
Effects of Pre-Operative Risk Factors on Intensive Care Unit Length of Stay (ICU-LOS) in Major Oral and Maxillofacial Cancer Surgery

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
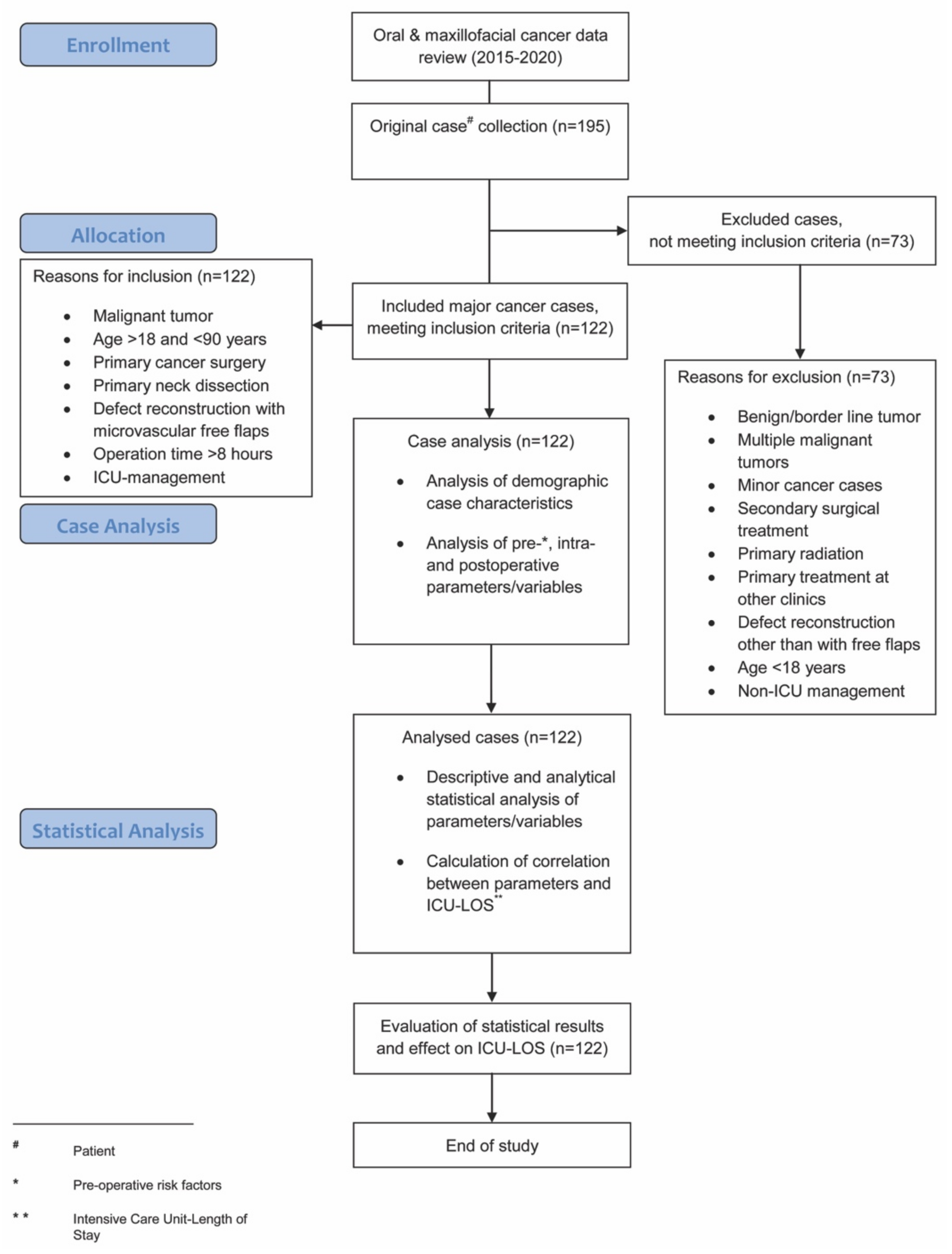
2.1. Patients
2.2. Surgical Procedure
- (1)
- In the absence of appropriate intermediate specialized or step-down units, or high nurse-to-patient ratio on the ward (recommended nurse-to-patient ratios of 1:2 or 1:1);
- (2)
- The co-morbidities, risk factors, and functional organ impairments that were present in many patients of the cohort; and,
- (3)
- The decision of the operating surgeon.
2.3. Post-Operative Management
2.4. Analyzed Parameters
2.5. Statistical Analysis
3. Results
4. Discussion
- (1)
- Although the literature provides studies with more cases, we tried to form a homogenous and representative cohort of patients over a 5-year period according to strict inclusion and exclusion criteria. Additionally, we used both single testing calculations and regression model analysis to provide valid correlation assessments between parameters and ICU-LOS.
- (2)
- A multi-center evaluation was not performed at this stage, because post-operative treatment protocols may vary widely between centers and, it would be difficult to ensure consistent patient management within one study population. This is probably also the reason why most existing studies in this field use single-center designs.
- (3)
- The ICU management of our study population was comparable to other reports in terms of sedation protocols, nurse-staffing ratios, or length of stay [9,19,33,34]. Age categories, the amount of blood loss, and urinary outputs during surgery were also similar to other cohorts in this field [19,20]. Furthermore, our treatment protocol followed the consensus and recommendations for optimal peri-operative care in major head and neck cancer surgery with free flap reconstruction [22]. Therefore, the results of this study should at least be partly valid for other institutions. Certainly, specific methods at our center may probably influence the study outcomes in some way, however, as this would probably also be true for other studies at other centers, we tried to decrease this limitation by evaluating patients over several years and creating a homogenous study cohort according to strictly defined criteria.
- (4)
- Since the primary outcome parameter of this study was ICU-LOS, we focused on patients that were postoperatively admitted to ICU. We did not separately include patients managed at step-down or intermediate care units. However, analysis of parameters affecting the length of stay in these units is planned for future research.
- (5)
- This study focused on defect reconstruction using microvascular free flaps. Other reconstruction types were not found to necessarily need to be transferred to the ICU for the immediate postoperative period. Since this work investigated the identification of prognostic parameters for a prolonged length of stay specifically in an ICU, those other reconstructions were excluded.
- (6)
- Since all patients included in this study were admitted to an ICU for the immediate postoperative period, no further differences were made in our retrospective analysis between “open” and “closed” ICU admissions. This study included all patients that were submitted to an ICU, independently of whether the units were run under an “open” or “closed (low intensity)” strategy. The results of this study are therefore valid for both “open” and “closed” ICUs. Independently from that, most of the postoperative treatment that was carried out could probably also have been carried out in non-ICU wards. Therefore, the results of this study may also be extrapolated for non-ICUs, such as specialized intermediate care, step-down units, or high-intensity nursing wards.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bianchi, B.; Ferri, A.; Ferrari, S.; Copelli, C.; Boni, P.; Baj, A.; Sesenna, E. Reconstruction of lateral through and through oromandibular defects following oncological resections. Microsurgery 2010, 30, 517–525. [Google Scholar] [CrossRef]
- Bianchi, B.; Ferri, A.; Ferrari, S.; Copelli, C.; Boni, P.; Sesenna, E. Reconstruction of anterior through and through oromandibular defects following oncological resections. Microsurgery 2010, 30, 97–104. [Google Scholar] [CrossRef]
- Pau, M.; Wallner, J.; Feichtinger, M.; Schwaiger, M.; Egger, J.; Cambiaso-Daniel, J.; Winter, R.; Jakse, N.; Zemann, W. Free thoracodorsal, perforator-scapular flap based on the angular artery (TDAP-Scap-aa): Clinical experiences and description of a novel technique for single flap reconstruction of extensive oromandibular defects. J. Craniomaxillofac. Surg. 2019, 47, 1617–1625. [Google Scholar] [CrossRef]
- Yokoo, S.; Komori, T.; Furudoi, S.; Umeda, M.; Nomura, T.; Hashikawa, K.; Ichinose, A.; Tahara, S. Three-dimensional reconstruction after oral oncologic surgery using single free radial forearm flaps or free rectus abdominis musculocutaneous flaps. J. Oral Sci. 2004, 46, 65–70. [Google Scholar] [CrossRef] [Green Version]
- Gusenoff, J.A.; Vega, S.J.; Jiang, S.; Behnam, A.B.; Sbitany, H.; Herrera, H.R.; Smith, A.; Serletti, J.M. Free tissue transfer: Comparison of outcomes between university hospitals and community hospitals. Plast. Reconstr. Surg. 2006, 118, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Novakovic, D.; Patel, R.S.; Goldstein, D.P.; Gullane, P.J. Salvage of failed free flaps used in head and neck reconstruction. Head Neck Oncol. 2009, 1, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bianchi, B.; Ferrari, S.; Poli, T.; Bertolini, F.; Raho, T.; Sesenna, E. Oromandibular reconstruction with simultaneous free flaps: Experience on 10 cases. Acta. Otorhinolaryngol. Ital. 2003, 23, 281–290. [Google Scholar]
- Wei, F.C.; Demirkan, F.; Chen, H.C.; Chen, I.H. Double free flaps in reconstruction of extensive composite mandibular defects in head and neck carcinoma. Plast. Reconstr. Surg. 1999, 103, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Lebherz-Eichinger, D.; Tudor, B.; Krenn, C.G.; Roth, G.A.; Seemann, R. Impact of different sedation protocols and perioperative procedures on patients admitted to the intensive care unit after maxillofacial tumor surgery of the lower jaw: A retrospective study. J. Craniomaxillofac. Surg. 2016, 44, 506–511. [Google Scholar] [CrossRef]
- Varadarajan, V.V.; Arshad, H.; Dziegielewski, P.T. Head and neck free flap reconstruction: What is the appropriate post-operative level of care? Oral Oncol. 2017, 75, 61–66. [Google Scholar] [CrossRef]
- Cervenka, B.; Olinde, L.; Gould, E.; Farwell, D.G.; Moore, M.; Kaufman, M.; Bewley, A.F. Use of a non-ICU specialty ward for immediate post-operative management of head and neck free flaps; a randomized controlled trial. Oral Oncol. 2019, 99, 104464. [Google Scholar] [CrossRef] [PubMed]
- Godden, D.R.; Patel, M.; Baldwin, A.; Woodwards, R.T. Need for intensive care after operations for head and neck cancer surgery. Br. J. Oral Maxillofac. Surg. 1999, 37, 502–505. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, J.H.; Polat, J.K. Microvascular flap reconstruction by otolaryngologists: Prevalence, postoperative care, and monitoring techniques. Laryngoscope 2007, 117, 485–490. [Google Scholar] [CrossRef]
- Allak, A.; Nguyen, T.N.; Shonka, D.C., Jr.; Reibel, J.F.; Levine, P.A.; Jameson, M.J. Immediate postoperative extubation in patients undergoing free tissue transfer. Laryngoscope 2011, 121, 763–768. [Google Scholar] [CrossRef] [PubMed]
- Arshad, H.; Ozer, H.G.; Thatcher, A.; Old, M.; Ozer, E.; Agarwal, A.; Jafari, H.; Birkheimer, D.; Basinger, H.; Forest, L.A.; et al. Intensive care unit versus non-intensive care unit postoperative management of head and neck free flaps: Comparative effectiveness and cost comparisons. Head Neck 2014, 36, 536–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panwar, A.; Smith, R.; Lydiatt, D.; Lindau, R.; Wieland, A.; Richards, A.; Shostrom, V.; Militsakh, O.; Lydiatt, W. Vascularized tissue transfer in head and neck surgery: Is intensive care unit-based management necessary? Laryngoscope 2016, 126, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.; Cordeiro, P.G.; Santamaria, E.; Shaha, A.R.; Pfister, D.G.; Shah, J.P. Factors associated with complications in microvascular reconstruction of head and neck defects. Plast. Reconstr. Surg. 1999, 103, 403–411. [Google Scholar] [CrossRef]
- Suh, J.D.; Sercarz, J.A.; Abemayor, E.; Calcaterra, T.C.; Rawnsley, J.D.; Alam, D.; Blackwell, K.E. Analysis of outcome and complications in 400 cases of microvascular head and neck reconstruction. Arch. Otolaryngol. Head Neck Surg. 2004, 130, 962–966. [Google Scholar] [CrossRef] [Green Version]
- Bhama, P.K.; Davis, G.E.; Bhrany, A.D.; Lam, D.J.; Futran, N.D. The effects of intensive care unit staffing on patient outcomes following microvascular free flap reconstruction of the head and neck: A pilot study. JAMA Otolaryngol. Head Neck Surg. 2013, 139, 37–42. [Google Scholar] [CrossRef] [Green Version]
- Booka, E.; Kamijo, T.; Matsumoto, T.; Takeuchi, M.; Kitani, T.; Nagaoka, M.; Imai, A.; Iida, Y.; Shimada, A.; Takebayashi, K.; et al. Incidence and risk factors for postoperative delirium after major head and neck cancer surgery. J. Craniomaxillofac. Surg. 2016, 44, 890–894. [Google Scholar] [CrossRef]
- Choi, N.Y.; Kim, E.H.; Baek, C.H.; Sohn, I.; Yeon, S.; Chung, M.K. Development of a nomogram for predicting the probability of postoperative delirium in patients undergoing free flap reconstruction for head and neck cancer. Eur. J. Surg. Oncol. 2017, 43, 683–688. [Google Scholar] [CrossRef] [PubMed]
- Dort, J.C.; Farwell, D.G.; Findlay, M.; Huber, G.F.; Kerr, P.; Shea-Budgell, M.A.; Simon, C.; Uppington, J.; Zygun, D.; Ljungqvist, O.; et al. Optimal Perioperative Care in Major Head and Neck Cancer Surgery with Free Flap Reconstruction: A Consensus Review and Recommendations From the Enhanced Recovery After Surgery Society. JAMA Otolaryngol. Head Neck Surg. 2017, 143, 292–303. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.; Wang, G.; Liu, S.; Zhou, S.; Lian, Y.; Zhang, C.; Yang, W. Risk factors for postoperative delirium in patients undergoing major head and neck cancer surgery: A meta-analysis. Jpn. J. Clin. Oncol. 2017, 47, 505–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, R.S.; McCluskey, S.A.; Goldstein, D.P.; Minkovich, L.; Irish, J.C.; Brown, D.H.; Gullane, P.J.; Lipa, J.E.; Gilbert, R.W. Clinicopathologic and therapeutic risk factors for perioperative complications and prolonged hospital stay in free flap reconstruction of the head and neck. Head Neck 2010, 32, 1345–1353. [Google Scholar] [CrossRef]
- De Melo, G.M.; Ribeiro, K.D.B.; Kowalski, L.P.; Deheinzelin, D. Risk factors for postoperative complications in oral cancer and their prognostic implications. Arch. Otolaryngol. Neck Surg. 2001, 127, 828–833. [Google Scholar]
- Sivagnanam, T.; Langton, S.G. Need for intensive care after operations for head and neck cancer surgery. Br. J. Oral Maxillofac. Surg. 2001, 39, 77. [Google Scholar] [CrossRef]
- Pfister, D.G.; Spencer, S.; Adelstein, A.; Adkins, D.; Anzai, Y.; Brizel, D.M.; Bruce, J.Y.; Busse, P.M.; Caudell, J.J.; Cmelak, A.J.; et al. Head and Neck Cancers, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2020, 18, 873–898. [Google Scholar] [CrossRef]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [Green Version]
- Rempel, V.; Grandoch, A.; Safi, A.F.; Buller, J.; Riekert, M.; Schick, V.; Nickenig, H.J.; Zöller, J.; Kreppel, M. The prognostic implications of comorbidity and risk factors for (post)operative complications, days spent in the intensive care unit (ICU), and length of hospitalization in patients with oral squamous cell carcinoma: A prospective study. J. Craniomaxillofac. Surg. 2020, 48, 868–874. [Google Scholar] [CrossRef]
- Gamil, M.; Fanning, A. The first 24 hours after surgery: A study of complications after 2153 consecutive operations. Anaesthesia 1991, 46, 712–715. [Google Scholar] [CrossRef]
- Lone, N.I.; Gillies, M.A.; Haddow, C.; Dobbie, R.; Rowan, K.M.; Wild, S.H.; Murray, G.D.; Walsh, T.S. Five-Year Mortality and Hospital Costs Associated with Surviving Intensive Care. Am. J. Respir. Crit. Care Med. 2016, 194, 198–208. [Google Scholar] [CrossRef]
- Sundermann, B.V.; Uhlmann, L.; Hoffmann, J.; Freier, K.; Thiele, O.C. The localization and risk factors of squamous cell carcinoma in the oral cavity: A retrospective study of 1501 cases. J. Craniomaxillofac. Surg. 2018, 46, 177–182. [Google Scholar] [CrossRef] [PubMed]
- To, E.W.H.; Tsang, W.M.; Lai, E.C.H.; Chu, M.C. Retrospective study on the need of intensive care unit admission after major head and neck surgery. ANZ J. Surg. 2002, 72, 11–14. [Google Scholar] [CrossRef]
- Haddock, N.T.; Gobble, R.M.; Levine, J.P. More consistent postoperative care and monitoring can reduce costs following microvascular free flap reconstruction. J. Reconstr. Microsurg. 2010, 26, 435–439. [Google Scholar] [CrossRef]
- Cornejo, A.; Ivatury, S.; Crane, C.N.; Myers, J.G.; Wang, H.T. Analysis of free flap complications and utilization of intensive care unit monitoring. J. Reconstr. Microsurg. 2013, 29, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Dassonville, O.; Bozec, A.; Chateau, Y.; Reyt, E.; Devauchelle, B.; Louis, M.Y.; Breton, P.; Julieron, M.; Yachouh, J.; Mallet, Y.; et al. Multicenter prospective micro-costing study evaluating mandibular free-flap reconstruction. Eur. Arch. Oto Rhino Laryngol. 2017, 274, 1103–1111. [Google Scholar] [CrossRef]
- Kesting, M.R.; Hölzle, F.; Wolff, K.D.; Wagenpfeil, S.; Hasler, R.J.; Wales, C.J.; Steinstraesser, L.; Rohleder, N.H. Use of microvascular flap technique in older adults with head and neck cancer: A persisting dilemma in reconstructive surgery? J. Am. Geriatr. Soc. 2011, 59, 398–405. [Google Scholar] [CrossRef]
- Densky, J.; Eskander, A.; Kang, S.; Chan, J.; Tweel, B.; Sitapara, J.; Ozer, E.; Agrawal, A.; Carrau, R.; Rocco, J.; et al. Risk Factors Associated with Postoperative Delirium in Patients Undergoing Head and Neck Free Flap Reconstruction. JAMA Otolaryngol. Head Neck Surg. 2019, 145, 216–221. [Google Scholar] [CrossRef]
- Nkenke, E.; Vairaktaris, E.; Stelzle, F.; Neukam, F.W.; St Pierre, M. No reduction in complication rate by stay in the intensive care unit for patients undergoing surgery for head and neck cancer and microvascular reconstruction. Head Neck 2009, 31, 1461–1469. [Google Scholar] [CrossRef] [PubMed]
- Le Gall, J.R.; Lemeshow, S.; Saulnier, F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef] [PubMed]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chron. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Metra, M.; Cotter, G.; Gheorghiade, M.; Dei Cas, L.; Voors, A.A. The role of the kidney in heart failure. Eur. Heart J. 2012, 33, 2135–2142. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | n (%) | Mean Age (±SD) |
| Male | 76 (62.3) | 61.9 (±9.6) |
| Female | 46 (37.7) | 60.9 (±10.6) |
| Overall | 122 (100) | 61.5 (±10.0) |
| Primary Tumor Site | n (%) | |
| Floor of Mouth | 35 (28.7) | |
| Mandible | 22 (18.0) | |
| Maxilla | 11 (9.0) | |
| Oropharynx | 23 (18.9) | |
| Other | 11 (9.0) | |
| Tongue | 19 (15.6) | |
| Tonsil | 1 (0.8) | |
| Primary Site of Neck Dissection | n (%) | |
| BLND | 67 (54.9) | |
| ULND | 55 (45.1) | |
| Intra-Operative Parameters | Min | Max | Mean | SD (±) |
|---|---|---|---|---|
| Blood Loss (estimated) (mL) | 260 | 670 | 445.3 | ±96.4 |
| Hemoglobin Level (g/dL) | 7.8 | 13.1 | 10.1 | ±1.4 |
| Urinary Output (mL) | 430 | 1730 | 989.5 | ±307.6 |
| Maximum Temperature (°C) | 37 | 39 | 38.1 | ±0.5 |
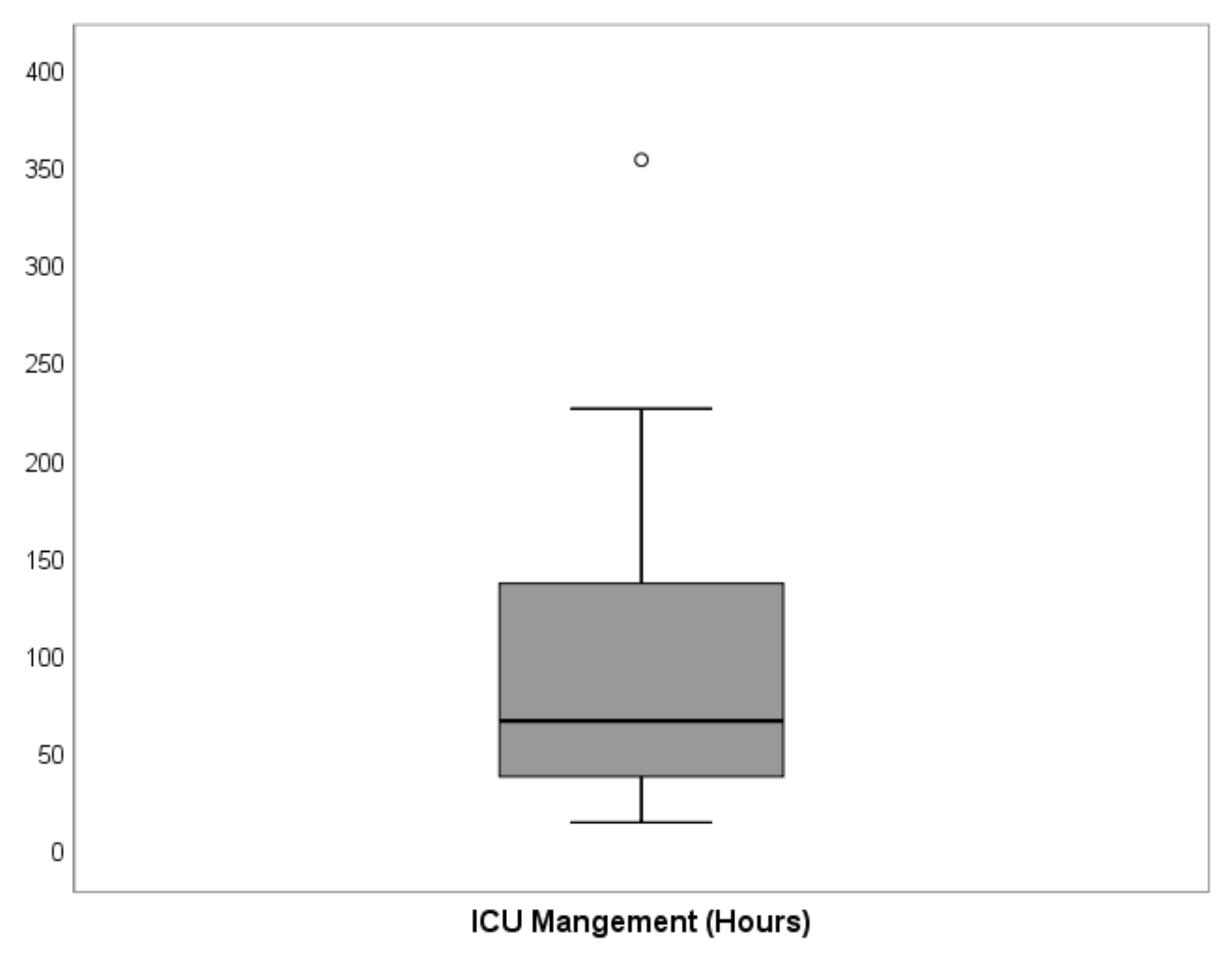
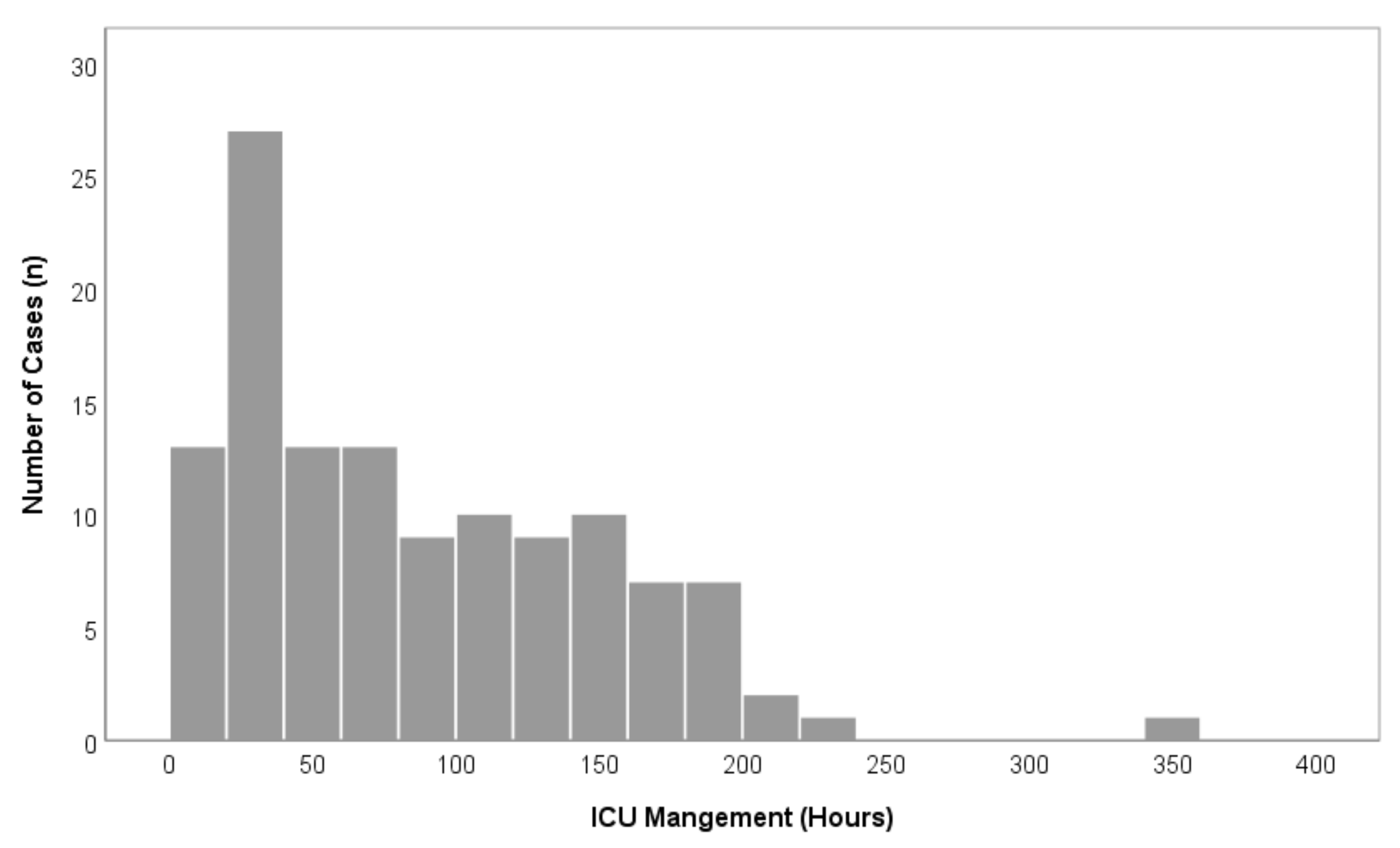
| Primary Outcome Parameter | Min | Max | Median | Mean | SD (±) |
|---|---|---|---|---|---|
| ICU-LOS (h) | 13.5 | 353.0 | 65.5 | 87.0 | ±63.3 |
| Parameter | Min | Max | Mean (±SD) | p-Value | |
| Age (years) | 42 | 82 | 61.5 (±10.0) | p = 0.879 | |
| BMI (kg/m2) | 17.5 | 40.1 | 27.0 (±5.2) | p = 0.038 | |
| Time of Surgery (h) | 8 | 16 | 11.4 (±2.2) | p = 0.312 | |
| Parameter | n | % | Mean ICU-LOS (±SD) | p-Value | |
| Sex | male | 76 | 62.3 | 85.5 (±61.5) | p = 0.609 |
| female | 46 | 37.7 | 89.5 (±66.8) | ||
| ASA Performance Status | I | 27 | 22.1 | 42.8 (±32.2) | p = 0.243 |
| (Grade I-VI) | II | 39 | 32.0 | 80.6 (±57.2) | |
| III | 55 | 45.1 | 113.8 (±66.5) | ||
| IV | 1 | 0.8 | 62.5 | ||
| Arterial Hypertension | + | 57 | 46.7 | 117.8 (±64.1) | p = 0.513 |
| (positive +, negative −) | − | 65 | 53.3 | 60.1 (±49.0) | |
| Diabetes Mellitus | + | 20 | 16.4 | 78.3 (±62.1) | p = 0.248 |
| (positive +, negative −) | − | 102 | 83.6 | 88.8 (±63.7) | |
| Adiposity (BMI >30 kg/m2) | + | 37 | 30.3 | 79.2 (±60.4) | p = 0.207 |
| (positive +, negative −) | − | 85 | 69.7 | 90.4 (±64.6) | |
| CAD | + | 32 | 26.2 | 69.8 (±53.7) | p = 0.930 |
| (positive +, negative −) | − | 90 | 73.8 | 93.2 (±65.6) | |
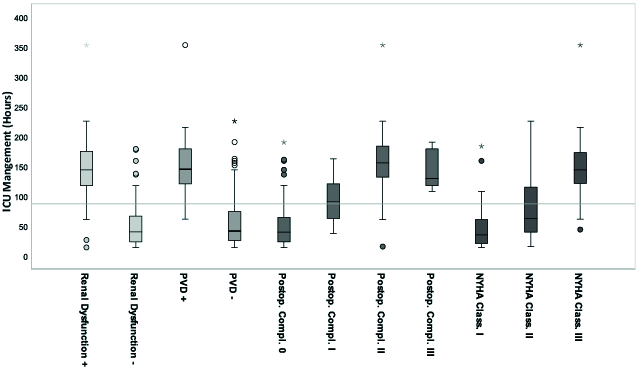
| Renal Dysfunction | + | 45 | 36.9 | 144.3 (±55.6) | p < 0.001 |
| (GFR <60 mL/min) | − | 77 | 63.1 | 53.6 (±38.9) | |
| Chronic Alcoholism | + | 91 | 74.6 | 89.4 (±63.8) | p = 0.932 |
| (estimated daily ethanol intake of >200 mL) | − | 31 | 25.4 | 80.2 (±62.3) | |
| Chronic Smoking | + | 104 | 85.2 | 84.8 (±63.8) | p = 0.725 |
| (>10 cigarettes daily for at least 3 years) | − | 18 | 14.8 | 100.1 (±60.3) | |
| COPD | + | 35 | 28.7 | 115.9 (±57.9) | p = 0.239 |
| − | 87 | 71.3 | 75.4 (±61.9) | ||
| Extent of Heart Failure | I | 48 | 39.3 | 45.5 (±35.9) | p = 0.009 |
| (NYHA Classification | II | 39 | 32.0 | 82.9 (±55.0) | |
| Grade I–IV) | III | 35 | 28.7 | 148.6 (±52.4) | |
| PVD | + | 37 | 30.3 | 151.5 (±50.6) | p = 0.010 |
| (positive +, negative −) | − | 85 | 69.7 | 59.0 (±45.3) | |
| Tumor Size | T1 | 9 | 7.4 | 58.3 (±110.7) | p = 0.214 |
| (T-Classification, T1–T4) | T2 | 42 | 34.4 | 53.9 (±42.5) | |
| (UICC 2017) | T3 | 29 | 23.8 | 103.7 (±50.4) | |
| T4 | 42 | 34.4 | 114.9 (±59.9) | ||
| Blood Transfusion | 0 | 67 | 54.9 | 51.7 (±39.9) | p = 0.603 |
| (Number of intra-operative Erythrocyte | 1 | 29 | 23.8 | 109.2 (±71.6) | |
| Concentrate–EC | 2 | 24 | 19.7 | 155.0 (±30.9) | |
| 1 EC = 345.3 mL suspension) | 3 | 2 | 1.6 | 134.3 (±37.2) | |
| Post-operative Complication | 0 | 73 | 59.8 | 52.8 (±39.4) | p = 0.023 |
| (Clavien-Dindo Classification | I | 13 | 10.7 | 93.2 (±40.0) | |
| Grade I–IV, 0 = normal) | II | 27 | 22.1 | 158.1 (±60.5) | |
| III | 9 | 7.4 | 142.9 (±32.4) | ||
| IV | 0 | 0 | 0 | ||
| Parameter | p-Value | Testing | Correlation Coefficient | Effect Size | 95% CI ćof Diff |
|---|---|---|---|---|---|
| Age (years) | p < 0.001 | Pearson | r = 0.587 | ||
| BMI (kg/m2) | p = 0.913 | Pearson | r = 0.010 | ||
| Time of Surgery (hours) | p = 0.001 | Pearson | r = 0.286 | ||
| Type of Neck Dissectionć (ULND, BLND) | p < 0.001 | t-test | Cohens’d = 1.01 | [36.7–77.6] | |
| Sex | p = 0.735 | t-test | Cohens’d = 0.06 | [−27.5–19.5] | |
| (men, women) | |||||
| ASA Performance Status | p < 0.001 | ANOVA | η2 = 0.19 | ||
| (Grade I-VI) | |||||
| Arterial Hypertension | p < 0.001 | t-test | Cohens’d = 1.01 | [37.4–78.0] | |
| Diabetes Mellitus | p = 0.501 | t-test | Cohens’d = 0.17 | [41.2–20.3] | |
| Adiposity (BMI > 30 kg/m2) | p = 0.370 | t-test | Cohens’d = 0.18 | [−35.9–13.5] | |
| CAD | p = 0.072 | t-test | Cohens’d = 0.39 | [−49.0–2.2] | |
| Renal Dysfunction | p < 0.001 | t-test | Cohens’d = 1.89 | [73.7–107.7] | |
| (GFR < 60 mL/min) | |||||
| Chronic Alcoholism | p = 0.488 | t-test | Cohens’d = 0.15 | [−16.9–35.3] | |
| (estimated daily ethanol intake of >200 mL) | |||||
| Chronic Smoking | p = 0.345 | t-test | Cohens’d = 0.25 | [−16.9–35.3] | |
| (>10 cigarettes daily for at least 30 years) | |||||
| COPD | p = 0.001 | t-test | Cohens’d = 0.68 | [−16.4–64.6] | |
| Extent of Heart Failure | p < 0.001 | ANOVA | η2 = 0.44 | ||
| NYHA Classification | |||||
| (Grade I-IV) | |||||
| PVD | p < 0.001 | t-test | Cohens’d = 3.03 | [74.2–110.8] | |
| Tumor Size (Classification, T1-T4) | p < 0.001 | Spearman | r = 0.487 | ||
| (UICC 2017) | |||||
| Blood Transfusion | p < 0.001 | Spearman | r = 0.672 | ||
| (Number of intra-operative Erythrocyte) | |||||
| Concentrate–EC | |||||
| (1 EC = 345.3 mL suspension) | |||||
| Post-operative Complicationć (Clavien Dindo Classificationć Grade I-IV, 0 = normal) | p < 0.001 | Spearman | r = 0.681 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wallner, J.; Schwaiger, M.; Edmondson, S.-J.; Mischak, I.; Egger, J.; Feichtinger, M.; Zemann, W.; Pau, M. Effects of Pre-Operative Risk Factors on Intensive Care Unit Length of Stay (ICU-LOS) in Major Oral and Maxillofacial Cancer Surgery. Cancers 2021, 13, 3937. https://doi.org/10.3390/cancers13163937
Wallner J, Schwaiger M, Edmondson S-J, Mischak I, Egger J, Feichtinger M, Zemann W, Pau M. Effects of Pre-Operative Risk Factors on Intensive Care Unit Length of Stay (ICU-LOS) in Major Oral and Maxillofacial Cancer Surgery. Cancers. 2021; 13(16):3937. https://doi.org/10.3390/cancers13163937
Chicago/Turabian StyleWallner, Juergen, Michael Schwaiger, Sarah-Jayne Edmondson, Irene Mischak, Jan Egger, Matthias Feichtinger, Wolfgang Zemann, and Mauro Pau. 2021. "Effects of Pre-Operative Risk Factors on Intensive Care Unit Length of Stay (ICU-LOS) in Major Oral and Maxillofacial Cancer Surgery" Cancers 13, no. 16: 3937. https://doi.org/10.3390/cancers13163937
APA StyleWallner, J., Schwaiger, M., Edmondson, S.-J., Mischak, I., Egger, J., Feichtinger, M., Zemann, W., & Pau, M. (2021). Effects of Pre-Operative Risk Factors on Intensive Care Unit Length of Stay (ICU-LOS) in Major Oral and Maxillofacial Cancer Surgery. Cancers, 13(16), 3937. https://doi.org/10.3390/cancers13163937