Simple Summary
HER2-low breast cancer (BC) accounts for more than half of breast cancer patients. Anti-HER2 therapy has been ineffective in HER2-low BC, for which palliative chemotherapy is the main treatment modality. The definitive efficacy of T-Dxd in HER2-low BC breaks previous treatment strategies, which will redefine HER2-low and thus reshape anti-HER2 therapy. This review summarizes detection technologies and novel agents for HER2-low BC, and explores their possible role in future clinics, to provide ideas for the diagnosis and treatment of HER2-low BC.
Abstract
HER2-low breast cancer (BC) has a poor prognosis, making the development of more suitable treatment an unmet clinical need. While chemotherapy is the main method of treatment for HER2-low BC, not all patients benefit from it. Antineoplastic therapy without chemotherapy has shown promise in clinical trials and is being explored further. As quantitative detection techniques become more advanced, they assist in better defining the expression level of HER2 and in guiding the development of targeted therapies, which include directly targeting HER2 receptors on the cell surface, targeting HER2-related intracellular signaling pathways and targeting the immune microenvironment. A new anti-HER2 antibody-drug conjugate called T-DM1 has been successfully tested and found to be highly effective in clinical trials. With this progress, it could eventually be transformed from a disease without a defined therapeutic target into a disease with a defined therapeutic molecular target. Furthermore, efforts are being made to compare the sequencing and combination of chemotherapy, endocrine therapy, and HER2-targeted therapy to improve prognosis to customize the subtype of HER2 low expression precision treatment regimens. In this review, we summarize the current and upcoming treatment strategies, to achieve accurate management of HER2-low BC.
1. Introduction
HER2-low breast cancer (BC), defined as HER2 immunohistochemistry (IHC) 2+ and in situ hybridization (ISH)-negative or IHC1+, accounts for 40–50% of breast cancers [1,2]. Genomics analysis has shown HER2-low BC to be a heterogeneous disease [3,4]. While it is not known how the HER2-low subtype causes cancer, most patients have poor prognostic factors, such as larger tumor sizes, higher histological grades, and more regional lymph node involvement [2,5,6,7,8,9,10].
Denkert et al. investigated 2310 HER2-negative BC patients receiving neoadjuvant chemotherapy, and found that approximately 60% of hormone receptor (HR) positive BC patients also had low HER2 expression compared to 33% of triple negative breast cancer (TNBC) patients [11]. Compared to HER2-0 BC, HER2-low BC showed distinctive molecular features. The divergent rates of germline changes for BRCA1/2 and other BC susceptibility genes differed in both cases. Upon comparison of PIK3CA and TP53 mutations, it was particularly evident that HER2-0 and HER2-low BC have distinctly different genetic origins, which implies that HER2-lowBC has the potential to become a biological entity [11].
Unfortunately, the low HER2 expression failed to provide clinical prognosis benefits. The available HER2-targeted therapies are inefficient in HER2-low BC, and treatment options are restricted after the initial treatment progression [12,13]. When classified as HER2-negative and treated with palliative chemotherapy [1], even if HER2-0 has more adverse tumor characteristics than HER2-low, clinical trials also show no difference in survival outcomes between the two [11,14,15,16], raising the question of whether HER2-low BC is overtreated or undertreated?
Recent advances in drug development have, however, changed the current view, indicating that HER2-low BC may benefit from anti-HER2 therapy [17,18,19]. Moreover, in a longitudinal study, the inconsistent rate of HER2 expression in patients with advanced or recurrent BC was as high as 38%, and more than a third of HER2-0 BC patients exhibited a trend of transformation to HER2-low BC in metastatic lesions [20]. The possibility of improving the treatment of HER2-low BC is of great clinical significance.
This review addresses the detection technology used for HER2 expression and discusses novel agents for HER2-low BC, in order to evaluate dosing regimens through clinical trials and propose ideas for the diagnosis and treatment of HER2-low BC.
2. Detection and Diagnosis of HER2
Regarding the positive impact of antibody–drug conjugates (ADCs), the most urgent challenge is to refine the definition of low HER2 expression. Indeed, the core content of the American Society of Clinical Oncology/College of American Pathologists (ASCO/CAP) guidelines for HER2 testing recommends screening HER2 overexpressing populations that can benefit from trastuzumab, with a relatively vague description of the borderline range for low HER2 expression [21].
IHC/ISH is the only standard technique currently applied to define HER2 expression. IHC involves a reaction between antigens and antibodies, resulting in protein coloration of the receptor. Since the detection value shows a linear dynamic range, it is difficult to make an accurate comparison of inferior or superior quantitative results [22]. ISH utilizes nucleic acid molecular probes to examine HER2 gene amplification status, but the signals are subject to photobleaching and fading over time [23].
Given the limitations of IHC/ISH, a new method is needed to improve the concordance of HER2-low detection. In this context, IHC combined with other quantitative techniques can be used to determine the initial HER2 level before ISH is used to exclude gene amplification, and HER2 can then be defined in the form of continuous numerical variables [17,24]. Ultimately, the HER2 threshold for producing antitumor activity will need to be analyzed and clinical trials employed to broaden the population for which HER2-targeted therapy may be effective.
2.1. HERmark ™
HERmark™ (Monogram Biosciences Inc., South San Francisco, CA, USA) allows for the accurate detection of HER2 expression in FFPE tissue samples, covering the majority of the dynamic range from 0 to 3+ [25]. It was found to be highly concordant with conventional HER2 assays (IHC and ISH), but HERmark™ is highly sensitive and specific [26,27,28]. As a reliable quantitative assessment tool, HERmark™, can be used for HER2-low BC, particularly in the case of ambiguous IHC test results [25]. Nonetheless, the core technical requirements have restricted its application to the central lab, limiting its use in a broader range of clinical settings.
2.2. Real-Time PCR
Real-time PCR (RT-PCR) allows for rapid and quantitative gene amplification analysis, giving ISH-like results and accurate quantification of HER2 levels in nonoverexpressing samples [29,30]. OncotypeDX and MammaTyper, derived from RT-PCR, can predict the outcome of chemotherapy and the possibility of recurrence in early HR-positive BC by analyzing mRNA extracted from FFPE samples [31,32]. Unfortunately, false-negative PCR results are often found, principally due to differences in the distribution of cells between different types of tumors, the mixing of noninvasive cancer components in the process of DNA/RNA extraction and the destruction of mRNA integrity in FFPE samples [33,34,35].
2.3. Multiplex Ligation-Dependent Probe Amplification
A modified quantitative technique for PCR, multiplex ligation-dependent probe amplification (MLPA), allows for the analysis of multiple gene amplifications and different portions of gene deletions [36]. When there is a discrepancy between IHC and ISH, MLPA may identify HER2-low but ISH+ cases [37]. Similar to RT-PCR, MLPA may also lack the ability to detect tumor heterogeneity due to differences in sample cuts. Copy-number changes detected by MLPA should be verified with other methods [38].
2.4. Time Resolved Fluorescence Resonance Energy Transfer
Time-resolved fluorescence resonance energy transfer (TR-FRET) quantifies the fluorescence signals emitted from energy transfers between two adjacent molecules to assess HER2 expression [39]. With the application of long-life fluorophore in TR-FRET, a delay can be introduced between the excitation pulse and the signal measurement window, thus eliminating the short-lived background autofluorescence in FFPE materials. It thus has higher sensitivity and lower false-positive rate and false-negative rates [40].
The clinical effectiveness of anti-HER2 therapy is the only way to asses HER2 detection. To confirm clinical benefits, new technologies must be compared to baseline testing. Once HER2 expression has been identified, selecting the most suitable treatment is the next step.
Anti-HER2 agents are gaining traction in the treatment of HER2-low BC, indicating HER2 expression as a possible therapeutic breakthrough. In terms of the drug effect mechanism, therapies related to HER2 can be divided into those targeting HER2 receptors on the cell surface, those targeting HER2-related intracellular signaling pathways and those targeting the immune microenvironment, as shown in Figure 1.
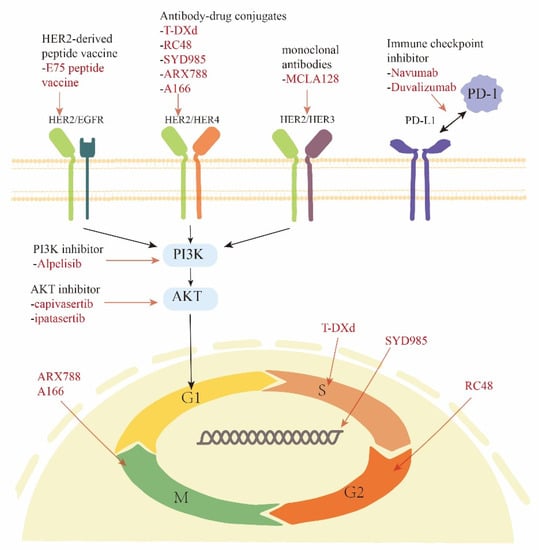
Figure 1.
HER2-related therapies for HER2-low breast cancer.
3. Therapy
3.1. Targeting HER2 Receptors on The Cell Surface
HER2-mediated tumorigenic signal production can be blocked through the competitive binding of exogenous HER2 antibodies to HER2 on the cell membrane surface, thereby delaying tumor progression [41]. A summary of novel drugs is provided in Table 1.

Table 1.
Summary of novel drugs targeted HER2 receptors in development for HER2-low BC.
3.1.1. ADC
An ADC consists of an antibody against a target antigen, cytotoxic drugs (payload) and cleavable or non-cleavable linkers [42] (Figure 2). ADCs exert cytocidal effects through targeting of surface antigens, internalization, enzymatic cleavage and drug release [43], resulting in high target selectivity and potent lethality in chemotherapy.
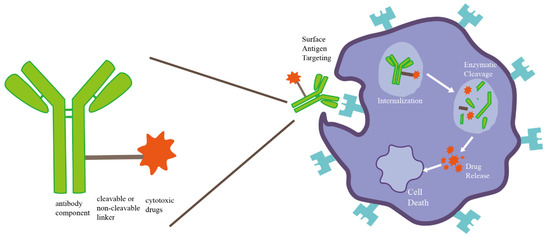
Figure 2.
Schematic diagram of ADC composition structure and drug mechanism.
Trastuzumab deruxtecan (T-DXd) is a broad-spectrum ADC composed of trastuzumab and a topoisomerase I inhibitor [44]. The payload of T-DXd proved to be highly membrane-permeable, exerting a powerful bystander effect [44]. Moreover, coupled with a drug structure different from that of the previously used paclitaxel and platinum-based chemotherapy for HER2-low BC, it resulted in a reduced risk of cross-resistance. As a corollary, it may become a good candidate for treatment of HER2-low BC.
The first clinical study (ClinicalTrials.gov identifier: NCT02564900) of T-DXd recruited 54 advanced HER2-low BC patients who progressed after standard treatment. Based upon the premise that the median number of treatment lines was up to 7.5, T-DXd performed spectacularly, with an objective remission rate (ORR) of 37.0% and a median duration of remission (DOR) of 10.4 months [45]. T-DXd was well-tolerated, with interstitial lung disease being the most prominent toxic reaction [46]. Excitingly, in the DESTINY-Breast04 phase III trial (ClinicalTrials.gov identifier: NCT03734029), significantly longer overall survival (OS) and progression-free survival (PFS) were seen in patients treated with T-DXd versus chemotherapy (OS, 23.9 vs. 17.9 months; hazard ratio (HR), 0.58; p = 0.001; PFS, 9.9 vs. 5.1 months; HR, 0.50; p < 0.001), leading to approval for T-Dxd in the NCCN and ASCO guidelines [47].
Additional efforts to broaden the applicability of T-DXd to a larger population, such as for HR+/HER2-low BC after the progress of endocrine therapy (ClinicalTrials.gov identifier: NCT04494425), are underway [48]. Moreover, combinations involving endocrine therapy, chemotherapy, immunotherapy and T-DXd are being explored (ClinicalTrials.gov identifier: NCT04556773) [49].
Other novel ADCs are RC48, SYD985 and A166, which use different cytotoxic drugs from T-Dxd (Table 2). They are currently in clinical development, showing encouraging results in phase I studies. In the C001CANCER phase I study (ClinicalTrials.gov identifier: NCT02881138) utilizing RC48, a significant improvement in OS and ORR was seen in an HER2-low cohort [50,51]. The SYD985.001 phase I study (ClinicalTrials.gov identifier: NCT02277717) evaluated all HER2-low BC patients who achieved a partial response (PR) with SYD985 [52]. In a phase I study (ClinicalTrials.gov identifier: NCT05311397), patients with relapsed or refractory solid cancers, including 51 with HER2-positive BC and 6 with HER2-low BC, received A166 [53]. To date, among the four evaluable patients with the HER2-low subtype, the disease control rate (DCR) for A166 was 75%, with manageable toxicity [54].
Table 2.
Structural characteristics of ADCs in ongoing clinical trials.
3.1.2. Monoclonal Antibodies
Despite the ineffectiveness of trastuzumab for HER2-low BC, the ability of ADCs to significantly improve prognosis has spurred interest in conventional targeted agents.
MGAH22 is an Fc-engineered anti-HER2 antibody [58]. In vitro, MGAH22 has similar antitumor effects to trastuzumab, while additionally improving and enhancing its antibody-dependent cell-mediated cytotoxicity (ADCC) [58].
A phase Ⅱ trial of MGAH22 (ClinicalTrials.gov identifier: NCT01828021) in patients with relapsed or refractory advanced BC, including HER2-low BC, has completed enrollment. The final results will be announced in the near future [59].
3.1.3. Bispecific Antibodies
HER2, an orphan receptor tyrosine kinase without a corresponding ligand, is often linked to EGFR, HER3 and HER4 [60]. Homogeneous or heterogeneous dimerization of HER2 rapidly activates downstream signaling cascades, thereby triggering tumor cell proliferation, migration, and invasion [61]. Bispecific antibodies (BsAbs) are single protein molecules that recognize two binding sites simultaneously, establishing an association between tumor cells and immune cells and blocking the appeal process [62].
A novel biparatopic antibody, MEDIA4276 binds to the 39S Fv and trastuzumab ScFV epitopes with site-specific conjugation to a microtubule inhibitor payload, inhibiting tumor cell proliferation more effectively than trastuzumab [63]. The antitumor effect of MEDI4276 was observed in several HER2-low cell lines in vitro. Further tests on HER2-low patient-derived xenografts (PDXs) excluded the interference of HR heterogeneity, which confirmed the tumor regression induced by MEDI4276 [64].
Unfortunately, in the phase Ⅱ dose-escalation and expansion study (ClinicalTrials.gov identifier: NCT02576548), even though MEDI4276 demonstrated obvious clinical activity, it still showed unbearable toxicity when the dose was higher than 0.3 mg/kg. Common toxicities included nausea, fatigue and vomiting [65]. The clinical development of MEDI4276 was severely delayed due to high incidences of drug-related adverse reactions, and it was therefore halted.
MCLA128 is a BsAb targeting HER2 and HER3 receptors with enhanced ADCC to directly inhibit tumor growth [66,67]. In 2017, researchers released the results of a phase Ⅱ study of MCLA128 (ClinicalTrials.gov identifier: NCT02912949). MCLA128 was administered with a median of 4.5 cycles to patients with HER2-positive metastatic BC who had received a median of 5.5 precious lines of metastatic therapy, and the clinical benefit rate (CBR) was 70% [68].
MCLA128 has the ability to overcome drug resistance in targeted therapy and endocrine therapy [66,69]. A phase Ⅱ study (ClinicalTrials.gov identifier: NCT03321981) enrolled patients with HER2-low BC who were estrogen receptor (ER)-positive and progressed to cyclin-dependent kinase 4 and 6 (CDK4/6) and endocrine therapy, with an effective 24 week CBR of 16.7% for MCLA128 combined with endocrine therapy [70]. No significant toxicity was observed.
3.1.4. Trispecific Antibody
At the 2021 AACR Annual Meeting, representatives from the Sanofi organization presented a novel HER2-targeted T-cell splice agent called SAR443216. SAR443216 is a trispecific antibody that binds to HER2, CD3 and CD28 antigenic sites and contains mutant IgG4-Fc lacking an effector function [71]. The binding of CD28 can activate the IL-2 and NF-κB pathways, induce the anti-apoptosis protein Bcl-xL and, subsequently, enhance T-cell-dependent cytotoxicity (TDCC). In preclinical models, SAR443216 activated both CD4 and CD8 T cells in HER2-expressing cancer cell lines (including HER2-low), stimulated the secretion of cytokines and granzyme B, and exerted an antitumor effect [71].
The first phase I/IB open monotherapy trial (ClinicalTrials.gov identifier: NCT05013554) of TED16925 will recruit patients with different solid tumors expressing HER2, including those with HER2-low BC.
3.1.5. Tyrosine Kinase Inhibitors
Tyrosine kinase inhibitors (TKIs) are pan-HER kinase inhibitors that interfere with or block HER2 signaling downstream by inhibiting tyrosine phosphorylation and the catalytic activity of the receptor [72]. As a result of its greater HER2 recognition ability and lower molecular weight, TKIs can prolong the action time of trastuzumab by regulating the ADCC effect and even cross the blood–brain barrier to protect against brain metastases [73].
Lapatinib, the first TKI approved against both HER2 and EGFR, enhanced HER2 expression in HER2-low BC cells [74], potentially transforming patients with refractory diseases into patients with tumors sensitive to trastuzumab [75,76,77,78].
Neratinib is an irreversible pan-HER inhibitor that more aggressively inhibits proliferation than lapatinib and may enable phenotypic alterations to increase ADCC mediated by trastuzumab [79,80,81,82,83].
Poziotinib, a novel oral quinazoline broad-spectrum HER inhibitor developed by Hanmi Pharm [84], overcomes the differences in drug binding sites, upregulates the expression of HER2 and enhances the activity of trastuzumab emtansine (T-DM1) [85]. In an open-label, multicenter, phase II clinical trial (ClinicalTrials.gov identifier: NCT02418689), a median PFS of 4.04 months was demonstrated when poziotinib was used in patients with refractory HER2-positive BC who had failed more than second-line HER2-targeted therapy [86,87]. Simmons et al. assessed efficacy outcomes gathered from eight clinical trials comparing third-line or higher therapy for HER2-positive BC. There were no differences in the results between T-Dxd and MCLA128, although poziotinib showed a survival benefit in a phase II trial [88].
Several other anti-HER2 TKIs, including pyrrolizidine, have been studied in light of these encouraging results (ClinicalTrials.gov identifier: NCT03412383) [89].
An issue that has emerged with TKI is the best application scenario for drugs. With the current results, TKI performs more as a synergist of HER2-targeting drugs, and related research is being explored.
3.2. Targeting HER2-Related Intracellular Signaling Pathways
Targeting PI3K/AKT/mTOR
The PI3K/AKT/mTOR signaling pathway is involved in the cell cycle, cell proliferation and angiogenesis and also regulates HER2 and ER receptor expression; it is thus a target for reversing endocrine resistance and HER2-targeted drug resistance [90,91,92]. Most studies combine PI3K inhibitors and Akt inhibitors with chemotherapy.
Allotype-specific PI3K inhibitors are widely used. They absorb the failure factors of pan-PI3K inhibitors; improve a variety of defects, such as off-target effects and toxicity; and specifically target the PI3Kp110 α, p110 β, p110 δ and p110 γ subtypes [93].
Alpelisib is the first PI3Kp110α isotype inhibitor to be approved by the FDA. Multiple clinical trials enrolling ER-positive BC patients have revealed the potential of alpelisib as a backline treatment option for endocrine-resistant BC [94,95,96,97,98]. The CBYL719XUS06T phase I/II study (ClinicalTrials.gov identifier: NCT02379247) investigated alpelisib with nab-paclitaxel in HER2-negative BC. In Phase I, 13 patients were divided into three groups treated with alpelisib (250, 300 and 350 mg) plus albumin paclitaxel, and no dose-limiting toxicity was observed [97]. In phase II, the median PFS was 8.7 months, and the ORR was 59%, with an overall response rate of 21% [99]. Regrettably, no further analysis was performed for the HER2-low subgroup.
AKT inhibitors are serine or threonine kinase molecules that target all AKT isoforms, strongly inhibit cell proliferation and AKT phosphorylation, and alleviate aggressive tumor behavior [100]. Almost all AKT inhibitors in clinical trials show limited therapeutic activities as single agents; therefore, combination therapeutic strategies are the main direction for research [101,102,103,104,105]. Nevertheless, conflicting results for AKT inhibitors in combination with chemotherapeutic agents have been observed in several clinical studies.
The BEECH phase Ib/II trial (ClinicalTrials.gov identifier: NCT01625286) evaluated capivasertib, an AKT inhibitor, with paclitaxel vs. paclitaxel alone in HR+/HER2- BC. There were similar dose intensities for paclitaxel between the treatment and control groups, with no significant difference in median PFS [106]. Comparatively, the PAKT trial (ClinicalTrials.gov identifier: NCT02423603) found capivasertib combined with paclitaxel to be superior to paclitaxel alone based on PFS (5.9 vs. 4.2 months; HR, 0.74; p = 0.06) [107,108].
In the FAIRLANE study, in which patients with TNBC received ipatasertib, another AKT inhibitor, with paclitaxel or paclitaxel alone, the pCR showed no clinical benefit or statistically significant improvement [109]. The PFS in LOTUS was improved under the same test conditions (ClinicalTrials.gov identifier: NCT02162719) [110].
In accordance with the different therapeutic effects of capivasertib or ipatasertib combined with chemotherapy, it is speculated that AKT mutations may not be the core driving event of cancer and that overactivation of the PI3K pathway cannot be effectively reduced by inhibiting AKT alone. Alternatively, a rapid attack may occur due to a tumor-acquired immune response or an inability to tolerate primary tumor drug resistance [111]. Since the pathways of cytotoxicity are unrelated to each other, AKT inhibitors should theoretically act synergistically with anti-HER2-targeted drugs.
3.3. Targeting the Immune Microenvironment
TNBC and HER2-positive groups present immunogenic features for BC, with a large number of tumor-infiltrating lymphocytes and higher levels of PD-L1, which are potential immunotherapy candidates [112,113]. Given the anti-tumor activity that HER2-targeted therapy can exert through the immune-mediated mechanism, immunotherapy and targeted therapy are being studied together.
3.3.1. HER2-Derived Peptide Vaccine
Vaccinations are a form of active immunotherapy in which the immune system recognizes antigens on the surface of cells. Directly attacking tumor cells and tumor stroma or indirectly resetting the immune system to antitumor detection mode are the principles of action, which enhance the sustained effectiveness of the antitumor immune response [114]. Tumors can benefit from vaccination when conventional cytotoxic or targeted drug therapies fail [114].
Tumor-associated antigens (TAAs), including HER2, are the basis of many vaccines used for BC. Current immunogenic HER2-derived peptides derive from different parts of HER2 molecules, such as E75 from the extracellular domain, GP2 from the transmembrane domain and AE37 from the intracellular domain [115]. Their tumor killing effects are usually achieved by triggering the immune system to target HER2-expressing cells and induce a tumor-specific immune response [116].
The E75 peptide (nelipepimut-S, NP-S) is the most widely researched and advanced vaccine for BC. Several clinical studies have observed that the application of the E75 vaccine can induce an immune response and maintain safety [115,116,117,118]. A trial found that, due to the possible immune tolerance of HER2 positivity, patients carrying HER2-low were able to show a stronger immune response, suggesting the need for further clinical studies targeting the HER2-low subgroup.
Subsequently, the PRESENT trial (ClinicalTrials.gov identifier: NCT01479244) recruited lymph node-positive, low-to-moderate HER2-expressing early BC women, who were randomly assigned to granulocyte–macrophage colony-stimulating factor (GM-CSF) or NP-S combined with GM-CSF groups [119]. The interim report revealed that the trial did not demonstrate a clinical benefit for vaccination alone but instead was terminated early by an independent data monitoring committee due to a rapidly increasing number of recurrent events [120]. Paradoxically, vaccination with trastuzumab significantly prolonged DFS in clinical studies conducted simultaneously. In contrast, the DFS of the control group in the GP2 test was 89%. When the median follow-up was more than 34 months, the DFS was still 100%, which suggests that there may be a synergistic effect between the HER2-targeted peptide vaccine and trastuzumab [118,120].
A prospective, randomized, single-blind, placebo-controlled phase IIb study (ClinicalTrials.gov identifier: NCT01570036) was revalidated in light of the above results. In short, 275 patients were randomly assigned to receive NP-S or placebo after one year of standard treatment with trastuzumab [121].
Intention to treat (ITT) analysis was performed at a median follow-up of 25.7 months. No significant difference in DFS was observed in HER2 IHC 1+ or 2+ BC (HR, 0.62; 95% CI, 0.31–1.25; p = 0.18). However, the TNBC subset showed potential benefits [121]. Similar outcomes were seen again in the clinical trial for the AE37 vaccine [122,123]. To clarify the meaning of TNBC in the context of HER2-derived peptide vaccines, further discussion should be given to HR status and HER2-0 and HER2-low subgroups.
3.3.2. Immune Checkpoint Inhibitor
Immune escape is the key mechanism of tumor occurrence and development. Generally, tumors block T-cell activation by connecting immune checkpoint receptors (ICR) with their ligands. A local microenvironment containing inflammatory cytokines can also induce the undifferentiated expression of PD-1 [124]. In preclinical experiments, blocking the inhibitory pathway of ICR–ligand interactions in the tumor microenvironment restores the functional immune response of TAAs [125,126]. Several monoclonal antibodies targeting ICR markers, including cytotoxic T lymphocyte-associated antigen (CTLA-4), programmed cell death protein 1 (PD-1) and programmed death ligand 1 (PD-L1), have shown good clinical activity in BC [127,128,129,130].
Trials are being conducted to determine whether immune checkpoint inhibitor (ICB) is effective when used in combination with anti-HER2 therapies. In a dose-escalation test of DS8201-A-U105 (ClinicalTrials.gov identifier: NCT03523572), the recommended dose (RDE) of T-Dxd combined with nivolumab was 5.4 mg/kg and 360 mg, respectively [131].
For the HER2-low cohort (n = 16), in the phase II dose-expansion trial, RDE was administered to 48 participants with an ORR of 37.5% and median PFS of 6.3 months (95% CI, 2.3-NE) after approximately 7 months of follow-up [132]. Despite the fact that T-Dxd combined with navumab showed an ORR similar to T-Dxd monotherapy, given that combination therapy has a much higher benefit rate than any single drug in preclinical models, clinical benefits cannot be determined without a longer follow-up.
Duvalizumab is a selective and high-affinity monoclonal antibody against human immunoglobulin G1K that completes the process of T-cell recognition and tumor cell killing by blocking the binding of PD-L1 to PD-1 and CD80 [133].
Cohort 6 of the multicenter, randomized, IB/II BEGONIA study (ClinicalTrials.gov identifier: NCT03742102) was designed to evaluate the potency of dovalizumab with T-DXD as a first-line treatment for HER2-low BC patients [134]. Eighteen patients had received more than one treatment at the time of the report, and data for twelve identifiable case assessments were obtained. Treatment resulted in 8 SDs and 1 PR, with an ORR of 66.7% [134]. Despite limited patient numbers, the combination showed positive safety and effectiveness.
Another study of pembrolizumab in combination with T-Dxd (ClinicalTrials.gov identifier: NCT04042701) is underway in light of the favorable efficacy of PD-1 inhibitors in HER2-low BC. The second phase of the trial will give the HER2-low cohort RDE treatment to obtain ORR outcomes through independent central evaluation (ICR), with preliminary results expected in May 2023 [135].
4. Other Therapies
Although there is more enthusiasm to develop tumor biologic therapies, given that chemotherapy and endocrine therapy are the main treatments for BC, it is necessary to compare the advantages and disadvantages with targeted therapies and determine the best order of sequential use.
4.1. Endocrine Therapy
In a retrospective study involving 3689 BC patients examining the intrinsic subtype distribution of PAM50, the HER2-low BC population was approximately 80.8% HR+. It is therefore crucial to examine whether HER2 expression levels impact the efficacy of endocrine therapies [1,10,136].
In the BIG1-98 trial, 3650 postmenopausal women were given letrozole and tamoxifen. Analysis of heterogeneity demonstrated that HER2 expression levels were not affected by the drug or the effects of endocrine therapy [137]. The TRANS-AIOG meta-analysis integrated data from three studies, ATAC, BIG1-98 and TEAM, and compared therapeutic strategies based on letrozole, tamoxifen or switching from letrozole to tamoxifen and found evidence, supporting the view that endocrine therapy can benefit various levels of HER2 expression [138]. AglaiaSchiza et al. further measured the effect of HER2-targeted therapy and denied the predictive value of HER2 status in postmenopausal BC patients for endocrine therapy. They reiterated that endocrine therapy is still the first option for HR-positive BC regardless of HER2 expression [139,140].
With the advent of endocrine therapy, drug resistance has increased. CDK4/6 inhibitors (CDK4/6i) are considered effective for retaining endocrine sensitivity by interfering with the ER cascade, inhibiting RB1 phosphorylation, and triggering G1 to S cell cycle arrest [141,142]. Since 2014, the MONARCH, PALOMA, and MONALEESA studies have demonstrated that CDK4/6i is gradually changing the course of endocrine therapy for advanced BC [143,144,145,146,147,148,149]. Palbociclib, ribociclib, and abemaciclib are currently approved as first-line treatments for HR+/HER2-negative BC in combination with aromatase inhibitors (AI) or as second-line treatments in combination with fulvestrant.
In addition, some scholars believe that bidirectional crosstalk between members of the human epidermal growth factor receptor family (HER) and the estrogen receptor (ER) is the basis of drug resistance; that is, high expression and amplification of HER2 drive the occurrence of endocrine resistance [150]. Kelvin et al. investigated the relationship between HER2 expression levels and the efficacy of CDK4/6i combined with letrozole or fulvestrant therapy in ER+/HER2-negative BC patients [151]. In HER2-low BC, the PFS was significantly shorter than in HER2-0 (8.9 months vs. 18.8 months, p = 0.014) [151]. HER2 upregulation is responsible for endocrine resistance, resulting in reduced PFS and pCR rates with overall endocrine therapy.
The ER and HER axes are being targeted simultaneously in order to improve the response of the HR+/HER2+ population to endocrine therapies and control the onset of endocrine resistance. Triple therapies targeting HER2, HER3 and ER evaluated in preclinical studies were effective in the ER+/HER2-low BC pdx model. Lumretuzumab (anti-HER3) and patuximab (anti-HER2) combined with fulvestrant maintained durable antitumor effects [69]. This drug combination has not shown promising safety or antitumor activity in clinical trials, and it has been limited by DLT, has a narrow treatment window and shows a high incidence of diarrhea [152].
Excitingly, the triple combination has been reversed with the development of the bispecific antibody MCLA-128, which directly and simultaneously targets HER2/HER3 and also greatly reduces drug toxicity [153]. In a phase II trial recruiting patients who had progressed after treatment with ET and CDK4/6i, adding MCLA-128 to the ET backline resulted in clinical benefit and even reversed endocrine sensitivity in 17% of these patients [70].
The NA-PHER2 trial (ClinicalTrials.gov identifier: NCT02530424) evaluated the drug combination of palbociclib, fulvestrant and dual HER2 blockade (trastuzumab, pertuzumab) [154]. The HR+/HER2-low BC cohort performed well at the endpoint, with Ki67 decreasing consistently from baseline to 2 weeks after treatment and before surgery (16 weeks) [155]. The above results show the preliminary efficacy of endocrine therapy involving CDK4/6i in combination with HER2-targeted drugs for HR+/HER2-low BC [155,156]. They confirm direct crosstalk between the HER and ER axis, and any single targeted therapy has limitations. HER-targeted therapy and endocrine therapy are therefore likely to be effective for patients with ER+/HER2-low BC who are resistant to endocrine therapy.
4.2. Chemotherapy
From the perspective of chemotherapy benefit, several clinical trials have found that HER2-low BC has a lower pCR rate than HER2-0 BC. However, the difference is not statistically significant, and the OS and DFS prognostic outcomes remain uncertain [157,158,159]. The currently available evidence suggests that chemotherapy regimens for HER2-low BC can still be managed with reference to HER2-negative BC. The difference is that paclitaxel- and anthracycline-based regimens for chemotherapy are preferred for the HR-negative subgroup (TNBC) in HER2-negative BC, regardless of early and late stages, whereas endocrine therapy is generally preferred in the HR-positive subgroup (luminal A/luminal B). Additional sequential or combination chemotherapy is recommended for intermediate/high-risk patients. Chemotherapy is recommended as the first line of treatment when the disease is critical and, progresses rapidly, and the ER is low [160,161,162].
5. Discussion and Future Prospects
Several new drugs now have shown clinical evidence that they can be used to treat HER2-low BC as part of HER2-targeted therapy, reflecting the clearly unmet treatment needs of HER2-low BC.
Researchers are exploring targeted therapies for HER2-low BC, but HER2 expression levels must be identified to guide treatment. While IHC/ISH assays have become an accepted standard of determination, their accuracy is low due to technical shortcomings. Other quantitative analysis techniques offer advantages and disadvantages, but they are limited by the core technical requirements, and cannot enter large-scale clinical trials; thus far, a unified standard that is suitable for use as a verification tool for IHC/ISH has not been formed.
Different HER2 expression levels respond differently to novel HER2-targeted therapies. The threshold for HER2 grouping should be redefined, abandoning the traditional dichotomy of HER2-positive and -negative. By repeatedly measuring HER2 expression levels across different disease nodes, we can redefine the treatment potential and molecular typing of HER2-negative breast cancer.
As a backbone therapy for patients with HER2-low BC, ADC analogs are unquestionably effective, but their efficacy against early-stage disease remains to be further confirmed. On the basis of the available evidence, we recommend that HER2-low BC be treated as two ER+/ER- groups.
Early-stage tumors are still managed as HER2-negative tumors. Patients carrying an ER+ will likely benefit from hormone therapy, and those with an ER- may benefit from anthracycline- or paclitaxel-based chemotherapy. In cases where the tumor is at an advanced stage, T-DXd can be applied first. When the results from inhibiting a single pathway are inadequate, further chemotherapy, endocrine therapy or immunotherapy can be considered. Clinical trials are prioritized whenever resistance occurs in the backline. Since there are a limited number of clinical trials stratified for HER2-low BC, the above results are still susceptible to error. There will, however, be an increasing number of studies that will focus on HER2-low BC in the future, providing an empirical basis for anti-HER2 therapeutics and creating more survival opportunities for HER2-low BC patients.
Author Contributions
Conceptualization, H.-Z.L. and J.-R.H.; methodology, F.-M.Y.; validation, X.F. and Y.-F.R.; writing—original draft preparation, H.-Z.L., J.-R.H., X.F. and Y.-F.R.; writing—review and editing, Z.-H.L. and F.-M.Y.; visualization, H.-Z.L. and Z.-H.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Sichuan Provincial Key Discipline Construction Project of Traditional Chinese Medicine—Oncology of TCM, No. 2100601.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Tarantino, P.; Hamilton, E.; Tolaney, S.M.; Cortes, J.; Morganti, S.; Ferraro, E.; Marra, A.; Viale, G.; Trapani, D.; Cardoso, F.; et al. HER2-Low Breast Cancer: Pathological and Clinical Landscape. J. Clin. Oncol. 2020, 38, 1951–1962. [Google Scholar] [CrossRef] [PubMed]
- Kurozumi, S.; Padilla, M.; Kurosumi, M.; Matsumoto, H.; Inoue, K.; Horiguchi, J.; Takeyoshi, I.; Oyama, T.; Ranger-Moore, J.; Allred, D.C.; et al. HER2 intratumoral heterogeneity analyses by concurrent HER2 gene and protein assessment for the prognosis of HER2 negative invasive breast cancer patients. Breast Cancer Res. Treat. 2016, 158, 99–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchiò, C.; Dell’Orto, P.; Annaratone, L.; Geyer, F.C.; Venesio, T.; Berrino, E.; Di Cantogno, L.V.; Garofoli, A.; Rangel, N.; Casorzo, L.; et al. The dilemma of HER2 double-equivocal breast carcinomas: Genomic profiling and implications for treatment. Am. J. Surg. Pathol. 2018, 42, 1190. [Google Scholar] [CrossRef] [PubMed]
- Buckley, N.E.; Forde, C.; McArt, D.G.; Boyle, D.P.; Mullan, P.B.; James, J.A.; Maxwell, P.; McQuaid, S.; Salto-Tellez, M. Quantification of HER2 heterogeneity in breast cancer–implications for identification of sub-dominant clones for personalised treatment. Sci Rep. 2016, 6, 23383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossi, V.; Sarotto, I.; Maggiorotto, F.; Berchialla, P.; Kubatzki, F.; Tomasi, N.; Redana, S.; Martinello, R.; Valabrega, G.; Aglietta, M.; et al. Moderate immunohistochemical expression of HER-2 (2+) without HER-2 gene amplification is a negative prognostic factor in early breast cancer. Oncologist 2012, 17, 1418–1425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agostinetto, E.; Rediti, M.; Fimereli, D.; Debien, V.; Piccart, M.; Aftimos, P.; Sotiriou, C.; de Azambuja, E. HER2-low breast cancer: Molecular characteristics and prognosis. Cancers 2021, 13, 2824. [Google Scholar] [CrossRef]
- Won, H.S.; Ahn, J.; Kim, Y.; Kim, J.S.; Song, J.Y.; Kim, H.K.; Lee, J.; Park, H.K.; Kim, Y.S. Clinical significance of HER2-low expression in early breast cancer: A nationwide study from the Korean Breast Cancer Society. Breast Cancer Res. 2022, 24, 22. [Google Scholar] [CrossRef] [PubMed]
- Gilcrease, M.Z.; Woodward, W.A.; Nicolas, M.M.; Corley, L.J.; Fuller, G.N.; Esteva, F.J.; Tucker, S.L.; Buchholz, T.A. Even low-level HER2 expression may be associated with worse outcome in node-positive breast cancer. Am. J. Surg. Pathol. 2009, 33, 759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eggemann, H.; Ignatov, T.; Burger, E.; Kantelhardt, E.J.; Fettke, F.; Thomssen, C.; Costa, S.D.; Ignatov, A. Moderate HER2 expression as a prognostic factor in hormone receptor positive breast cancer. Breast Cancer Res. Treat. 2015, 22, 725–733. [Google Scholar] [CrossRef] [Green Version]
- Schettini, F.; Chic, N.; Brasó-Maristany, F.; Paré, L.; Pascual, T.; Conte, B.; Martínez-Sáez, O.; Adamo, B.; Vidal, M.; Barnadas, E.; et al. Clinical, pathological, and PAM50 gene expression features of HER2-low breast cancer. NPJ Breast Cancer 2021, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Denkert, C.; Seither, F.; Schneeweiss, A.; Link, T.; Blohmer, J.U.; Just, M.; Wimberger, P.; Forberger, A.; Tesch, H.; Jackisch, C.; et al. Clinical and molecular characteristics of HER2-low-positive breast cancer: Pooled analysis of individual patient data from four prospective, neoadjuvant clinical trials. Lancet Oncol. 2021, 22, 1151–1161. [Google Scholar] [CrossRef]
- Fehrenbacher, L.; Cecchini, R.S.; Geyer, C.E.; Rastogi, P., Jr.; Costantino, J.P.; Atkins, J.N.; Crown, J.P.; Polikoff, J.; Boileau, J.F.; Provencher, L.; et al. NSABP B-47/NRG Oncology Phase III Randomized Trial Comparing Adjuvant Chemotherapy with or without Trastuzumab in High-Risk Invasive Breast Cancer Negative for HER2 by FISH and with IHC 1+ or 2. J. Clin. Oncol. 2020, 38, 444–453. [Google Scholar] [CrossRef] [PubMed]
- Gianni, L.; Lladó, A.; Bianchi, G.; Cortes, J.; Kellokumpu-Lehtinen, P.L.; Cameron, D.A.; Miles, D.; Salvagni, S.; Wardley, A.; Goeminne, J.C.; et al. Open-label, phase II, multicenter, randomized study of the efficacy and safety of two dose levels of Pertuzumab, a human epidermal growth factor receptor 2 dimerization inhibitor, in patients with human epidermal growth factor receptor 2-negative metastatic breast cancer. J. Clin. Oncol. 2010, 28, 1131–1137. [Google Scholar] [PubMed] [Green Version]
- Rosso, C.; Voutsadakis, I.A. Characteristics, Clinical Differences and Outcomes of Breast Cancer Patients with Negative or Low HER2 Expression. Clin. Breast Cancer 2022, 22, 391–397. [Google Scholar] [CrossRef] [PubMed]
- de Moura Leite, L.; Cesca, M.G.; Tavares, M.C.; Santana, D.M.; Saldanha, E.F.; Guimarães, P.T.; Sá, D.; Simões, M.; Viana, R.L.; Rocha, F.G.; et al. HER2-low status and response to neoadjuvant chemotherapy in HER2 negative early breast cancer. Breast Cancer Res. Treat. 2021, 190, 155–163. [Google Scholar] [CrossRef]
- Koleva-Kolarova, R.G.; Oktora, M.P.; Robijn, A.L.; Greuter, M.J.W.; Reyners, A.K.L.; Buskens, E.; de Bock, G.H. Increased life expectancy as a result of non-hormonal targeted therapies for HER2 or hormone receptor positive metastatic breast cancer: A systematic review and meta-analysis. Cancer Treat. Rev. 2017, 55, 16–25. [Google Scholar] [CrossRef] [Green Version]
- Takegawa, N.; Tsurutani, J.; Kawakami, H.; Yonesaka, K.; Kato, R.; Haratani, K.; Hayashi, H.; Takeda, M.; Nonagase, Y.; Maenishi, O.; et al. [fam-] trastuzumab deruxtecan, antitumor activity is dependent on HER2 expression level rather than on HER2 amplification. Int. J. Cancer 2019, 145, 3414–3424. [Google Scholar] [CrossRef]
- Bradley, R.; Braybrooke, J.; Gray, R.; Hills, R.; Liu, Z.; Peto, R.; Davies, L.; Dodwell, D.; McGale, P.; Pan, H.; et al. Trastuzumab for early-stage, HER2-positive breast cancer: A meta-analysis of 13,864 women in seven randomised trials. Lancet Oncol. 2021, 21, 1139–1150. [Google Scholar] [CrossRef]
- Ogitani, Y.; Hagihara, K.; Oitate, M.; Naito, H.; Agatsuma, T. Bystander killing effect of DS-8201a, a novel anti-human epidermal growth factor receptor 2 antibody–drug conjugate, in tumors with human epidermal growth factor receptor 2 heterogeneity. Cancer Sci. 2016, 107, 1039–1046. [Google Scholar] [CrossRef] [PubMed]
- Miglietta, F.; Griguolo, G.; Bottosso, M.; Giarratano, T.; Lo Mele, M.; Fassan, M.; Cacciatore, M.; Genovesi, E.; De Bartolo, D.; Vernaci, G.; et al. Evolution of HER2-low expression from primary to recurrent breast cancer. NPJ Breast Cancer 2021, 7, 137. [Google Scholar] [CrossRef] [PubMed]
- Wolff, A.C.; Hammond, M.E.H.; Allison, K.H.; Harvey, B.E.; Mangu, P.B.; Bartlett, J.M.S.; Bilous, M.; Ellis, I.O.; Fitzgibbons, P.; Hanna, W.; et al. Human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline focused update. J. Clin. Oncol. 2018, 142, 1364–1382. [Google Scholar]
- Torlakovic, E.E.; Nielsen, S.; Francis, G.; Garratt, J.; Gilks, B.; Goldsmith, J.D.; Hornick, J.L.; Hyjek, E.; Ibrahim, M.; Miller, K.; et al. Standardization of positive controls in diagnostic immunohistochemistry: Recommendations from the International Ad Hoc Expert Committee. Appl. Immunohistochem. Mol. Morphol. 2015, 23, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Furrer, D.; Sanschagrin, F.; Jacob, S.; Diorio, C. Advantages and disadvantages of technologies for HER2 testing in breast cancer specimens. Am. J. Clin. Pathol. 2015, 144, 686–703. [Google Scholar] [CrossRef] [PubMed]
- Scaltriti, M.; Nuciforo, P.; Bradbury, I.; Sperinde, J.; Agbor-Tarh, D.; Campbell, C.; Chenna, A.; Winslow, J.; Serra, V.; Parra, J.L.; et al. High HER2 expression correlates with response to the combination of lapatinib and trastuzumab. Clin. Cancer Res. 2015, 21, 569–576. [Google Scholar] [CrossRef] [Green Version]
- Larson, J.S.; Goodman, L.J.; Tan, Y.; Defazio-Eli, L.; Paquet, A.C.; Cook, J.W.; Rivera, A.; Frankson, K.; Bose, J.; Chen, L.; et al. Analytical validation of a highly quantitative, sensitive, accurate, and reproducible assay (HERmark®) for the measurement of HER2 total protein and HER2 homodimers in FFPE breast cancer tumor specimens. Pathol. Res. Int. 2010, 2010, 814176. [Google Scholar] [CrossRef] [PubMed]
- Perez, E.A.; Suman, V.J.; Davidson, N.E.; Martino, S.; Kaufman, P.A.; Lingle, W.L.; Flynn, P.J.; Ingle, J.N.; Visscher, D.; Jenkins, R.B. HER2 testing by local, central, and reference laboratories in specimens from the North Central Cancer Treatment Group N9831 intergroup adjuvant trial. J. Clin. Oncol. 2006, 24, 3032–3038. [Google Scholar] [CrossRef]
- Yardley, D.A.; Kaufman, P.A.; Huang, W.; Krekow, L.; Savin, M.; Lawler, W.E.; Zrada, S.; Starr, A.; Einhorn, H.; Schwartzberg, L.S.; et al. Quantitative measurement of HER2 expression in breast cancers: Comparison with ‘real-world’routine HER2 testing in a multicenter Collaborative Biomarker Study and cor.rrelation with overall survival. Breast Cancer Res. 2015, 17, 41. [Google Scholar] [CrossRef] [Green Version]
- Huang, W.; Reinholz, M.; Weidler, J.; Yolanda, L.; Paquet, A.; Whitcomb, J.; Lingle, W.; Jenkins, R.B.; Chen, B.; Larson, J.S.; et al. Comparison of central HER2 testing with quantitative total HER2 expression and HER2 homodimer measurements using a novel proximity-based assay. Am. J. Clin. Pathol. 2010, 134, 303–311. [Google Scholar] [CrossRef] [Green Version]
- Susini, T.; Bussani, C.; Marini, G.; Nori, J.; Olivieri, S.; Molino, C.; Bianchi, S.; Vezzosi, V.; Paglierani, M.; Giachi, M.; et al. Preoperative assessment of HER-2/neu status in breast carcinoma: The role of quantitative real-time PCR on core-biopsy specimens. Gynecol. Oncol. 2010, 116, 234–239. [Google Scholar] [CrossRef]
- Koudelakova, V.; Berkovcova, J.; Trojanec, R.; Vrbkova, J.; Radova, L.; Ehrmann, J.; Kolar, Z.; Melichar, B.; Hajduch, M. Evaluation of HER2 gene status in breast cancer samples with indeterminate fluorescence in situ hybridization by quantitative real-time PCR. J. Mol. Diagn 2015, 17, 446–455. [Google Scholar] [CrossRef]
- Cronin, M.; Sangli, C.; Liu, M.L.; Pho, M.; Dutta, D.; Nguyen, A.; Jeong, J.; Wu, J.; Langone, K.C.; Watson, D. Analytical Validation of the Onco type DX Genomic Diagnostic Test for Recurrence Prognosis and Therapeutic Response Prediction in Node-Negative, Estrogen Receptor–Positive Breast Cancer. Clin. Chem. 2007, 53, 1084–1091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caselli, E.; Pelliccia, C.; Teti, V.; Bellea, G.; Mandarano, M.; Ferri, I.; Hartmann, K.; Laible, M.; Sahin, U.; Varga, Z.; et al. Looking for more reliable biomarkers in breast cancer: Comparison between routine methods and RT-qPCR. PLoS ONE 2021, 16, e0255580. [Google Scholar] [CrossRef] [PubMed]
- Benöhr, P.; Henkel, V.; Speer, R.; Vogel, U.; Sotlar, K.; Aydeniz, B.; Reiser, A.; Neubauer, H.; Tabiti, K.; Wallwiener, D.; et al. Her-2/neu expression in breast cancer-a comparison of different diagnostic methods. Anticancer Res. 2005, 25, 1895–1900. [Google Scholar]
- Jacquemier, J.; Spyratos, F.; Esterni, B.; Mozziconacci, M.J.; Antoine, M.; Arnould, L.; Lizard, S.; Bertheau, P.; Lehmann-Che, J.; Fournier, C.B.; et al. SISH/CISH or qPCR as alternative techniques to FISH for determination of HER2 amplification status on breast tumors core needle biopsies: A multicenter experience based on 840 cases. BMC Cancer 2013, 13, 351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dabbs, D.J.; Klein, M.E.; Mohsin, S.K.; Tubbs, R.R.; Shuai, Y.; Bhargava, R. High false-negative rate of HER2 quantitative reverse transcription polymerase chain reaction of the Oncotype DX test: An independent quality assurance study. J. Clin. Oncol. 2011, 29, 4279–4285. [Google Scholar] [CrossRef] [PubMed]
- Purnomosari, D.; Aryandono, T.; Setiaji, K.; Nugraha, S.B.; Pals, G.; van Diest, P.J. Comparison of multiplex ligation dependent probe amplification to immunohistochemistry for assessing HER-2/neu amplification in invasive breast cancer. Biotech. Histochem. 2006, 81, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Wolff, A.C.; Hammond, M.E.; Schwartz, J.N.; Hagerty, K.L.; Allred, D.C.; Cote, R.J.; Dowsett, M.; Fitzgibbons, P.L.; Hanna, W.M.; Langer, A.; et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth facto.or receptor 2 testing in breast cancer. J. Clin. Oncol. 2007, 131, 18–43. [Google Scholar]
- Sapino, A.; Goia, M.; Recupero, D.; Marchiò, C. Current challenges for HER2 testing in diagnostic pathology: State of the art and controversial issues. Front. Oncol. 2013, 3, 129. [Google Scholar] [CrossRef] [Green Version]
- Ho-Pun-Cheung, A.; Bazin, H.; Boissière-Michot, F.; Mollevi, C.; Simony-Lafontaine, J.; Landas, E.; Bleuse, J.P.; Chardès, T.; Prost, J.F.; Pèlegrin, A.; et al. Quantification of HER1, HER2 and HER3 by time-resolved Förster resonance energy transfer in FFPE triple-negative breast cancer samples. Br. J. Cancer 2020, 122, 397–404. [Google Scholar] [CrossRef]
- Wesley, N.A.; Skrajna, A.; Simmons, H.C.; Budziszewski, G.R.; Azzam, D.N.; Cesmat, A.P.; McGinty, R.K. Time Resolved-Fluorescence Resonance Energy Transfer platform for quantitative nucleosome binding and footprinting. Protein Sci. 2022, 31, e4339. [Google Scholar] [CrossRef]
- Moasser, M.M. The oncogene HER2: Its signaling and transforming functions and its role in human cancer pathogenesis. Oncogene 2007, 26, 6469–6487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panowski, S.; Bhakta, S.; Raab, H.; Polakis, P.; Junutula, J.R. Site-specific antibody drug conjugates for cancer therapy. mAbs 2014, 6, 34–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staudacher, A.H.; Brown, M.P. Antibody drug conjugates and bystander killing: Is antigen-dependent internalisation required? Br. J. Cancer 2017, 117, 1736–1742. [Google Scholar] [CrossRef]
- Ogitani, Y.; Aida, T.; Hagihara, K.; Yamaguchi, J.; Ishii, C.; Harada, N.; Soma, M.; Okamoto, H.; Oitate, M.; Arakawa, S.; et al. DS-8201a, A Novel HER2-Targeting ADC with a Novel DNA Topoisomerase I Inhibitor, demonstrates a Promising Antitumor Efficacy with Differentiation fr.rom T-DM1Preclinical Efficacy of DS-8201a, a Novel HER2-Targeting ADC. Clin. Cancer Res. 2016, 22, 5097–5108. [Google Scholar] [CrossRef] [Green Version]
- Modi, S.; Park, H.; Murthy, R.K.; Iwata, H.; Tamura, K.; Tsurutani, J.; Moreno-Aspitia, A.; Doi, T.; Sagara, Y.; Redfern, C.; et al. Antitumor activity and safety of trastuzumab deruxtecan in patients with HER2-low–expressing advanced breast cancer: Results from a phase Ib study. J. Clin. Oncol. 2020, 38, 1887. [Google Scholar] [CrossRef] [PubMed]
- Powell, C.A.; Camidge, D.R.; Gemma, A.; Kusumoto, M.; Baba, T.; Kuwano, K.; Bankier, A.; Kiura, K.; Tamura, K.; Modi, S.; et al. Abstract P6-17-06: Characterization, monitoring and management of interstitial lung disease in patients with metastatic breast cancer: Analysis of data available from multiple studies of DS-8201a, a HER2-targeted antibody drug conjugate with a topoisomerase I inhibitor payload. Cancer Res. 2019, 79 (Suppl. S4), P6-17. [Google Scholar]
- Modi, S.; Jacot, W.; Yamashita, T.; Sohn, J.; Vidal, M.; Tokunaga, E.; Tsurutani, J.; Ueno, N.T.; Prat, A.; Chae, Y.S.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. N. Engl. J. Med. 2022, 387, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Bardia, A.; Barrios, C.; Dent, R.; Hu, X.; Óshaughnessy, J.; Yonemori, K.; Darilay, A.; Boston, S.; Liu, Y.; Patel, G.; et al. Abstract OT-03-09: Trastuzumab deruxtecan (T-DXd; DS-8201) vs investigator’s choice of chemotherapy in patients with hormone receptor-positive (HR+), HER2 low metastatic breast cancer whose disease has progressed on endocrine therapy in the metastatic setting: A randomized, global phase 3 trial (DESTINY-Breast06). Cancer Res. 2021, 81 (Suppl. S4), OT-03. [Google Scholar]
- Jhaveri, K.; Hamilton, E.; Loi, S.; Schmid, P.; Darilay, A.; Gao, C.; Patel, G.; Wrona, M.; Andre, F. Abstract OT-03-05: Trastuzumab deruxtecan (T-DXd; DS-8201) in combination with other anticancer agents in patients with HER2-low metastatic breast cancer: A phase 1b, open-label, multicenter, dose-finding and dose-expansion study (DESTINY-Breast08). Cancer Res. 2021, 81 (Suppl. S4), OT-03. [Google Scholar] [CrossRef]
- Xu, B.; Wang, J.; Fang, J.; Chen, X.; Han, Y.; Li, Q.; Zhang, P.; Yuan, P.; Ma, F.; Luo, Y.; et al. Abstract PD4-06: Early clinical development of RC48-ADC in patients with HER2 positive metastatic breast cancer. Cancer Res. 2020, 80 (Suppl. S4), PD4-06. [Google Scholar] [CrossRef]
- Wang, J.; Liu, Y.; Zhang, Q.; Feng, J.; Fang, J.; Chen, X.; Han, Y.; Li, Q.; Zhang, P.; Yuan, P.; et al. RC48-ADC, a HER2-targeting antibody-drug conjugate, in patients with HER2-positive and HER2-low expressing advanced or metastatic breast cancer: A pooled analysis of two studies. J. Clin. Oncol. 2021, 39, 15. [Google Scholar] [CrossRef]
- Banerji, U.; van Herpen, C.M.L.; Saura, C.; Thistlethwaite, F.; Lord, S.; Moreno, V.; Macpherson, I.R.; Boni, V.; Rolfo, C.; de Vries, E.G.E.; et al. Trastuzumab duocarmazine in locally advanced and metastatic solid tumours and HER2-expressing breast cancer: A phase 1 dose-escalation and dose-expansion study. Lancet Oncol. 2019, 20, 1124–1135. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Lian, W.; Zhao, X.; Qi, W.; Xu, J.; Xiao, L.; Qing, Y.; Xue, T.; Wang, J. A phase I study of safety and pharmacokinetics of A166, a novel selective inhibitor of human epidermal growth factor receptor-2 in Chinese patients with advanced solid tumors. J. Clin. Oncol. 2020, 38, e13007. [Google Scholar] [CrossRef]
- Hu, X.; Zhang, J.; Liu, R.; Gao, S.; Qing, Y.; Yi, S.; Yuan, J.; Chen, H.; Fan, B.; Zheng, H.; et al. Phase I study of A166 in patients with HER2-expressing locally advanced or metastatic solid tumors. J. Clin. Oncol. 2021, 39, 1024. [Google Scholar] [CrossRef]
- Oganesyan, V.; Peng, L.; Bee, J.S.; Li, J.; Perry, S.R.; Comer, F.; Xu, L.; Cook, K.; Senthil, K.; Clarke, L.; et al. Structural insights into the mechanism of action of a biparatopic anti-HER2 antibody. J. Biol. Chem. 2018, 293, 8439–8448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dokter, W.; Ubink, R.; van der Lee, M.; van der Vleuten, M.; van Achterberg, T.; Jacobs, D.; Loosveld, E.; van den Dobbelsteen, D.; Egging, D.; Mattaar, E. Preclinical Profile of the HER2-Targeting ADC SYD983/SYD985: Introduction of a New Duocarmycin-Based Linker-Drug PlatformPreclinical Profile of SYD983/SYD985. Mol. Cancer Ther. 2014, 13, 2618–2629. [Google Scholar] [CrossRef] [Green Version]
- Sharma, A.; Riaz, K.M.; Gill, M.S.; Patnaik, A.; Ulahannan, S.V.; Wang, J.S.; Gombos, D.S.; Ang, Q.; Cicic, D.; Bergonio, G.R.; et al. Reversible HER2 antibody-drug conjugate–induced ocular toxicity. Can. J. Ophthalmol. 2022, 57, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Nordstrom, J.L.; Gorlatov, S.; Zhang, W.; Yang, Y.; Huang, L.; Burke, S.; Li, H.; Ciccarone, V.; Zhang, T.; Stavenhagen, J.; et al. Anti-tumor activity and toxicokinetics analysis of MGAH22, an anti-HER2 monoclonal antibody with enhanced Fcγ receptor binding properties. Breast Cancer Res. 2011, 13, R123. [Google Scholar] [CrossRef] [Green Version]
- Im, S.A.; Cardoso, F.; Cortes, J.; Curigliano, G.; Pegram, M.D.; Rugo, H.S.; Brown-Glaberman, U.; Yardley, D.A.; Kim, S.-B.; de Boer , M.; et al. Abstract PS10-12: Integrated safety summary of single agent and combination margetuximab in phase 1, 2, and 3 studies of HER2-positive advanced cancers and metastatic breast cancer (MBC). Cancer Res. 2021, 81 (Suppl. S4), PS10-12. [Google Scholar]
- Hayes, D.F. HER2 and breast cancer—A phenomenal success story. N. Engl. J. Med. 2019, 381, 1284–1286. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Mo, Y.; Tang, M.; Shen, J.; Qi, Y.; Zhao, W.; Huang, Y.; Xu, Y.; Qian, C. Bispecific antibodies: From research to clinical application. Front. Immunol. 2021, 12, 1555. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, S.S.; Khalili, S.; Baradaran, B.; Bidar, N.; Shahbazi, M.A.; Mosafer, J.; Hashemzaei, M.; Mokhtarzadeh, A.; Hamblin, M.R. Bispecific monoclonal antibodies for targeted immunotherapy of solid tumors: Recent advances and clinical trials. Int. J. Biol. Macromol. 2021, 167, 1030–1047. [Google Scholar] [CrossRef] [PubMed]
- Rinnerthaler, G.; Gampenrieder, S.P.; Greil, R. HER2 directed antibody-drug-conjugates beyond T-DM1 in breast cancer. Int. J. Mol. Sci. 2019, 20, 1115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.Y.; Perry, S.R.; Muniz-Medina, V.; Wang, X.; Wetzel, L.K.; Rebelatto, M.C.; Hinrichs, M.J.; Bezabeh, B.Z.; Fleming, R.L.; Dimasi, N.; et al. A biparatopic HER2-targeting antibody-drug conjugate induces tumor regression in primary models refractory to or ineligible for HER2-targeted therapy. Cancer Cell 2016, 29, 117–129. [Google Scholar] [CrossRef] [Green Version]
- Pegram, M.D.; Hamilton, E.P.; Tan, A.R.; Storniolo, A.M.; Balic, K.; Rosenbaum, A.I.; Liang, M.; He, P.; Marshall, S.; Scheuber, A.; et al. First-in-human, phase 1 dose-escalation study of biparatopic anti-HER2 antibody–drug conjugate MEDI4276 in patients with HER2-positive advanced breast or gastric cancer. Mol. Cancer Ther. 2021, 20, 1442–1453. [Google Scholar] [CrossRef] [PubMed]
- Geuijen, C.A.W.; De Nardis, C.; Maussang, D.; Rovers, E.; Gallenne, T.; Hendriks, L.J.A.; Visser, T.; Nijhuis, R.; Logtenberg, T.; de Kruif, J.; et al. Unbiased combinatorial screening identifies a bispecific IgG1 that potently inhibits HER3 signaling via HER2-guided ligand blockade. Cancer Cell 2018, 33, 922–936. [Google Scholar] [CrossRef] [Green Version]
- De Nardis, C.; Hendriks, L.J.A.; Poirier, E.; Arvinte, T.; Gros, P.; Bakker, A.B.H.; de Kruif, J. A new approach for generating bispecific antibodies based on a common light chain format and the stable architecture of human immunoglobulin G1. Lancet Oncol. 2017, 292, 14706–14717. [Google Scholar] [CrossRef] [Green Version]
- Alsina, M.; Boni, V.; Schellens, J.H.; Moreno, V.; Bol, K.; Westendorp, M.; Sirulnik, L.A.; Tabernero, J.; Calvo, E. First-in-human phase 1/2 study of MCLA-128, a full length IgG1 bispecific antibody targeting HER2 and HER3: Final phase 1 data and preliminary activity in HER2+ metastatic breast cancer (MBC). J. Clin. Oncol. 2017, 35 (Suppl. S15), 2522. [Google Scholar] [CrossRef]
- Collins, D.; Jacob, W.; Cejalvo, J.M.; Ceppi, M.; James, I.; Hasmann, M.; Crown, J.; Cervantes, A.; Weisser, M.; Bossenmaier, B. Direct estrogen receptor (ER)/HER family crosstalk mediating sensitivity to lumretuzumab and pertuzumab in ER+ breast cancer. PLoS ONE 2017, 12, e0177331. [Google Scholar] [CrossRef]
- Pistilli, B.; Wildiers, H.; Hamilton, E.P.; Ferreira, A.A.; Dalenc, F.; Vidal, M.; Gavila, J.; Goncalves, A.; Murias, C.; Fournier, C.B.; et al. Clinical activity of MCLA-128 (zenocutuzumab) in combination with endocrine therapy (ET) in ER+/HER2-low, non-amplified metastatic breast cancer (MBC) patients (pts) with ET-resistant disease who had progressed on a CDK4/6 inhibitor (CDK4/6i). J. Clin. Oncol 2020, 38 (Suppl. S15), 1037. [Google Scholar] [CrossRef]
- Wenwen, S.; Sri, V.; Zhili, S.; Edward, S.; Zhen, X.; Liqing, C.; Virna, C.R.; Sukhvinder, S.; Dinesh, B.; Wu, L.; et al. SAR443216, a novel trispecific T cell engager with potent T cell-dependent cytotoxicity for HER2-low tumors. Cancer Res. 2021, 81 (Suppl. S13), 1825. [Google Scholar]
- Schroeder, R.L.; Stevens, C.L.; Sridhar, J. Small molecule tyrosine kinase inhibitors of ErbB2/HER2/Neu in the treatment of aggressive breast cancer. Molecules 2014, 19, 15196–15212. [Google Scholar] [CrossRef] [Green Version]
- Ríos-Luci, C.; Díaz-Rodríguez, E.; Gandullo-Sánchez, L.; Díaz-Gil, L.; Ocaña, A.; Pandiella, A. Adaptive resistance to trastuzumab impairs response to neratinib and lapatinib through deregulation of cell death mechanisms. Cancer Lett. 2020, 470, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Scaltriti, M.; Verma, C.; Guzman, M.; Jimenez, J.; Parra, J.L.; Pedersen, K.; Smith, D.J.; Landolfi, S.; Cajal, S.R.Y.; Arribas, J.; et al. Lapatinib, a HER2 tyrosine kinase inhibitor, induces stabilization and accumulation of HER2 and potentiates trastuzumab-dependent cell cytotoxicity. Oncogene 2009, 28, 803–814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomez, H.L.; Doval, D.C.; Chavez, M.A.; Ang, P.C.; Aziz, Z.; Nag, S.; Ng, C.; Franco, S.X.; Chow, L.W.; Arbushites, M.C.; et al. Efficacy and safety of lapatinib as first-line therapy for ErbB2-amplified locally advanced or metastatic breast cancer. J. Clin. Oncol. 2008, 26, 2999–3005. [Google Scholar] [CrossRef] [PubMed]
- Johnston, S.; Trudeau, M.; Kaufman, B.; Boussen, H.; Blackwell, K.; LoRusso, P.; Lombardi, D.P.; Ben, A.S.; Citrin, D.L.; DeSilvio, M.L.; et al. Phase II study of predictive biomarker profiles for response targeting human epidermal growth factor receptor 2 (HER-2) in advanced inflammatory breast cancer with lapatinib monotherapy. J. Clin. Oncol. 2008, 26, 1066–1072. [Google Scholar] [CrossRef] [PubMed]
- Blackwell, K.L.; Burstein, H.J.; Storniolo, A.M.; Rugo, H.; Sledge, G.; Koehler, M.; Ellis, C.; Casey, M.; Vukelja, S.; Bischoff, J.; et al. Randomized study of Lapatinib alone or in combination with trastuzumab in women with ErbB2-positive, trastuzumab-refractory metastatic breast cancer. J. Clin. Oncol. 2010, 28, 1124–1130. [Google Scholar] [CrossRef]
- Maruyama, T.; Mimura, K.; Izawa, S.; Inoue, A.; Shiba, S.; Watanabe, M.; Kawaguchi, Y.; Inoue, M.; Nogata, H.; Inoue, S.; et al. Lapatinib enhances herceptin-mediated antibody-dependent cellular cytotoxicity by up-regulation of cell surface HER2 expression. Anticancer Res. 2011, 31, 2999–3005. [Google Scholar] [PubMed]
- Cocco, E.; Javier, C.F.; Razavi, P.; Won, H.H.; Cai, Y.; Rossi, V.; Chan, C.; Cownie, J.; Soong, J.; Toska, E.; et al. Neratinib is effective in breast tumors bearing both amplification and mutation of ERBB2 (HER2). Sci. Signal. 2018, 11, eaat9773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.W.; Liu, M.C.; Yee, D.; Yau, C.; van’t Veer, L.J.; Symmans, W.F.; Paoloni, M.; Perlmutter, J.; Hylton, N.M.; Hogarth, M.; et al. Adaptive randomization of neratinib in early breast cancer. N. Engl. J. Med. 2016, 375, 11–22. [Google Scholar] [CrossRef]
- Collins, D.M.; Conlon, N.T.; Kannan, S.; Verma, C.S.; Eli, L.D.; Lalani, A.S.; Crown, J. Preclinical characteristics of the irreversible pan-HER kinase inhibitor neratinib compared with lapatinib: Implications for the treatment of HER2-positive and HER2-mutated breast cancer. Cancers 2019, 11, 737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, D.M.; Gately, K.; Hughes, C.; Edwards, C.; Davies, A.; Madden, S.F.; O’Byrne, K.J.; O’Donovan, N.; Crown, J. Tyrosine kinase inhibitors as modulators of trastuzumab-mediated antibody-dependent cell-mediated cytotoxicity in breast cancer cell lines. Cell Immunol. 2017, 319, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Connell, C.M.; Doherty, G.J. Activating HER2 mutations as emerging targets in multiple solid cancers. ESMO Open 2017, 2, e000279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.Y.; Park, K.; Im, S.A.; Jung, K.H.; Sohn, J.; Lee, K.S.; Kim, J.H.; Yang, Y.; Park, Y.H. Clinical implications of HER2 mRNA expression and intrinsic subtype in refractory HER2-positive metastatic breast cancer treated with pan-HER inhibitor, poziotinib. Breast Cancer Res. Treat. 2020, 184, 743–753. [Google Scholar] [CrossRef]
- Robichaux, J.P.; Elamin, Y.Y.; Vijayan, R.S.K.; Nilsson, M.B.; Hu, L.; He, J.; Zhang, F.; Pisegna, M.; Poteete, A.; Sun, H.; et al. Pan-cancer landscape and analysis of ERBB2 mutations identifies poziotinib as a clinically active inhibitor and enhancer of T-DM1 activity. Cancer Cell 2019, 36, 444–457. [Google Scholar] [CrossRef]
- Park, Y.H.; Lee, K.H.; Sohn, J.H.; Lee, K.S.; Jung, K.H.; Kim, J.H.; Lee, K.H.; Ahn, J.S.; Kim, T.Y.; Kim, G.M.; et al. A phase II trial of the pan-HER inhibitor poziotinib, in patients with HER2-positive metastatic breast cancer who had received at least two prior HER2-directed regimens: Results of the NOV120101-203 trial. Int. J. Cancer 2018, 143, 3240–3247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.Y.; Lee, E.; Park, K.; Jung, H.H.; Park, W.Y.; Lee, K.H.; Sohn, J.; Lee, K.S.; Jung, K.H.; Kim, J.H.; et al. Molecular alterations and poziotinib efficacy, a pan-HER inhibitor, in human epidermal growth factor receptor 2 (HER2)-positive breast cancers: Combined exploratory biomarker analysis from a phase II clinical trial of poziotinib for refractory HER2-positive breast cancer patients. Int. J. Cancer 2019, 145, 1669–1678. [Google Scholar]
- Simmons, C.; Rayson, D.; Joy, A.A.; Henning, J.W.; Lemieux, J.; McArthur, H.; Card, P.B.; Dent, R.; Brezden-Masley, C. Current and future landscape of targeted therapy in HER2-positive advanced breast cancer: Redrawing the lines. Ther. Adv. Med. Oncol. 2022, 14, 17588359211066677. [Google Scholar] [CrossRef] [PubMed]
- Yi, Z.; Rong, G.; Guan, Y.; Li, J.; Chang, L.; Li, H.; Liu, B.; Wang, W.; Guan, X.; Ouyang, Q.; et al. Molecular landscape and efficacy of HER2-targeted therapy in patients with HER2-mutated metastatic breast cancer. NPJ Breast Cancer 2020, 6, 59. [Google Scholar] [CrossRef]
- Haque, M.M.; Desai, K.V. Pathways to endocrine therapy resistance in breast cancer. Front. Endocrinol. 2019, 10, 573. [Google Scholar] [CrossRef]
- Hasson, S.P.; Rubinek, T.; Ryvo, L.; Wolf, I. Endocrine resistance in breast cancer: Focus on the phosphatidylinositol 3-kinase/akt/mammalian target of rapamycin signaling pathway. Breast Care 2013, 8, 248–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miranda, F.; Prazeres, H.; Mendes, F.; Martins, D.; Schmitt, F. Resistance to endocrine therapy in HR+ and/or HER2+ breast cancer: The most promising predictive biomarkers. Mol. Biol. Rep. 2022, 49, 717–733. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Sun, M.M.; Zhang, G.G.; Yang, J.; Chen, K.S.; Xu, W.W.; Li, B. Targeting PI3K/Akt signal transduction for cancer therapy. Signal Transduct. Target. Ther. 2021, 6, 425. [Google Scholar] [CrossRef] [PubMed]
- Vuylsteke, P.; Huizing, M.; Petrakova, K.; Roylance, R.; Laing, R.; Chan, S.; Abell, F.; Gendreau, S.; Rooney, I.; Apt, D.; et al. Pictilisib PI3Kinase inhibitor (a phosphatidylinositol 3-kinase [PI3K] inhibitor) plus paclitaxel for the treatment of hormone receptor-positive, HER2-negative, locally recurrent, or metastatic breast cancer: Interim analysis of the multicentre, placebo-controlled, phase II randomised PEGGY study. Ann. Oncol. 2016, 27, 2059–2066. [Google Scholar] [PubMed]
- Mayer, I.A.; Abramson, V.G.; Formisano, L.; Balko, J.M.; Estrada, M.V.; Sanders, M.E.; Juric, D.; Solit, D.; Berger, M.F.; Won, H.H. A Phase Ib Study of Alpelisib (BYL719), a PI3Kα-Specific Inhibitor, with Letrozole in ER+/HER2- Metastatic Breast CancerAlpelisib and Letrozole in ER+ Metastatic Breast Cancer. Clin. Cancer Res. 2017, 23, 26–34. [Google Scholar] [CrossRef] [Green Version]
- André, F.; Ciruelos, E.; Rubovszky, G.; Campone, M.; Loibl, S.; Rugo, H.S.; Iwata, H.; Conte, P.; Mayer, I.A.; Kaufman, B.; et al. Alpelisib for PIK3CA-mutated, hormone receptor–positive advanced breast cancer. Lancet Oncol. 2019, 380, 1929–1940. [Google Scholar] [CrossRef] [PubMed]
- Mayer, I.A.; Prat, A.; Egle, D.; Blau, S.; Fidalgo, J.; Gnant, M.; Fasching, P.A.; Colleoni, M.; Wolff, A.C.; Winer, E.P.; et al. A Phase II Randomized Study of Neoadjuvant Letrozole Plus Alpelisib for Hormone Receptor-Positive, Human Epidermal Growth Factor Receptor 2-Negative Breast Cancer (NEO-ORB) Neoadjuvant Letrozole Plus Alpelisib for Breast Cancer. Clin. Cancer Res. 2019, 25, 2975–2987. [Google Scholar] [CrossRef] [Green Version]
- Juric, D.; Janku, F.; Rodón, J.; Burris, H.A.; Mayer, I.A.; Schuler, M.; Seggewiss-Bernhardt, R.; Gil-Martin, M.; Middleton, M.R.; Baselga, J.; et al. Alpelisib plus fulvestrant in PIK3CA-altered and PIK3CA-wild-type estrogen receptor–positive advanced breast cancer: A phase 1b clinical trial. JAMA Oncol. 2019, 5, e184475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, P.; Abramson, V.G.; O’Dea, A.; Nye, L.; Mayer, I.; Pathak, H.B.; Hoffmann, M.; Stecklein, S.R.; Elia, M.; Lewis, S.; et al. Clinical and biomarker results from Phase I/II study of PI3K inhibitor, BYL719 (Alpelisib) plus Nab-paclitaxel in HER2 negative metastatic breast cancer. Clin. Cancer Res. 2021, 27, 3896–3904. [Google Scholar] [CrossRef]
- Iksen; Pothongsrisit, S.; Pongrakhananon, V. Targeting the PI3K/AKT/mTOR signaling pathway in lung cancer: An update regarding potential drugs and natural products. Molecules 2021, 26, 4100. [Google Scholar] [CrossRef]
- Prêtre, V.; Wicki, A. Inhibition of Akt and other AGC kinases: A target for clinical cancer therapy? Semin. Cancer Biol. 2018, 48, 70–77. [Google Scholar] [CrossRef]
- Alzahrani, A.S. PI3K/Akt/mTOR inhibitors in cancer: At the bench and bedside. Semin. Cancer Biol. 2019, 59, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Sangai, T.; Akcakanat, A.; Chen, H.; Tarco, E.; Wu, Y.; Do, K.A.; Miller, T.W.; Arteaga, C.L.; Mills, G.B.; Gonzalez-Angulo, A.M.; et al. Biomarkers of Response to Akt Inhibitor MK-2206 in Breast CancerAntitumor Activity of MK-2206. Clin. Cancer Res. 2012, 18, 5816–5828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xing, Y.; Lin, N.U.; Maurer, M.A.; Chen, H.; Mahvash, A.; Sahin, A.; Akcakanat, A.; Li, Y.; Abramson, V.; Litton, J.; et al. Phase II trial of AKT inhibitor MK-2206 in pat.tients with advanced breast cancer who have tumors with PIK3CA or AKT mutations, and/or PTEN loss/PTEN mutation. Breast Cancer Res. 2019, 21, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, B.R.; Greenwood, H.; Dudley, P.; Crafter, C.; Yu, D.H.; Zhang, J.; Li, J.; Gao, B.; Ji, Q.; Maynard, J.; et al. Preclinical Pharmacology of AZD5363, an Inhibitor of AKT: Pharmacodynamics, Antitumor Activity, and Correlation of Monotherapy Activity with Genetic BackgroundAZD5363, an Oral Inhibitor of AKT. Mol. Cancer Ther. 2012, 11, 873–887. [Google Scholar] [CrossRef] [Green Version]
- Turner, N.C.; Alarcón, E.; Armstrong, A.C.; Philco, M.; Chuken, Y.; Sablin, M.P.; Tamura, K.; Villanueva, A.; Perez-Fidalgo, J.A.; Cheung, S.Y.A.; et al. BEECH: A dose-finding run-in followed by a randomised phase II study assessing the efficacy of AKT inhibitor capivasertib (AZD5363) combined with paclitaxel in patients with estrogen receptor-positive advanced or metastatic breast cancer, and in a PIK3CA mutant sub-population. Ann. Oncol. 2019, 30, 774–780. [Google Scholar]
- Schmid, P.; Abraham, J.; Chan, S.; Wheatley, D.; Brunt, A.M.; Nemsadze, G.; Baird, R.D.; Park, Y.H.; Hall, P.S.; Perren, T.; et al. Capivasertib plus paclitaxel versus placebo plus paclitaxel as first-line therapy for metastatic triple-negative breast cancer: The PAKT trial. J. Clin. Oncol. 2020, 38, 423–433. [Google Scholar] [CrossRef]
- Oliveira, M.; Saura, C.; Nuciforo, P.; Calvo, I.; Andersen, J.; Passos-Coelho, J.L.; Gil, G.M.; Bermejo, B.; Patt, D.A.; Ciruelos, E.; et al. FAIRLANE, a double-blind placebo-controlled randomized phase II trial of neoadjuvant ipatasertib plus paclitaxel for early triple-negative breast cancer. Ann. Oncol. 2019, 30, 1289–1297. [Google Scholar] [CrossRef]
- Schmid, P.; Cortes, J.; Robson, M.; Iwata, H.; Hegg, R.; Verma, S.; Nechaeva, M.; Xu, B.; Haddad, V.; Imedio, E.R.; et al. Abstract OT2-08-02: Capivasertib and paclitaxel in first-line treatment of patients with metastatic triple-negative breast cancer: A phase III trial (CAPItello-290). Cancer Res. 2020, 80 (Suppl. S4), OT2-08. [Google Scholar] [CrossRef]
- Kim, S.B.; Dent, R.; Im, S.A.; Espié, M.; Blau, S.; Tan, A.R.; Isakoff, S.J.; Oliveira, M.; Saura, C.; Wongchenko, M.J.; et al. Ipatasertib plus paclitaxel versus placebo plus paclitaxel as first-line therapy for metastatic triple-negative breast cancer (LOTUS): A multicentre, randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Oncol. 2017, 18, 1360–1372. [Google Scholar] [CrossRef]
- Martorana, F.; Motta, G.; Pavone, G.; Motta, L.; Stella, S.; Vitale, S.R.; Manzella, L.; Vigneri, P. AKT inhibitors: New weapons in the fight against breast cancer? Front. Pharmacol. 2021, 12, 662232. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.D.; Payne, K.K.; Posey, A.D.; Hill, C.; Conejo-Garcia, J.; June, C.H.; Tchou, J. Immunotherapy for breast cancer: Current and future strategies. Curr. Surg. Rep. 2017, 5, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Awadhi, A.; Lee Murray, J.; Ibrahim, N. Developing anti-HER 2 vaccines: B reast cancer experience. Int. J. Cancer 2018, 143, 2126–2132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arab, A.; Yazdian-Robati, R.; Behravan, J. HER2-positive breast cancer immunotherapy: A focus on vaccine development. Arch. Immunol. Ther. Exp. 2020, 68, 2. [Google Scholar] [CrossRef] [PubMed]
- Peoples, G.E.; Holmes, J.P.; Hueman, M.T.; Mittendorf, E.A.; Amin, A.; Khoo, S.; Dehqanzada, Z.A.; Gurney, J.M.; Woll, M.M.; Ryan, G.B.; et al. Combined clinical trial results of a HER2/neu (E75) vaccine for the prevention of recurrence in high-risk breast cancer patients: U.S. Military Cancer Institute Clinical Trials Group Study I-01 and I-02. Clin. Cancer Res. 2008, 14, 797–803. [Google Scholar] [CrossRef] [Green Version]
- Benavides, L.C.; Gates, J.D.; Carmichael, M.G.; Patil, R.; Holmes, J.P.; Hueman, M.T.; Mittendorf, E.A.; Craig, D.; Stojadinovic, A.; Ponniah, S.; et al. The impact of HER2/neu expression level on response to the E75 vaccine: From US Military Cancer Institute Clinical Trials Group Study I-01 and I-02. Clin. Cancer Res. 2009, 15, 2895–2904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peoples, G.E.; Gurney, J.M.; Hueman, M.T.; Woll, M.M.; Ryan, G.B.; Storrer, C.E.; Fisher, C.; Shriver, C.D.; Ioannides, C.G.; Ponniah, S. Clinical trial results of a HER2/neu (E75) vaccine to prevent recurrence in high-risk breast cancer patients. J. Clin. Oncol. 2005, 23, 7536–7545. [Google Scholar] [CrossRef] [PubMed]
- Mittendorf, E.A.; Clifton, G.T.; Holmes, J.P.; Schneble, E.; van Echo, D.; Ponniah, S.; Peoples, G.E. Final report of the phase I/II clinical trial of the E75 (nelipepimut-S) vaccine with booster inoculations to prevent disease recurrence in high-risk breast cancer patients. Ann. Oncol. 2014, 25, 1735–1742. [Google Scholar] [CrossRef]
- Mittendorf, E.A.; Lu, B.; Melisko, M.; Price Hiller, J.; Bondarenko, I.; Brunt, A.M.; Sergii, G.; Petrakova, K.; Peoples, G.E. Efficacy and Safety Analysis of Nelipepimut-S Vaccine to Prevent Breast Cancer Recurrence: A Randomized, Multicenter, Phase III Clinical Trial Randomized Phase III Trial of Nelipepimut-S in Breast Cancer. Clin. Cancer Res. 2019, 25, 4248–4254. [Google Scholar] [CrossRef] [Green Version]
- Mittendorf, E.A.; Ardavanis, A.; Litton, J.K.; Shumway, N.M.; Hale, D.F.; Murray, J.L.; Perez, S.A.; Ponniah, S.; Baxevanis, C.N.; Papamichail, M.; et al. Primary analysis of a prospective, randomized, single-blinded phase II trial evaluating the HER2 peptide GP2 vaccine in breast cancer patients to prevent recurrence. Oncotarget 2016, 7, 66192. [Google Scholar] [CrossRef] [Green Version]
- Clifton, G.T.; Hale, D.; Vreeland, T.J.; Hickerson, A.T.; Litton, J.K.; Alatrash, G.; Murthy, R.K.; Qiao, N.; Philips, A.V.; Lukas, J.J.; et al. Results of a Randomized Phase IIb Trial of Nelipepimut-S+ Trastuzumab versus Trastuzumab to Prevent Recurrences in Patients with High-Risk HER2 Low-Expressing Breast CancerPhase IIb Breast Cancer Trial of Nelipepimut-S+ Trastuzumab. Clin. Cancer Res. 2020, 26, 2515–2523. [Google Scholar] [CrossRef] [Green Version]
- McCarthy, P.M.; Clifton, G.T.; Vreeland, T.J.; Adams, A.M.; O’Shea, A.E.; Peoples, G.E. AE37: A HER2-targeted vaccine for the prevention of breast cancer recurrence. Exp. Opin. Investig. Drugs 2021, 30, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Mittendorf, E.A.; Ardavanis, A.; Symanowski, J.; Murray, J.L.; Shumway, N.M.; Litton, J.K.; Hale, D.F.; Perez, S.A.; Anastasopoulou, E.A.; Pistamaltzian, N.F.; et al. Primary analysis of a prospective, randomized, single-blinded phase II trial evaluating the HER2 peptide AE37 vaccine in breast cancer patients to prevent recurrence. Ann. Oncol. 2016, 27, 1241–1248. [Google Scholar] [CrossRef] [PubMed]
- Stephen, T.L.; Payne, K.K.; Chaurio, R.A.; Allegrezza, M.J.; Zhu, H.; Perez-Sanz, J.; Perales-Puchalt, A.; Nguyen, J.M.; Vara-Ailor, A.E.; Eruslanov, E.B.; et al. SATB1 expression governs epigenetic repression of PD-1 in tumor-reactive T cells. Immunity 2017, 46, 51–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curdy, N.; Lanvin, O.; Laurent, C.; Fournié, J.J.; Franchini, D.M. Regulatory mechanisms of inhibitory immune checkpoint receptors expression. Trends Cell Biol. 2019, 29, 777–790. [Google Scholar] [CrossRef] [PubMed]
- Bozeman, E.N.; He, S.; Shafizadeh, Y.; Selvaraj, P. Therapeutic efficacy of PD-L1 blockade in a breast cancer model is enhanced by cellular vaccines expressing B7-1 and glycolipid-anchored IL-12. Hum. Vaccin Immunother. 2016, 12, 421–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanda, R.; Chow, L.Q.; Dees, E.C.; Berger, R.; Gupta, S.; Geva, R.; Pusztai, L.; Pathiraja, K.; Aktan, G.; Cheng, J.D.; et al. Pembrolizumab in patients with advanced triple-negative breast cancer: Phase Ib KEYNOTE-012 study. J. Clin. Oncol. 2016, 34, 2460. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.; Lee, S.H.; Ejadi, S.; Even, C.; Cohen, R.B.; Le Tourneau, C.; Mehnert, J.M.; Algazi, A.; van Brummelen, E.M.J.; Saraf, S.; et al. Safety and antitumor activity of pembrolizumab in patients with programmed death-ligand 1–positive nasopharyngeal carcinoma: Results of the KEYNOTE-028 study. Clin. Cancer Res. 2017, 35, 4050–4056. [Google Scholar] [CrossRef]
- Adams, S.; Diamond, J.R.; Hamilton, E.P.; Pohlmann, P.R.; Tolaney, S.M.; Molinero, L.; He, X.; Waterkamp, D.; Funke, R.P.; Powderly, J.D. Phase Ib trial of atezolizumab in combination with nab-paclitaxel in patients with metastatic triple-negative breast cancer (mTNBC). J. Clin. Oncol. 2020, 34, 1009. [Google Scholar] [CrossRef]
- Adams, S.; Othus, M.; Patel, S.P.; Miller, K.D.; Chugh, R.; Schuetze, S.M.; Chamberlin, M.D.; Haley, B.J.; Storniolo, A.M.V.; Reddy, M.P.; et al. A Multicenter Phase II Trial of Ipilimumab and Nivolumab in Unresectable or Metastatic Metaplastic Breast Cancer: Cohort 36 of Dual Anti–CTLA-4 and Anti–PD-1 Blockade in Rare Tumors (DART, SWOG S1609) Ipilimumab and Nivolumab in Rare Tumors S1609: Metaplastic. Clin. Cancer Res. 2022, 28, 271–278. [Google Scholar] [PubMed]
- Hamilton, E.; Shapiro, C.L.; Petrylak, D.; Boni, V.; Martin, M.; Conte, G.D.; Cortes, J.; Agarwal, L.; Arkenau, H.T.; Tan, A.R.; et al. Abstract PD3-07: Trastuzumab deruxtecan (T-DXd; DS-8201) with nivolumab in patients with HER2-expressing, advanced breast cancer: A 2-part, phase 1b, multicenter, open-label study. Cancer Res. 2021, 81 (Suppl. S4), PD3-07. [Google Scholar] [CrossRef]
- Müller, P.; Kreuzaler, M.; Khan, T.; Thommen, D.S.; Martin, K.; Glatz, K.; Savic, S.; Harbeck, N.; Nitz, U.; Gluz, O.; et al. Trastuzumab emtansine (T-DM1) renders HER2+ breast cancer highly susceptible to CTLA-4/PD-1 blockade. Sci. Transl. Med. 2015, 7, 315ra188. [Google Scholar] [CrossRef]
- Powles, T.; van der Heijden, M.S.; Castellano, D.; Galsky, M.D.; Loriot, Y.; Petrylak, D.P.; Ogawa, O.; Park, S.H.; Lee, J.L.; De Giorgi, U.; et al. Durvalumab alone and durvalumab plus tremelimumab versus chemotherapy in previously untreated patients 860 with unresectable, locally advanced or metastatic urothelial carcinoma (DANUBE): A randomised, open-label, multicentre, phase 3 trial. Lancet Oncol. 2020, 21, 1574–1588. [Google Scholar] [CrossRef]
- Peter, S.; Seock-Ah, I.; Anne, A.; Yeon, H.P.; Wei-Pang, C.; Zbigniew, N.; Simon, L.; Piotr, J.W.; Yen-Shen, L.; Hannah, D.; et al. BEGONIA: Phase 1b/2 study of durvalumab (D) combinations in locally advanced/metastatic triple-negative breast cancer (TNBC)—Initial results from arm 1, d+ paclitaxel (P), and arm 6, d+ trastuzumab deruxtecan (T-DXd). J. Clin. Oncol. 2020, 39, 15. [Google Scholar]
- Borghaei, H.; Besse, B.; Bardia, A.; Mazieres, J.; Popat, S.; Augustine, B.; D’amelio, A.M.; Barrios, D.; Rugo, H.S. Trastuzumab deruxtecan (T-DXd; DS-8201) in combination with pembrolizumab in patients with advanced/metastatic breast or non-small cell lung cancer (NSCLC): A phase Ib, multicenter, study. J. Clin. Oncol. 2020, 38, 15. [Google Scholar] [CrossRef]
- Marchiò, C.; Annaratone, L.; Marques, A.; Casorzo, L.; Berrino, E.; Sapino, A. Evolving concepts in HER2 evaluation in breast cancer: Heterogeneity, HER2-low carcinomas and beyond. Semin. Cancer Biol. 2021, 72, 123–135. [Google Scholar] [CrossRef]
- Rasmussen, B.B.; Regan, M.M.; Lykkesfeldt, A.E.; Dell’Orto, P.; Del Curto, B.; Henriksen, K.L.; Mastropasqua, M.G.; Price, K.N.; Méry, E.; Lacroix-Triki, M.; et al. Adjuvant letrozole versus tamoxifen according to centrally-assessed ERBB2 status for postmenopausal women with endocrine-responsive early breast cancer: Supplementary results from the BIG 1-98 randomised trial. Lancet Oncol. 2008, 9, 23–28. [Google Scholar] [CrossRef]
- Bartlett, J.; Ahmed, I.; Regan, M.M.; Sestak, I.; Mallon, E.A.; Dell’Orto, P.; Thürlimann, B.; Seynaeve, C.; Putter, H.; Van de Velde, C.; et al. HER2 status predicts for upfront AI benefit: A TRANS-AIOG meta-analysis of 12, 129 patients from ATAC, BIG 1-98 and TEAM with centrally determined HER2. Eur. J. Cancer 2017, 79, 129–138. [Google Scholar] [CrossRef]
- Schiza, A.; Mauri, D.; Fredriksson, I.; Anna-Karin, W.; Valachis, A. Predictive role of HER2-status on the effectiveness of endocrine adjuvant treatment in postmenopausal breast cancer patients: A population-based cohort study. Breast Cancer Res. Treat. 2021, 186, 779–789. [Google Scholar] [CrossRef]
- Taskaynatan, H.; Kucukzeybek, Y.; Alacacioglu, A.; Yildiz, Y.; Salman, T.; Oflazoglu, U.; Varol, U.; Bolat, K.B.; Kemal, A.M.; Oktay, T.M. Is adjuvant chemotherapy necessary for Luminal A-like breast cancer. J. BUON 2018, 23, 877–882. [Google Scholar]
- Goel, S.; De Cristo, M.J.; McAllister, S.S.; Zhao, J.J. CDK4/6 inhibition in cancer: Beyond cell cycle arrest. Trends Cell Biol. 2018, 28, 911–925. [Google Scholar] [CrossRef]
- Lloyd, M.R.; Spring, L.M.; Bardia, A.; Wander, S.A. Mechanisms of Resistance to CDK4/6 Blockade in Advanced Hormone Receptor–positive, HER2-negative Breast Cancer and Emerging Therapeutic Opportunities. Clin. Cancer Res. 2022, 28, 821–830. [Google Scholar] [CrossRef]
- Finn, R.S.; Crown, J.P.; Lang, I.; Boer, K.; Bondarenko, I.M.; Kulyk, S.O.; Ettl, J.; Patel, R.; Pinter, T.; Schmidt, M.; et al. The cyclin-dependent kinase 4/6 inhibitor palbociclib in combination with letrozole versus letrozole alone as first-line treatment of oestrogen receptor-positive, HER2-negative, advanced breast cancer (PALOMA-1/TRIO-18): A randomised phase 2 study. Lancet Oncol. 2015, 26, 25–35. [Google Scholar] [CrossRef]
- Finn, R.S.; Martin, M.; Rugo, H.S.; Jones, S.; Im, S.A.; Gelmon, K.; Harbeck, N.; Lipatov, O.N.; Walshe, J.M.; Moulder, S.; et al. Palbociclib and letrozole in advanced breast cancer. N. Engl. J. Med. 2016, 375, 1925–1936. [Google Scholar] [CrossRef] [PubMed]
- Turner, N.C.; Slamon, D.J.; Ro, J.; Bondarenko, I.; Im, S.A.; Masuda, N.; Colleoni, M.; DeMichele, A.; Loi, S.; Verma, S.; et al. Overall survival with palbociclib and fulvestrant in advanced breast cancer. N. Engl. J. Med. 2018, 379, 1926–1936. [Google Scholar] [CrossRef]
- Dickler, M.N.; Tolaney, S.M.; Rugo, H.S.; Cortés, J.; Diéras, V.; Patt, D.; Wildiers, H.; Hudis, C.A.; O’Shaughnessy, J.; Zamora, E.; et al. MONARCH 1, A Phase II Study of Abemaciclib, a CDK4 and CDK6 Inhibitor, as a Single Agent, in Patients with Refractory HR+/HER2- Metastatic Breast CancerPhase II Study of Abemaciclib in HR+/HER2- MBC. Clin. Cancer Res. 2017, 23, 5218–5224. [Google Scholar] [CrossRef] [Green Version]
- Sledge, G.W.; Toi, M., Jr.; Neven, P.; Sohn, J.; Inoue, K.; Pivot, X.; Burdaeva, O.; Okera, M.; Masuda, N.; Kaufman, P.A.; et al. MONARCH 2: Abemaciclib in combination with fulvestrant in women with HR+/HER2- advanced breast cancer who had progressed while receiving endocrine therapy. J. Clin. Oncol. 2017, 35, 2875–2884. [Google Scholar] [CrossRef]
- Hortobagyi, G.N.; Stemmer, S.M.; Burris, H.A.; Yap, Y.S.; Sonke, G.S.; Paluch-Shimon, S.; Campone, M.; Petrakova, K.; Blackwell, K.L.; Winer, E.P.; et al. Updated results from MONALEESA-2, a phase III trial of first-line ribociclib plus letrozole versus placebo plus letrozole in hormone receptor-positive, HER2-negative advanced breast cancer. Lancet Oncol. 2018, 29, 1541–1547. [Google Scholar] [CrossRef]
- Slamon, D.J.; Neven, P.; Chia, S.; Fasching, P.A.; De Laurentiis, M.; Im, S.A.; Petrakova, K.; Bianchi, G.V.; Esteva, F.J.; Martín, M. Overall survival with ribociclib plus fulvestrant in advanced breast cancer. N. Engl. J. Med. 2020, 382, 514–524. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wang, Q.; Wang, Q.; Cao, J.; Sun, J.; Zhu, Z. Mechanisms of resistance to estrogen receptor modulators in ER+/HER2-advanced breast cancer. Cell Mol. Life Sci. 2020, 77, 559–572. [Google Scholar] [CrossRef] [PubMed]
- Bao, K.; Sutanto, L.; Tse, S.; Man Cheung, K.; Chan, J. The association of ERBB2-low expression with the efficacy of cyclin-dependent kinase 4/6 inhibitor in hormone receptor–positive, ERBB2-negative metastatic breast cancer. JAMA Netw. Open 2021, 4, e2133132. [Google Scholar] [CrossRef] [PubMed]
- Schneeweiss, A.; Park-Simon, T.W.; Albanell, J.; Lassen, U.; Cortés, J.; Dieras, V.; May, M.; Schindler, C.; Marmé, F.; Cejalvo, J.M.; et al. Phase Ib study evaluating safety and cli.inical activity of the anti-HER3 antibody lumretuzumab combined with the anti-HER2 antibody pertuzumab and paclitaxel in HER3-positive, HER2-low metastatic breast cancer. Investig. New Drugs 2018, 36, 848–859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Vries Schultink, A.; Doornbos, R.P.; Bakker, A.; Bol, K.; Throsby, M.; Geuijen, C.; Maussang, D.; Schellens, J.; Beijnen, J.H.; Huitema, A.D. Translational PK-PD modeling analysis of MCLA-128, a HER2/HER3 bispecific monoclonal antibody, to predict 918 clinical efficacious exposure and dose. Investig. New Drugs 2018, 36, 1006–1015. [Google Scholar] [CrossRef] [Green Version]
- Gianni, L.; Bisagni, G.; Colleoni, M.; Del Mastro, L.; Zamagni, C.; Mansutti, M.; Zambetti, M.; Frassoldati, A.; De Fato, R.; Valagussa, P.; et al. Neoadjuvant treatment with trastuzumab and pertuzumab plus palbociclib and fulvestrant in HER2-positive, ER-positive breast cancer (NA-PHER2): An exploratory, open-label, phase 2 study. Lancet Oncol. 2018, 19, 249–256. [Google Scholar] [CrossRef]
- Gianni, L.; Bisagni, G.; Colleoni, M.; Del Mastro, L.; Zamagni, C.; Mansutti, M.; Zambetti, M.; Frassoldati, A.; Barlera, S.; Valagussa, P.; et al. Ki67 during and after neoadjuvant trastuzumab, pertuzumab and palbociclib plus or minus fulvestrant in HER2 and ER-positive breast cancer: The NA- CPHER2 Michelangelo study. J. Clin. Oncol. 2019, 37, 527. [Google Scholar] [CrossRef]
- O’Brien, N.A.; McDermott, M.; Conklin, D.; Luo, T.; Ayala, R.; Salgar, S.; Chau, K.; DiTomaso, E.; Babbar, N.; Su, F.; et al. Targeting activated PI3K/mTOR signaling overcomes acquired resistance to CDK4/6-based therapies in preclinical models of hormone receptor-positive breast cancer. Breast Cancer Res. 2020, 22, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Reinert, T.; Sartori, G.P.; Souza, A.A.; Pellegrini, R.; Rosa, M.L.; Rossatto, N.; Coelho, G.P.; Litvin, I.E.; Zerwes, F.; Millen, E.; et al. Abstract PS4-22: Prevalence of HER2-low and HER2-zero subgroups and correlation with response to neoadjuvant chemotherapy (NACT) in patients with HER2-negative breast cancer. Cancer Res. 2021, 81 (Suppl. S4), PS4-22. [Google Scholar] [CrossRef]
- Tong, Y.; Chen, X.; Fei, X.; Lin, L.; Wu, J.; Huang, O.; He, J.; Zhu, L.; Chen, W.; Li, Y.; et al. Can breast cancer patients with HER2 dual-equivocal tumours be managed as HER2-negative disease? Eur. J. Cancer 2018, 89, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Richard, G.; Rosie, B.; Jeremy, B.; Zulian, L.; Richard, P.; Lucy, D.; David, D.; Paul, M.; Hongchao, P.; Carolyn, T.; et al. Increasing the dose intensity of chemotherapy by more frequent administration or sequential scheduling: A patient-level meta-analysis of 37298 women with early breast cancer in 26 randomised trials. Lancet 2019, 393, 1440–1452. [Google Scholar]
- Zambelli, A.; Simoncini, E.; Giordano, M.; La Verde, N.; Farina, G.; Torri, V.; Colombo, G.; Piacentini, G.; Fotia, V.; Vassalli, L.; et al. Prospective observational study on the impact of the 21-gene assay on treatment decisions and resources optimization in breast cancer patients in Lombardy: The BONDX study. Breast 2020, 52, 1–7. [Google Scholar] [CrossRef]
- Sparano, J.A.; Gray, R.J.; Makower, D.F.; Pritchard, K.I.; Albain, K.S.; Hayes, D.F.; Geyer, C.E.; Dees, E.C., Jr.; Perez, E.A.; Olson, J.A.; et al. Prospective validation of a 21-gene expression assay in breast cancer. N. Engl. J. Med. 2015, 373, 2005–2014. [Google Scholar] [CrossRef] [PubMed]
- Rugo, H.S.; Rumble, R.B.; Macrae, E.; Barton, D.L.; Connolly, H.K.; Dickler, M.N.; Fallowfield, L.; Fowble, B.; Ingle, J.N.; Jahanzeb, M.; et al. Endocrine therapy for hormone receptor-positive metastatic breast cancer: American Society of Clinical Oncology Guideline. J. Clin. Oncol. 2016, 34, 3069–3103. [Google Scholar] [CrossRef] [PubMed]
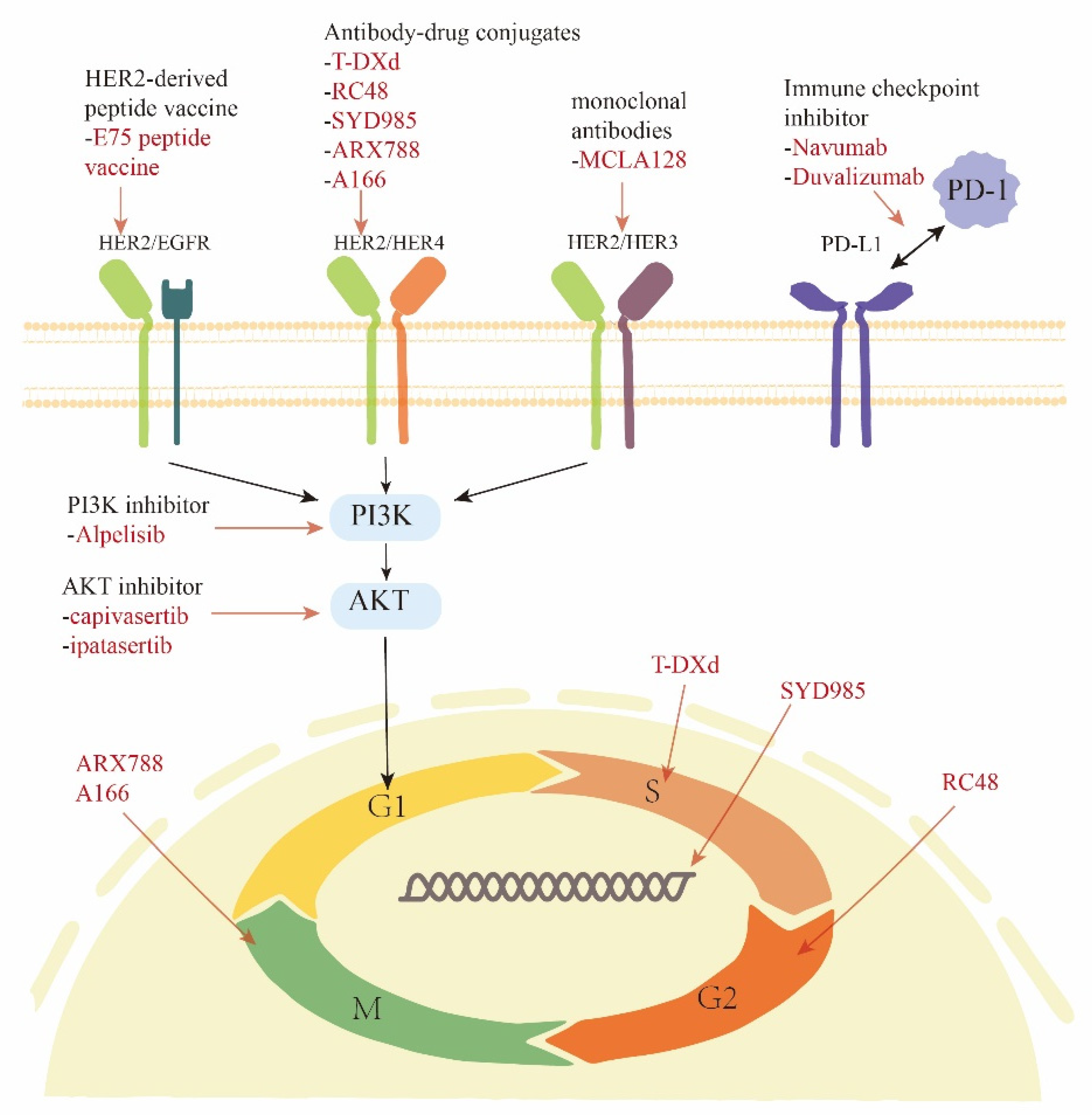
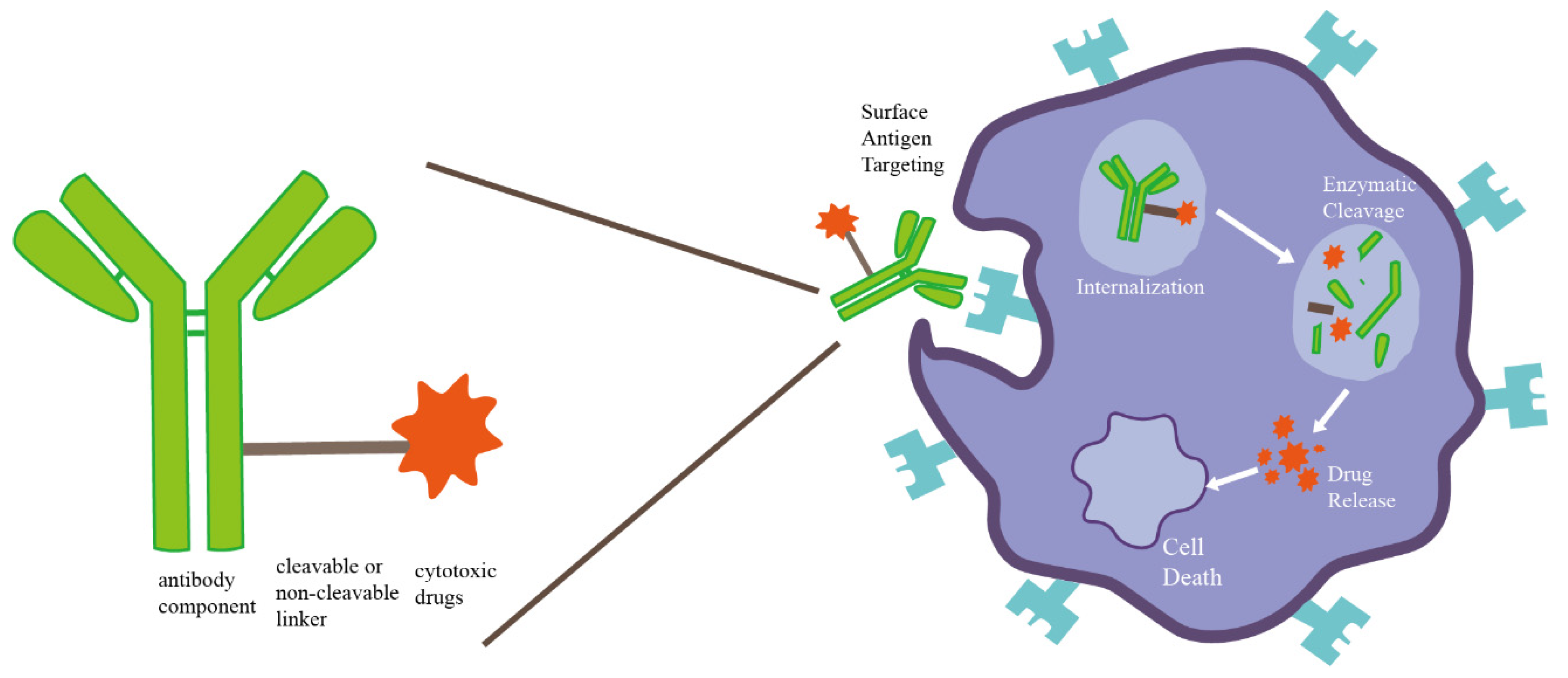
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).