
Superior Overall Survival in Patients with Colorectal Cancer, Regular Aspirin Use, and Combined Wild-Type PIK3CA and KRAS-Mutated Tumors

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Cohort
2.2. Detection of PIK3CA Mutations
2.3. Detection of KRAS Mutations
2.4. Statistical Analysis
3. Results
3.1. Patients
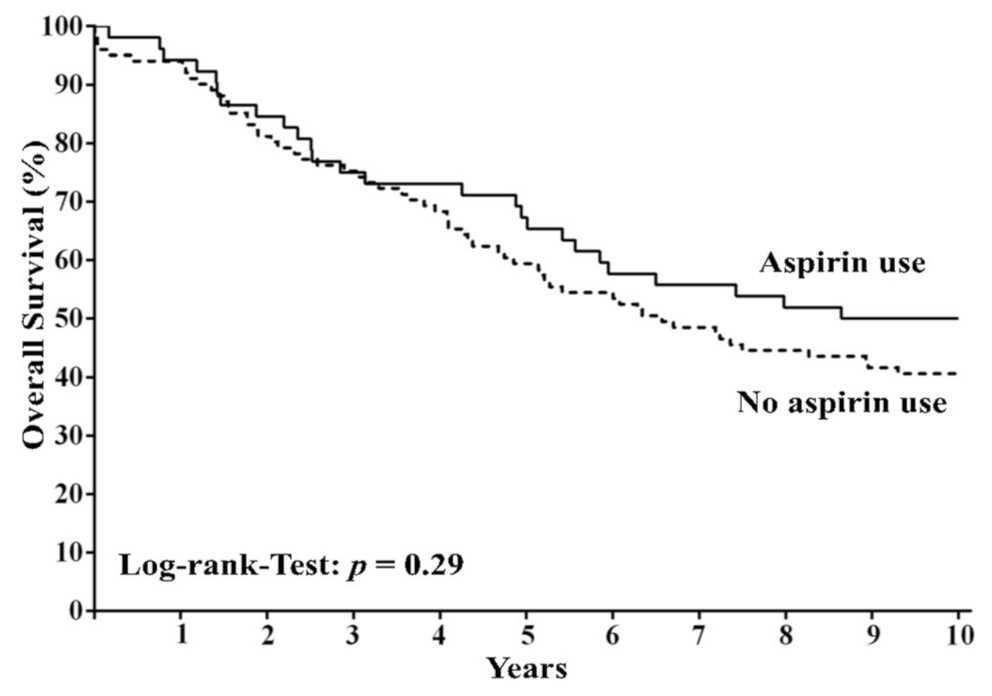
3.2. Aspirin Use and Survival in the Cohort of 153 Patients
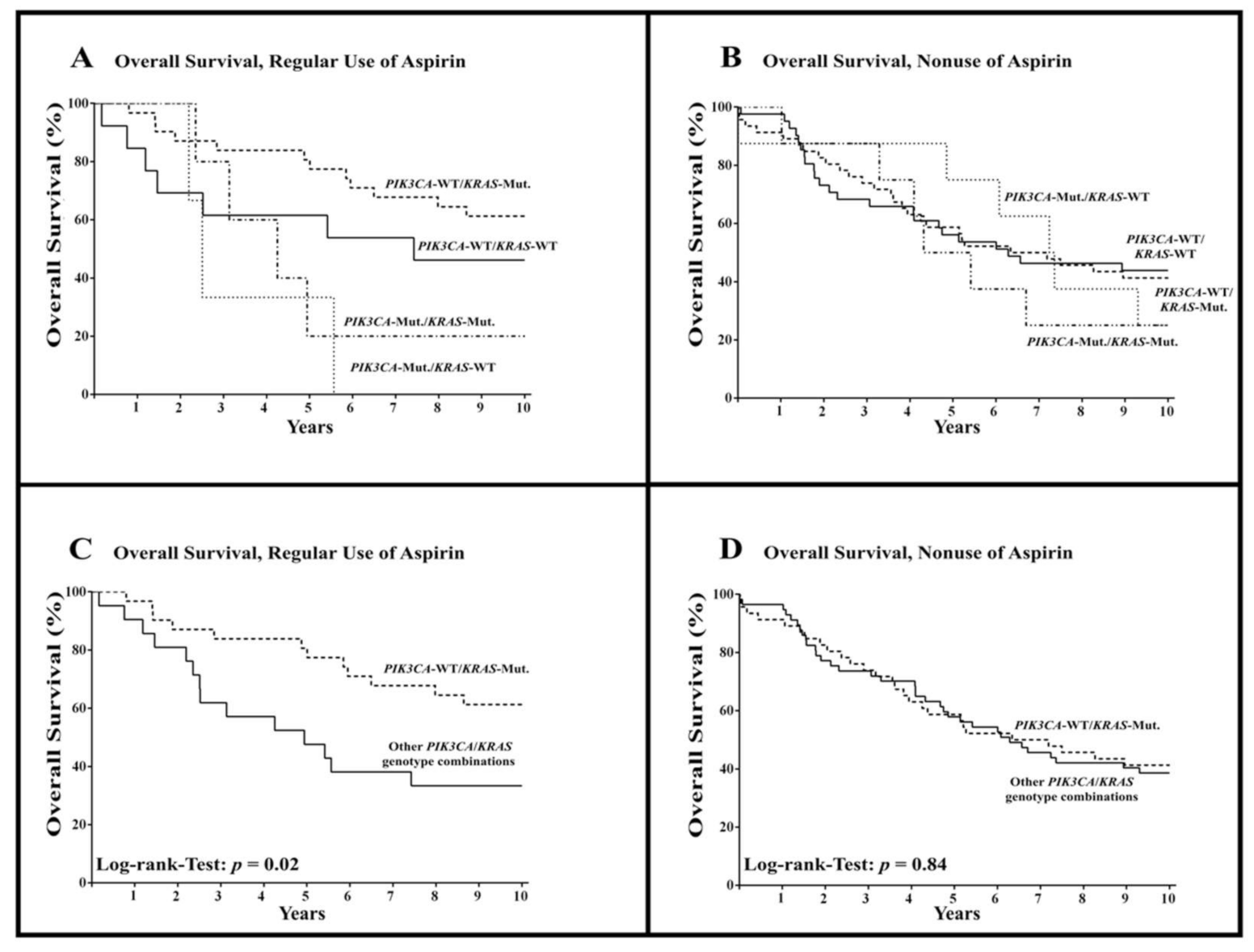
3.3. Aspirin Use and Survival According to PIK3CA und KRAS Mutational Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stewart, B.W.; Wild, C.P. World Cancer Report 2014; International Agency for Research on Cancer: Lyon, France; Geneva, Switzerland, 2014. [Google Scholar]
- Chan, A.T.; Ogino, S.; Fuchs, C.S. Aspirin use and survival after diagnosis of colorectal cancer. Jama 2009, 302, 649–658. [Google Scholar] [CrossRef]
- Rothwell, P.M.; Wilson, M.; Elwin, C.-E.; Norrving, B.; Algra, A.; Warlow, C.P.; Meade, T.W. Long-term effect of aspirin on colorectal cancer incidence and mortality: 20-year follow-up of five randomised trials. Lancet 2010, 376, 1741–1750. [Google Scholar] [CrossRef]
- Rothwell, P.M.; Wilson, M.; Price, J.F.; Belch, J.F.; Meade, T.W.; Mehta, Z. Effect of daily aspirin on risk of cancer metastasis: A study of incident cancers during randomised controlled trials. Lancet 2012, 379, 1591–1601. [Google Scholar] [CrossRef]
- Bains, S.J.; Mahic, M.; Myklebust, T.A.; Smastuen, M.C.; Yaqub, S.; Dorum, L.M.; Bjornbeth, B.A.; Moller, B.; Brudvik, K.W.; Tasken, K. Aspirin As Secondary Prevention in Patients with Colorectal Cancer: An Unselected Population-Based Study. J. Clin. Oncol. 2016, 34, 2501–2508. [Google Scholar] [CrossRef] [PubMed]
- Goh, C.H.; Goh, H.H.; Leong, W.Q.; Chew, M.H.; Pan, Y.S.; Tony, L.K.H.; Chew, L.; Tan, I.B.H.; Toh, H.C.; Tang, C.L.; et al. Post-operative aspirin use and colorectal cancer-specific survival in patients with stage I-III colorectal cancer. Anticancer Res. 2014, 34, 7407–7414. [Google Scholar] [PubMed]
- McCowan, C.; Munro, A.J.; Donnan, P.T.; Steele, R.J.C. Use of aspirin post-diagnosis in a cohort of patients with colorectal cancer and its association with all-cause and colorectal cancer specific mortality. Eur. J. Cancer 2013, 49, 1049–1057. [Google Scholar] [CrossRef] [PubMed]
- Hennekens, C.H.; Schneider, W.R. The need for wider and appropriate utilization of aspirin and statins in the treatment and prevention of cardiovascular disease. Expert Rev. Cardiovasc. Ther. 2008, 6, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Ittaman, S.V.; VanWormer, J.J.; Rezkalla, S.H. The role of aspirin in the prevention of cardiovascular disease. Clin. Med. Res. 2014, 12, 147–154. [Google Scholar] [CrossRef] [Green Version]
- Williams, C.S.; Mann, M.; DuBois, R.N. The role of cyclooxygenases in inflammation, cancer, and development. Oncogene 1999, 18, 7908–7916. [Google Scholar] [CrossRef] [Green Version]
- Ogino, S.; Fuchs, C.S.; Giovannucci, E. How many molecular subtypes? Implications of the unique tumor principle in personalized medicine. Expert Rev. Mol. Diagn. 2012, 12, 621–628. [Google Scholar] [CrossRef] [Green Version]
- Coyle, C.; Cafferty, F.H.; Langley, R.E. Aspirin and Colorectal Cancer Prevention and Treatment: Is It for Everyone? Curr. Colorectal Cancer Rep. 2016, 12, 27–34. [Google Scholar] [CrossRef] [Green Version]
- Liao, X.; Lochhead, P.; Nishihara, R.; Morikawa, T.; Kuchiba, A.; Yamauchi, M.; Imamura, Y.; Qian, Z.R.; Baba, Y.; Shima, K.; et al. Aspirin use, tumor PIK3CA mutation, and colorectal-cancer survival. N. Engl. J. Med. 2012, 367, 1596–1606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domingo, E.; Church, D.N.; Sieber, O.; Ramamoorthy, R.; Yanagisawa, Y.; Johnstone, E.; Davidson, B.; Kerr, D.J.; Tomlinson, I.P.M.; Midgley, R. Evaluation of PIK3CA mutation as a predictor of benefit from nonsteroidal anti-inflammatory drug therapy in colorectal cancer. J. Clin. Oncol. 2013, 31, 4297–4305. [Google Scholar] [CrossRef] [PubMed]
- Kothari, N.; Kim, R.; Jorissen, R.N.; Desai, J.; Tie, J.; Wong, H.-L.; Faragher, I.; Jones, I.; Day, F.L.; Li, S.; et al. Impact of regular aspirin use on overall and cancer-specific survival in patients with colorectal cancer harboring a PIK3CA mutation. Acta Oncol. 2015, 54, 487–492. [Google Scholar] [CrossRef]
- Murphy, C.; Turner, N.; Wong, H.-L.; Sinnathamby, M.; Tie, J.; Lee, B.; Desai, J.; Skinner, I.; Christie, M.; Hutchinson, R.; et al. Examining the impact of regular aspirin use and PIK3CA mutations on survival in stage 2 colon cancer. Intern. Med. J. 2017, 47, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Reimers, M.S.; Bastiaannet, E.; Langley, R.E.; van Eijk, R.; van Vlierberghe, R.L.P.; Lemmens, V.E.P.; van Herk-Sukel, M.P.P.; van Wezel, T.; Fodde, R.; Kuppen, P.J.K.; et al. Expression of HLA class I antigen, aspirin use, and survival after a diagnosis of colon cancer. JAMA Intern. Med. 2014, 174, 732–739. [Google Scholar] [CrossRef] [Green Version]
- Wu, W.K.K.; Sung, J.J.Y.; Lee, C.W.; Yu, J.; Cho, C.H. Cyclooxygenase-2 in tumorigenesis of gastrointestinal cancers: An update on the molecular mechanisms. Cancer Lett. 2010, 295, 7–16. [Google Scholar] [CrossRef]
- Burn, J.; Gerdes, A.-M.; Macrae, F.; Mecklin, J.-P.; Moeslein, G.; Olschwang, S.; Eccles, D.; Evans, D.G.; Maher, E.R.; Bertario, L.; et al. Long-term effect of aspirin on cancer risk in carriers of hereditary colorectal cancer: An analysis from the CAPP2 randomised controlled trial. Lancet 2011, 378, 2081–2087. [Google Scholar] [CrossRef] [Green Version]
- Tomozawa, S.; Nagawa, H.; Tsuno, N.; Hatano, K.; Osada, T.; Kitayama, J.; Sunami, E.; Nita, M.E.; Ishihara, S.; Yano, H.; et al. Inhibition of haematogenous metastasis of colon cancer in mice by a selective COX-2 inhibitor, JTE-522. Br. J. Cancer 1999, 81, 1274–1279. [Google Scholar] [CrossRef] [Green Version]
- Yao, M.; Lam, E.C.; Kelly, C.R.; Zhou, W.; Wolfe, M.M. Cyclooxygenase-2 selective inhibition with NS-398 suppresses proliferation and invasiveness and delays liver metastasis in colorectal cancer. Br. J. Cancer 2004, 90, 712–719. [Google Scholar] [CrossRef] [Green Version]
- Alfonso, L.; Ai, G.; Spitale, R.C.; Bhat, G.J. Molecular targets of aspirin and cancer prevention. Br. J. Cancer 2014, 111, 61–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, A.T.; Ogino, S.; Fuchs, C.S. Aspirin and the risk of colorectal cancer in relation to the expression of COX-2. N. Engl. J. Med. 2007, 356, 2131–2142. [Google Scholar] [CrossRef] [PubMed]
- Ferrández, A.; Piazuelo, E.; Castells, A. Aspirin and the prevention of colorectal cancer. Best practice & research. Clin. Gastroenterol 2012, 26, S185–S195. [Google Scholar]
- Nosho, K.; Kawasaki, T.; Ohnishi, M.; Suemoto, Y.; Kirkner, G.J.; Zepf, D.; Yan, L.; Longtine, J.A.; Fuchs, C.S.; Ogino, S. PIK3CA mutation in colorectal cancer: Relationship with genetic and epigenetic alterations. Neoplasia 2008, 10, 534–541. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.S.; Menter, D.G.; Kopetz, S. Right Versus Left Colon Cancer Biology: Integrating the Consensus Molecular Subtypes. J. Natl. Compr. Cancer Netw. 2017, 15, 411–419. [Google Scholar] [CrossRef] [Green Version]
- Yamauchi, M.; Morikawa, T.; Kuchiba, A.; Imamura, Y.; Qian, Z.R.; Nishihara, R.; Liao, X.; Waldron, L.; Hoshida, Y.; Huttenhower, C.; et al. Assessment of colorectal cancer molecular features along bowel subsites challenges the conception of distinct dichotomy of proximal versus distal colorectum. Gut 2012, 61, 847–854. [Google Scholar] [CrossRef]
- Gao, M.; Guo, K.-M.; Wei, Y.-M.; Ma, M.-M.; Cai, J.-R.; Xia, T.-T.; Ye, Q.-J. Aspirin inhibits the proliferation of human uterine leiomyoma cells by downregulation of KRasp110α interaction. Oncol. Rep. 2017, 38, 2507–2517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, C.; Li, W.B.; Liu, J.B.; Lu, J.W.; Feng, J.F. Autophagy: Novel applications of nonsteroidal anti-inflammatory drugs for primary cancer. Cancer Med. 2018, 7, 471–484. [Google Scholar] [CrossRef]
- Castoldi, F.; Humeau, J.; Martins, I.; Lachkar, S.; Loew, D.; Dingli, F.; Durand, S.; Enot, D.; Bossut, N.; Chery, A.; et al. Autophagy-mediated metabolic effects of aspirin. Cell Death Discov. 2020, 6, 129. [Google Scholar] [CrossRef]
- Huang, Z.; Fang, W.; Liu, W.; Wang, L.; Liu, B.; Liu, S. Aspirin induces Beclin-1-dependent autophagy of human hepatocellular carcinoma cell. Eur. J. Pharmacol. 2018, 823, 58–64. [Google Scholar] [CrossRef]
- Zeng, X.; Overmeyer, J.H.; Maltese, W.A. Functional specificity of the mammalian Beclin-Vps34 PI 3-kinase complex in macroautophagy versus endocytosis and lysosomal enzyme trafficking. J. Cell Sci. 2006, 15, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.; Li, Y.; Zhang, C.; Yi, H.; Wu, C.; Wang, J.; Liu, Y.; Tan, J.; Wen, J. Downregulation of Beclin 1 and impairment of autophagy in a small population of colorectal cancer. Dig. Dis. Sci. 2013, 58, 2887–2894. [Google Scholar] [CrossRef] [Green Version]
- Robert Koch Institut (Ed.) Bericht zum Krebsgeschehen in Deutschland 2016; Zentrum für Krebsregisterdaten: Berlin, Germany, 2016. [Google Scholar]
- Barault, L.; Veyrie, N.; Jooste, V.; Lecorre, D.; Chapusot, C.; Ferraz, J.-M.; Lièvre, A.; Cortet, M.; Bouvier, A.-M.; Rat, P.; et al. Mutations in the RAS-MAPK, PI(3)K (phosphatidylinositol-3-OH kinase) signaling network correlate with poor survival in a population-based series of colon cancers. Int. J. Cancer 2008, 122, 2255–2259. [Google Scholar] [CrossRef] [PubMed]
- Schmoll, H.J.; Stein, A.; Van Cutsem, E.; Price, T.; Hofheinz, R.D.; Nordlinger, B.; Daisne, J.F.; Janssens, J.; Brenner, B.; Reinel, H.; et al. Pre- and Postoperative Capecitabine Without or With Oxaliplatin in Locally Advanced Rectal Cancer: PETACC 6 Trial by EORTC GITCG and ROG, AIO, AGITG, BGDO, and FFCD. J. Clin. Oncol. 2021, 39, 17–29. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Patients (n = 153) | Wild-Type PIK3CA | Mutant PIK3CA | ||
|---|---|---|---|---|---|
| No Aspirin Use | Aspirin Use | No Aspirin Use | Aspirin Use | ||
| Sex—no. (%) | |||||
| Male | 90 (59%) | 46 (54%) | 26 (59%) | 11 (69%) | 7 (88%) |
| Female | 63 (41%) | 39 (46%) | 18 (41%) | 5 (31%) | 1 (12%) |
| Age—year | 69.9 ± 7.7 | 68.8 ± 11.6 | 71.6 ± 7.6 | 69.4 ± 9.0 | 72.4 ± 5.0 |
| Tumor location—no. (%) | |||||
| Rectum | 46 (30%) | 25 (29%) | 17 (39%) | 3 (19%) | 1 (13%) |
| Distal colon | 68 (44%) | 42 (49%) | 15 (34%) | 6 (38%) | 5 (63%) |
| Proximal colon | 39 (25%) | 18 (21%) | 12 (27%) | 7 (44%) | 2 (25%) |
| Disease stage—no. (%) | |||||
| I | 39 (25%) | 22 (26%) | 10 (23%) | 4 (25%) | 3 (37%) |
| II | 53 (35%) | 31 (36%) | 16 (36%) | 5 (31%) | 1 (13%) |
| III | 56 (37%) | 29 (34%) | 16 (36%) | 7 (44%) | 4 (50%) |
| IV | 5 (3%) | 3 (4%) | 2 (5%) | 0 (0%) | 0 (0%) |
| Tumor differentiation—no. (%) | |||||
| G1 | 5 (3%) | 2 (2%) | 1 (2%) | 0 (0%) | 2 (25%) |
| G2 | 133 (87%) | 73 (86%) | 41 (93%) | 15 (94%) | 4 (50%) |
| G3 | 15 (10%) | 10 (12%) | 2 (5%) | 1 (6%) | 2 (25%) |
| KRAS | |||||
| Wild-type | 66 (43%) | 41 (48%) | 14 (32%) | 8 (50%) | 3 (38%) |
| Mutant | 87 (57%) | 44 (52%) | 30 (68%) | 8 (50%) | 5 (62%) |
| Aspirin Use | Number of Patients | Dead at 10 Years after Diagnosis | Alive at 10 Years after Diagnosis | p-Value |
|---|---|---|---|---|
| Yes | 0.02 | |||
| PIK3CA-WT/KRAS-Mut. | 31 | 12 (39%) | 19 (61%) | |
| Other PIK3CA/KRAS genotype combinations (except PIK3CA-WT/KRAS-Mut.) | 21 | 14 (67%) | 7 (33%) | |
| No | 0.84 | |||
| PIK3CA-WT/KRAS-Mut. | 45 | 26 (58%) | 19 (42%) | |
| Other PIK3CA/KRAS genotype combinations (except PIK3CA-WT/KRAS-Mut.) | 56 | 34 (61%) | 22 (39%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gebauer, L.; Nist, A.; Mernberger, M.; Stiewe, T.; Moll, R.; Stabla, K.; Klinge, U.; Mack, E.; Brendel, C.; Neubauer, A. Superior Overall Survival in Patients with Colorectal Cancer, Regular Aspirin Use, and Combined Wild-Type PIK3CA and KRAS-Mutated Tumors. Cancers 2021, 13, 4959. https://doi.org/10.3390/cancers13194959
Gebauer L, Nist A, Mernberger M, Stiewe T, Moll R, Stabla K, Klinge U, Mack E, Brendel C, Neubauer A. Superior Overall Survival in Patients with Colorectal Cancer, Regular Aspirin Use, and Combined Wild-Type PIK3CA and KRAS-Mutated Tumors. Cancers. 2021; 13(19):4959. https://doi.org/10.3390/cancers13194959
Chicago/Turabian StyleGebauer, Leonie, Andrea Nist, Marco Mernberger, Thorsten Stiewe, Roland Moll, Kathleen Stabla, Uwe Klinge, Elisabeth Mack, Cornelia Brendel, and Andreas Neubauer. 2021. "Superior Overall Survival in Patients with Colorectal Cancer, Regular Aspirin Use, and Combined Wild-Type PIK3CA and KRAS-Mutated Tumors" Cancers 13, no. 19: 4959. https://doi.org/10.3390/cancers13194959
APA StyleGebauer, L., Nist, A., Mernberger, M., Stiewe, T., Moll, R., Stabla, K., Klinge, U., Mack, E., Brendel, C., & Neubauer, A. (2021). Superior Overall Survival in Patients with Colorectal Cancer, Regular Aspirin Use, and Combined Wild-Type PIK3CA and KRAS-Mutated Tumors. Cancers, 13(19), 4959. https://doi.org/10.3390/cancers13194959