HPV-Induced Oropharyngeal Cancer and the Role of the E7 Oncoprotein Detection via Brush Test

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Results
2.1. Study Population
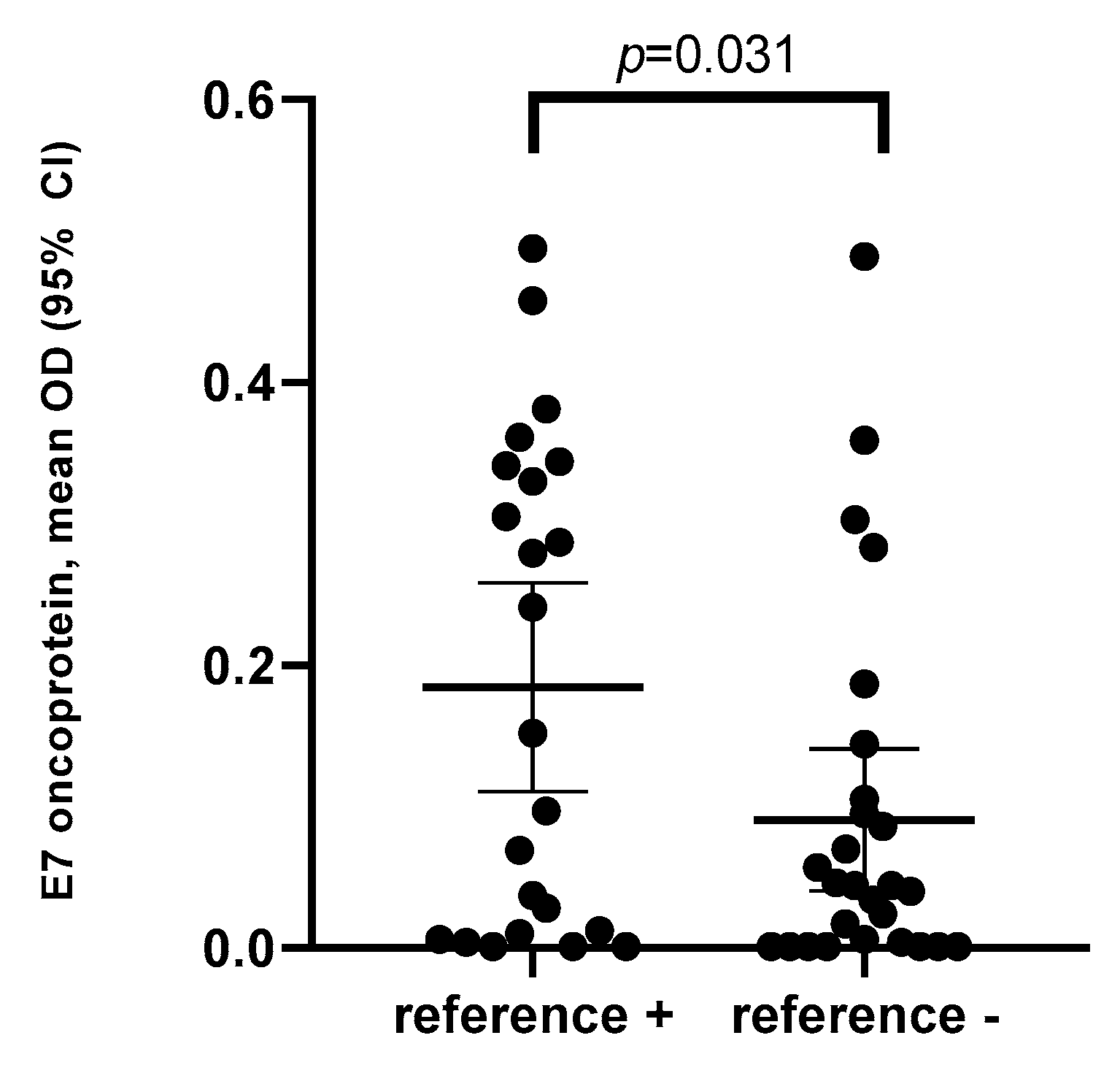
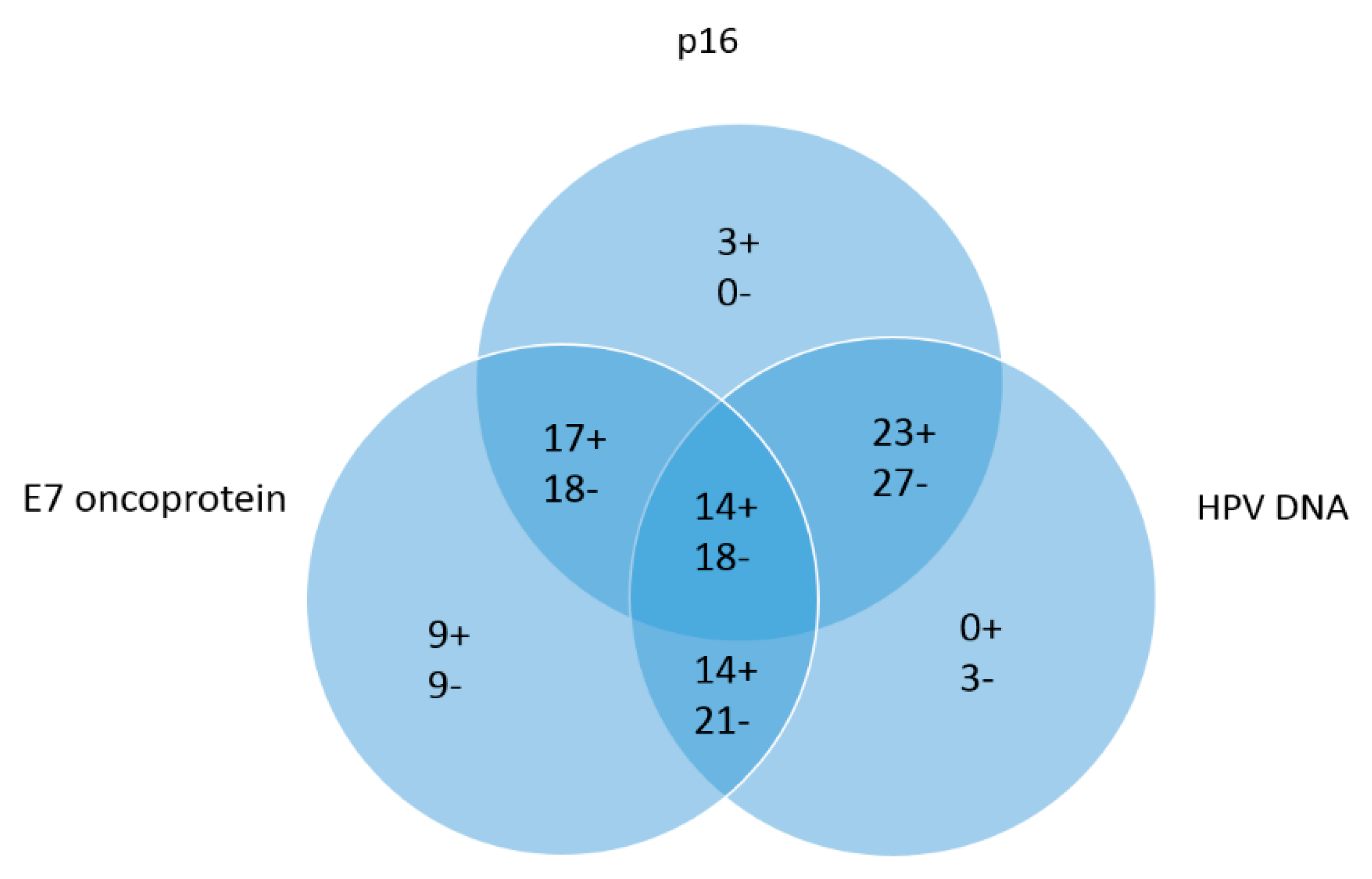
2.2. Detection of E7 Oncoprotein, HPV DNA and p16
2.3. Sensitivity, Specificity and Accuracy
3. Discussion
4. Materials and Methods
4.1. Specimen Harvest and Handling
4.2. E7 Oncoprotein Detection by Brush Test
4.3. DNA Amplification and HPV Genotyping
4.4. Immunohistochemistry
4.5. Data Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chaturvedi, A.K.; Engels, E.A.; Pfeiffer, R.M.; Hernandez, B.Y.; Xiao, W.; Kim, E.; Jiang, B.; Goodman, M.T.; Sibug-Saber, M.; Cozen, W.; et al. Human papillomavirus and rising oropharyngeal cancer incidence in the United States. J. Clin. Oncol. 2011, 29, 4294–4301. [Google Scholar] [CrossRef] [PubMed]
- Mahal, B.A.; Catalano, P.J.; Haddad, R.I.; Hanna, G.J.; Kass, J.I.; Schoenfeld, J.D.; Tishler, R.B.; Margalit, D.N. Incidence and Demographic Burden of HPV-Associated Oropharyngeal Head and Neck Cancers in the United States. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1660–1667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wittekindt, C.; Wagner, S.; Bushnak, A.; Prigge, E.S.; von Knebel Doeberitz, M.; Wurdemann, N.; Bernhardt, K.; Pons-Kuhnemann, J.; Maulbecker-Armstrong, C.; Klussmann, J.P. Increasing Incidence rates of Oropharyngeal Squamous Cell Carcinoma in Germany and Significance of Disease Burden Attributed to Human Papillomavirus. Cancer Prev. Res. (Phila) 2019, 12, 375–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahlstrom, K.R.; Bell, D.; Hanby, D.; Li, G.; Wang, L.E.; Wei, Q.; Williams, M.D.; Sturgis, E.M. Socioeconomic characteristics of patients with oropharyngeal carcinoma according to tumor HPV status, patient smoking status, and sexual behavior. Oral Oncol. 2015, 51, 832–838. [Google Scholar] [CrossRef] [Green Version]
- Sturgis, E.M.; Cinciripini, P.M. Trends in head and neck cancer incidence in relation to smoking prevalence: An emerging epidemic of human papillomavirus-associated cancers? Cancer 2007, 110, 1429–1435. [Google Scholar] [CrossRef]
- Schnelle, C.; Whiteman, D.C.; Porceddu, S.V.; Panizza, B.J.; Antonsson, A. Past sexual behaviors and risks of oropharyngeal squamous cell carcinoma: A case-case comparison. Int. J. Cancer 2017, 140, 1027–1034. [Google Scholar] [CrossRef]
- Wagner, S.; Wittekindt, C.; Sharma, S.J.; Wuerdemann, N.; Juttner, T.; Reuschenbach, M.; Prigge, E.S.; von Knebel Doeberitz, M.; Gattenlohner, S.; Burkhardt, E.; et al. Human papillomavirus association is the most important predictor for surgically treated patients with oropharyngeal cancer. Br. J. Cancer 2017, 116, 1604–1611. [Google Scholar] [CrossRef] [Green Version]
- Kofler, B.; Laban, S.; Busch, C.J.; Lorincz, B.; Knecht, R. New treatment strategies for HPV-positive head and neck cancer. Eur. Arch. Oto-Rhino-Laryngol. 2014, 271, 1861–1867. [Google Scholar] [CrossRef]
- Mirghani, H.; Bellera, C.; Delaye, J.; Dolivet, G.; Fakhry, N.; Bozec, A.; Garrel, R.; Malard, O.; Jegoux, F.; Maingon, P.; et al. Prevalence and characteristics of HPV-driven oropharyngeal cancer in France. Cancer Epidemiol. 2019, 61, 89–94. [Google Scholar] [CrossRef]
- Jung, A.C.; Briolat, J.; Millon, R.; de Reynies, A.; Rickman, D.; Thomas, E.; Abecassis, J.; Clavel, C.; Wasylyk, B. Biological and clinical relevance of transcriptionally active human papillomavirus (HPV) infection in oropharynx squamous cell carcinoma. Int. J. Cancer 2010, 126, 1882–1894. [Google Scholar] [CrossRef]
- Mena, M.; Taberna, M.; Tous, S.; Marquez, S.; Clavero, O.; Quiros, B.; Lloveras, B.; Alejo, M.; Leon, X.; Quer, M.; et al. Double positivity for HPV-DNA/p16(ink4a) is the biomarker with strongest diagnostic accuracy and prognostic value for human papillomavirus related oropharyngeal cancer patients. Oral Oncol. 2018, 78, 137–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasmussen, J.H.; Gronhoj, C.; Hakansson, K.; Friborg, J.; Andersen, E.; Lelkaitis, G.; Klussmann, J.P.; Wittekindt, C.; Wagner, S.; Vogelius, I.R.; et al. Risk profiling based on p16 and HPV DNA more accurately predicts location of disease relapse in patients with oropharyngeal squamous cell carcinoma. Ann. Oncol. 2019, 30, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Narisawa-Saito, M.; Kiyono, T. Basic mechanisms of high-risk human papillomavirus-induced carcinogenesis: Roles of E6 and E7 proteins. Cancer Sci. 2007, 98, 1505–1511. [Google Scholar] [CrossRef] [PubMed]
- zur Hausen, H. Papillomaviruses causing cancer: Evasion from host-cell control in early events in carcinogenesis. J. Natl. Cancer Inst. 2000, 92, 690–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moody, C.A.; Laimins, L.A. Human papillomavirus oncoproteins: Pathways to transformation. Nat Rev. Cancer 2010, 10, 550–560. [Google Scholar] [CrossRef]
- Gonzalez, S.L.; Stremlau, M.; He, X.; Basile, J.R.; Munger, K. Degradation of the retinoblastoma tumor suppressor by the human papillomavirus type 16 E7 oncoprotein is important for functional inactivation and is separable from proteasomal degradation of E7. J. Virol. 2001, 75, 7583–7591. [Google Scholar] [CrossRef] [Green Version]
- Agorastos, T.; Chatzistamatiou, K.; Moysiadis, T.; Kaufmann, A.M.; Skenderi, A.; Lekka, I.; Koch, I.; Soutschek, E.; Boecher, O.; Kilintzis, V.; et al. Human papillomavirus E7 protein detection as a method of triage to colposcopy of HPV positive women, in comparison to genotyping and cytology. Final results of the PIPAVIR study. Int. J. Cancer 2017, 141, 519–530. [Google Scholar] [CrossRef]
- Foster, C.C.; Seiwert, T.Y.; MacCracken, E.; Blair, E.A.; Agrawal, N.; Melotek, J.M.; Portugal, L.; Brisson, R.J.; Gooi, Z.; Spiotto, M.T.; et al. Dose and Volume De-Escalation for Human Papillomavirus-Positive Oropharyngeal Cancer is Associated with Favorable Post-Treatment Functional Outcomes. Int. J. Radiat. Oncol. Biol. Phys. 2020. [Google Scholar] [CrossRef]
- Bigelow, E.O.; Seiwert, T.Y.; Fakhry, C. Deintensification of treatment for human papillomavirus-related oropharyngeal cancer: Current state and future directions. Oral Oncol. 2020, 105, e104652. [Google Scholar] [CrossRef]
- Patel, R.R.; Ludmir, E.B.; Augustyn, A.; Zaorsky, N.G.; Lehrer, E.J.; Ryali, R.; Trifiletti, D.M.; Adeberg, S.; Amini, A.; Verma, V. De-intensification of therapy in human papillomavirus associated oropharyngeal cancer: A systematic review of prospective trials. Oral Oncol. 2020, 103, e104608. [Google Scholar] [CrossRef]
- Liang, C.; Marsit, C.J.; McClean, M.D.; Nelson, H.H.; Christensen, B.C.; Haddad, R.I.; Clark, J.R.; Wein, R.O.; Grillone, G.A.; Houseman, E.A.; et al. Biomarkers of HPV in head and neck squamous cell carcinoma. Cancer Res. 2012, 72, 5004–5013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riechelmann, H.; Neagos, A.; Netzer-Yilmaz, U.; Gronau, S.; Scheithauer, M.; Rockemann, M.G. The ASA-score as a comorbidity index in patients with cancer of the oral cavity and oropharynx. Laryngo-Rhino-Otol. 2006, 85, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Grisar, K.; Dok, R.; Schoenaers, J.; Dormaar, T.; Hauben, E.; Jorissen, M.; Nuyts, S.; Politis, C. Differences in human papillomavirus-positive and -negative head and neck cancers in Belgium: An 8-year retrospective, comparative study. Oral Surg., Oral Med. Oral Pathol. Oral Radiol. 2016, 121, 456–460. [Google Scholar] [CrossRef] [PubMed]
- Beynon, R.A.; Lang, S.; Schimansky, S.; Penfold, C.M.; Waylen, A.; Thomas, S.J.; Pawlita, M.; Waterboer, T.; Martin, R.M.; May, M.; et al. Tobacco smoking and alcohol drinking at diagnosis of head and neck cancer and all-cause mortality: Results from head and neck 5000, a prospective observational cohort of people with head and neck cancer. Int. J. Cancer 2018, 143, 1114–1127. [Google Scholar] [CrossRef] [PubMed]
- Deschler, D.G.; Richmon, J.D.; Khariwala, S.S.; Ferris, R.L.; Wang, M.B. The "new" head and neck cancer patient-young, nonsmoker, nondrinker, and HPV positive: Evaluation. Otolaryngol. Head Neck Surg. 2014, 151, 375–380. [Google Scholar] [CrossRef] [Green Version]
- Lassen, P.; Lacas, B.; Pignon, J.P.; Trotti, A.; Zackrisson, B.; Zhang, Q.; Overgaard, J.; Blanchard, P.; Group, M.C. Prognostic impact of HPV-associated p16-expression and smoking status on outcomes following radiotherapy for oropharyngeal cancer: The MARCH-HPV project. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2018, 126, 107–115. [Google Scholar] [CrossRef]
- Kaliff, M.; Karlsson, M.G.; Sorbe, B.; Bohr Mordhorst, L.; Helenius, G.; Lillsunde-Larsson, G. HPV-negative Tumors in a Swedish Cohort of Cervical Cancer. Int. J. Gynecol. Pathol. 2020, 39, 279–288. [Google Scholar] [CrossRef]
- Arroyo Muhr, L.S.; Lagheden, C.; Eklund, C.; Lei, J.; Nordqvist-Kleppe, S.; Sparen, P.; Sundstrom, K.; Dillner, J. Sequencing detects human papillomavirus in some apparently HPV-negative invasive cervical cancers. J. Gen. Virol. 2020, 101, 265–270. [Google Scholar] [CrossRef] [Green Version]
- Mills, A.M.; Dirks, D.C.; Poulter, M.D.; Mills, S.E.; Stoler, M.H. HR-HPV E6/E7 mRNA In Situ Hybridization: Validation Against PCR, DNA In Situ Hybridization, and p16 Immunohistochemistry in 102 Samples of Cervical, Vulvar, Anal, and Head and Neck Neoplasia. Am. J. Surg. Pathol. 2017, 41, 607–615. [Google Scholar] [CrossRef]
- Rietbergen, M.M.; Snijders, P.J.; Beekzada, D.; Braakhuis, B.J.; Brink, A.; Heideman, D.A.; Hesselink, A.T.; Witte, B.I.; Bloemena, E.; Baatenburg-De Jong, R.J.; et al. Molecular characterization of p16-immunopositive but HPV DNA-negative oropharyngeal carcinomas. Int. J. Cancer 2014, 134, 2366–2372. [Google Scholar] [CrossRef]
- Parfenov, M.; Pedamallu, C.S.; Gehlenborg, N.; Freeman, S.S.; Danilova, L.; Bristow, C.A.; Lee, S.; Hadjipanayis, A.G.; Ivanova, E.V.; Wilkerson, M.D.; et al. Characterization of HPV and host genome interactions in primary head and neck cancers. Proc. Natl. Acad. Sci. USA 2014, 111, 15544–15549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrone, F.; Gloghini, A.; Cortelazzi, B.; Bossi, P.; Licitra, L.; Pilotti, S. Isolating p16-positive/HPV-negative oropharyngeal cancer: An effort worth making. Am J Surg Pathol 2011, 35, 774–777. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, P.M.; Yu, Z.; Haffty, B.G.; Kowalski, D.; Harigopal, M.; Brandsma, J.; Sasaki, C.; Joe, J.; Camp, R.L.; Rimm, D.L.; et al. Molecular classification identifies a subset of human papillomavirus--associated oropharyngeal cancers with favorable prognosis. J. Clin. Oncol. 2006, 24, 736–747. [Google Scholar] [CrossRef] [PubMed]
- LeConte, B.A.; Szaniszlo, P.; Fennewald, S.M.; Lou, D.I.; Qiu, S.; Chen, N.W.; Lee, J.H.; Resto, V.A. Differences in the viral genome between HPV-positive cervical and oropharyngeal cancer. PLoS ONE 2018, 13, e0203403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kofler, B.; Borena, W.; Manzl, C.; Dudas, J.; Wegscheider, A.S.; Jansen-Durr, P.; Schartinger, V.; Riechelmann, H. Sensitivity of tumor surface brushings to detect human papilloma virus DNA in head and neck cancer. Oral Oncol. 2017, 67, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Abreu, A.L.; Souza, R.P.; Gimenes, F.; Consolaro, M.E. A review of methods for detect human Papillomavirus infection. Virol. J. 2012, 9, e262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mason, A.G.S.; Vettorato, M.; Negri, G.; Mian, C.; Brusauro, F.; Bortolozzo, K. Detection of high-risk HPV genotypes in cervical samples: A comparison study of a novel real time pcr/reverse line blot-based technique and the digene HC2 assay. Pathologica 2012, 6, 104–146. [Google Scholar]

{kind=link}
{kind=link}
| Variables | N (%) |
|---|---|
| Male | 46 (82.1%) |
| Female | 10 (17.9%) |
| Mean age | 65.4 years (±10.12) |
| E7 positivity * | 26 (46.4%) |
| HPV Subtypes | Number and Percent of HPV + OPC Patients |
|---|---|
| HPV 16 | 19 patients (83%) |
| HPV 18 | 2 patients (9%) |
| HPV 33 | 1 patient (4%) |
| HPV 58 | 1 patient (4%) |
| Variables | E7 Positive (n = 26) | E7 Negative (n = 30) | p-Value |
|---|---|---|---|
| Sex | |||
| Male | 22 | 24 | p = 0.73 |
| Female | 4 | 6 | |
| Age | |||
| ≤65 years | 10 | 10 | p = 0.45 |
| >65 years | 16 | 20 | |
| ASA score | |||
| ASA I/II | 19 | 14 | p = 0.04 |
| ASA III/IV | 7 | 16 | |
| Smoking | |||
| Non-smokers | 16 | 8 | p = 0.009 |
| Smoker | 10 | 22 | |
| Alcohol consumption | |||
| Daily | 8 | 13 | p = 0.33 |
| Not daily | 18 | 17 | |
| Clinical T-stage | |||
| cT1/T2 | 14 | 16 | p = 1.0 |
| cT3/4 | 12 | 14 | |
| UICCC | |||
| Stage I | 1 | 3 | p = 0.84 |
| Stage II | 4 | 4 | |
| Stage III | 6 | 7 | |
| Stage IV | 15 | 16 | |
| Subsite oropharynx | |||
| Palatine tonsil | 17 | 19 | p = 0.14 |
| Base of tongue | 9 | 6 | |
| Uvula | 0 | 3 | |
| Lateral pharyngeal wall | 0 | 2 | |
| Therapy | |||
| Surgery only | 3 | 5 | p = 0.72 |
| Surgery and PORT | 3 | 4 | |
| Surgery and RCT/RIT | 1 | 0 | |
| Primary RCT/RIT | 14 | 13 | |
| Primary RT | 2 | 3 | |
| Chemo only | 2 | 3 | |
| p16 | |||
| Positive | 17 | 12 | p = 0.05 |
| Negative | 9 | 18 | |
| HPV DNA | |||
| Positive | 14 | 9 | p = 0.06 |
| Negative | 12 | 21 | |
| Follow up | |||
| No recurrence | 15 | 20 | p = 0.55 |
| Progression | 6 | 9 |
| HPV DNA | p16 | |||
|---|---|---|---|---|
| Negative | Positive | Total | p-Value | |
| Negative | 27 | 6 | 33 | p < 0.001 |
| Positive | 0 | 23 | 23 | |
| Total | 27 | 29 | 56 | |
| Reference Method | E7 Oncoprotein | |||
|---|---|---|---|---|
| Negative | Positive | Total | p-Value | |
| Negative | 18 | 9 | 27 | p = 0.048 |
| Positive | 9 | 14 | 23 | |
| Total | 27 | 23 | 50 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borena, W.; Schartinger, V.H.; Dudas, J.; Ingruber, J.; Greier, M.C.; Steinbichler, T.B.; Laimer, J.; Stoiber, H.; Riechelmann, H.; Kofler, B. HPV-Induced Oropharyngeal Cancer and the Role of the E7 Oncoprotein Detection via Brush Test. Cancers 2020, 12, 2388. https://doi.org/10.3390/cancers12092388
Borena W, Schartinger VH, Dudas J, Ingruber J, Greier MC, Steinbichler TB, Laimer J, Stoiber H, Riechelmann H, Kofler B. HPV-Induced Oropharyngeal Cancer and the Role of the E7 Oncoprotein Detection via Brush Test. Cancers. 2020; 12(9):2388. https://doi.org/10.3390/cancers12092388
Chicago/Turabian StyleBorena, Wegene, Volker H. Schartinger, Jozsef Dudas, Julia Ingruber, Maria C. Greier, Teresa B. Steinbichler, Johannes Laimer, Heribert Stoiber, Herbert Riechelmann, and Barbara Kofler. 2020. "HPV-Induced Oropharyngeal Cancer and the Role of the E7 Oncoprotein Detection via Brush Test" Cancers 12, no. 9: 2388. https://doi.org/10.3390/cancers12092388