The Unique Pharmacometrics of Small Molecule Therapeutic Drug Tracer Imaging for Clinical Oncology


Simple Summary
Abstract
1. Introduction
2. What Does Tumor Signal on a Drug Tracer Image Signify?
3. Drug Tracer Imaging to Guide Patient Selection
4. Tumor Pharmacokinetics for Image-Guided Dosing Design
5. How to Make a Drug Tracer
6. Does Drug Tracer Imaging Offer Any Advantages over Conventional Tissue-Based PK/PD Biomarkers?
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- O’Connor, J.P.B.; Aboagye, E.O.; Adams, J.E.; Aerts, H.J.W.L.; Barrington, S.; Beer, A.J.; Boellaard, R.; Bohndiek, S.E.; Brady, M.; Brown, G.; et al. Imaging biomarker roadmap for cancer studies. Nat. Rev. Clin. Oncol. 2017, 14, 169–186. [Google Scholar] [CrossRef] [PubMed]
- Workman, P.; Aboagye, E.O.; Chung, Y.-L.; Griffiths, J.R.; Hart, R.; Leach, M.O.; Maxwell, R.J.; McSheehy, P.M.J.; Price, P.M.; Zweit, J. Minimally invasive pharmacokinetic and pharmacodynamic technologies in hypothesis-testing clinical trials of innovative therapies. J. Natl. Cancer Inst. 2006, 98, 580–598. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute U.S. National Institutes of Health. A Workshop Regarding What In-Vivo Molecular Imaging Probes Are Needed to Support Future Translational Studies in Cancer Therapeutics. In Strategies for Imaging Priority Targets; NCI: Washington, DC, USA, 2002. Available online: www.cancer.gov (accessed on 1 September 2020).
- Weber, W.A.; Czernin, J.; Phelps, M.E.; Herschman, H.R. Technology Insight: Novel imaging of molecular targets is an emerging area crucial to the development of targeted drugs. Nat. Clin. Pract. Oncol. 2008, 5, 44–54. [Google Scholar] [CrossRef]
- Workman, P.; Burrows, F.; Neckers, L.; Rosen, N. Drugging the cancer chaperone HSP90: Combinatorial therapeutic exploitation of oncogene addiction and tumor stress. Ann. N. Y. Acad. Sci. 2007, 1113, 202–216. [Google Scholar] [CrossRef]
- Seddon, B.M.; Workman, P. The role of functional and molecular imaging in cancer drug discovery and development. Br. J. Radiol. 2003, 76 (Suppl. S2), S128–S138. [Google Scholar] [CrossRef]
- Dunphy, M.P.; Pressl, C.; Pillarsetty, N.; Grkovski, M.; Modi, S.; Jhaveri, K.; Norton, L.; Beattie, B.J.; Zanzonico, P.B.; Zatorska, D.; et al. First-in-Human Trial of Epichaperome-Targeted Positron Emission Tomography in Cancer Patients. Clin. Cancer Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Pillarsetty, N.; Jhaveri, K.; Taldone, T.; Caldas-Lopes, E.; Punzalan, B.; Joshi, S.; Bolaender, A.; Uddin, M.M.; Rodina, A.; Yan, P.; et al. Paradigms for Precision Medicine in Epichaperome Cancer Therapy. Cancer Cell 2019, 36, 559–573. [Google Scholar] [CrossRef]
- Krebs, S.; Veach, D.R.; Carter, L.M.; Grkovski, M.; Fornier, M.; Mauro, M.J.; Voss, M.H.; Danila, D.C.; Burnazi, E.; Null, M.; et al. First-in-Human Trial of Dasatinib-Derivative Tracer for Tumor Kinase-Targeted Positron Emission Tomography. J. Nucl. Med. 2020. [Google Scholar] [CrossRef]
- Veach, D.R.; Namavari, M.; Pillarsetty, N.; Santos, E.B.; Beresten-Kochetkov, T.; Lambek, C.; Punzalan, B.J.; Antczak, C.; Smith-Jones, P.M.; Djaballah, H.; et al. Synthesis and biological evaluation of a fluorine-18 derivative of dasatinib. J. Med. Chem. 2007, 50, 5853–5857. [Google Scholar] [CrossRef]
- Schuhmacher, A.; Gassmann, O.; Hinder, M. Changing R & D models in research-based pharmaceutical companies. J. Transl. Med. 2016, 14, 105. [Google Scholar]
- Wouters, O.J.; McKee, M.; Luyten, J. Estimated research and development investment needed to bring a new medicine to market, 2009–2018. JAMA 2020, 323, 844–853. [Google Scholar] [CrossRef]
- DiMasi, J.A.; Grabowski, H.G.; Hansen, R.W. Innovation in the pharmaceutical industry: New estimates of R & D costs. J. Health Econ. 2016, 47, 20–33. [Google Scholar]
- Peck, C.C.; Cross, J.T. “Getting the dose right”: Facts, a blueprint, and encouragements. Clin. Pharmacol. Ther. 2007, 82, 12–14. [Google Scholar] [CrossRef]
- Powell, J.R.; Gobburu, J.V. Pharmacometrics at FDA: Evolution and impact on decisions. Clin. Pharmacol. Ther. 2007, 82, 97–102. [Google Scholar] [CrossRef]
- Propper, D.; De Bono, J.; Saleem, A.; Ellard, S.; Flanagan, E.; Paul, J.; Ganesan, T.; Talbot, D.; O Aboagye, E.; Price, P.; et al. Use of positron emission tomography in pharmacokinetic studies to investigate therapeutic advantage in a phase I study of 120-hour intravenous infusion XR5000. J. Clin. Oncol. 2003, 21, 203–210. [Google Scholar] [CrossRef]
- Saleem, A.; Brown, G.D.; Brady, F.; Aboagye, E.O.; Osman, S.; Luthra, S.K.; O Ranicar, A.S.; Brock, C.S.; Stevens, M.F.G.; Newlands, E.; et al. Metabolic activation of temozolomide measured in vivo using positron emission tomography. Cancer Res. 2003, 63, 2409–2415. [Google Scholar]
- Presant, C.; Wolf, W.; Waluch, V.; Wiseman, C.; Kennedy, P.; Blayney, D.; Brechner, R.; Kennedy, D. Association of intratumoral pharmacokinetics of fluorouracil with clinical response. Lancet 1994, 343, 1184–1187. [Google Scholar] [CrossRef]
- Kissel, J.; Brix, G.; Bellemann, M.E.; Strauss, L.G. Dimitrakopoulou-Strauss, A.; Port, R.; Haberkorn, U.; Lorenz, W.J. Pharmacokinetic analysis of 5-[18F] fluorouracil tissue concentrations measured with positron emission tomography in patients with liver metastases from colorectal adenocarcinoma. Cancer Res. 1997, 57, 3415–3423. [Google Scholar]
- Presant, C.A.; Wolf, W.; Waluch, V.; Wiseman, C.L.; Weitz, I.; Shani, J. Enhancement of fluorouracil uptake in human colorectal and gastric cancers by interferon or by high-dose Methotrexate: An in vivo human study using noninvasive 19f-magnetic resonance spectroscopy. J. Clin. Oncol. 2000, 18, 255. [Google Scholar] [CrossRef]
- Presant, C.A.; Jacobson, J.; Wolf, W.; Waluch, V.; Weitz, I.C.; Macdonald, J.S. Does leucovorin alter the intratumoral pharmacokinetics of 5-fluorouracil (5-fu)? A southwest oncology group study. Investig. New Drugs 2002, 20, 369–376. [Google Scholar] [CrossRef]
- Levi, J.; Lam, T.; Goth, S.R.; Yaghoubi, S.; Bates, J.; Ren, G.; Jivan, S.; Huynh, T.; Blecha, J.E.; Khattri, R.; et al. Imaging of activated t cells as an early predictor of immune response to anti-PD-1 Therapy. Cancer Res. 2019, 79, 3455–3465. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.; Le, T.M.; Wei, L.; Poddar, S.; Bazzy, J.; Wang, X.; Uong, N.T.; Abt, E.R.; Capri, J.R.; Austin, W.R.; et al. [18F]CFA as a clinically translatable probe for PET imaging of deoxycytidine kinase activity. Proc. Natl. Acad. Sci. USA 2016, 113, 4027–4032. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.M.; Chiu, C.H.; Chen, W.T.; Wu, C.H.; Lin, P.Y.; Huang, Y.Y.; Chen, J.-H.; Tzen, K.-Y.; Shiue, C.-Y.; Lin, W.-J. Evaluation of 5-[(18)F]fluoro-2′-deoxycytidine as a tumor imaging agent: A comparison of [(18)F]FdUrd, [(18)F]FLT and [(18)F]FDG. Appl. Radiat. Isot. 2019, 148, 152–159. [Google Scholar] [CrossRef]
- Young, C.R.; Adler, S.; Eary, J.F.; Lindenberg, M.L.; Jacobs, P.M.; Collins, J.; Kummar, S.; Kurdziel, K.A.; Choyke, P.L.; Mena, E. Biodistribution, tumor detection, and radiation dosimetry of (18)F-5-Fluoro-2′-deoxycytidine with tetrahydrouridine in solid tumors. J. Nucl. Med. 2019, 60, 492–496. [Google Scholar] [CrossRef] [PubMed]
- Muthu, P.; Chen, H.X.; Lutz, S. Redesigning human 2′-deoxycytidine kinase enantioselectivity for L-nucleoside analogues as reporters in positron emission tomography. ACS Chem. Biol. 2014, 9, 2326–2333. [Google Scholar] [CrossRef]
- Boothman, D.A.; Briggle, T.V.; Greer, S. Protective, tumor-selective dual pathway activation of 5-fluoro-2′-deoxycytidine provided by tetrahydrouridine in mice bearing mammary adenocarcinoma-755. Cancer Res. 1987, 47, 2344–2353. [Google Scholar]
- Radu, C.G.; Shu, C.J.; Nair-Gill, E.; Shelly, S.M.; Barrio, J.R.; Satyamurthy, N.; Phelps, M.E.; Witte, O.N. Molecular imaging of lymphoid organs and immune activation by positron emission tomography with a new [18F]-labeled 2′-deoxycytidine analog. Nat. Med. 2008, 14, 783–788. [Google Scholar] [CrossRef]
- Kurdziel, K.A.; Kiesewetter, D.O.; Carson, R.E.; Eckelman, W.C.; Herscovitch, P. Biodistribution, radiation dose estimates, and in vivo Pgp modulation studies of 18F-paclitaxel in nonhuman primates. J. Nucl. Med. 2003, 44, 1330–1339. [Google Scholar]
- Kurdziel, K.A.; Kalen, J.D.; Hirsch, J.I.; Wilson, J.D.; Agarwal, R.; Barrett, D.; Bear, H.D.; McCumiskey, J.F. Imaging multidrug resistance with 4-[18F]fluoropaclitaxel. Nucl. Med. Biol. 2007, 34, 823–831. [Google Scholar] [CrossRef]
- Gangloff, A.; Hsueh, W.-A.; Kesner, A.L.; O Kiesewetter, D.; Pio, B.S.; Pegram, M.D.; Beryt, M.; Townsend, A.; Czernin, J.; E Phelps, M.; et al. Estimation of paclitaxel biodistribution and uptake in human-derived xenografts in vivo with (18)F-fluoropaclitaxel. J. Nucl. Med. 2005, 46, 1866–1871. [Google Scholar]
- Kurdziel, K.A.; Kiesewetter, D.O. PET imaging of multidrug resistance in tumors using 18F-fluoropaclitaxel. Curr. Top. Med. Chem. 2010, 10, 1792–1798. [Google Scholar] [CrossRef] [PubMed]
- Fei, X.; Wang, J.-Q.; Miller, K.D.; Sledge, G.W.; Hutchins, G.D.; Zheng, Q.-H. Synthesis of [18F]Xeloda as a novel potential PET radiotracer for imaging enzymes in cancers. Nucl. Med. Biol. 2004, 31, 1033–1041. [Google Scholar] [CrossRef] [PubMed]
- Bauer, T.M.; Shaw, A.T.; Johnson, M.L.; Navarro, A.; Gainor, J.F.; Thurm, H.; Pithavala, Y.K.; Abbattista, A.; Peltz, G.; Felip, E. Brain penetration of lorlatinib: Cumulative incidences of CNS and Non-CNS progression with lorlatinib in patients with previously treated ALK-positive non-small-cell lung cancer. Target. Oncol. 2020, 15, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Collier, T.L.; Normandin, M.D.; Stephenson, N.A.; Livni, E.; Liang, S.H.; Wooten, D.W.; Esfahani, S.A.; Stabin, M.G.; Mahmood, U.; Chen, J.; et al. Synthesis and preliminary PET imaging of 11C and 18F isotopologues of the ROS1/ALK inhibitor lorlatinib. Nat. Commun. 2017, 8, 15761. [Google Scholar] [CrossRef]
- Bahce, I.; Smit, E.F.; Lubberink, M.; Van Der Veldt, A.A.M.; Yaqub, M.; Windhorst, A.D.; Schuit, R.C.; Thunnissen, E.; Heideman, D.A.M.; Postmus, P.E.; et al. Development of [(11)C]erlotinib positron emission tomography for in vivo evaluation of EGF receptor mutational status. Clin. Cancer Res. 2013, 19, 183–193. [Google Scholar] [CrossRef]
- Bahce, I.; Yaqub, M.; Errami, H.; Schuit, R.C.; Schober, P.; Thunnissen, E.; Windhorst, A.D.; Lammertsma, A.A.; Smit, E.F.; Hendrikse, N.H. Effects of erlotinib therapy on [11C]erlotinib uptake in EGFR mutated, advanced NSCLC. EJNMMI Res. 2016, 6, 10. [Google Scholar] [CrossRef]
- Slobbe, P.; Windhorst, A.D.; Walsum, M.S.-V.; Smit, E.F.; Niessen, H.G.; Solca, F.; Stehle, G.; Van Dongen, G.A.M.S.; Poot, A.J. A comparative PET imaging study with the reversible and irreversible EGFR tyrosine kinase inhibitors [(11)C]erlotinib and [(18)F]afatinib in lung cancer-bearing mice. EJNMMI Res. 2015, 5, 14. [Google Scholar] [CrossRef]
- Chopra, A.; Shan, L.; Eckelman, W.C.; Leung, K.; Latterner, M.; Bryant, S.H.; Menkens, A. [(11)C]N-(3-Ethynylphenyl)-6,7-bis(2-methoxyethoxy)-4-quinazolinamine. In Molecular Imaging and Contrast Agent Database (MICAD). Mol. Imaging Biol. 2012, 14, 4–13. [Google Scholar] [CrossRef]
- Varrone, A.; Varnäs, K.; Jucaite, A.; Cselényi, Z.; Johnström, P.; Schou, M.; Vazquez-Romero, A.; Moein, M.M.; Halldin, C.; Brown, A.P.; et al. A PET study in healthy subjects of brain exposure of (11)C-labelled osimertinib—A drug intended for treatment of brain metastases in non-small cell lung cancer. J. Cereb. Blood Flow Metab. 2019. [Google Scholar] [CrossRef]
- Huang, S.; Han, Y.; Chen, M.; Hu, K.; Qi, Y.; Sun, P.; Wang, M.; Wu, H.; Li, G.; Wang, Q.; et al. Radiosynthesis and biological evaluation of (18)F-labeled 4-anilinoquinazoline derivative ((18)F-FEA-Erlotinib) as a potential EGFR PET agent. Bioorg. Med. Chem. Lett. 2018, 28, 1143–1148. [Google Scholar] [CrossRef]
- Marijn, V.; Läppchen, T.; Jansen, H.T.; Kivits, S.; Van Driel, A.; Van De Steeg, E.; Van Der Hoorn, J.W.; Sio, C.F.; Steinbach, O.C.; DeGroot, J. PET-CT imaging with [(18)F]-gefitinib to measure Abcb1a/1b (P-gp) and Abcg2 (Bcrp1) mediated drug-drug interactions at the murine blood-brain barrier. Nucl. Med. Biol. 2015, 42, 833–841. [Google Scholar]
- Song, Y.; Xiao, Z.; Wang, K.; Wang, X.; Zhang, C.; Fang, F.; Sun, X.; Shen, B. Development and Evaluation of (18)F-IRS for Molecular Imaging Mutant EGF Receptors in NSCLC. Sci. Rep. 2017, 7, 3121. [Google Scholar] [CrossRef] [PubMed]
- Slobbe, P.; Poot, A.J.; Haumann, R.; Schuit, R.C.; Windhorst, A.D.; Van Dongen, G.A.M.S. Two anti-angiogenic TKI-PET tracers, [(11)C]axitinib and [(11)C]nintedanib: Radiosynthesis, in vivo metabolism and initial biodistribution studies in rodents. Nucl. Med. Biol. 2016, 43, 612–624. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.; Xie, L.; Zhang, Y.; Fujinaga, M.; Mori, W.; Kurihara, Y.; Yamasaki, T.; Wang, F.; Zhang, M.-R. Pharmacokinetic evaluation of [(11)C]CEP-32496 in nude mice Bearing BRAF(V600E) mutation-induced melanomas. Mol. Imaging 2018, 17, 1536012118795952. [Google Scholar] [CrossRef]
- Saleem, A.; Searle, G.E.; Kenny, L.M.; Huiban, M.; Kozlowski, K.; Waldman, A.; Woodley, L.; Palmieri, C.; Lowdell, C.; Kaneko, T.; et al. Lapatinib access into normal brain and brain metastases in patients with Her-2 overexpressing breast cancer. EJNMMI Res. 2015, 5, 30. [Google Scholar] [CrossRef]
- Poot, A.J.; Van Der Wildt, B.; Walsum, M.S.-V.; Rongen, M.; Schuit, R.C.; Hendrikse, N.H.; Eriksson, J.; Van Dongen, G.A.M.S.; Windhorst, A.D. [11C] Sorafenib: Radiosynthesis and preclinical evaluation in tumor-bearing mice of a new TKI-PET tracer. Nucl. Med. Biol. 2013, 40, 488–497. [Google Scholar] [CrossRef]
- NCT02700763. [18F] Dabrafenib Molecular Imaging in Melanoma Brain Metastasis. Available online: www.clinicaltrials.gov (accessed on 1 September 2020).
- Rodina, A.; Wang, T.; Yan, P.; Gomes, E.D.; Dunphy, M.P.S.; Pillarsetty, N.; Koren, J.I.; Gerecitano, J.F.; Taldone, T.; Zong, H.; et al. The epichaperome is an integrated chaperome network that facilitates tumour survival. Nature 2016, 538, 397–401. [Google Scholar] [CrossRef]
- Di Gialleonardo, V.; Signore, A.; Glaudemans, A.W.; Dierckx, R.A.J.O.; De Vries, E.F. N-(4-18F-fluorobenzoyl)interleukin-2 for PET of human-activated T lymphocytes. J. Nucl. Med. 2012, 53, 679–686. [Google Scholar] [CrossRef]
- Hartimath, S.V.; Manuelli, V.; Zijlma, R.; Signore, A.; Nayak, T.K.; Freimoser-Grundschober, A.; Klein, C.; Dierckx, R.A.; De Vries, E. Pharmacokinetic properties of radiolabeled mutant Interleukin-2v: A PET imaging study. Oncotarget 2018, 9, 7162–7174. [Google Scholar] [CrossRef]
- Zheng, Q.-H.; Fei, X.; DeGrado, T.R.; Wang, J.-Q.; Stone, K.L.; Martinez, T.D.; Gay, D.J.; Baity, W.L.; Mock, B.H.; E Glick-Wilson, B.; et al. Synthesis, biodistribution and micro-PET imaging of a potential cancer biomarker carbon-11 labeled MMP inhibitor (2R)-2-[[4-(6-fluorohex-1-ynyl)phenyl]sulfonylamino]-3-methylbutyric acid [11C]methyl ester. Nucl. Med. Biol. 2003, 30, 753–760. [Google Scholar] [CrossRef]
- Han, N.; Jiang, Y.; Gai, Y.; Liu, Q.; Yuan, L.; Wang, Y.; Li, M.; Zhang, Y.; Lan, X. (11)C-Labeled Pictilisib (GDC-0941) as a molecular tracer targeting phosphatidylinositol 3-Kinase (PI3K) for breast cancer imaging. Contrast Media Mol. Imaging 2019, 2019, 1760184. [Google Scholar] [CrossRef]
- Donnelly, D.J.; Smith, R.A.; Morin, P.; Lipovsek, D.; Gokemeijer, J.; Cohen, D.; Lafont, V.; Tran, T.; Cole, E.L.; Wright, M.; et al. Synthesis and Biologic Evaluation of a Novel (18)F-Labeled Adnectin as a PET Radioligand for Imaging PD-L1 Expression. J. Nucl. Med. 2018, 59, 529–535. [Google Scholar] [CrossRef]
- Makvandi, M.; Pantel, A.; Schwartz, L.E.; Xu, K.; Hsieh, C.-J.; Kim, H.; Li, S.-H.; Doot, R.; Lee, S.; Simpkins, F.; et al. Abstract 3716: Exploring the significance of PARP-1 expression for therapy and clinical PET/CT imaging of PARP-1 in ovarian cancer. Cancer Res. 2017, 77 (Suppl. S13), 3716. [Google Scholar]
- Graham, M.M.; Weber, W.A. Evaluation of the Efficacy of Targeted Imaging Agents. J. Nucl. Med. 2016, 57, 653–659. [Google Scholar] [CrossRef]
- European Imaging Biomarkers Alliance. Available online: http://www.eibir.org/scientific-activities/joint-initiatives/eiball/ (accessed on 1 September 2020).
- FDA Biomarker Qualification Program. Available online: https://www.fda.gov/Drugs/DevelopmentApprovalProcess/DrugDevelopmentToolsQualificationProgram/BiomarkerQualificationProgram/default.htm (accessed on 1 September 2020).
- FDA-NIH Biomarker Working Group. BEST (Biomarkers, EndpointS, and Other Tools) Resource. 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK326791/ (accessed on 29 May 2020).
- National Biomarker Development Alliance. Available online: http://nbdabiomarkers.org (accessed on 1 September 2020).
- National Cancer Institute (NCI) Cancer Imaging Program. Available online: https://imaging.cancer.gov/default.htm (accessed on 1 September 2020).
- NCI Clinical Trials Working Group (CTWG) Biomarker Study Evaluation Guidelines. Available online: https://www.cancer.gov/about-nci/organization/ccct/funding/biqsfp/2017-biomarker-study-eval-guide.pdf (accessed on 1 September 2020).
- Bergström, M.; Grahnén, A.; Långström, B. Positron emission tomography microdosing: A new concept with application in tracer and early clinical drug development. Eur. J. Clin. Pharmacol. 2003, 59, 357–366. [Google Scholar] [CrossRef]
- Westerterp, M.; Pruim, J.; Oyen, W.J.; Hoekstra, O.; Paans, A.; Visser, E.; Van Lanschot, J.; Sloof, G.; Boellaard, R. Quantification of FDG PET studies using standardised uptake values in multi-centre trials: Effects of image reconstruction, resolution and ROI definition parameters. Eur. J. Nucl. Med. Mol. Imaging 2007, 34, 392–404. [Google Scholar] [CrossRef]
- Banerji, U.; Workman, P. Critical parameters in targeted drug development: The pharmacological audit trail. Semin. Oncol. 2016, 43, 436–445. [Google Scholar] [CrossRef]
- Jain, R.K. Delivery of molecular and cellular medicine to solid tumors. Adv. Drug Deliv. Rev. 2012, 64, 353–365. [Google Scholar] [CrossRef]
- Badawi, R.D.; Shi, H.; Hu, P.; Chen, S.; Xu, T.; Price, P.M.; Ding, Y.; Spencer, B.A.; Nardo, L.; Liu, W.; et al. First human imaging studies with the EXPLORER total-body pet scanner. J. Nucl. Med. 2019, 60, 299–303. [Google Scholar] [CrossRef]
- Wang, T.; Rodina, A.; Dunphy, M.P.; Corben, A.; Modi, S.; Guzman, M.L.; Gewirth, D.T.; Chiosis, G. Chaperome heterogeneity and its implications for cancer study and treatment. J. Biol. Chem. 2019, 294, 2162–2179. [Google Scholar] [CrossRef]
- Taldone, T.; Wang, T.; Rodina, A.; Pillarsetty, N.V.K.; Digwal, C.S.; Sharma, S.; Yan, P.; Joshi, S.; Pagare, P.P.; Bolaender, A.; et al. A chemical biology approach to the chaperome in cancer-HSP90 and beyond. Cold Spring Harb. Perspect Biol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Joshi, S.; Wang, T.; Araujo, T.L.S.; Sharma, S.; Brodsku, J.L.; Chiosis, G. Adapting to stress—Chaperome networks in cancer. Nat. Rev. Cancer 2018, 18, 562–575. [Google Scholar] [CrossRef] [PubMed]
- Dunphy, M.P.; Zanzonico, P.; Veach, D.; Somwar, R.; Pillarsetty, N.; Lewis, J.S.; Larson, S. Dosimetry of (18)F-labeled tyrosine kinase inhibitor SKI-249380, a dasatinib-tracer for PET imaging. Mol. Imaging Biol. 2010. [Google Scholar] [CrossRef]
- Ulaner, G.A.; Hyman, D.M.; Lyashchenko, S.K.; Lewis, J.S.; Carrasquillo, J.A. 89Zr-Trastuzumab PET/CT for Detection of Human Epidermal Growth Factor Receptor 2-Positive Metastases in Patients With Human Epidermal Growth Factor Receptor 2-Negative Primary Breast Cancer. Clin. Nucl. Med. 2017, 42, 912–917. [Google Scholar] [CrossRef]
- Luo, F.R.; Barrett, Y.; Ji, P.; Holly, P.; McCann, E.; Rhyne, P.; Clarke, E.; He, K.; Bleichardt, E.; Blackwood-Chirchir, M. Dasatinib (BMS-354825) pharmacokinetics correlate with pSRC pharmacodynamics in phase I studies of patients with cancer (CA180002, CA180003). J. Clin. Oncol. Meet. Abstr. 2006, 24 (Suppl. S18), 3046. [Google Scholar] [CrossRef]
- Hiwase, D.K.; Saunders, V.; Hewett, D.; Frede, A.; Zrim, S.; Dang, P.; Eadie, L.N.; To, L.B.; Melo, J.; Kumar, S.; et al. Dasatinib cellular uptake and efflux in chronic myeloid leukemia cells: Therapeutic implications. Clin. Cancer Res. 2008, 14, 3881–3888. [Google Scholar] [CrossRef]
- Luo, F.R.; Yang, Z.; Camuso, A.; Smykla, R.; McGlinchey, K.; Fager, K.; Flefleh, C.; Castaneda, S.; Inigo, I.; Kan, D.; et al. Dasatinib (BMS-354825) pharmacokinetics and pharmacodynamic biomarkers in animal models predict optimal clinical exposure. Clin. Cancer Res. 2006, 12, 7180–7186. [Google Scholar] [CrossRef]
- Chen, Y.; Agarwal, S.; Shaik, N.M.; Chen, C.; Yang, Z.; Elmquist, W.F. P-glycoprotein and breast cancer resistance protein influence brain distribution of dasatinib. J. Pharmacol. Exp. Ther. 2009, 330, 956–963. [Google Scholar] [CrossRef]
- Giannoudis, A.; Davies, A.; Lucas, C.M.; Harris, R.J.; Pirmohamed, M.; Clark, R.E. Effective dasatinib uptake may occur without human organic cation transporter 1 (hOCT1): Implications for the treatment of imatinib-resistant chronic myeloid leukemia. Blood 2008, 112, 3348–3354. [Google Scholar] [CrossRef]
- Lagas, J.S.; Van Waterschoot, R.A.; Van Tilburg, V.A.; Hillebrand, M.J.; Lankheet, N.; Rosing, H.; Beijnen, J.H.; Schinkel, A.H. Brain accumulation of dasatinib is restricted by P-glycoprotein (ABCB1) and breast cancer resistance protein (ABCG2) and can be enhanced by elacridar treatment. Clin. Cancer Res. 2009, 15, 2344–2351. [Google Scholar] [CrossRef]
- Porkka, K.; Koskenvesa, P.; Lundán, T.; Rimpiläinen, J.; Mustjoki, S.; Smykla, R.; Wild, R.; Luo, R.; Arnan, M.; Brethon, B.; et al. Dasatinib crosses the blood-brain barrier and is an efficient therapy for central nervous system Philadelphia chromosome-positive leukemia. Blood 2008, 112, 1005–1012. [Google Scholar] [CrossRef] [PubMed]
- Burgess, M.R.; Skaggs, B.J.; Shah, N.P.; Lee, F.Y.; Sawyers, C.L. Comparative analysis of two clinically active BCR-ABL kinase inhibitors reveals the role of conformation-specific binding in resistance. Proc. Natl. Acad. Sci. USA 2005, 102, 3395–3400. [Google Scholar] [CrossRef] [PubMed]
- Lamberts, S.; Barker, W.; Reubi, J.-C.; Krenning, E. Somatostatin-receptor imaging in the localization of endocrine tumors. N. Engl. J. Med. 1990, 323, 1246–1249. [Google Scholar] [CrossRef] [PubMed]
- Lamberts, S.W.; Hofland, L.J.; van Koetsveld, P.M.; Reubi, J.C.; Bruining, H.A.; Barker, W.H.; Krenning, E.P. Parallel in vivo and in vitro detection of functional somatostatin receptors in human endocrine pancreatic tumors: Consequences with regard to diagnosis, localization, and therapy. J. Clin. Endocrinol. Metab. 1990, 71, 566–574. [Google Scholar] [CrossRef] [PubMed]
- Hsueh, W.-A.; Kesner, A.L.; Gangloff, A.; Pegram, M.D.; Beryt, M.; Czernin, J.; Phelps, M.E.; Silverman, D.H.S. Predicting chemotherapy response to paclitaxel with 18F-Fluoropaclitaxel and PET. J. Nucl. Med. 2006, 47, 1995–1999. [Google Scholar]
- Kurdziel, K.A.; Kalen, J.D.; Hirsch, J.I.; Wilson, J.D.; Bear, H.D.; Logan, J.; McCumisky, J.; Moorman-Sykes, K.; Adler, S.; Choyke, P.L. Human dosimetry and preliminary tumor distribution of 18F-fluoropaclitaxel in healthy volunteers and newly diagnosed breast cancer patients using PET/CT. J. Nucl. Med. 2011, 52, 1339–1345. [Google Scholar] [CrossRef]
- Li, Z.; Ivanov, A.A.; Su, R.; Gonzalez-Pecchi, V.; Qi, Q.; Liu, S.; Webber, P.; McMillan, E.; Rusnak, L.; Pham, C.; et al. The OncoPPi network of cancer-focused protein–protein interactions to inform biological insights and therapeutic strategies. Nat. Commun. 2017, 8, 14356. [Google Scholar] [CrossRef]
- Caldas-Lopes, E.; Cerchietti, L.; Ahn, J.H.; Clement, C.C.; Robles, A.I.; Rodina, A.; Moulick, K.; Taldone, T.; Gozman, A.; Guo, Y.; et al. Hsp90 inhibitor PU-H71, a multimodal inhibitor of malignancy, induces complete responses in triple-negative breast cancer models. Proc. Natl. Acad. Sci. USA 2009, 106, 8368–8373. [Google Scholar] [CrossRef]
- Scheibe, P.O.; Vera, D.R.; Eckelman, W.C. What is to be gained by imaging the same animal before and after treatment? Nucl. Med. Biol. 2005, 32, 727–732. [Google Scholar] [CrossRef]
- Harte, R.J.; Matthews, J.; O’Reilly, S.M.; Tilsley, D.O.; Osman, S.; Brown, G.; Luthra, S.J.; Brady, F.; Jones, T.; Price, P.M. Tumor, normal tissue, and plasma pharmacokinetic studies of fluorouracil biomodulation with N-phosphonacetyl-L-aspartate, folinic acid, and interferon alfa. J. Clin. Oncol. 1999, 17, 1580–1588. [Google Scholar] [CrossRef]
- Saleem, A.; Price, P.M. Early tumor drug pharmacokinetics is influenced by tumor perfusion but not plasma drug exposure. Clin. Cancer Res. 2008, 14, 8184–8190. [Google Scholar] [CrossRef]
- Saleem, A.; Yap, J.; Osman, S.; Brady, F.; Suttle, B.; Lucas, S.V.; Jones, T.; Price, P.M.; Aboagye, E.O.; Yap, J.; et al. Modulation of fluorouracil tissue pharmacokinetics by eniluracil: In-vivo imaging of drug action. Lancet 2000, 355, 2125–2131. [Google Scholar] [CrossRef]
- Evelhoch, J.L. In vivo 19F nuclear magnetic resonance spectroscopy: A potential monitor of 5-fluorouracil pharmacokinetics and metabolism. Invest. New Drugs 1989, 7, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Wolf, W.; Presant, C.A.; Servis, K.L.; El-Tahtawy, A.; Albright, M.J.; Barker, P.B.; Ring, R.; Atkinson, D.; Ong, R.; King, M. Tumor trapping of 5-fluorouracil: In vivo 19F NMR spectroscopic pharmacokinetics in tumor-bearing humans and rabbits. Proc. Natl. Acad. Sci. USA 1990, 87, 492–496. [Google Scholar] [CrossRef] [PubMed]
- Findlay, M.P.N.; Leach, M.O.; Cunningham, D.; Collins, D.J.; Payne, G.S.; Glaholm, J.; Mansi, J.L.; McCready, V.R. The non-invasive monitoring of low dose, infusional 5-fluorouracil and its modulation by interferon-{alpha} using in vivo 19F magnetic resonance spectroscopy in patients with colorectal cancer: A pilot study. Ann. Oncol. 1993, 4, 597–602. [Google Scholar] [CrossRef]
- Saleem, A.; Harte, R.J.; Matthews, J.; Osman, S.; Brady, F.; Luthra, S.K.; Brown, G.D.; Bleehen, N.; Connors, T.; Jones, T.; et al. Pharmacokinetic evaluation of N-[2-(dimethylamino)ethyl]acridine-4-carboxamide in patients by positron emission tomography. J. Clin. Oncol. 2001, 19, 1421–1429. [Google Scholar] [CrossRef]
- Rosso, L.; Brock, C.S.; Gallo, J.M.; Saleem, A.; Price, P.M.; Turkheimer, F.; Aboagye, E.O. A new model for prediction of drug distribution in tumor and normal tissues: Pharmacokinetics of temozolomide in glioma patients. Cancer Res. 2009, 69, 120–127. [Google Scholar] [CrossRef]
- Burvenich, I.; Parakh, S.; Parslow, A.C.; Lee, S.T.; Gan, H.K.; Scott, A.M. Receptor occupancy imaging studies in oncology drug development. AAPS J. 2018, 20, 43. [Google Scholar] [CrossRef]
- Kluger, H.M.; Dudek, A.; McCann, C.; Rink, L.; Ritacco, J.; Adrada, C.; Phouyaphone, N.; Southard, N.; Sznol, M. A phase II trial of dasatinib in advanced melanoma. J. Clin. Oncol. 2009, 27, 9010. [Google Scholar] [CrossRef]
- Brierley, R. 2009 ASCO Annual Meeting. J. Clin. Oncol. 2009, 27, 650. [Google Scholar] [CrossRef]
- Johnson, F.M.; Agrawal, S.; Burris, H.; Rosen, L.; Dhillon, N.; Hong, D.; Blackwood-Chirchir, A.; Luo, F.R.; Sy, O.; Kaul, S.; et al. Phase 1 pharmacokinetic and drug-interaction study of dasatinib in patients with advanced solid tumors. Cancer 2010, 116, 1582–1591. [Google Scholar] [CrossRef]
- Demetri, G.D.; Russo, P.A.; MacPherson, I.; Wang, D.; Morgan, J.A.; Brunton, V.G.; Paliwal, P.; Agrawal, S.; Voi, M.; Evans, T.J. Phase I dose-escalation and pharmacokinetic study of dasatinib in patients with advanced solid tumors. Clin. Cancer Res. 2009, 15, 6232–6240. [Google Scholar] [CrossRef] [PubMed]
- Le Tourneau, C.; Lee, J.J.; Siu, L.L. Dose escalation methods in phase I cancer clinical trials. J. Natl. Cancer Inst. 2009, 101, 708–720. [Google Scholar] [CrossRef] [PubMed]
- Sessa, C.; Shapiro, G.I.; Bhalla, K.N.; Britten, C.; Jacks, K.S.; Mita, M.; Papadimitrakopoulou, V.; Pluard, T.; Samuel, T.A.; Akimov, M.; et al. First-in-human phase I dose-escalation study of the HSP90 inhibitor AUY922 in patients with advanced solid tumors. Clin. Cancer Res. 2013, 19, 3671–3680. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, G.; Soverini, S.; Iacobucci, I.; Baccarani, M. Intermittent targeting as a tool to minimize toxicity of tyrosine kinase inhibitor therapy. Nat. Clin. Pract. Oncol. 2009, 6, 68–69. [Google Scholar] [CrossRef]
- Van Der Veldt, A.A.M.; Lubberink, M.; Bahce, I.; Walraven, M.; De Boer, M.P.; Greuter, H.N.; Hendrikse, N.H.; Eriksson, J.; Windhorst, A.D.; Postmus, P.E.; et al. Rapid decrease in delivery of chemotherapy to tumors after anti-VEGF therapy: Implications for scheduling of anti-angiogenic drugs. Cancer Cell 2012, 21, 82–91. [Google Scholar] [CrossRef]
- Wolf, W.; Presant, C.A. Tumor-based pharmacokinetics has greater significance for anticancer drugs than does blood-based pharmacokinetics. Clin. Phamrmacol. Ther. 2004, 76, 508–509. [Google Scholar] [CrossRef]
- Harte, R.J.O.R.S.; Matthews, J.C.; Babarovic, R.; Brown, G.; Osman, S.; Jones, T.; Price, P.M. Towards chemotherapy dose individualization with tracer derived tissue and tumor pharmacokinetic (pk) parameters. Proc. Am. Meeting ASCO 1995, 14, 1493. [Google Scholar]
- Saleem, A.; Murphy, P.; Plisson, C.; Lahn, M. Why are we failing to implement imaging studies with radiolabelled new molecular entities in early oncology drug development? Sci. World J. 2014, 2014, 269605. [Google Scholar] [CrossRef]
- Saleem, A.; Searle, G.; Kenny, L.M.; Huiban, M.; Waldman, A.; Downie, L.; Lau, M.; Murphy, P.S.; Kozlowski, K.; Lewis, Y.; et al. Brain and tumor penetration of carbon-11–labeled lapatinib ([11C]Lap) in patients (pts) with HER2-overexpressing metastatic breast cancer (MBC). J. Clin. Oncol. 2013, 31 (Suppl. S15), 635. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Chemotherapy |
|---|
| C-11 N-[(2′-dimethylamino)ethyl]acridine-4-carboxamide (XR5000) [16] C-11 Temozolomide [17] F-18 5-Fluorouracil [18,19,20,21] F-18 AraG [22] F-18 Clofarabine [23] F-18 Deoxycytidine [24,25,26,27,28] F-18 Paclitaxel [29,30,31,32] F-18 Xeloda [33] |
| Anaplastic Lymphoma Kinase (ALK) Inhibitors |
| C-11 Lorlatinib [34,35] F-18 Lorlatinib [35] |
| Epidermal Growth Factor Receptor (EGFR) Tyrosine Kinase Inhibitors |
| C-11 Erlotinib [36,37,38] C-11 Gefitinib [39] C-11 Osimertinib [40] F-18 FEA-Erlotinib [41] F-18 Gefitinib [42] F-18 IRS [43] |
| Other Tyrosine Kinase Inhibitors |
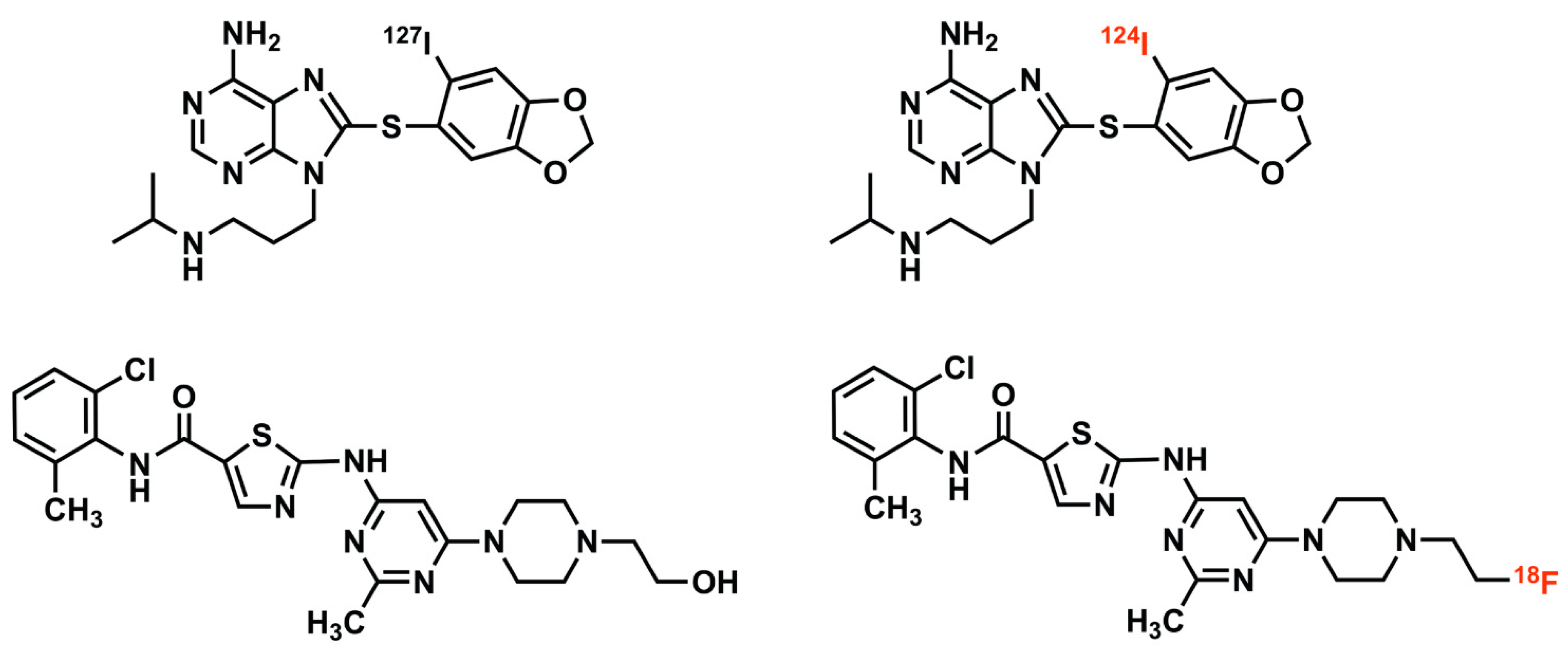
| C-11 Axitinib [44] C-11 CEP-32496 [45] C-11 Lapatinib [46] C-11 Nintedanib [44] C-11 Sorafenib [47] F-18 Afatinib [38] F-18 Dabrafenib [48] F-18 SKI249380 (Dasatinib Analogue) [9] |
| Epichaperome Inhibitor |
| I-124 PU-H71 [7,8,49] |
| IL2-Receptor/Cytokine |
| F-18 IL-2 [50] F-18 FB-IL2v [51] |
| Matrix Metalloproteinase Inhibitor |
| C-11 (2R)-2-[[4-(6-fluorohex-1-ynyl)phenyl]sulfonylamino]-3-methylbutyric acid methyl ester [52] |
| Phosphatidylinositol 3-Kinase (PI3K) Inhibitor |
| C-11 Pictilisib (GDC-0941) [53] |
| PD-L1 |
| F-18 BMS-986192 [54] |
| Poly(Adenosine Diphosphate Ribose) Polymerase (Parp) Inhibitor |
| F-18 Fluorthanatrace [55] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dunphy, M.P.S.; Pillarsetty, N. The Unique Pharmacometrics of Small Molecule Therapeutic Drug Tracer Imaging for Clinical Oncology. Cancers 2020, 12, 2712. https://doi.org/10.3390/cancers12092712
Dunphy MPS, Pillarsetty N. The Unique Pharmacometrics of Small Molecule Therapeutic Drug Tracer Imaging for Clinical Oncology. Cancers. 2020; 12(9):2712. https://doi.org/10.3390/cancers12092712
Chicago/Turabian StyleDunphy, Mark P. S., and Nagavarakishore Pillarsetty. 2020. "The Unique Pharmacometrics of Small Molecule Therapeutic Drug Tracer Imaging for Clinical Oncology" Cancers 12, no. 9: 2712. https://doi.org/10.3390/cancers12092712
APA StyleDunphy, M. P. S., & Pillarsetty, N. (2020). The Unique Pharmacometrics of Small Molecule Therapeutic Drug Tracer Imaging for Clinical Oncology. Cancers, 12(9), 2712. https://doi.org/10.3390/cancers12092712