
Non-Invasive Biomarkers for Earlier Detection of Pancreatic Cancer—A Comprehensive Review


Abstract
:Simple Summary
Abstract
1. Introduction
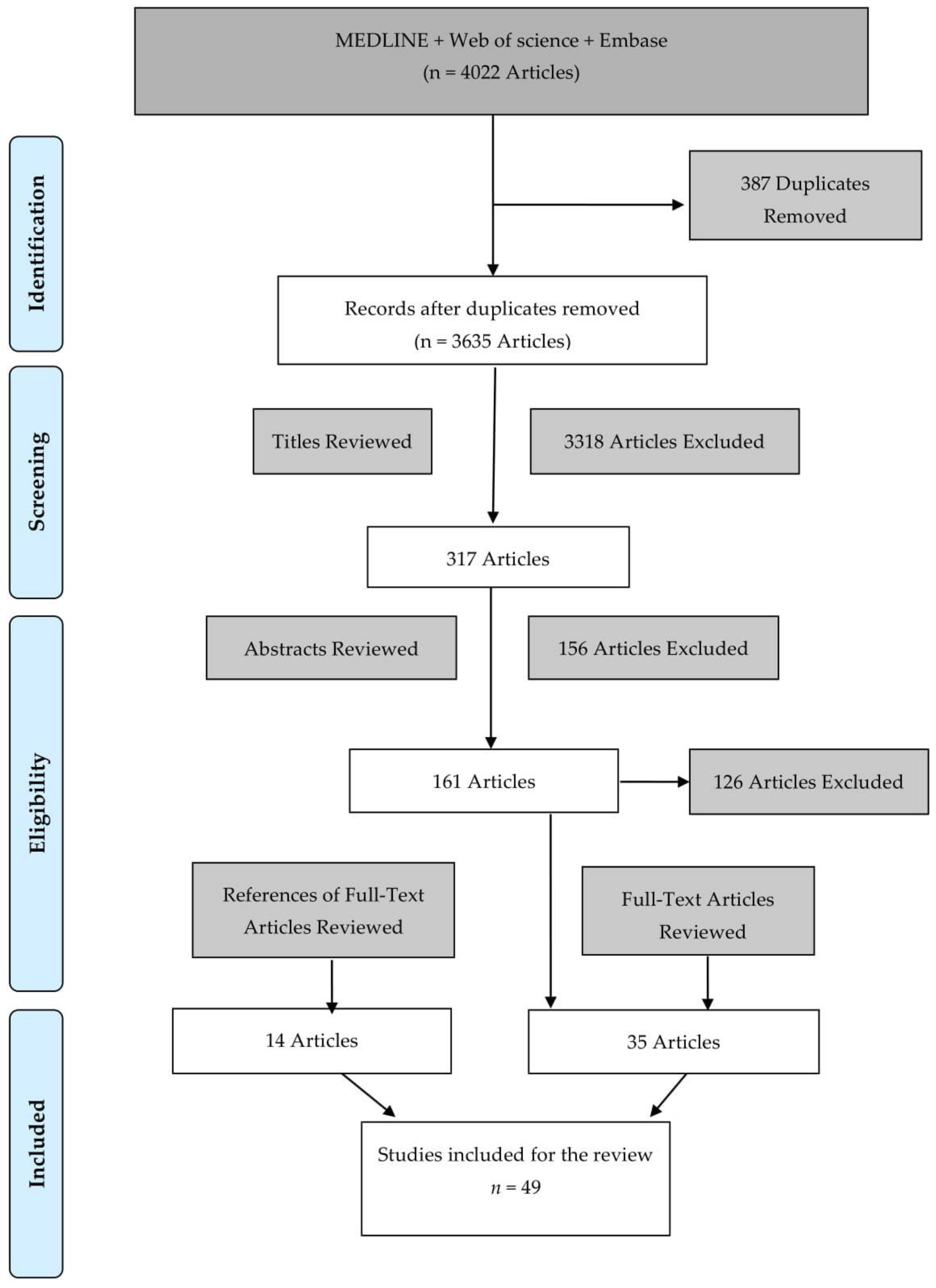
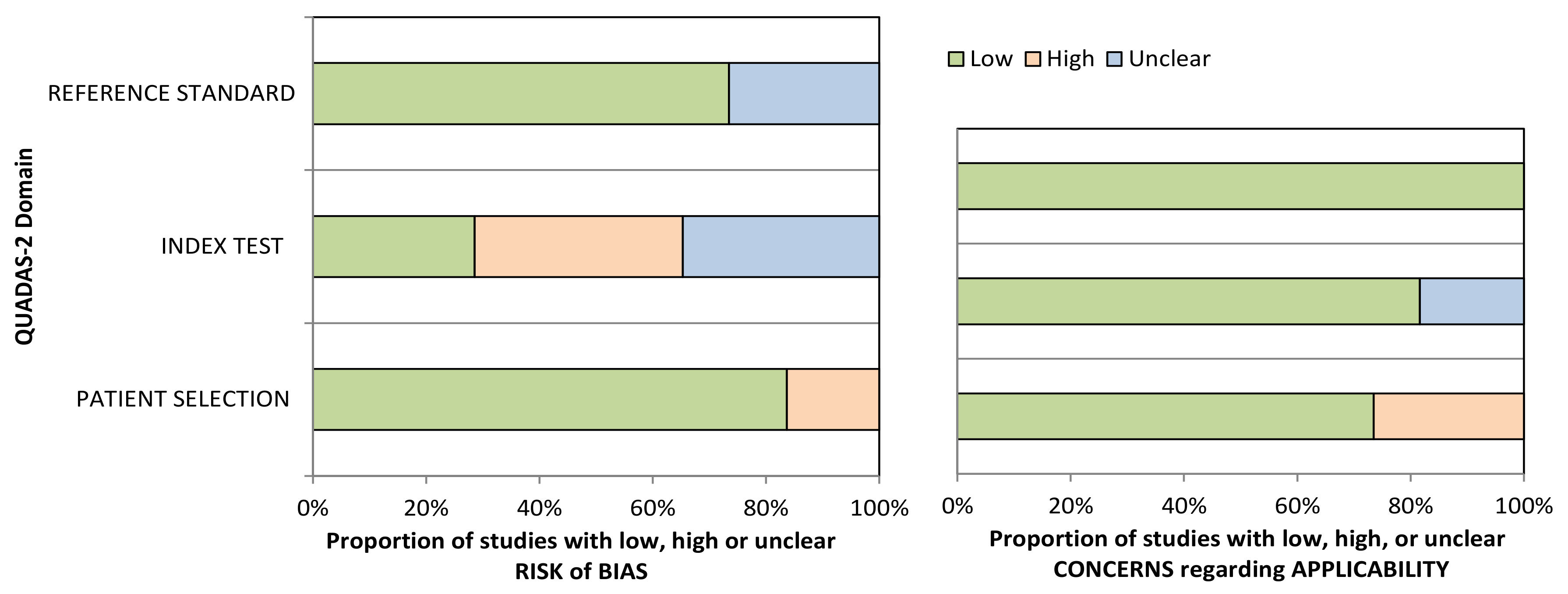
2. Methods
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Nr. | Study | Risk of Bias | Applicability Concerns | Score | ||||
|---|---|---|---|---|---|---|---|---|
| Patient Selection | Index Test | Reference Standard | Patient Selection | Index Test | Reference Standard | |||
| 1 | Gold et al., 2010 [37] | ☺ | ? | ? | ☺ | ☺ | ☺ | Low |
| 2 | Joergensen et al., 2010 [38] | ☺ | ? | ☺ | ☺ | ☺ | ☺ | Low |
| 3 | Marten et al., 2010 [39] | ☹ | ? | ☺ | ☹ | ? | ☺ | High |
| 4 | Brand et al., 2011 [17] | ☺ | ☺ | ? | ☹ | ☺ | ☺ | Low |
| 5 | Park et al., 2012 [21] | ☺ | ? | ☺ | ☺ | ☺ | ☺ | Low |
| 6 | Capello et al., 2013 [40] | ☺ | ☺ | ☺ | ☹ | ☺ | ☺ | Low |
| 7 | Gold et al., 2013 [41] | ☺ | ? | ☺ | ☺ | ☺ | ☺ | Low |
| 8 | Kobayashi et al., 2013 [42] | ☺ | ☹ | ☺ | ☹ | ☺ | ☺ | Low |
| 9 | Li et al., 2013 [43] | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | Low |
| 10 | Zhao et al., 2013 [44] | ☹ | ☹ | ? | ☺ | ☺ | ☺ | High |
| 11 | Chung et al., 2014 [45] | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | Low |
| 12 | Lee et al., 2014 [46] | ☺ | ☺ | ☺ | ☹ | ☺ | ☺ | Low |
| 13 | Nolen et al., 2014 [47] | ☺ | ☺ | ☺ | ☹ | ☺ | ☺ | Low |
| 14 | Ren et al., 2014 [48] | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | Low |
| 15 | Schultz et al., 2014 [49] | ☺ | ? | ☺ | ☺ | ☺ | ☺ | Low |
| 16 | Yang et al., 2014 [50] | ☺ | ☹ | ? | ☹ | ? | ☺ | High |
| 17 | Zhang et al., 2014 [51] | ☺ | ? | ☺ | ☺ | ☺ | ☺ | Low |
| 18 | Debernardi et al., 2015 [52] | ☹ | ? | ? | ☺ | ☺ | ☺ | High |
| 19 | Han et al., 2015 [53] | ☺ | ☹ | ☺ | ☺ | ☺ | ☺ | Low |
| 20 | Melo et al., 2015 [54] | ☺ | ? | ☺ | ☺ | ☺ | ☺ | Low |
| 21 | Radon et al., 2015 [55] | ☺ | ? | ☺ | ☺ | ☺ | ☺ | Low |
| 22 | Ankeny et al., 2016 [56] | ☺ | ☹ | ? | ☺ | ? | ☺ | High |
| 23 | Guo et al., 2016 [57] | ☺ | ☺ | ☺ | ☹ | ☺ | ☺ | Low |
| 24 | Henriksen et al., 2016 [58] | ☺ | ☹ | ? | ☺ | ☺ | ☺ | Low |
| 25 | Sogawa et al., 2016 [59] | ☺ | ☹ | ☺ | ☺ | ☺ | ☺ | Low |
| 26 | Yoneyama et al., 2016 [60] | ☺ | ? | ☺ | ☹ | ☺ | ☺ | Low |
| 27 | Balasenthil et al., 2017 [61] | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | Low |
| 28 | Yang et al., 2017 [62] | ☺ | ? | ☺ | ☺ | ? | ☺ | Low |
| 29 | Capello et al., 2017 [63] | ☺ | ? | ☺ | ☺ | ☺ | ☺ | Low |
| 30 | Hussein et al., 2017 [64] | ☹ | ☹ | ☺ | ☹ | ☺ | ☺ | High |
| 31 | Kaur et al., 2017 [65] | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | Low |
| 32 | Kim et al., 2017 [66] | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | Low |
| 33 | Lai et al., 2017 [67] | ☹ | ☹ | ☺ | ☹ | ☺ | ☺ | High |
| 34 | Park et al., 2017 [68] | ☺ | ☹ | ☺ | ☺ | ☺ | ☺ | Low |
| 35 | Schott et al., 2017 [69] | ☹ | ☹ | ? | ☺ | ☺ | ☺ | High |
| 36 | Arasaradnam et al., 2018 [70] | ☹ | ? | ? | ☺ | ☺ | ☺ | High |
| 37 | Dong et al., 2018 [71] | ☺ | ? | ☺ | ☺ | ☺ | ☺ | Low |
| 38 | Guo et al., 2018 [72] | ☹ | ☹ | ? | ☺ | ☺ | ☺ | High |
| 39 | Mellby et al., 2018 [74] | ☺ | ? | ☺ | ☺ | ☺ | ☺ | Low |
| 40 | Traeger et al., 2018 [75] | ☺ | ☹ | ☺ | ☺ | ☺ | ☺ | Low |
| 41 | Zhou et al., 2018 [76] | ☺ | ☹ | ☺ | ☹ | ? | ☺ | High |
| 42 | Berger et al., 2019 [77] | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | Low |
| 43 | Eissa et al., 2019 [78] | ☺ | ☹ | ? | ☺ | ☺ | ☺ | Low |
| 44 | Fahrmann et al., 2019 [79] | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | Low |
| 45 | Lewis et al., 2019 [73] | ☺ | ? | ? | ☹ | ? | ☺ | High |
| 46 | Yu et al., 2019 [80] | ☺ | ☹ | ☺ | ☺ | ☺ | ☺ | Low |
| 47 | Takahashi et al., 2019 [81] | ☺ | ☹ | ? | ☺ | ? | ☺ | High |
| 48 | Wei et al., 2019 [82] | ☺ | ☹ | ☺ | ☺ | ? | ☺ | Low |
| 49 | Yang et al., 2020 [83] | ☺ | ☺ | ☺ | ☺ | ? | ☺ | Low |
References
- Pereira, S.P.; Oldfield, L.; Ney, A.; Hart, P.A.; Keane, M.G.; Pandol, S.J.; Li, D.; Greenhalf, W.; Jeon, C.Y.; Koay, E.J.; et al. Early detection of pancreatic cancer. Lancet Gastroenterol. Hepatol. 2020, 5, 698–710. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- da Costa, W.L., Jr.; Oluyomi, A.O.; Thrift, A.P. Trends in the Incidence of Pancreatic Adenocarcinoma in All 50 United States Examined Through an Age-Period-Cohort Analysis. JNCI Cancer Spectr. 2020, 4, pkaa033. [Google Scholar] [CrossRef]
- Rawla, P.; Sunkara, T.; Gaduputi, V. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors. World J. Oncol. 2019, 10, 10–27. [Google Scholar] [CrossRef]
- Lin, Q.J.; Yang, F.; Jin, C.; Fu, D.L. Current status and progress of pancreatic cancer in China. World J. Gastroenterol. 2015, 21, 7988–8003. [Google Scholar] [CrossRef]
- Shen, G.Q.; Aleassa, E.M.; Walsh, R.M.; Morris-Stiff, G. Next-Generation Sequencing in Pancreatic Cancer. Pancreas 2019, 48, 739–748. [Google Scholar] [CrossRef] [PubMed]
- Bortesi, L.; Pesci, A.; Bogina, G.; Castelli, P.; Zamboni, G. Ductal Adenocarcinoma of the Pancreas. Surg. Pathol. Clin. 2011, 4, 487–521. [Google Scholar] [CrossRef]
- CancerResearchUK. Pancreatic Cancer Statistics 2015–2017. Available online: http://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/pancreatic-cancer (accessed on 15 July 2020).
- Pancreatic Cancer UK. Pancreatic Cancer Statistics. Available online: https://www.pancreaticcancer.org.uk/what-we-do/media-centre/pancreatic-cancer-statistics (accessed on 2 July 2020).
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Jansen, L.; Balavarca, Y.; Molina-Montes, E.; Babaei, M.; van der Geest, L.; Lemmens, V.; Van Eycken, L.; De Schutter, H.; Johannesen, T.B.; et al. Resection of pancreatic cancer in Europe and USA: An international large-scale study highlighting large variations. Gut 2019, 68, 130. [Google Scholar] [CrossRef]
- Shimizu, Y.; Yasui, K.; Matsueda, K.; Yanagisawa, A.; Yamao, K. Small carcinoma of the pancreas is curable: New computed tomography finding, pathological study and postoperative results from a single institute. J. Gastroenterol. Hepatol. 2005, 20, 1591–1594. [Google Scholar] [CrossRef]
- Ishikawa, O.; Ohigashi, H.; Imaoka, S.; Nakaizumi, A.; Uehara, H.; Kitamura, T.; Kuroda, C. Minute carcinoma of the pancreas measuring 1 cm or less in diameter—Collective review of Japanese case reports. Hepatogastroenterology 1999, 46, 8–15. [Google Scholar]
- Yachida, S.; Jones, S.; Bozic, I.; Antal, T.; Leary, R.; Fu, B.; Kamiyama, M.; Hruban, R.H.; Eshleman, J.R.; Nowak, M.A.; et al. Distant metastasis occurs late during the genetic evolution of pancreatic cancer. Nature 2010, 467, 1114–1117. [Google Scholar] [CrossRef] [Green Version]
- Ghaneh, P.; Costello, E.; Neoptolemos, J.P. Biology and management of pancreatic cancer. Gut 2007, 56, 1134–1152. [Google Scholar] [CrossRef]
- Brand, R.E.; Nolen, B.M.; Zeh, H.J.; Allen, P.J.; Eloubeidi, M.A.; Goldberg, M.; Elton, E.; Arnoletti, J.P.; Christein, J.D.; Vickers, S.M.; et al. Serum biomarker panels for the detection of pancreatic cancer. Clin. Cancer Res. 2011, 17, 805–816. [Google Scholar] [CrossRef] [Green Version]
- Chan, A.; Diamandis, E.P.; Blasutig, I.M. Strategies for discovering novel pancreatic cancer biomarkers. J. Proteom. 2013, 81, 126–134. [Google Scholar] [CrossRef] [Green Version]
- Tempero, M.A.; Uchida, E.; Takasaki, H.; Burnett, D.A.; Steplewski, Z.; Pour, P.M. Relationship of carbohydrate antigen 19-9 and Lewis antigens in pancreatic cancer. Cancer Res. 1987, 47, 5501–5503. [Google Scholar]
- FDA. FDA 510K Summary. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf2/K020566.pdf (accessed on 20 February 2021).
- Park, H.-D.; Kang, E.-S.; Kim, J.-W.; Lee, K.-T.; Lee, K.H.; Park, Y.S.; Park, J.-O.; Lee, J.; Heo, J.S.; Choi, S.H.; et al. Serum CA19-9, cathepsin D, and matrix metalloproteinase-7 as a diagnostic panel for pancreatic ductal adenocarcinoma. Proteomics 2012, 12, 3590–3597. [Google Scholar] [CrossRef] [PubMed]
- Ritts, R.E.; Pitt, H.A. CA 19-9 in pancreatic cancer. Surg. Oncol. Clin. N. Am. 1998, 7, 93–101. [Google Scholar] [CrossRef]
- Duffy, M.J.; van Dalen, A.; Haglund, C.; Hansson, L.; Klapdor, R.; Lamerz, R.; Nilsson, O.; Sturgeon, C.; Topolcan, O. Clinical utility of biochemical markers in colorectal cancer: European Group on Tumour Markers (EGTM) guidelines. Eur. J. Cancer 2003, 39, 718–727. [Google Scholar] [CrossRef]
- Ballehaninna, U.K.; Chamberlain, R.S. The clinical utility of serum CA 19-9 in the diagnosis, prognosis and management of pancreatic adenocarcinoma: An evidence based appraisal. J. Gastrointest. Oncol. 2012, 3, 105–119. [Google Scholar] [CrossRef]
- Passerini, R.; Cassatella, M.C.; Boveri, S.; Salvatici, M.; Radice, D.; Zorzino, L.; Galli, C.; Sandri, M.T. The pitfalls of CA19-9: Routine testing and comparison of two automated immunoassays in a reference oncology center. Am. J. Clin. Pathol. 2012, 138, 281–287. [Google Scholar] [CrossRef] [Green Version]
- Duffy, M.J.; Sturgeon, C.; Lamerz, R.; Haglund, C.; Holubec, V.L.; Klapdor, R.; Nicolini, A.; Topolcan, O.; Heinemann, V. Tumor markers in pancreatic cancer: A European Group on Tumor Markers (EGTM) status report. Ann. Oncol. 2010, 21, 441–447. [Google Scholar] [CrossRef]
- Herlyn, M.; Steplewski, Z.; Herlyn, D.; Koprowski, H. Colorectal carcinoma-specific antigen: Detection by means of monoclonal antibodies. Proc. Natl. Acad. Sci. USA 1979, 76, 1438–1442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hotakainen, K.; Tanner, P.; Alfthan, H.; Haglund, C.; Stenman, U.H. Comparison of three immunoassays for CA 19-9. Clin. Chim. Acta 2009, 400, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, W. The clinical utility of the CA 19-9 tumor-associated antigen. Am. J. Gastroenterol. 1990, 85, 350–355. [Google Scholar]
- Stern, P.; Friedecky, B.; Bartos, V.; Bezdickova, D.; Vavrova, J.; Uhrova, J.; Rozprimova, L.; Zima, T.; Palicka, V. Comparison of different immunoassays for CA 19-9. Clin. Chem. Lab. Med. 2001, 39, 1278–1282. [Google Scholar] [CrossRef]
- Goh, S.K.; Gold, G.; Christophi, C.; Muralidharan, V. Serum carbohydrate antigen 19-9 in pancreatic adenocarcinoma: A mini review for surgeons. ANZ J. Surg. 2017, 87, 987–992. [Google Scholar] [CrossRef]
- Jain, K.K. The Handbook of Biomarkers; Humana Press: Totowa, NJ, USA, 2010. [Google Scholar]
- Young, M.R.; Wagner, P.D.; Ghosh, S.; Rinaudo, J.A.; Baker, S.G.; Zaret, K.S.; Goggins, M.; Srivastava, S. Validation of Biomarkers for Early Detection of Pancreatic Cancer: Summary of The Alliance of Pancreatic Cancer Consortia for Biomarkers for Early Detection Workshop. Pancreas 2018, 47, 135–141. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PloS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Whiting, P.; Rutjes, A.W.; Reitsma, J.B.; Bossuyt, P.M.; Kleijnen, J. The development of QUADAS: A tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med. Res. Methodol. 2003, 3, 25. [Google Scholar] [CrossRef] [Green Version]
- Gold, D.V.; Goggins, M.; Modrak, D.E.; Newsome, G.; Liu, M.; Shi, C.; Hruban, R.H.; Goldenberg, D.M. Detection of early-stage pancreatic adenocarcinoma. Cancer Epidemiol. Biomark. Prev. 2010, 19, 2786–2794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joergensen, M.T.; Brunner, N.; De Muckadell, O.B.S. Comparison of Circulating MMP-9, TIMP-1 and CA19-9 in the Detection of Pancreatic Cancer. Anticancer Res. 2010, 30, 587–592. [Google Scholar] [PubMed]
- Marten, A.; Buchler, M.W.; Werft, W.; Wente, M.N.; Kirschfink, M.; Schmidt, J. Soluble iC3b as an Early Marker for Pancreatic Adenocarcinoma Is Superior to CA19.9 and Radiology. J. Immunother. 2010, 33, 219–224. [Google Scholar] [CrossRef]
- Capello, M.; Cappello, P.; Linty, F.C.; Chiarle, R.; Sperduti, I.; Novarino, A.; Salacone, P.; Mandili, G.; Naccarati, A.; Sacerdote, C.; et al. Autoantibodies to Ezrin are an early sign of pancreatic cancer in humans and in genetically engineered mouse models. J. Hematol. Oncol. 2013, 6, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gold, D.V.; Gaedcke, J.; Ghadimi, B.M.; Goggins, M.; Hruban, R.H.; Liu, M.L.; Newsome, G.; Goldenberg, D.M. PAM4 enzyme immunoassay alone and in combination with CA 19-9 for the detection of pancreatic adenocarcinoma. Cancer 2013, 119, 522–528. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, T.; Nishiumi, S.; Ikeda, A.; Yoshie, T.; Sakai, A.; Matsubara, A.; Izumi, Y.; Tsumura, H.; Tsuda, M.; Nishisaki, H.; et al. A novel serum metabolomics-based diagnostic approach to pancreatic cancer. Cancer Epidemiol. Biomark. Prev. 2013, 22, 571–579. [Google Scholar] [CrossRef] [Green Version]
- Li, A.; Yu, J.; Kim, H.; Wolfgang, C.L.; Canto, M.I.; Hruban, R.H.; Goggins, M. MicroRNA array analysis finds elevated serum miR-1290 accurately distinguishes patients with low-stage pancreatic cancer from healthy and disease controls. Clin. Cancer Res. 2013, 19, 3600–3610. [Google Scholar] [CrossRef] [Green Version]
- Zhao, C.; Zhang, J.; Zhang, S.; Yu, D.; Chen, Y.; Liu, Q.; Shi, M.; Ni, C.; Zhu, M. Diagnostic and biological significance of microRNA-192 in pancreatic ductal adenocarcinoma. Oncol. Rep. 2013, 30, 276–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, H.W.; Lim, J.B. Clinical significance of elevated serum soluble CD40 ligand levels as a diagnostic and prognostic tumor marker for pancreatic ductal adenocarcinoma. J. Transl. Med. 2014, 12, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.J.; Na, K.; Jeong, S.K.; Lim, J.S.; Kim, S.A.; Song, S.Y.; Kim, H.; Hancock, W.S.; Paik, Y.K. Identification of human complement factor B as a novel biomarker candidate for pancreatic ductal adenocarcinoma. J. Proteome Res. 2014, 13, 4878–4888. [Google Scholar] [CrossRef] [PubMed]
- Nolen, B.M.; Brand, R.E.; Prosser, D.; Velikokhatnaya, L.; Allen, P.J.; Zeh, H.J.; Grizzle, W.E.; Huang, Y.; Lomakin, A.; Lokshin, A.E. Prediagnostic serum biomarkers as early detection tools for pancreatic cancer in a large prospective cohort study. PLoS ONE 2014, 9, e94928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, C.; Chen, Y.; Han, C.; Fu, D.; Chen, H. Plasma interleukin-11 (IL-11) levels have diagnostic and prognostic roles in patients with pancreatic cancer. Tumour Biol. 2014, 35, 11467–11472. [Google Scholar] [CrossRef]
- Schultz, N.A.; Dehlendorff, C.; Jensen, B.V.; Bjerregaard, J.K.; Nielsen, K.R.; Bojesen, S.E.; Calatayud, D.; Nielsen, S.E.; Yilmaz, M.; Holländer, N.H.; et al. MicroRNA biomarkers in whole blood for detection of pancreatic cancer. JAMA 2014, 311, 392–404. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.Y.; Sun, Y.W.; Liu, D.J.; Zhang, J.F.; Li, J.; Hua, R. MicroRNAs in stool samples as potential screening biomarkers for pancreatic ductal adenocarcinoma cancer. Am. J. Cancer Res. 2014, 4, 663–673. [Google Scholar] [PubMed]
- Zhang, P.J.; Zou, M.; Wen, X.Y.; Gu, F.; Li, J.; Liu, G.X.; Dong, J.X.; Deng, X.X.; Gao, J.; Li, X.L.; et al. Development of serum parameters panels for the early detection of pancreatic cancer. Int. J. Cancer 2014, 134, 2646–2655. [Google Scholar] [CrossRef]
- Debernardi, S.; Massat, N.J.; Radon, T.P.; Sangaralingam, A.; Banissi, A.; Ennis, D.P.; Dowe, T.; Chelala, C.; Pereira, S.P.; Kocher, H.M.; et al. Noninvasive urinary miRNA biomarkers for early detection of pancreatic adenocarcinoma. Am. J. Cancer Res. 2015, 5, 3455–3466. [Google Scholar]
- Han, S.X.; Zhou, X.; Sui, X.; He, C.C.; Cai, M.J.; Ma, J.L.; Zhang, Y.Y.; Zhou, C.Y.; Ma, C.X.; Varela-Ramirez, A.; et al. Serum dickkopf-1 is a novel serological biomarker for the diagnosis and prognosis of pancreatic cancer. Oncotarget 2015, 6, 19907–19917. [Google Scholar] [CrossRef] [Green Version]
- Melo, S.A.; Luecke, L.B.; Kahlert, C.; Fernandez, A.F.; Gammon, S.T.; Kaye, J.; LeBleu, V.S.; Mittendorf, E.A.; Weitz, J.; Rahbari, N.; et al. Glypican-1 identifies cancer exosomes and detects early pancreatic cancer. Nature 2015, 523, 177–182. [Google Scholar] [CrossRef] [Green Version]
- Radon, T.P.; Massat, N.J.; Jones, R.; Alrawashdeh, W.; Dumartin, L.; Ennis, D.; Duffy, S.W.; Kocher, H.M.; Pereira, S.P.; Guarner, L.; et al. Identification of a Three-Biomarker Panel in Urine for Early Detection of Pancreatic Adenocarcinoma. Clin. Cancer Res. 2015, 21, 3512–3521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ankeny, J.S.; Court, C.M.; Hou, S.; Li, Q.; Song, M.; Wu, D.; Chen, J.F.; Lee, T.; Lin, M.; Sho, S.; et al. Circulating tumour cells as a biomarker for diagnosis and staging in pancreatic cancer. Br. J. Cancer 2016, 114, 1367–1375. [Google Scholar] [CrossRef] [Green Version]
- Guo, X.; Lv, X.; Fang, C.; Wang, F.; Wang, D.; Zhao, J.; Ma, Y.; Xue, Y.; Bai, Q.; Yao, X.; et al. Dysbindin as a novel biomarker for pancreatic ductal adenocarcinoma identified by proteomic profiling. Int. J. Cancer 2016, 139, 1821–1829. [Google Scholar] [CrossRef] [Green Version]
- Henriksen, S.D.; Madsen, P.H.; Larsen, A.C.; Johansen, M.B.; Drewes, A.M.; Pedersen, I.S.; Krarup, H.; Thorlacius-Ussing, O. Cell-free DNA promoter hypermethylation in plasma as a diagnostic marker for pancreatic adenocarcinoma. Clin. Epigenetics 2016, 8, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Sogawa, K.; Takano, S.; Iida, F.; Satoh, M.; Tsuchida, S.; Kawashima, Y.; Yoshitomi, H.; Sanda, A.; Kodera, Y.; Takizawa, H.; et al. Identification of a novel serum biomarker for pancreatic cancer, C4b-binding protein α-chain (C4BPA) by quantitative proteomic analysis using tandem mass tags. Br. J. Cancer 2016, 115, 949–956. [Google Scholar] [CrossRef]
- Yoneyama, T.; Ohtsuki, S.; Honda, K.; Kobayashi, M.; Iwasaki, M.; Uchida, Y.; Okusaka, T.; Nakamori, S.; Shimahara, M.; Ueno, T.; et al. Identification of IGFBP2 and IGFBP3 As Compensatory Biomarkers for CA19-9 in Early-Stage Pancreatic Cancer Using a Combination of Antibody-Based and LC-MS/MS-Based Proteomics. PLoS ONE 2016, 11, e0161009. [Google Scholar] [CrossRef] [PubMed]
- Balasenthil, S.; Huang, Y.; Liu, S.; Marsh, T.; Chen, J.; Stass, S.A.; KuKuruga, D.; Brand, R.; Chen, N.; Frazier, M.L.; et al. A Plasma Biomarker Panel to Identify Surgically Resectable Early-Stage Pancreatic Cancer. J. Natl. Cancer Inst. 2017, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, K.S.; Im, H.; Hong, S.; Pergolini, I.; del Castillo, A.F.; Wang, R.; Clardy, S.; Huang, C.-H.; Pille, C.; Ferrone, S.; et al. Multiparametric plasma EV profiling facilitates diagnosis of pancreatic malignancy. Sci. Transl. Med. 2017, 9, eaal3226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capello, M.; Bantis, L.; Scelo, G.; Zhao, Y.; Dhillon, D.; Wang, H.; Abbruzzese, J.; Maitra, A.; Tempero, M.; Brand, R.; et al. Sequential validation of bloodbased protein biomarker candidates for early-stage pancreatic cancer. In Proceedings of the 107th Annual Meeting of the American Association for Cancer Research, AACR 2016, New Orleans, LA, USA, 16–20 April 2016; Volume 76. [Google Scholar]
- Hussein, N.A.; Kholy, Z.A.; Anwar, M.M.; Ahmad, M.A.; Ahmad, S.M. Plasma miR-22-3p, miR-642b-3p and miR-885-5p as diagnostic biomarkers for pancreatic cancer. J. Cancer Res. Clin. Oncol. 2017, 143, 83–93. [Google Scholar] [CrossRef]
- Kaur, S.; Smith, L.; Patel, A.; Menning, M.; Watley, D.; Malik, S.; Krishn, S.; Mallya, K.; Aithal, A.; Sasson, A.; et al. A Combination of MUC5AC and CA19-9 Improves the Diagnosis of Pancreatic Cancer: A Multicenter Study. Am. J. Gastroenterol. 2017, 112, 172–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Bamlet, W.R.; Oberg, A.L.; Chaffee, K.G.; Donahue, G.; Cao, X.J.; Chari, S.; Garcia, B.A.; Petersen, G.M.; Zaret, K.S. Detection of early pancreatic ductal adenocarcinoma with thrombospondin-2 and CA19-9 blood markers. Sci. Transl. Med. 2017, 9, eaah5583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, X.Y.; Wang, M.; McElyea, S.D.; Sherman, S.; House, M.; Korc, M. A microRNA signature in circulating exosomes is superior to exosomal glypican-1 levels for diagnosing pancreatic cancer. Cancer Lett. 2017, 393, 86–93. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Choi, Y.; Namkung, J.; Yi, S.G.; Kim, H.; Yu, J.; Kim, Y.; Kwon, M.S.; Kwon, W.; Oh, D.Y.; et al. Diagnostic performance enhancement of pancreatic cancer using proteomic multimarker panel. Oncotarget 2017, 8, 93117–93130. [Google Scholar] [CrossRef] [Green Version]
- Schott, S.; Yang, R.X.; Stocker, S.; Canzian, F.; Giese, N.; Bugert, P.; Bergmann, F.; Strobel, O.; Hackert, T.; Sohn, C.; et al. HYAL2 methylation in peripheral blood as a potential marker for the detection of pancreatic cancer-a case control study. Oncotarget 2017, 8, 67614–67625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arasaradnam, R.P.; Wicaksono, A.; O’Brien, H.; Kocher, H.M.; Covington, J.A.; Crnogorac-Jurcevic, T. Noninvasive Diagnosis of Pancreatic Cancer Through Detection of Volatile Organic Compounds in Urine. Gastroenterology 2018, 154, 485–487.e481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, D.; Jia, L.; Zhang, L.; Ma, N.; Zhang, A.; Zhou, Y.; Ren, L. Periostin and CA242 as potential diagnostic serum biomarkers complementing CA19.9 in detecting pancreatic cancer. Cancer Sci. 2018, 109, 2841–2851. [Google Scholar] [CrossRef] [Green Version]
- Guo, X.B.; Yin, H.S.; Wang, J.Y. Evaluating the diagnostic and prognostic value of long non-coding RNA SNHG15 in pancreatic ductal adenocarcinoma. Eur. Rev. Med. Pharm. Sci. 2018, 22, 5892–5898. [Google Scholar] [CrossRef]
- Lewis, J.M.; Vyas, A.D.; Qiu, Y.; Messer, K.S.; White, R.; Heller, M.J. Integrated Analysis of Exosomal Protein Biomarkers on Alternating Current Electrokinetic Chips Enables Rapid Detection of Pancreatic Cancer in Patient Blood. ACS Nano 2018, 12, 3311–3320. [Google Scholar] [CrossRef]
- Mellby, L.D.; Nyberg, A.P.; Johansen, J.S.; Wingren, C.; Nordestgaard, B.G.; Bojesen, S.E.; Mitchell, B.L.; Sheppard, B.C.; Sears, R.C.; Borrebaeck, C.A.K. Serum Biomarker Signature-Based Liquid Biopsy for Diagnosis of Early-Stage Pancreatic Cancer. J. Clin. Oncol. 2018, 36, 2887–2894. [Google Scholar] [CrossRef] [PubMed]
- Michael Traeger, M.; Rehkaemper, J.; Ullerich, H.; Steinestel, K.; Wardelmann, E.; Senninger, N.; Abdallah Dhayat, S. The ambiguous role of microRNA-205 and its clinical potential in pancreatic ductal adenocarcinoma. J. Cancer Res. Clin. Oncol. 2018, 144, 2419–2431. [Google Scholar] [CrossRef]
- Zhou, C.Y.; Dong, Y.P.; Sun, X.; Sui, X.; Zhu, H.; Zhao, Y.Q.; Zhang, Y.Y.; Mason, C.; Zhu, Q.; Han, S.X. High levels of serum glypican-1 indicate poor prognosis in pancreatic ductal adenocarcinoma. Cancer Med. 2018, 7, 5525–5533. [Google Scholar] [CrossRef] [Green Version]
- Berger, A.W.; Schwerdel, D.; Reinacher-Schick, A.; Uhl, W.; Algül, H.; Friess, H.; Janssen, K.-P.; König, A.; Ghadimi, M.; Gallmeier, E.; et al. A Blood-Based Multi Marker Assay Supports the Differential Diagnosis of Early-Stage Pancreatic Cancer. Theranostics 2019, 9, 1280–1287. [Google Scholar] [CrossRef]
- Eissa, M.A.L.; Lerner, L.; Abdelfatah, E.; Shankar, N.; Canner, J.K.; Hasan, N.M.; Yaghoobi, V.; Huang, B.; Kerner, Z.; Takaesu, F.; et al. Promoter methylation of ADAMTS1 and BNC1 as potential biomarkers for early detection of pancreatic cancer in blood. Clin. Epigenetics 2019, 11, 59. [Google Scholar] [CrossRef] [PubMed]
- Fahrmann, J.F.; Bantis, L.E.; Capello, M.; Scelo, G.; Dennison, J.B.; Patel, N.; Murage, E.; Vykoukal, J.; Kundnani, D.L.; Foretova, L.; et al. A Plasma-Derived Protein-Metabolite Multiplexed Panel for Early-Stage Pancreatic Cancer. J. Natl. Cancer Inst. 2019, 111, 372–379. [Google Scholar] [CrossRef]
- Yu, S.; Li, Y.; Liao, Z.; Wang, Z.; Wang, Z.; Li, Y.; Qian, L.; Zhao, J.; Zong, H.; Kang, B.; et al. Plasma extracellular vesicle long RNA profiling identifies a diagnostic signature for the detection of pancreatic ductal adenocarcinoma. Gut 2020, 69, 540–550. [Google Scholar] [CrossRef]
- Takahashi, K.; Ota, Y.; Kogure, T.; Suzuki, Y.; Iwamoto, H.; Yamakita, K.; Kitano, Y.; Fujii, S.; Haneda, M.; Patel, T.; et al. Circulating extracellular vesicle-encapsulated HULC is a potential biomarker for human pancreatic cancer. Cancer Sci. 2020, 111, 98–111. [Google Scholar] [CrossRef] [Green Version]
- Wei, T.; Zhang, X.; Zhang, Q.; Yang, J.; Chen, Q.; Wang, J.; Li, X.; Chen, J.; Ma, T.; Li, G.; et al. Vimentin-positive circulating tumor cells as a biomarker for diagnosis and treatment monitoring in patients with pancreatic cancer. Cancer Lett. 2019, 452, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; LaRiviere, M.J.; Ko, J.; Till, J.E.; Christensen, T.; Yee, S.S.; Black, T.A.; Tien, K.; Lin, A.; Shen, H.; et al. A Multianalyte Panel Consisting of Extracellular Vesicle miRNAs and mRNAs, cfDNA, and CA19-9 Shows Utility for Diagnosis and Staging of Pancreatic Ductal Adenocarcinoma. Clin. Cancer Res. 2020, 26, 3248–3258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pang, Y.; Holmes, M.V.; Chen, Z.; Kartsonaki, C. A review of lifestyle, metabolic risk factors, and blood-based biomarkers for early diagnosis of pancreatic ductal adenocarcinoma. J. Gastroenterol. Hepatol. 2019, 34, 330–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, A.E.; Hernandez, Y.G.; Frucht, H.; Lucas, A.L. Pancreatic ductal adenocarcinoma: Risk factors, screening, and early detection. World J. Gastroenterol. 2014, 20, 11182–11198. [Google Scholar] [CrossRef]
- Ghatnekar, O.; Andersson, R.; Svensson, M.; Persson, U.; Ringdahl, U.; Zeilon, P.; Borrebaeck, C.A. Modelling the benefits of early diagnosis of pancreatic cancer using a biomarker signature. Int. J. Cancer 2013, 133, 2392–2397. [Google Scholar] [CrossRef] [PubMed]
- Frampton, A.E.; Prado, M.M.; López-Jiménez, E.; Fajardo-Puerta, A.B.; Jawad, Z.A.R.; Lawton, P.; Giovannetti, E.; Habib, N.A.; Castellano, L.; Stebbing, J.; et al. Glypican-1 is enriched in circulating-exosomes in pancreatic cancer and correlates with tumor burden. Oncotarget 2018, 9, 19006–19013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, W.H.; Wang, W.Q.; Han, X.; Gao, H.L.; Li, T.J.; Xu, S.S.; Li, S.; Xu, H.X.; Li, H.; Ye, L.Y.; et al. Advances on diagnostic biomarkers of pancreatic ductal adenocarcinoma: A systems biology perspective. Comput. Struct. Biotechnol. J. 2020, 18, 3606–3614. [Google Scholar] [CrossRef]
- Almeida, P.P.; Cardoso, C.P.; de Freitas, L.M. PDAC-ANN: An artificial neural network to predict pancreatic ductal adenocarcinoma based on gene expression. BMC Cancer 2020, 20, 82. [Google Scholar] [CrossRef] [Green Version]
- Muhammad, W.; Hart, G.R.; Nartowt, B.; Farrell, J.J.; Johung, K.; Liang, Y.; Deng, J. Pancreatic Cancer Prediction Through an Artificial Neural Network. Front. Artif. Intell. 2019, 2, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marya, N.B.; Powers, P.D.; Chari, S.T.; Gleeson, F.C.; Leggett, C.L.; Abu Dayyeh, B.K.; Chandrasekhara, V.; Iyer, P.G.; Majumder, S.; Pearson, R.K.; et al. Utilisation of artificial intelligence for the development of an EUS-convolutional neural network model trained to enhance the diagnosis of autoimmune pancreatitis. Gut 2020. [Google Scholar] [CrossRef] [PubMed]
- Khatri, I.; Bhasin, M.K. A Transcriptomics-Based Meta-Analysis Combined With Machine Learning Identifies a Secretory Biomarker Panel for Diagnosis of Pancreatic Adenocarcinoma. Front. Genet. 2020, 11, 572284. [Google Scholar] [CrossRef] [PubMed]
- Chung, W.Y.; Correa, E.; Yoshimura, K.; Chang, M.C.; Dennison, A.; Takeda, S.; Chang, Y.T. Using probe electrospray ionization mass spectrometry and machine learning for detecting pancreatic cancer with high performance. Am. J. Transl. Res. 2020, 12, 171–179. [Google Scholar] [PubMed]
- Sollie, S.; Michaud, D.S.; Sarker, D.; Karagiannis, S.N.; Josephs, D.H.; Hammar, N.; Santaolalla, A.; Walldius, G.; Garmo, H.; Holmberg, L.; et al. Chronic inflammation markers are associated with risk of pancreatic cancer in the Swedish AMORIS cohort study. BMC Cancer 2019, 19, 858. [Google Scholar] [CrossRef] [Green Version]
- de la Fuente, J.; Sharma, A.; Chari, S.; Majumder, S. Peripheral blood monocyte counts are elevated in the pre-diagnostic phase of pancreatic cancer: A population based study. Pancreatology 2019, 19, 1043–1048. [Google Scholar] [CrossRef]
- Cui, Y.; Shu, X.O.; Li, H.L.; Yang, G.; Wen, W.; Gao, Y.T.; Cai, Q.; Rothman, N.; Yin, H.Y.; Lan, Q.; et al. Prospective study of urinary prostaglandin E2 metabolite and pancreatic cancer risk. Int. J. Cancer 2017, 141, 2423–2429. [Google Scholar] [CrossRef] [PubMed]
- Jenkinson, C.; Elliott, V.L.; Evans, A.; Oldfield, L.; Jenkins, R.E.; O’Brien, D.P.; Apostolidou, S.; Gentry-Maharaj, A.; Fourkala, E.O.; Jacobs, I.J.; et al. Decreased Serum Thrombospondin-1 Levels in Pancreatic Cancer Patients Up to 24 Months Prior to Clinical Diagnosis: Association with Diabetes Mellitus. Clin. Cancer Res. 2016, 22, 1734–1743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, D.P.; Sandanayake, N.S.; Jenkinson, C.; Gentry-Maharaj, A.; Apostolidou, S.; Fourkala, E.O.; Camuzeaux, S.; Blyuss, O.; Gunu, R.; Dawnay, A.; et al. Serum CA19-9 is significantly upregulated up to 2 years before diagnosis with pancreatic cancer: Implications for early disease detection. Clin. Cancer Res. 2015, 21, 622–631. [Google Scholar] [CrossRef] [Green Version]
- Capello, M.; Bantis, L.E.; Scelo, G.; Zhao, Y.; Li, P.; Dhillon, D.S.; Patel, N.J.; Kundnani, D.L.; Wang, H.; Abbruzzese, J.L.; et al. Sequential Validation of Blood-Based Protein Biomarker Candidates for Early-Stage Pancreatic Cancer. J. Natl. Cancer Inst. 2017, 109, djw266. [Google Scholar] [CrossRef] [PubMed]
- Mirus, J.E.; Zhang, Y.; Li, C.I.; Lokshin, A.E.; Prentice, R.L.; Hingorani, S.R.; Lampe, P.D. Cross-species antibody microarray interrogation identifies a 3-protein panel of plasma biomarkers for early diagnosis of pancreas cancer. Clin. Cancer Res. 2015, 21, 1764–1771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magis, A.T.; Rappaport, N.; Conomos, M.P.; Omenn, G.S.; Lovejoy, J.C.; Hood, L.; Price, N.D. Untargeted longitudinal analysis of a wellness cohort identifies markers of metastatic cancer years prior to diagnosis. Sci. Rep. 2020, 10, 16275. [Google Scholar] [CrossRef]
- Moore, H.M.; Kelly, A.B.; Jewell, S.D.; McShane, L.M.; Clark, D.P.; Greenspan, R.; Hayes, D.F.; Hainaut, P.; Kim, P.; Mansfield, E.A.; et al. Biospecimen reporting for improved study quality (BRISQ). Cancer Cytopathol. 2011, 119, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.F.; Korevaar, D.A.; Altman, D.G.; Bruns, D.E.; Gatsonis, C.A.; Hooft, L.; Irwig, L.; Levine, D.; Reitsma, J.B.; de Vet, H.C.W.; et al. STARD 2015 guidelines for reporting diagnostic accuracy studies: Explanation and elaboration. BMJ Open 2016, 6, e012799. [Google Scholar] [CrossRef]
- Altman, D.G.; McShane, L.M.; Sauerbrei, W.; Taube, S.E. Reporting Recommendations for Tumor Marker Prognostic Studies (REMARK): Explanation and elaboration. PLoS Med. 2012, 9, e1001216. [Google Scholar] [CrossRef] [Green Version]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef]
- Crosby, D.; Lyons, N.; Greenwood, E.; Harrison, S.; Hiom, S.; Moffat, J.; Quallo, T.; Samuel, E.; Walker, I. A roadmap for the early detection and diagnosis of cancer. Lancet Oncol. 2020, 21, 1397–1399. [Google Scholar] [CrossRef]
- Kunovsky, L.; Tesarikova, P.; Kala, Z.; Kroupa, R.; Kysela, P.; Dolina, J.; Trna, J. The Use of Biomarkers in Early Diagnostics of Pancreatic Cancer. Can. J. Gastroenterol. Hepatol. 2018, 2018, 5389820. [Google Scholar] [CrossRef] [PubMed]
- Paulovich, A.G.; Whiteaker, J.R.; Hoofnagle, A.N.; Wang, P. The interface between biomarker discovery and clinical validation: The tar pit of the protein biomarker pipeline. Proteom. Clin. Appl. 2008, 2, 1386–1402. [Google Scholar] [CrossRef] [Green Version]
- Rifai, N.; Gillette, M.A.; Carr, S.A. Protein biomarker discovery and validation: The long and uncertain path to clinical utility. Nat. Biotechnol. 2006, 24, 971–983. [Google Scholar] [CrossRef] [PubMed]
- Root, A.; Allen, P.; Tempst, P.; Yu, K. Protein Biomarkers for Early Detection of Pancreatic Ductal Adenocarcinoma: Progress and Challenges. Cancers 2018, 10, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Immunovia. Available online: https://immunovia.com/about-us (accessed on 25 August 2020).
- Debernardi, S.; O’Brien, H.; Algahmdi, A.S.; Malats, N.; Stewart, G.D.; Plješa-Ercegovac, M.; Costello, E.; Greenhalf, W.; Saad, A.; Roberts, R.; et al. A combination of urinary biomarker panel and PancRISK score for earlier detection of pancreatic cancer: A case–control study. PLoS Med. 2020, 17, e1003489. [Google Scholar] [CrossRef] [PubMed]
- Blyuss, O.; Zaikin, A.; Cherepanova, V.; Munblit, D.; Kiseleva, E.M.; Prytomanova, O.M.; Duffy, S.W.; Crnogorac-Jurcevic, T. Development of PancRISK, a urine biomarker-based risk score for stratified screening of pancreatic cancer patients. Br. J. Cancer 2020, 122, 692–696. [Google Scholar] [CrossRef]
- Clinicaltrials.gov. Early Detection of Pancreatic Adenocarcinoma (PDAC) Using a Panel of Biomarkers (UroPanc). Available online: https://clinicaltrials.gov/ct2/show/NCT04449406 (accessed on 3 March 2021).
- Cohen, J.D.; Li, L.; Wang, Y.; Thoburn, C.; Afsari, B.; Danilova, L.; Douville, C.; Javed, A.A.; Wong, F.; Mattox, A.; et al. Detection and localization of surgically resectable cancers with a multi-analyte blood test. Science 2018, 359, 926–930. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.C.; Oxnard, G.R.; Klein, E.A.; Swanton, C.; Seiden, M.V.; Consortium, C. Sensitive and specific multi-cancer detection and localization using methylation signatures in cell-free DNA. Ann. Oncol. 2020, 31, 745–759. [Google Scholar] [CrossRef]
- Killock, D. CancerSEEK and destroy—A blood test for early cancer detection. Nat. Rev. Clin. Oncol. 2018, 15, 133. [Google Scholar] [CrossRef]
| Inclusion Criteria |
|---|
| 1. Pancreatic Ductal Adenocarcinoma |
| 2. Non-invasive method of obtaining a liquid biopsy e.g., plasma, serum, urine, saliva, stool |
| 3. Original data with reported AUC, SN and SP of a proposed biomarker |
| 4. Human studies |
| 5. Manuscripts from January 2010 until August 2020 |
| Exclusion Criteria |
| 1. No specification of what type of pancreatic cancer it was |
| 2. Invasive procedures to obtain the biomarker e.g., tissue biopsy |
| 3. No recorded data either of SN, SP and/or AUC for the tested biomarker |
| 4. Biomarker used for a purpose other than detection e.g., prognostic biomarkers |
| 5. Abstracts, Conference reports/writings, NHS reports, Review Articles |
| Reference | Specimen Type | Biomarker | Clinical Setting | Subjects | Sensitivity (%) | Specificity (%) | AUC |
|---|---|---|---|---|---|---|---|
| Gold et al., 2010 [37] | Serum | PAM4 | 68 PDAC, 19 HC | PDAC vs. HC | 82.0 | 95.0 | 0.92 (0.84–0.97) |
| Joergensen et al., 2010 [38] | Serum | CA19-9 MMP-9 TIMP1 | 51 PDAC, 52 HC | PDAC vs. HC | 86.0 58.8 47.1 | 73.0 34.6 69.2 | 0.84 (0.77–0.92) 0.50 (0.39–0.61) 0.64 (0.53–0.74) |
| Marten et al., 2010 [39] | Plasma | siC3b | 157 PDAC, 38 HC | 2–4mo prior radiologically defined recurrence | 54.0 | 94.0 | 0.85 |
| siC3b | 0–2mo prior radiologically defined recurrence | 62.0 | 94.0 | 0.84 | |||
| Brand et al., 2011 [17] | Serum | CA19-9 CA19-9 + ICAM-1 + OPG CA19-9 + CEA +TIMP-1 | 160 PDAC, 74 BPD, 107 HC | TS: PDAC vs. HC PDAC vs. BPD PDAC vs. HC | 57,2 88.0 76.0 | 90.0 90.0 90.0 | 0.83 (0.81–0.86) 0.93 (0.91–0.95) 0.86 |
| CA19-9 CA19-9 + ICAM-1 + OPG CA19-9 + CEA +TIMP-1 CA19-9 | 173 PDAC, 70 BPD, 120 HC | VS: PDAC vs. BPD PDAC vs. HC PDAC vs. BPC PDAC vs. BPC | 56.4 78.0 71.2 52.1 | 90.0 94.1 88.6 90.2 | 0.82 (0.78–0.86) 0.91 (0.88–0.95) 0.83 (0.88–0.89) 0.78 (0.74–0.83) | ||
| Park et al., 2012 [21] | Serum | Cathepsin D MMP-7 CA19-9 CA19-9 + Cathepsin D + MMP-7 | 109 PDAC, 40 HC, 30 CP | TS: PDAC vs. HC + CP | 54.0 72.0 74.0 88.0 | 80.0 80.0 80.0 80.0 | 0.67 0.81 0.84 0.90 (p = 0.002) |
| Cathepsin D MMP-7 CA19-9 CA19-9 + Cathepsin D + MMP-7 | 129 PDAC, 74 HC, 72 CP | VS: PDAC vs. HC + CP | 53.0 65.0 78.0 89.0 | 79.0 79.0 84.0 77.0 | 0.65 0.77 0.88 0.91 (p = 0.002) | ||
| Capello et al., 2013 [40] | Serum | EZR-autoantibody | 69 PDAC, 46 CP, 60 HC, 12 Aim, 50 Non-PDAC | PDAC vs. HC + CP + Aim | 93.2 | 75.5 | 0.90 |
| PDAC vs. non-PDAC cancer | 94.9 | 96.4 | 0.99 | ||||
| Gold et al., 2013 [41] | Serum | PAM4 CA19-9 PAM4 + CA19-9 | 298 PDAC, 120 BPD, 50 CP | PDAC vs. BPD | 74.0 77.0 84.0 | 85.0 73.0 83.0 | 0.87 (p = 0.0001) 0.85 (p = 0.0257) 0.91 |
| PAM4 CA19-9 PAM4 + CA19-9 | PDAC vs. CP | 74.0 77.0 84.0 | 86.0 68.0 82.0 | 0.87 (p = 0.0001) 0.84 (p = 0.0073) 0.91 | |||
| Kobayashi et al., 2013 [42] | Serum | Diagnostic Model * CA19-9 CEA Diagnostic Model * CA19-9 CEA | 43 PDAC, 42 HC | TS: PDAC vs. HC | 86.0 62.8 44.2 | 88.1 100.0 97.6 | 0.93 (0.86–0.97) 0.82 (0.70–0.90) 0.80 (0.69–0.88) |
| 9 PDAC (stage 0-IIB), 41 HC, 23 CP | VS: PDAC stage 0-IIB vs. HC + CP | 77.8 55.6 44.4 | 78.1 85.9 79.7 | 0.76 (0.66–0.86) 0.79 (0.68–0.88) 0.67 (0.55–0.76) | |||
| Li et al., 2013 [43] | Serum | CA19-9 miR-1290 miR-146a miR-484 | 41 PDAC, 19 HC, 35 CP | PC vs. HC | 71.0 88.0 78.0 76.0 | 90.0 84.0 79.0 63.0 | 0.86 0.96 (0.91–1.00) 0.82 (0.71–0.92) 0.78 |
| CA19-9 miR-1290 miR-146a miR-484 | PDAC vs. CP | 71.0 83.0 73.0 75.0 | 63.0 69.0 80.0 69.0 | 0.71 0.81 (0.71–0.91) 0.78 (0.68–0.89) 0.75 | |||
| Zhao et al., 2013 [44] | Serum | miR -192 | 70 PDAC, 40 HC | PDAC vs. HC | 76.0 | 55.0 | 0.63 (0.51–0.75) |
| Chung et al., 2014 [45] | Serum | sCD40L CA19-9 CEA | 55 PDAC, 30 CP, 30 HC | VS: PDAC vs. CP vs. HC | 80 80 68.9 | 85.5 72.7 60 | 0.88 0.78 0.70 |
| Lee et al., 2014 [46] | Serum | CFB CA19-9 CFB + CA19-9 | 41 PDAC, 44 HC, 12 CP, 31 HCC, 22 CC, 35 GC | PDAC vs. non-PDAC | 73.1 80.4 90.1 | 97.9 70.0 97.2 | 0.958 (0.956–0.959) 0.833 (0.829–0.837) 0.986 (p < 0.001) |
| Nolen et al., 2014 [47] | Serum | CA19-9 CA19-9 + CEA CA19-9 + CEA + Cyfra 21-1 | 343 PDAC, 227 HC | 1–12 months Pre-diagnostic PDAC vs. HC | 25.7 26.7 32.4 | 95.0 95.0 95.0 | 0.680 0.67 0.69 |
| CA19-9 CA19-9 + CEA CA19-9 + CEA + Cyfra 21-1 | 12–35 months Pre-diagnostic PDAC vs. HC | 17.2 28.1 29.7 | 95.0 95.0 95.0 | 0.63 0.66 0.66 | |||
| Ren et al., 2014 [48] | Serum | IL-11p | 44 PDAC, 30 HC | PDAC vs. HC | 97.7 | 70.0 | 0.901 (p < 0.001) |
| Schultz et al., 2014 [49] | Serum | Index 1 (miR-145, -150, -223, -636) Index 2 (miR-26b, -34a, -122, -126, -145, -150, -223, -505, -636, -885.5p) CA19-9 Index 1 + CA19-9 Index 2 + CA19-9 | 143 PDAC, 18 CP, 69 HC | DC: PDAC vs. HC + CP | 85.0 | 73.0 | 0.88 (0.85–0.92) |
| 85.0 88.0 85.0 85.0 | 86.0 92.0 93.0 97.0 | 0.93 (0.89–0.96) 0.87 (0.82–0.92) 0.88 (0.83–0.93) 0.95 (0.92–0.98) | |||||
| Index 1 Index 2 CA19-9 Index 1 + CA19-9 Index 2 + CA19-9 | 180 PDAC, 199 HC | TS: PDAC vs. HC | 85.0 85.0 86.0 85.0 85.0 | 64.0 85.0 99.0 95.0 98.0 | 0.86 (0.82–0.90) 0.93 (0.89–0.96) 0.90 (0.87–0.94) 0.93 (0.90–0.96) 0.97 (0.95–0.98) | ||
| Index 1 Index 2 CA19-9 Index 1 + CA19-9 Index 2 + CA19-9 | 86 PDAC, 7 CP, 44 HC | VS: PDAC vs. HC + CP | 85.0 85.0 79.0 85.0 85.0 | 45.0 51.0 88.0 88.0 86.0 | 0.83 (0.76–0.90) 0.81 (0.73–0.87) 0.89 (0.83–0.95) 0.93 (0.88–0.97) 0.92 (0.87–0.96) | ||
| Yang et al., 2014 [50] | Stool | miR-21 miR-155 miR -216 miR-216 + miR-21+ miR-155 | 30 PDAC, 15 HC | PDAC vs. HC | 90.0 76.7 86.7 83.3 | 66.7 73.3 60.0 83.3 | 0.80 (0.68–0.92) 0.72 (0.58–0.86) 0.73 (0.60–0.86) 0.87 (0.77–0.96) |
| Zhang et al., 2014 [51] | Serum | CA19-9 + Albumin + CRP + IL-8 CA19-9 CA19-9 + Albumin + CRP + IL-8 CA19-9 | 163 PDAC (77 Early stage I-II), 109 BC, 200 HC | All stage PDAC vs. HC All stage PDAC vs. HC Early stage PDAC vs. HC Early stage PDAC vs. HC | 99.4 80.6 96.1 72.7 | 90.0 90.0 90.0 90.0 | 0.98 (0.97–1.00) 0.85 (0.80–0.90) 0.97 (0.95–1.00) 0.83 (0.75–0.90) |
| CA19-9 + CO2 +CRP + IL-6 CA19-9 CA19-9 + CO2 +CRP + IL-6 CA19-9 | All stage PDAC vs. BC All stage PDAC vs. BC Early stage PDAC vs. BC Early stage PDAC vs. BC | 74.2 53.4 75.3 40.3 | 90.0 90.0 90.0 90.0 | 0.89 (0.86–0.93) 0.75 (0.69–0.81) 0.87 (0.82–0.93) 0.69 (0.61–0.78) | |||
| Debernardi et al., 2015 [52] | Urine | miR-143 miR-223 miR-30e miR-143 + miR-30e | 6 PDAC (stage I), 26 HC | Stage I PDAC vs. HC | 83.3 83.3 83.3 83.3 | 88.5 76.9 80.8 96.2 | 0.86 (0.70–1.00) 0.80 (0.59–1.00) 0.85 (0.67–1.00) 0.92 (0.79–1.00) |
| Han et al., 2015 [53] | Serum | Dickkopf-1 (DKK1) CA19-9 | 140 PDAC, (62 Early stage I-II), 48 HC, 18 BPT, 26 CP | PDAC vs. HC + BPT + CP | 89.3 73.6 | 79.4 83.7 | 0.92 (0.88–0.95) 0.85 (0.80–0.90) |
| Dickkopf-1 (DKK1) CA19-9 | PDAC vs. BPT + CP | 89.3 73.6 | 72.7 81.8 | 0.89 (0.83–0.95) 0.83 (0.77–0.89) | |||
| Dickkopf-1 (DKK1) CA19-9 | Early-PDAC vs. HC + BPT + CP | 85.5 64.5 | 79.3 83.7 | 0.89 (0.84–0.94) 0.81 (0.74–0.89) | |||
| Dickkopf-1 (DKK1) CA19-9 | Early-PDAC vs. BPT + CP | 85.5 64.5 | 72.7 81.8 | 0.85 (0.78–0.93) 0.78 (0.70–0.87) | |||
| Melo et al., 2015 [54] | Serum | GPC1 + crExos CA19-9 | 190 PDAC, 100 HC, 26 BPD | DS: PDAC vs. HC + BPD | 100.0 76.8 | 100.0 64.3 | 1.00 (0.99–1.00) 0.74 (0.70–0.83) |
| GPC1 + crExos GPC1 (ELISA) | 56 PDAC, 20 HC, 6 BPD | VS: PDAC vs. HC + BPD | 100.0 82.1 | 100.0 75.0 | 1.00 (0.96–1.00) 0.78 (0.68–0.87) | ||
| Radon et al., 2015 [55] | Urine | LYVE1 REG1A TFF1 LYVE1 + REG1A + TFF1 + (Creatinine +Age) | 143 PDAC (stage I-IV), 59 HC | TS: PDAC vs. HC | 76.9 62.2 72.7 76.9 | 88.1 94.9 59.3 89.8 | 0.85 (0.80–0.90) 0.82 (0.77–0.88) 0.69 (0.61–0.77) 0.89 (0.85–0.94) |
| LYVE1 REG1A TFF1 LYVE1 + REG1A + TFF1 + (Creatinine +Age) | 56 PDAC (stage I-II), 61 HC | 67.9 75.0 78.6 82.1 | 91.8 68.9 52.5 88.5 | 0.84 (0.77–0.91) 0.75 (0.66–0.84) 0.70 (0.60–0.79) 0.90 (0.84–0.96) | |||
| LYVE1 + REG1A + TFF1 + (Creatinine +Age) | 49 PDAC (stage I-IV), 28 HC | VS: PDAC vs. HC | 75.5 | 100 | 0.92 (0.84–1.00) | ||
| LYVE1 + REG1A + TFF1 + (Creatinine +Age) | 56 PDAC (stage I-II), 61 HC | 80.0 | 76.9 | 0.93 (0.84–1.00) | |||
| Plasma CA19-9 Panel (LYVE1 + REG1A + TFF1) Panel + Plasma CA19-9 | 71 PDAC (stage I-II), 28 HC | Exploratory Comparison | 83.1 93.0 94.4 | 92.9 92.9 100 | 0.88 (0.81–0.95) 0.97 (0.95–1.00) 0.99 (0.98–1.00) | ||
| Ankeny et al., 2016 [56] | Serum | CTCs and KRAS mutation analysis | 72 PDAC, 28 non-adenocarcinoma | PDAC vs. non-adenocarcinoma | 78.0 | 96.4 | 0.87 (0.80–0.94) |
| Guo et al., 2016 [57] | Serum | DTNBP1 CA19-9 | 250 PDAC, 70 CP, 80 BBO, 150 HC | PDAC vs. BBO + CP + HC | 81.9 76.3 | 84.7 52.5 | 0.85 (0.81–0.89) 0.74 (0.70–0.78) |
| DTNBP1 CA19-9 | PDAC vs. CP | 73.9 66.3 | 78.9 73.2 | 0.80 (0.75–0.86) 0.69 (0.63–0.75) | |||
| DTNBP1 CA19-9 | PDAC vs. BBO | 82.3 53.8 | 84.0 49.4 | 0.85 (0.80–0.89) 0.59 (0.53–0.65) | |||
| Henriksen et al., 2016 [58] | Plasma | (Model13): age >65+ BMP3+ RASSF1A+ BNC1+ MESTv2+ TFPI2+ APC+ SFRP1 + SFRP2 | 95 PDAC, 97 CP, 27 “screened negative” | PDAC vs. screened negative + CP | 73.0 | 83.0 | 0.86 (0.81–0.91) |
| Sogawa et al., 2016 [59] | Serum | C4BPA CA19-9 CEA C4BPA + CA19-9 | 66 PDAC, 40 HC, 20 CP | PDAC vs. HC + CP | 67.3 71.2 34.6 86.4 | 95.4 95.4 95.4 95.4 | 0.86 (p < 0.001) 0.85 0.77 0.93 |
| C4BPA CA19-9 CEA | 18 PDAC (stage I-II), 40 HC, 20 CP | PDAC stage I-II vs. HC + CP | 50.0 22.2 22.2 | 95.4 95.4 95.4 | 0.91 (p < 0.001) 0.74 0.87 | ||
| Yoneyama et al., 2016 [60] | Serum | CA19-9 IGFBP2 IGFBP3 | 38 PDAC (stage I-II), 65 HC | Stage I-II PDAC vs. HC | 60.5 68.4 76.3 | 92.3 67.7 70.7 | 0.84 (0.75–0.93) 0.71 (0.60–0.81) 0.77 (0.67–0.86) |
| Balasenthil et al., 2017 [61] | Plasma | CA19-9 | 55 PDAC (stage IA/ IB-IIA), 61HC | Stage IA/ IB-IIA vs. HC | 71.0 | 61.0 | 0.74 (0.64–0.84) |
| TNC + TFP1 + CA19-9 | 55 PDAC (stage IA/ IB-IIA), 62 CP | Stage IA/ IB-IIA vs. CP | 73.0 | 82.0 | 0.79 (0.70–0.87) | ||
| CA19-9 TNC + TFP1 + CA19-9 | 71.0 73.0 | 44.0 71.0 | 0.69 (0.58–0.79) 0.75 (0.65–0.84) | ||||
| Yang et al., 2017 [62] | Plasma | EGFR EPCAM HER2 MUC1 GPC1 WNT2 GRP94 B7-H3 EGFR + EPCAM + HER2 + MUC1 EGFR + EPCAM + GPC1 + WNT2 EGFR + EPCAM + MUC1 + GPC1 + WNT2 EGFR + EPCAM + HER2 + MUC1 + GPC1 + WNT2 | 22 PDAC, 10 HC | TS: PDAC vs. HC | 73 73 59 36 55 77 73 50 91 100 100 100 | 100 100 90 100 60 90 70 100 100 100 100 100 | 0.90 (0.79–1) 0.88 (0.77–0.99) 0.72 (0.55–0.89) 0.66 (0.48–0.84) 0.48 (0.28–0.67) 0.84 (0.71–0.96) 0.73 (0.55–0.90) 0.75 (0.58–0.93) 0.99 (0.97–1) 1.0 1.0 1.0 |
| EGFR EPCAM HER2 MUC1 GPC1 WNT2 GRP94 EGFR + EPCAM + HER2 + MUC1 EGFR + EPCAM + GPC1 + WNT2 EGFR + EPCAM + MUC1 + GPC1 + WNT2 EGFR + EPCAM + HER2 + MUC1 + GPC1 + WNT2 | 22 PDAC, 8 CP, 5 BPD, 8 other abdominal indications | VS: PDAC vs. CP vs. BPD vs. other abdominal indications | 59 45 59 36 82 64 55 86 82 86 95 | 76 95 85 90 52 76 71 86 90 81 81 | 67 (51–81) 70 (54–83) 72 (56–85) 63 (47–77) 67 (51–81) 70 (54–83) 63 (47–77) 86 (72–95) 86 (72–95) 84 (69–93) 88 (75–96) | ||
| Capello et al., 2017 [63] | Serum/ Plasma | CA19-9 TIMP1 + LRG1 + CA19-9 TIMP1 + LRG1 + CA19-9 (“OR” Rule) CA19-9 | 39 early stage PDAC, 82 HC | TS: early stage PDAC vs. HC | 53.8 66.7 72.6 84.9 | 95.0 95.0 95.0 95.0 | 0.82 (0.74–0.91) 0.89 (0.82–0.96) 0.88 (0.81–0.96) 0.95 (0.92–0.98) |
| CA19-9 TIMP1 + LRG1 + CA19-9 | 73 early stage PDAC, 60 HC | VS: early stage PDAC vs. HC | 84.9 28.8 | 95.0 95.0 | 0.96 (0.89–1.00) 0.82 (0.74–0.91) | ||
| Hussein et al., 2017 [64] | Serum | miR-22-3p miR-642b-3p miR-885-5p CA19-9 | 35 PDAC (33 early stage, 2 late stage) 15 HC | PDAC vs. HC | 97.1 100 100 91.4 | 93.3 100 100 100 | 0.94 (p < 0.001) 1.00 (p < 0.001) 1.00 (p < 0.001) 0.92 (p < 0.001) |
| Kaur et al., 2017 [65] | Serum | MUC5AC CA19-9 | 70 PDAC (stage I or II), 43 CP, 35 HC, 30 BC | Early PDAC vs. HC | 83.0 56.0 | 80.0 95.0 | 0.87 (0.79–0.95) 0.72 (0.59–0.84) |
| MUC5AC CA19-9 | Early PDAC vs. BC | 67.0 48.0 | 87.0 89.0 | 0.85 (0.76–0.93) 0.71 (0.59–0.83) | |||
| MUC5AC CA19-9 | Early PDAC vs. CP | 83.0 48.0 | 77.0 86.0 | 0.84 (0.76–0.92) 0.62 (0.50–0.74) | |||
| MUC5AC CA19-9 MUC5AC + CA19-9 | PDAC vs. HC + BC + CP | 89.0 79.0 83.0 | 70.0 43.0 83.0 | 0.88 (0.83–0.93) 0.61 (0.54–0.68) 0.91 (0.86–0.95) | |||
| Kim et al., 2017 [66] | Plasma | CA19-9 (≥55) THBS2 (36ng/mL cut-off) CA19-9 + THBS2 | 58 (stage I-II, phase 2a), 80 HC | PDAC stage I or II vs. HC | 69.0 33.0 74.1 | 100 96.0 96.3 | 0.85 (0.80–0.89) 0.83 (0.78–0.89) 0.95 (0.92–0.98) |
| CA19-9 THBS2 CA19-9 + THBS2 | 88 (stage I-II, phase 2b), 140 HC | 77.7 58.4 88.3 | 98.6 93.6 92.9 | 0.83 (0.79–0.97) 0.89 (0.85–0.92) 0.96 (0.94–0.98) | |||
| Lai et al., 2017 [67] | Plasma | CA19-9 miR-10b miR-21 miR-30c miR-106b miR-20a miR-181a miR-483 miR-let7a miR-122 | 29 PDAC, 6 HC | PDAC vs. HC | 86.0 100.0 86.0 100.0 97.0 93.0 97.0 66.0 93.0 100.0 | 100.0 100.0 100.0 100.0 100.0 100.0 100.0 67.0 100.0 67.0 | 0.92 (p < 0.001) 1.00 (p < 0.001) 0.95 (p < 0.001) 1.00 (p < 0.001) 0.98 (p < 0.001) 0.99 (p < 0.001) 0.97 (p < 0.001) 0.67 (p = 0.20) 0.99 (p < 0.001) 0.89 (p = 0.003) |
| Park et al., 2017 [68] | Serum | LRG1 + TTR + CA19-9 CA19-9 LRG1 + TTR + CA19-9 CA19-9 LRG1 + TTR + CA19-9 CA19-9 LRG1 + TTR + CA19-9 CA19-9 LRG1 + TTR + CA19-9 CA19-9 | 80 PDAC (50 stage I-II) (29 CA19-9 negative PDAC), 68 HC, 21 BPD, 52 Thyroid Ca, 52 Breast Ca, 45 Colorectal Ca) | PDAC vs. HC + BPC (n = 89) PDAC stage I-II vs. HC + BPC (n = 89) PDAC vs. Other Cancers (n = 149) PDAC vs. BPD CA19-9 negative PDAC (n = 29) vs. HC + BPC | 82.5 72.5 76.0 64.0 82.5 72.5 82.5 72.5 51.7 24.1 | 92.1 88.8 92.1 88.8 83.9 87.9 85.7 81.0 92.1 88.8 | 0.93 (p < 0.01) 0.83 0.91 (p < 0.01) 0.79 0.90 (p < 0.001) 0.80 0.90 0.81 0.83 (p < 0.001) 0.52 |
| Schott et al., 2017 [69] | Serum | HYAL2 Methylation | 82 PDAC, 191 HC 60 PDAC (stage I-II), 191 HC | PDAC vs. HC PDAC stage I-II vs. HC | 75.6 66.7 | 93.7 95.3 | 0.92 (0.88–0.96) 0.93 (0.89–0.98) |
| Arasaradnam et al., 2018 [70] | Urine | Volatile organic compounds | 4 PDAC stage I, 5 stage IIA, 35 stage IIB, 24 stage III, 12 stage IV, 81 HC | TS: PDAC vs. HC VS: PDAC vs. HC PDAC stage I -II vs. HC PDAC stage I -II vs. PDAC stage III-IV | 0.91 0.90 0.91 0.82 | 0.83 0.81 0.78 0.89 | 0.92 (0.88–0.96) 0.92 (0.85–0.98) 0.89 (0.83–0.94) 0.92 (0.86–0.97) |
| Dong et al., 2018 [71] | Serum | CA19-9 POSTN CA242 CA19-9 + POSTN CA19-9 + CA242 POSTN+ CA242 CA19-9 + POSTN+ CA242 | 30 PDAC (early stage), 68 PDAC (late stage), 32 BPC, 37 HC, 27 PDAC (CA19-9 negative) | TS: HC vs. early PDAC | 96.7 70.0 81.1 93.3 90.0 83.3 96.7 | 83.8 75.7 81.1 94.6 94.6 86.5 94.6 | 0.94 (0.86–0.99) 0.78 (0.66–0.87) 0.89 (0.79–0.95) 0.97 (0.90–1.00) 0.96 (0.88–0.99) 0.90 (0.80–0.96) 0.98 (0.90–1.00) |
| CA19-9 POSTN CA242 CA19-9 + POSTN CA19-9 + CA242 POSTN+ CA242 CA19-9 + POSTN+ CA242 | BPC vs. all PDAC | 85.7 64.3 58.1 84.7 75.5 67.4 84.7 | 81.3 87.5 87.5 90.6 90.6 96.9 90.6 | 0.88 (0.82–0.93) 0.81 (0.74–0.88) 0.78 (0.70–0.85) 0.93 (0.88–0.97) 0.89 (0.83–0.94) 0.87 (0.80–0.92) 0.94 (0.88–0.97) | |||
| CA19-9 POSTN CA242 CA19-9 + POSTN CA19-9 + CA242 POSTN+ CA242 CA19-9 + POSTN+ CA242 | 38 PDAC (early stage), 77 PDAC (late stage), 43 BPC; 37 HC, 29 PDAC (CA19-9 negative) | BPC vs. early PDAC | 86.7 53.3 83.3 96.7 90.0 56.7 96.7 | 81.3 87.5 62.5 75.0 78.1 96.9 75.0 | 0.88 (0.77–0.95) 0.74 (0.61–0.84) 0.78 (0.66–0.88) 0.90 (0.80–0.96) 0.90 (0.79–0.96) 0.80 (0.68–0.89) 0.92 (0.82–0.97) | ||
| CA19-9 POSTN CA242 CA19-9 + POSTN CA19-9 + CA242 POSTN+ CA242 CA19-9 + POSTN+ CA242 | VS: HC vs. early PDAC | 86.8 63.2 57.9 86.8 86.8 79.0 92.1 | 94.6 78.4 100 97.3 97.3 94.6 97.3 | 0.94 (0.86–0.98) 0.78 (0.66–0.86) 0.83 (0.73–0.91) 0.95 (0.88–0.99) 0.97 (0.90–1.00) 0.92 (0.84–0.97) 0.98 (0.92–1.00) | |||
| CA19-9 POSTN CA242 CA19-9 + POSTN CA19-9 + CA242 POSTN+ CA242 CA19-9 + POSTN+ CA242 | BPC vs. all PDAC | 84.4 77.4 60.0 83.5 77.4 84.4 80.0 | 81.4 79.1 93.0 93.0 88.4 83.7 97.7 | 0.88 (0.82–0.93) 0.82 (0.76–0.88) 0.79 (0.72–0.85) 0.92 (0.87–0.96) 0.90 (0.84–0.94) 0.89 (0.83–0.93) 0.93 (0.88–0.96) | |||
| CA19-9 POSTN CA242 CA19-9 + POSTN CA19-9 + CA242 POSTN+ CA242 CA19-9 + POSTN+ CA242 | BPC vs. early PDAC | 86.8 65.8 57.9 65.8 76.3 76.3 83.6 | 79.1 79.1 93.0 93.0 93.0 86.1 88.4 | 0.87 (0.78–0.93) 0.72 (0.61–0.82) 0.77 (0.66–0.85) 0.84 (0.75–0.92) 0.92 (0.83–0.97) 0.84 (0.74–0.91) 0.90 (0.81–0.96) | |||
| Guo et al., 2018 [72] | Serum | SNHG15 | 171 PDAC, 59 HC | PDAC vs. HC | 68.3 | 89.6 | 0.73 (p < 0.01) |
| Lewis et al., 2018 [73] | Whole blood, plasma, serum | GPC1 + CD63 | 20 PDAC 6 BPD | PDAC vs. BPD | 81 | 70 | 0.79 (0.99–1.00) |
| Mellby et al., 2018 [74] | Plasma | Panel of 29 biomarkers | 15 PDAC stage I, 75 stage II, 15 stage III, 38 stage IV 57 CP, 20 IPMN, 219 HC | TS 2: PDAC stage I-II vs. HC | 95 | 94 | 0.96 (0.94–0.98) |
| VS (USA cohort): PDAC stage I-II vs. HC | 93 | 95 | 0.96 (0.94–0.98) | ||||
| Traeger et al., 2018 [75] | Serum | miRNA-205 CA19-9 miRNA-205 +CA19-9 | 47 PDAC, 16 CP, 5 IPMN, 17 BPC, 17 HC | PDAC vs. non-PDAC | 0.643 0.810 0.867 | 0.684 0.768 0.933 | 0.70 (0.548–0.789) 0.79 (0.698–0.887) 0.89 (0.782–0.995) |
| Zhou et al., 2018 [76] | Serum | GPC1 CA19-9 | 156 PDAC, 20 BPT, 16 CP, 163 HC | PDAC vs. HC + BPT + CP | 76.92 82.69 | 70.85 93.97 | 0.80 (0.749–0.841) 0.91 (0.868–0.947) |
| GPC1 CA19-9 | PDAC vs. HC | 76.92 82.69 | 70.55 97.55 | 0.81 (0.763–0.856) 0.91 (0.875–0.953) | |||
| GPC1 CA19-9 | Early PDAC vs. HC + BPT + CP | 68.06 79.17 | 70.85 93.97 | 0.76 (0.695–0.816) 0.88 (0.816–0.946) | |||
| GPC1 CA19-9 | Early PDAC vs. HC | 68.06 79.17 | 70.55 97.55 | 0.77 (0.705–0.830) 0.89 (0.824–0.953) | |||
| Berger et al., 2019 [77] | Plasma | CA19-9 THBS2 cfDNA CA19-9 + THBS2 THBS2 + CA19-9 + cfDNA | 52 PDAC, 15 IPMN, 32 CP | TS: PDAC vs. IPMN vs. CP | 55 41 32–86 1 73 41–86 1 | 91 96 70–100 1 91 78–96 1 | 0.80 0.73 0.90 0.87 0.94 |
| CA19-9 THBS2 cfDNA CA19-9 + THBS2 THBS2 + CA19-9 + cfDNA | VS: PDAC vs. IPMN vs. CP | 63 50 43–80 1 80 50–93 1 | 96 96 79–96 1 96 92–96 1 | 0.70 0.63 0.81 0.78 0.88 | |||
| Eissa et al., 2019 [78] | Plasma | ADAMTS1 | 39 PDAC, 95 HC | PDAC vs. HC | 87.2 | 95.8 | 0.91 (0.77–0.90) |
| BNC1 | 64.1 | 93.7 | 0.79 (0.63–0.78) | ||||
| ADAMTS1 and/or BNC1 | 97.4 | 91.6 | 0.95 (0.71–0.86) | ||||
| Fahrmann et al., 2019 [79] | Plasma | AcSperm+ DAS + indole-derivative+ LysoPC(18:0) + LysoPC(20:3) | 29 PDAC, 10 HC | TS: PDAC vs. HC | 69.0 | 99.0 | 0.90 (0.818–0.989) |
| AcSperm+ DAS + indole-derivative+ LysoPC(18:0) + LysoPC(20:3) | 39 Resectable PDAC, 82 HC | VS: PDAC vs. HC | 66.7 | 43.3 | 0.89 (0.828–0.996) | ||
| Indole-derivative LysoPC(18:0) LysoPC(20:3) AcSperm DAS | 23.1 51.3 48.7 33.3 51.3 | 11.3 26.3 11.3 27.5 27.5 | 0.73 (0.631–0.822) 0.84 (0.764–0.920) 0.84 0.757–0.925) 0.76 (0.659–0.852) 0.80 (0.712–0.890) | ||||
| Yu et al., 2019 [80] | Plasma | d-signature: EV long RNA (FGA, KRT19, HIST1H2BK, ITIH2, MARCH2, CLDN1, MAL2 and TIMP1) | 284 PDAC, 100 CP, 117 HC | PDAC vs. CP vs. HC d-signature with CA19-9 | 93.68 | 91.57 | 0.936 (0.889–0.983) |
| Takahashi et al., 2019 [81] | Serum | Circulating EV-encapsulated HULC | 20 PDAC, 22 IPMN, 21 HC | PDAC vs. IPMN vs. HC | 80 | 92.1 | 0.92 |
| Wei et al., 2019 [82] | Plasma | Vimetin-positive CTCs | 100 PDAC, 16 IPMN, 30 HC | PDAC vs. IPMN vs. HC | 65 | 100 | 0.968 |
| Yang et al., 2020 [83] | Plasma | EV miRNAs and mRNAs, cfDNA, ccfDNA KRAS G12D/V/R mutations and CA19-9 | 30 CP + BPC, 49 PDAC, 57 HC | PDAC vs. non-PDAC vs. HC | 88 | 95 | 0.95 (p= 0.103) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brezgyte, G.; Shah, V.; Jach, D.; Crnogorac-Jurcevic, T. Non-Invasive Biomarkers for Earlier Detection of Pancreatic Cancer—A Comprehensive Review. Cancers 2021, 13, 2722. https://doi.org/10.3390/cancers13112722
Brezgyte G, Shah V, Jach D, Crnogorac-Jurcevic T. Non-Invasive Biomarkers for Earlier Detection of Pancreatic Cancer—A Comprehensive Review. Cancers. 2021; 13(11):2722. https://doi.org/10.3390/cancers13112722
Chicago/Turabian StyleBrezgyte, Greta, Vinay Shah, Daria Jach, and Tatjana Crnogorac-Jurcevic. 2021. "Non-Invasive Biomarkers for Earlier Detection of Pancreatic Cancer—A Comprehensive Review" Cancers 13, no. 11: 2722. https://doi.org/10.3390/cancers13112722