
Loss of Paid Employment up to 4 Years after Colorectal Cancer Diagnosis—A Nationwide Register-Based Study with a Population-Based Reference Group

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
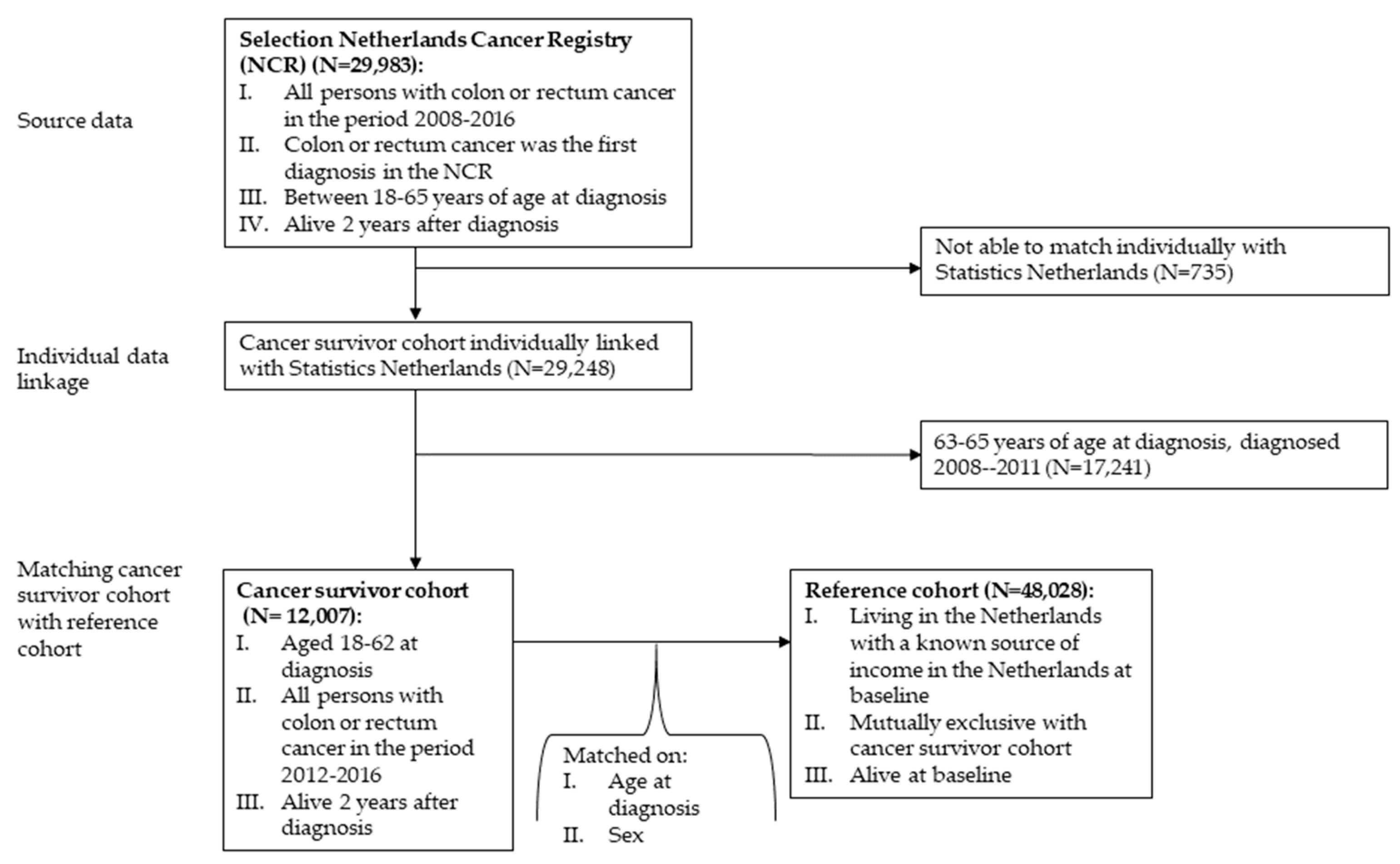
2.1. Datasets and Study Sample
2.2. Measures
2.2.1. Sociodemographic Characteristics
2.2.2. Work-Related Characteristics
2.2.3. Cancer-Related Characteristics
2.2.4. Loss of Paid Employment
2.3. Statistical Analyses
3. Results
3.1. Characteristics of Cancer Survivor Sample and Reference Sample
3.2. Comparison between Cancer Survivor Sample and the Population-Based Reference Sample
3.3. Cancer Survivor Sample
3.3.1. Disability Benefits
3.3.2. Unemployment Benefits
3.3.3. Social Welfare
3.3.4. Loss of Paid Employment
4. Discussion
4.1. Interpretation of the Findings
4.2. Strengths and Limitations
4.3. Recommendations for Further Research and Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Netherlands Cancer Registry. Available online: www.iknl.nl/nkr-cijfers.nl (accessed on 1 April 2021).
- Statistics Netherlands. Available online: www.cbs.nl (accessed on 1 April 2021).
- Schreuders, E.H.; Ruco, A.; Rabeneck, L.; Schoen, R.E.; Sung, J.J.; Young, G.P.; Kuipers, E.J. Colorectal cancer screening: A global overview of existing programmes. Gut 2015, 64, 1637–1649. [Google Scholar] [CrossRef] [PubMed]
- De Boer, A.; Taskila, T.; Ojajärvi, A.; van Dijk, F.; Verbeek, J. Cancer survivors and unemployment-A meta-analysis and meta-regression. JAMA 2009, 301, 753–762. [Google Scholar] [CrossRef] [PubMed]
- Schuring, M.; Mackenbach, J.; Voorham, T.; Burdorf, A. The effect of re-employment on perceived health. J. Epidemiol. Community Health 2011, 65, 639–644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallo, W.T.; Teng, H.M.; Falba, T.A.; Kasl, S.V.; Krumholz, H.M.; Bradley, E.H. The impact of late career job loss on myocardial infarction and stroke: A 10 year follow up using the health and retirement survey. Occup. Environ. Med. 2006, 63, 683–687. [Google Scholar] [CrossRef] [PubMed]
- Duijts, S.F.; Kieffer, J.M.; van Muijen, P.; van der Beek, A.J. Sustained employability and health-related quality of life in cancer survivors up to four years after diagnosis. Acta Oncol. 2017, 56, 174–182. [Google Scholar] [CrossRef] [Green Version]
- Thomas, C.; Benzeval, M.; Stansfeld, S.A. Employment transitions and mental health: An analysis from the British household panel survey. J. Epidemiol. Community Health 2005, 59, 243–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsson, M.I.; Saboonchi, F.; Alexanderson, K.; Olsson, M.; Wennman-Larsen, A.; Petersson, L.M. Changes in importance of work and vocational satisfaction during the 2 years after breast cancer surgery and factors associated with this. J. Cancer Surviv. 2016, 10, 564–572. [Google Scholar] [CrossRef]
- Tiedtke, C.; de Rijk, A.; de Casterle, B.D.; Christiaens, M.R.; Donceel, P. Experiences and concerns about ‘returning to work’ for women breast cancer survivors: A literature review. Psychooncology 2010, 19, 677–683. [Google Scholar] [CrossRef]
- Wells, M.; Williams, B.; Firnigl, D.; Lang, H.; Coyle, J.; Kroll, T.; MacGillivray, S. Supporting ‘work-related goals’ rather than ‘return to work’ after cancer? A systematic review and meta-synthesis of 25 qualitative studies. Psychooncology 2013, 22, 1208–1219. [Google Scholar] [CrossRef] [PubMed]
- Timperi, A.W.; Ergas, I.J.; Rehkopf, D.H.; Roh, J.M.; Kwan, M.L.; Kushi, L.H. Employment status and quality of life in recently diagnosed breast cancer survivors. Psychooncology 2013, 22, 1411–1420. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.E.; Scherer, S.; Wiskemann, J.; Steindorf, K. Return to work after breast cancer: The role of treatment-related side effects and potential impact on quality of life. Eur. J. Cancer Care 2019, 28, e13051. [Google Scholar] [CrossRef] [PubMed]
- Beesley, V.L.; Vallance, J.K.; Mihala, G.; Lynch, B.M.; Gordon, L.G. Association between change in employment participation and quality of life in middle-aged colorectal cancer survivors compared with general population controls. Psychooncology 2017, 26, 1354–1360. [Google Scholar] [CrossRef] [Green Version]
- Syse, A.; Tretli, S.; Kravdal, O. Cancer’s impact on employment and earnings--a population-based study from Norway. J. Cancer Surviv. 2008, 2, 149–158. [Google Scholar] [CrossRef] [Green Version]
- Gordon, L.G.; Beesley, V.L.; Mihala, G.; Koczwara, B.; Lynch, B.M. Reduced employment and financial hardship among middle-aged individuals with colorectal cancer. Eur. J. Cancer Care 2017, 26, e12744. [Google Scholar] [CrossRef] [PubMed]
- Pearce, A.; Tomalin, B.; Kaambwa, B.; Horevoorts, N.; Duijts, S.; Mols, F.; van de Poll-Franse, L.; Koczwara, B. Financial toxicity is more than costs of care: The relationship between employment and financial toxicity in long-term cancer survivors. J. Cancer Surviv. 2019, 13, 10–20. [Google Scholar] [CrossRef]
- Loisel, P.; Durand, M.J.; Berthelette, D.; Vezina, N.; Baril, R.; Gagnon, D.; Lariviere, C.; Tremblay, C. Disability prevention-new paradigm for the management of occupational back pain. Dis. Manag. Health Outcomes 2001, 9, 351–360. [Google Scholar] [CrossRef]
- Feuerstein, M.; Todd, B.L.; Moskowitz, M.C.; Bruns, G.L.; Stoler, M.R.; Nassif, T.; Yu, X. Work in cancer survivors: A model for practice and research. J. Cancer Surviv. 2010, 4, 415–437. [Google Scholar] [CrossRef]
- Islam, T.; Dahlui, M.; Abd Majid, H.; Nahar, A.M.; Taib, N.A.M.; Su, T.T. Factors associated with return to work of breast cancer survivors: A systematic review. BMC Public Health 2014, 14 (Suppl. 3), S8. [Google Scholar] [CrossRef] [Green Version]
- de Boer, A.; Greidanus, M.A.; Dewa, C.S.; Duijts, S.F.A.; Tamminga, S.J. Introduction to special section on: Current topics in cancer survivorship and work. J. Cancer Surviv. 2020, 14, 101–105. [Google Scholar] [CrossRef] [Green Version]
- Butow, P.; Laidsaar-Powell, R.; Konings, S.; Lim, C.Y.S.; Koczwara, B. Return to work after a cancer diagnosis: A meta-review of reviews and a meta-synthesis of recent qualitative studies. J. Cancer Surviv. 2020, 14, 114–134. [Google Scholar] [CrossRef]
- den Bakker, C.M.; Anema, J.R.; Zaman, A.; de Vet, H.C.W.; Sharp, L.; Angenete, E.; Allaix, M.E.; Otten, R.H.J.; Huirne, J.A.F.; Bonjer, H.J.; et al. Prognostic factors for return to work and work disability among colorectal cancer survivors; A systematic review. PLoS ONE 2018, 13, e0200720. [Google Scholar] [CrossRef]
- den Bakker, C.M.; Anema, J.R.; Huirne, J.A.F.; Twisk, J.; Bonjer, H.J.; Schaafsma, F.G. Predicting return to work among patients with colorectal cancer. Br. J. Surg. 2020, 107, 140–148. [Google Scholar] [CrossRef] [Green Version]
- Sanchez, K.M.; Richardson, J.L.; Mason, H.R. The return to work experiences of colorectal cancer survivors. AAOHN J. 2004, 52, 500–510. [Google Scholar] [CrossRef] [PubMed]
- Gordon, L.G.; Beesley, V.L.; Lynch, B.M.; Mihala, G.; McGrath, C.; Graves, N.; Webb, P.M. The return to work experiences of middle-aged Australian workers diagnosed with colorectal cancer: A matched cohort study. BMC Public Health 2014, 14, 963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhalla, A.; Williams, J.P.; Hurst, N.G.; Speake, W.J.; Tierney, G.M.; Tou, S.; Lund, J.N. One-third of patients fail to return to work 1 year after surgery for colorectal cancer. Tech. Coloproctol. 2014, 18, 1153–1159. [Google Scholar] [CrossRef]
- Earle, C.C.; Chretien, Y.; Morris, C.; Ayanian, J.Z.; Keating, N.L.; Polgreen, L.A.; Wallace, R.; Ganz, P.A.; Weeks, J.C. Employment among survivors of lung cancer and colorectal cancer. J. Clin. Oncol. 2010, 28, 1700–1705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlsen, K.; Harling, H.; Pedersen, J.; Christensen, K.B.; Osler, M. The transition between work, sickness absence and pension in a cohort of Danish colorectal cancer survivors. BMJ Open 2013, 3. [Google Scholar] [CrossRef] [Green Version]
- van Egmond, M.P.; Anema, J.R.; Singh, A.; van der Beek, A.J.; Duijts, S.F. Factors associated with (non-)participation of cancer survivors with job loss in a supportive return to work program. Support Care Cancer 2016, 24, 3175–3184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamminga, S.J.; Verbeek, J.H.; Bos, M.M.; Fons, G.; Kitzen, J.J.; Plaisier, P.W.; Frings-Dresen, M.H.; de Boer, A.G. Effectiveness of a hospital-based work support intervention for female cancer patients-a multi-centre randomised controlled trial. PLoS ONE 2013, 8, e63271. [Google Scholar] [CrossRef]
- Roick, J.; Danker, H.; Kersting, A.; Briest, S.; Dietrich, A.; Dietz, A.; Einenkel, J.; Papsdorf, K.; Lordick, F.; Meixensberger, J.; et al. Factors associated with non-participation and dropout among cancer patients in a cluster-randomised controlled trial. Eur. J. Cancer Care 2018, 27. [Google Scholar] [CrossRef]
- Netherlands Comprehensive Cancer Organisation. Available online: www.iknl.nl (accessed on 7 June 2021).
- Schoenfeld, D. Partial residuals for the proportional hazards regression model. Biometrika 1982, 69, 239–241. [Google Scholar] [CrossRef]
- Schoenfeld, D. Chi-squared goodness-of-fit tests for the proportional hazards regression model. Biometrika 1980, 67, 145–153. [Google Scholar] [CrossRef]
- Paalman, C.H.; van Leeuwen, F.E.; Aaronson, N.K.; de Boer, A.G.; van de Poll-Franse, L.; Oldenburg, H.S.; Schaapveld, M. Employment and social benefits up to 10 years after breast cancer diagnosis: A population-based study. Br. J. Cancer 2016, 114, 81–87. [Google Scholar] [CrossRef] [Green Version]
- Therneau, T. A Package for Survival Analysis in R; R Package Version: 3.2-10 2021; Springer: New York, NY, USA, 2021. [Google Scholar]
- Therneau, T.M.; Grambsch, P.M. Modeling Survival Data: Extending the Cox Model; Springer: New York, NY, USA, 2000. [Google Scholar]
- Hauglann, B.K.; Saltyte Benth, J.; Fossa, S.D.; Tveit, K.M.; Dahl, A.A. A controlled cohort study of sickness absence and disability pension in colorectal cancer survivors. Acta Oncol. 2014, 53, 735–743. [Google Scholar] [CrossRef] [Green Version]
- Beermann, L.C.; Alexanderson, K.; Martling, A.; Chen, L. Overall and diagnosis-specific sickness absence and disability pension in colorectal cancer survivors and references in Sweden. J. Cancer Surviv. 2021. [Google Scholar] [CrossRef]
- van Muijen, P.; Weevers, N.L.; Snels, I.A.; Duijts, S.F.; Bruinvels, D.J.; Schellart, A.J.; Van der Beek, A.J. Predictors of return to work and employment in cancer survivors: A systematic review. Eur. J. Cancer Care 2013, 22, 144–160. [Google Scholar] [CrossRef]
- Ervasti, J.; Virtanen, M.; Lallukka, T.; Friberg, E.; Mittendorfer-Rutz, E.; Lundstrom, E.; Alexanderson, K. Permanent work disability before and after ischaemic heart disease or stroke event: A nationwide population-based cohort study in Sweden. BMJ Open 2017, 7, e017910. [Google Scholar] [CrossRef]
- Vooijs, M.; Leensen, M.C.; Hoving, J.L.; Daams, J.G.; Wind, H.; Frings-Dresen, M.H. Disease-generic factors of work participation of workers with a chronic disease: A systematic review. Int. Arch. Occup. Environ. Health 2015, 88, 1015–1029. [Google Scholar] [CrossRef]
- Kim, S.E.; Paik, H.Y.; Yoon, H.; Lee, J.E.; Kim, N.; Sung, M.K. Sex- and gender-specific disparities in colorectal cancer risk. World J. Gastroenterol. 2015, 21, 5167–5175. [Google Scholar] [CrossRef]
- Coutu, M.F.; Durand, M.J.; Cote, D.; Tremblay, D.; Sylvain, C.; Gouin, M.M.; Bilodeau, K.; Nastasia, I.; Paquette, M.A. How does Gender Influence Sustainable Return to Work Following Prolonged Work Disability? An Interpretive Description Study. J. Occup. Rehabil. 2021. [Google Scholar] [CrossRef] [PubMed]
- Rottenberg, Y.; Ratzon, N.Z.; Cohen, M.; Hubert, A.; Uziely, B.; de Boer, A.G. Unemployment risk at 2 and 4 years following colorectal cancer diagnosis: A population based study. Eur. J. Cancer. 2016, 69, 70–76. [Google Scholar] [CrossRef]
- Sharp, L.; Torp, S.; Van Hoof, E.; de Boer, A. Cancer and its impact on work among the self-employed: A need to bridge the knowledge gap. Eur. J. Cancer Care 2017, 26, e12746. [Google Scholar] [CrossRef] [PubMed]
- Bains, M.; Munir, F.; Yarker, J.; Steward, W.; Thomas, A. Return-to-work guidance and support for colorectal cancer patients: A feasibility study. Cancer Nurs. 2011, 34, E1–E12. [Google Scholar] [CrossRef]
- Zaman, A.; Tytgat, K.; Klinkenbijl, J.H.G.; de Boer, A.; Frings-Dresen, M.H.W. Process evaluation of a tailored work-related support intervention for patients diagnosed with gastrointestinal cancer. J. Cancer Surviv. 2020, 14, 59–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burbach, J.P.; Kurk, S.A.; Coebergh van den Braak, R.R.; Dik, V.K.; May, A.M.; Meijer, G.A.; Punt, C.J.; Vink, G.R.; Los, M.; Hoogerbrugge, N.; et al. Prospective Dutch colorectal cancer cohort: An infrastructure for long-term observational, prognostic, predictive and (randomized) intervention research. Acta Oncol. 2016, 55, 1273–1280. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, P.; Laurberg, S.; Andersen, N.T.; Steenstra., I.; Nielsen, C.V.; Maribo, T.; Juul, T. Differences in work participation between incident colon and rectal cancer patients-a 10-year follow-up study with matched controls. J. Cancer Surviv. 2021. [Google Scholar] [CrossRef] [PubMed]
- Gordon, L.G.; Lynch, B.M.; Beesley, V.L.; Graves, N.; McGrath, C.; O’Rourke, P.; Webb, P.M. The Working After Cancer Study (WACS): A population-based study of middle-aged workers diagnosed with colorectal cancer and their return to work experiences. BMC Public Health 2011, 11, 604. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Cancer Survivor Cohort(N = 12,007) | Reference Cohort(N = 48,028) | ||
|---|---|---|---|
| Paid work one month before diagnosis (N (% yes)) | 8275 (69%) | 32,143 (68%) | |
| Age at time of colorectal cancer diagnosis (mean (±SD)) | 55.4 (±6.9) | 55.4 (± 6.9) 1 | |
| Sex N (% male) | 6844 (57%) | 27,444 (57%) 1 | |
| Treatment * | Surgery | 11,400 (95%) | NA |
| Chemotherapy | 6093 (51%) | ||
| Radiotherapy | 3398 (28%) | ||
| Targeted | 695 (6%) | ||
| Stage at diagnosis | I | 2800 (23%) | NA |
| II | 2762 (23%) | ||
| III | 4860 (40%) | ||
| IV | 1585 (13%) | ||
| Flex work (N (% yes)) | 464 (6%) | 1735 (5%) | |
| Self-employed (N (% yes)) | 1242 (10%) | 5118 (11%) | |
| Income before diagnosis | <500 | 2755 (23%) | 11,778 (25%) |
| 500–20 k | 2262 (19%) | 8785 (18%) | |
| 20 k–35 k | 2216 (19%) | 8808 (19%) | |
| 35 k–50 k | 2166 (18%) | 8207 (17%) | |
| >50 k | 2535 (21%) | 9934 (21%) | |
| Cancer Survivor Cohort(N = 8275) | Reference Cohort(N = 32,143) | ||
|---|---|---|---|
| Age at diagnosis/baseline | <45 | 742 (9%) | 3000 (9%) |
| 45–55 | 2673 (32%) | 10,272 (32%) | |
| 56–60 | 2447 (30%) | 9645 (30%) | |
| >60 | 2413 (29%) | 9226 (29%) | |
| Sex N (% male) | 5150 (62%) | 19,906 (62%) | |
| Treatment * | Surgery | 7852 (95%) | NA |
| Chemotherapy | 4323 (52%) | ||
| Radiotherapy | 2453 (30%) | ||
| Targeted | 507 (6%) | ||
| Stage at diagnosis | I | 1835 (22%) | NA |
| II | 1900 (23%) | ||
| III | 3402 (41%) | ||
| IV | 1138 (14%) | ||
| Flex work (N (% yes)) | 316 (6%) | 1193 (6%) | |
| Self-employed (N (% yes)) | 1242 (15%) | 5118 (16%) | |
| Income before diagnosis | <500 | 153 (2%) | 597 (2%) |
| 500–20 k | 1764 (21%) | 6774 (21%) | |
| 20 k–35 k | 2071 (25%) | 8170 (26%) | |
| 35 k–50 k | 2048 (25%) | 7686 (24%) | |
| >50 k | 2217 (27%) | 8800 (27%) | |
| Disability Benefits (2–4 Years) 1 | Unemployment Benefits 0–4 Years 2 | Social Welfare 0–4 Years 3 | Loss of Paid Employment (2–4 Years) 4 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Number of Observations | N = 24,655 | N = 40,418 | N = 40,418 | N = 22,865 | |||||
| HR (95 CI%) | p-Value | HR (95 CI%) | p-Value | HR (95 CI%) | p-Value | HR (95 CI%) | p-Value | ||
| Colorectal cancer | Colorectal cancer | 4.41 (3.90, 4.98) | <0.001 | 0.73 (0.66,0.79) | <0.001 | - | - | 1.56 (1.42, 1.71) | <0.001 |
| No colorectal cancer * | Reference | - | Reference | - | - | - | Reference | - | |
| Age at diagnosis/baseline | <45 | 1.16 (0.94, 1.43) | 0.167 | - | - | 1.31 (1.00, 1.72) | 0.048 | 1.21 (1.05, 1.39) | 0.007 |
| 45–55 * | Reference | - | - | Reference | Reference | ||||
| 56–60 | 1.02 (0.88, 1.19) | 0.779 | - | - | 0.67 (0.53, 0.84) | 0.001 | 1.00 (0.90, 1.10) | 0.965 | |
| >60 | 0.70 (0.59, 0.83) | <0.001 | - | - | 0.39 (9.29, 0.53) | <0.001 | 0.70 (0.62, 0.78) | <0.001 | |
| Sex | Male | - | - | - | - | 0.59 (0.49, 0.71) | <0.001 | - | - |
| Female * | - | - | - | - | Reference | - | - | ||
| Self-employed | Yes | 0.42 (0.34, 0.54) | <0.001 | - | - | 1.37 (1.07, 1.75) | 0.011 | 0.66 (0.57, 0.75) | <0.001 |
| No * | Reference | - | - | Reference | - | Reference | - | ||
| Disability Benefits (2–4 Years) 1 | Unemployment Benefits (0–4 Years) 2 | Social Welfare (0–4 Years) 3 | Loss of Paid Employment (2–4 Years) 4 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Number of Observations | N = 4694 | N = 8275 | N = 8275 | N = 4290 | |||||
| HR (95 CI%) | p-Value | HR (95 CI%) | p-Value | HR (95 CI%) | p-Value | HR (95 CI%) | p-Value | ||
| Surgery | Yes | 0.91 (0.64, 1.31) | 0.626 | 1.34 (0.77, 2.34) | 0.300 | 0.51 (0.23, 1.12) | 0.092 | 0.84 (0.60, 1.18) | 0.310 |
| No * | Reference | - | - | - | - | - | - | - | |
| Chemotherapy | Yes | 1.35 (1.06, 1.73) | 0.017 | 0.89 [0.70, 1.13) | 0.345 | - | - | 1.22 (0.97, 1.53) | 0.087 |
| No * | Reference | - | - | - | - | - | - | - | |
| Radiotherapy | Yes | 1.31 (1.09, 1.57) | 0.004 | - | - | - | - | 1.37 (1.15, 1.63) | <0.001 |
| No * | Reference | - | - | - | - | - | - | - | |
| Targeted | Yes | 1.07 (0.73, 1.56) | 0.731 | 0.78 [0.45, 1.38) | 0.398 | - | - | 0.92 (0.63, 1.36) | 0.684 |
| No * | Reference | - | - | - | - | - | - | - | |
| Cancer stage | I * | Reference | - | Reference | - | Reference | - | Reference | |
| II | 1.67 (1.19, 2.34) | 0.003 | 0.86 [0.68, 1.08) | 0.188 | 1.75 (0.89, 3.44) | 0.106 | 1.20 (0.92, 1.58) | 0.186 | |
| III | 2.03 (1.42, 2.91) | <0.001 | 0.72 [0.54, 0.96) | 0.026 | 1.32 (0.70, 2.48) | 0.399 | 1.26 (0.92, 1.71) | 0.129 | |
| IV | 3.09 (2.06, 4.62) | <0.001 | 0.60 [0.40, 0.89) | 0.012 | 1.75 (0.82, 3.74) | 0.150 | 1.89 (1.33, 2.70) | <0.001 | |
| Age at diagnosis | <45 | 1.32 (1.00, 1.74) | 0.053 | - | - | 0.74 (0.39, 1.43) | 0.377 | 1.30 (1.00, 1.69) | 0.054 |
| 45–55 * | Reference | - | - | - | - | Reference | - | Reference | |
| 56–60 | 1.06 (0.86, 1.30] | 0.605 | - | - | 0.62 (0.38, 1.00) | 0.052 | 1.04 (0.85, 1.26) | 0.715 | |
| >60 | 0.77 (0.60, 0.98] | 0.035 | - | - | 0.21 (0.09, 0.46) | <0.001 | 0.64 (0.51, 0.81) | <0.001 | |
| Self-employed | Yes | 0.41 (0.29, 0.58] | <0.001 | 0.44 [0.32, 0.60) | <0.001 | 1.28 (0.79, 2.08) | 0.317 | - | - |
| No * | Reference | - | Reference | Reference | - | - | - | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Wind, A.; Tamminga, S.J.; Bony, C.A.G.; Diether, M.; Ludwig, M.; Velthuis, M.J.; Duijts, S.F.A.; de Boer, A.G.E.M. Loss of Paid Employment up to 4 Years after Colorectal Cancer Diagnosis—A Nationwide Register-Based Study with a Population-Based Reference Group. Cancers 2021, 13, 2868. https://doi.org/10.3390/cancers13122868
de Wind A, Tamminga SJ, Bony CAG, Diether M, Ludwig M, Velthuis MJ, Duijts SFA, de Boer AGEM. Loss of Paid Employment up to 4 Years after Colorectal Cancer Diagnosis—A Nationwide Register-Based Study with a Population-Based Reference Group. Cancers. 2021; 13(12):2868. https://doi.org/10.3390/cancers13122868
Chicago/Turabian Stylede Wind, Astrid, Sietske J. Tamminga, Claudia A. G. Bony, Maren Diether, Martijn Ludwig, Miranda J. Velthuis, Saskia F. A. Duijts, and Angela G. E. M. de Boer. 2021. "Loss of Paid Employment up to 4 Years after Colorectal Cancer Diagnosis—A Nationwide Register-Based Study with a Population-Based Reference Group" Cancers 13, no. 12: 2868. https://doi.org/10.3390/cancers13122868