
Relationship between Dose Prescription Methods and Local Control Rate in Stereotactic Body Radiotherapy for Early Stage Non-Small-Cell Lung Cancer: Systematic Review and Meta-Analysis

 , , and
, , and 
Abstract
:Simple Summary
Abstract
1. Introduction
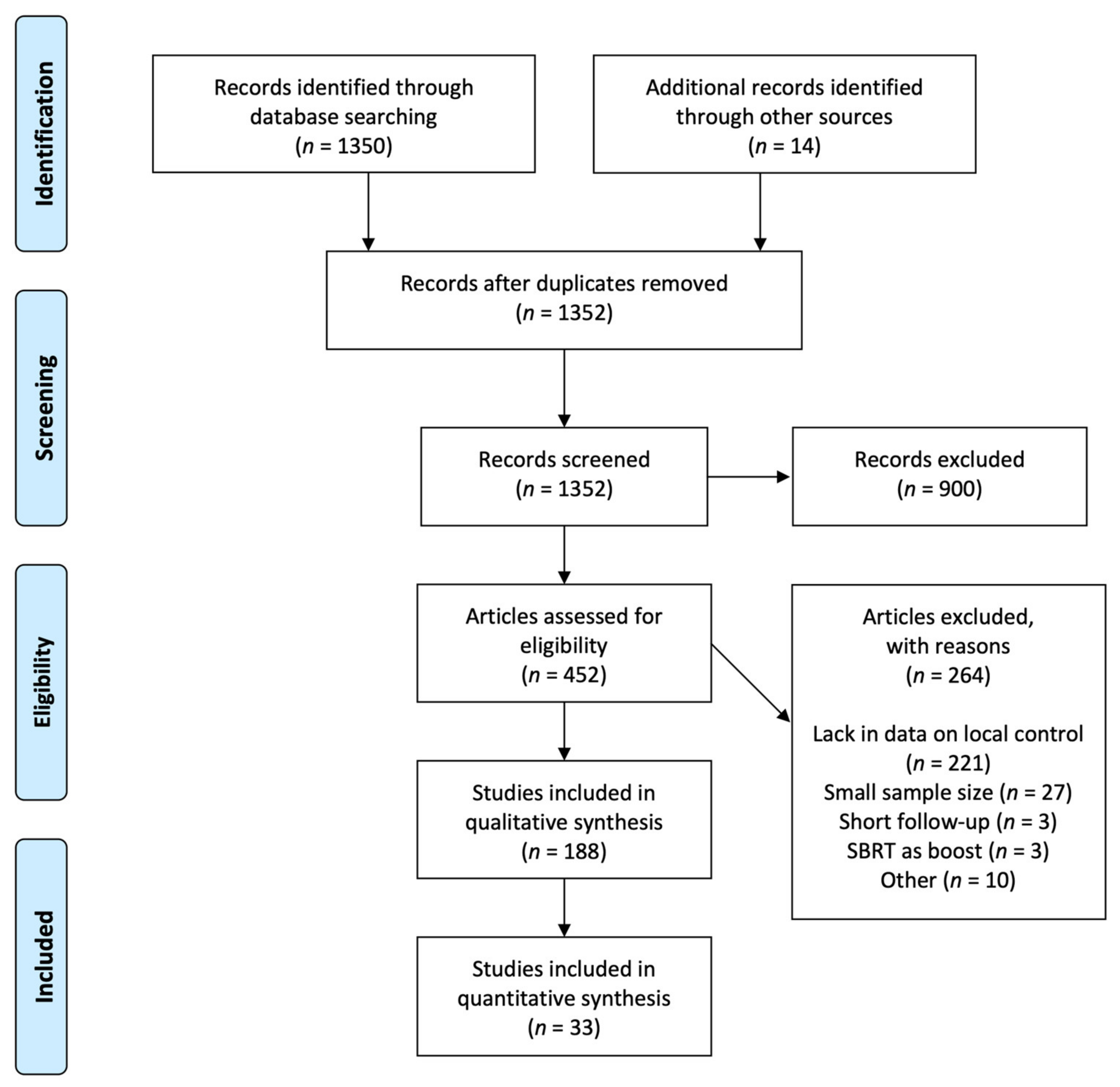
2. Materials and Methods
2.1. Study Overview
2.2. Study Selection and Design
2.3. Study Selection-Patients
2.4. Study Selection-Treatment
2.5. Study Search
2.6. Study Quality Assessment
2.7. Outcomes
2.8. Data Extraction
2.9. Statistics
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guckenberger, M.; Allgauer, M.; Appold, S.; Dieckmann, K.; Ernst, I.; Ganswindt, U.; Holy, R.; Nestle, U.; Nevinny-Stickel, M.; Semrau, S.; et al. Safety and efficacy of stereotactic body radiotherapy for stage 1 non-small-cell lung cancer in routine clinical practice: A patterns-of-care and outcome analysis. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2013, 8, 1050–1058. [Google Scholar] [CrossRef] [Green Version]
- Ricardi, U.; Frezza, G.; Filippi, A.R.; Badellino, S.; Levis, M.; Navarria, P.; Salvi, F.; Marcenaro, M.; Trovo, M.; Guarneri, A.; et al. Stereotactic Ablative Radiotherapy for stage I histologically proven non-small cell lung cancer: An Italian multicenter observational study. Lung Cancer 2014, 84, 248–253. [Google Scholar] [CrossRef]
- Nagata, Y.; Hiraoka, M.; Shibata, T.; Onishi, H.; Kokubo, M.; Karasawa, K.; Shioyama, Y.; Onimaru, R.; Kozuka, T.; Kunieda, E.; et al. Prospective Trial of Stereotactic Body Radiation Therapy for Both Operable and Inoperable T1N0M0 Non-Small Cell Lung Cancer: Japan Clinical Oncology Group Study JCOG0403. Int. J. Radiat. Oncol. Biol. Phys. 2015, 93, 989–996. [Google Scholar] [CrossRef] [PubMed]
- Haque, W.; Szeja, S.; Tann, A.; Kalra, S.; Teh, B.S. Changes in Treatment Patterns and Overall Survival in Patients with Early-Stage Non-Small Cell Lung Cancer in the United States After the Incorporation of Stereotactic Ablative Radiation Therapy: A Population-based Analysis. Am. J. Clin. Oncol. 2018, 41, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Dalwadi, S.M.; Szeja, S.S.; Bernicker, E.H.; Butler, E.B.; Teh, B.S.; Farach, A.M. Practice Patterns and Outcomes in Elderly Stage I Non-Small-cell Lung Cancer: A 2004 to 2012 SEER Analysis. Clin. Lung Cancer 2018, 19, e269–e276. [Google Scholar] [CrossRef] [PubMed]
- De Ruiter, J.C.; Heineman, D.J.; Daniels, J.M.; van Diessen, J.N.; Damhuis, R.A.; Hartemink, K.J. The role of surgery for stage I non-small cell lung cancer in octogenarians in the era of stereotactic body radiotherapy in The Netherlands. Lung Cancer 2020, 144, 64–70. [Google Scholar] [CrossRef]
- Diwanji, T.P.; Mohindra, P.; Vyfhuis, M.; Snider, J.W., 3rd; Kalavagunta, C.; Mossahebi, S.; Yu, J.; Feigenberg, S.; Badiyan, S.N. Advances in radiotherapy techniques and delivery for non-small cell lung cancer: Benefits of intensity-modulated radiation therapy, proton therapy, and stereotactic body radiation therapy. Transl. Lung Cancer Res. 2017, 6, 131–147. [Google Scholar] [CrossRef] [Green Version]
- Nagata, Y.; Hiraoka, M.; Mizowaki, T.; Narita, Y.; Matsuo, Y.; Norihisa, Y.; Onishi, H.; Shirato, H. Survey of stereotactic body radiation therapy in Japan by the Japan 3-D Conformal External Beam Radiotherapy Group. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 343–347. [Google Scholar] [CrossRef]
- Timmerman, R.; Paulus, R.; Galvin, J.; Michalski, J.; Straube, W.; Bradley, J.; Fakiris, A.; Bezjak, A.; Videtic, G.; Johnstone, D.; et al. Stereotactic body radiation therapy for inoperable early stage lung cancer. JAMA 2010, 303, 1070–1076. [Google Scholar] [CrossRef] [Green Version]
- Timmerman, R.D.; Paulus, R.; Pass, H.I.; Gore, E.M.; Edelman, M.J.; Galvin, J.; Straube, W.L.; Nedzi, L.A.; McGarry, R.C.; Robinson, C.G.; et al. Stereotactic Body Radiation Therapy for Operable Early-Stage Lung Cancer: Findings from the NRG Oncology RTOG 0618 Trial. JAMA Oncol. 2018, 4, 1263–1266. [Google Scholar] [CrossRef]
- Guckenberger, M.; Andratschke, N.; Dieckmann, K.; Hoogeman, M.S.; Hoyer, M.; Hurkmans, C.; Tanadini-Lang, S.; Lartigau, E.; Mendez Romero, A.; Senan, S.; et al. ESTRO ACROP consensus guideline on implementation and practice of stereotactic body radiotherapy for peripherally located early stage non-small cell lung cancer. Radiother. Oncol. 2017, 124, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Giglioli, F.R.; Strigari, L.; Ragona, R.; Borzì, G.R.; Cagni, E.; Carbonini, C.; Clemente, S.; Consorti, R.; El Gawhary, R.; Esposito, M.; et al. Lung stereotactic ablative body radiotherapy: A large scale multi-institutional planning comparison for interpreting results of multi-institutional studies. Phys. Med. 2016, 32, 600–606. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Zabel-du Bois, A.; Milker-Zabel, S.; Huber, P.; Schlegel, W.; Debus, J. Linac-based radiosurgery or hypofractionated stereotactic radiotherapy in the treatment of large cerebral arteriovenous malformations. Int. J. Radiat. Oncol. Biol. Phys. 2006, 64, 1049–1054. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Kawahara, D.; Ozawa, S.; Kimura, T.; Saito, A.; Nishio, T.; Nakashima, T.; Ohno, Y.; Murakami, Y.; Nagata, Y. Marginal prescription equivalent to the isocenter prescription in lung stereotactic body radiotherapy: Preliminary study for Japan Clinical Oncology Group trial (JCOG1408). J. Radiat. Res. 2017, 58, 149–154. [Google Scholar] [CrossRef]
- Xiao, Y.; Papiez, L.; Paulus, R.; Timmerman, R.; Straube, W.L.; Bosch, W.R.; Michalski, J.; Galvin, J.M. Dosimetric evaluation of heterogeneity corrections for RTOG 0236: Stereotactic body radiotherapy of inoperable stage I-II non-small-cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 1235–1242. [Google Scholar] [CrossRef] [Green Version]
- Wallace, B.C.; Dahabreh, I.J.; Trikalinos, T.A.; Lau, J.; Trow, P.; Schmid, C.H. Closing the Gap between Methodologists and End-Users: R as a Computational Back-End. J. Stat. Softw. 2012, 49, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Nagata, Y.; Takayama, K.; Matsuo, Y.; Norihisa, Y.; Mizowaki, T.; Sakamoto, T.; Sakamoto, M.; Mitsumori, M.; Shibuya, K.; Araki, N.; et al. Clinical outcomes of a phase I/II study of 48 Gy of stereotactic body radiotherapy in 4 fractions for primary lung cancer using a stereotactic body frame. Int. J. Radiat. Oncol. Biol. Phys. 2005, 63, 1427–1431. [Google Scholar] [CrossRef]
- Salazar, O.M.; Sandhu, T.S.; Lattin, P.B.; Chang, J.H.; Lee, C.K.; Groshko, G.A.; Lattin, C.J. Once-weekly, high-dose stereotactic body radiotherapy for lung cancer: 6-year analysis of 60 early-stage, 42 locally advanced, and 7 metastatic lung cancers. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, 707–715. [Google Scholar] [CrossRef]
- Takeda, A.; Sanuki, N.; Kunieda, E.; Ohashi, T.; Oku, Y.; Takeda, T.; Shigematsu, N.; Kubo, A. Stereotactic body radiotherapy for primary lung cancer at a dose of 50 Gy total in five fractions to the periphery of the planning target volume calculated using a superposition algorithm. Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 442–448. [Google Scholar] [CrossRef]
- Fakiris, A.J.; McGarry, R.C.; Yiannoutsos, C.T.; Papiez, L.; Williams, M.; Henderson, M.A.; Timmerman, R. Stereotactic body radiation therapy for early-stage non-small-cell lung carcinoma: Four-year results of a prospective phase II study. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 677–682. [Google Scholar] [CrossRef]
- Brown, W.T.; Wu, X.; Fayad, F.; Fowler, J.F.; García, S.; Monterroso, M.I.; de la Zerda, A.; Schwade, J.G. Application of robotic stereotactic radiotherapy to peripheral stage I non-small cell lung cancer with curative intent. Clin. Oncol. (R. Coll. Radiol. (Great Br.)) 2009, 21, 623–631. [Google Scholar] [CrossRef]
- Ricardi, U.; Filippi, A.R.; Guarneri, A.; Giglioli, F.R.; Ciammella, P.; Franco, P.; Mantovani, C.; Borasio, P.; Scagliotti, G.V.; Ragona, R. Stereotactic body radiation therapy for early stage non-small cell lung cancer: Results of a prospective trial. Lung Cancer 2010, 68, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Grills, I.S.; Mangona, V.S.; Welsh, R.; Chmielewski, G.; McInerney, E.; Martin, S.; Wloch, J.; Ye, H.; Kestin, L.L. Outcomes after stereotactic lung radiotherapy or wedge resection for stage I non-small-cell lung cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 928–935. [Google Scholar] [CrossRef] [PubMed]
- Shirata, Y.; Jingu, K.; Koto, M.; Kubozono, M.; Takeda, K.; Sugawara, T.; Kadoya, N.; Matsushita, H. Prognostic factors for local control of stage I non-small cell lung cancer in stereotactic radiotherapy: A retrospective analysis. Radiat. Oncol. 2012, 7, 182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inoue, T.; Katoh, N.; Onimaru, R.; Shimizu, S.; Tsuchiya, K.; Suzuki, R.; Sakakibara-Konishi, J.; Shinagawa, N.; Oizumi, S.; Shirato, H. Stereotactic body radiotherapy using gated radiotherapy with real-time tumor-tracking for stage I non-small cell lung cancer. Radiat. Oncol. 2013, 8, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, O.; Mitsuyoshi, T.; Miyazaki, M.; Teshima, T.; Nishiyama, K.; Ubbels, J.F.; Bolt, R.A.; Langendijk, J.A.; Widder, J. Dose-volume-response analysis in stereotactic radiotherapy for early lung cancer. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2014, 112, 262–266. [Google Scholar] [CrossRef]
- Hamaji, M.; Chen, F.; Matsuo, Y.; Kawaguchi, A.; Morita, S.; Ueki, N.; Sonobe, M.; Nagata, Y.; Hiraoka, M.; Date, H. Video-assisted thoracoscopic lobectomy versus stereotactic radiotherapy for stage I lung cancer. Ann. Thorac. Surg. 2015, 99, 1122–1129. [Google Scholar] [CrossRef]
- Lindberg, K.; Nyman, J.; Riesenfeld Källskog, V.; Hoyer, M.; Lund, J.; Lax, I.; Wersäll, P.; Karlsson, K.; Friesland, S.; Lewensohn, R. Long-term results of a prospective phase II trial of medically inoperable stage I NSCLC treated with SBRT—The Nordic experience. Acta Oncol. 2015, 54, 1096–1104. [Google Scholar] [CrossRef] [Green Version]
- Shibamoto, Y.; Hashizume, C.; Baba, F.; Ayakawa, S.; Miyakawa, A.; Murai, T.; Takaoka, T.; Hattori, Y.; Asai, R. Stereotactic body radiotherapy using a radiobiology-based regimen for stage I non-small-cell lung cancer: Five-year mature results. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2015, 10, 960–964. [Google Scholar] [CrossRef] [Green Version]
- Hayashi, S.; Tanaka, H.; Hoshi, H. Imaging characteristics of local recurrences after stereotactic body radiation therapy for stage I non-small cell lung cancer: Evaluation of mass-like fibrosis. Thorac. Cancer 2015, 6, 186–193. [Google Scholar] [CrossRef] [Green Version]
- Shaverdian, N.; Tenn, S.; Veruttipong, D.; Wang, J.; Hegde, J.; Lee, C.; Cao, M.; Agazaryan, N.; Steinberg, M.; Kupelian, P.; et al. The significance of PTV dose coverage on cancer control outcomes in early stage non-small cell lung cancer patients treated with highly ablative stereotactic body radiation therapy. Br. J. Radiol. 2016, 89, 20150963. [Google Scholar] [CrossRef] [Green Version]
- Tsurugai, Y.; Kozuka, T.; Ishizuka, N.; Oguchi, M. Relationship between the consolidation to maximum tumor diameter ratio and outcomes following stereotactic body radiotherapy for stage I non-small-cell lung cancer. Lung Cancer 2016, 92, 47–52. [Google Scholar] [CrossRef]
- Navarro-Martin, A.; Aso, S.; Cacicedo, J.; Arnaiz, M.; Navarro, V.; Rosales, S.; de Blas, R.; Ramos, R.; Guedea, F. Phase II Trial of SBRT for Stage I NSCLC: Survival, Local Control, and Lung Function at 36 Months. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2016, 11, 1101–1111. [Google Scholar] [CrossRef] [Green Version]
- Mancini, B.R.; Park, H.S.; Harder, E.M.; Rutter, C.E.; Corso, C.D.; Decker, R.H.; Husain, Z.A. Elderly patients undergoing SBRT for inoperable early-stage NSCLC achieve similar outcomes to younger patients. Lung Cancer 2016, 97, 22–27. [Google Scholar] [CrossRef]
- Aoki, M.; Akimoto, H.; Sato, M.; Hirose, K.; Kawaguchi, H.; Hatayama, Y.; Seino, H.; Kakehata, S.; Tsushima, F.; Fujita, H.; et al. Impact of pretreatment whole-tumor perfusion computed tomography and 18F-fluorodeoxyglucose positron emission tomography/computed tomography measurements on local control of non-small cell lung cancer treated with stereotactic body radiotherapy. J. Radiat. Res. 2016, 57, 533–540. [Google Scholar] [CrossRef]
- Sun, B.; Brooks, E.D.; Komaki, R.U.; Liao, Z.; Jeter, M.D.; McAleer, M.F.; Allen, P.K.; Balter, P.A.; Welsh, J.D.; O’Reilly, M.S.; et al. 7-year follow-up after stereotactic ablative radiotherapy for patients with stage I non-small cell lung cancer: Results of a phase 2 clinical trial. Cancer 2017, 123, 3031–3039. [Google Scholar] [CrossRef]
- Miyakawa, A.; Shibamoto, Y.; Baba, F.; Manabe, Y.; Murai, T.; Sugie, C.; Yanagi, T.; Takaoka, T. Stereotactic body radiotherapy for stage I non-small-cell lung cancer using higher doses for larger tumors: Results of the second study. Radiat. Oncol. 2017, 12, 152. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Song, S.Y.; Kim, S.S.; Choi, W.; Je, H.U.; Back, G.M.; Cho, B.; Jeong, S.Y.; Choi, E.K. Feasible Optimization of Stereotactic Ablative Radiotherapy Dose by Tumor Size for Stage I Non-small-cell Lung Cancer. Clin. Lung Cancer 2018, 19, e253–e261. [Google Scholar] [CrossRef]
- Raghavan, G.; Shaverdian, N.; Chan, S.; Chu, F.I.; Lee, P. Comparing Outcomes of Patients with Early-Stage Non-Small-Cell Lung Cancer Treated with Stereotactic Body Radiotherapy Based on Frailty Status. Clin. Lung Cancer 2018, 19, e759–e766. [Google Scholar] [CrossRef]
- Cummings, M.A.; Ma, S.J.; Hermann, G.; Serra, L.; Syed, Y.; Malhotra, H.K.; Chen, Y.; Milano, M.T.; Gomez-Suescun, J.A.; Singh, D.P.; et al. Comparison of Single- and Five-fraction Regimens of Stereotactic Body Radiation Therapy for Peripheral Early-stage Non-small-cell Lung Cancer: A Two-institution Propensity-matched Analysis. Clin. Lung Cancer 2018, 19, 511–517. [Google Scholar] [CrossRef]
- Karasawa, K.; Hayakawa, S.; Machitori, Y.; Shibata, Y.; Ogawa, H.; Ito, K.; Shimizuguchi, T.; Kawamoto, T.; Nihei, K. Accelerated Hypofractionated Radiotherapy Versus Stereotactic Body Radiotherapy for the Treatment of Stage I Nonsmall Cell Lung Cancer-A Single Institution Experience with Long-Term Follow-Up. Technol. Cancer Res. Treat. 2018, 17, 1533033818806318. [Google Scholar] [CrossRef]
- Menoux, I.; Antoni, D.; Truntzer, P.; Keller, A.; Massard, G.; Noël, G. Stereotactic body radiation therapy for stage I non-small cell lung carcinomas: Moderate hypofractionation optimizes outcome. Lung Cancer 2018, 126, 201–207. [Google Scholar] [CrossRef]
- Tsurugai, Y.; Takeda, A.; Sanuki, N.; Eriguchi, T.; Aoki, Y.; Oku, Y.; Akiba, T.; Sugawara, A.; Kunieda, E. Stereotactic body radiotherapy for patients with non-small-cell lung cancer using RapidArc delivery and a steep dose gradient: Prescription of 60% isodose line of maximum dose fitting to the planning target volume. J. Radiat. Res. 2019, 60, 364–370. [Google Scholar] [CrossRef]
- Ball, D.; Mai, G.T.; Vinod, S.; Babington, S.; Ruben, J.; Kron, T.; Chesson, B.; Herschtal, A.; Vanevski, M.; Rezo, A.; et al. Stereotactic ablative radiotherapy versus standard radiotherapy in stage 1 non-small-cell lung cancer (TROG 09.02 CHISEL): A phase 3, open-label, randomised controlled trial. Lancet Oncol. 2019, 20, 494–503. [Google Scholar] [CrossRef]
- Weiss, E.; Deng, X.; Mukhopadhyay, N.; Jan, N. Effects of the recurrence pattern on patient survival following SABR for stage I lung cancer. Acta Oncol. 2020, 59, 427–433. [Google Scholar] [CrossRef]
- Shu, Z.; Dong, B.; Shi, L.; Shen, W.; Hang, Q.; Wang, J.; Chen, Y. Stereotactic body radiotherapy for elderly patients (≥ 75 years) with early-stage non-small cell lung cancer. J. Cancer Res. Clin. Oncol. 2020, 146, 1263–1271. [Google Scholar] [CrossRef]
- Duvergé, L.; Bondiau, P.Y.; Claude, L.; Supiot, S.; Vaugier, L.; Thillays, F.; Doyen, J.; Ricordel, C.; Léna, H.; Bellec, J.; et al. Discontinuous stereotactic body radiotherapy schedule increases overall survival in early-stage non-small cell lung cancer. Lung Cancer 2021, 157, 100–108. [Google Scholar] [CrossRef]
- Onishi, H.; Shirato, H.; Nagata, Y.; Hiraoka, M.; Fujino, M.; Gomi, K.; Niibe, Y.; Karasawa, K.; Hayakawa, K.; Takai, Y.; et al. Hypofractionated stereotactic radiotherapy (HypoFXSRT) for stage I non-small cell lung cancer: Updated results of 257 patients in a Japanese multi-institutional study. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2007, 2, S94–S100. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Yang, F.; Li, B.; Li, H.; Liu, J.; Huang, W.; Wang, D.; Yi, Y.; Wang, J. Which is the optimal biologically effective dose of stereotactic body radiotherapy for Stage I non-small-cell lung cancer? A meta-analysis. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, e305–e316. [Google Scholar] [CrossRef] [PubMed]
- Tateishi, Y.; Takeda, A.; Horita, N.; Tsurugai, Y.; Eriguchi, T.; Kibe, Y.; Sanuki, N.; Kaneko, T. Stereotactic body radiotherapy with a high maximum dose improves local control, cancer-specific death and overall survival in peripheral early-stage non-small cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2021, 111, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Inagaki, T.A.-O.; Doi, H.A.-O.; Ishida, N.; Ri, A.; Tatsuno, S.; Wada, Y.A.-O.; Uehara, T.A.-O.; Inada, M.; Nakamatsu, K.; Hosono, M.; et al. Escalated Maximum Dose in the Planning Target Volume Improves Local Control in Stereotactic Body Radiation Therapy for T1-2 Lung Cancer. Cancers 2022, 14, 933. [Google Scholar] [CrossRef] [PubMed]
- Klement, R.J.; Sonke, J.J.; Allgäuer, M.; Andratschke, N.; Appold, S.; Belderbos, J.; Belka, C.; Blanck, O.; Dieckmann, K.; Eich, H.T.; et al. Correlating Dose Variables with Local Tumor Control in Stereotactic Body Radiation Therapy for Early-Stage Non-Small Cell Lung Cancer: A Modeling Study on 1500 Individual Treatments. Int. J. Radiat. Oncol. Biol. Phys. 2020, 107, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Zhou, S.; Balter, P.; Shen, C.; Gomez, D.R.; Welsh, J.D.; Lin, S.H.; Chang, J.Y. Planning Target Volume D95 and Mean Dose Should Be Considered for Optimal Local Control for Stereotactic Ablative Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 1226–1235. [Google Scholar] [CrossRef] [PubMed]
- Kestin, L.; Grills, I.; Guckenberger, M.; Belderbos, J.; Hope, A.J.; Werner-Wasik, M.; Sonke, J.J.; Bissonnette, J.P.; Xiao, Y.; Yan, D. Dose-response relationship with clinical outcome for lung stereotactic body radiotherapy (SBRT) delivered via online image guidance. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2014, 110, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Van Baardwijk, A.; Tomé, W.A.; van Elmpt, W.; Bentzen, S.M.; Reymen, B.; Wanders, R.; Houben, R.; Ollers, M.; Lambin, P.; De Ruysscher, D. Is high-dose stereotactic body radiotherapy (SBRT) for stage I non-small cell lung cancer (NSCLC) overkill? A systematic review. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2012, 105, 145–149. [Google Scholar] [CrossRef] [Green Version]
- International Commission on Radiation Units and Measurements. Report91: Prescribing, Recording, and Reporting of Stereotactic Treatments with Small Photon Beams. J. ICRU 2014, 14, 1–152. [Google Scholar]
- Fogliata, A.; Cozzi, L. Dose calculation algorithm accuracy for small fields in non-homogeneous media: The lung SBRT case. Phys. Med. 2017, 44, 157–162. [Google Scholar] [CrossRef]
- Liu, H.; Zhuang, T.; Stephans, K.; Videtic, G.; Raithel, S.; Djemil, T.; Xia, P. Dose differences in intensity-modulated radiotherapy plans calculated with pencil beam and Monte Carlo for lung SBRT. J. Appl. Clin. Med. Phys. 2015, 16, 91–99. [Google Scholar] [CrossRef]
- Ojala, J.J.; Kapanen, M.K.; Hyödynmaa, S.J.; Wigren, T.K.; Pitkänen, M.A. Performance of dose calculation algorithms from three generations in lung SBRT: Comparison with full Monte Carlo-based dose distributions. J. Appl. Clin. Med. Phys. 2014, 15, 4662. [Google Scholar] [CrossRef]
- Latifi, K.; Oliver, J.; Baker, R.; Dilling, T.J.; Stevens, C.W.; Kim, J.; Yue, B.; Demarco, M.; Zhang, G.G.; Moros, E.G.; et al. Study of 201 non-small cell lung cancer patients given stereotactic ablative radiation therapy shows local control dependence on dose calculation algorithm. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 1108–1113. [Google Scholar] [CrossRef]
- Ohri, N.; Tomé, W.; Kalnicki, S.; Garg, M. Stereotactic body radiation therapy for stage I non-small cell lung cancer: The importance of treatment planning algorithm and evaluation of a tumor control probability model. Pract. Radiat. Oncol. 2018, 8, e33–e39. [Google Scholar] [CrossRef]
- Tai, A.; Liu, F.; Gore, E.; Li, X.A. An analysis of tumor control probability of stereotactic body radiation therapy for lung cancer with a regrowth model. Phys. Med. Biol. 2016, 61, 3903–3913. [Google Scholar] [CrossRef]
- Santiago, A.; Barczyk, S.; Jelen, U.; Engenhart-Cabillic, R.; Wittig, A. Challenges in radiobiological modeling: Can we decide between LQ and LQ-L models based on reviewed clinical NSCLC treatment outcome data? Radiat. Oncol. 2016, 11, 67. [Google Scholar] [CrossRef] [Green Version]
- Park, C.; Papiez, L.; Zhang, S.; Story, M.; Timmerman, R.D. Universal survival curve and single fraction equivalent dose: Useful tools in understanding potency of ablative radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 847–852. [Google Scholar] [CrossRef]
- Eriguchi, T.; Takeda, A.; Kimura, Y.; Sanuki, N. In Regard to Lee et al. Int. J. Radiat. Oncol. Biol. Phys. 2021, 111, 1088–1089. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| 1st Author | Year | Country | n | Median f/u (Month) | Nominal/Peripheral/Central Dose (Gy) | Fraction | Nominal/Peripheral/Central/Average BED (Gy) | 3-Year LC (%) |
|---|---|---|---|---|---|---|---|---|
| Nagata [19] | 2005 | Japan | 32 | 30 | 48/42.0/48.0 | 4 | 105.6/86.1/105.6/95.9 | 95 |
| Salazar [20] | 2008 | USA | 60 | 38 | 40/40.0/52.0 | 4 | 80.0/80.0/119.6/99.8 | 98 |
| Takeda [21] | 2009 | Japan | 121 | 31 | 50/50.0/62.5 | 5 | 100.0/100.0/140.6/120.3 | 94 |
| Fakiris [22] | 2009 | USA | 34 | 50 | 60/54.0/75.0 | 3 | 180.0/151.2/262.5/206.9 | 88 |
| Fakiris | 2009 | USA | 36 | 50 | 66/59.4/82.5 | 3 | 211.2/177.0/309.4/243.2 | 88 |
| Brown [23] | 2009 | USA | 31 | 28 | 60/60.0/88.2 | 3 | 180.0/180.0/347.5/263.8 | 85.8 |
| Ricardi [24] | 2010 | Italy | 62 | 28 | 45/45.0/56.3 | 3 | 112.5/112.5/161.7/137.1 | 87.8 |
| Grills [25] | 2010 | USA | 58 | 30 | 48/48.0/– | 4 | 105.6/105.6/–/– | 96 |
| Timmerman [9] | 2010 | USA | 55 | 34 | 60/60.0/– | 3 | 180.0/180.0/–/– | 97.6 |
| Shirata [26] | 2012 | Japan | 45 | 30 | 48/43.2/48.0 | 4 | 105.6/89.9/105.6/97.7 | 100 |
| Shirata | 2012 | Japan | 29 | 30 | 60/54.0/60.0 | 8 | 105.0/90.5/105.0/97.7 | 82.1 |
| Inoue [27] | 2013 | Japan | 109 | 25 | 40/40.0/48.0 | 4 | 80.0/80.0/105.6/92.8 | 81 |
| Suzuki [28] | 2014 | Japan | 162 | 39 | 48/–/48.0 | 4 | 105.6/–/105.6/– | 84 |
| Hamaji [29] | 2015 | Japan | 104 | 43 | 48/42.0/48.0 | 4 | 105.6/86.1/105.6/95.9 | 77 |
| Lindberg [30] | 2015 | Sweden | 57 | 42 | 45/45.0/67.2 | 3 | 112.5/112.5/217.7/165.1 | 92 |
| Shibamoto [31] | 2015 | Japan | 180 | 53 | 48/43.2/48.0 | 4 | 105.6/89.9/105.6/97.7 | 85 |
| Hayashi [32] | 2015 | Japan | 81 | 29 | 48/42.0/48.0 | 4 | 105.6/86.1/105.6/95.9 | 91.8 |
| Nagata [3] | 2015 | Japan | 169 | 56 | 48/42.0/48.0 | 4 | 105.6/86.1/105.6/95.9 | 87.6 |
| Shaverdian [33] | 2016 | USA | 110 | 29 | 54/54.0/65.6 | 3 | 151.2/151.2/209.0/180.1 | 100 |
| Tsurugai [34] | 2016 | Japan | 234 | 35 | 48/42.0/48.0 | 4 | 105.6/86.1/105.6/95.9 | 89 |
| Navarro-Martin [35] | 2016 | Spain | 38 | 48 | 54/54.0/70.2 | 4 | 151.2/151.2/234.5/192.8 | 94 |
| Mancini [36] | 2016 | USA | 251 | 36 | 54/54.0/– | 3 | 151.2/151.2/–/– | 85.3 |
| Aoki [37] | 2016 | Japan | 74 | 25 | 50/45.0/50.0 | 5 | 100.0/85.5/100.0/92.8 | 85 |
| Sun [38] | 2017 | USA | 65 | 86 | 50/50.0/– | 4 | 112.5/112.5/–/– | 95 |
| Miyakawa [39] | 2017 | Japan | 71 | 44 | 48/43.2/48.0 | 4 | 105.6/89.9/105.6/97.7 | 88 |
| Lee [40] | 2018 | Korea | 155 | 32 | 60/60.0/72.7 | 4 | 150.0/150.0/204.8/177.4 | 86.3 |
| Raghavan [41] | 2018 | USA | 140 | 39 | 54/54.0/– | 3 | 151.2/151.2/–/– | 93.4 |
| Cummings [42] | 2018 | USA | 65 | 24 | 30/30.0/– | 1 | 120.0/120.0/–/– | 84 |
| Cummings | 2018 | USA | 98 | 40 | 50/40.0/50.0 | 5 | 100.0/72.0/100.0/86.0 | 83 |
| Karasawa [43] | 2018 | Japan | 56 | 127 | 48/42.0/48.0 | 4 | 105.6/86.1/105.6/95.9 | 78.2 |
| Menoux [44] | 2018 | U.K. | 90 | 35 | 60/60.0/75.0 | 8 | 105.0/105.0/145.3/125.2 | 94 |
| Tsurugai [45] | 2019 | Japan | 157 | 28 | 50/50.0/83.3 | 5 | 100.0/100.0/222.1/161.0 | 99 |
| Tsurugai | 2019 | Japan | 66 | 28 | 60/50.0/100.0 | 5 | 132.0/100.0/300.0/200.0 | 100 |
| Ball [46] | 2019 | Australia | 66 | 31 | 48/48.0/– | 4 | 105.6/105.6/–/– | 85 |
| Weiss [47] | 2020 | USA | 100 | 32 | 48/48.0/60.0 | 4 | 105.6/105.6/150.0/127.8 | 92 |
| Shu [48] | 2020 | China | 68 | 46 | 50/50.0/– | 5 | 100.0/100.0/–/– | 95.6 |
| Duvergé [49] | 2021 | France | 418 | 41 | 54/54.0/– | 4 | 126.9/126.9/–/– | 88 |
| UVA | MVA (+Percentage of T1 Tumor, Patient Age, f/u Period, Year of Publication) | |||
|---|---|---|---|---|
| Coefficient (95%CI) (×10−3) | p | Coefficient (95%CI) (×10−3) | p | |
| Nominal BED | 2.6 (−4.5–9.7) | 0.48 | 2.9 (−6.7–12.6) | 0.55 |
| Central BED | 3.6 (3.0–6.8) | 0.03 | 5.4(1.6–9.1) | <0.01 |
| Peripheral BED | 3.7 (−3.0–10.4) | 0.28 | 6.3 (–0.3–15.9) | 0.20 |
| Average BED | 4.4 (−0.6–9.4) | 0.08 | 7.4 (1.2–13.6) | 0.02 |
| Percentage of T1 tumor | −1.0 (−12.5–10.4) | 0.86 | – | – |
| Median patient age | −0.1 (−0.8–0.7) | 0.88 | – | – |
| Median f/u period | −0.1 (−0.2–0.1) | 0.18 | – | – |
| Year of publication | −0.1 (−0.6–0.4) | 0.63 | – | – |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eriguchi, T.; Takeda, A.; Nemoto, T.; Tsurugai, Y.; Sanuki, N.; Tateishi, Y.; Kibe, Y.; Akiba, T.; Inoue, M.; Nagashima, K.; et al. Relationship between Dose Prescription Methods and Local Control Rate in Stereotactic Body Radiotherapy for Early Stage Non-Small-Cell Lung Cancer: Systematic Review and Meta-Analysis. Cancers 2022, 14, 3815. https://doi.org/10.3390/cancers14153815
Eriguchi T, Takeda A, Nemoto T, Tsurugai Y, Sanuki N, Tateishi Y, Kibe Y, Akiba T, Inoue M, Nagashima K, et al. Relationship between Dose Prescription Methods and Local Control Rate in Stereotactic Body Radiotherapy for Early Stage Non-Small-Cell Lung Cancer: Systematic Review and Meta-Analysis. Cancers. 2022; 14(15):3815. https://doi.org/10.3390/cancers14153815
Chicago/Turabian StyleEriguchi, Takahisa, Atsuya Takeda, Takafumi Nemoto, Yuichiro Tsurugai, Naoko Sanuki, Yudai Tateishi, Yuichi Kibe, Takeshi Akiba, Mari Inoue, Kengo Nagashima, and et al. 2022. "Relationship between Dose Prescription Methods and Local Control Rate in Stereotactic Body Radiotherapy for Early Stage Non-Small-Cell Lung Cancer: Systematic Review and Meta-Analysis" Cancers 14, no. 15: 3815. https://doi.org/10.3390/cancers14153815
APA StyleEriguchi, T., Takeda, A., Nemoto, T., Tsurugai, Y., Sanuki, N., Tateishi, Y., Kibe, Y., Akiba, T., Inoue, M., Nagashima, K., & Horita, N. (2022). Relationship between Dose Prescription Methods and Local Control Rate in Stereotactic Body Radiotherapy for Early Stage Non-Small-Cell Lung Cancer: Systematic Review and Meta-Analysis. Cancers, 14(15), 3815. https://doi.org/10.3390/cancers14153815