
Neoadjuvant Chemoradiotherapy versus Chemotherapy for Gastroesophageal Junction Adenocarcinoma; Which Is the Optimal Treatment Option?

 ,
,  , , , and
, , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
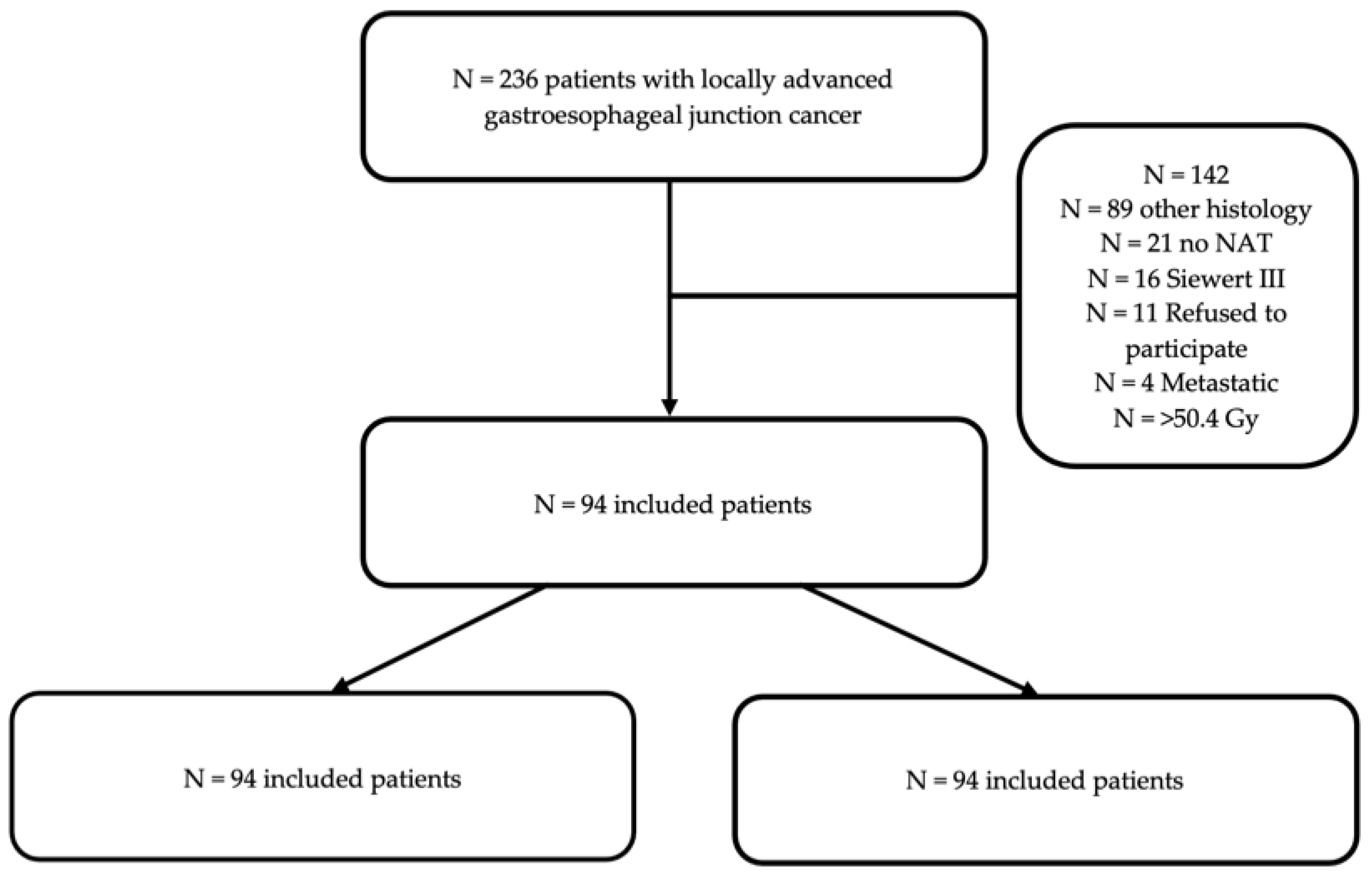
2.2. Inclusion and Exclusion Criteria
2.3. Ethics and Reporting
2.4. Study Definitions and Outcome Measures
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Treatment Details, Postoperative Outcomes (Table 2)

{kind=link}
{kind=link}
{kind=link}
| Surgical and Postop. Variables | All Patients N = 94 | RCT N = 67 | CT N = 27 | p-Value |
|---|---|---|---|---|
| Surgical approach | 0.086 | |||
| Lewis Santy (%) | 86 (91.5) | 64 (95.5) | 22 (81.5) | |
| Transhiatal (%) | 8 (8.5) | 3 (4.5) | 5 (18.5) | |
| Laparoscopy (%) | 84 (89.3) | 61 (91) | 23 (85.1) | 0.404 |
| Thoracosopy (%) | 45 (47.8) | 29 (43.2) | 16 (59.2) | 0.077 |
| Operative time (min) | 300.4 (71.9) | 306.8 (77) | 284.5(55.2) | 0.122 |
| NAT-Surgery interval (days) | 48.4 (15.1) | 50.3 (14.9) | 43.3 (14.8) | 0.052 |
| Clavien–Dindo grade [19] (%) | 0.988 | |||
| 0 | 31 (33) | 21 (31.3) | 10 (37) | |
| I | 2 (2.1) | 1 (1.5) | 1 (3.7) | |
| II | 18 (19.1) | 13 (19.4) | 5 (18.5) | |
| IIIA | 6 (6.3) | 4 (6) | 2 (7.4) | |
| IIIB | 10 (10.6) | 7 (10.4) | 3 (11.1) | |
| IV | 22 (23.4) | 17 (25.3) | 5 (18.5) | |
| V | 5 (5.3) | 4 (6) | 1 (3.7) | |
| Pulmonary complications (%) | 48 (51) | 36 (53.7) | 12 (44.4) | 0.376 |
| Cardiovascular complications (%) | 27 (28.7) | 24 (35.8) | 3 (11.1) | 0.017 |
| Anastomotic leakage (%) | 27 (28.7) | 20 (29.8) | 7 (26) | 0.704 |
| Length of stay (days) | 28.3 (31.9) | 30.1 (34.9) | 23.7 (22.1) | 0.287 |
| Length of ICU stay (days) | 7.1 (20.2) | 8.8 (23.5) | 3.2 (6.5) | 0.086 |
3.3. Histological Analysis, Tumor Response to Treatment
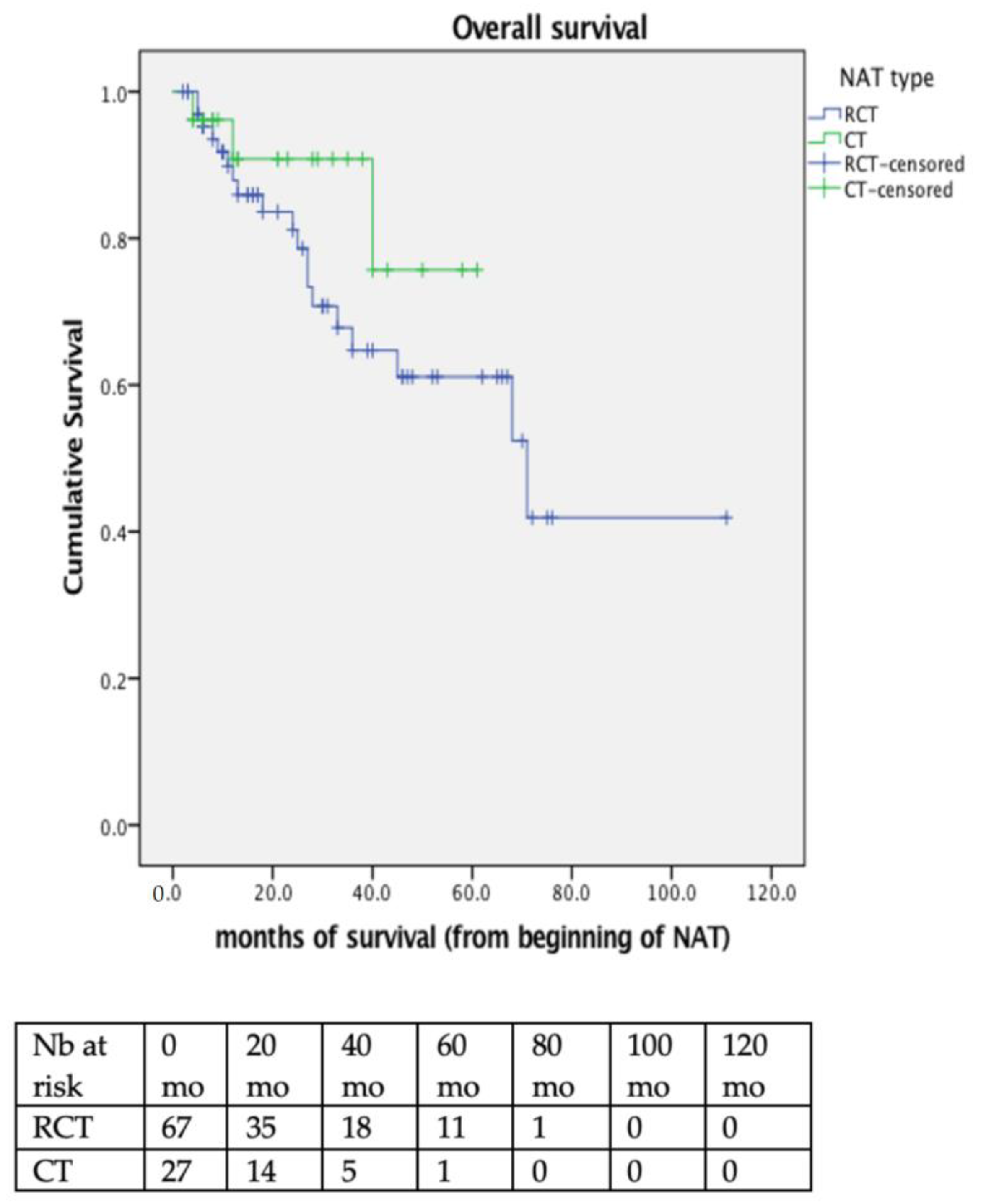
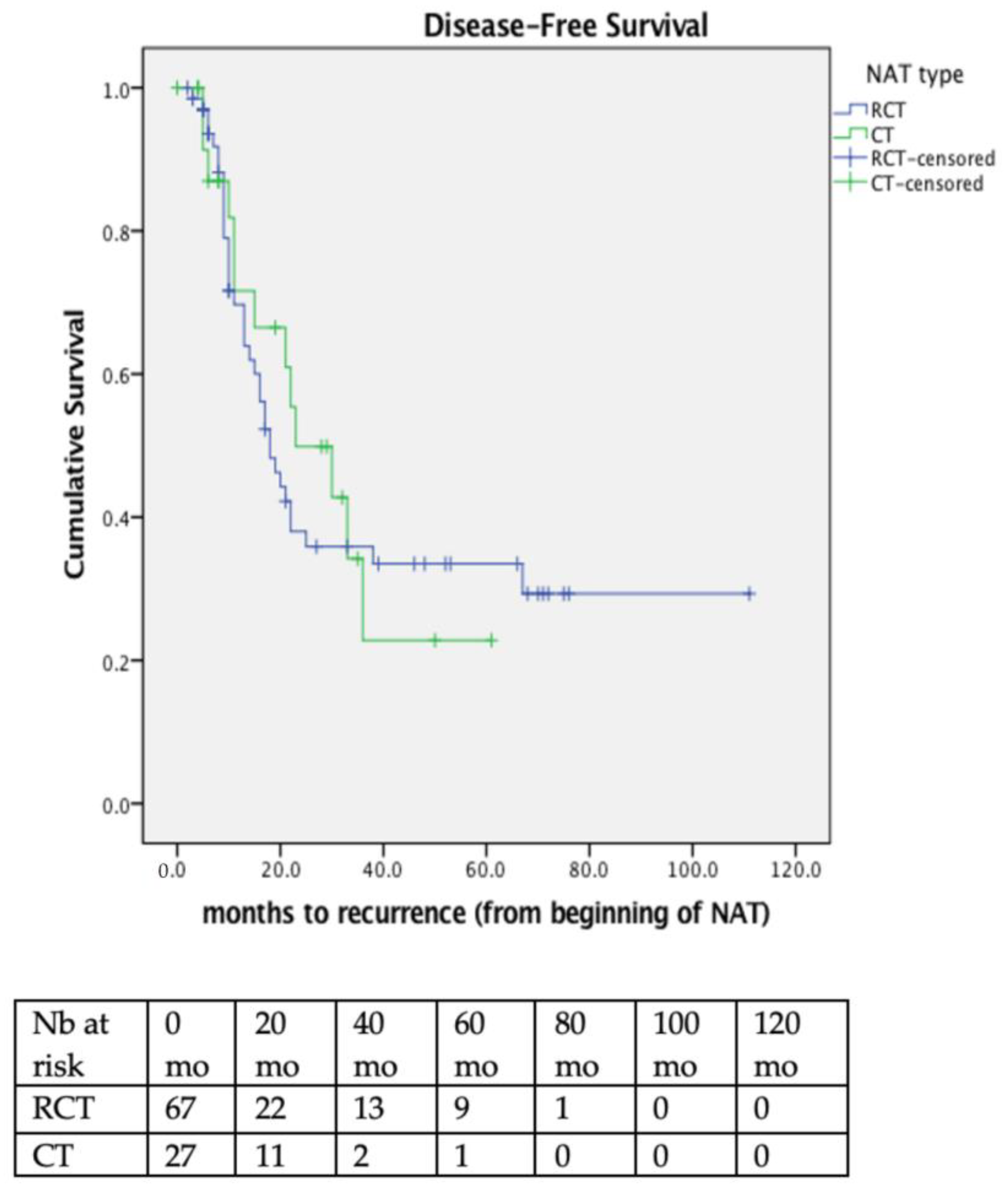
3.4. Long-Term Survival and Recurrence Patterns
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- International Agency for Research on Cancer; WHO. Available online: https://gco.iarc.fr/ (accessed on 9 August 2022).
- Obermannova, R.; Alsina, M.; Cervantes, A.; Leong, T.; Lordick, F.; Nilsson, M.; van Grieken, N.C.T.; Vogel, A.; Smyth, E.C.; Committee, E.G. Oesophageal cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2022, 33, 992–1004. [Google Scholar] [CrossRef]
- Griffin, S.M.; Jones, R.; Kamarajah, S.K.; Navidi, M.; Wahed, S.; Immanuel, A.; Hayes, N.; Phillips, A.W. Evolution of Esophagectomy for Cancer Over 30 Years: Changes in Presentation, Management and Outcomes. Ann. Surg. Oncol. 2021, 28, 3011–3022. [Google Scholar] [CrossRef]
- Al-Batran, S.E.; Homann, N.; Pauligk, C.; Goetze, T.O.; Meiler, J.; Kasper, S.; Kopp, H.G.; Mayer, F.; Haag, G.M.; Luley, K.; et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): A randomised, phase 2/3 trial. Lancet 2019, 393, 1948–1957. [Google Scholar] [CrossRef] [PubMed]
- Van Hagen, P.; Hulshof, M.C.; van Lanschot, J.J.; Steyerberg, E.W.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.; Richel, D.J.; Nieuwenhuijzen, G.A.; Hospers, G.A.; Bonenkamp, J.J.; et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N. Engl. J. Med. 2012, 366, 2074–2084. [Google Scholar] [CrossRef] [PubMed]
- Stahl, M.; Walz, M.K.; Stuschke, M.; Lehmann, N.; Meyer, H.J.; Riera-Knorrenschild, J.; Langer, P.; Engenhart-Cabillic, R.; Bitzer, M.; Konigsrainer, A.; et al. Phase III comparison of preoperative chemotherapy compared with chemoradiotherapy in patients with locally advanced adenocarcinoma of the esophagogastric junction. J. Clin. Oncol. 2009, 27, 851–856. [Google Scholar] [CrossRef]
- Burmeister, B.H.; Thomas, J.M.; Burmeister, E.A.; Walpole, E.T.; Harvey, J.A.; Thomson, D.B.; Barbour, A.P.; Gotley, D.C.; Smithers, B.M. Is concurrent radiation therapy required in patients receiving preoperative chemotherapy for adenocarcinoma of the oesophagus? A randomised phase II trial. Eur. J. Cancer 2011, 47, 354–360. [Google Scholar] [CrossRef]
- Klevebro, F.; von Dobeln, A.G.; Wang, N.; Johnsen, G.; Jacobsen, A.B.; Friesland, S.; Hatlevoll, I.; Glenjen, N.I.; Lind, P.; Tsai, J.A.; et al. A randomized clinical trial of neoadjuvant chemotherapy versus neoadjuvant chemoradiotherapy for cancer of the oesophagus or gastro-oesophageal junction. Ann. Oncol. 2016, 27, 660–667. [Google Scholar] [CrossRef]
- Von Dobeln, G.A.; Klevebro, F.; Jacobsen, A.B.; Johannessen, H.O.; Nielsen, N.H.; Johnsen, G.; Hatlevoll, I.; Glenjen, N.I.; Friesland, S.; Lundell, L.; et al. Neoadjuvant chemotherapy versus neoadjuvant chemoradiotherapy for cancer of the esophagus or gastroesophageal junction: Long-term results of a randomized clinical trial. Dis. Esophagus. 2019, 32. [Google Scholar] [CrossRef]
- Markar, S.R.; Noordman, B.J.; Mackenzie, H.; Findlay, J.M.; Boshier, P.R.; Ni, M.; Steyerberg, E.W.; van der Gaast, A.; Hulshof, M.; Maynard, N.; et al. Multimodality treatment for esophageal adenocarcinoma: Multi-center propensity-score matched study. Ann. Oncol. 2017, 28, 519–527. [Google Scholar] [CrossRef]
- Kamarajah, S.K.; A Griffiths, E. Postoperative and Pathological Outcomes of CROSS and FLOT as Neoadjuvant Therapy for Esophageal and Junctional Adenocarcinoma. Ann. Surg. 2022; online ahead of print. [Google Scholar] [CrossRef]
- Donlon, N.E.; Moran, B.; Kamilli, A.; Davern, M.; Sheppard, A.; King, S.; Donohoe, C.L.; Lowery, M.; Cunningham, M.; Ravi, N.; et al. CROSS Versus FLOT Regimens in Esophageal and Esophagogastric Junction Adenocarcinoma: A Propensity-matched Comparison. Ann. Surg. 2022, 276, 792–798. [Google Scholar] [CrossRef]
- Hoeppner, J.; Lordick, F.; Brunner, T.; Glatz, T.; Bronsert, P.; Rothling, N.; Schmoor, C.; Lorenz, D.; Ell, C.; Hopt, U.T.; et al. ESOPEC: Prospective randomized controlled multicenter phase III trial comparing perioperative chemotherapy (FLOT protocol) to neoadjuvant chemoradiation (CROSS protocol) in patients with adenocarcinoma of the esophagus (NCT02509286). BMC Cancer 2016, 16, 503. [Google Scholar] [CrossRef]
- Reynolds, J.V.; Preston, S.R.; O’Neill, B.; Baeksgaard, L.; Griffin, S.M.; Mariette, C.; Cuffe, S.; Cunningham, M.; Crosby, T.; Parker, I.; et al. ICORG 10-14: NEOadjuvant trial in Adenocarcinoma of the oEsophagus and oesophagoGastric junction International Study (Neo-AEGIS). BMC Cancer 2017, 17, 401. [Google Scholar] [CrossRef]
- Lorenzen, S.; Biederstadt, A.; Ronellenfitsch, U.; Reissfelder, C.; Monig, S.; Wenz, F.; Pauligk, C.; Walker, M.; Al-Batran, S.E.; Haller, B.; et al. RACE-trial: Neoadjuvant radiochemotherapy versus chemotherapy for patients with locally advanced, potentially resectable adenocarcinoma of the gastroesophageal junction—A randomized phase III joint study of the AIO, ARO and DGAV. BMC Cancer 2020, 20, 886. [Google Scholar] [CrossRef]
- Kelly, R.J.; Ajani, J.A.; Kuzdzal, J.; Zander, T.; Van Cutsem, E.; Piessen, G.; Mendez, G.; Feliciano, J.; Motoyama, S.; Lievre, A.; et al. Adjuvant Nivolumab in Resected Esophageal or Gastroesophageal Junction Cancer. N. Engl. J. Med. 2021, 384, 1191–1203. [Google Scholar] [CrossRef] [PubMed]
- Noordman, B.J.; Spaander, M.C.W.; Valkema, R.; Wijnhoven, B.P.L.; van Berge Henegouwen, M.I.; Shapiro, J.; Biermann, K.; van der Gaast, A.; van Hillegersberg, R.; Hulshof, M.; et al. Detection of residual disease after neoadjuvant chemoradiotherapy for oesophageal cancer (preSANO): A prospective multicentre, diagnostic cohort study. Lancet Oncol. 2018, 19, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Rice, T.W.; Ishwaran, H.; Ferguson, M.K.; Blackstone, E.H.; Goldstraw, P. Cancer of the Esophagus and Esophagogastric Junction: An Eighth Edition Staging Primer. J. Thorac. Oncol. 2017, 12, 36–42. [Google Scholar] [CrossRef]
- St-Amour, P.; Winiker, M.; Sempoux, C.; Fasquelle, F.; Demartines, N.; Schafer, M.; Mantziari, S. The “Real R0”: A Resection Margin Smaller Than 0.1 cm is Associated with a Poor Prognosis After Oncologic Esophagectomy. Ann. Surg. Oncol. 2021, 28, 7095–7106. [Google Scholar] [CrossRef]
- Mandard, A.M.; Dalibard, F.; Mandard, J.C.; Marnay, J.; Henry-Amar, M.; Petiot, J.F.; Roussel, A.; Jacob, J.H.; Segol, P.; Samama, G.; et al. Pathologic assessment of tumor regression after preoperative chemoradiotherapy of esophageal carcinoma. Clinicopathologic correlations. Cancer 1994, 73, 2680–2686. [Google Scholar] [CrossRef]
- Goense, L.; van der Sluis, P.C.; van Rossum, P.S.N.; van der Horst, S.; Meijer, G.J.; Haj Mohammad, N.; van Vulpen, M.; Mook, S.; Ruurda, J.P.; van Hillegersberg, R. Perioperative chemotherapy versus neoadjuvant chemoradiotherapy for esophageal or GEJ adenocarcinoma: A propensity score-matched analysis comparing toxicity, pathologic outcome, and survival. J. Surg. Oncol. 2017, 115, 812–820. [Google Scholar] [CrossRef] [PubMed]
- Giugliano, D.N.; Berger, A.C.; Pucci, M.J.; Rosato, E.L.; Evans, N.R.; Meidl, H.; Lamb, C.; Levine, D.; Palazzo, F. Comparative Quantitative Lymph Node Assessment in Localized Esophageal Cancer Patients After R0 Resection With and Without Neoadjuvant Chemoradiation Therapy. J. Gastrointest. Surg. 2017, 21, 1377–1384. [Google Scholar] [CrossRef] [PubMed]
- Brunner, M.; Merkel, S.; Krautz, C.; Kersting, S.; Grutzmann, R.; Weber, G.F. The Prognostic Value of the Number of Harvested Negative Lymph Nodes in Patients Treated by Esophagectomy with or without Neoadjuvant Chemoradiation. Anticancer Res. 2020, 40, 2833–2840. [Google Scholar] [CrossRef]
- Gottlieb-Vedi, E.; Kauppila, J.H.; Mattsson, F.; Hedberg, J.; Johansson, J.; Edholm, D.; Lagergren, P.; Nilsson, M.; Lagergren, J. Extent of Lymphadenectomy and Long-Term Survival in Esophageal Cancer. Ann. Surg. 2021; online ahead of print. [Google Scholar] [CrossRef]
- Lutfi, W.; Martinez-Meehan, D.; Dhupar, R.; Christie, N.; Sarkaria, I.; Ekeke, C.; Baker, N.; Luketich, J.D.; Okusanya, O.T. Higher lymph node harvest in patients with a pathologic complete response after neoadjuvant therapy for esophageal cancer is associated with improved survival. J. Surg. Oncol. 2020, 121, 654–661. [Google Scholar] [CrossRef]
- Stahl, M.; Walz, M.K.; Riera-Knorrenschild, J.; Stuschke, M.; Sandermann, A.; Bitzer, M.; Wilke, H.; Budach, W. Preoperative chemotherapy versus chemoradiotherapy in locally advanced adenocarcinomas of the oesophagogastric junction (POET): Long-term results of a controlled randomised trial. Eur. J. Cancer 2017, 81, 183–190. [Google Scholar] [CrossRef]
- Cools-Lartigue, J.; Markar, S.; Mueller, C.; Hofstetter, W.; Nilsson, M.; Ilonen, I.; Soderstrom, H.; Rasanen, J.; Gisbertz, S.; Hanna, G.B.; et al. An International Cohort Study of Prognosis Associated with Pathologically Complete Response Following Neoadjuvant Chemotherapy versus Chemoradiotherapy of Surgical Treated Esophageal Adenocarcinoma. Ann. Surg. 2022, 276, 799–805. [Google Scholar] [CrossRef]
- Klevebro, F.; Johnsen, G.; Johnson, E.; Viste, A.; Myrnas, T.; Szabo, E.; Jacobsen, A.B.; Friesland, S.; Tsai, J.A.; Persson, S.; et al. Morbidity and mortality after surgery for cancer of the oesophagus and gastro-oesophageal junction: A randomized clinical trial of neoadjuvant chemotherapy vs. neoadjuvant chemoradiation. Eur. J. Surg. Oncol. 2015, 41, 920–926. [Google Scholar] [CrossRef]
- Sunde, B.; Lindblad, M.; Malmstrom, M.; Hedberg, J.; Lagergren, P.; Nilsson, M. Health-related quality of life one year after the diagnosis of oesophageal cancer: A population-based study from the Swedish National Registry for Oesophageal and Gastric Cancer. BMC Cancer 2021, 21, 1277. [Google Scholar] [CrossRef]



| Demographic Variables | All Patients N = 94 | RCT N = 67 (71%) | CT N = 27 (29%) | p-Value |
|---|---|---|---|---|
| Male gender (%) | 79 (84) | 57 (85.1) | 22 (81.5) | 0.667 |
| ASA class | 0.833 | |||
| 1–2 (%) | 64 (68.0) | 46 (68.6) | 18 (66.6) | |
| 3–4 (%) | 28 (29.7) | 19 (28.3) | 9 (33.3) | |
| Unknown | 2 | - | - | |
| Age, years | 62 [9.7] | 62.1 [10.1] | 61.9 [8.7] | 0.927 |
| BMI, kg/m2 | 25.2 [4.0] | 24.7 [3.8] | 26.4 [4.0] | 0.064 |
| Weight loss at baseline (kg) | 6.7 (5.6) | 6.5 (5.5) | 7.6 (5.9) | 0.569 |
| Weight loss during NAT (kg) | 3.0 (6.7) | 3.6 (6.3) | 1.2 (7.3) | 0.219 |
| Baseline WHO status | 0.150 | |||
| 0–1 (%) | 71 (75.5) | 53 (79.1) | 18 (66.7) | |
| 2–3 (%) | 23 (24.4) | 14 (20.9) | 9 (33.3) | |
| GERD (%) | 54 (57.4) | 36 (53.7) | 18 (66.6) | 0.251 |
| Distance to the Z-line (cm) * | 38.5 (4.5) | 37.9 (4.9) | 40.1 (2.6) | 0.022 |
| Superior tumor margin (cm) * | 34.5 (3.5) | 34.0 (3.6) | 36 (3.0) | 0.013 |
| Inferior tumor margin (cm) * | 39.5 (3.3) | 39.1 (3.1) | 40.8 (3.7) | 0.074 |
| cT stage | 0.897 | |||
| 2 (%) | 7 (7.2) | 5 (7.4) | 2 (7.4) | |
| 3–4 (%) | 76 (80.8) | 56 (83.5) | 20 (74) | |
| pTx | 11 | - | - | |
| cN stage | 0.984 | |||
| 0 (%) | 20 (21.3) | 15 (22.4) | 5 (18.5) | |
| 14 (51.8) | ||||
| 3 (11.1) | ||||
| SUVmax (g/L) | 14 [7.1] | 14.5 [7.5] | 12.7 [5.6] | 0.233 |
| Radiotherapy dose | <0.001 | |||
| 41.4 Gy (%) | 25 (26.5) | 24 (35.8) | 1 ** (3.7) | |
| 45 Gy (%) | 17 (18.0) | 17 (25.3) | 0 (0) | |
| 50.4 Gy (%) | 22 (23.4) | 22 (32.8) | 0 (0) | |
| Chemotherapy regimen | <0.001 | |||
| 5FU-platin (%) | 5 (5.3) | 3 (4.4) | 2 (7.4) | |
| EOX (%) | 17 (18.0) | 3 (4.4) | 14 (51.8) | |
| FLOT (%) | 10 (10.6) | 1 (1.5) | 9 (33.3) | |
| Platin-Taxol (%) | 56(59.5) | 55(82) | 1(3.7) | |
| Others (%) | 5 (5.3) | 5 (7.4) | 0 (0) | |
| Unknown | 1 | 0 | 1 | |
| Treatment modification due to toxicity (%) | 20 (21.2) | 11 (16.4) | 9 (33.3) | 0.076 |
| Histopathologic Variables | All Patients N = 94 | RCT N = 67 | CT N = 27 | p-Value |
|---|---|---|---|---|
| ypT stage (%) | 0.858 | |||
| 0 | 11 (11.7) | 9 (13.4) | 2 (7.4) | |
| 1 | 13 (13.8) | 8 (12) | 5 (18.5) | |
| 2 | 10 (10.6) | 8 (12) | 2 (7.4) | |
| 3 | 57 (60.3) | 40 (59.7) | 17 (63) | |
| 4 | 3 (3.2) | 2 (3) | 1 (3.7) | |
| ypN stage (%) | 0.057 | |||
| 0 | 46 (49) | 37 (55.2) | 9 (33.3) | |
| 1 | 21 (22.3) | 14 (20.9) | 7 (26) | |
| 2 | 17 (18) | 12 (18) | 5 (18.5) | |
| 3 | 10 (10.6) | 4 (6) | 6 (22.2) | |
| R1 resection (%) | 24 (25.5) | 16 (23.8) | 8 (29.6) | 0.628 |
| Circumferential resection margin (mm) | 3.0 (6.7) | 2.4 (3.1) | 4.2 (11.2) | 0.492 |
| Tumor regression grade (TRG) [22] (%) | 0.009 | |||
| 1 | 11 (11.7) | 9 (13.4) | 2 (7.4) | |
| 2 | 24 (25.5) | 19 (28.3) | 5 (18.5) | |
| 3 | 20 (21.2) | 18 (26.8) | 2 (7.4) | |
| 4 | 33 (35.1) | 19 (28.3) | 14 (51.8) | |
| 5 | 3 (3.2) | 0 (0) | 2 (11.1) | |
| Lymphovascular invasion (L1) (%) | 32 (34) | 18 (26.8) | 14 (51.8) | 0.041 |
| Microvascular invasion (V1) (%) | 27 (28.7) | 17 (25.3) | 10 (37) | 0.305 |
| Perineural invasion (Pn1) (%) | 31 (32.0) | 18 (26.8) | 13 (48.1) | 0.096 |
| Signet-ring histology (%) | 16 (17) | 10 (15) | 6 (22.2) | 0.410 |
| HER2 (+) status (%) | 8 (8.5) | 6 (9) | 2 (7.4) | 0.472 |
| Positive lymph nodes (%) | 2.3 [4.2] | 1.7 [2.6] | 4.0 [6.5] | 0.083 |
| Harvested lymph nodes (%) | 24.4 [10.5] | 21.6 [7.6] | 31.3 [13] | 0.001 |
| Barrett’s metaplasia (%) | 34 (36.1) | 27 (40.3) | 7 (26) | 0.256 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zandirad, E.; Teixeira Farinha, H.; Barberá-Carbonell, B.; Geinoz, S.; Demartines, N.; Schäfer, M.; Mantziari, S. Neoadjuvant Chemoradiotherapy versus Chemotherapy for Gastroesophageal Junction Adenocarcinoma; Which Is the Optimal Treatment Option? Cancers 2022, 14, 5856. https://doi.org/10.3390/cancers14235856
Zandirad E, Teixeira Farinha H, Barberá-Carbonell B, Geinoz S, Demartines N, Schäfer M, Mantziari S. Neoadjuvant Chemoradiotherapy versus Chemotherapy for Gastroesophageal Junction Adenocarcinoma; Which Is the Optimal Treatment Option? Cancers. 2022; 14(23):5856. https://doi.org/10.3390/cancers14235856
Chicago/Turabian StyleZandirad, Eric, Hugo Teixeira Farinha, Beatriz Barberá-Carbonell, Sandrine Geinoz, Nicolas Demartines, Markus Schäfer, and Styliani Mantziari. 2022. "Neoadjuvant Chemoradiotherapy versus Chemotherapy for Gastroesophageal Junction Adenocarcinoma; Which Is the Optimal Treatment Option?" Cancers 14, no. 23: 5856. https://doi.org/10.3390/cancers14235856
APA StyleZandirad, E., Teixeira Farinha, H., Barberá-Carbonell, B., Geinoz, S., Demartines, N., Schäfer, M., & Mantziari, S. (2022). Neoadjuvant Chemoradiotherapy versus Chemotherapy for Gastroesophageal Junction Adenocarcinoma; Which Is the Optimal Treatment Option? Cancers, 14(23), 5856. https://doi.org/10.3390/cancers14235856