
Circulating Cell-Free DNA as Biomarker of Taxane Resistance in Metastatic Castration-Resistant Prostate Cancer

 ,
,  ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Design
2.3. Study Procedures
2.4. Statistical Analysis
3. Results
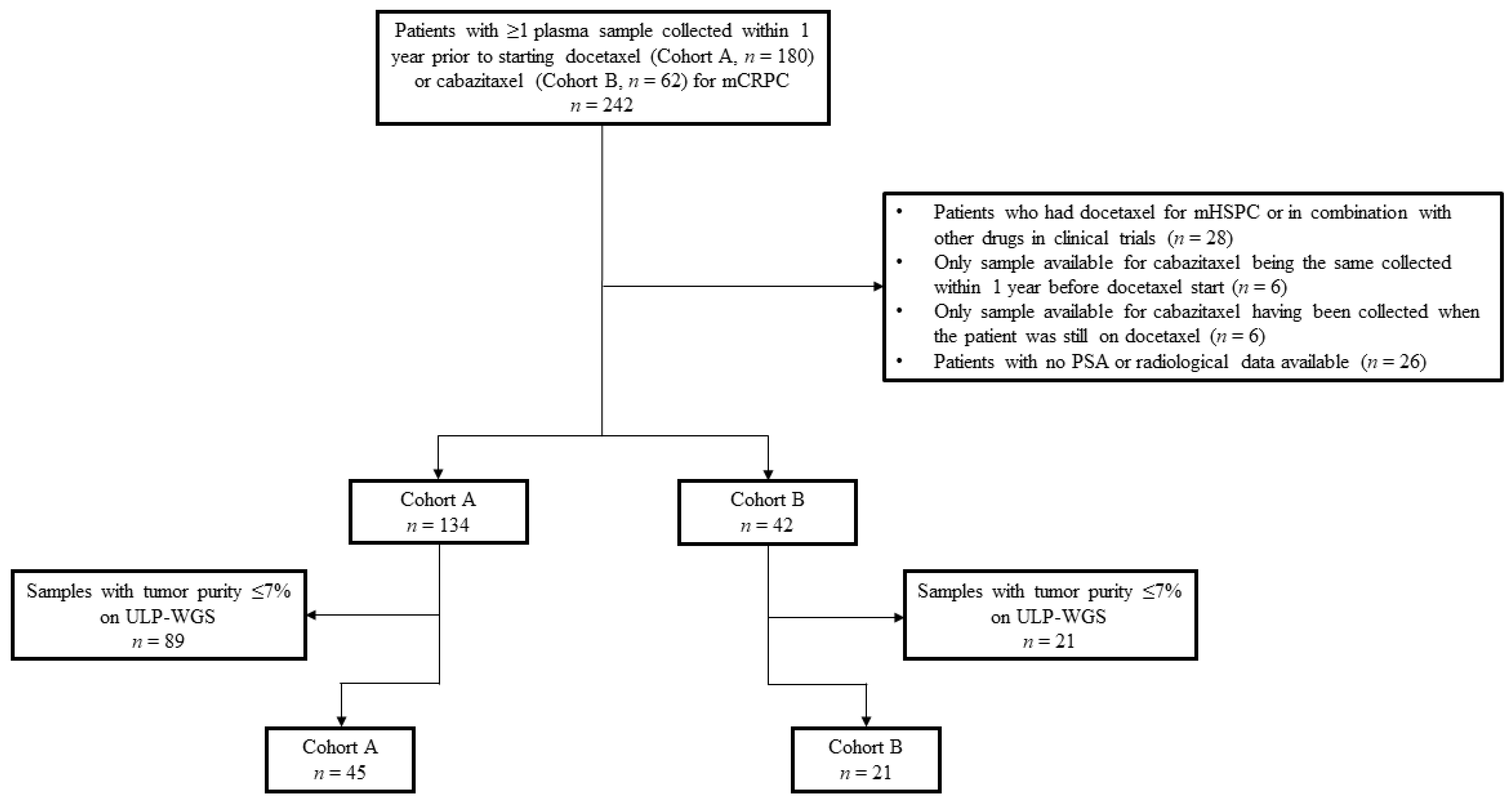
3.1. Cohorts
3.2. Patient Characteristics
3.3. Laboratory and Clinical Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Scher, H.I.; Solo, K.; Valant, J.; Todd, M.B.; Mehra, M. Prevalence of Prostate Cancer Clinical States and Mortality in the United States: Estimates Using a Dynamic Progression Model. PLoS ONE 2015, 10, e0139440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrylak, D.P.; Tangen, C.M.; Hussain, M.H.A.; Lara, P.N., Jr.; Jones, J.A.; Taplin, M.E.; Burch, P.A.; Berry, D.; Moinpour, C.; Kohli, M.; et al. Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate cancer. N. Engl. J. Med. 2004, 351, 1513–1520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berthold, D.R.; Pond, G.R.; Soban, F.; de Wit, R.; Eisenberger, M.; Tannock, I.F. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer: Updated survival in the TAX 327 study. J. Clin. Oncol. 2008, 26, 242–245. [Google Scholar] [CrossRef]
- De Bono, J.S.; Oudard, S.; Ozguroglu, M.; Hansen, S.; Machiels, J.P.; Kocak, I.; Gravis, G.; Bodrogi, I.; Mackenzie, M.J.; Shen, L.; et al. Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: A randomised open-label trial. Lancet 2010, 376, 1147–1154. [Google Scholar] [CrossRef]
- Oudard, S.; Fizazi, K.; Sengeløv, L.; Daugaard, G.; Saad, F.; Hansen, S.; Hjälm-Eriksson, M.; Jassem, J.; Thiery-Vuillemin, A.; Caffo, O.; et al. Cabazitaxel Versus Docetaxel As First-Line Therapy for Patients With Metastatic Castration-Resistant Prostate Cancer: A Randomized Phase III Trial-FIRSTANA. J. Clin. Oncol. 2017, 35, 3189–3197. [Google Scholar] [CrossRef]
- Galletti, E.; Magnani, M.; Renzulli, M.L.; Botta, M. Paclitaxel and docetaxel resistance: Molecular mechanisms and development of new generation taxanes. Chem. Med. Chem. 2007, 2, 920–942. [Google Scholar] [CrossRef] [PubMed]
- Kosaka, T.; Miyajima, A.; Shirotake, S.; Suzuki, E.; Kikuchi, E.; Oya, M. Long-term androgen ablation and docetaxel up-regulate phosphorylated Akt in castration resistant prostate cancer. J. Urol. 2011, 185, 2376–2381. [Google Scholar] [CrossRef] [PubMed]
- Conteduca, V.; Mosca, A.; Brighi, N.; de Giorgi, U.; Rescigno, P. New Prognostic Biomarkers in Metastatic Castration-Resistant Prostate Cancer. Cells 2021, 10, 193. [Google Scholar] [CrossRef]
- Graf, R.P.; Hullings, M.; Barnett, E.S.; Carbone, E.; Dittamore, R.; Scher, H.I. Clinical Utility of the Nuclear-localized AR-V7 Biomarker in Circulating Tumor Cells in Improving Physician Treatment Choice in Castration-resistant Prostate Cancer. Eur. Urol. 2020, 77, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Reed, K.; Hembruff, S.L.; Laberge, M.L.; Villeneuve, D.J.; Côté, G.B.; Parissenti, A.M. Hypermethylation of the ABCB1 downstream gene promoter accompanies ABCB1 gene amplification and increased expression in docetaxel-resistant MCF-7 breast tumor cells. Epigenetics 2008, 3, 270–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.C.; Juric, D.; Francisco, B.; Yu, R.X.; Duran, G.E.; Chen, K.G.; Chen, X.; Sikic, B.I. Regional Activation of Chromosomal Arm 7q with and without Gene Amplification in Taxane-selected Human Ovarian Cancer Cell Lines. Genes Chromosomes Cancer 2006, 45, 365–374. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Liu, C.; Nadiminty, N.; Lou, W.; Tummala, R.; Evans, C.P.; Gao, A.C. Inhibition of ABCB1 expression overcomes acquired docetaxel resistance in prostate cancer. Mol. Cancer Ther. 2013, 12, 1829–1836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomlins, S.A.; Rhodes, D.R.; Perner, S.; Dhanasekaran, S.M.; Mehra, R.; Sun, X.W.; Varambally, S.; Cao, X.; Tchinda, J.; Kuefer, R.; et al. Recurrent fusion of TMPRSS2 and ETS transcription factor genes in prostate cancer. Science 2005, 310, 644–648. [Google Scholar] [CrossRef]
- Galletti, G.; Matov, A.; Beltran, H.; Fontugne, J.; Mosquera, J.M.; Cheung, C.; MacDonald, T.Y.; Sung, M.; O′Toole, S.; Kench, J.G.; et al. ERG induces taxanes resistance in castration resistant prostate cancer. Nat. Commun. 2014, 5, 5548. [Google Scholar] [CrossRef] [Green Version]
- Komura, K.; Jeong, S.H.; Hinohara, K.; Qu, F.; Wang, X.; Hiraki, M.; Azuma, H.; Mary Lee, G.S.; Kantoff, P.W.; Sweeney, C.J. Resistance to docetaxel in prostate cancer is associated with androgen receptor activation and loss of KDM5D expression. Proc. Natl. Acad. Sci. USA 2016, 113, 6259–6264. [Google Scholar] [CrossRef] [Green Version]
- Grasso, C.S.; Wu, Y.M.; Robinson, F.R.; Cao, X.; Dhanasekaran, S.M.; Khan, A.P.; Quist, M.J.; Jing, X.; Lonigro, R.J.; Brenner, J.C.; et al. The Mutational Landscape of Lethal Castrate Resistant Prostate Cancer. Nature 2012, 487, 239–243. [Google Scholar] [CrossRef] [Green Version]
- Robinson, D.; Van Allen, E.M.; Wu, Y.M.; Wu, Y.M.; Schultz, N.; Lonigro, R.J.; Mosquera, J.M.; Montgomery, B.; Taplin, M.E.; Pritchard, C.C.; et al. Integrative Clinical Genomics of Advanced Prostate Cancer. Cell 2015, 162, 454. [Google Scholar] [CrossRef] [Green Version]
- Sher, H.I.; Morris, M.J.; Stadler, W.M.; Higano, C.; Basch, E.; Fizazi, K.; Antonarakis, E.S.; Beer, T.M.; Carducci, M.A.; Chi, K.N.; et al. Trial Design and Objectives for Castration-Resistant Prostate Cancer: Updated Recommendations From the Prostate Cancer Clinical Trials Working Group 3. J. Clin. Oncol. 2016, 34, 1402–1418. [Google Scholar] [CrossRef] [Green Version]
- Haber, D.A.; Velculescu, V.E. Blood-based analyses of cancer: Circulating tumor cells and circulating tumor DNA. Cancer Discov. 2014, 4, 650–661. [Google Scholar] [CrossRef] [Green Version]
- Goodall, J.; Mateo, J.; Yuan, W.; Mossop, H.; Porta, N.; Miranda, S.; Perez-Lopez, R.; Dolling, D.; Robinson, D.R.; Sandhu, S.; et al. Circulating Cell-Free DNA to Guide Prostate Cancer Treatment with PARP Inhibition. Cancer Discov. 2017, 7, 1006–1017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choudhury, A.D.; Werner, L.; Francini, E.; Wei, X.X.; Ha, G.; Freeman, S.S.; Justin Rhoades, J.; Reed, S.C.; Gydush, G.; Rotem, D. Tumor fraction in cell-free DNA as a biomarker in prostate cancer. JCI Insight. 2018, 3, e122109. [Google Scholar] [CrossRef] [PubMed]
- Adalsteinsson, V.A.; Ha, G.; Freeman, S.S.; Choudhury, A.D.; Stover, D.G.; Parsons, H.A.; Gydush, G.; Reed, S.C.; Rotem, D.; Rhoades, J.; et al. Scalable whole-exome sequencing of cell-free DNA reveals high concordance with metastatic tumors. Nat. Commun. 2017, 8, 1324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stover, D.G.; Parsons, H.A.; Ha, G.; Freeman, S.S.; Barry, W.T.; Guo, H.; Choudhury, A.D.; Gydush, G.; Reed, S.C.; Rhoades, J.; et al. Association of Cell-Free DNA Tumor Fraction and Somatic Copy Number Alterations With Survival in Metastatic Triple-Negative Breast Cancer. J. Clin. Oncol. 2018, 36, 543–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, W.K.; Hayes, J.; Evan, C.; Manola, J.; George, D.J.; Waldron, H.; Donovan, M.; Varner, J.; Orechia, J.; Katcher, B.; et al. Development of an Integrated Prostate Cancer Research Information System. Clin. Genitourin. Cancer. 2006, 5, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- McLendon, R.; Friedman, A.; Bigner, D.; Van Meir, E.G.; Brat, D.J.; Mastrogianakis, G.M.; Olson, J.J.; Mikkelsen, T.; Lehman, N.; Aldape, K.; et al. Comprehensive genomic characterization defines human glioblastoma genes and core pathways. Nature 2008, 455, 1061–1068. [Google Scholar]
- Mermel, C.H.; Schumacher, S.E.; Hill, B.; Meyerson, M.L.; Beroukhim, R.; Getz, G. GISTIC2.0 facilitates sensitive and confident localization of the targets of focal somatic copy-number alteration in human cancers. Genome Biol. 2011, 12, R41. [Google Scholar] [CrossRef] [Green Version]
- Weir, B.A.; Woo, M.S.; Getz, G.; Perner, S.; Ding, L.; Beroukhim, R.; Lin, W.M.; Province, M.A.; Kraja, A.; Johnson, L.A.; et al. Characterizing the cancer genome in lung adenocarcinoma. Nature 2007, 450, 893–898. [Google Scholar] [CrossRef]
- Chiang, D.Y.; Villanueva, A.; Hoshida, Y.; Peix, J.; Newell, P.; Minguez, B.; LeBlanc, A.C.; Donovan, D.J.; Thung, S.N.; Solé, M.; et al. Focal gains of VEGFA and molecular classification of hepatocellular carcinoma. Cancer Res. 2008, 68, 6779–6788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beroukhim, R.; Mermel, C.; Porter, D.; Wei, G.; Raychaudhuri, S.; Donovan, J.; Barretina, J.; Boehm, J.S.; Dobson, J.; Urashima, M.; et al. The landscape of somatic copy-number alteration across human cancers. Nature 2010, 463, 899–905. [Google Scholar] [CrossRef]
- Firth, D. Bias reduction of maximum likelihood estimates. Biometrika 1993, 80, 27–38. [Google Scholar] [CrossRef]
- Heinze, G.; Schemper, M. A solution to the problem of separation in logistic regression. Stat. Med. 2002, 21, 2409–2419. [Google Scholar] [CrossRef] [PubMed]
- Landau, D.A.; Carter, S.L.; Stojanov, P.; McKenna, A.; Stevenson, K.; Lawrence, M.S.; Sougnez, C.; Stewart, C.; Sivachenko, A.; Wang, L.; et al. Evolution and impact of subclonal mutations in chronic lymphocytic leukemia. Cell 2013, 152, 714–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Späth, S.S.; Marjani, S.L.; Zhang, X.; Pan, W. Characterization of cancer genomic heterogeneity by next-generation sequencing advances precision medicine in cancer treatment. Precis. Clin. Med. 2018, 1, 29–48. [Google Scholar] [CrossRef] [Green Version]
- Pantel, K.; Alix-Panabières, C. Liquid biopsy and minimal residual disease—Latest advances and implications for cure. Nat. Rev. Clin. Oncol. 2019, 16, 409–424. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Yan Sun, Y. Efflux mechanism and pathway of verapamil pumping by human P-glycoprotein. Arch Biochem. Biophys. 2020, 696, 108675. [Google Scholar] [CrossRef]
- Fan, Y.F.; Zhang, W.; Zeng, L.; Lei, Z.N.; Cai, C.Y.; Gupta, P.; Yang, D.H.; Cui, Q.; Qin, Z.D.; Chen, Z.S.; et al. Dacomitinib antagonizes multidrug resistance (MDR) in cancer cells by inhibiting the efflux activity of ABCB1 and ABCG2 transporters. Cancer Lett. 2018, 421, 186–198. [Google Scholar] [CrossRef]
- Bernardes Marques, M.; Pontes Machado, A.; Antiqueira Santos, P.; Carrett-Dias, M.; Soares Araújo, G.; da Silva Alves, B.; Santos de Oliveira, B.; da Silva, F.M.R.J.; Dora, C.L.; Delgado Cañedo, A.; et al. Anti-MDR Effects of Quercetin and its Nanoemulsion in Multidrug Resistant Human Leukemia Cells. Anticancer Agents Med. Chem. 2021, 21, 1911–1920. [Google Scholar] [CrossRef]
- Vermunt, M.A.C.; Robbrecht, D.G.J.; Devriese, L.A.; Janssen, J.M.; Thijssen, B.; Keessen, M.; van Eijk, M.; Kessels, R.; Eskens, F.A.L.M.; Beijnen, J.H.; et al. ModraDoc006, an oral docetaxel formulation in combination with ritonavir (ModraDoc006/r), in metastatic castration-resistant prostate cancer patients: A phase Ib study. Cancer Rep. 2021, e1367. [Google Scholar] [CrossRef]
- Hodges, L.M.; Markova, S.M.; Chinn, L.W.; Gow, J.M.; Kroetz, D.L.; Klein, T.E.; Altman, R.B. Very important pharmacogene summary: ABCB1 (MDR1, P-glycoprotein). Pharm. Genom. 2011, 21, 152–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Variables | Cohorts | |
|---|---|---|
| Docetaxel (A) n = 45 | Cabazitaxel (B) n = 21 | |
| Still alive, n (%) | ||
| No | 44 (98) | 15 (71) |
| Yes | 1 (2) | 6 (29) |
| Prior treatments for mCRPC, n (%) | ||
| 0 | 12 (27) | 0 (0) |
| 1–3 | 23 (51) | 6 (29) |
| ≥4 | 10 (22) | 15 (71) |
| Prior abiraterone acetate, n (%) | ||
| No | 39 (87) | 9 (43) |
| Yes | 6 (13) | 12 (57) |
| Prior enzalutamide, n (%) | ||
| No | 43 (96) | 14 (67) |
| Yes | 2 (4) | 7 (33) |
| Prior radium-223, n (%) | ||
| No | 44 (98) | 19 (90) |
| Yes | 1 (2) | 2 (10) |
| Prior docetaxel, n (%) | ||
| No | 45 (100) | 0 (0) |
| Yes | 0 (0) | 21 (100) |
| Resistance, n (%) | ||
| No | 19 (42) | 3 (14) |
| Yes | 26 (58) | 18 (86) |
| PSA decline ≥ 80% within 4 months from taxane start, n (%) | ||
| No | 36 (80) | 20 (95) |
| Yes | 9 (20) | 1 (5) |
| PSA decline ≥ 50% within 4 months from taxane start, n (%) | ||
| No | 26 (58) | 18 (86) |
| Yes | 19 (42) | 3 (14) |
| Radiological response within 4 months from taxane start, n (%) | ||
| No | 42 (93) | 21 (100) |
| Yes | 2 (4) | 0 (0) |
| N/A | 1 (2) | 0 (0) |
| Cycles of taxane, n (%) | ||
| 1–3 | 12 (27) | 12 (57) |
| 4–6 | 4 (9) | 2 (10) |
| >6 | 24 (53) | 7 (33) |
| N/A | 5 (11) | 0 (0) |
| ABCB1 Amplification, n (%) | No ABCB1 Amplification, n (%) | Total, n (%) | |
|---|---|---|---|
| Resistance, n (%) | 6 (13.3) | 20 (44.5) | 26 (57.8) |
| No resistance, n (%) | 3 (6.7) | 16 (35.5) | 19 (42.2) |
| Total, n (%) | 9 (20.0) | 36 (80.0) | 45 (100.0) |
| ABCB1 Amplification, n (%) | No ABCB1 Amplification, n (%) | Total, n (%) | |
|---|---|---|---|
| Resistance, n (%) | 2 (9.5) | 16 (76.2) | 18 (85.7) |
| No resistance, n (%) | 0 (0.00) | 3 (14.3) | 3 (14.3) |
| Total, n (%) | 2 (9.5) | 19 (90.5) | 21 (100.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Francini, E.; Ou, F.-S.; Rhoades, J.; Wolfe, E.G.; O’Connor, E.P.; Ha, G.; Gydush, G.; Kelleher, K.M.; Bhatt, R.S.; Balk, S.P.; et al. Circulating Cell-Free DNA as Biomarker of Taxane Resistance in Metastatic Castration-Resistant Prostate Cancer. Cancers 2021, 13, 4055. https://doi.org/10.3390/cancers13164055
Francini E, Ou F-S, Rhoades J, Wolfe EG, O’Connor EP, Ha G, Gydush G, Kelleher KM, Bhatt RS, Balk SP, et al. Circulating Cell-Free DNA as Biomarker of Taxane Resistance in Metastatic Castration-Resistant Prostate Cancer. Cancers. 2021; 13(16):4055. https://doi.org/10.3390/cancers13164055
Chicago/Turabian StyleFrancini, Edoardo, Fang-Shu Ou, Justin Rhoades, Eric G. Wolfe, Edward P. O’Connor, Gavin Ha, Gregory Gydush, Kaitlin M. Kelleher, Rupal S. Bhatt, Steven P. Balk, and et al. 2021. "Circulating Cell-Free DNA as Biomarker of Taxane Resistance in Metastatic Castration-Resistant Prostate Cancer" Cancers 13, no. 16: 4055. https://doi.org/10.3390/cancers13164055
APA StyleFrancini, E., Ou, F.-S., Rhoades, J., Wolfe, E. G., O’Connor, E. P., Ha, G., Gydush, G., Kelleher, K. M., Bhatt, R. S., Balk, S. P., Sweeney, C. J., Adalsteinsson, V. A., Taplin, M.-E., & Choudhury, A. D. (2021). Circulating Cell-Free DNA as Biomarker of Taxane Resistance in Metastatic Castration-Resistant Prostate Cancer. Cancers, 13(16), 4055. https://doi.org/10.3390/cancers13164055