
Predicting Prognosis of Breast Cancer Patients with Brain Metastases in the BMBC Registry—Comparison of Three Different GPA Prognostic Scores

 , , , , , ,
, , , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Patients’ Characteristics
2.2. Survival Analysis
2.3. Prognostic Indices
2.4. Diagnostic Accuracy of GPA Scores
3. Discussion
4. Materials and Methods
4.1. Calculation of GPA Scores
4.2. Biological Subtype and ECOG/Karnofsky Performance Status
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Smedby, K.E.; Brandt, L.; Bäcklund, M.L.; Blomqvist, P. Brain metastases admissions in Sweden between 1987 and 2006. Br. J. Cancer 2009, 101, 1919–1924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witzel, I.; Oliveira-Ferrer, L.; Pantel, K.; Muller, V.; Wikman, H. Breast cancer brain metastases: Biology and new clinical perspectives. Breast Cancer Res. 2016, 18, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witzel, I.; Laakmann, E.; Weide, R.; Neunhöffer, T.; Park-Simon, T.-J.; Schmidt, M.; Fasching, P.; Hesse, T.; Polasik, A.; Mohrmann, S.; et al. Treatment and outcomes of patients in the Brain Metastases in Breast Cancer Network Registry. Eur. J. Cancer 2018, 102, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laakmann, E.; Riecke, K.; Goy, Y.; Kersten, J.F.; Krüll, A.; Müller, V.; Petersen, C.; Witzel, I. Comparison of nine prognostic scores in patients with brain metastases of breast cancer receiving radiotherapy of the brain. J. Cancer Res. Clin. Oncol. 2015, 142, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Bentzen, S.M.; Li, J.; Renschler, M.F.; Mehta, M.P. Relationship between neurocognitive function and quality of life after whole-brain radiotherapy in patients with brain metastasis. Int. J. Radiat. Oncol. 2008, 71, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Sperduto, P.W.; Berkey, B.; Gaspar, L.E.; Mehta, M.; Curran, W. A new prognostic index and comparison to three other indices for patients with brain metastases: An analysis of 1960 patients in the RTOG database. Int. J. Radiat. Oncol. 2008, 70, 510–514. [Google Scholar] [CrossRef] [PubMed]
- Antoni, D.; Clavier, J.-B.; Pop, M.; Schumacher, C.; Lefebvre, F.; Noel, G. Institutional, retrospective analysis of 777 patients with brain metastases: Treatment outcomes and diagnosis-specific prognostic factors. Int. J. Radiat. Oncol. 2013, 86, 630–637. [Google Scholar] [CrossRef] [PubMed]
- Sperduto, P.W.; Kased, N.; Roberge, D.; Xu, Z.; Shanley, R.; Luo, X.; Sneed, P.K.; Chao, S.T.; Weil, R.J.; Suh, J.; et al. Effect of tumor subtype on survival and the graded prognostic assessment for patients with breast cancer and brain metastases. Int. J. Radiat. Oncol. 2012, 82, 2111–2117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sperduto, P.W.; Mesko, S.; Li, J.; Cagney, D.; Aizer, A.; Lin, N.U.; Nesbit, E.; Kruser, T.J.; Chan, J.; Braunstein, S.; et al. Beyond an updated graded prognostic assessment (Breast GPA): A prognostic index and trends in treatment and survival in breast cancer brain metastases from 1985 to today. Int. J. Radiat. Oncol. 2020, 107, 334–343. [Google Scholar] [CrossRef] [PubMed]
- Tabouret, E.; Metellus, P.; Gonçalves, A.; Esterni, B.; Charaffe-Jauffret, E.; Viens, P.; Tallet, A. Assessment of prognostic scores in brain metastases from breast cancer. Neuro Oncol. 2014, 16, 421–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, P.D.; Ahluwalia, M.S.; Khan, O.H.; Asher, A.L.; Wefel, J.S.; Gondi, V. Whole-brain radiotherapy for brain metastases: Evolution or revolution? J. Clin. Oncol. 2018, 36, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Lin, N.U.; Borges, V.; Anders, C.; Murthy, R.K.; Paplomata, E.; Hamilton, E.; Hurvitz, S.; Loi, S.; Okines, A.; Abramson, V.; et al. Intracranial efficacy and survival with tucatinib plus trastuzumab and capecitabine for previously treated HER2-positive breast cancer with brain metastases in the HER2CLIMB trial. J. Clin. Oncol. 2020, 38, 2610–2619. [Google Scholar] [CrossRef] [PubMed]
- Perez, E.A.; Awada, A.; O’Shaughnessy, J.; Rugo, H.S.; Twelves, C.; Im, S.A.; Gomez-Pardo, P.; Schwartzberg, L.S.; Dieras, V.; Yardley, D.A.; et al. Etirinotecan pegol (NKTR-102) versus treatment of physician’s choice in women with advanced breast cancer previously treated with an anthracycline, a taxane, and capecitabine (BEACON): A randomised, open-label, multicentre, phase 3 trial. Lancet Oncol. 2015, 16, 1556–1568. [Google Scholar] [CrossRef]
- Darlix, A.; Louvel, G.; Fraisse, J.; Jacot, W.; Brain, E.; Debled, M.; Mouret-Reynier, M.A.; Goncalves, A.; Dalenc, F.; Delaloge, S.; et al. Impact of breast cancer molecular subtypes on the incidence, kinetics and prognosis of central nervous system metastases in a large multicentre real-life cohort. Br. J. Cancer 2019, 121, 991–1000. [Google Scholar] [CrossRef] [PubMed]
- Gianni, L.; Pienkowski, T.; Im, Y.-H.; Roman, L.; Tseng, L.-M.; Liu, M.-C.; Lluch, A.; Staroslawska, E.; De La Haba-Rodriguez, J.; Im, S.-A.; et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): A randomised multicentre, open-label, phase 2 trial. Lancet Oncol. 2012, 13, 25–32. [Google Scholar] [CrossRef]
- Sperduto, P.W.; Kased, N.; Roberge, D.; Chao, S.T.; Shanley, R.; Luo, X.; Sneed, P.K.; Suh, J.; Weil, R.J.; Jensen, A.W.; et al. The effect of tumor subtype on the time from primary diagnosis to development of brain metastases and survival in patients with breast cancer. J. Neurooncol. 2013, 112, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Melisko, M.E.; Moore, D.H.; Sneed, P.K.; De Franco, J.; Rugo, H.S. Brain metastases in breast cancer: Clinical and pathologic characteristics associated with improvements in survival. J. Neurooncol. 2008, 88, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Zindler, J.D.; Rodrigues, G.; Haasbeek, C.J.; De Haan, P.F.; Meijer, O.W.; Slotman, B.J.; Lagerwaard, F.J. The clinical utility of prognostic scoring systems in patients with brain metastases treated with radiosurgery. Radiother. Oncol. 2013, 106, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Nieder, C.; Marienhagen, K.; Thamm, R.; Astner, S.; Molls, M.; Norum, J. Prediction of very short survival in patients with brain metastases from breast cancer. Clin. Oncol. 2008, 20, 337–339. [Google Scholar] [CrossRef] [PubMed]
- Blanche, P.; Dartigues, J.F.; Jacqmin-Gadda, H. Estimating and comparing time-dependent areas under receiver operating characteristic curves for censored event times with competing risks. Stat. Med. 2013, 32, 5381–5397. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| GPA | 0 points | 0.5 points | 1.0 points | |
|---|---|---|---|---|
| Karnofsky | ≤60 | 70–80 | 90–100 | |
| Number of BM | ≥4 | 2–3 | 1 | |
| ECM | yes | no | ||
| Age | ≥60 | 50–59 | <50 | |
| group 1: 0–1P; 2:1.5–2.5P; 3: 3.0P; 4: 3.5–4.0P | ||||
| Breast-GPA | 0 points | 0.5 points | 1.0 points | 1.5 points |
| Karnofsky | ≤50 | 60 | 70–80 | 90–100 |
| Subtype | TNBC | n/a | LumA | HER2 |
| Age | ≥60 | <60 | n/a | n/a |
| group 1:0–1 P.; 2:1.5–2.0 P.;3: 2.5–3.0 P.; 4:3.5–4.0 P. | ||||
| Updated Breast-GPA | 0 points | 0.5 points | 1.0 points | 1.5 points |
| Karnofsky | ≤60 | 70–80 | 90–100 | n/a |
| Subtype | TNBC | n/a | LumA | HER2, LumB |
| Age | ≥60 | <60 | n/a | n/a |
| Number of BM | >1 | =1 | n/a | n/a |
| ECM | yes | no | ||
| group 1: 0–1P.; 2: 1.5–2.0 P.; 3:2.5–3.0 P.; 4: 3.5–4.0 P. | ||||
| Parameter | Category | Number (%) |
|---|---|---|
| Age at first diagnosis of BC, years | Median | 53.0 |
| range | 20.0, 87.0 | |
| missing | 0 | |
| Age at diagnosis of BM, years | Median | 57.0 |
| range | 25.0, 90.0 | |
| missing | 0 | |
| Histological tumour type | ductal or ductal-lobular-invasive | 691 (78.8) |
| lobular-invasive | 60 (6.8) | |
| other | 126 (14.4) | |
| missing | 5 | |
| Biological subtype (according to Sperduto 2012) | TNBC (HR−/HER2−) | 197 (22.3) |
| Luminal A (HR+, HER2−) | 295 (33.4) | |
| Luminal B/HER2 enriched (HR+, HER2+) | 221 (25.1) | |
| HER2 (HR−, HER2+) | 169 (19.2) | |
| missing | 0 | |
| KPS at diagnosis of BM | 100% | 119 (13.5) |
| 80–90% | 393 (44.6) | |
| 60–70% | 267 (30.3) | |
| 40–50% | 80 (9.1) | |
| 10–30% | 23 (2.6) | |
| missing | 0 | |
| Number of BM | 1 | 234 (26.5) |
| 2–3 | 245 (27.8) | |
| ≥4 | 403 (45.7) | |
| missing | 0 | |
| Diagnostic method to detect BM | only clinical | 9 (1.0) |
| CT w/o clinical | 209 (23.8) | |
| MRI w/o clinical | 589 (67.1) | |
| CT and MRI w/o clinical | 71 (8.1) | |
| missing | 4 | |
| Local treatment of BM | Surgery only | 34 (4.5) |
| Radiotherapy only | 544 (71.3) | |
| Surgery and radiotherapy | 185 (24.2) | |
| missing | 119 | |
| ECM | no | 138 (15.6) |
| yes | 744 (84.4) | |
| Leptomeningeal metastases | no | 814 (92.7) |
| yes | 64 (7.3) | |
| missing | 4 |
| Parameter | Category | Median Survival (months) | 95%-CI | HR | 95% CI | p-Value |
|---|---|---|---|---|---|---|
| Age at diagnosis of BM, binary | <60 | 11.3 | (9.6, 13.7) | |||
| ≥60 | 5 | (3.9, 5.9) | 1.53 | (1.32, 1.77) | <0.001 | |
| ECM | no | 15.6 | (10.8, 23.8) | |||
| yes | 7.8 | (6.4, 9.0) | 1.67 | (1.34, 2.08) | <0.001 | |
| Number of BM | 1 | 14.1 | (10.3, 19.2) | |||
| 2–3 | 9.7 | (6.1, 12.3) | 1.34 | (1.09, 1.65) | 0.005 | |
| ≥4 | 6.2 | (5.1, 7.2) | 1.80 | (1.50, 2.16) | <0.001 | |
| Biological subtype (acc. to Sperduto 2012) | TNBC | 4.8 | (3.8, 6.1) | |||
| Luminal A (HR+, HER2-) | 6.0 | (5.0, 7.9) | 0.79 | (0.65, 0.95) | 0.014 | |
| Luminal B (HR+, HER2+) | 16.0 | (13.0, 21.7) | 0.43 | (0.34, 0.53) | <0.001 | |
| HER2 (HR-, HER2+) | 12.3 | (9.2, 17.3) | 0.49 | (0.39, 0.62) | <0.001 | |
| KPS | 100% | 17.9 | (12.9, 22.1) | |||
| 80–90% | 13.0 | (10.8, 15.1) | 1.26 | (0.99, 1.60) | 0.057 | |
| 60–70% | 4.4 | (3.5, 5.2) | 2.28 | (1.78, 2.92) | <0.001 | |
| 40–50% | 2.9 | (2.2, 3.9) | 3.66 | (2.68,5.00) | <0.001 | |
| 10–30% | 2.1 | (1.1, 3.0) | 4.76 | (2.97, 7.63) | <0.001 |
| Parameter | Group | Points | Number of Patients | Median Survival (months) | HR | 95%-CI | p-Value |
|---|---|---|---|---|---|---|---|
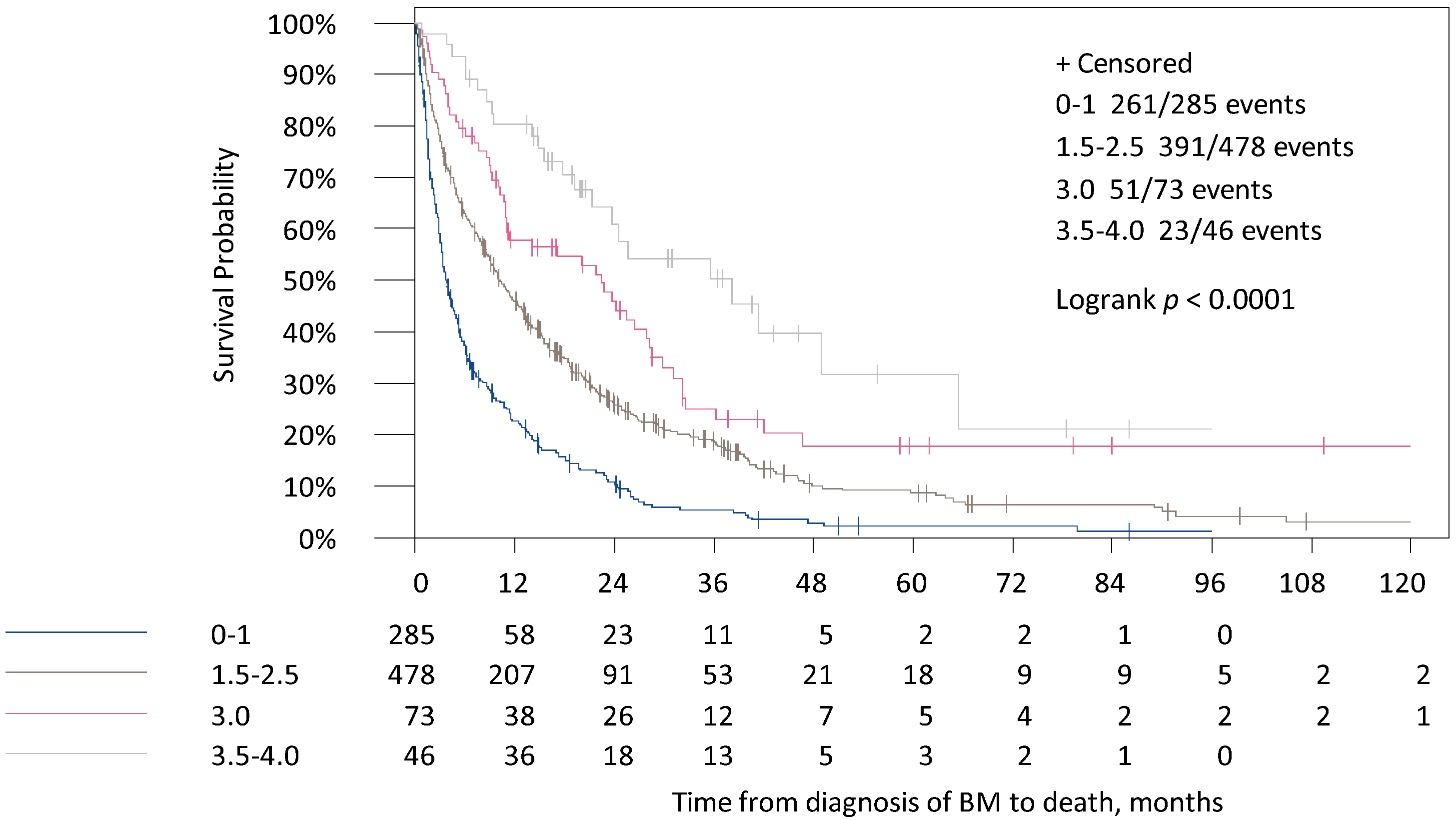
| Original GPA | 1 | 0–1 | 285 | 3.7 | |||
| 2 | 1.5–2.5 | 478 | 10.1 | 0.53 | (0.46, 0.63) | <0.001 | |
| 3 | 3.0 | 73 | 22.4 | 0.34 | (0.25, 0.46) | <0.001 | |
| 4 | 3.5–4.0 | 46 | 38.2 | 0.21 | (0.14, 0.32) | <0.001 | |
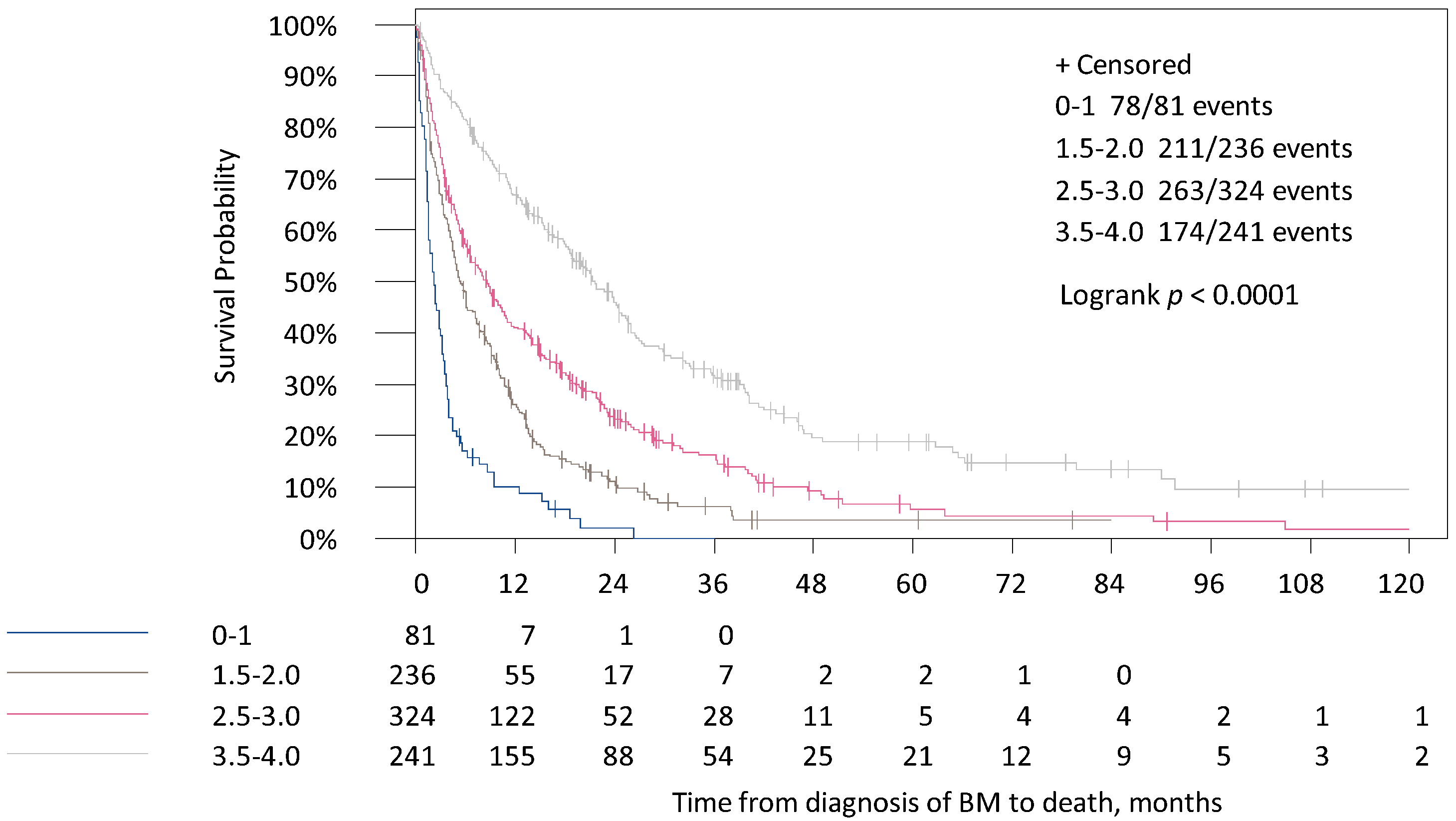
| Breast-GPA | 1 | 0–1 | 81 | 2.2 | |||
| 2 | 1.5–2.0 | 236 | 5.4 | 0.47 | (0.36, 0.61) | <0.001 | |
| 3 | 2.5–3.0 | 324 | 8.6 | 0.31 | (0.24, 0.41) | <0.001 | |
| 4 | 3.5–4.0 | 241 | 21.7 | 0.17 | (0.13, 0.23) | <0.001 | |
| updated Breast-GPA | 1 | 0–1 | 114 | 2.7 | |||
| 2 | 1.5–2.0 | 327 | 5.2 | 0.63 | (0.50, 0.78) | <0.001 | |
| 3 | 2.5–3.0 | 352 | 15.2 | 0.29 | (0.23, 0.37) | <0.001 | |
| 4 | 3.5–4.0 | 89 | 32.2 | 0.15 | (0.11, 0.21) | <0.001 |
| GPA-Score | Timepoint | Time-Dependent Sensitivity (%) (95%-CI) | Time-Dependent Specificity (%) (95%-CI) | Time-Dependent PPV (%) (95%-CI) | Time-Dependent NPV (%) (95%-CI) |
|---|---|---|---|---|---|
| Original GPA | 12 months | 92.2 (89.9, 94.6) | 21.8 (17.4, 26.2) | 62.6 (59.1, 66.1) | 66.3 (57.7, 75.0) |
| Breast-GPA | 12 months | 68.1 (64.0, 72.2) | 68.7 (63.8, 73.7) | 75.6 (71.6, 79.6) | 60.2 (55.4, 65.0) |
| updated Breast GPA | 12 months | 84.8 (81.7, 88.0) | 48.1 (42.8, 53.4) | 69.9 (66.2, 73.6) | 69.1 (63.2, 74.9) |
| GPA-Score | Time Point | Time-Dependent Sensitivity (%) (95%-CI) | Time-Dependent Specificity (%) (95%-CI) | Time-Dependent PPV (%) (95%-CI) | Time-Dependent NPV (%) (95%-CI) |
|---|---|---|---|---|---|
| Original GPA | 3 months | 24.4 (18.9, 29.9) | 91.6 (89.4, 93.7) | 51.3 (42.0, 60.6) | 76.9 (73.9, 79.9) |
| Breast-GPA | 3 months | 6.8 (3.6, 10.1) | 98.4 (97.5, 99.4) | 61.4 (42.7, 80.2) | 74.4 (71.4, 77.3) |
| updatedBreast-GPA | 3 months | 11.5 (7.4, 15.6) | 97.5 (96.3, 98.7) | 62.7 (48.3, 77.2) | 75.2 (72.2, 78.1) |
| GPA-Score | Time Point | AUC (%) (95%-CI) | Comparison | p-Value |
|---|---|---|---|---|
| Original GPA | 3 months | 70.0 (66.3, 73.7) | ||
| Original GPA | 12 months | 69.5 (66.0, 73.1) | ||
| Breast-GPA | 3 months | 69.1 (65.3, 73.0) | Breast-GPA vs. original GPA | 0.698 |
| Breast-GPA | 12 months | 73.0 (69.6, 76.4) | 0.086 | |
| updated Breast-GPA | 3 months | 71.4 (67.8, 75.0) | Breast-GPA vs. updated Breast-GPA | 0.010 |
| updated Breast-GPA | 12 months | 74.2 (70.9, 77.5) | 0.176 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riecke, K.; Müller, V.; Weide, R.; Schmidt, M.; Park-Simon, T.-W.; Möbus, V.; Mundhenke, C.; Polasik, A.; Lübbe, K.; Hesse, T.; et al. Predicting Prognosis of Breast Cancer Patients with Brain Metastases in the BMBC Registry—Comparison of Three Different GPA Prognostic Scores. Cancers 2021, 13, 844. https://doi.org/10.3390/cancers13040844
Riecke K, Müller V, Weide R, Schmidt M, Park-Simon T-W, Möbus V, Mundhenke C, Polasik A, Lübbe K, Hesse T, et al. Predicting Prognosis of Breast Cancer Patients with Brain Metastases in the BMBC Registry—Comparison of Three Different GPA Prognostic Scores. Cancers. 2021; 13(4):844. https://doi.org/10.3390/cancers13040844
Chicago/Turabian StyleRiecke, Kerstin, Volkmar Müller, Rudolf Weide, Marcus Schmidt, Tjoung-Won Park-Simon, Volker Möbus, Christoph Mundhenke, Arkadius Polasik, Kristina Lübbe, Tobias Hesse, and et al. 2021. "Predicting Prognosis of Breast Cancer Patients with Brain Metastases in the BMBC Registry—Comparison of Three Different GPA Prognostic Scores" Cancers 13, no. 4: 844. https://doi.org/10.3390/cancers13040844