis. Endoscopy 2012, 44, E265–E266. [Google Scholar] [CrossRef] [PubMed]
- Gimeno-García, A.Z.; Elwassief, A.; Paquin, S.C.; Sahai, A.V. Fatal complication after endoscopic ultrasound-guided celiac plexus neurolysis. Endoscopy 2012, 44, E267. [Google Scholar] [CrossRef] [PubMed]
- Jang, H.Y.; Cha, S.W.; Lee, B.H.; Jung, H.E.; Choo, J.W.; Cho, Y.J.; Ju, H.Y.; Cho, Y.D. Hepatic and splenic infarction and bowel ischemia following endoscopic ultrasound-guided celiac plexus neurolysis. Clin. Endosc. 2013, 46, 306–309. [Google Scholar] [CrossRef] [PubMed]
- Minaga, K.; Kitano, M.; Imai, H.; Miyata, T.; Kudo, M. Acute spinal cord infarction after EUS-guided celiac plexus neurolysis. Gastrointest. Endosc. 2016, 83, 1039–1040. [Google Scholar] [CrossRef] [PubMed]
- Facciorusso, A.; Maso, M.D.; Barone, M.; Muscatiello, N. Echoendoscopic ethanol ablation of tumor combined to celiac plexus neurolysis improved pain control in a patient with pancreatic adenocarcinoma. Endosc. Ultrasound 2015, 4, 342–344. [Google Scholar] [CrossRef] [PubMed]
- Mulhall, A.M.; Rashkin, M.C.; Pina, E.M. Bilateral diaphragmatic paralysis: A rare complication related to endoscopic ultrasound-guided celiac plexus neurolysis. Ann. Am. Thorac. Soc. 2016, 13, 1660–1662. [Google Scholar] [CrossRef] [PubMed]
- Köker, I.H.; Aralaşmak, A.; Ünver, N.; Asil, T.; Şentürk, H. Spinal cord ischemia after endoscopic ultrasound guided celiac plexus neurolysis: Case report and review of the literature. Scand. J. Gastroenterol. 2017, 52, 1158–1161. [Google Scholar] [CrossRef] [PubMed]
- Lu, F.; Dong, J.; Tang, Y.; Huang, H.; Liu, H.; Song, L.; Zhang, K. Bilateral vs. unilateral endoscopic ultrasound-guided celiac plexus neurolysis for abdominal pain management in patients with pancreatic malignancy: A systematic review and meta-analysis. Support. Care Cancer 2017. [Google Scholar] [CrossRef]
- Kaufman, M.; Singh, G.; Das, S.; Concha-Parra, R.; Erber, J.; Micames, C.; Gress, F. Efficacy of endoscopic ultrasound-guided celiac plexus block and celiac plexus neurolysis for managing abdominal pain associated with chronic pancreatitis and pancreatic cancer. J. Clin. Gastroenterol. 2010, 44, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Puli, S.R.; Reddy, J.B.; Bechtold, M.L.; Antillon, M.R.; Brugge, W.R. EUS-guided celiac plexus neurolysis for pain due to chronic pancreatitis or pancreatic cancer pain: A meta-analysis and systematic review. Dig. Dis. Sci. 2009, 54, 2330–2337. [Google Scholar] [CrossRef] [PubMed]
- Michaels, A.J.; Draganov, P.V. Endoscopic ultrasonography guided celiac plexus neurolysis and celiac plexus block in the management of pain due to pancreatic cancer and chronic pancreatitis. World J. Gastroenterol. 2007, 13, 3575–3580. [Google Scholar] [CrossRef] [PubMed]
- Penman, I.D. State of the art: Putting EUS-guided block/neurolysis into perspective. Gastrointest. Endosc. 2009, 69, S174–S175. [Google Scholar] [CrossRef] [PubMed]
- Barreto, S.G.; Saccone, G.T. Pancreatic nociception—Revisiting the physiology and pathophysiology. Pancreatology 2012, 12, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Kitoh, T.; Tanaka, S.; Ono, K.; Ohfusa, Y.; Ina, H.; Otagiri, T. Combined neurolytic block of celiac, inferior mesenteric and superior hypogastric plexuses for incapacitating abdominal and/or pelvic cancer pain. J. Anesth. 2005, 19, 328–332. [Google Scholar] [CrossRef] [PubMed]
- Adler, D.G.; Conway, J.D.; Coffie, J.M.; Disario, J.A.; Mishkin, D.S.; Shah, R.J.; Somogyi, L.; Tierney, W.M.; Wong Kee Song, L.M.; Petersen, B.T.; et al. EUS accessories. Gastrointest. Endosc. 2007, 66, 1076–1081. [Google Scholar] [CrossRef] [PubMed]
- Gleeson, F.C.; Levy, M.J.; Papachristou, G.I.; Pelaez-Luna, M.; Rajan, E.; Clain, J.E.; Topazian, M.D. Frequency of visualization of presumed celiac ganglia by endoscopic ultrasound. Endoscopy 2007, 39, 620–624. [Google Scholar] [CrossRef] [PubMed]
- Ha, T.; Kim, G.; Kang, D.; Song, G.; Kim, S.; Lee, J. Detection of celiac ganglia with radial scanning endoscopic ultrasonography. Korean J. Intern. Med. 2008, 23, 5–8. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.J.; Wiersema, M.J. EUS-guided celiac plexus neurolysis and celiac plexus block. Gastrointest. Endosc. 2003, 57, 923–930. [Google Scholar] [CrossRef]
- Yan, B.M.; Myers, R.P. Neurolytic celiac plexus block for pain control in unresectable pancreatic cancer. Am. J. Gastroenterol. 2007, 102, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Sánchez, M.V.; Jenssen, C.; Faiss, S.; Napoléon, B. Interventional endoscopic ultrasonography: An overview of safety and complications. Surg. Endosc. 2014, 28, 712–734. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| First Author (Year) [Reference] | Study Design | No. of Patients | Procedure | Outcomes | Complications |
|---|---|---|---|---|---|
| Wiersema (1996) [8] | Prospective? Non-randomized | 30 | EUS-CPN Bilateral | Pain improvement in 79 to 88% of patients with a median follow-up of 10 weeks | Self-limited complications Diarrhea 13.3% Pain increase 3.3% |
| Gunaratnam (2001) [15] | Prospective Non-randomized | 58 | EUS-CPN Bilateral | Decline in pain score after EUS-CPN in 78% of patients | No major complications Pain increase 8.6% |
| Tran (2006) [16] | Retrospective Non-randomized | 8 | EUS-CPN Unilateral | Pain improvement in 70% of 10 procedures (8 patients) | Not described |
| Sakamoto (2006) [17] | Retrospective Non-randomized | 13 | EUS-CPN Bilateral | Pain improvement in 84.6% of patients | Self-limited complications Inebriation 7.7% Pain increase 7.7% Hypotension 15.4% |
| Levy (2008) [10] | Retrospective Non-randomized | 36 (Malignant 18) | EUS-CGN | Pain improvement in 94% of patients | Pain increase 36.1% Hypotension 33.3% Diarrhea 16.6% |
| Ramirez-Luna (2008) [18] | Retrospective Non-randomized | 11 | EUS-CPN Unilateral | Pain improvement in 72% of patients at 4 weeks after CPN | No major complications Transient pain increase 45.4% |
| Sahai (2009) [19] | Retrospective Non-randomized | 160 (Malignant 81) | EUS-CPN Bilateral 89 Unilateral 71 | Pain improvement; 70.4% (bilateral) vs 45.9% (unilateral) Bilateral CPN is more effective than unilateral CPN | Retroperitoneal bleeding 1% (bilateral CPN) |
| Sakamoto (2010) [11] | Retrospective Non-randomized | 67 | EUS-CPN 34 EUS-BPN 33 | Reduction in pain score on days 7 and 30; EUS-BPN > EUS-CPN | No serious complications No cases of prolonged hospitalization |
| Ascunce (2011) [25] | Retrospective Non-randomized | 64 | EUS-CGN 40 EUS-CPN 24 | Pain improvement at 1 week after neurolysis; 65.0% (CGN) vs. 25.0% (bilateral CPN) | Transient pain increase 1.6%, Diarrhea 23.4%, Hypotension 1.6% |
| Iwata (2011) [26] | Retrospective Non-randomized | 47 | EUS-CPN Unilateral | Pain improvement; 68.1% Complete pain relief; 36.2% | Transient hypotension 17.0%, Inebriation 8.5%, Diarrhea 23.4% |
| Wyse (2011) [27] | Prospective Randomized | 48 | EUS-CPN Bilateral | Randomized trial; EUS-CPN vs conventional drug-based pain management Pain relief at 3 months; CPN > drug-based pain management | No evidence of early or late complications |
| LeBlanc (2011) [28] | Prospective Randomized | 50 | EUS-CPN Bilateral 21 Unilateral 29 | Randomized trial; bilateral CPN vs unilateral CPN Pain relief and survival; no difference between the groups | Transient pain increase 36%, Hypotension 2% |
| Wiechowska-Kozłowska (2012) [29] | Retrospective Non-randomized | 29 | EUS-CPN Bilateral | Pain improvement; 86% Complete pain relief; 14% | Transient diarrhea 10.3%, Hypotension 3.4%, Pain increase 6.9% |
| Wang (2012) [32] | Prospective Non-randomized | 23 | EUS-guided irradiation | EUS-guided celiac ganglion irradiation (iodine-125 seeds) Pain improvement in 82.6% of patients at 2 weeks | No major complications Constipation 21.7% Nausea 8.7% |
| Leblanc (2013) [33] | Prospective Randomized | 20 | EUS-CPN Unilateral (+EUS-CGN) | Randomized trial; EUS-CPN using 10 mL vs. 20 mL alcohol Similar clinical outcomes between the groups | Self-limited complications Lightheadedness 5% Diarrhea 10% Nausea 15% |
| Seicean (2013) [34] | Retrospective Non-randomized | 32 | EUS-CPN Unilateral | Pain improvement in 75% of patients | No complications |
| Doi (2013) [35] | Prospective Randomized | 68 | EUS-CGN 34 EUS-CPN 34 | Randomized trial; EUS-CGN vs. EUS-CPN (unilateral) Pain improvement; 73.5% (CGN) vs. 45.5% (CPN) Complete pain relief; 50% (CGN) vs. 18.2% (CPN) | Transient hypotension 4.5%, Inebriation 3.0%, Pain increase 25.4%, Diarrhea 7.5% |
| Téllez-Ávila (2013) [37] | Retrospective Non-randomized | 53 | EUS-CPN Unilateral 21 Bilateral 32 | Bilateral vs. unilateral CPN No significant difference between the groups | No major complications Transient pain increase 1.9% |
| Si-Jie (2014) [36] | Retrospective Non-randomized | 41 | EUS-CGN 26 EUS-CPN 15 | Pain improvement in 90.2% and 61.0% of patients at 1 week and at 3 months, respectively | Transient hypotension 4.9% |
| Ishiwatari (2014) [38] | Retrospective Non-randomized | 22 | EUS-CPN Phenol 6 Ethanol 16 | Pain improvement in 83% and 69% of patients in the phenol and ethanol groups, respectively | Minor complications Phenol group 16.7%, ethanol group 37.5% Inebriation 12.5% (ethanol group) |
| Ishiwatari (2015) [39] | Prospective Non-randomized | 9 | EUS-CPN Phenol-glycerol | Complete, partial and no pain relief in 44.4%, 44.4% and 11.1% of patients at 7 days after the procedure | Minor complications 33.3% |
| Fujii-Lau (2015) [40] | Retrospective Non-randomized | 230 | EUS-CPN or EUS-CGN | EUS-guided celiac neurolysis was associated with longer survival compared with non-EUS approaches | Mild adverse events; 7 patients (1.7%) Moderate to severe adverse events; 5 patients (1.2%) |
| Bang (2016) [41] | Prospective Non-randomized | 51 | EUS-CPN Unilateral | Heart rate change during CPN in 49.0% of patients Better pain relief in the heart rate change cohort | Diarrhea 33.3% |
| Minaga (2016) [43] | Retrospective Non-randomized | 112 | EUS-BPN 65 EUS-BPN + EUS-CGN 47 | Pain improvement in 78% of patient at 1 week EUS-BPN in combination with EUS-CGN is a predictor of a good pain response | Major; Paraplegia 1% Minor; Inebriation 8.0%, Hypotension 4.5%, Pain increase 3.6%, Diarrhea 3.6% |
| Facciorusso (2017) [42] | Retrospective Non-randomized | 123 | EUS-CPN 58 EUS-CPN + ablation 65 | EUS-guided tumor ethanol ablation combined with EUS-CPN increased pain relief and complete pain response rate | No severe treatment-related complications |
| First Author (Year) [Reference] | Complications | Procedure | Neurolytic Agents/Anesthetic Agents | Outcomes |
|---|---|---|---|---|
| Muscatiello (2006) [46] | Retroperitoneal abscess | CPN | Alcohol/Bupivacaine | EUS-guided puncture, complete resolution |
| Mittal (2012) [48] | Paraplegia | CGN + CPN | Alcohol/Bupivacaine | No improvement |
| Fujii-Lau (2012) [49] | Paraplegia | CGN + CPN | Alcohol/Bupivacaine | No improvement |
| Gimeno-García (2012) [50] | Celiac artery thrombosis, hepatic, kidney, splenic infarction, bowel ischemia | CPN Bilateral | Alcohol/Bupivacaine | Conservative treatment, died 8 days later |
| Jang (2013) [51] | Hepatic, splenic infarction, bowel ischemia | CPN Unilateral | Alcohol, triamcinolone acetonide/Bupivacaine | Conservative treatment, died 27 days later |
| Minaga (2016) [52] | Paraplegia | CPN Bilateral | Alcohol/Lidocaine | No improvement |
| Mulhall (2016) [54] | Bilateral diaphragmatic paralysis | CPN | No description | Mechanical ventilation, no improvement |
| Köker (2017) [55] | Paraplegia | CPN Bilateral | Alcohol/Bupivacaine | No improvement |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minaga, K.; Takenaka, M.; Kamata, K.; Yoshikawa, T.; Nakai, A.; Omoto, S.; Miyata, T.; Yamao, K.; Imai, H.; Sakamoto, H.; et al. Alleviating Pancreatic Cancer-Associated Pain Using Endoscopic Ultrasound-Guided Neurolysis. Cancers 2018, 10, 50. https://doi.org/10.3390/cancers10020050
Minaga K, Takenaka M, Kamata K, Yoshikawa T, Nakai A, Omoto S, Miyata T, Yamao K, Imai H, Sakamoto H, et al. Alleviating Pancreatic Cancer-Associated Pain Using Endoscopic Ultrasound-Guided Neurolysis. Cancers. 2018; 10(2):50. https://doi.org/10.3390/cancers10020050
Chicago/Turabian StyleMinaga, Kosuke, Mamoru Takenaka, Ken Kamata, Tomoe Yoshikawa, Atsushi Nakai, Shunsuke Omoto, Takeshi Miyata, Kentaro Yamao, Hajime Imai, Hiroki Sakamoto, and et al. 2018. "Alleviating Pancreatic Cancer-Associated Pain Using Endoscopic Ultrasound-Guided Neurolysis" Cancers 10, no. 2: 50. https://doi.org/10.3390/cancers10020050
APA StyleMinaga, K., Takenaka, M., Kamata, K., Yoshikawa, T., Nakai, A., Omoto, S., Miyata, T., Yamao, K., Imai, H., Sakamoto, H., Kitano, M., & Kudo, M. (2018). Alleviating Pancreatic Cancer-Associated Pain Using Endoscopic Ultrasound-Guided Neurolysis. Cancers, 10(2), 50. https://doi.org/10.3390/cancers10020050