
Survival Analysis in Endometrial Carcinomas by Type of Surgical Approach: A Matched-Pair Study

 , , ,
, , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
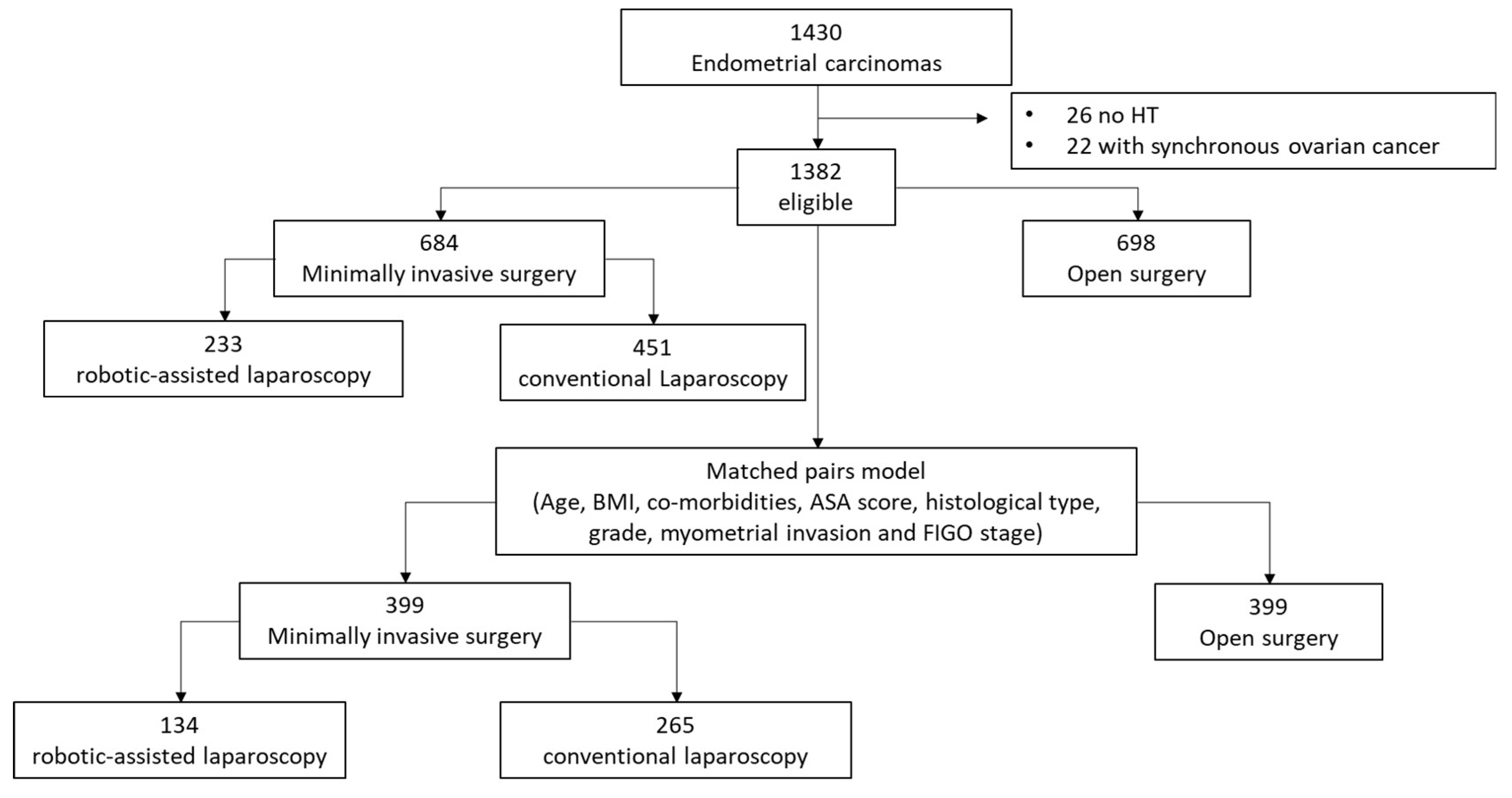
2.1. Study Design and Participants
2.2. Matched-Pair Model
2.3. Statistical Analysis
3. Results
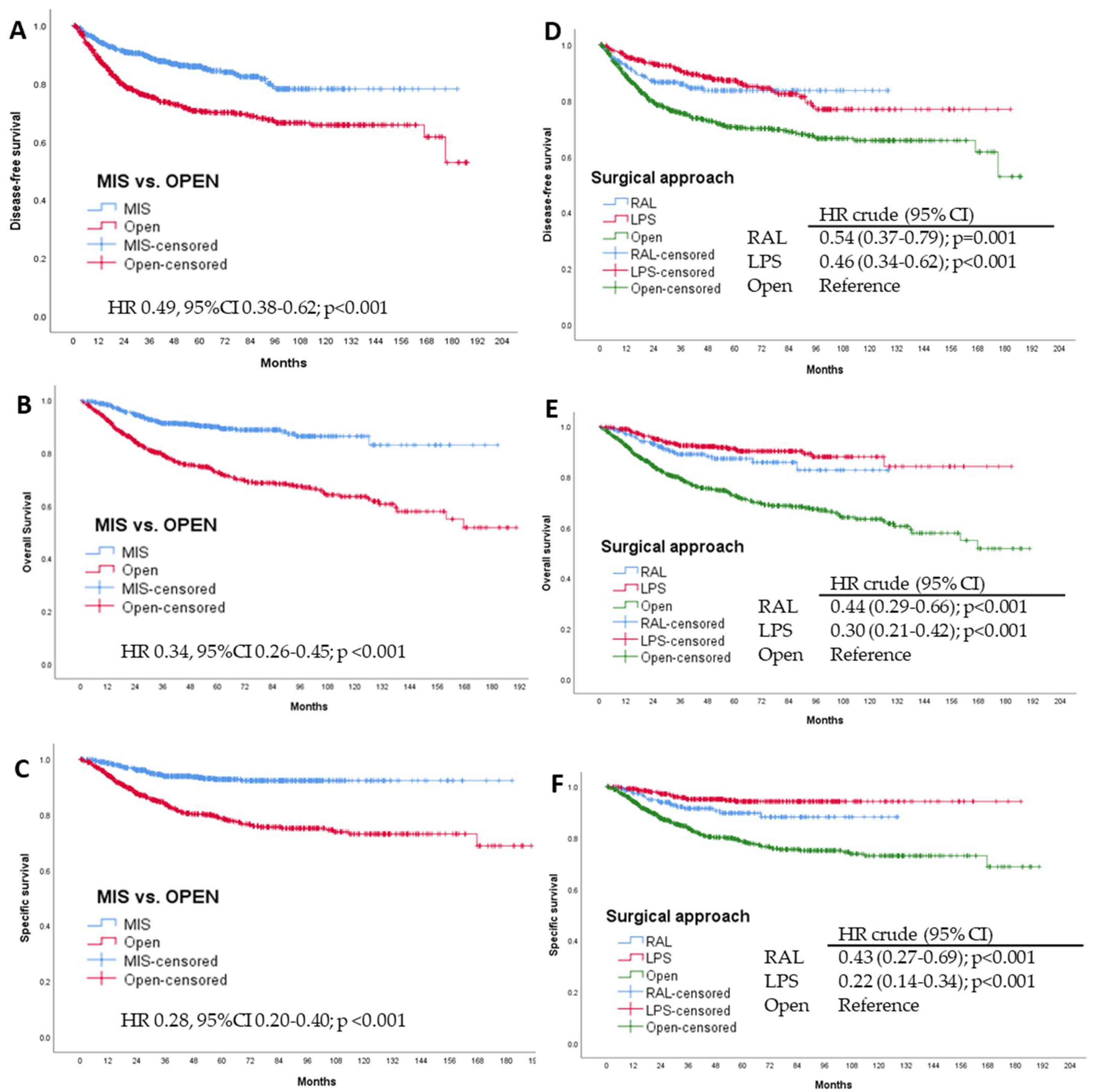
3.1. Whole Sample: MIS vs. Open Surgery
3.2. Whole Sample: MIS Subanalysis
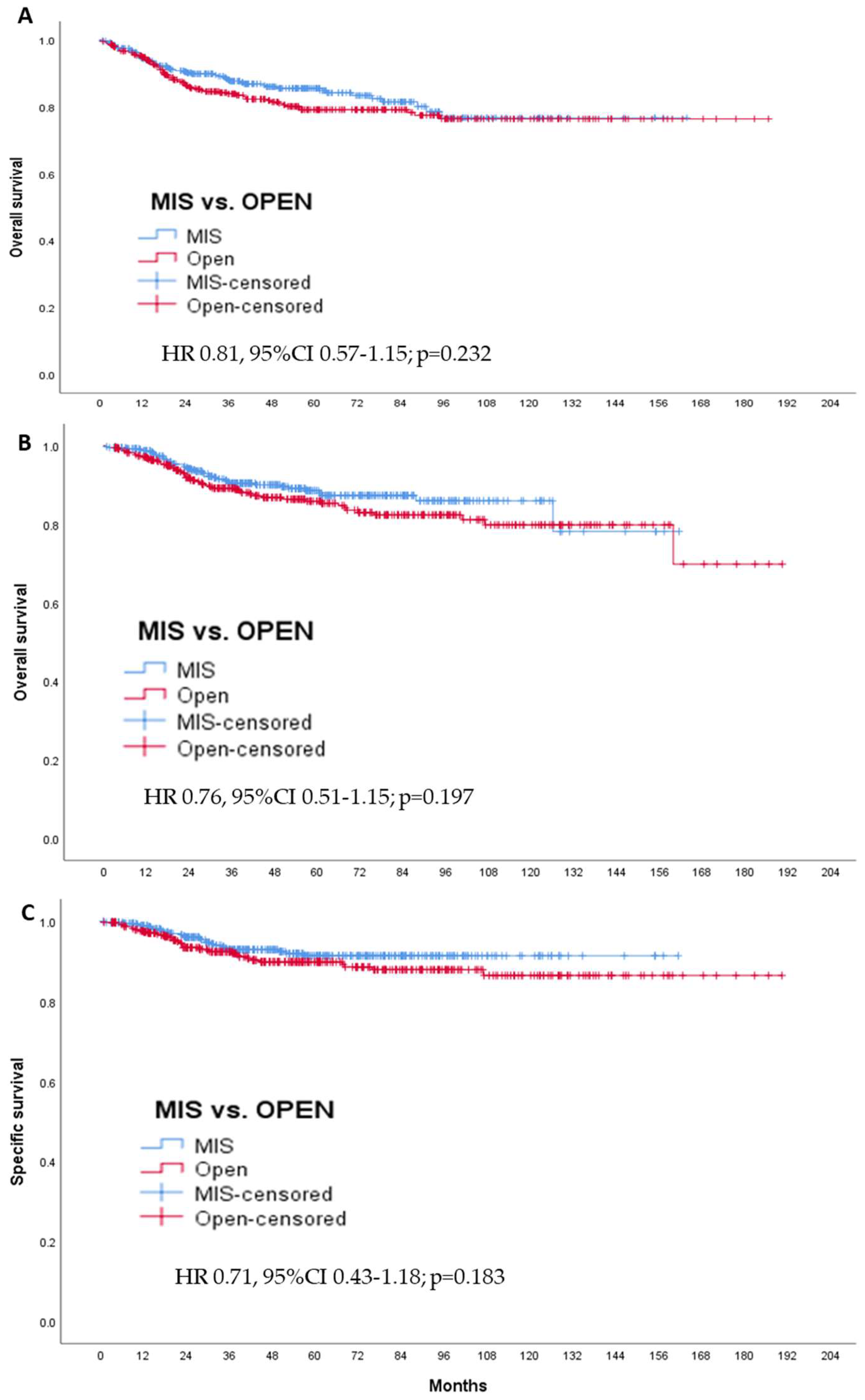
3.3. Matched-Pair Analysis: MIS vs. Open Surgery
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataran, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2018, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramirez, P.T.; Frumovitz, M.; Pareja, R.; López, A.; Vieira, M.; Ribeiro, M.; Buda, A.; Yan, X.; Shuzhong, Y.; Chetty, N. Minimally invasive versus abdominal radical hysterectomy for cervical cancer. N. Engl. J. Med. 2018, 379, 1895–1904. [Google Scholar] [CrossRef] [PubMed]
- Melamed, A.; Margul, D.J.; Chen, L.; Keating, N.L.; Del Carmen, L.G.; Yang, J.; Seagle, B.L.; Alexander, A.; Barber, E.L.; Rice, L.W.; et al. Survival after minimally invasive radical hysterectomy for early-stage cervical cancer. N. Engl. J. Med. 2018, 379, 1905–1914. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.L.; Piedmonte, M.R.; Spirtos, N.M.; Eisenkop, S.M.; Schlaerth, J.B.; Mannel, R.S.; Spiegel, G.; Barakat, R.; Pearl, M.L.; Sharma, S.K. Laparoscopy compared with laparotomy for comprehensive surgical staging of uterine cancer: Gynecologic Oncology Group Study LAP2. J. Clin. Oncol. 2009, 27, 5331–5336. [Google Scholar] [CrossRef]
- Jørgensen, S.L.; Mogensen, O.; Chunsen, S.; Korsholm, M.; Lund, K.; Jensen, P. Survival after a nationwide introduction of robotic surgery in women with early-stage endometrial cancer: A population-based prospective cohort study. Eur. J. Cancer 2019, 109, 1–11. [Google Scholar] [CrossRef]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13 (Suppl. S1), S31–S34. [Google Scholar] [CrossRef]
- Oncoguía SEGO (ES). Cancer de Endometrio 2010. Guías de Práctica Clínica en Cancer Ginecologico y; Publicaciones SEGO: Mamario, Madrid, 2010. [Google Scholar]
- Colombo, N.; Creutzberg, C.; Amant, F.; Bosse, T.; Martín, A.G.; Ledermann, J.; Marth, C.; Nout, A.R.; Querleu, D.; Mirza, M.R.; et al. ESMO-ESGO-ESTRO Consensus Conference on Endometrial Cancer: Diagnosis, Treatment and Follow-up. Int. J. Gynecol. Cancer 2016, 26, 2–30. [Google Scholar] [CrossRef] [Green Version]
- Janda, M.; Gebski, V.; Davies, L.C.; Forder, P.; Brand, A.; Hogg, R.; Jobling, T.W.; Land, R.; Manolitsas, R.; Nascimento, M. Effect of Total Laparoscopic Hysterectomy vs Total Abdominal Hysterectomy on Disease-Free Survival Among Women With Stage I Endometrial Cancer: A Randomized Clinical Trial. JAMA 2017, 317, 1224–1233. [Google Scholar] [CrossRef] [Green Version]
- Walker, J.L.; Piedmonte, M.R.; Spirtos, N.M.; Eisenkop, S.M.; Schlaerth, J.B.; Mannel, R.; Barakat, R.; Pearl, M.; Sudarshan, K.S. Recurrence and survival after random assignment to laparoscopy versus laparotomy for comprehensive surgical staging of uterine cancer: Gynecologic Oncology Group LAP2 Study. J. Clin. Oncol. 2012, 30, 695–700. [Google Scholar] [CrossRef] [Green Version]
- Jørgensen, S.L.; Mogensen, O.; Wu, C.; Lund, K.; Iachina, M.; Korsholm, M.; Jensen, P.T. Nationwide Introduction of Minimally Invasive Robotic Surgery for Early-Stage Endometrial Cancer and Its Association With Severe Complications. JAMA Surg. 2019, 154, 530–538. [Google Scholar] [CrossRef] [Green Version]
- Beck, T.L.; Schiff, M.A.; Goff, B.A.; Urban, R.R. Robotic, laparoscopic or open hysterectomy: Surgical outcomes by approach in endometrial cancer. J. Minim. Invasive Gynecol. 2018, 25, 986–993. [Google Scholar] [CrossRef] [PubMed]
- Janda, M.; Gebski, V.; Brand, A.; Hogg, R.; Jobling, T.W.; Land, R.; Manolitsas, T.; McCartney, A.; Nascimento, M.; Neesham, D.; et al. Quality of life after total laparoscopic hysterectomy versus total abdominal hysterectomy. Lancet Oncol. 2010, 11, 772–780. [Google Scholar] [CrossRef] [Green Version]
- Zullo, F.; Palomba, S.; Russo, T.; Falbo, A.; Constantino, M.; Tolino, A.; Zupi, E.; Tagliaferri, P.; Venuta, S. A prospective randomized comparison between laparoscopic and laparotomic approaches in women with early-stage endometrial cancer: A focus on the quality of life. Am. J. Obstet. Gynecol. 2005, 193, 1344–1352. [Google Scholar] [CrossRef] [PubMed]
- Park, D.A.; Lee, D.H.; Kim, S.W.; Lee, S.H. Comparative safety and effectiveness of robot-assisted laparoscopic hysterectomy versus conventional laparoscopy and laparotomy for endometrial cancer: A systematic review and meta-analysis. Eur. J. Surg. Oncol. 2016, 42, 1303–1314. [Google Scholar] [CrossRef]
- Kyrgiou, M.; Swart, A.M.; Qian, W.; Warwick, J. A Comparison of Outcomes Following Laparoscopic and Open Hysterectomy With or Without Lymphadenectomy for Presumed Early-Stage Endometrial Cancer: Results From the Medical Research Council ASTEC Trial. Int. J. Gynecol. Cancer 2015, 25, 1424–1436. [Google Scholar] [CrossRef]
- Asher, R.; Obermair, A.; Janda, M.; Gebski, V. Disease-Free and Survival Outcomes for Total Laparoscopic Hysterectomy Compared With Total Abdominal Hysterectomy in Early-Stage Endometrial Carcinoma: A Meta-analysis. Int. J. Gynecol. Cancer 2018, 28, 529–538. [Google Scholar] [CrossRef]
- Coronado, P.J.; Herráiz, M.A.; Magrina, J.F.; Fasero, M.; Vidart, J.A. Comparison of perioperative outcomes and cost of robotic-assisted laparoscopy, laparoscopy and laparotomy for endometrial cáncer. Eur. J. Obstet. Gynecol. Reprod Biol. 2012, 165, 289–294. [Google Scholar] [CrossRef]
- Monterossi, G.; Ghezzi, F.; Vizza, E.; Zannoni, G.F.; Uccela, S.; Corrado, G.; Restaino, S.; Quagliozzi, L.; Casarin, J.; Dinoi, G.; et al. Minimally invasive approach in type II endometrial cáncer: Is it wise and safe? J. Minim. Invasive Gynecol. 2017, 24, 438–445. [Google Scholar] [CrossRef]
- Segarra-Vidal, B.; Dinoi, G.; Zorrilla-Vaca, A.; Mariani, A.; Student, V.; Garcia, N.A.; Abella, A.L.; Ramirez, P.T. Minimally Invasive Compared With Open Hysterectomy in High-Risk Endometrial Cancer. Obstet. Gynecol. 2021, 138, 828–837. [Google Scholar] [CrossRef]
- Scaletta, G.; Dinoi, G.; Capozzi, V.; Cianci, S.; Pelligra, S.; Ergasti, R.; Fagotti, A.; Scambia, G.; Fanfani, F. Comparison of minimally invasive surgery with laparotomic approach in the treatment of high-risk endometrial cancer: A systematic review. Eur. J. Surg. Oncol. 2020, 46, 782–788. [Google Scholar] [CrossRef]
- Koh, W.J.; Abu-Rustum, N.; Bean, S.; Bradley, K.; Campos, S.; Cho, K.R.; Chon, H.S.; Chu, C.; Cohn, D.; Crispens, M.A. Uterine Neoplasms, Version 1.2018, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Can. Netw. 2018, 16, 170–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int. J. Gynecol. Cancer 2021, 31, 12–39. [Google Scholar] [CrossRef] [PubMed]
- Concin, N.; Planchamp, F.; Abu-Rustum, N.; Ataseven, B.; Cibula, D.; Fagotti, A.; Fotopoulou, C.; Knapp, P.; Marth, C.; Morice, P.; et al. European Society of Gynaecological Oncology quality indicators for the surgical treatment of endometrial carcinoma. Int. J. Gynecol. Cancer 2021, 31, 1508–1529. [Google Scholar] [CrossRef] [PubMed]
- Padilla-Iserte, P.; Quintana, R.; Marina, T.; Lago, V.; Matute, L.; Domingo, S. Uterine manipulator in endometrial cancer: A video is worth a thousand words. Int. J. Gynecol. Cancer 2021, 31, 147. [Google Scholar] [CrossRef]
- Padilla-Iserte, P.; Lago, V.; Tauste, C.; Díaz-Feijoo, B.; Gil-Moreno, A.; Oliver, R.; Coronado, P.; Salamanca, M.B.M.; Pantoja-Garrido, M.; Marcos-Sanmartin, J.; et al. Impact of uterine manipulator on oncological outcome in endometrial cancer surgery. Am. J. Obstet. Gynecol. 2021, 224, 65.e1–65.e11. [Google Scholar] [CrossRef] [PubMed]
- Ran, L.; Jin, J.; Xu, Y.; Youquan, B.; Song, F. Comparison of robotic surgery with laparoscopy and laparotomy for treatment of endometrial cancer: A meta-analysis. PLoS ONE 2014, 26, e108361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gala, R.B.; Margulies, R.; Steinberg, A.; Murphy, M.; Lukban, J.; Jeppson, P.; Aschkenazi, S.; Olivera, C.; South, M.; Lowenstein, L.; et al. Systematic review of robotic surgery in gynecology: Robotic techniques compared with laparoscopy and laparotomy. J. Minim. Invasive Gynecol. 2014, 21, 353–361. [Google Scholar] [CrossRef]
- Gracia, M.; García-Santos, J.; Ramírez, M.; Bellón, M.; Herráiz, M.A.; Coronado, P. Value of robotic surgery in endometrial cancer by body mass index. Int. J. Gynaecol. Obstet 2020, 150, 398–405. [Google Scholar] [CrossRef]
- Subramaniam, A.; Kim, K.H.; Bryant, S.A.; Zhang, B.; Sikes, C.; Kimball, K.J.; Kilgore, L.C.; Huh, W.K.; Straughn, J.M., Jr.; Alvarez, R.D. A cohort study evaluating robotic versus laparotomy surgical outcomes of obese women with endometrial carcinoma. Gynecol. Oncol. 2011, 122, 604–607. [Google Scholar] [CrossRef]
- Seamon, L.G.; Bryant, S.A.; Rheaume, P.S.; Kimball, K.J.; Huh, W.K.; Fowler, J.M.; Phillips, G.S.; Cohn, D.E. Comprehensive surgical staging for endometrial cancer in obese patients: Comparing robotics and laparotomy. Obstet Gynecol. 2009, 114, 16–21. [Google Scholar] [CrossRef]
- Rebeles, S.A.; Muntz, H.G.; Wieneke-Broghammer, C.; Vason, E.; McGonigle, K.F. Robot-assisted total laparoscopic hysterectomy in obese and morbidly obese women. J. Robot. Surg. 2009, 3, 14. [Google Scholar] [CrossRef] [PubMed]
- Lau, S.; Buzaglo, K.; Vaknin, Z.; Brin, S.; Kaufer, R.; Drummond, N.; Gourdji, I.; Aubin, S.; Rosberger, Z.; Gotlieb, W.H. Relationship between body mass index and robotic surgery outcomes of women diagnosed with endometrial cancer. Int. J. Gynecol. Cancer 2011, 21, 722–729. [Google Scholar] [CrossRef] [PubMed]
- Bernardini, M.Q.; Gien, L.T.; Tipping, H.; Murphy, J.; Rosen, B.P. Surgical outcome of robotic surgery in morbidly obese patient with endometrial cancer compared to laparotomy. Int. J. Gynecol. Cancer 2012, 22, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Eoh, K.J.; Nam, E.; Kim, S.W.; Shin, M.; Kim, S.; Kim, J.; Kim, Y. Nationwide Comparison of Surgical and Oncologic Outcomes in Endometrial Cancer Patients Undergoing Robotic, Laparoscopic, and Open Surgery: A Population-Based Cohort Study. Cancer Res. Treat. 2021, 53, 549–557. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | MIS N = 684 | Open N = 698 | p-Value |
|---|---|---|---|
| Age (years) | 65.5 ± 10.5 | 67.2 ± 10.7 | 0.003 |
| BMI (kg/m2) | 29.0 ± 5.8 | 30.2 ± 5.5 | <0.001 |
| Associated diseases 1 | 427 (62.4) | 475 (68.1) | 0.028 |
| American Society of Anesthesiologists (ASA) | <0.001 | ||
| 480 (74.4) | 344 (50.5) | |
| 141 (21.9) | 211 (31.0) | |
| 24 (3.7) | 126 (18.5) | |
| Family history of cancer | <0.001 | ||
| 431 (63.3) | 520 (75.1) | |
| 48 (7.0) | 16 (2.3) | |
| 9 (1.3) | 19 (2.7) | |
| 64 (9.4) | 46 (6.6) | |
| 132 (19.0) | 97 (13.3) | |
| Years from menopause | 2.9 ± 0.4 | 2.9 ± 0.5 | 0.581 |
| Parity | 1.9 ± 1.6 | 2.0 ± 1.8 | 0.081 |
| Histologic subtype | <0.001 | ||
| 605 (88.5) | 506 (72.5) | |
| 44 (6.4) | 88 (12.6) | |
| 17 (2.5) | 38 (5.4) | |
| 12 (1.8) | 59 (8.5) | |
| 6 (0.9) | 7 (1.0) | |
| Histological grade | <0.001 | ||
| 537 (78.5) | 429 (61.7) | |
| 147 (21.5) | 266 (38.3) | |
| Myometrial invasion | <0.001 | ||
| 364 (53.2) | 296 (42.4) | |
| 320 (46.8) | 402 (57.6) | |
| LVSI (n = 1330) | 0.002 | ||
| 554 (82.1) | 492 (75.1) | |
| 121 (17.9) | 163 (24.9) | |
| Postoperative stage | <0.001 | ||
| 621 (90.8) | 578 (82.8) | |
| 63 (9.2) | 120 (17.2) | |
| FIGO stage | <0.001 | ||
| 563 (82.3) | 485 (69.5) | |
| 35 (5.1) | 56 (8.0) | |
| 73 (10.7) | 114 (16.3) | |
| 13 (1.9) | 43 (6.2) | |
| Lymphadenectomy | 0.623 | ||
| 236 (34.5) | 238 (34.1) | |
| 285 (41.7) | 292 (41.8) | |
| 162 (23.7) | 164 (23.5) | |
| 1 (0.1) | 4 (0.6) | |
| ESGO risk group | <0.001 | ||
| 248 (36.3) | 133 (19.1) | |
| 166 (24.3) | 170 (24.4) | |
| 80 (11.7) | 72 (10.3) | |
| 177 (25.9) | 280 (40.1) | |
| 14 (1.9) | 43 (6.1) | |
| Adjuvant therapies | <0.001 | ||
| 274 (40.1) | 218 (31.2) | |
| 332 (48.5) | 331 (47.4) | |
| 10 (1.5) | 32 (4.6) | |
| 68 (9.9) | 117 (16.8) | |
| Length of follow-up (months) | 57.3 ± 34.5 | 63.5 ± 46.4 | 0.012 |
| Variable | Robotic N = 233 | LPS N = 451 | p-Value |
|---|---|---|---|
| Age (years) | 65.7 ± 10.3 | 65.5 ± 10.6 | 0.800 |
| BMI (kg/m2) | 29.2 ± 5.9 | 28.9 ± 5.8 | 0.404 |
| Associated diseases 1 | 145 (62.2) | 282 (62.5) | 0.940 |
| American Society of Anesthesiologists (ASA) | 0.016 | ||
| 165 (72.2) | 315 (75.4) | |
| 59 (26.0) | 82 (19.6) | |
| 3 (1.3) | 21 (5.0) | |
| Years from menopause | 2.9 ± 0.3 | 2.9 ± 0.2 | 0.762 |
| Parity | 1.7 ± 0.1 | 1.5 ± 0.1 | 0.063 |
| Histologic subtype | 0.373 | ||
| 204 (87.6) | 401 (88.9) | |
| 16 (6.9) | 28 (6.2) | |
| 5 (2.1) | 12 (2.7) | |
| 7 (3.0) | 5 (1.1) | |
| 1 (0.4) | 5 (1.1) | |
| Histological grade | 0.051 | ||
| 173 (74.2) | 364 (80.7) | |
| 60 (25.8) | 87 (19.3) | |
| Myometrial invasion | 0.052 | ||
| 136 (58.4) | 228 (50.6) | |
| 97 (41.6) | 223 (49.4) | |
| LVSI (n = 1330) | 0.039 | ||
| 201 (86.3) | 353 (79.9) | |
| 32 (13.7) | 89 (20.1) | |
| Postoperative stage | 0.479 | ||
| 209 (89.7) | 412 (91.4) | |
| 24 (10.3) | 39 (8.6) | |
| FIGO stage | 0.421 | ||
| 185 (79.4) | 378 (83.8) | |
| 12 (5.2) | 23 (5.1) | |
| 30 (12.9) | 43 (9.5) | |
| 6 (2.6) | 7 (1.6) | |
| Lymphadenectomy | <0.001 | ||
| 74 (31.8) | 162 (35.9) | |
| 120 (51.5) | 165 (36.6) | |
| 38 (16.3) | 124 (27.5) | |
| 1 (0.4) | 0 (0) | |
| ESGO risk group | <0.001 | ||
| 103 (44.2) | 145 (32.2) | |
| 41 (17.6) | 125 (27.7) | |
| 15 (6.4) | 65 (14.4) | |
| 68 (29.2) | 109 (24.2) | |
| 6 (2.6) | 7 (1.6) | |
| Adjuvant therapies | 0.012 | ||
| 100 (42.9) | 174 (38.6) | |
| 96 (41.2) | 236 (52.3) | |
| 5 (2.10) | 5 (1.1) | |
| 32 (13.7) | 36 (8.0) | |
| Lenth of follow up | 50.8 ± 30.2 | 60.6 ± 36.0 | 0.013 |
| Variable | MIS N = 399 | Open N = 399 | p-Value |
|---|---|---|---|
| Age (years) | 66.4 ± 10.4 | 66.0 ±10.8 | 0.861 |
| BMI (kg/m2) | 30.0 ± 5.8 | 30.4 ± 5.5 | 0.318 |
| Associated diseases 1 | 270 (67.7) | 270 (67.7) | >0.999 |
| American Society of Anesthesiologists (ASA) | >0.999 | ||
| 268 (67.2) | 268 (67.2) | |
| 102 (25.6) | 102 (25.6) | |
| 29 (7.2) | 29 (7.2) | |
| Years from menopause | 2.9 ± 0.4 | 2.8 ± 0.5 | 0.063 |
| Parity | 2.1 ± 1.9 | 2.1 ± 1.9 | 0.996 |
| Histologic subtype | >0.999 | ||
| 345 (86.5) | 345 (86.5) | |
| 31 (7.8) | 31 (7.8) | |
| 12 (3.0) | 12 (3.0) | |
| 9 (2.3) | 9 (2.3) | |
| 2 (0.5) | 2 (0.5) | |
| Histological grade | >0.999 | ||
| 295 (73.9) | 295 (73.9) | |
| 104 (26.1) | 104 (26.1) | |
| Myometrial invasion | >0.999 | ||
| 189 (47.4) | 189 (47.4) | |
| 210 (52.6) | 210 (52.6) | |
| LVSI (n = 765) | 0.349 | ||
| 320 (81.6) | 314 (83.7) | |
| 72 (18.4) | 59 (15.7) | |
| Postoperative Stage | >0.999 | ||
| 346 (86.7) | 346 (86.7) | |
| 53 (13.3) | 53 (13.3) | |
| FIGO stage | 0.623 | ||
| 324 (81.2) | 318 (79.7) | |
| 22 (5.5) | 29 (7.3) | |
| 45 (11.3) | 41 (10.0) | |
| 8 (2.0) | 12 (3.0) | |
| Lymphadenectomy | 0.175 | ||
| 118 (29.6) | 130 (32.6) | |
| 169 (42.4) | 184 (46.1) | |
| 111 (27.8) | 84 (21.1) | |
| 1 (0.3) | 1 (0.3) | |
| ESGO risk group | 0.837 | ||
| 112 (28.1) | 112 (28.1) | |
| 115 (28.8) | 121 (30.3) | |
| 46 (11.5) | 40 (10.0) | |
| 118 (29.6) | 114 (28.6) | |
| 8 (2.0) | 12 (3.0) | |
| Adjuvant therapies | 0.423 | ||
| 142 (35.6) | 144 (36.1) | |
| 204 (51.1) | 192 (48.1) | |
| 7 (1.8) | 14 (3.5) | |
| 46 (11.5) | 49 (12.3) | |
| Length of follow-up | 57.7 ± 34.5 | 63.5 ± 46.4 | 0.012 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coronado, P.J.; Rychlik, A.; Baquedano, L.; García-Pineda, V.; Martínez-Maestre, M.A.; Querleu, D.; Zapardiel, I. Survival Analysis in Endometrial Carcinomas by Type of Surgical Approach: A Matched-Pair Study. Cancers 2022, 14, 1081. https://doi.org/10.3390/cancers14041081
Coronado PJ, Rychlik A, Baquedano L, García-Pineda V, Martínez-Maestre MA, Querleu D, Zapardiel I. Survival Analysis in Endometrial Carcinomas by Type of Surgical Approach: A Matched-Pair Study. Cancers. 2022; 14(4):1081. https://doi.org/10.3390/cancers14041081
Chicago/Turabian StyleCoronado, Pluvio J., Agnieszka Rychlik, Laura Baquedano, Virginia García-Pineda, Maria A. Martínez-Maestre, Denis Querleu, and Ignacio Zapardiel. 2022. "Survival Analysis in Endometrial Carcinomas by Type of Surgical Approach: A Matched-Pair Study" Cancers 14, no. 4: 1081. https://doi.org/10.3390/cancers14041081
APA StyleCoronado, P. J., Rychlik, A., Baquedano, L., García-Pineda, V., Martínez-Maestre, M. A., Querleu, D., & Zapardiel, I. (2022). Survival Analysis in Endometrial Carcinomas by Type of Surgical Approach: A Matched-Pair Study. Cancers, 14(4), 1081. https://doi.org/10.3390/cancers14041081