1. Introduction
Glioblastoma (GBM) is the most common and aggressive primary brain tumor. While chemoradiotherapy with temozolomide (TMZ) represents standard first-line therapy after surgery [
1], the standard of care for second-line treatment has not been defined. Treatment options include re-surgery, re-irradiation and systemic pharmacotherapy—mostly nitrosoureas [
2,
3]. Bevacizumab demonstrated that it prolongs progression-free survival (PFS) without improving overall survival (OS) [
4]; yet, immunotherapy with checkpoint inhibitors showed no efficacy in glioma patients [
5,
6].
Some recent studies have improved knowledge on molecular pathways and specific gene mutations driving the origin and progression of GBM; we are therefore seeing some promising results due to specific targeted therapies (i.e., BRAF inhibitors, TRK inhibitors and regorafenib) [
2,
7,
8], even though the benefit of these new treatments needs further evaluation.
EGFR (epidermal growth factor receptor) is a transmembrane tyrosine kinase involved in many intracellular pathways regulating DNA synthesis and cell proliferation. Its signaling abnormalities have a prominent role in the pathogenesis of GBM; approximately 50% of GBM patients have tumors harboring EGFR amplification on chromosome 7 and half of these cases have the exon 2–7 deletion, known as EGFR variant III (EGFRvIII) [
9]. However, many EGFR tyrosine kinase inhibitors (TKIs) such as gefitinib [
10], erlotinib [
11] and afatinib [
12] failed to demonstrate efficacy in both newly-diagnosed and recurrent GBM.
Depatuxizumab Mafodotin (Depatux-M; ABT-414) is an antibody-drug conjugate composed of the anti-EGFR monoclonal antibody conjugated to monomethyl auristatin F (mafodotin), an antimicrotubule agent [
13]. After interaction with the tumor-specific binding site (exposed and available in the case of EGFR amplification), Depatux-M is internalized in the cell and mafodotin is released, thus killing the cell [
14]. Depatux-M was initially evaluated in the phase 1 M12-356 (NCT01800695) trial [
15]; this study analyzed the safety, preliminary efficacy and pharmacokinetics of Depatux-M alone or in combination with TMZ in patients with newly-diagnosed or recurrent GBM. The combination arm showed interesting results in the recurrent GBM population, with an objective response rate of 14.3% and a 6-month OS of 69.1%. A subsequent phase 2 study was planned on the basis of this promising data: INTELLANCE 2/EORTC1410 (NCT02343406) was a multicenter, randomized open label study comparing Depatux-M plus TMZ (arm 1) versus Depatux-M alone (arm 2) versus standard treatment of TMZ/lomustine (arm 3/control arm) in EGFR-amplified GBM at first recurrence/progression after standard chemoradiotherapy [
16]. Although the study did not reach the primary endpoint of OS, at the time of long-term follow-up the combination arm demonstrated a statistically longer OS compared to the other arms. Worth noting among patients treated with the combination regimen is that the benefit in OS was more consistent for those who relapsed/progressed more than 16 weeks after the start of the last cycle of TMZ. The Depatux-M toxicity profile was similar to the phase 1 study’s observed toxicities.
We performed this multicenter study in order to better evaluate the safety and efficacy of this combination regimen in the real-life population of recurrent GBM patients.
2. Results
A total of 36 patients were enrolled from seven Institutions of the Italian Association of Neuro-Oncology (AINO) from October 2018 to June 2019. Baseline patient and tumor characteristics are shown in
Table 1: the median age was 57 years, the ECOG PS was 0–1 in 88% of patients, 42% received the treatment as second-line therapy and 27% underwent further chemotherapy at subsequent progression. Most patients presented IDH 1–2 wild type status (94%) and methylated MGMT promoter (64%). The median number of Depatux-M infusions was 4 (range 1–24). Most patients (81%) started Depatux-M plus TMZ more than 16 weeks since the last TMZ cycle. No patient received surgery after the experimental treatment.
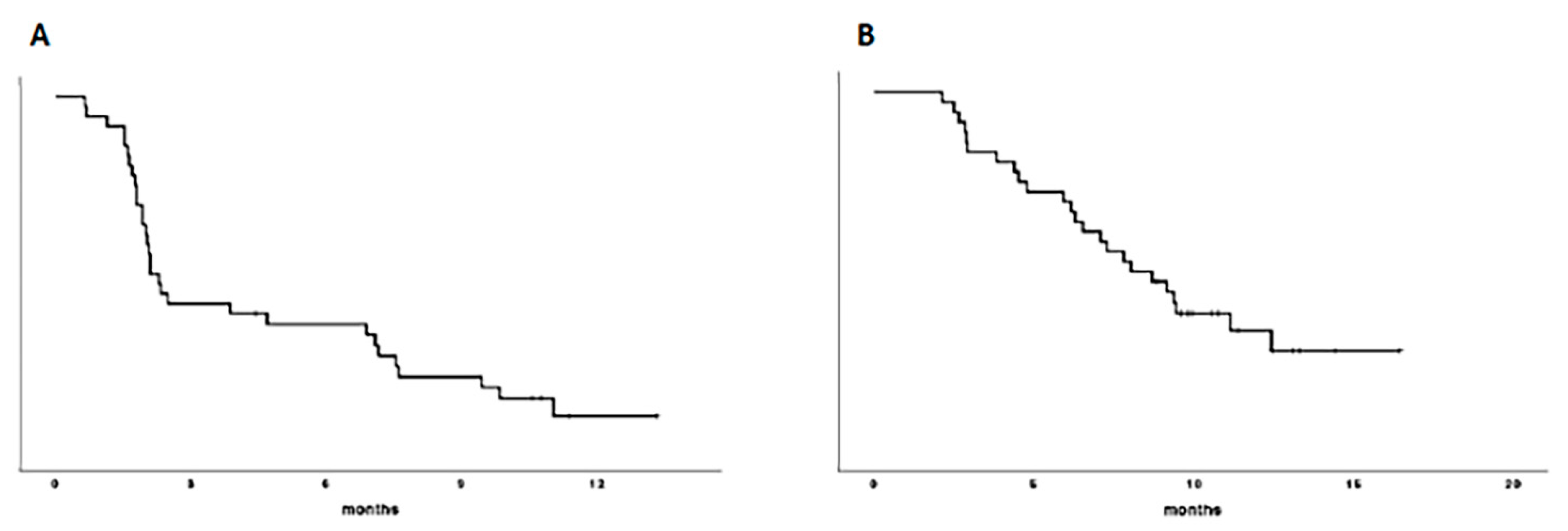
At the time of analysis, 24 patients (67%) had died and 31 patients (86%) had progressed. Median PFS was 2.1 months (95% CI, 1.7–2.4) and the 6 month-PFS was 38% (
Figure 1A); median OS was 8.04 months (95% CI, 5.3–10.7) and the 12 month-OS was 37% (
Figure 1B);
Figure 1. PFS (A) and OS (B) curves.
On univariate and multivariate analysis, the MGMT methylation status was an independent prognosticator for longer OS (see
Table 2 and
Table 3); ECOG PS, number of prior lines of therapy and the time starting Depatux-M since TMZ were not significantly correlated to OS.
None of the factor studied were significantly correlated to PFS on multivariate analysis.
One (3%) out of 36 patients and 4 (11%) out of 36 patients had a complete response and a partial response, respectively, with an objective response rate of 14% (see
Table 4). Additionally, 13 patients (36%) had stable disease, resulting in a disease control rate (DCR) of 50%. No clinical or molecular factors were associated with DCR (see
Table 5).
The most frequent Depatux-M related adverse events (AEs) were ocular and were observed in 81% of patients (any grade); in most cases the ocular events occurred after the second administration of Depatux-M. Ocular AEs were attributed to microcystic keratopathy and included keratitis (67%), photophobia (8%), eye pain (3%) and conjunctivitis (3%). Grade 3 keratitis was reported in four cases (11%) and no grade 4 adverse events were recorded (see
Table 6). Hematological toxicities (mainly thrombocytopenia) were reported in 17 patients (47%) and in six cases (17%) were classified as grade 3–4. Grade 3 hypertransaminasemia was recorded in one patient (3%), two cases (6%) documented as grade 3 venous thrombosis and grade 1–2 hypertension was reported in only one case (3%).
Ocular toxicity led to Depatux-M dose delay and dose reductions in 28% and 17% of patients, respectively, while its early permanent discontinuation occurred in two patients (5% of cases). No drug-related death was reported.
3. Discussion
To our knowledge, this is the first study to assess the role of Depatux-M plus TMZ in recurrent EGFR-amplified GBM patients in a real-life world. Clinical benefits were very close to those reported in the combination therapy arm in the previous phase 2 trial. The INTELLANCE 2 protocol was a randomized multicentric study which analyzed the efficacy of Depatux-M alone versus Depatux-M plus TMZ versus the standard treatment of lomustine or TMZ in EGFR-amplified GBM patients relapsing after the Stupp protocol [
16]. The primary analysis of the INTELLANCE 2 study with a median follow-up of 14.4 months (199 subjects had died) showed a trend of longer survival for the combination regimen versus the standard treatment: the 12m-OS rate was 39.7% versus 28.2%, respectively, with a
p value of 0.06 (HR = 0.71, 95% CI, 0.50–1.02); in the subsequent long-term analysis with a median follow-up of 28.7 months (237 patients had died), the OS difference between the two arms became statistically significant: the 2-year survival in the combination arm was 19.8% versus 5.2% in the control arm (
p = 0.017; HR = 0.66, 95% CI, 0.47–0.93). Interestingly, in INTELLANCE 2, the MGMT methylation status was not statistically associated with a longer OS while the clinical benefit of the Depatux-M plus TMZ combination was more consistent in patients relapsing more than 16 weeks after the end of TMZ treatment. Conversely, we reported a statistically longer OS in patients with MGMT promoter methylated tumors and no survival advantage for patients starting the treatment after 16 weeks since TMZ; this could be due to the smaller population analyzed in this real-world study, although the presence of methylated MGMT can represent a significant predictor of TMZ efficacy [
17]. Moreover, more patients with methylated MGMT were enrolled in our study compared to the INTELLANCE 2 trial: 61% versus 48.9%, respectively. Yet, the high rate of MGMT methylated patients, as well as the high rate of patients who started treatment more than 16 weeks after the end of TMZ, may have contributed to the clinical benefit observed in the present study.
Even though most of the patients in our study were treated beyond second-line therapy (58%), we reported a similar OS to the prior randomized INTELLANCE 2 study; indeed, 58% of patients received the therapy as a third or subsequent line of treatment. Yet, our results were similar or even superior to those reported in some larger phase 2 or 3 studies analyzing the recurrent GBM population. In the EORTC 26101 trial [
4], 437 patients were treated with lomustine plus bevacizumab or lomustine alone, reporting a 12m-OS rate of 31.5% and 34.1%, respectively. In the TAMIGA trial [
18], 123 patients with recurrent GBM after receiving radiation therapy, plus bevacizumab and TMZ as a first-line treatment, were randomized to receive bevacizumab plus lomustine or lomustine alone: the 12m-OS rate was 11.7% and 16.5%, respectively. Yet, the randomized phase 2 REGOMA trial [
7] showed a statistically longer OS in recurrent GBM patients when treated with regorafenib compared to standard lomustine: the 12m-OS rate was 38.9% versus 15.0%, respectively. Due to this important clinical benefit, regorafenib was included in the NCCN 2020 guidelines and was approved by the Italian Medicines Agency (AIFA) as the preferred treatment for the recurrent GBM population [
2].
Worth noting in this real-word study analyzing the efficacy and safety of Depatux-M plus TMZ outside the context of randomized controlled trials is that we demonstrated the benefit of this combination regimen, also in terms of disease control rate. Indeed, we reported a DCR of 50% (one patient with complete response, four with partial response and 13 with stable disease), which is again very close to that observed in INTELLANCE 2 (48% of evaluable cases). Hovewer, an important limit of our study is the relatively small number of included cases and this could impact the results of our “real-life” analysis both in terms of tolerability and efficacy.
As regards safety, similar to INTELLANCE 2, the most common adverse events were ocular and reported in 81% of patients compared to the 87% observed in the phase 2 study. However, we observed grade 3 ocular toxicity (all cases of keratitis) in only 11% of patients (no grade 4 ocular toxicity was recorded) versus 40% observed in the prior phase 1 study [
15] (mostly keratitis in 13% of cases) and 32.9% shown in INTELLANCE 2 trial. Different factors may have contributed to the lower incidence of severe ocular toxicity observed in our study. An increased expertise regarding the management of Depatux-M has been gained by neuro-oncologists which have previously participated in the INTELLANCE 1 and 2 trials; another key factor contributing the management of ocular toxicity is that all patients enrolled in our study were followed by a dedicated ophthalmologist. Indeed, it was already demonstrated that the ocular side effects caused by Depatux-M can be reversible and moderate if carefully managed [
19,
20]. In our study, Depatux-M dose reduction occurred in 17% of patients versus 12% reported in the previous phase 1 study, while dose delays occurred in only 28% versus the 58% seen in the prior study [
15]. The lower rate of patients having dose delays may also have a positive impact on survival.
The addition of Depatux-M to standard radiation and TMZ in newly-diagnosed EGFR-amplified GBM patients was investigated in the randomized phase 3 INTELLANCE 1 trial. This trial was recently stopped after an interim analysis due to a lack of survival benefit for patients receiving Depatux-M compared with the placebo when added to the standard therapy. Despite this recent failure, based on our data and on the INTELLANCE 2 long-term analysis, the combination regimen may be effective in a more favorable subgroup of recurrent EGFR-amplified GBM patients. About that, recent post-hoc detailed molecular analyses on patients treated within the INTELLANCE 2/EORTC 1410 phase 2 clinical trial demonstrated that tumors harboring EGFR single-nucleotide variants (SNVs) have improved survival in the Depatux-M plus TMZ combination arm [
21]; EGFR mutations result in a receptor that is hypersensitive to ligand and increase transformation towards the active conformation of the protein. Unfortunately, we did not perform these molecular analyses to confirm the predictor role of EGFR SNVs on treatment efficacy.



 ,
, 



{kind=link}