Immune-Related Thyroiditis as a Predictor for Survival in Metastatic Renal Cell Carcinoma

 ,
,  , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Study Variables
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Thyroid Hormone Dynamics
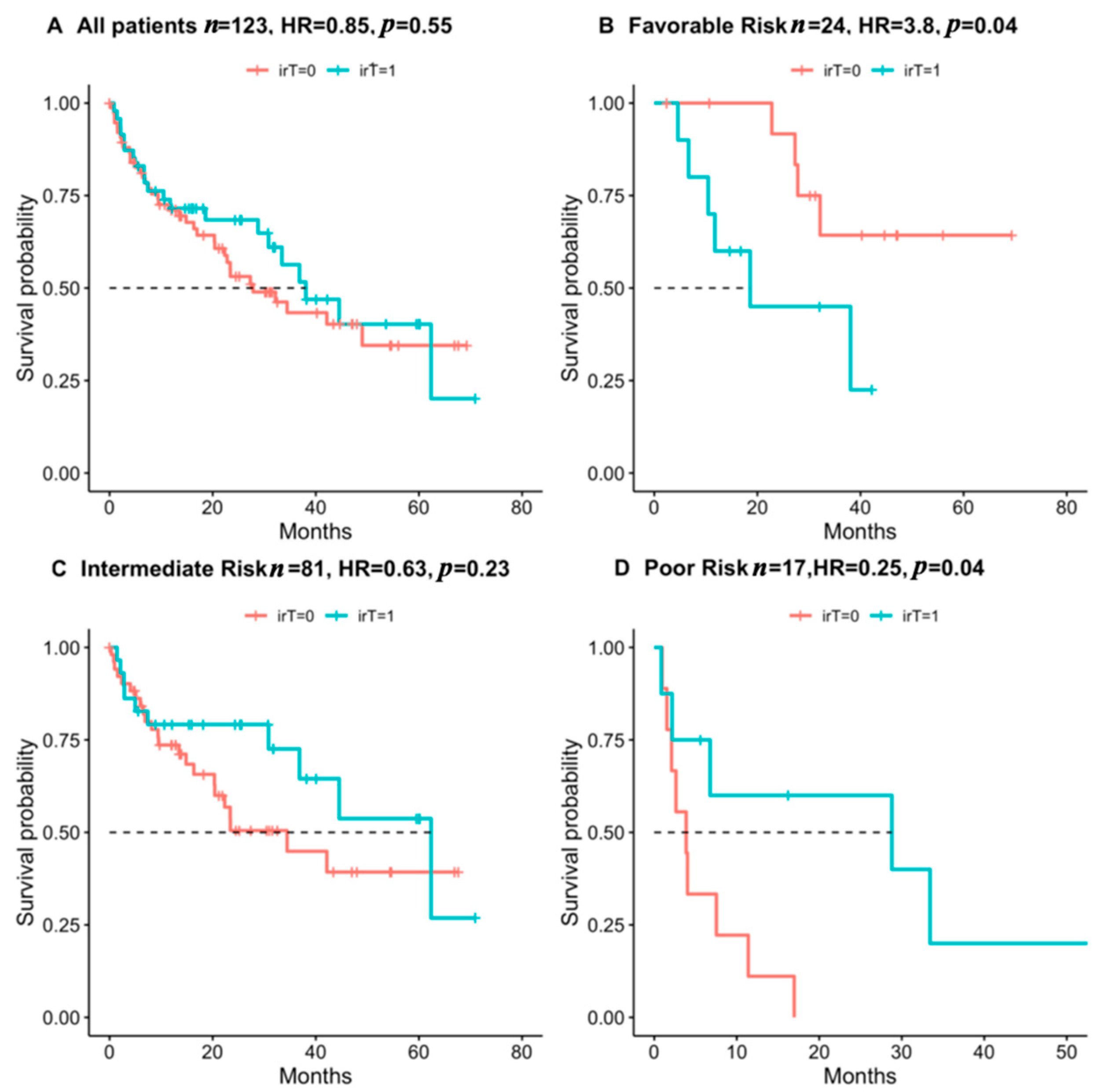
3.3. Immune Checkpoint Induced Thyroiditis as a Predictor for Survival in RCC Patients
3.4. Prevalence of Other Immune-Related Adverse Events and Effect on Survival
4. Discussion
4.1. irT among Patients with mRCC
4.2. irT and Survival
4.3. Other irAE
4.4. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Postow, M.A.; Sidlow, R.; Hellmann, M.D. Immune-Related Adverse Events Associated with Immune Checkpoint Blockade. N. Engl. J. Med. 2018, 378, 158–168. [Google Scholar] [CrossRef]
- Tran, J.; Ornstein, M.C. Clinical Review on the Management of Metastatic Renal Cell Carcinoma. JCO Oncol. Pract. 2021, OP-21. [Google Scholar] [CrossRef]
- Heng, D.Y.C.; Xie, W.; Regan, M.M.; Warren, M.A.; Golshayan, A.R.; Sahi, C.; Eigl, B.J.; Ruether, J.D.; Cheng, T.; North, S.; et al. Prognostic Factors for Overall Survival in Patients With Metastatic Renal Cell Carcinoma Treated With Vascular Endothelial Growth Factor–Targeted Agents: Results From a Large, Multicenter Study. J. Clin. Oncol. 2009, 27, 5794–5799. [Google Scholar] [CrossRef]
- Heng, D.Y.C.; Xie, W.; Regan, M.M.; Harshman, L.C.; Bjarnason, G.A.; Vaishampayan, U.N.; Mackenzie, M.; Wood, L.; Donskov, F.; Tan, M.-H.; et al. External validation and comparison with other models of the International Metastatic Renal-Cell Carcinoma Database Consortium prognostic model: A population-based study. Lancet Oncol. 2013, 14, 141. [Google Scholar] [CrossRef] [Green Version]
- Grünwald, V.; Powles, T.; Kopyltsov, E.; Kozlov, V.; Gordoa, T.A.; Eto, M.; Hutson, T.E.; Motzer, R.J.; Winquist, E.; Maroto-Rey, P.; et al. Analysis of the CLEAR study in patients (pts) with advanced renal cell carcinoma (RCC): Depth of response and efficacy for selected subgroups in the lenvatinib (LEN) + pembrolizumab (PEMBRO) and sunitinib (SUN) treatment arms. J. Clin. Oncol. 2021, 39, 4560. [Google Scholar] [CrossRef]
- Akamatsu, H.; Murakami, E.; Oyanagi, J.; Shibaki, R.; Kaki, T.; Takase, E.; Tanaka, M.; Harutani, Y.; Yamagata, N.; Okuda, Y.; et al. Immune-Related Adverse Events by Immune Checkpoint Inhibitors Significantly Predict Durable Efficacy Even in Responders with Advanced Non-Small Cell Lung Cancer. Oncologist 2020, 25, e679. [Google Scholar] [CrossRef] [Green Version]
- Paderi, A.; Giorgione, R.; Giommoni, E.; Mela, M.M.; Rossi, V.; Doni, L.; Minervini, A.; Carini, M.; Pillozzi, S.; Antonuzzo, L. Association between Immune Related Adverse Events and Outcome in Patients with Metastatic Renal Cell Carcinoma Treated with Immune Checkpoint Inhibitors. Cancers 2021, 13, 860. [Google Scholar] [CrossRef]
- Kotwal, A.; Kottschade, L.; Ryder, M. PD-L1 Inhibitor-Induced Thyroiditis Is Associated with Better Overall Survival in Cancer Patients. Thyroid 2020, 30, 177. [Google Scholar] [CrossRef]
- Basak, E.A.; van der Meer, J.W.M.; Hurkmans, D.P.; Schreurs, M.W.J.; Hoop, E.O.; van der Veldt, A.A.M.; Bins, S.; Joosse, A.; Koolen, S.L.W.; Debets, R.; et al. Overt Thyroid Dysfunction and Anti-Thyroid Antibodies Predict Response to Anti-PD-1 Immunotherapy in Cancer Patients. Thyroid 2020, 30, 966–973. [Google Scholar] [CrossRef]
- Al Mushref, M.; Guido, P.A.; Collichio, F.A.; Moore, D.T.; Clemmons, D.R. Thyroid Dysfunction, Recovery, and Prognosis in Melanoma Patients Treated with Immune Checkpoint Inhibitors: A Retrospective Review. Endocr. Pract. 2020, 26, 36–42. [Google Scholar] [CrossRef]
- Peiró, I.; Palmero, R.; Iglesias, P.; Díez, J.J.; Simó-Servat, A.; Marín, J.A.; Jiménez, L.; Domingo-Domenech, E.; Mancho-Fora, N.; Nadal, E.; et al. Thyroid dysfunction induced by nivolumab: Searching for disease patterns and outcomes. Endocrine 2019, 64, 605–613. [Google Scholar] [CrossRef]
- Percik, R.; Liel, Y.; Urban, D.; Bar, J.; Ben-Ami, E.; Tailakh, M.A. Thyroid dysfunction and survival in cancer patients treated with immune checkpoint inhibitors: Analyses from a large single tertiary cancer center database. Acta Oncol. 2021, 60, 1466–1471. [Google Scholar] [CrossRef] [PubMed]
- Kotwal, A.; Gustafson, M.P.; Bornschlegl, S.; Kottschade, L.; Delivanis, D.A.; Dietz, A.B.; Gandhi, M.; Ryder, M. Immune Checkpoint Inhibitor-Induced Thyroiditis Is Associated with Increased Intrathyroidal T Lymphocyte Subpopulations. Thyroid 2020, 30, 1440. [Google Scholar] [CrossRef]
- Angell, T.E.; Min, L.; Wieczorek, T.J.; Hodi, F.S. Unique cytologic features of thyroiditis caused by immune checkpoint inhibitor therapy for malignant melanoma. Genes Dis. 2018, 5, 46. [Google Scholar] [CrossRef] [PubMed]
- Imblum, B.A.; Baloch, Z.W.; Fraker, D.; LiVolsi, V.A. Pembrolizumab-Induced Thyroiditis. Endocr. Pathol. 2019, 30, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, T.; Iwama, S.; Yasuda, Y.; Okada, N.; Tsunekawa, T.; Onoue, T.; Takagi, H.; Hagiwara, D.; Ito, Y.; Morishita, Y.; et al. Patients With Antithyroid Antibodies Are Prone To Develop Destructive Thyroiditis by Nivolumab: A Prospective Study. J. Endocr. Soc. 2018, 2, 241. [Google Scholar] [CrossRef]
- Mazarico, I.; Capel, I.; Giménez-Palop, O.; Albert, L.; Berges, I.; Luchtenberg, F.; García, Y.; Fernández-Morales, L.A.; De Pedro, V.J.; Caixàs, A.; et al. Low frequency of positive antithyroid antibodies is observed in patients with thyroid dysfunction related to immune check point inhibitors. J. Endocrinol. Investig. 2019, 42, 1443–1450. [Google Scholar] [CrossRef]
- Street, S.; Chute, D.; Strohbehn, I.; Zhao, S.; Rengarajan, M.; Faje, A.; Seethapathy, H.; Lee, M.; Seethapathy, R.; Drobni, Z.; et al. The positive effect of immune checkpoint inhibitor-induced thyroiditis on overall survival accounting for immortal time bias: A retrospective cohort study of 6596 patients. Ann. Oncol. 2021, 32, 1050–1051. [Google Scholar] [CrossRef]
- Muir, C.A.; Clifton-Bligh, R.J.; Long, G.V.; Scolyer, R.A.; Lo, S.N.; Carlino, M.S.; Tsang, V.H.M.; Menzies, A.M. Thyroid Immune-related Adverse Events Following Immune Checkpoint Inhibitor Treatment. J. Clin. Endocrinol. Metab. 2021, 106, e3704–e3713. [Google Scholar] [CrossRef]
- Chalan, P.; Di Dalmazi, G.; Pani, F.; De Remigis, A.; Corsello, A.; Caturegli, P. Thyroid dysfunctions secondary to cancer immunotherapy. J. Endocrinol. Investig. 2018, 41, 625. [Google Scholar] [CrossRef]
- Wolter, P.; Stefan, C.; Decallonne, B.; Dumez, H.; Bex, M.; Carmeliet, P.; Schöffski, P. The clinical implications of sunitinib-induced hypothyroidism: A prospective evaluation. Br. J. Cancer 2008, 99, 448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palapattu, G.S.; Kristo, B.; Rajfer, J. Paraneoplastic Syndromes in Urologic Malignancy: The Many Faces of Renal Cell Carcinoma. Rev. Urol. 2002, 4, 163. [Google Scholar] [PubMed]
- Manola, J.; Royston, P.; Elson, P.; McCormack, J.B.; Mazumdar, M.; Négrier, S.; Escudier, B.; Eisen, T.; Dutcher, J.; Atkins, M.; et al. Prognostic Model for Survival in Patients with Metastatic Renal Cell Carcinoma: Results from the International Kidney Cancer Working Group. Clin. Cancer Res. 2011, 17, 5443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Négrier, S.; Escudier, B.; Gomez, F.; Douillard, J.Y.; Ravaud, A.; Chevreau, C.; Buclon, M.; Pérol, D.; Lasset, C. Prognostic factors of survival and rapid progression in782 patients with metastatic renal carcinomas treated by cytokines: A report from the Groupe Français d’Immunothérapie. Ann. Oncol. 2002, 13, 1460–1468. [Google Scholar] [CrossRef]
- Rini, B.I.; Dorff, T.B.; Elson, P.; Rodriguez, C.S.; Shepard, D.; Wood, L.; Humbert, J.; Pyle, L.; Wong, Y.-N.; Finke, J.H.; et al. Active surveillance in metastatic renal-cell carcinoma: A prospective, phase 2 trial. Lancet Oncol. 2016, 17, 1317–1324. [Google Scholar] [CrossRef]
- Dall’Olio, F.G.; Marabelle, A.; Caramella, C.; Garcia, C.; Aldea, M.; Chaput, N.; Robert, C.; Besse, B. Tumour burden and efficacy of immune-checkpoint inhibitors. Nat. Rev. Clin. Oncol. 2022, 19, 75–90. [Google Scholar] [CrossRef]
- Kim, S.I.; Cassella, C.R.; Byrne, K.T. Tumor Burden and Immunotherapy: Impact on Immune Infiltration and Therapeutic Outcomes. Front. Immunol. 2021, 11, 3762. [Google Scholar] [CrossRef]
- Bilen, M.A.; Shabto, J.M.; Martini, D.J.; Liu, Y.; Lewis, C.; Collins, H.; Akce, M.; Kissick, H.; Carthon, B.C.; Shaib, W.L.; et al. Sites of metastasis and association with clinical outcome in advanced stage cancer patients treated with immunotherapy. BMC Cancer 2019, 19, 857. [Google Scholar] [CrossRef]
- Paderi, A.; Gambale, E.; Botteri, C.; Giorgione, R.; Lavacchi, D.; Brugia, M.; Mazzoni, F.; Giommoni, E.; Bormioli, S.; Amedei, A.; et al. Association of Systemic Steroid Treatment and Outcome in Patients Treated with Immune Checkpoint Inhibitors: A Real-World Analysis. Molecules 2021, 26, 5789. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | Overall | Immune-Related Thyroiditis | No Immune-Related Thyroiditis | p |
|---|---|---|---|---|
| N (%) | 123 (100) | 47 (38) | 76 (62) | |
| Gender, male (%) | 87 (70.7) | 31 (66) | 56 (73.7) | 0.477 |
| Age at diagnosis (median (IQR)) | 62 (53, 69) | 65 (58, 69) | 61 (51, 69) | 0.110 |
| Background autoimmunity (%) | 8 (6.5) | 2 (4.3) | 6 (7.9) | 0.675 |
| Background thyroid dysfunction (%) | 11 (8.9) | 6 (12.8) | 5 (6.6) | 0.399 |
| RCC subtype (%) | 0.726 | |||
| Clear Cell | 103 (86.6) | 41 (87.2) | 62 (86.1) | |
| Other | 20 (13.3) | 6 (12.8) | 14 (13.9) | |
| Number of metastatic sites (median (IQR)) | 2 (1, 3) | 2 (1, 3) | 2 (1, 3) | 0.814 |
| Heng risk group (%) | 0.645 | |||
| Favorable | 24 (19.7) | 10 (21.3) | 14 (18.7) | |
| Intermediate | 81 (66.4) | 29 (61.7) | 52 (69.3) | |
| Poor | 17 (13.9) | 8 (17.0) | 9 (12.0) | |
| Received prior VEGFi (%) | 64 (52) | 25 (53.2) | 39 (51.3) | 0.987 |
| Thyroid dysfunction after VEGFi treatment (%) | 29 (23.8) | 15 (32.6) | 14 (18.4) | 0.118 |
| CPI type (%) | 0.047 | |||
| Ipilimumab–Nivolumab | 60 (48.8) | 22 (46.8) | 38 (50.0) | |
| Nivolumab | 35 (28.5) | 12 (25.5) | 23 (30.3) | |
| Pembrolizumab-Axitinib | 17 (13.8) | 7 (14.9) | 10 (13.2) | |
| Avelumab-Axitinib | 6 (4.9) | 1 (2.1) | 5 (6.6) | |
| Other | 5 (4.1) | 5 (10.6) | 0 (0.0) |
| Variables | All Patients, n (%) | Univariable HR (CI, p Value) | High Risk Patients, n (%) | Univariable HR (CI, p Value) |
|---|---|---|---|---|
| N | 123 | 42 | ||
| Immune-related adverse events other than irT, any | 57 (47.1) | 0.34 (0.20–0.59, p < 0.001) | 15 (36.6) | 0.47 (0.19–1.15, p = 0.098) |
| Treated by high dose steroids | 37 (30.1) | 0.48 (0.26–0.89, p = 0.020) | 9 (21.4) | 0.74 (0.25–2.18, p = 0.589) |
| Immune-related thyroiditis | 47 (38.2) | 0.85 (0.50–1.45, p = 0.550) | 17 (40.5) | 0.28 (0.10–0.76, p = 0.012) |
| Encephalitis | 2 (1.6) | NA | 2 (4.8) | NA |
| Pruritus | 9 (7.3) | 0.42 (0.13–1.36, p = 0.149) | 2 (4.8) | NA |
| Rash | 9 (7.3) | 0.28 (0.07–1.14, p = 0.076) | 1 (2.4) | NA |
| Neuropathy | 3 (2.4) | NA | 1 (2.4) | NA |
| Nephritis | 6 (4.9) | 0.44 (0.11–1.80, p = 0.253) | 1 (2.4) | NA |
| Arthritis or myositis | 4 (3.3) | NA | 1 (2.4) | NA |
| Hepatitis | 15 (12.2) | 0.62 (0.25–1.55, p = 0.304) | 5 (11.9) | 0.55 (0.13–2.34, p = 0.417) |
| Pneumonitis | 7 (5.7) | 0.47 (0.11–1.91, p = 0.289) | 1 (2.4) | NA |
| Diarrhea or colitis or gastritis | 15 (12.2) | 0.46 (0.18–1.15, p = 0.096) | 2 (4.8) | NA |
| Hypoadrenalism | 3 (2.4) | NA | 3 (7.1) | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sagie, S.; Gadot, M.; Levartovsky, M.; Gantz Sorotsky, H.; Berger, R.; Sarfaty, M.; Percik, R. Immune-Related Thyroiditis as a Predictor for Survival in Metastatic Renal Cell Carcinoma. Cancers 2022, 14, 875. https://doi.org/10.3390/cancers14040875
Sagie S, Gadot M, Levartovsky M, Gantz Sorotsky H, Berger R, Sarfaty M, Percik R. Immune-Related Thyroiditis as a Predictor for Survival in Metastatic Renal Cell Carcinoma. Cancers. 2022; 14(4):875. https://doi.org/10.3390/cancers14040875
Chicago/Turabian StyleSagie, Shira, Moran Gadot, Meital Levartovsky, Hadas Gantz Sorotsky, Raanan Berger, Michal Sarfaty, and Ruth Percik. 2022. "Immune-Related Thyroiditis as a Predictor for Survival in Metastatic Renal Cell Carcinoma" Cancers 14, no. 4: 875. https://doi.org/10.3390/cancers14040875