Simple Summary
Ramucirumab has been shown to be effective as a second-line agent after sorafenib in hepatocellular carcinoma (HCC) patients whose α-fetoprotein was ≥400 ng/mL. We performed a retrospective cohort study to investigate ramucirumab efficacy in a real-world setting. Progression-free survival (PFS) was consistent through treatment lines, modified albumin–bilirubin (mALBI) grade, Barcelona Clinic for Liver Cancer (BCLC) stage, and α-fetoprotein (AFP) level. By contrast, ascites was more frequently seen in mALBI 2b/3 patients and, therefore, should be carefully monitored.
Abstract
Background: The present study aimed to clarify the efficacy and safety of ramucirumab in a real-world setting, including patients who experienced two or more systemic treatments or whose hepatic reserve was deteriorated. Methods: In total, 79 patients with hepatocellular carcinoma (HCC) from 14 institutes throughout Japan were retrospectively analyzed. The response was evaluated using the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1, and AEs were recorded according to the Common Terminology Criteria for AEs (CTCAE) version 5.0. Results: Median overall survival (OS) in the total cohort was 7.5 months (m). Median OS was 8.8 m in patients who were administered ramucirumab as a second-line treatment, while it was 7.3 m in third- or later-line treatment. Progression-free survival rates in the second- and third- or later-line therapies were 3.2 m and 3.2 m, respectively. The disease control rate (DCR) in the study was 43%. There were no statistically significant differences in DCR between the treatment courses. Regarding adverse events (AEs), the development of ascites was observed significantly more frequently in modified albumin–bilirubin (mALBI) 2b/3 patients than in mALBI 1/2a patients (54.5% vs. 25.0%, p = 0.03). Conclusions: Ramucirumab is useful as a second-line therapy and feasible as a third- or later-line treatment for HCC.
1. Introduction
The treatment of hepatocellular carcinoma (HCC) has seen rapid development [1]. In the past few years, first-line therapies [2], as well as several second-line treatments, have been newly introduced [3]. One of the second-line agents is ramucirumab, which is a human monoclonal antivascular endothelial growth factor receptor-2 antibody. In the REACH trial, ramucirumab initially showed its efficacy in a subgroup of HCC patients who have high α-fetoprotein (AFP) levels [4]. Later, the REACH-2 trial [5] was conducted as the second-line setting after sorafenib, enrolling only patients with AFP levels of ≥400 ng/mL. Consequently, the REACH-2 study showed that ramucirumab significantly prolonged survival when compared with placebo. Following these results, ramucirumab was approved for second-line treatment for HCC patients with AFP levels of ≥400 ng/mL.
Presently, a combination of atezolizumab plus bevacizumab is the first choice of first-line treatment [6]. For patients for whom this treatment can not apply, sorafenib [7] and lenvatinib [8] are chosen as the first-line molecularly targeted agents (MTA). As second-line treatments, regorafenib [9] and cabozantinib [10] are available besides ramucirumab, whereas both sorafenib and lenvatinib, which were not administered as the first line, are also being used. Although the evidence was initially presented as the second-line treatment after sorafenib, these drugs are chosen as the second- or further-line treatment after lenvatinib. In addition, ramucirumab was reported not to impact liver function negatively [11]. Given this situation, there are still many questions to be answered with real-world clinical data for patients who experienced two or more systemic therapies, whose liver function has deteriorated, or who have comorbidities. The real-world data of systemic therapy have been highlighted and revealed many significant findings that could not be clarified in clinical trials [12,13,14,15,16]. The present study aimed to determine the optimal sequential treatment for HCC patients and the treatment strategy of ramucirumab treatment.
2. Materials and Methods
2.1. Patients
Patients treated with ramucirumab for intermediate or advanced stage HCC from 14 hospitals throughout Japan were identified from the clinical database. All patients had received at least one MTA treatment before receiving ramucirumab. Patients who were administered ramucirumab for at least two cycles were analyzed. We retrospectively collected baseline characteristics and clinical data during ramucirumab treatment, including information on any prior treatment course, the Eastern Cooperative Oncology Group performance status (ECOG-PS), Barcelona Clinic for Liver Cancer (BCLC) stage, tumor burden, and hepatic reserve evaluated by Child–Pugh grade, as well as albumin–bilirubin (ALBI) grade. Baseline AFP was ≥400 ng/mL in all the patients. Written informed consent was received from each patient for the ramucirumab treatment; however, the requirement for informed consent for the study was waived because of its retrospective nature. This study was conducted in accordance with the Declaration of Helsinki, and the institutional ethical committee of Musashino Red Cross Hospital approved the study protocol (approval number: 2039).
2.2. Treatment Procedures
Ramucirumab (8 mg/kg) was administered intravenously every two weeks. Dose reduction and treatment discontinuation of ramucirumab was decided per the information prescribed by the manufacturer. An initial dose modification was allowed when the attending physicians deemed it necessary for any appropriate reason, such as proteinuria, due to prior therapy and/or patient comorbidity.
2.3. Outcomes
Overall survival (OS) was defined as the time from the first administration of ramucirumab to the date when the patient died due to any cause or the date of the last visit. The initial imaging assessment was performed at 8 ± 2 weeks after the initiation of ramucirumab administration, followed by every 2–3 months. The response was evaluated using the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 [17]. Progression-free survival (PFS) was defined as the time from the first drug administration to the date when the progression or any cause of death was recorded or the date of the last radiological evaluation. AEs were recorded according to the Common Terminology Criteria for AEs (CTCAE) version 5.0. The results were analyzed in total enrolled patients, and subgroups were stratified by the treatment course of ramucirumab or liver function reserve.
2.4. Statistical Analysis
Continuous variables are provided as medians with interquartile ranges and compared using the Mann–Whitney U test or Kruskal–Wallis test. Categorical variables are given as numbers and percentages and compared using Fisher’s exact test. Survival data were analyzed using the Kaplanؘ–Meier method and compared using a log-rank test. A probability (p) value of <0.05 was considered statistically significant. All statistical analyses were conducted using the graphical interface of R (EZR) [18].
3. Results
3.1. Patients
Table 1 shows the baseline characteristics of the patients enrolled in the present study. A total of 79 patients with a median age of 71 from 14 institutes across Japan were enrolled in this study. Among these, 17 (21.5%) were females, and hepatitis C was the most frequent cause of background liver disease. Regarding the treatment course, ramucirumab was administered as the second-, third-, fourth-, and fifth-line treatments in 40 (50.6%), 13 (16.4%), 24 (30.3%), and 2 (2.5%) patients, respectively. Among 40 patients who were administered ramucirumab as second-line therapy, 34 had received lenvatinib as the first-line treatment, while 4 had received sorafenib. Forty-four patients (55.7%) were classified as ECOG-PS 1, whereas only two patients were ECOG-PS 2. Hepatic reserve at Child–Pugh grade A was seen in 44 (55.7%) patients, and the Child–Pugh score was ≤7 in 63 (79.7%) patients. Modified albumin–bilirubin (mALBI) grade 1 or 2a was seen in 24 (30.4%). Overall, 40 (50.6%) patients were classified as BCLC stage C, 39 (49.4%) of whom had extrahepatic spread, and 27 (34.2%) had a major vascular invasion. The median observational time was 6.3 months.

Table 1.
Baseline characteristics.
Regarding previous treatment before ramucirumab, 53 (67%) patients had received lenvatinib as the first-line therapy, whereas sorafenib had been administered as first-line therapy for 22 (28%) patients. Lenvatinib was administered at any line of treatment in 73 patients before ramucirumab. Atezolizumab plus bevacizumab combination had administered in six patients before ramucirumab. In Table 2, the data on treatment history before ramucirumab therapy are summarized.
Table 2.
Treatment history according to the number of regimens before ramucirumab.
3.2. Overall Survival (OS)
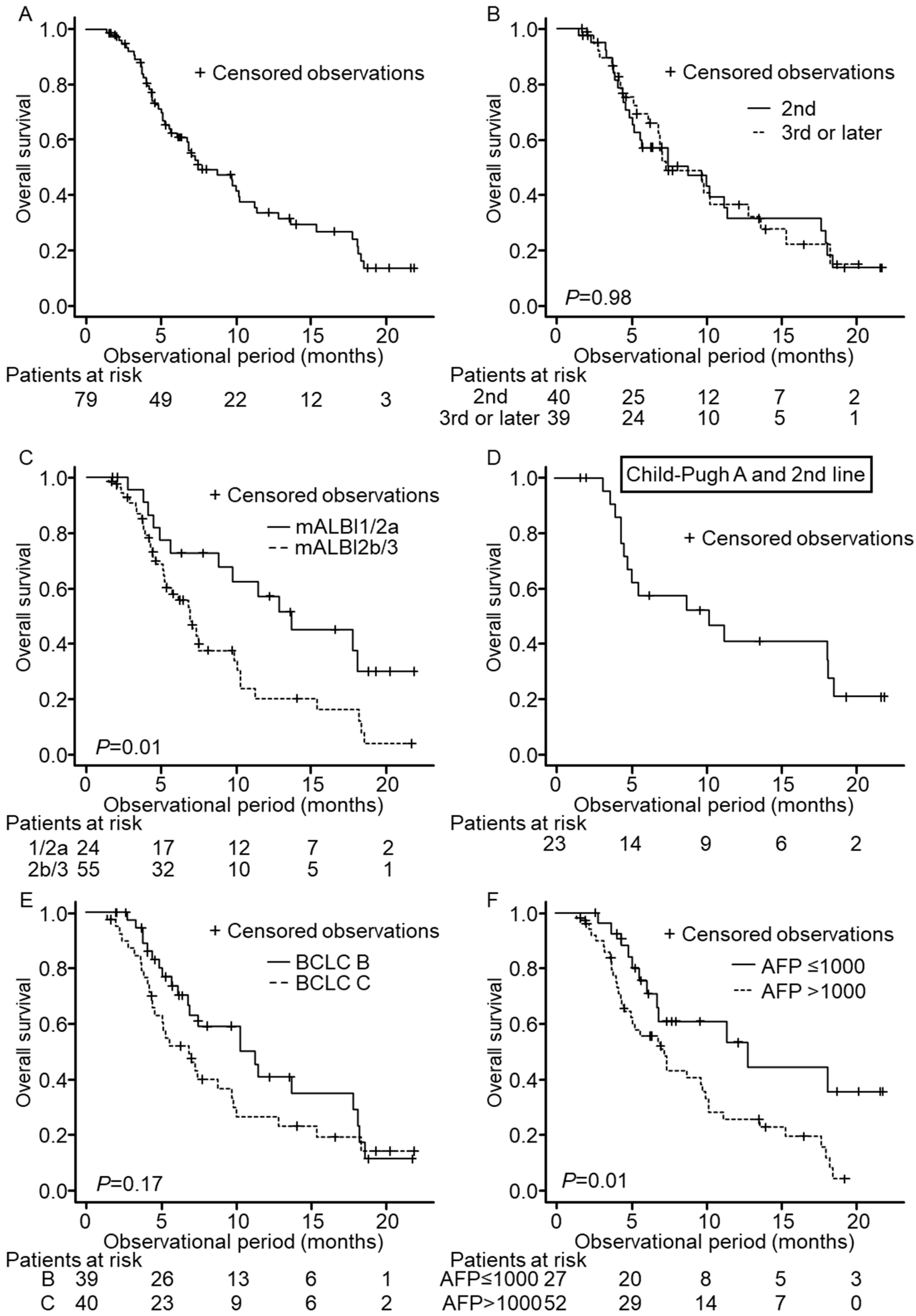
In total, 51 patients out of 79 died during the follow-up period. The median overall survival (OS) was 7.5 months (Figure 1A). In terms of the treatment course, the OS of patients with second-line treatment patients was not significantly different from patients with third- or later-line treatment (median OS 8.8 months vs. 7.3 months, p = 0.98; Figure 1B). With regard to hepatic reserve, OS of Child–Pugh A patients (n = 44) tended to show longer survival than that of Child–Pugh B/C patients (n = 35) (median OS 10.3 months vs. 6.7 months, p = 0.06). OS of mALBI grade 1/2a patients was significantly longer than that of mALBI 2b/3 patients (median OS 13.6 months vs. 6.9 months, p = 0.01, Figure 1C). To compare with the REACH-2 trial, we analyzed 23 patients who were Child–Pugh A at baseline and administered ramucirumab as second-line treatment. The median OS of this subgroup was 10.3 months (Figure 1D), which was comparable to the median OS of the REACH-2 trial, with 8.5 months. According to BCLC stage (Figure 1E), OS was not significantly different between BCLC stage B and C (11.2 months vs. 6.9 months, p = 0.17), whereas OS whose baseline AFP > 1000 ng/mL showed significantly shorter survival than those with baseline AFP ≤ 1000 ng/mL (Figure 1F, 12.8 months vs. 7.3 months, p = 0.01).
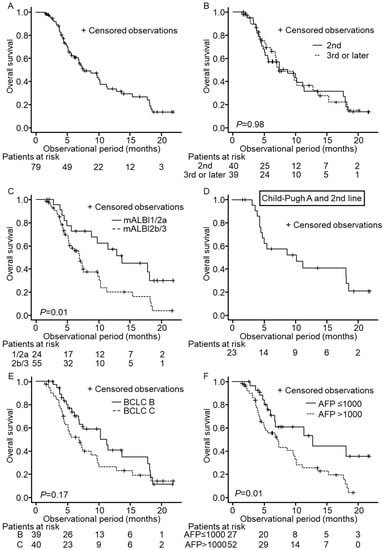
Figure 1.
Overall survival (OS) of patients enrolled in this study. Censored observations are marked as + in each Kaplan–Meier curve. Each panel shows OS in the entire cohort (A), OS according to the treatment course of ramucirumab (B), mALBI grade (C), BCLC stage (E), and AFP level (F), respectively. Panel (D) shows OS in patients of 2nd-line treatment with Child–Pugh A.
3.3. Progression-Free Survival (PFS) and Radiological Response
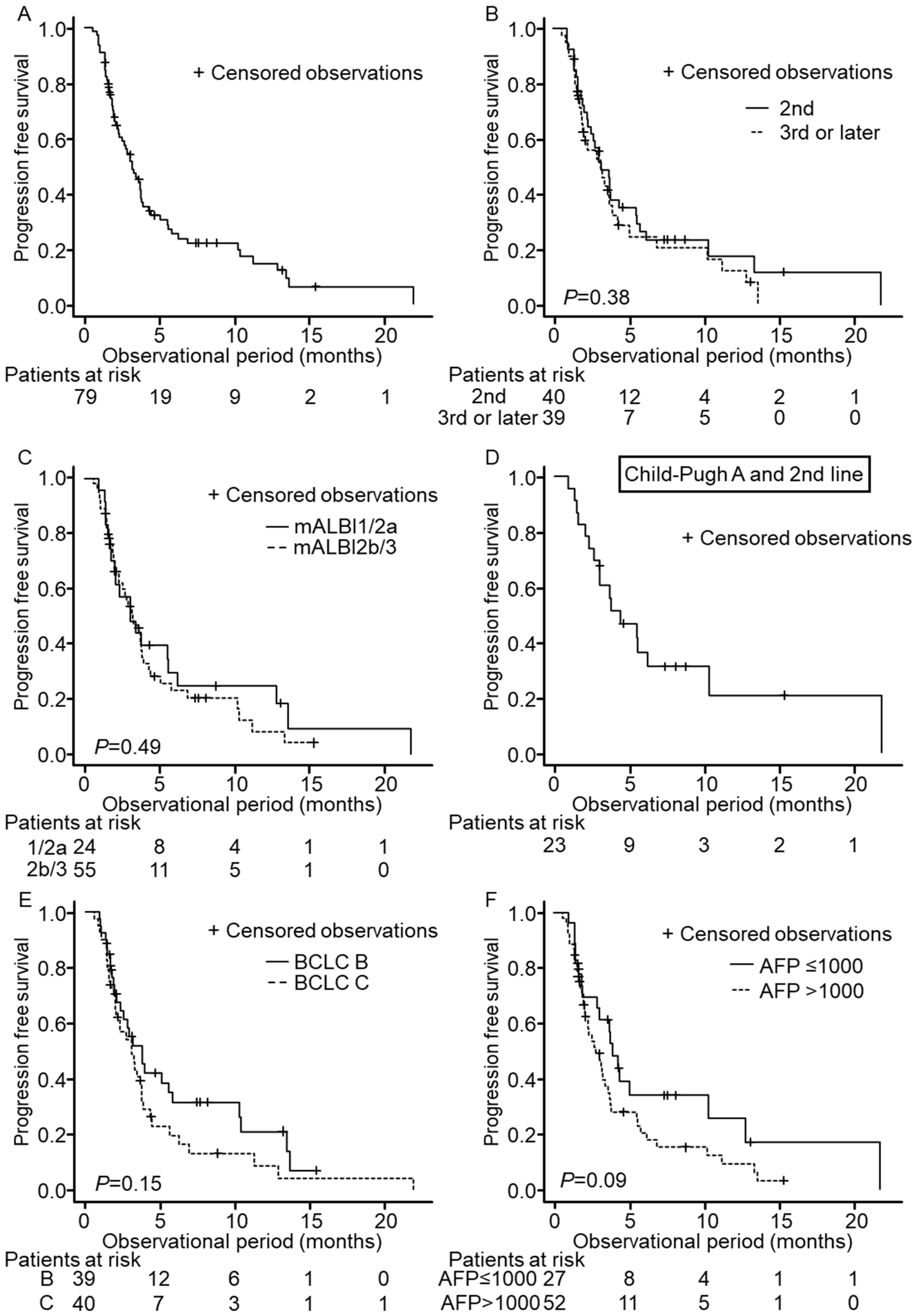
PFS was 3.2 months in all patients (Figure 2A), and no significant difference was seen between PFS in second- and third- or later-line treatment (median PFS 3.2 m vs. 3.2 m, p = 0.38, Figure 2B). Furthermore, no significant difference was observed between mALBI grade 1/2a and 2b/3, BCLC stage B and C, or baseline AFPs ≤ 1000 ng/mL and >1000 ng/mL (Figure 2C,E,F). Median PFS of Child–Pugh A patients who were administered ramucirumab as second-line was 4.4 months (Figure 2D). Again, this result was comparable to the median PFS of the REACH-2 trial, with 2.8 months. Among the enrolled patients, 65 patients underwent at least 1 radiological assessment, and we observed radiological progression in 41 patients during the follow-up period. Best response as identified by RECIST ver. 1.1 was PR in 1 patient and SD in 27 patients, and the disease control rate (DCR) was 43.0%. DCR was not significantly different between second-line treatment and third- or later-line treatment.
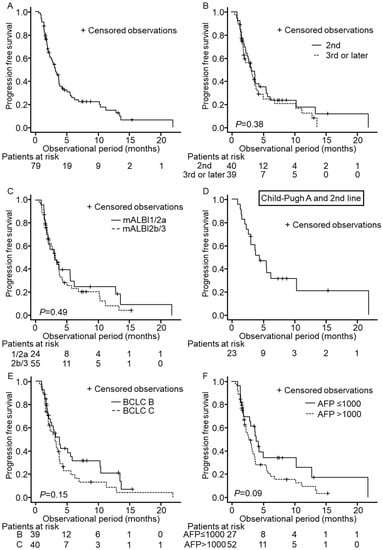
Figure 2.
Progression-free survival (PFS) of patients enrolled in this study. Censored observations are marked as + in each Kaplan–Meier curve. Panel (A) shows PFS in the entire cohort. PFS according to the treatment course of ramucirumab (B), mALBI grade (C), BCLC stage (E), and AFP level (F) are presented. Panel (D) shows PFS in patients of 2nd-line treatment with Child–Pugh A.
3.4. Adverse Events (AEs)
An AE at any grade was observed in 73 (92.4%) patients. A grade 3 AE was recorded in 20 (25.3%) patients, and 16 (20.2%) patients discontinued ramucirumab due to a treatment-related AE. Table 3 lists all the AE observed in the present study. The most frequent AE was hypertension, followed by fatigue and appetite loss, most of which were grade 1 or 2. The development or worsening of ascites was observed in 36 patients, and 8 of those did not undergo any additional treatment, whereas 28 were managed by diuretics. The most frequent grade 3 AE was peripheral edema in nine patients, followed by ascites in four patients. Neither the frequency of any grade AE nor grade 3 AE was significantly different between the treatment courses. There was no statistically significant difference in the frequency of any grade AE or any grade 3 AE between Child–Pugh A and Child–Pugh B/C patients. However, peripheral edema, ascites, and diarrhea were significantly more frequent in Child–Pugh B/C patients than in Child–Pugh A patients (peripheral edema; 57.1% vs. 31.8%, p = 0.04, ascites; 68.6% vs. 27.3%, p < 0.001, diarrhea; 25.7% vs. 4.5%, p = 0.009). Ascites was significantly more frequent in mALBI 2b/3 patients than in mALBI 1/2a patients (54.5% vs. 25.0%, p = 0.03).
Table 3.
Adverse events during ramucirumab treatment.
3.5. Change in AFP during Ramucirumab Treatment and Subsequent Treatment after Ramucirumab
During ramucirumab therapy, we observed AFP dynamics in 72 patients. AFP decrease of over 20% at week four was seen in nine patients, while AFP increased by less than 20% in 19 patients. Patients without over 20% increase in AFP at week 4 showed significantly longer PFS than those with over 20% increase (median PFS 3.8 vs. 2.3 months, p = 0.02). Furthermore, 63 patients were followed up after ramucirumab. Thirty-five (55.6%) received subsequent treatment, including 19 patients who received systemic treatment and seven patients who received transarterial chemoembolization (TACE). Patients who received subsequent treatment after radiological progression had longer survival than those who did not (10.2 months vs. 6.8 months, p = 0.005). Patients with baseline mALBI grade 1/2a had a significantly higher probability of subsequent treatment than patients with mALBI 2b/3 (83.3% vs. 44.4%, p = 0.006).
4. Discussion
The present study provides real-life data on ramucirumab-treated patients, including those who had received two or more MTA treatments before. Our data also demonstrated that ramucirumab treatment was effective and safe for patients who had received lenvatinib or other MTAs. PFS was consistent through treatment lines, mALBI grade, BCLC stage, and AFP level. In patients with a deteriorated liver function such as Child–Pugh B or mALBI 2b/3, several AEs were more frequent than those whose liver function was preserved. Therefore, AE monitoring and management are essential in Child–Pugh B or mALBI 2b/3 patients. Our data suggest that ramucirumab treatment can expect consistent PFS in a wide range of patients. After the approval of atezolizumab and bevacizumab combination therapy, MTAs sequential therapy has become critical for HCC patients [19,20,21,22,23]. There are still clinical questions such as optimal sequential usage of available systemic treatments.
REACH and REACH-2 trials were conducted in the second-line setting after sorafenib for Child–Pugh A patients; however, there was little evidence about the efficacy and safety of ramucirumab for patients after lenvatinib or multiple lines of treatment. In our study, 85% of second-line patients, and 90% of all patients had a treatment history of lenvatinib. Regarding the efficacy, the OS of Child–Pugh A patients treated with second-line ramucirumab therapy was comparable to the result of the REACH-2 trial. Kuzuya et al. first reported on the outcome of ramucirumab treatment after lenvatinib and provided similar observations in 12 patients [24]. Hiraoka et al. reported the efficacy of ramucirumab treatment as second- to fourth-line after lenvatinib in 28 patients [25], which provided evidence of ramucirumab in third- or later-line treatment. Our data confirmed these reports in a larger cohort. Regarding safety, the frequency of any grade AE and grade 3 AE in our cohort was not significantly different from that of the REACH or the REACH-2 trial, suggesting that the safety profile would not vary in patients who had received lenvatinib. Kasuya et al. also reported no serious AE in seven patients who received ramucirumab as the second or third line after lenvatinib [26]. These results suggest that ramucirumab can be used safely even after lenvatinib.
The subanalyses of the clinical trial clarified the survival benefits of ramucirumab in the elderly [27] and the Japanese subgroup [28,29]. In contrast, we focused on the efficacy of ramucirumab as the third- or later-line therapy. Our data revealed no statistical differences between the second- and third- or later-line therapy in the OS or PFS. OS in our cohort was shorter than that of the REACH-2 trial. This result could be attributed to the baseline hepatic reserve since the REACH-2 trial only included Child–Pugh A patients, while the cohort in the present study comprised 38.2% Child–Pugh B patients. The survival benefit for Child–Pugh B patients was also marginal in an exploratory analysis of the REACH trial [30]. It should be noted that the evidence of clinical benefit of ramucirumab for Child–Pugh B patients is still not enough. Baseline hepatic reserve is a critical factor for the treatment strategy of unresectable HCC patients [31,32] and a predictive factor for patients whether they can be a candidate for next-line treatment [33,34]. In the present study, subsequent treatment was significantly more frequent in mALBI 1/2a patients. Therefore, treatment strategy during preserved liver function is essential. Meanwhile, the PFS was consistent regardless of treatment history, BCLC stage, and mALBI grade. In terms of AE, the development or worsening of ascites and peripheral edema was significantly more common in Child–Pugh B/C patients. In a recent study, Kudo et al. reported that ascites were not unfavorable AE in ramucirumab treatment [35]. For Child–Pugh B/C patients, careful observation and appropriate management for ascites should be considered.
Our study has several limitations. The retrospective study design and the short duration of the follow-up period are major limitations. The median observational time of this study was relatively short at 6.3 months; therefore, analyses after prolonged follow-up should be considered. Additionally, because of the study design, which relied on data collection from many institutions, detailed data are lacking. A larger cohort with a longer follow-up period and detailed data are needed to confirm and further elucidate our results.
5. Conclusions
In conclusion, besides the second-line therapy, ramucirumab treatment was feasible as a third- or later-line treatment for hepatocellular carcinoma. The PFS using ramucirumab in the real-world setting, including patients administered ramucirumab after lenvatinib, was comparable with the PFS observed in the REACH-2 trial.
Author Contributions
Conceptualization, Japanese Red Cross Liver Study Group, Y.Y. and M.K. (Masayuki Kurosaki); methodology, Y.Y.; software, Y.Y.; validation, M.K. (Masayuki Kurosaki); formal analysis, Y.Y. and M.K. (Masayuki Kurosaki); investigation, Y.Y., Y.H., C.H., M.A., C.O., K.J., H.O., T.T. (Toshifumi Tada), S.N., K.F., H.K., K.T. (Keiji Tsuji), Y.K., T.A., T.T. (Takashi Tamada), Y.U., M.K. (Masahiko Kondo) and A.M.; resources, N.I.; data curation, Y.Y.; writing—original draft preparation, Y.Y.; writing—review and editing, M.K. (Masayuki Kurosaki) and K.T. (Kaoru Tsuchiya); visualization, Y.Y.; supervision, N.I.; project administration, N.I.; funding acquisition, M.K. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by a grant-in-aid from the Japan Agency for Medical Research and Development (grant number: JP20fk0210067h0001, URL: https://www.amed.go.jp/en/index.html (accessed on 15 June 2022)).
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board (approval number: 2039).
Informed Consent Statement
Written informed consent was received from each patient for the treatment, and the requirement for informed consent for the study was waived because of its retrospective nature.
Data Availability Statement
The datasets supporting the study conclusions are included within this manuscript.
Acknowledgments
We express our sincere thanks to all the patients and their families who participated in this study.
Conflicts of Interest
Y.Y. received a grant from the Uehara Memorial Foundation and Miyakawa Memorial Research Foundation. Y.Y. received a speaker’s bureau from Eli Lilly, Chugai, Eisai, and Takeda. M.K. (Masayuki Kurosaki) received speaker’s bureau from Gilead, AbbVie, Bayer, Eli Lilly, Chugai, Eisai, and Otsuka. K.T. received speaker’s bureau from Bayer, Chugai, Takeda, Eisai, and Eli Lilly. N.I. received speaker’s bureau from Bayer, Chugai, Eli Lilly, Eisai, and Takeda. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Abbreviations
| Hepatocellular carcinoma | HCC |
| α-Fetoprotein | AFP |
| molecularly targeted agents | MTA |
| Adverse events | AEs |
| Eastern Cooperative Oncology Group performance status | ECOG-PS |
| Barcelona Clinic for Liver Cancer | BCLC |
| Modified albumin–bilirubin grade | mALBI grade |
| Overall survival | OS |
| Progression-free survival | PFS |
| Response Evaluation Criteria in Solid Tumors | RECIST |
| The Common Terminology Criteria for AEs | CTCAE |
| Disease control rate | DCR |
References
- Faivre, S.; Rimassa, L.; Finn, R.S. Molecular therapies for HCC: Looking outside the box. J. Hepatol. 2020, 72, 342–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Rimassa, L.; Worns, M.A. Navigating the new landscape of second-line treatment in advanced hepatocellular carcinoma. Liver Int. 2020, 40, 1800–1811. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.X.; Park, J.O.; Ryoo, B.Y.; Yen, C.J.; Poon, R.; Pastorelli, D.; Blanc, J.F.; Chung, H.C.; Baron, A.D.; Pfiffer, T.E.; et al. Ramucirumab versus placebo as second-line treatment in patients with advanced hepatocellular carcinoma following first-line therapy with sorafenib (REACH): A randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 2015, 16, 859–870. [Google Scholar] [CrossRef]
- Zhu, A.X.; Kang, Y.K.; Yen, C.J.; Finn, R.S.; Galle, P.R.; Llovet, J.M.; Assenat, E.; Brandi, G.; Pracht, M.; Lim, H.Y.; et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased alpha-fetoprotein concentrations (REACH-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 282–296. [Google Scholar] [CrossRef]
- Sonbol, M.B.; Riaz, I.B.; Naqvi, S.A.A.; Almquist, D.R.; Mina, S.; Almasri, J.; Shah, S.; Almader-Douglas, D.; Uson Junior, P.L.S.; Mahipal, A.; et al. Systemic Therapy and Sequencing Options in Advanced Hepatocellular Carcinoma: A Systematic Review and Network Meta-analysis. JAMA Oncol. 2020, 6, e204930. [Google Scholar] [CrossRef]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [Green Version]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [Green Version]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.L.; El-Khoueiry, A.B.; Rimassa, L.; Ryoo, B.Y.; Cicin, I.; Merle, P.; Chen, Y.; Park, J.W.; et al. Cabozantinib in Patients with Advanced and Progressing Hepatocellular Carcinoma. N. Engl. J. Med. 2018, 379, 54–63. [Google Scholar] [CrossRef]
- Kudo, M.; Galle, P.R.; Brandi, G.; Kang, Y.K.; Yen, C.J.; Finn, R.S.; Llovet, J.M.; Assenat, E.; Merle, P.; Chan, S.L.; et al. Effect of ramucirumab on ALBI grade in patients with advanced HCC: Results from REACH and REACH-2. JHEP Rep. 2021, 3, 100215. [Google Scholar] [CrossRef] [PubMed]
- Ogushi, K.; Chuma, M.; Uojima, H.; Hidaka, H.; Numata, K.; Kobayashi, S.; Hirose, S.; Hattori, N.; Fujikawa, T.; Nakazawa, T.; et al. Safety and Efficacy of Lenvatinib Treatment in Child-Pugh A and B Patients with Unresectable Hepatocellular Carcinoma in Clinical Practice: A Multicenter Analysis. Clin. Exp. Gastroenterol. 2020, 13, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Maruta, S.; Ogasawara, S.; Ooka, Y.; Obu, M.; Inoue, M.; Itokawa, N.; Haga, Y.; Seki, A.; Okabe, S.; Azemoto, R.; et al. Potential of Lenvatinib for an Expanded Indication from the REFLECT Trial in Patients with Advanced Hepatocellular Carcinoma. Liver Cancer 2020, 9, 382–396. [Google Scholar] [CrossRef]
- Sho, T.; Suda, G.; Ogawa, K.; Shigesawa, T.; Suzuki, K.; Nakamura, A.; Ohara, M.; Umemura, M.; Kawagishi, N.; Natsuizaka, M.; et al. Lenvatinib in patients with unresectable hepatocellular carcinoma who do not meet the REFLECT trial eligibility criteria. Hepatol. Res. 2020, 50, 966–977. [Google Scholar] [CrossRef] [PubMed]
- Tsuchiya, K.; Kurosaki, M.; Sakamoto, A.; Marusawa, H.; Kojima, Y.; Hasebe, C.; Arai, H.; Joko, K.; Kondo, M.; Tsuji, K.; et al. The Real-World Data in Japanese Patients with Unresectable Hepatocellular Carcinoma Treated with Lenvatinib from a Nationwide Multicenter Study. Cancers 2021, 13, 2608. [Google Scholar] [CrossRef] [PubMed]
- Kirino, S.; Tsuchiya, K.; Kurosaki, M.; Kaneko, S.; Inada, K.; Yamashita, K.; Osawa, L.; Hayakawa, Y.; Sekiguchi, S.; Okada, M.; et al. Relative dose intensity over the first four weeks of lenvatinib therapy is a factor of favorable response and overall survival in patients with unresectable hepatocellular carcinoma. PLoS ONE 2020, 15, e0231828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Takeda, H.; Nishijima, N.; Nasu, A.; Komekado, H.; Kita, R.; Kimura, T.; Kudo, M.; Osaki, Y. Long-term antitumor effect of lenvatinib on unresectable hepatocellular carcinoma with portal vein invasion. Hepatol. Res. 2019, 49, 594–599. [Google Scholar] [CrossRef]
- Hatanaka, T.; Kakizaki, S.; Nagashima, T.; Namikawa, M.; Tojima, H.; Shimada, Y.; Takizawa, D.; Naganuma, A.; Arai, H.; Sato, K.; et al. Analyses of objective response rate, progression-free survival, and adverse events in hepatocellular carcinoma patients treated with lenvatinib: A multicenter retrospective study. Hepatol. Res. 2020, 50, 382–395. [Google Scholar] [CrossRef]
- Chuma, M.; Uojima, H.; Hiraoka, A.; Kobayashi, S.; Toyoda, H.; Tada, T.; Hidaka, H.; Iwabuchi, S.; Numata, K.; Itobayashi, E.; et al. Analysis of efficacy of lenvatinib treatment in highly advanced hepatocellular carcinoma with tumor thrombus in the main trunk of the portal vein or tumor with more than 50% liver occupation: A multicenter analysis. Hepatol. Res. 2021, 51, 201–215. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Kumada, T.; Hatanaka, T.; Tada, T.; Kariyama, K.; Tani, J.; Fukunishi, S.; Atsukawa, M.; Hirooka, M.; Tsuji, K.; et al. Therapeutic efficacy of lenvatinib as third line treatment following regorafenib for unresectable hepatocellular carcinoma progression. Hepatol. Res. 2021, 51, 880–889. [Google Scholar] [CrossRef] [PubMed]
- Tomonari, T.; Sato, Y.; Tani, J.; Hirose, A.; Ogawa, C.; Morishita, A.; Tanaka, H.; Tanaka, T.; Taniguchi, T.; Okamoto, K.; et al. Comparison of therapeutic outcomes of sorafenib and lenvatinib as primary treatments for hepatocellular carcinoma with a focus on molecular-targeted agent sequential therapy: A propensity score-matched analysis. Hepatol. Res. 2021, 51, 472–481. [Google Scholar] [CrossRef] [PubMed]
- Kuzuya, T.; Ishigami, M.; Ito, T.; Ishizu, Y.; Honda, T.; Ishikawa, T.; Fujishiro, M. Initial Experience of Ramucirumab Treatment After Lenvatinib Failure for Patients With Advanced Hepatocellular Carcinoma. Anticancer Res. 2020, 40, 2089–2093. [Google Scholar] [CrossRef]
- Hiraoka, A.; Kumada, T.; Tada, T.; Ogawa, C.; Tani, J.; Fukunishi, S.; Atsukawa, M.; Hirooka, M.; Tsuji, K.; Ishikawa, T.; et al. Therapeutic efficacy of ramucirumab after lenvatinib for post-progression treatment of unresectable hepatocellular carcinoma. Gastroenterol. Rep. 2021, 9, 133–138. [Google Scholar] [CrossRef]
- Kasuya, K.; Kawamura, Y.; Kobayashi, M.; Shindoh, J.; Kobayashi, Y.; Kajiwara, A.; Iritani, S.; Fujiyama, S.; Hosaka, T.; Saitoh, S.; et al. Efficacy and Safety of Ramucirumab in Patients with Unresectable Hepatocellular Carcinoma with Progression after Treatment with Lenvatinib. Intern. Med. 2021, 60, 345–351. [Google Scholar] [CrossRef]
- Kudo, M.; Galle, P.R.; Llovet, J.M.; Finn, R.S.; Vogel, A.; Motomura, K.; Assenat, E.; Merle, P.; Brandi, G.; Daniele, B.; et al. Ramucirumab in elderly patients with hepatocellular carcinoma and elevated alpha-fetoprotein after sorafenib in REACH and REACH-2. Liver Int. 2020, 40, 2008–2020. [Google Scholar] [CrossRef]
- Kudo, M.; Hatano, E.; Ohkawa, S.; Fujii, H.; Masumoto, A.; Furuse, J.; Wada, Y.; Ishii, H.; Obi, S.; Kaneko, S.; et al. Ramucirumab as second-line treatment in patients with advanced hepatocellular carcinoma: Japanese subgroup analysis of the REACH trial. J. Gastroenterol. 2017, 52, 494–503. [Google Scholar] [CrossRef]
- Kudo, M.; Okusaka, T.; Motomura, K.; Ohno, I.; Morimoto, M.; Seo, S.; Wada, Y.; Sato, S.; Yamashita, T.; Furukawa, M.; et al. Ramucirumab after prior sorafenib in patients with advanced hepatocellular carcinoma and elevated alpha-fetoprotein: Japanese subgroup analysis of the REACH-2 trial. J. Gastroenterol. 2020, 55, 627–639. [Google Scholar] [CrossRef] [Green Version]
- Zhu, A.X.; Baron, A.D.; Malfertheiner, P.; Kudo, M.; Kawazoe, S.; Pezet, D.; Weissinger, F.; Brandi, G.; Barone, C.A.; Okusaka, T.; et al. Ramucirumab as Second-Line Treatment in Patients With Advanced Hepatocellular Carcinoma: Analysis of REACH Trial Results by Child-Pugh Score. JAMA Oncol. 2017, 3, 235–243. [Google Scholar] [CrossRef]
- Kaneko, S.; Tsuchiya, K.; Yasui, Y.; Inada, K.; Kirino, S.; Yamashita, K.; Osawa, L.; Hayakawa, Y.; Sekiguchi, S.; Higuchi, M.; et al. Strategy for advanced hepatocellular carcinoma based on liver function and portal vein tumor thrombosis. Hepatol. Res. 2020, 50, 1375–1385. [Google Scholar] [CrossRef] [PubMed]
- Terashima, T.; Yamashita, T.; Takata, N.; Toyama, T.; Shimakami, T.; Takatori, H.; Arai, K.; Kawaguchi, K.; Kitamura, K.; Yamashita, T.; et al. Comparative analysis of liver functional reserve during lenvatinib and sorafenib for advanced hepatocellular carcinoma. Hepatol. Res. 2020, 50, 871–884. [Google Scholar] [CrossRef] [PubMed]
- Uchikawa, S.; Kawaoka, T.; Aikata, H.; Kodama, K.; Nishida, Y.; Inagaki, Y.; Hatooka, M.; Morio, K.; Nakahara, T.; Murakami, E.; et al. Clinical outcomes of sorafenib treatment failure for advanced hepatocellular carcinoma and candidates for regorafenib treatment in real-world practice. Hepatol. Res. 2018, 48, 814–820. [Google Scholar] [CrossRef] [PubMed]
- Kuzuya, T.; Ishigami, M.; Ito, T.; Ishizu, Y.; Honda, T.; Ishikawa, T.; Hirooka, Y.; Fujishiro, M. Clinical characteristics and outcomes of candidates for second-line therapy, including regorafenib and ramucirumab, for advanced hepatocellular carcinoma after sorafenib treatment. Hepatol. Res. 2019, 49, 1054–1065. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Ikeda, M.; Galle, P.R.; Yamashita, T.; Finn, R.S.; Liang, K.; Wang, C.; Sakaguchi, S.; Abada, P.; Widau, R.C.; et al. Ramucirumab in patients with advanced hepatocellular carcinoma and elevated alpha-fetoprotein: Outcomes by treatment-emergent ascites. Hepatol. Res. 2021, 51, 715–721. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).