Distribution of Lymph Node Metastases in Esophageal Carcinoma Patients Undergoing Upfront Surgery: A Systematic Review



Abstract
1. Introduction
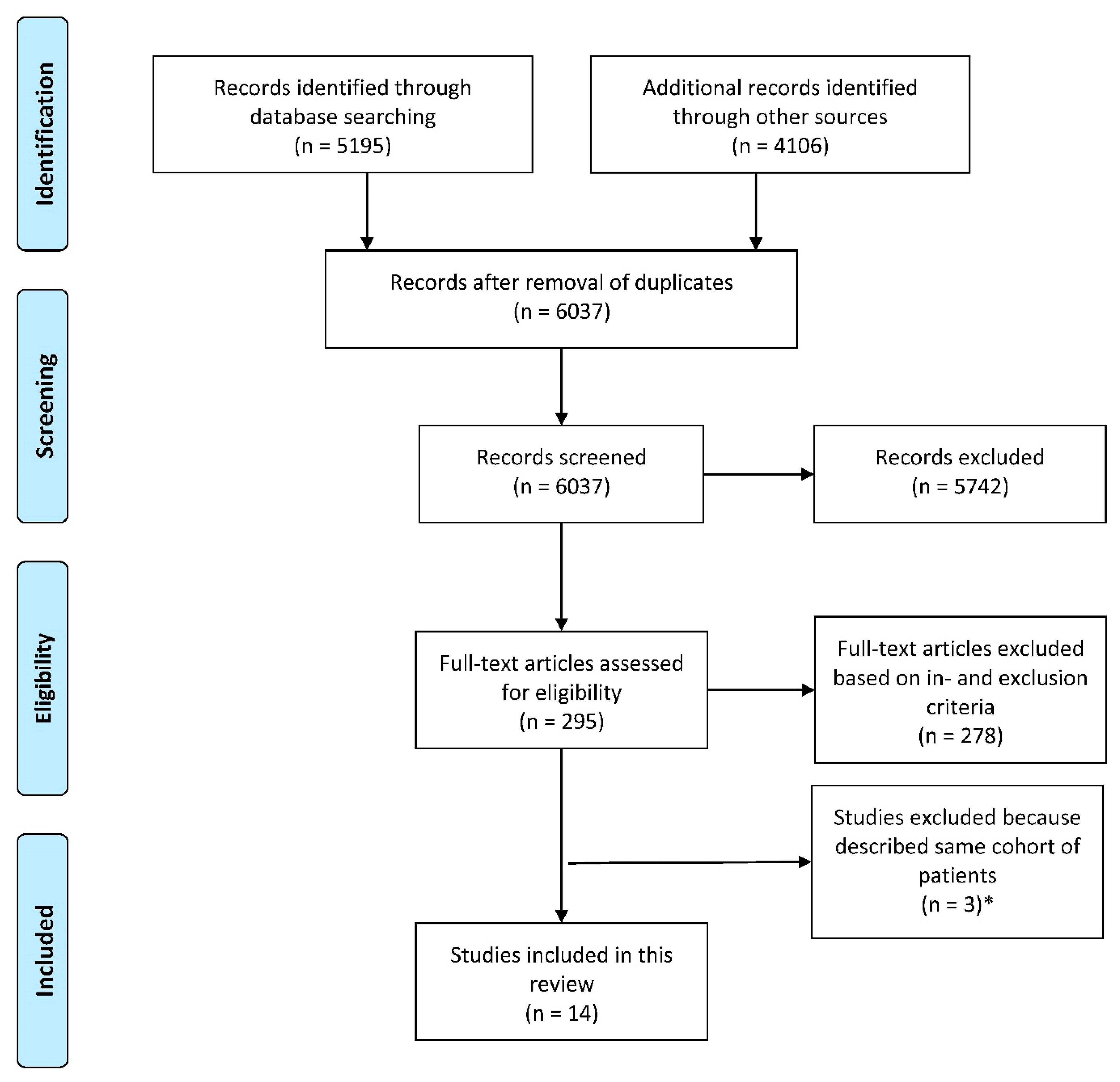
2. Methods
2.1. Data Extraction
2.2. Statistical Analysis
3. Results
3.1. Reporting Standard
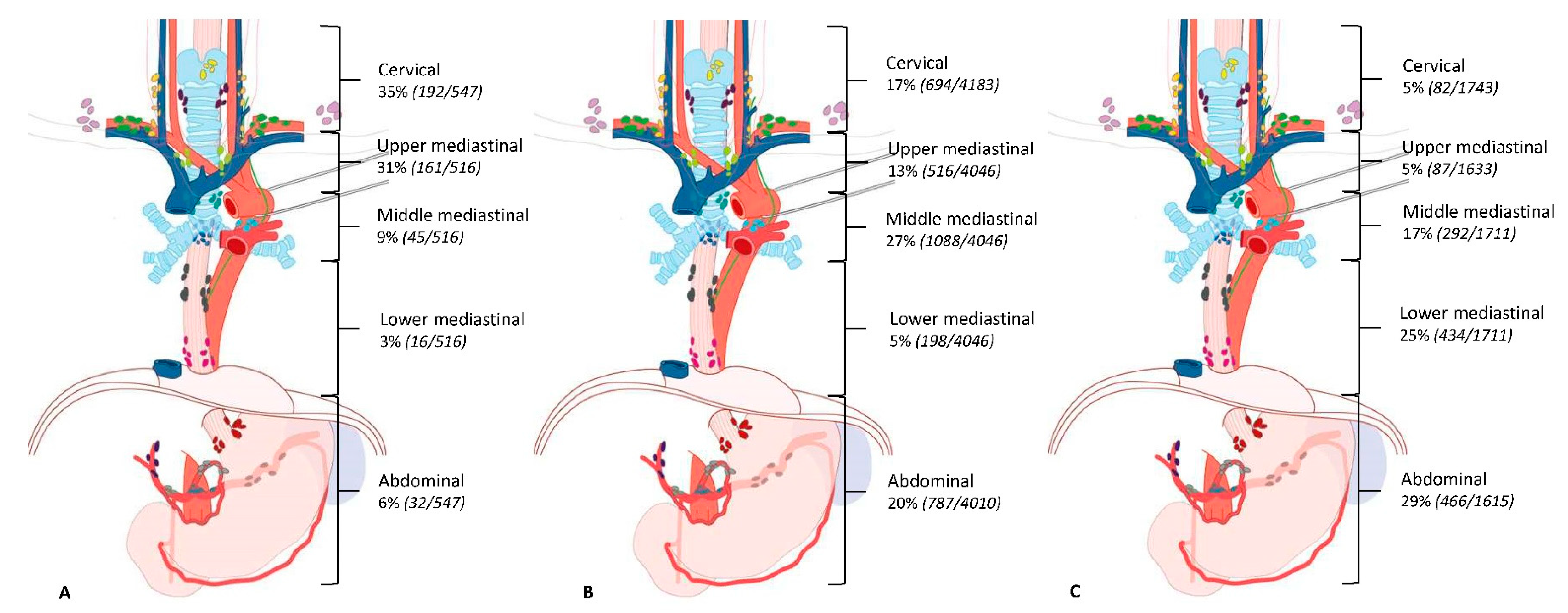
3.2. Distribution Pattern for Esophageal Squamous Cell Carcinoma
3.3. Distribution Pattern for Esophageal Adenocarcinoma
3.4. Distribution of LN Metastases in Relation to pT-Stage
4. Discussion
4.1. Lymphatic Distribution Pattern for Squamous Cell Carcinoma
4.2. Lymphatic Distribution Pattern for Adenocarcinoma
5. Conclusions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Search | Query | Items Found |
|---|---|---|
| #1 | (((((((((((“Esophageal Neoplasms”[Mesh] OR “Esophagectomy”[Mesh] OR ((esophagus[tiab] OR esophageal[tiab] OR esophagogastric[tiab] OR oesophagus[tiab] OR oesophageal[tiab] OR oesophagogastric[tiab] OR gastroesophag*[tiab] OR gastrooesophag*[tiab]) AND (neoplas*[tiab] OR cancer*[tiab] OR carcino*[tiab] OR adenocarcino*[tiab] OR tumor[tiab] OR tumors[tiab] OR tumour[tiab] OR tumours[tiab] OR malig*[tiab])) OR esophagectom*[tiab])) AND (“Lymph Nodes”[Mesh] OR “Lymphatic Metastasis”[Mesh] OR ((lymph[tiab] OR lymphatic[tiab]) AND (node*[tiab] OR nodal[tiab] OR metastas*[tiab])))))) AND ((“Neoplasm Staging”[Mesh] OR staging[tiab] OR TNM[tiab] OR number[tiab] OR extent[tiab] OR extended[tiab] OR scoring[tiab] OR score[tiab] OR classif*[tiab] OR categor*[tiab] OR criteria[tiab] OR 2-field*[tiab] OR two-field*[tiab] OR 3-field*[tiab] OR three-field*[tiab] OR node status[tiab] OR nodal status[tiab] OR D1[tiab] OR D2[tiab] OR N0[tiab] OR N1[tiab] OR N2[tiab] OR N3[tiab] OR pattern*[tiab] OR drainage[tiab] OR spread[tiab] OR pathway*[tiab] OR depth[tiab])))) NOT ((express*[ti] OR overexpress*[ti] OR gene[ti] OR genes[ti] OR protein*[ti] OR p53[ti] OR serum[ti] OR (case[ti] AND report[ti]))) NOT (Animals[Mesh] NOT Humans[Mesh])) AND (english[la] OR dutch[la])))) | 4106 |
| # | Searches | Results |
|---|---|---|
| 1 | exp esophagus tumor/or esophagus resection/or esophagectom*.ti,ab,kw. or ((esophagus or esophageal or esophagogastric or oesophagus or oesophageal or oesophagogastric or gastroesophag* or gastrooesophag*) and (neoplas* or cancer* or carcino* or adenocarcino* or tumor or tumors or tumour or tumours or malig*)).ti,ab,kw. | 127708 |
| 2 | (exp lymph node/or exp lymph node metastasis/or ((lymph or lymphatic) and (node* or nodal or metastas*)).ti,ab,kw.) and (cancer staging/or (staging or TNM or number or extent or extended or scoring or score or classif* or categor* or criteria or 2-field* or two-field* or 3-field* or three-field* or node status or nodal status or D1 or D2 or N0 or N1 or N2 or N3 or pattern* or drainage or spread or pathway* or depth).ti,ab,kw.) | 208651 |
| 3 | 1 and 2 | 10765 |
| 4 | (express* or overexpress* or gene or genes or protein* or p53 or serum or (case and report)).ti. | 2592018 |
| 5 | animal/ not human/ | 1423187 |
| 6 | conference abstract.pt. or conference paper/ or letter/ | 4893909 |
| 7 | 3 not 4 not 5 not 6 | 6444 |
| 8 | limit 7 to (dutch or english) | 5195 |
References
- Mariette, C.; Piessen, G.; Briez, N.; Triboulet, J.P. The Number of Metastatic Lymph Nodes and the Ratio Between Metastatic and Examined Lymph Nodes Are Independent Prognostic Factors in Esophageal Cancer Regardless of Neoadjuvant Chemoradiation or Lymphadenectomy Extent. Ann. Surg. 2008, 247, 365–371. [Google Scholar] [CrossRef] [PubMed]
- O’Riordan, J.M.; Rowley, S.; Murphy, J.O.; Ravi, N.; Byrne, P.J.; Reynolds, J.V. Impact of solitary involved lymph node on outcome in localized cancer of the esophagus and esophagogastric junction. J. Gastrointest. Surg. 2007, 11, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Okholm, C.; Svendsen, L.B.; Achiam, M.P. Status and prognosis of lymph node metastasis in patients with cardia cancer—A systematic review. Surg. Oncol. 2014, 23, 140–146. [Google Scholar] [CrossRef]
- Koenig, A.M.; Prenzel, K.L.; Bogoevski, D.; Yekebas, E.F.; Bubenheim, M.; Faithova, L.; Vashist, Y.K.; Gawad, K.A.; Baldus, S.E.; Schneider, P.M.; et al. Strong impact of micrometastatic tumor cell load in patients with esophageal carcinoma. Ann. Surg. Oncol. 2009, 16, 454–462. [Google Scholar] [CrossRef] [PubMed]
- Smit, J.K.; Pultrum, B.B.; van Dullemen, H.M.; Van Dam, G.M.; Groen, H.; Plukker, J.T.M. Prognostic factors and patterns of recurrence in esophageal cancer assert arguments for extended two-field transthoracic esophagectomy. Am. J. Surg. 2010, 200, 446–453. [Google Scholar] [CrossRef]
- Phillips, A.W.; Lagarde, S.M.; Navidi, M.; Disep, B.; Griffin, S.M. Impact of extent of lymphadenectomy on survival, post neoadjuvant chemotherapy and trans-thoracic esophagectomy. Ann Surg. 2016, 265, 750–756. [Google Scholar] [CrossRef]
- Castoro, C.; Scarpa, M.; Cagol, M.; Ruol, A.; Cavallin, F.; Alfieri, R.; Zanchettin, G.; Rugge, M.; Ancona, E. Nodal Metastasis From Locally Advanced Esophageal Cancer: How Neoadjuvant Therapy Modifies Their Frequency and Distribution. Ann. Surg. Oncol. 2011, 18, 3743–3754. [Google Scholar] [CrossRef]
- Sharma, D.; Thakur, A.; Toppo, S.; Chandrakar, S.K. Lymph node counts in indians in relation to lymphadenectomy for carcinoma of the oesophagus and stomach. Asian J. Surg. 2005, 28, 116–120. [Google Scholar] [CrossRef][Green Version]
- Mizutani, M.; Murakami, G.; Nawata, S.I.; Hitrai, I.; Kimura, W. Anatomy of right recurrent nerve node: Why does early metastasis of esophageal cancer occur in it? Surg. Radiol. Anat. 2006, 28, 333–338. [Google Scholar] [CrossRef]
- Prenzel, K.L.; Bollschweiler, E.; Schröder, W.; Mönig, S.P.; Drebber, U.; Vallboehmer, D.; Hölscher, A.H. Prognostic relevance of skip metastases in esophageal cancer. Ann. Thorac. Surg. 2010, 90, 1662–1667. [Google Scholar] [CrossRef]
- Liu, J.; Liu, Q.; Wang, Y.; Xia, Z.; Zhao, G. Nodal skip metastasis is associated with a relatively poor prognosis in thoracic esophageal squamous cell carcinoma. Eur. J. Surg. Oncol. 2016, 42, 1202–1205. [Google Scholar] [CrossRef] [PubMed]
- Akutsu, Y.; Matsubara, H. Lymph node dissection for esophageal cancer. Gen. Thorac. Cardiovasc. Surg. 2013, 61, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Mariette, C.; Piessen, G. Oesophageal cancer: How radical should surgery be? Eur. J. Surg. Oncol. 2012, 38, 210–213. [Google Scholar] [CrossRef]
- Japanese Esophageal Sociey. Japanese Classification of Esophageal Cancer, 11th Edition: Part I. Esophagus 2017, 14, 1–36. [Google Scholar] [CrossRef] [PubMed]
- Rice, T.W.; Patil, D.T.; Blackstone, E.H. AJCC/UICC staging of cancers of the esophagus and esophagogastric junction: Application to clinical practice. Ann. Cardiothorac. Surg. 2017, 6, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Ye, T.; Sun, Y.; Zhang, Y.; Zhang, Y.; Chen, H. Three-field or two-field resection for thoracic esophageal cancer: A meta-analysis. Ann. Thorac. Surg. 2013, 96, 1933–1941. [Google Scholar] [CrossRef]
- van Rijswijk, A.S.; Hagens, E.R.C.; van der Peet, D.L.; van Berge Henegouwen, M.I.; Gisbertz, S.S. Differences in Esophageal Cancer Surgery in Terms of Surgical Approach and Extent of Lymphadenectomy: Findings of an International Survey. Ann. Surg. Oncol. 2019, 26, 2063–2072. [Google Scholar] [CrossRef]
- Willaert, W.; Mareel, M.; Van De Putte, D.; Van Nieuwenhove, Y.; Pattyn, P.; Ceelen, W. Lymphatic spread, nodal count and the extent of lymphadenectomy in cancer of the colon. Cancer Treat. Rev. 2014, 40, 405–413. [Google Scholar] [CrossRef]
- Salhab, M.; Patani, N.; Mokbel, K. Sentinel lymph node micrometastasis in human breast cancer: An update. Surg. Oncol. 2011, 20, e195–e206. [Google Scholar] [CrossRef]
- Nappo, G.; Perinel, J.; El Bechwaty, M.; Adham, M. The standardization of pancreatoduodenectomy where are we? Pancreas 2016, 45, 493–502. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (Minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Sharma, S.; Fujita, H.; Yamana, H.; Kakegawa, T. Patterns of lymph node metastasis in 3-field dissection for carcinoma in the thoracic esophagus. Surg. Today 1994, 24, 410–414. [Google Scholar] [CrossRef] [PubMed]
- Van De Ven, C.; De Leyn, P.; Coosemans, W.; Van Raemdonck, D.; Lerut, T. Three-field lymphadenectomy and pattern of lymph node spread in T3 adenocarcinoma of the distal esophagus and the gastro-esophageal junction. Eur. J. Cardio Thorac. Surg. 1999, 15, 769–773. [Google Scholar] [CrossRef]
- Igaki, H.; Kato, H.; Tachimori, Y.; Sato, H. Prognostic evaluation for squamous cell carcinomas of the lower thoracic esophagus treated with three-field lymph node dissection. Eur. J. Cardiothorac. Surg. 2001, 19, 887–893. [Google Scholar] [CrossRef]
- Dresner, S.M.; Lamb, P.J.; Bennett, M.K.; Hayes, N.; Griffin, S.M. The pattern of metastatic lymph node dissemination from adenocarcinoma of the esophagogastric junction. Surgery 2001, 129, 103–109. [Google Scholar] [CrossRef]
- Chen, J.; Liu, S.; Pan, J.; Zheng, X.; Zhu, K.; Zhu, J.; Xiao, J.; Ying, M. The pattern and prevalence of lymphatic spread in thoracic oesophageal squamous cell carcinoma. Eur. J. Cardiothorac. Surg. 2009, 36, 480–486. [Google Scholar] [CrossRef] [PubMed]
- Tachimori, Y.; Nagai, Y.; Kanamori, N.; Hokamura, N.; Igaki, H. Pattern of lymph node metastases of esophageal squamous cell carcinoma based on the anatomical lymphatic drainage system. Dis. Esophagus 2011, 24, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Yang, S.; Zhang, Y.; Xiang, J.; Chen, H. Thoracic recurrent laryngeal lymph node metastases predict cervical node metastases and benefit from three-field dissection in selected patients with thoracic esophageal squamous cell carcinoma. J. Surg. Oncol. 2012, 105, 548–552. [Google Scholar] [CrossRef] [PubMed]
- Kosugi, S.I.; Kawaguchi, Y.; Kanda, T.; Ishikawa, T.; Sakamoto, K.; Akaike, H.; Fujii, H.; Wakai, T. Cervical lymph node dissection for clinically submucosal carcinoma of the thoracic esophagus. Ann. Surg. Oncol. 2013, 20, 4016–4021. [Google Scholar] [CrossRef]
- Cheng, J.; Kong, L.; Huang, W.; Li, B.; Li, H.; Wang, Z.; Zhang, J.; Zhou, T.; Sun, H. Explore the radiotherapeutic clinical target volume delineation for thoracic esophageal squamous cell carcinoma from the pattern of lymphatic metastases. J. Thorac. Oncol. 2013, 8, 359–365. [Google Scholar] [CrossRef]
- Lin, Z.; Chen, W.; Chen, Y.; Peng, X.; Zhu, K.; Lin, Y.; Lin, Q.; Hu, Z. A new classification of lymph node metastases according to the lymph node stations for predicting prognosis in surgical patients with esophageal squamous cell carcinoma. Oncotarget 2016, 7, 76261–76273. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Guan, H.; Huang, W.; Zhang, Z.; Zhao, D.; Liu, Y.; Zhou, T.; Li, B. Precise delineation of clinical target volume for crossing-segments thoracic esophageal squamous cell carcinoma based on the pattern of lymph node metastases. J. Thorac. Dis. 2015, 7, 2313–2320. [Google Scholar] [CrossRef] [PubMed]
- Duan, X.-F.; Tang, P.; Shang, X.-B.; Jiang, H.-J.; Yu, Z.-T. The prevalence of lymph node metastasis for pathological T1 esophageal cancer: A retrospective study of 143 cases. Surg. Oncol. 2018, 27, 1–6. [Google Scholar] [CrossRef]
- Park, S.Y.; Suh, J.W.; Kim, D.J.; Park, J.C.; Kim, E.H.; Lee, C.Y.; Lee, J.G.; Paik, H.C.; Chung, K.Y. Near-Infrared Lymphatic Mapping of the Recurrent Laryngeal Nerve Nodes in T1 Esophageal Cancer. Ann. Thorac. Surg. 2018, 105, 1613–1620. [Google Scholar] [CrossRef] [PubMed]
- Pedrazzani, C.; de Manzoni, G.; Marrelli, D.; Giacopuzzi, S.; Corso, G.; Minicozzi, A.M.; Rampone, B.; Roviello, F. Lymph node involvement in advanced gastroesophageal junction adenocarcinoma. J. Thorac. Cardiovasc. Surg. 2007, 134, 378–385. [Google Scholar] [CrossRef]
- Gertler, R.; Stein, H.J.; Schuster, T.; Rondak, I.-C.; Hofler, H.; Feith, M. Prevalence and topography of lymph node metastases in early esophageal and gastric cancer. Ann. Surg. 2014, 259, 96–101. [Google Scholar] [CrossRef]
- Künzli, H.T.; van Berge Henegouwen, M.I.; Gisbertz, S.S.; van Esser, S.; Meijer, S.L.; Bennink, R.J.; Wiezer, M.J.; Seldenrijk, C.A.; Bergman, J.J.G.H.M.; Weusten, B.L.A.M.; et al. Pilot-study on the feasibility of sentinel node navigation surgery in combination with thoracolaparoscopic lymphadenectomy without esophagectomy in early esophageal adenocarcinoma patients. Dis. Esophagus 2017, 30, 1–8. [Google Scholar] [CrossRef]
- Management, C. Anatomy of lymphatic drainage of the esophagus and lymph node metastasis of thoracic esophageal cancer. Cancer Manag. Res. 2018, 10, 6295–6303. [Google Scholar]
- Murakami, G.; Sato, I.; Shimada, K.; Dong, C.; Kato, Y.; Imazeki, T. Direct lymphatic drainage from the esophagus into the thoracic duct. Surg. Radiol. Anat. 1994, 16, 399–407. [Google Scholar] [CrossRef]
- Akiyama, H.; Tsurumaru, M.; Udagawa, H.; Kajiyama, Y. Radical lymph node dissection for cancer of the thoracic esophagus. Ann. Surg. 1994, 220, 363–364. [Google Scholar] [CrossRef]
- Wang, F.; Zheng, Y.; Wang, Z.; Zheng, Q.; Huang, Q.; Liu, S. Nodal Skip Metastasis in Esophageal Squamous Cell Carcinoma Patients Undergoing Three-Field Lymphadenectomy. Ann. Thorac. Surg. 2017, 104, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- He, S.-L.; Yang, Y.-S.; Wang, W.-P.; Zhang, H.-L.; Wang, Y.-C.; Chen, L.-Q. Prognostic Evaluation of Nodal Skip Metastasis for Thoracic Esophageal Squamous Cell Carcinoma. Ann. Thorac. Surg. 2019, 108, 1717–1723. [Google Scholar] [CrossRef] [PubMed]
- Kumakura, Y.; Yokobori, T.; Yoshida, T.; Hara, K.; Sakai, M.; Sohda, M.; Miyazaki, T.; Yokoo, H.; Handa, T.; Yorifuji, H.; et al. Elucidation of the Anatomical Mechanism of Nodal Skip Metastasis in Superficial Thoracic Esophageal Squamous Cell Carcinoma. Ann. Surg. Oncol. 2018, 25, 1221–1228. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.; Kim, H.K.; Choi, Y.S.; Kim, K.; Shim, Y.M. Clinical stage T1-T2N0M0 oesophageal cancer: Accuracy of clinical staging and predictive factors for lymph node metastasis. Eur. J. Cardiothorac. Surg. 2014, 46, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Talsma, A.K.; Shapiro, J.; Looman, C.W.; van Hagen, P.; Steyerberg, E.W.; van der Gaast, A.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.L.; van Lanschot, J.J.B.; CROSS Study Group. Lymph node retrieval during esophagectomy with and without neoadjuvant chemoradiotherapy: Prognostic and therapeutic impact on survival. Ann. Surg. 2014, 260, 783–786. [Google Scholar] [CrossRef] [PubMed]
- Hagens, E.R.C.; Künzli, H.T.; van Rijswijk, A.S.; Meijer, S.L.; Mijnals, R.C.D.; Weusten, B.L.; Geijsen, E.D.; van Laarhoven, H.W.M.; van Berge Henegouwen, M.I.; Gisbertz, S.S. Distribution of lymph node metastases in esophageal adenocarcinoma after neoadjuvant chemoradiation therapy: A prospective study. Surg. Endosc. 2019. [Google Scholar] [CrossRef]
- Ma, J.B.; Song, Y.P.; Yu, J.M.; Zhou, W.; Cheng, E.C.; Zhang, X.Q.; Kong, L. Feasibility of involved-field conformal radiotherapy for cervical and upper-thoracic esophageal cancer. Oncol. Res. Treat. 2011, 34, 599–604. [Google Scholar] [CrossRef]
- Huang, W.; Li, B.; Gong, H.; Yu, J.; Sun, H.; Zhou, T.; Zhang, Z.; Liu, X. Pattern of lymph node metastases and its implication in radiotherapeutic clinical target volume in patients with thoracic esophageal squamous cell carcinoma: A report of 1077 cases. Radiother. Oncol. 2010, 95, 229–233. [Google Scholar] [CrossRef]
- Zhang, J.; Liu, Y.; Che, F.; Luo, Y.; Huang, W.; Heng, X.; Li, B. Pattern of lymph node metastasis in thoracic esophageal squamous cell carcinoma with poor differentiation. Mol. Clin. Oncol. 2018, 8, 760–766. [Google Scholar] [CrossRef]
- Hagens, E.R.C.; van Berge Henegouwen, M.I.; Van Sandick, J.W.; Cuesta, M.A.; Van Der Peet, D.L.; Heisterkamp, J.; Nieuwenhuijzen, G.A.P.; Rosman, C.; Scheepers, J.J.G.; Van Hillegersberg, R.; et al. Distribution of lymph node metastases in esophageal carcinoma [TIGER study]: Study protocol of a multinational observational study. BMC Cancer 2019, 19, 662. [Google Scholar] [CrossRef]


| Node Region | Station Number (JES) | Name of Station (JES) | Station Number (AJCC) | Name of Node Station (AJCC) |
|---|---|---|---|---|
| Cervical | 104R | Right supraclavicular lymph nodes | ||
| 104L | Left supraclavicular lymph nodes | |||
| 101R | Right cervical paraesophageal lymph nodes | 1R | Right lower cervical paratracheal lymph nodes | |
| 101L | Left cervical paraesophageal lymph nodes | 1L | Left lower cervical paratracheal lymph nodes | |
| 102 | Deep cervical lymph nodes | |||
| 103 | Peripharyngeal lymph nodes | |||
| Upper mediastinal | 105 | Upper thoracic paraesophageal lymph nodes | 8up | Posterior mediastinal lymph nodes |
| 106preR | Right pretracheal lymph nodes | |||
| 106preL | Left pretracheal lymph nodes | |||
| 106recR | Right recurrent nerve lymph nodes | 2R | Right and left upper paratracheal nodes (including lymph nodes along the recurrent laryngeal nerve and the cervical paratracheal lymph nodes) | |
| 106recL | Left recurrent nerve lymph nodes | 2L + 4L | Left upper paratracheal nodes + Left lower paratrachal lymph nodes | |
| 106tbR | Right tracheobronchial lymph nodes | Right lower paratrachal lymph nodes | ||
| 106tbL | Left tracheobronchial lymph nodes | 4L | Left lower paratrachal lymph nodes | |
| Middle mediastinal | 107 | Subcarinal lymph nodes | 7 | Subcarinal lymph nodes |
| 108 | Middle thoracic paraesophageal lymph nodes | 8M | Middle thoracic paraesophageal lymph nodes | |
| 109R | Right main bronchus lymph nodes | 7 | Subcarinal lymph nodes | |
| 109L | Left main bronchus lymph nodes | 7 | Subcarinal lymph nodes | |
| Lower mediastinal | 110 | Lower thoracic paraesophageal lymph nodes | 8Lo | Lower thoracic paraesophageal lymph nodes |
| 111 | Supradiaphragmatic lymph nodes | 15 | Diaphragmatic lymph nodes | |
| 112 | Posterior mediastinal lymph nodes | 9 | Pulmonary ligament lymph nodes | |
| Abdominal lymph node stations | 1 | Right paracardial lymph nodes | 16 | Paracardial lymph nodes |
| 2 | Left paracardial lymph nodes | 16 | Paracardial lymph nodes | |
| 3 | Lesser curvature lymph nodes | 17 | Lymph nodes along the left gastric artery | |
| 4 | Lymph nodes along the greater curvature | |||
| 7 | Lymph nodes along the left gastric artery | 17 | Lymph nodes along the left gastric artery | |
| 9 | Celiac lymph nodes | 20 | Celiac lymph nodes | |
| 8 | Lymph nodes along the common hepatic artery | 18 | Lymph nodes along the common hepatic artery | |
| 11 | Splenic artery lymph nodes | 19 | Splenic artery lymph nodes | |
| 19 | Infradiaphragmatic lymph nodes | 16 | Paracardial lymph nodes |
| No | First Author | Year of Publication | Study Design | Country | Number of Patients | Inclusion Period | 2- or 3-Field Lymphadenectomy | Lymph Node Classification System Used | Use of Immunohistochemistry Staining | MINORS Score | How Detailed Are the Locations of Lymph Node Metastases Described? | How Are the Locations of Nodal Metastases Reported? |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | S. Sharma [22] | 1994 | Retrospective study | Japan | 70 | 1985–1991 | 3-field | No standard classification used | NR | 10 | Description of several stations in cervical, thoracic, and abdominal regions. | Number of patients with resected and positive lymph nodes reported per station. |
| 2 | C. van de Ven [23] | 1999 | Prospective observational study | Belgium | 37 | 1994–1998 | 3-field | No standard classification used | NR | 11 | Description of several stations in cervical, thoracic, and abdominal regions. | Number of patients with resected and positive lymph nodes reported per region. |
| 3 | H. Igaki [24] | 2001 | Retrospective study | Japan | 96 | 1986–1998 | 3-field | No standard classification used | NR | 8 | No description of stations. Cervical, upper mediastinal, middle mediastinal, lower mediastinal, perigastric, and celiac regions described. | Number of patients with resected and positive lymph nodes reported per region. Numbers per station were not provided. |
| 4 | S.M. Dresner [25] | 2001 | Retrospective study | United Kingdom | 104 | 1996–1999 | 2-field | No standard classification used | NR | 10 | Description of stations in lower thoracic and abdominal regions. | Number of patients with resected and positive lymph nodes reported for the abdominal region. Numbers per station were not provided. |
| 5 | J. Chen [26] | 2009 | Retrospective study | China | 1850 | 1993–2006 | 3-field | JES | H&E | 12 | Description of stations according to JES in cervical, upper mediational, middle mediastinal, lower mediastinal and abdominal region. | Number of patients with resected and positive lymph nodes reported per region and station. |
| 6 | Y. Tachimori [27] | 2011 | Retrospective study | Japan | 356 | 2001–2005 | 3-field | No standard classification used | NR | 10 | No description of stations. Cervical, upper mediastinal, middle mediastinal, lower mediastinal, perigastric and celiac regions described. | Number of patients with resected and positive lymph nodes reported per region. Numbers per station were not provided. |
| 7 | C. Castoro [7] | 2011 | Retrospective study | Italy | 248 | 1992–2007 | 2-field and 3-field | No standard classification used | H&E and PAS | 11 | Description of stations in cervical, thoracic and abdominal regions. | Number of patients with resected and positive lymph nodes reported per station.* |
| 8 | H. Li [28] | 2012 | Retrospective study | China | 200 | 2000–2010 | 3-field | No standard classification used | H&E | 11 | No description of stations. Cervical, mediastinal, recurrent laryngeal nerve and abdominal regions described. | Number of patients with resected and positive lymph nodes reported per region and the recurrent laryngeal nerve station. |
| 9 | S. Kosugi [29] | 2013 | Retrospective study | Japan | 86 | 1992–2011 | 3-field | JES | NR | 11 | Description of stations according to JES in cervical, upper mediational, middle mediastinal, lower mediastinal, perigastric, and suprapancreatic regions. | Number of patients with resected and positive lymph nodes reported per station. |
| 10 | J. Cheng [30] | 2013 | Retrospective study | China | 1893 | 2003–2011 | 2-field and 3-field | JES | H&E | 9 | Description of stations according to JES in cervical, upper mediational, middle mediastinal, lower mediastinal, and abdominal region. | Number of patients with resected and positive lymph nodes reported per region and per a selected number of stations. |
| 11 | Z. Lin [31] | 2016 | Prospective observational study | China | 260 | 2009–2013 | 3-field | AJCC | H&E | 13 | Description of stations according to AJCC in the thoracic and abdominal region. | Number of patients with resected and positive lymph nodes reported per station. |
| 12 | Y. Dong [32] | 2015 | Retrospective study | China | 3587 | 2000–2014 | 2-field and 3-field | JES | NR | 10 | Description of stations according to JES in the cervical, upper mediastinal, middle mediastinal, lower mediastinal, and abdominal regions. | Number of patients with resected and positive lymph nodes reported per region. Numbers per station were not provided.* |
| 13 | X. Duan [33] | 2017 | Retrospective study | China | 136 | 2014–2016 | 2-field and 3-field | No standard classification used | NR | 11 | Description of stations in thoracic and abdominal regions. | Number of patients with resected and positive lymph nodes reported per station. |
| 14 | S. Park [34] | 2018 | Prospective observational study | Korea | 29 | 2014–2018 | 3-field | JES | H&E | 10 | Description of stations according to JES in the cervical, upper mediastinal, middle mediastinal, lower mediastinal, and abdominal regions. | Number of patients with resected and positive lymph nodes reported per station. |
| No | First Author | Sex, Male n (%) | Age, in years | Histology | T-Stage *, n (%) | N-Stage *, n (%) | Location of the Tumor, n (%) | Surgical Approach | Number of Dissected Lymph Nodes per Patient | Percentage of Patients with Lymph Node Metastases | Overall Percentage of Positive Lymph Nodes |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | S. Sharma [22] | 62 (89) | mean 58.5 | SCC | pT1 11 (16) pT2 12 (17) pT3 46 (65) pT5 1 (2) | pN0 20 (29) pN1 50 (71) | UTE 10 (14) MTE 37 (53) LTE 23 (33) | Open procedures | mean 82 | 71% (50/70) | 4% (208/5720) |
| 2 | C. van de Ven [23] | NR | NR | AC | cT3 | NR | LTE 17 (46) GEJ 20 (54) | Open procedures | mean 60, SD 17 | NR | 14% (323/2240) |
| 3 | H. Igaki [24] | 85 (97) | mean 62 [range 42–86] | SCC | pT1 27 (28) pT2 16 (16) pT3 53 (56) | pN0 36 (38) pN1 60 (62) | LTE | Open procedures | NR | 66% (63/96) | NR |
| 4 | S.M. Dresner [25] | 91 (88) | mean 63 [range 30–78] | AC | NR | NR | GEJ | Open procedures | median 22 [range 11–57] | 70% (73/104) | 21% (508/2476) |
| 5 | J. Chen [26] | 1351 (73) | median 55 [range 27–54] | SCC | cT1 109 (6) cT2 348 (19) cT3 1215 (65) cT4 178 (10) | NR | UTE 289 (16) MTE 1381 (74) LTE 180 (10) | Open procedures | mean 26 [range 15–71] | 58% (1081/1850) | 9% (4350/47470) |
| 6 | Y. Tachimori [27] | 314 (88) | mean 63 [range 41–80] | SCC | pT1 127 (36) pT2 40 (11) pT3 183 (51) pT4 6 (2) | pN0 110 (31) pN1 116 (33) pN2 81 (23) pN3 49 (13) | UTE 55 (15) MTE 173 (49) LTE 128 (36) | Open procedures | NR | NR | NR |
| 6 | C. Castoro [7] | 327 (81) | median 63 [IQR 56–70] | SCC 116 (47) AC 132 (53) | cT1 5 (2) cT2 42 (17) cT3 201 (81) | cN0 107 (43) cN1 141 (57) | UTE (all SCC) 25 (10) MTE (all SCC) 50 (20) LTE (AC 15, SCC 41) 56 (23) GEJ (all AC) 117 (47) | Open procedures | AC median 19.5 [IQR 15–27] SCC median 16 [IQR 12–21] | AC 54% (63/116) SCC 67% (88/132) | NR |
| 8 | H. Li [28] | 163 (82) | mean 57, SD 9 | SCC | pT1 18 (9) pT2 45 (23) pT3 114 (56) pT4 23 (12) | NR | UTE 31 (15) MTE 137 (69) LTE 32 (16) | Open procedures | NR | NR | NR |
| 9 | S. Kosugi [29] | 78 (91) | mean 60, SD 7 | SCC | pT1a 7 (8) pT1b 75 (87) pT2 4 (5) | pN0 48 (56) pN1 31 (36) pN2 6 (7) pN3 1 (1) | UTE 17 (20) MTE 59 (69) LTE 10 (11) | Open procedures | NR | 47% (40/86) | NR |
| 10 | J. Cheng [30] | 1474 (78) | < 40: 1% 41–59: 48% ≥60: 51% | SCC | cTis 10 (1) cT1 103 (5) cT2 345 (18) cT4 1173 (62) cT4 262 (14) | NR | UTE 82 (4) MTE 1266 (67) LTE 545 (29) | Open procedures | mean 13 | 46% (865/1893) | NR |
| 11 | Z. Lin [31] | 59 (23) | median 61 [IQR 52–67] | SCC | pT1 30 (11) pT2 44 (17) pT3 164 (63) pT4 22 (9) | pN0 119 (46) pN1 67 (25) pN2 54 (21) pN3 20 (8) | UTE 28 (11) MTE 173 (67) LTE 59 (22) | Open procedures | median 35 [IQR 25–46] | 54% (141/260) | 15% (316/2097) |
| 12 | Y. Dong [32] | 2536 (72) | median 61 | SCC | pT1 435 (14) pT2 935 (25) pT3 1992 (55) pT4 225 (6) | pN0 2223 (62) pN1 1233 (34) pN2 98 (3) pN3 33 (1) | UTE 189 (5) MTE 1837 (51) LTE 1561 (44) | Hybrid procedures | mean 20 [range 16–50] | 38% (1.364/3587) | 4% (2870/71740) |
| 13 | X. Duan [33] | 128 (95) | mean 63, SD 9 | AC | pT1-2 17 (13) pT3-4 119 (87) | pN0 44 (32) pN1 64 (47) pN2 21 (15) pN3 7 (6) | GEJ | Open procedures | mean 15 | 68% (92/136) | 21% (431/2083) |
| 14 | S. Park [34] | 26 (90) | mean 63, SD 7 | SCC | cT1 | cN0 25 (86) cN1 4 (14) | MTE 17 (59) LTE 12 (41) | Robot-assisted procedures | mean 55, SD 17 | 86% (25/29) | NR |
| Lymph Node Station | Squamous Cell Carcinoma | Adenocarcinoma | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Upper Thoracic Esophagus | Middle Thoracic Esophagus | Lower Thoracic Esophagus | Gastroesophageal Junction | |||||||||||||
| Cervical region | ||||||||||||||||
| Right supraclavicular lymph nodes | 9% | 34 | / | 381 | 10% | 266 | / | 2684 | 13% | 100 | / | 748 | NR | |||
| Left supraclavicular lymph nodes | 5% | 14 | / | 299 | 5% | 67 | / | 1418 | 3% | 6 | / | 203 | NR | |||
| Right cervical paraesophageal lymph nodes | 34% | 103 | / | 299 | 24% | 345 | / | 1418 | 10% | 20 | / | 203 | NR | |||
| Left cervical paraesophageal lymph nodes | 22% | 65 | / | 299 | 11% | 152 | / | 1418 | 4% | 8 | / | 203 | NR | |||
| Right deep cervical lymph nodes | 2% | 5 | / | 289 | <1% | 4 | / | 1381 | 0% | 0 | / | 180 | NR | |||
| Left deep cervical lymph nodes | 2% | 5 | / | 289 | 1% | 8 | / | 1381 | 0% | 0 | / | 180 | NR | |||
| Peripharyngeal lymph nodes | 1% | 2 | / | 289 | <1% | 1 | / | 1381 | 0% | 0 | / | 180 | NR | |||
| Upper mediastinal region | ||||||||||||||||
| Upper thoracic paraesophageal lymph nodes | 10% | 40 | / | 388 | 6% | 163 | / | 2811 | 3% | 7 | / | 214 | NR | |||
| Right pretracheal lymph nodes | 12% | 43 | / | 371 | 6% | 81 | / | 1381 | 2% | 3 | / | 180 | NR | |||
| Left pretracheal lymph nodes | 9% | 28 | / | 299 | 7% | 101 | / | 1418 | 2% | 4 | / | 203 | NR | |||
| Right recurrent nerve lymph nodes | 60% | 6 | / | 10 | 23% | 15 | / | 66 | 15% | 8 | / | 52 | NR | |||
| Left recurrent nerve lymph nodes | 11% | 32 | / | 289 | 7% | 102 | / | 1410 | 3% | 7 | / | 209 | NR | |||
| Tracheobronchial lymph nodes | 12% | 10 | / | 82 | 12% | 17 | / | 145 | 6% | 3 | / | 49 | NR | |||
| Middle mediastinal region | ||||||||||||||||
| Subcarinal lymph nodes | 8% | 32 | / | 398 | 18% | 517 | / | 2913 | 14% | 121 | / | 836 | 25% | 1 | / | 4 |
| Middle thoracic paraesophageal lymph nodes | 5% | 20 | / | 388 | 23% | 595 | / | 2542 | 21% | 170 | / | 804 | 2% | 1 | / | 45 |
| Right main bronchus lymph nodes | <1% | 1 | / | 289 | 2% | 24 | / | 1410 | 2% | 4 | / | 209 | 0% | 0 | / | 10 |
| Left main bronchus lymph nodes | 1% | 2 | / | 289 | 3% | 37 | / | 1410 | 2% | 5 | / | 209 | 6% | 2 | / | 31 |
| Lower mediastinal region | ||||||||||||||||
| Lower thoracic paraesophageal lymph nodes | 3% | 12 | / | 388 | 8% | 221 | / | 2851 | 23% | 184 | / | 809 | 10% | 10 | / | 96 |
| Supradiaphragmatic lymph nodes | 0% | 0 | / | 306 | <1% | 3 | / | 1504 | 5% | 39 | / | 778 | 0% | 0 | / | 5 |
| Posterior mediastinal lymph nodes | 3% | 10 | / | 316 | 7% | 102 | / | 1545 | 5% | 14 | / | 259 | 0% | 0 | / | 17 |
| Abdominal region | ||||||||||||||||
| Right paracardial lymph nodes | 1% | 2 | / | 199 | 3% | 48 | / | 1447 | 12% | 27 | / | 232 | 26% | 33 | / | 128 |
| Left paracardial lymph nodes | 3% | 10 | / | 299 | 7% | 201 | / | 2684 | 13% | 97 | / | 748 | 37% | 48 | / | 131 |
| Lesser curvature lymph nodes | 3% | 9 | / | 299 | 10% | 273 | / | 2713 | 11% | 89 | / | 777 | 29% | 37 | / | 127 |
| Lymph nodes along the greater curvature | 0% | 0 | / | 289 | <1% | 1 | / | 1381 | 0% | 0 | / | 180 | 12% | 5 | / | 41 |
| Lymph nodes along the left gastric artery | 4% | 11 | / | 299 | 16% | 238 | / | 1528 | 28% | 76 | / | 269 | 48% | 29 | / | 60 |
| Celiac lymph nodes | NR | 2% | 1 | / | 56 | 3% | 1 | / | 33 | 14% | 4 | / | 29 | |||
| Lymph nodes along the common hepatic artery | <1% | 1 | / | 289 | 3% | 40 | / | 1483 | 5% | 37 | / | 774 | 14% | 5 | / | 37 |
| Splenic artery lymph nodes | NR | 2% | 1 | / | 59 | 0% | 0 | / | 31 | 26% | 11 | / | 43 | |||
| Infradiaphragmatic lymph nodes | NR | NR | NR | NR | ||||||||||||
| Subaortic lymph nodes | NR | 10% | 2 | / | 21 | 0% | 0 | / | 6 | NR | ||||||
| Para-aortic lymph nodes | NR | 10% | 1 | / | 10 | 0% | 0 | / | 3 | NR | ||||||
| Lymph Node Region | MTE | LTE | UTE | MTE | LTE | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| pT1-2 | pT2-3 | pT1-2 | pT2-3 | pT1 | pT2-4 | pT1 | pT2-4 | pT1 | pT2-4 | |
| n = 315 | n = 915 | n = 171 | n = 470 | n = 22 | n = 33 | n = 67 | n = 106 | n = 38 | n = 90 | |
| Cervical region | 3% | 5% | 2% | 3% | 14% | 21% | 12% | 25% | 0% | 6% |
| Upper mediastinal region | 3% | 6% | 2% | 5% | 55% | 85% | 22% | 61% | 13% | 27% |
| Middle mediastinal region | 18% | 38% | 9% | 19% | 5% | 9% | 6% | 49% | 5% | 23% |
| Lower mediastinal region | 2% | 3% | 27% | 39% | 0% | 9% | 9% | 25% | 5% | 27% |
| Abdominal region | 11% | 16% | 25% | 33% | NR | NR | NR | NR | NR | NR |
| Perigastric region | NR | NR | NR | NR | 0% | 6% | 24% | 54% | 39% | 66% |
| Celiac region | NR | NR | NR | NR | 0% | 9% | 3% | 5% | 0% | 9% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hagens, E.R.C.; van Berge Henegouwen, M.I.; Gisbertz, S.S. Distribution of Lymph Node Metastases in Esophageal Carcinoma Patients Undergoing Upfront Surgery: A Systematic Review. Cancers 2020, 12, 1592. https://doi.org/10.3390/cancers12061592
Hagens ERC, van Berge Henegouwen MI, Gisbertz SS. Distribution of Lymph Node Metastases in Esophageal Carcinoma Patients Undergoing Upfront Surgery: A Systematic Review. Cancers. 2020; 12(6):1592. https://doi.org/10.3390/cancers12061592
Chicago/Turabian StyleHagens, Eliza R. C., Mark I. van Berge Henegouwen, and Suzanne S. Gisbertz. 2020. "Distribution of Lymph Node Metastases in Esophageal Carcinoma Patients Undergoing Upfront Surgery: A Systematic Review" Cancers 12, no. 6: 1592. https://doi.org/10.3390/cancers12061592
APA StyleHagens, E. R. C., van Berge Henegouwen, M. I., & Gisbertz, S. S. (2020). Distribution of Lymph Node Metastases in Esophageal Carcinoma Patients Undergoing Upfront Surgery: A Systematic Review. Cancers, 12(6), 1592. https://doi.org/10.3390/cancers12061592