
Neutrophil-to-Lymphocyte Ratio as a Biomarker Predicting Overall Survival after Chemoembolization for Intermediate-Stage Hepatocellular Carcinoma


 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
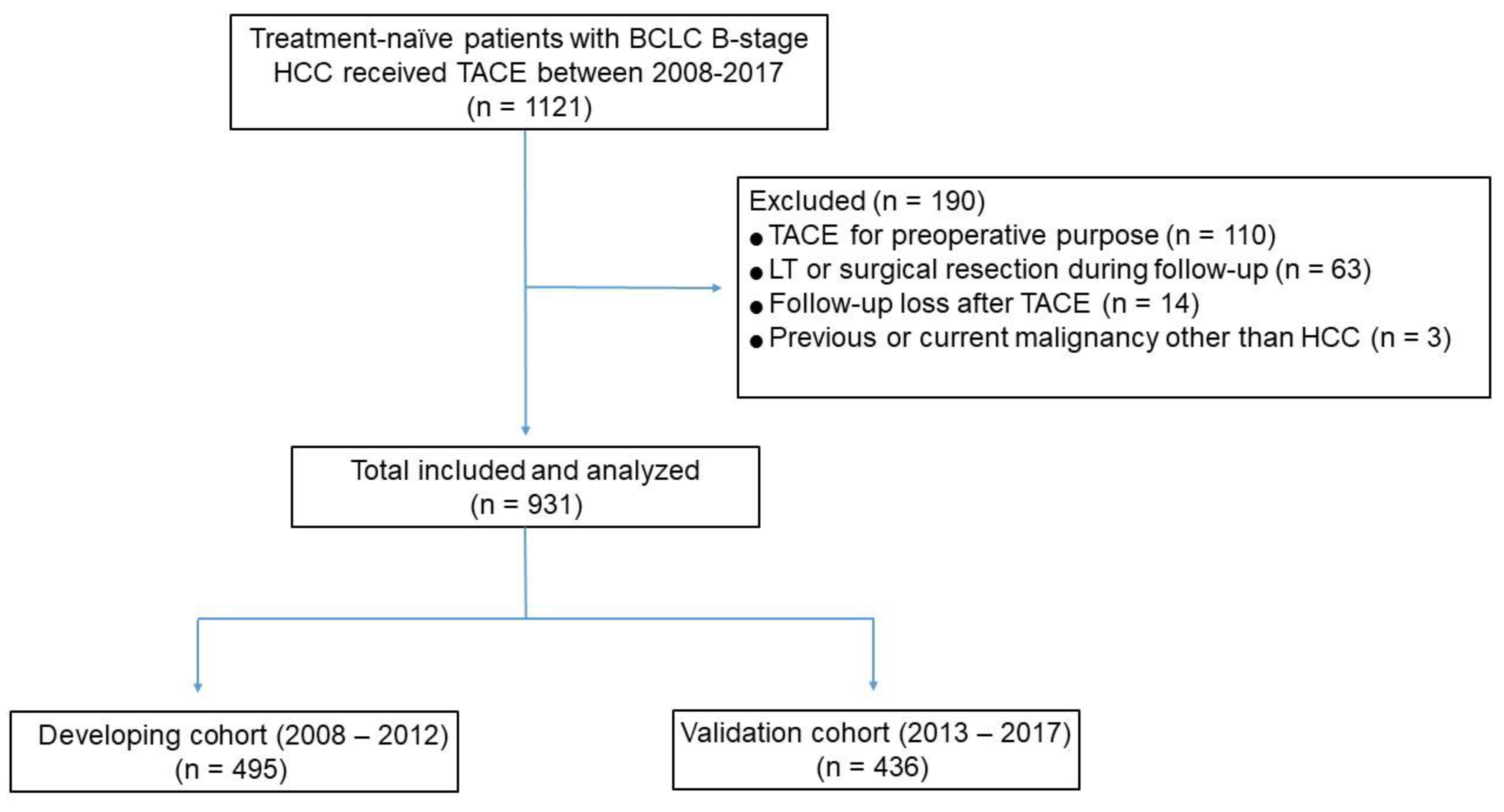
2.1. Study Design and Patients
2.2. Transarterial Chemoembolization
2.3. Study End Point
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
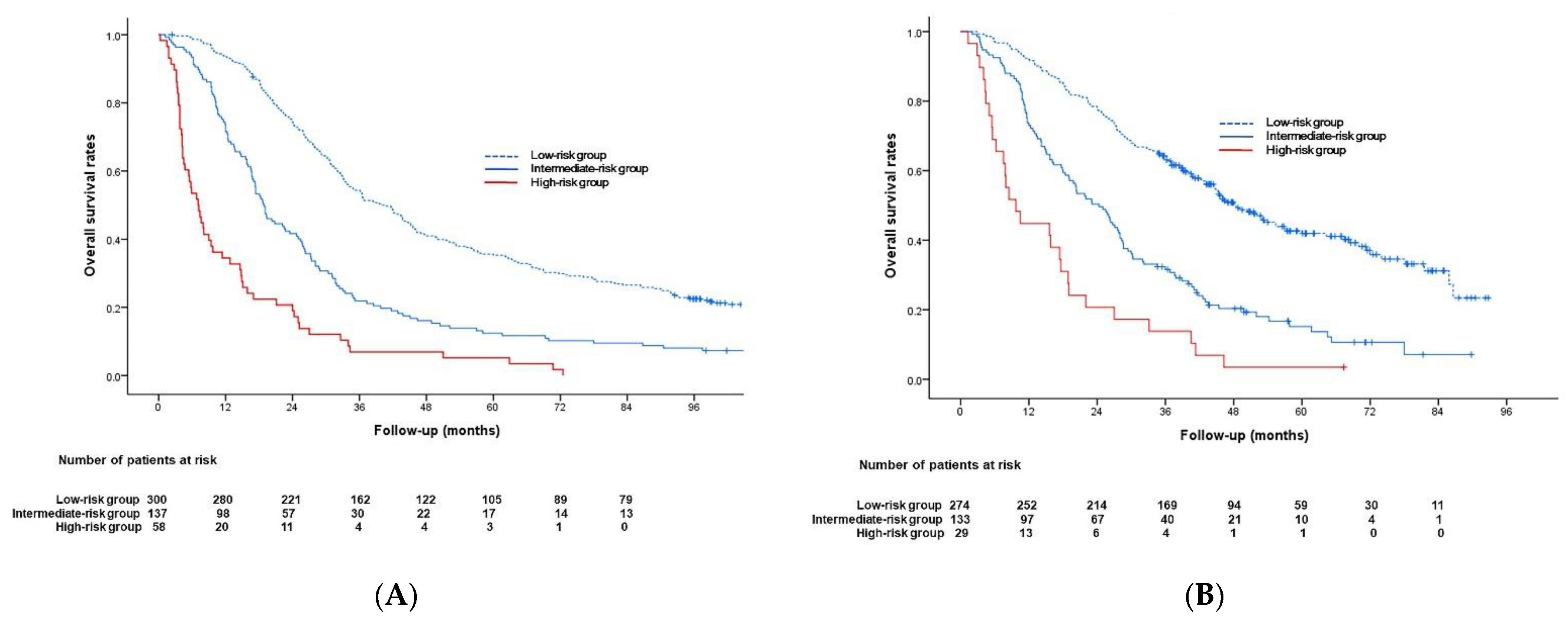
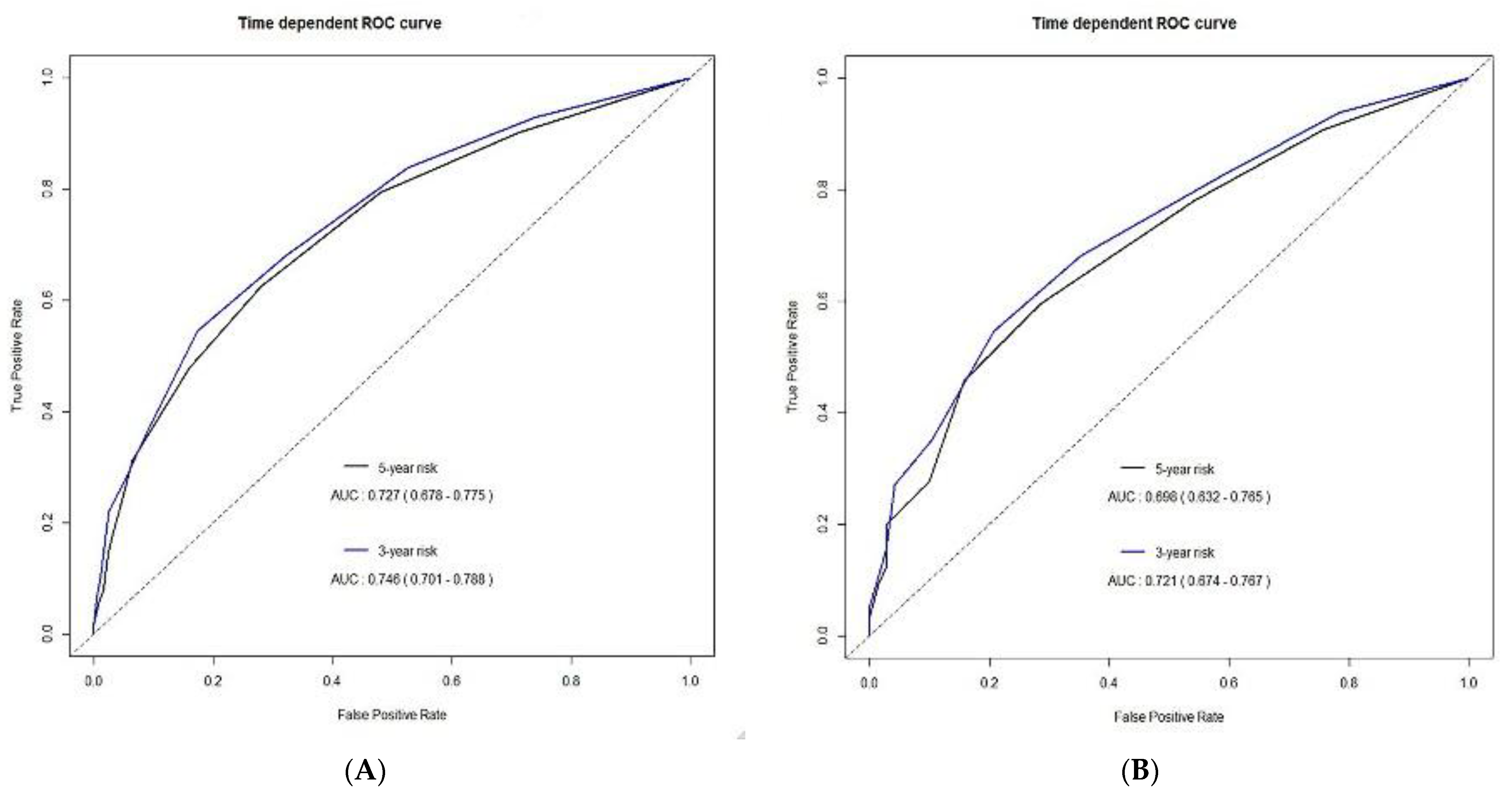
3.2. Model Predicting Overall Survival
3.3. Tumor Response 6 Months after TACE
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Llovet, J.M.; Burroughs, A.; Bruix, J. Hepatocellular carcinoma. Lancet 2003, 362, 1907–1917. [Google Scholar] [CrossRef] [Green Version]
- Llovet, J.M.; Bruix, J. Systematic review of randomized trials for unresectable hepatocellular carcinoma: Chemoembolization improves survival. Hepatology 2003, 37, 429–442. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.K.; Law, N.M.; Ng, H.S.; Machin, D. Simple clinical prognostic model for hepatocellular carcinoma in developing countries and its validation. J. Clin. Oncol. 2003, 21, 2294–2298. [Google Scholar] [CrossRef]
- Schoniger-Hekele, M.; Muller, C.; Kutilek, M.; Oesterreicher, C.; Ferenci, P.; Gangl, A. Hepatocellular carcinoma in Central Europe:prognostic features and survival. Gut 2001, 48, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Llovet, J.M. Prognostic prediction and treatment strategy in hepatocellular carcinoma. Hepatology 2002, 35, 519–524. [Google Scholar] [CrossRef]
- Cabibbo, G.; Genco, C.; Di Marco, V.; Barbara, M.; Enea, M.; Parisi, P.; Brancatelli, G.; Romano, P.; Craxi, A.; Camma’, C. Predicting survival in patients with hepatocellular carcinoma treated by transarterial chemoembolisation. Aliment. Pharmacol. Ther. 2011, 34, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Jung, M.R.; Park, Y.K.; Jeong, O.; Seon, J.W.; Ryu, S.Y.; Kim, D.Y.; Kim, Y.J. Elevated preoperative neutrophil to lymphocyte ratio predicts poor survival following resection of late stage gastric cancer. J. Surg. Oncol. 2011, 104, 504–510. [Google Scholar] [CrossRef]
- Azab, B.; Bhatt, V.R.; Phookan, J.; Murukutla, S.; Kohn, N.; Terjanian, T.; Widmann, W.D. Usefulness of the neutrophilto-lymphocyte ration in predicting short- and long-term mortality in breast cancer patients. Ann. Surg. Oncol. 2012, 19, 217–224. [Google Scholar] [CrossRef]
- Li, Y.-W.; Qiu, S.-J.; Fan, J.; Zhou, J.; Gao, Q.; Xiao, Y.-S.; Xu, Y.-F. Intratumoral neutrophils: A poor prognostic factor for hepatocellular carcinoma following resection. J. Hepatol. 2011, 54, 497–505. [Google Scholar] [CrossRef]
- Fogar, P.; Sperti, C.; Basso, D.; Sanzari, M.C.; Greco, E.; Davoli, C.; Navaglia, F.; Zambon, C.-F.; Pasquali, C.; Venza, E.; et al. Decreased total lymphocyte counts in pancreatic cancer: An index of adverse outcome. Pancreas 2006, 32, 22–28. [Google Scholar] [CrossRef]
- Mano, Y.; Shirabe, K.; Yamashita, Y.; Harimoto, N.; Tsujita, E.; Takeishi, K.; Aishima, S.; Ikegami, T.; Yoshizumi, T.; Yamanaka, T.; et al. Preoperative neutrophil-to-lymphocyte ratio is a predictor of survival after hepatectomy for hepatocellular carcinoma: A retrospective analysis. Ann. Surg. 2013, 258, 301–305. [Google Scholar] [CrossRef]
- Lué, A.; Serrano, M.T.; Bustamante, F.J.; Iñarrairaegui, M.; Arenas, J.I.; Testillano, M.; Lorente, S.; Gil, C.; De La Torre, M.; Gomez, A.; et al. Neutrophil-to-lymphocyte ratio predicts survival in european patients with hepatocellular carcinoma administered sorafenib. Oncotarget 2017, 8, 103077–103086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiyu, X.; Junyu, L.; Yi, B.; Yongchang, Z. Prognostic role of neutrophil-to-lymphocyte ratio in unresectable hepatocellular cancer patients treated with trans-arterial chemoembolization. Transl. Cancer Res. 2018, 7, 1122–1134. [Google Scholar]
- European Association for The Study of The Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Gaba, R.C.; Lokken, R.P.; Hickey, R.M.; Lipnik, A.J.; Lewandowski, R.J.; Salem, R.; Brown, D.B.; Walker, T.G.; Silberzweig, J.E.; Baerlocher, M.O.; et al. Quality improvement guidelines for transarterial chemoembolization and embolization of hepatic malignancy. J. Vasc. Interv. Radiol. 2017, 28, 1210–1223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, B.K.; Shim, J.H.; Kim, S.U.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Kim, K.M.; Lim, Y.-S.; Han, K.-H.; Lee, H.C. Risk prediction for patients with hepatocellular carcinoma undergoing chemoembolization: Development of a prediction model. Liver Int. 2016, 36, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.; Hung, Y.; Liu, C.; Lee, R.; Su, C.; Huo, T.; Li, C.; Chao, Y.; Lin, H.; Hou, M.; et al. A new ALBI-based model to predict survival after transarterial chemoembolization for BCLC stage B hepatocellular carcinoma. Liver Int. 2019, 39, 1704–1712. [Google Scholar] [CrossRef] [PubMed]
- Bannaga, A.; Arasaradnam, R.P. Neutrophil to lymphocyte ratio and albumin bilirubin grade in hepatocellular carcinoma: A systematic review. World J. Gastroenterol. 2020, 26, 5022–5049. [Google Scholar] [CrossRef]
- Lencioni, R.; Llovet, J. Modified RECIST (mRECIST) assessment for hepatoeellular carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sullivan, L.M.; Massaro, J.M.; D’Agostino Sr, R.B. Presentation of multivariate data for clinical use: The framingham study risk score functions. Stat. Med. 2004, 23, 1631–1660. [Google Scholar] [CrossRef]
- Uno, H.; Cai, T.; Tian, L.; Wei, L.J. Evaluating prediction rules for t-year survivors with censored regression models. J. Am. Stat. Assoc. 2007, 102, 527–537. [Google Scholar] [CrossRef]
- Huang, Z.-L.; Luo, J.; Chen, M.-S.; Li, J.-Q.; Shi, M. Blood neutrophil-to lymphocyte ratio predicts survival in patients with unresectable hepatocellular carcinoma undergoing transarterial chemoembolization. J. Vasc. Interv. Radiol. 2011, 22, 702–709. [Google Scholar] [CrossRef] [PubMed]
- McNally, M.E.; Martinez, A.; Khabiri, H.; Guy, G.; Michaels, A.J.; Hanje, J.; Kirkpatrick, R.; Bloomston, M.; Schmidt, C.R. Inflammatory markers are associated with outcome in patients with unresectable hepatocellular carcinoma undergoing transarterial chemoembolization. Ann. Surg. Oncol. 2013, 20, 923–928. [Google Scholar] [CrossRef]
- Wang, C.; Wang, M.; Zhang, X.; Zhao, S.; Hu, J.; Han, G.; Liu, L. The neutrophil-to-lymphocyte ratio is a predictive factor for the survival of patients with hepatocellular carcinoma undergoing transarterial chemoembolization. Ann. Transl. Med. 2020, 8, 541. [Google Scholar] [CrossRef] [PubMed]
- Chon, Y.E.; Park, H.; Hyun, H.K.; Ha, Y.; Na Kim, M.; Kim, B.K.; Lee, J.H.; Kim, S.U.; Kim, D.Y.; Ahn, S.H.; et al. Development of a new nomogram including neutrophil-to-lymphocyte ratio to predict survival in patients with hepatocellular carcinoma undergoing transarterial chemoembolization. Cancers 2019, 11, 509. [Google Scholar] [CrossRef] [Green Version]
- Bolondi, L.; Burroughs, A.; Dufour, J.F.; Galle, P.R.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.L.; Sangro, B. Heterogeneity of patients with intermediate (BCLC B) hepatocellular carcinoma: Proposal for a subclassification to facilitate treatment decisions. Semin. Liver Dis. 2012, 32, 348–359. [Google Scholar] [PubMed]
- Xiao, W.-K.; Chen, D.; Li, S.-Q.; Fu, S.-J.; Peng, B.-G.; Liang, L.-J. Prognostic significance of neutrophil-lymphocyte ratio in hepatocellular carcinoma: A meta-analysis. BMC Cancer 2014, 14, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Memon, K.; Kulik, L.; Lewandowski, R.J.; Wang, E.; Riaz, A.; Ryu, R.K.; Sato, K.T.; Marshall, K.; Gupta, R.; Nikolaidis, P.; et al. Radiographic response to locoregional therapy in hepatocellular carcinoma predicts patient survival times. Gastroenterology 2011, 141, 526–535.e1–2. [Google Scholar] [CrossRef]
- Cruz, J.C.; Watchmaker, J.M.; Albin, M.M.; Wang, L.; Wu, G.; Baker, J.C.; Fritsche, M.R.; Alexopoulos, S.P.; Matsuoka, L.; Fleming, J.W.; et al. Neutrophil/Lymphocyte ratio predicts increased risk of immediate progressive disease following chemoembolization of hepatocellular carcinoma. J. Vasc. Interv. Radiol. 2019, 30, 1887–1892. [Google Scholar] [CrossRef]
- Hickey, R.M.; Kulik, L.M.; Nimeiri, H.; Kalyan, A.; Kircher, S.; Desai, K.; Riaz, A.; Lewandowski, R.J.; Salem, R. Immuno-oncology and its opportunities for interventional radiologists: Immune checkpoint inhibition and potential synergies with interventional oncology procedures. J. Vasc. Interv. Radiol. 2017, 28, 1487–1494. [Google Scholar] [CrossRef]
- Prince, D.; Liu, K.; Xu, W.; Chen, M.; Sun, J.-Y.; Lu, X.-J.; Ji, J. Management of patients with intermediate stage hepatocellular carcinoma. Ther. Adv. Med. Oncol. 2020, 12, 1–17. [Google Scholar] [CrossRef]
- Yi, P.S.; Wang, H.; Li, J.S. Evolution and current status of the subclassification of intermediate hepatocellular carcinoma. World J. Gastrointest. Surg. 2020, 12, 85–92. [Google Scholar] [CrossRef]
- Golfieri, R.; Bargellini, I.; Spreafico, C.; Trevisani, F. Patients with Barcelona Clinic Liver Cancer Stages B and C hepatocellular carcinoma: Time for a subclassification. Liver Cancer 2019, 8, 78–91. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Shim, J.H.; Lee, H.C.; Sung, K.-B.; Ko, H.-K.; Ko, G.-Y.; Gwon, D.I.; Kim, J.W.; Lim, Y.-S.; Park, S.H. New intermediate-stage subclassification for patients with hepatocellular carcinoma treated with transarterial chemoembolization. Liver Int. 2017, 37, 1861–1868. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Xia, D.; Bai, W.; Wang, E.; Sun, J.; Huang, M.; Mu, W.; Yin, G.; Li, H.; Zhao, H.; et al. Development of a prognostic score for recommended TACE candidates with hepatocellular carcinoma: A multicenter observational study. J. Hepatol. 2019, 70, 893–903. [Google Scholar] [CrossRef]
- Hu, K.; Tang, B.; Yuan, J.; Lu, S.; Li, M.; Chen, R.; Zhang, L.; Ren, Z.; Yin, X. A new substage classification strategy for Barcelona Clinic Liver Cancer stage B patients with hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2019, 34, 1984–1991. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.-H.; Kee, K.-M.; Lin, C.-Y.; Hung, C.-H.; Chen, C.-H.; Lee, C.-M.; Lu, S.-N. Validation and modification of a proposed substaging system for patients with intermediate hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2015, 30, 358–363. [Google Scholar] [CrossRef]
- Lee, Y.J.; Lee, Y.R.; Seo, C.G.; Goh, H.G.; Kim, T.H.; Yim, S.Y.; Han, N.Y.; Lee, J.M.; Choi, H.S.; Kim, E.S.; et al. How should we assign large infiltrative hepatocellular carcinomas for staging? Cancers 2020, 12, 2589. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients | Development Cohort | Validation Cohort | p-Value |
|---|---|---|---|---|
| Patients | 931 | 495 | 436 | |
| Age, years | 59.4 ± 9.8 | 58.2 ± 9.9 | 60.8 ± 9.6 | <0.001 |
| Sex | >0.999 | |||
| Male | 810 (87) | 431 (87.1) | 379 (86.9) | |
| Female | 121 (13) | 64 (12.9) | 57 (13.1) | |
| Etiology | 0.071 | |||
| HBV | 699 (75.1) | 385 (77.8) | 314 (72.1) | |
| HCV | 101 (10.8) | 52 (10.5) | 49 (11.2) | |
| Others | 131 (14.1) | 58 (11.7) | 73 (16.7) | |
| Child–Pugh class | 0.556 | |||
| A | 812 (87.2) | 435 (87.9) | 377 (86.5) | |
| B | 119 (12.8) | 60 (12.1) | 59 (13.5) | |
| Maximum tumor size, cm | 0.792 | |||
| ≤5 | 424 (45.5) | 223 (45.1) | 201 (46.1) | |
| >5 | 507 (54.5) | 272 (54.9) | 235 (53.9) | |
| Number of tumors | 0.262 | |||
| 2–3 | 421 (45.2) | 215 (43.4) | 206 (47.2) | |
| ≥4 | 510 (54.8) | 280 (56.6) | 230 (52.8) | |
| Tumor involvement | 0.893 | |||
| Unilobar | 373 (40.1) | 197 (39.8) | 176 (40.4) | |
| Bilobar | 558 (59.9) | 298 (60.2) | 260 (59.6) | |
| AFP, ng/mL | 0.254 | |||
| <200 | 560 (60.2) | 289 (58.4) | 271 (62.2) | |
| ≥200 | 371 (39.8) | 206 (41.6) | 165 (37.8) | |
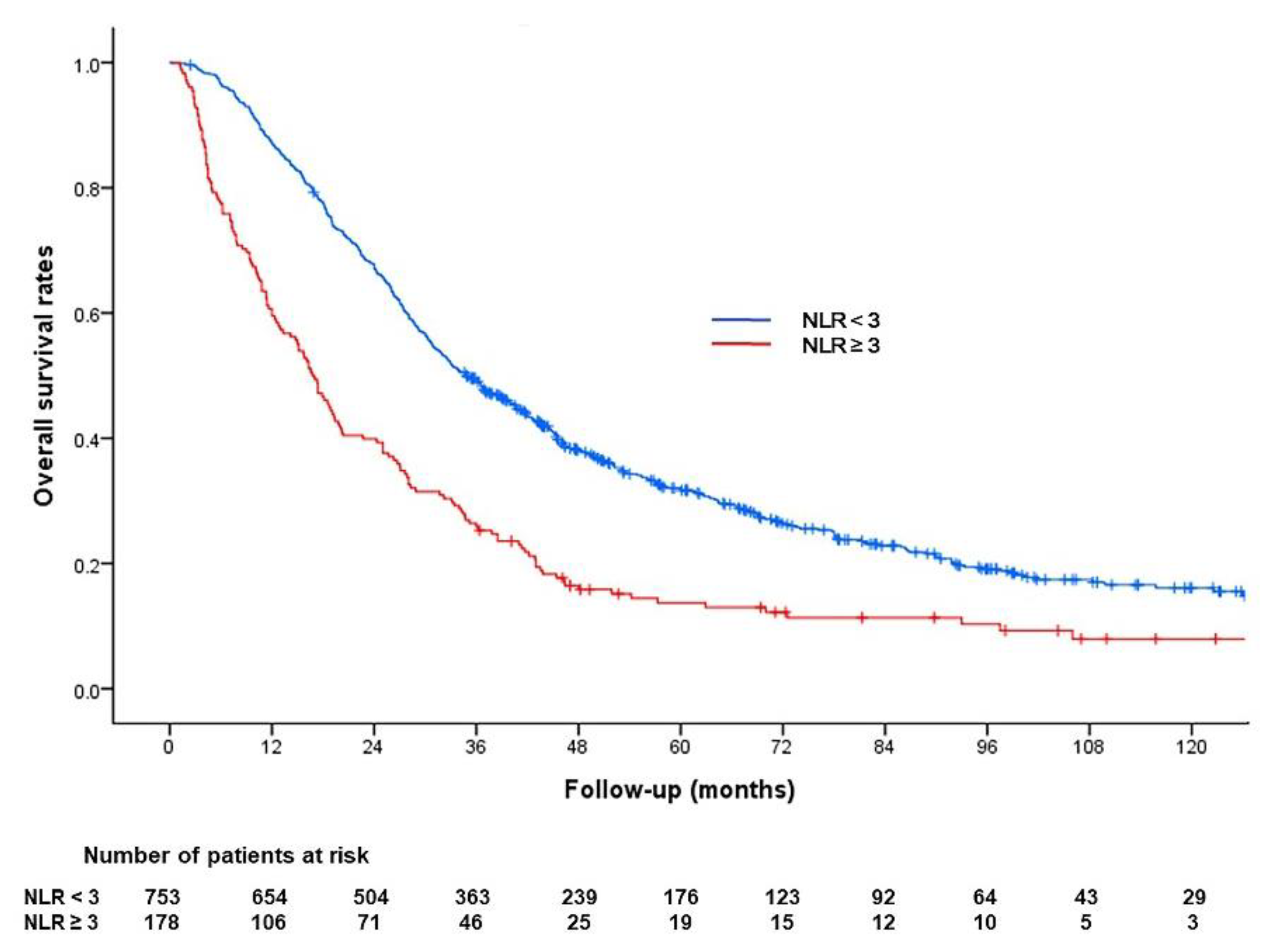
| Neutrophil/lymphocyte ratio | 0.867 | |||
| <3 | 753 (80.9) | 399 (80.6) | 354 (81.2) | |
| ≥3 | 178 (19.1) | 96 (19.4) | 82 (18.8) |
| Variable | Univariable Cox Regression Analysis | Multivariable Cox Regression Analysis | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | Adjusted HR | 95% CI | p-Value | β-Coefficients | Beta (W-Wref)/B | Risk Point | |||
| Maximum tumor size > 5 cm | 1.73 | 1.43 | 2.09 | <0.001 | 1.30 | 1.06 | 1.61 | 0.013 | 0.27 | 1.29 | 1 |
| Tumor number ≥ 4 | 2.08 | 1.71 | 2.53 | <0.001 | 1.67 | 1.35 | 2.05 | <0.001 | 0.51 | 2.47 | 2 |
| Infiltrative tumor type | 3.11 | 2.40 | 4.02 | <0.001 | 2.28 | 1.73 | 3.01 | <0.001 | 0.82 | 3.99 | 4 |
| Bilobar involvement | 1.63 | 1.34 | 1.99 | <0.001 | |||||||
| AFP ≥ 200 ng/mL | 1.47 | 1.21 | 1.77 | <0.001 | 1.23 | 1.01 | 1.50 | 0.042 | 0.21 | 1.00 | 1 |
| Neutrophil/lymphocyte ratio ≥ 3 | 1.93 | 1.53 | 2.44 | <0.001 | 1.41 | 1.10 | 1.81 | 0.007 | 0.35 | 1.67 | 2 |
| Child–Pugh B | 1.64 | 1.24 | 2.18 | 0.001 | 1.66 | 1.24 | 2.23 | <0.001 | 0.51 | 2.46 | 2 |
| Age | 1.00 | 0.99 | 1.01 | 0.541 | |||||||
| Male sex | 1.06 | 0.79 | 1.41 | 0.706 | |||||||
| Etiology | 0.436 | ||||||||||
| HBV | 1 | ||||||||||
| HCV | 1.19 | 0.88 | 1.63 | 0.263 | |||||||
| Others | 1.12 | 0.84 | 1.49 | 0.433 | |||||||
| Variable | Univariable Logistic Regression Analysis | Multivariable Logistic Regression Analysis | ||||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | Adjusted OR | 95% CI | p-Value | |||
| Maximum tumor size > 5 cm | 4.17 | 3.05 | 5.69 | <0.001 | 2.18 | 1.53 | 3.10 | <0.001 |
| Tumor number ≥ 4 | 5.18 | 3.75 | 7.17 | <0.001 | 3.44 | 2.37 | 4.98 | <0.001 |
| Infiltrative tumor type | 6.06 | 4.02 | 9.13 | <0.001 | 3.18 | 1.99 | 5.07 | <0.001 |
| Bilobar involvement | 2.74 | 2.01 | 3.72 | <0.001 | 1.38 | 0.96 | 2.00 | 0.085 |
| AFP ≥ 200 ng/mL | 2.52 | 1.89 | 3.34 | <0.001 | 1.76 | 1.27 | 2.45 | 0.001 |
| Neutrophil/lymphocyte ratio ≥ 3 | 4.36 | 3.10 | 6.14 | <0.001 | 3.35 | 2.27 | 4.94 | <0.001 |
| Child Pugh B | 1.67 | 1.13 | 2.47 | 0.011 | 1.40 | 0.87 | 2.24 | 0.166 |
| Age | 0.98 | 0.96 | 0.99 | 0.002 | 0.99 | 0.98 | 1.01 | 0.290 |
| Male sex | 1.37 | 0.92 | 2.04 | 0.116 | ||||
| Etiology | 0.859 | |||||||
| HBV | 1 | |||||||
| HCV | 1.03 | 0.66 | 1.61 | 0.900 | ||||
| Others | 0.89 | 0.59 | 1.35 | 0.608 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chu, H.H.; Kim, J.H.; Shim, J.H.; Gwon, D.I.; Ko, H.-K.; Shin, J.H.; Ko, G.-Y.; Yoon, H.-K.; Kim, N. Neutrophil-to-Lymphocyte Ratio as a Biomarker Predicting Overall Survival after Chemoembolization for Intermediate-Stage Hepatocellular Carcinoma. Cancers 2021, 13, 2830. https://doi.org/10.3390/cancers13112830
Chu HH, Kim JH, Shim JH, Gwon DI, Ko H-K, Shin JH, Ko G-Y, Yoon H-K, Kim N. Neutrophil-to-Lymphocyte Ratio as a Biomarker Predicting Overall Survival after Chemoembolization for Intermediate-Stage Hepatocellular Carcinoma. Cancers. 2021; 13(11):2830. https://doi.org/10.3390/cancers13112830
Chicago/Turabian StyleChu, Hee Ho, Jin Hyoung Kim, Ju Hyun Shim, Dong Il Gwon, Heung-Kyu Ko, Ji Hoon Shin, Gi-Young Ko, Hyun-Ki Yoon, and Nayoung Kim. 2021. "Neutrophil-to-Lymphocyte Ratio as a Biomarker Predicting Overall Survival after Chemoembolization for Intermediate-Stage Hepatocellular Carcinoma" Cancers 13, no. 11: 2830. https://doi.org/10.3390/cancers13112830