
A Novel Blood-Based microRNA Diagnostic Model with High Accuracy for Multi-Cancer Early Detection


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
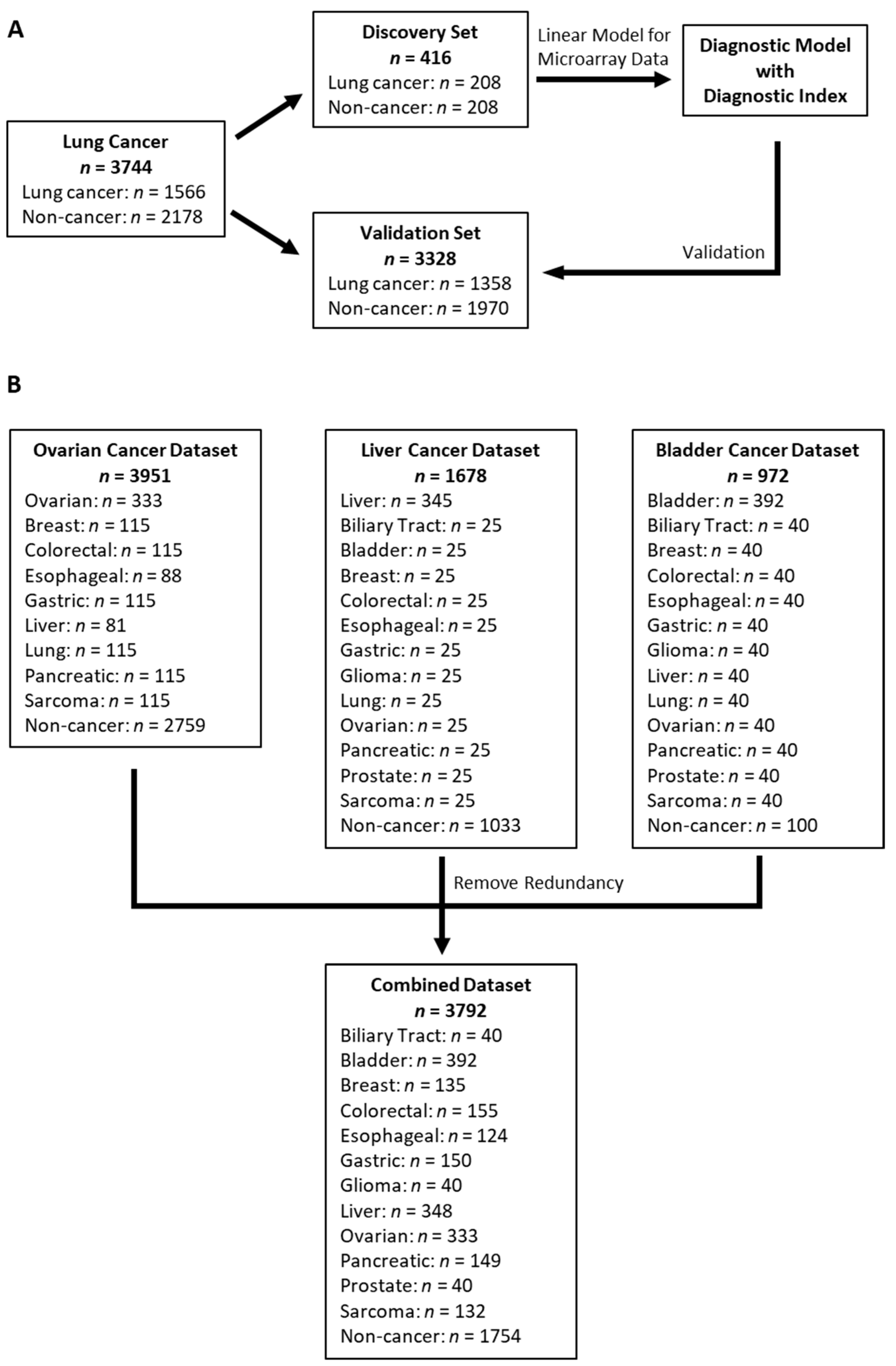
2.1. Study Design
2.2. Participants and Serum Samples
2.3. miRNA Microarray Expression Analysis
2.4. Diagnostic Model Development
2.5. Statistical Analysis
3. Results
3.1. Participants and Datasets
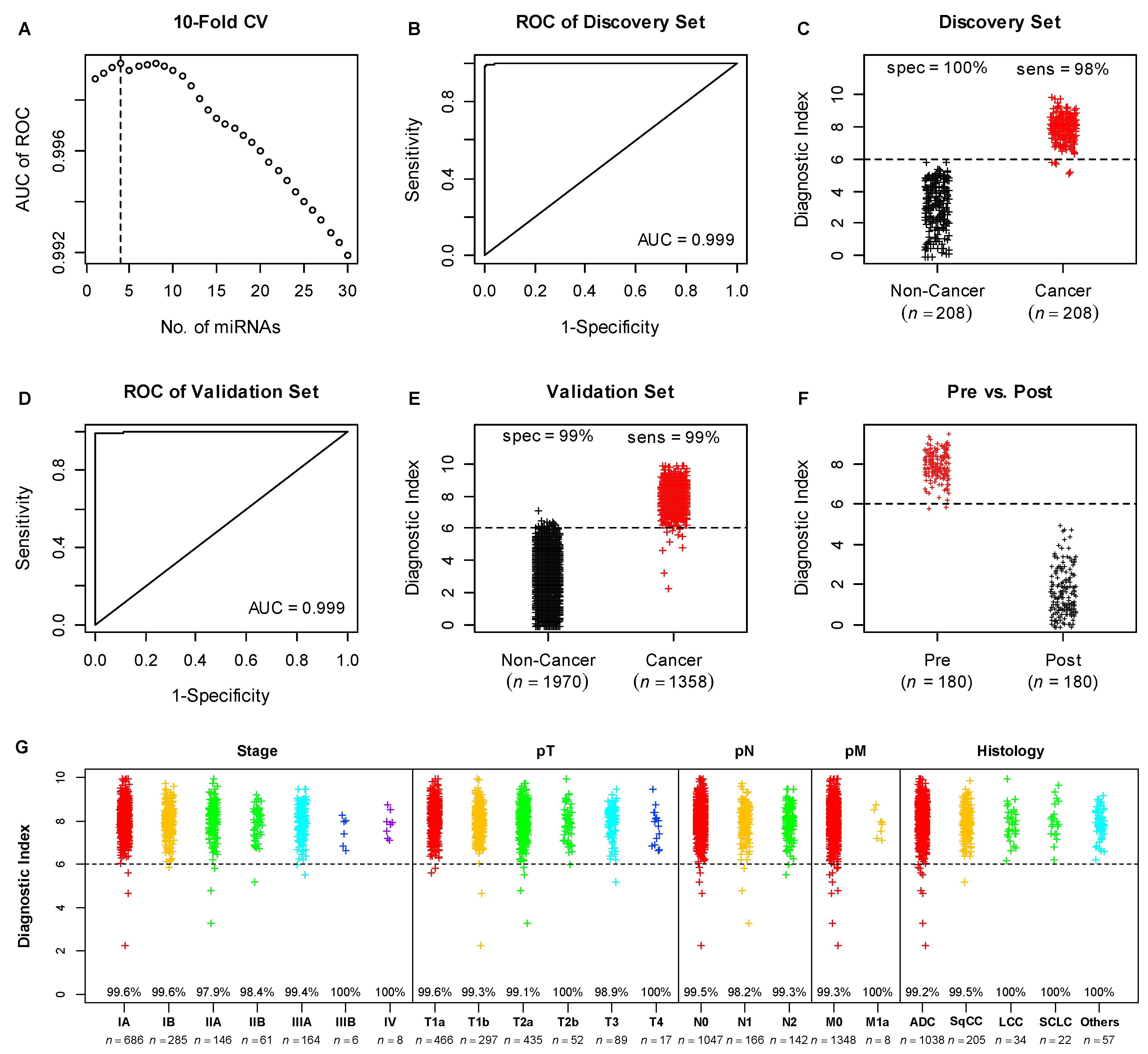
3.2. Development of Diagnostic Model
3.3. Validation of the Diagnostic Model in the Lung Cancer Validation Set
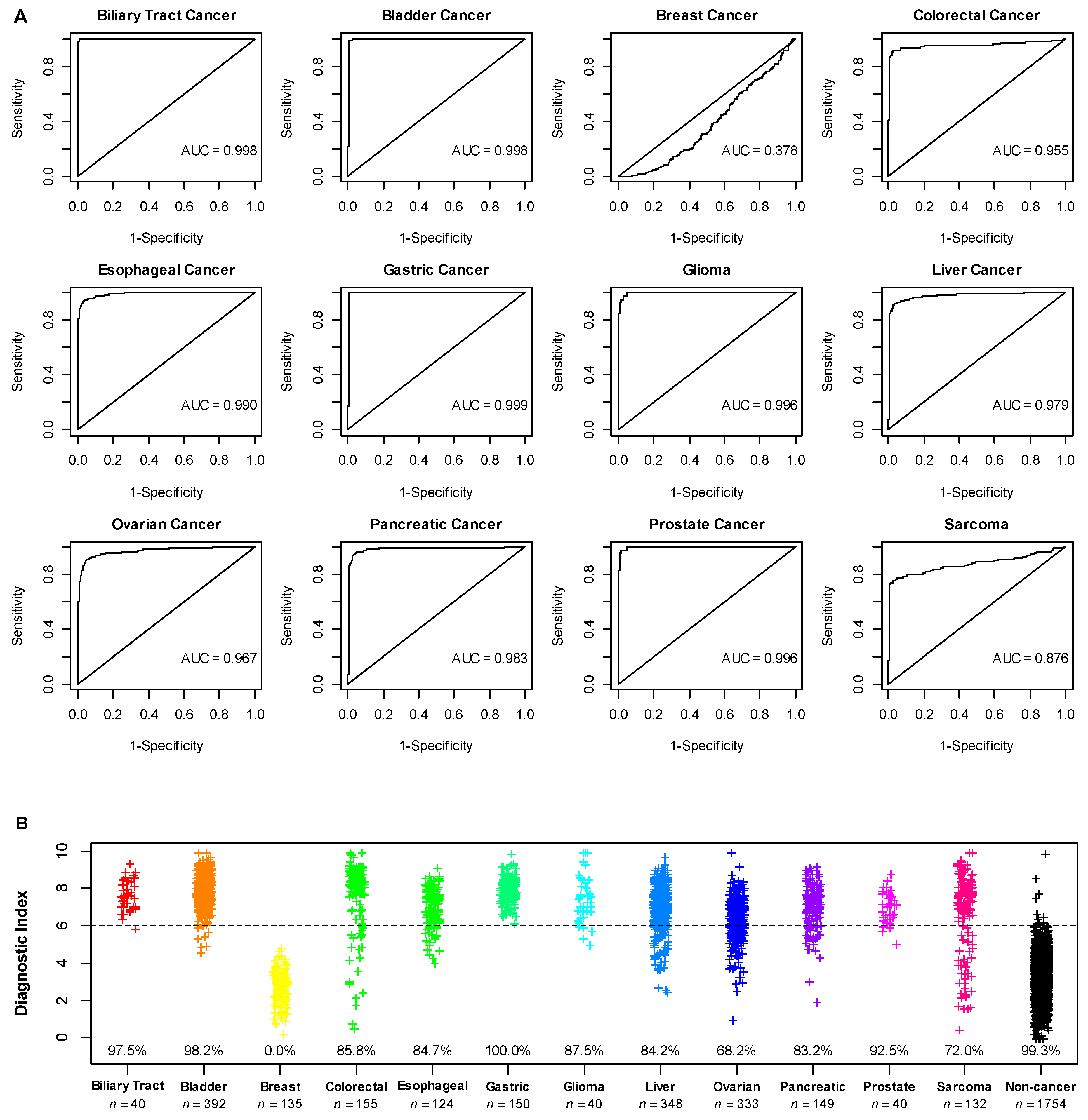
3.4. Application of the Diagnostic Model in Additional Cancer Types
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Ahlquist, D.A. Universal Cancer Screening: Revolutionary, Rational, and Realizable. NPJ Precis. Oncol. 2018, 2, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Noone, A.M.; Howlader, N.; Krapcho, M.; Miller, D.; Brest, A.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; Lewis, D.R.; et al. SEER Cancer Statistics Review, 1975–2015; National Cancer Institute: Rockville, MD, USA, 2018. [Google Scholar]
- Siu, A.L. U.S. Preventive Services Task Force Screening for Breast Cancer: U.S. Preventive Services Task Force Recommendation Statement. Ann. Intern. Med. 2016, 164, 279–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- US Preventive Services Task Force; Curry, S.J.; Krist, A.H.; Owens, D.K.; Barry, M.J.; Caughey, A.B.; Davidson, K.W.; Doubeni, C.A.; Epling, J.W.; Kemper, A.R.; et al. Screening for Cervical Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2018, 320, 674–686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- US Preventive Services Task Force; Davidson, K.W.; Barry, M.J.; Mangione, C.M.; Cabana, M.; Caughey, A.B.; Davis, E.M.; Donahue, K.E.; Doubeni, C.A.; Krist, A.H.; et al. Screening for Colorectal Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2021, 325, 2564–2575. [Google Scholar] [CrossRef]
- US Preventive Services Task Force; Krist, A.H.; Davidson, K.W.; Mangione, C.M.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Davis, E.M.; Donahue, K.E.; Doubeni, C.A.; et al. Screening for Lung Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2021, 325, 330–338. [Google Scholar] [CrossRef]
- Jemal, A.; Fedewa, S.A. Lung Cancer Screening With Low-Dose Computed Tomography in the United States-2010 to 2015. JAMA Oncol. 2017, 3, 1278–1281. [Google Scholar] [CrossRef]
- Liang, P.S.; Wheat, C.L.; Abhat, A.; Brenner, A.T.; Fagerlin, A.; Hayward, R.A.; Thomas, J.P.; Vijan, S.; Inadomi, J.M. Adherence to Competing Strategies for Colorectal Cancer Screening Over 3 Years. Am. J. Gastroenterol. 2016, 111, 105–114. [Google Scholar] [CrossRef] [Green Version]
- US Preventive Services Task Force; Grossman, D.C.; Curry, S.J.; Owens, D.K.; Bibbins-Domingo, K.; Caughey, A.B.; Davidson, K.W.; Doubeni, C.A.; Ebell, M.; Epling, J.W.; et al. Screening for Prostate Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2018, 319, 1901–1913. [Google Scholar] [CrossRef]
- Croswell, J.M.; Kramer, B.S.; Kreimer, A.R.; Prorok, P.C.; Xu, J.-L.; Baker, S.G.; Fagerstrom, R.; Riley, T.L.; Clapp, J.D.; Berg, C.D.; et al. Cumulative Incidence of False-Positive Results in Repeated, Multimodal Cancer Screening. Ann. Fam. Med. 2009, 7, 212–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, J.; Hayder, H.; Zayed, Y.; Peng, C. Overview of MicroRNA Biogenesis, Mechanisms of Actions, and Circulation. Front. Endocrinol. 2018, 9, 402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarzenbach, H.; Nishida, N.; Calin, G.A.; Pantel, K. Clinical Relevance of Circulating Cell-Free MicroRNAs in Cancer. Nature reviews. Clin. Oncol. 2014, 11, 145–156. [Google Scholar] [CrossRef]
- Hannafon, B.N.; Ding, W.-Q. Intercellular Communication by Exosome-Derived MicroRNAs in Cancer. Int. J. Mol. Sci. 2013, 14, 14240–14269. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, P.S.; Parkin, R.K.; Kroh, E.M.; Fritz, B.R.; Wyman, S.K.; Pogosova-Agadjanyan, E.L.; Peterson, A.; Noteboom, J.; O’Briant, K.C.; Allen, A.; et al. Circulating MicroRNAs as Stable Blood-Based Markers for Cancer Detection. Proc. Natl. Acad. Sci. USA 2008, 105, 10513–10518. [Google Scholar] [CrossRef] [Green Version]
- Asakura, K.; Kadota, T.; Matsuzaki, J.; Yoshida, Y.; Yamamoto, Y.; Nakagawa, K.; Takizawa, S.; Aoki, Y.; Nakamura, E.; Miura, J.; et al. A MiRNA-Based Diagnostic Model Predicts Resectable Lung Cancer in Humans with High Accuracy. Commun. Biol. 2020, 3, 134. [Google Scholar] [CrossRef] [Green Version]
- Yokoi, A.; Matsuzaki, J.; Yamamoto, Y.; Yoneoka, Y.; Takahashi, K.; Shimizu, H.; Uehara, T.; Ishikawa, M.; Ikeda, S.-I.; Sonoda, T.; et al. Integrated Extracellular MicroRNA Profiling for Ovarian Cancer Screening. Nat. Commun. 2018, 9, 4319. [Google Scholar] [CrossRef]
- Usuba, W.; Urabe, F.; Yamamoto, Y.; Matsuzaki, J.; Sasaki, H.; Ichikawa, M.; Takizawa, S.; Aoki, Y.; Niida, S.; Kato, K.; et al. Circulating MiRNA Panels for Specific and Early Detection in Bladder Cancer. Cancer Sci. 2019, 110, 408–419. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Kondo, S.; Matsuzaki, J.; Esaki, M.; Okusaka, T.; Shimada, K.; Murakami, Y.; Enomoto, M.; Tamori, A.; Kato, K.; et al. Highly Sensitive Circulating MicroRNA Panel for Accurate Detection of Hepatocellular Carcinoma in Patients with Liver Disease. Hepatol. Commun. 2020, 4, 284–297. [Google Scholar] [CrossRef]
- Ritchie, M.E.; Phipson, B.; Wu, D.; Hu, Y.; Law, C.W.; Shi, W.; Smyth, G.K. Limma Powers Differential Expression Analyses for RNA-Sequencing and Microarray Studies. Nucleic Acids Res. 2015, 43, e47. [Google Scholar] [CrossRef]
- Huang, H.; Jiang, Y.; Wang, Y.; Chen, T.; Yang, L.; He, H.; Lin, Z.; Liu, T.; Yang, T.; Kamp, D.W.; et al. MiR-5100 Promotes Tumor Growth in Lung Cancer by Targeting Rab6. Cancer Lett. 2015, 362, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Liu, X.; Tian, Q.; Liang, T.; Chang, P. Increasing Expression of MiR-5100 in Non-Small-Cell Lung Cancer and Correlation with Prognosis. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 3592–3597. [Google Scholar] [PubMed]
- Zhang, H.-M.; Li, H.; Wang, G.-X.; Wang, J.; Xiang, Y.; Huang, Y.; Shen, C.; Dai, Z.-T.; Li, J.-P.; Zhang, T.-C.; et al. MKL1/MiR-5100/CAAP1 Loop Regulates Autophagy and Apoptosis in Gastric Cancer Cells. Neoplasia 2020, 22, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Chijiiwa, Y.; Moriyama, T.; Ohuchida, K.; Nabae, T.; Ohtsuka, T.; Miyasaka, Y.; Fujita, H.; Maeyama, R.; Manabe, T.; Abe, A.; et al. Overexpression of MicroRNA-5100 Decreases the Aggressive Phenotype of Pancreatic Cancer Cells by Targeting PODXL. Int. J. Oncol. 2016, 48, 1688–1700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, Z.; Lyu, B.; Hou, D.; Liu, X. Mir-5100 Mediates Proliferation, Migration and Invasion of Oral Squamous Cell Carcinoma Cells Via Targeting SCAI. J. Investig. Surg. Off. J. Acad. Surg. Res. 2021, 34, 834–841. [Google Scholar] [CrossRef] [PubMed]
- Ma, Q.; Wang, Y.; Zhang, H.; Wang, F. MiR-1290 Contributes to Colorectal Cancer Cell Proliferation by Targeting INPP4B. Oncol. Res. 2018, 26, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.; An, H.-J.; Lee, M.-J.; Song, J.-Y.; Jeong, J.-Y.; Lee, J.-H.; Jeong, H.-C. Hsa-MiR-1246 and Hsa-MiR-1290 Are Associated with Stemness and Invasiveness of Non-Small Cell Lung Cancer. Lung Cancer 2016, 91, 15–22. [Google Scholar] [CrossRef]
- Yan, L.; Cai, K.; Sun, K.; Gui, J.; Liang, J. MiR-1290 Promotes Proliferation, Migration, and Invasion of Glioma Cells by Targeting LHX6. J. Cell. Physiol. 2018, 233, 6621–6629. [Google Scholar] [CrossRef]
- Qin, W.-J.; Wang, W.-P.; Wang, X.-B.; Zhang, X.-T.; Du, J.-D. MiR-1290 Targets CCNG2 to Promote the Metastasis of Oral Squamous Cell Carcinoma. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 10332–10342. [Google Scholar] [CrossRef]
- Klein, E.A.; Richards, D.; Cohn, A.; Tummala, M.; Lapham, R.; Cosgrove, D.; Chung, G.; Clement, J.; Gao, J.; Hunkapiller, N.; et al. Clinical Validation of a Targeted Methylation-Based Multi-Cancer Early Detection Test Using an Independent Validation Set. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2021, 32, 1167–1177. [Google Scholar] [CrossRef]
- Cohen, J.D.; Li, L.; Wang, Y.; Thoburn, C.; Afsari, B.; Danilova, L.; Douville, C.; Javed, A.A.; Wong, F.; Mattox, A.; et al. Detection and Localization of Surgically Resectable Cancers with a Multi-Analyte Blood Test. Science 2018, 359, 926–930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, X.; Gole, J.; Gore, A.; He, Q.; Lu, M.; Min, J.; Yuan, Z.; Yang, X.; Jiang, Y.; Zhang, T.; et al. Non-Invasive Early Detection of Cancer Four Years before Conventional Diagnosis Using a Blood Test. Nat. Commun. 2020, 11, 3475. [Google Scholar] [CrossRef] [PubMed]
- Cristiano, S.; Leal, A.; Phallen, J.; Fiksel, J.; Adleff, V.; Bruhm, D.C.; Jensen, S.Ø.; Medina, J.E.; Hruban, C.; White, J.R.; et al. Genome-Wide Cell-Free DNA Fragmentation in Patients with Cancer. Nature 2019, 570, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Nelson, H.D.; Fu, R.; Cantor, A.; Pappas, M.; Daeges, M.; Humphrey, L. Effectiveness of Breast Cancer Screening: Systematic Review and Meta-Analysis to Update the 2009 U.S. Preventive Services Task Force Recommendation. Ann. Intern. Med. 2016, 164, 244–255. [Google Scholar] [CrossRef]
- Lennon, A.M.; Buchanan, A.H.; Kinde, I.; Warren, A.; Honushefsky, A.; Cohain, A.T.; Ledbetter, D.H.; Sanfilippo, F.; Sheridan, K.; Rosica, D.; et al. Feasibility of Blood Testing Combined with PET-CT to Screen for Cancer and Guide Intervention. Science 2020, 369, eabb9601. [Google Scholar] [CrossRef]
- Beer, T.; McDonnell, C.; Nadauld, L.; Liu, M.; Klein, E.; Reid, R.; Marinac, C.; Chung, K.; Lopatin, M.; Fung, E.; et al. Interim Results of PATHFINDER, a Clinical Use Study Using a Methylation-Based Multi-Cancer Early Detection Test. J. Clin. Oncol. 2021, 39, 3010. [Google Scholar] [CrossRef]
- Lehman, C.D.; Arao, R.F.; Sprague, B.L.; Lee, J.M.; Buist, D.S.M.; Kerlikowske, K.; Henderson, L.M.; Onega, T.; Tosteson, A.N.A.; Rauscher, G.H.; et al. National Performance Benchmarks for Modern Screening Digital Mammography: Update from the Breast Cancer Surveillance Consortium. Radiology 2017, 283, 49–58. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration Cologuard Summary of Safety and Effectiveness Data (Premarket Approval Application P130017). 2014.
- National Lung Screening Trial Research Team; Church, T.R.; Black, W.C.; Aberle, D.R.; Berg, C.D.; Clingan, K.L.; Duan, F.; Fagerstrom, R.M.; Gareen, I.F.; Gierada, D.S.; et al. Results of Initial Low-Dose Computed Tomographic Screening for Lung Cancer. N. Engl. J. Med. 2013, 368, 1980–1991. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Lung Cancer [17] * | Characteristics | Bladder Cancer [19] * | Characteristics | Ovarian Cancer [18] * | Characteristics | Liver Cancer [20] * | |
|---|---|---|---|---|---|---|---|
| n = 1566 | n = 392 | n = 333 | n = 348 | ||||
| Age (mean, SD) | 65 (10) | Age (mean, SD) | 68 (11) | Age (mean, SD) | 57 (12) | Age (mean, SD) | 68 (9) |
| Gender | Gender | Stage | Gender | ||||
| Male | 895 (57%) | Male | 283 (72%) | I | 82 (25%) | Male | 268 (78%) |
| Female | 671 (43%) | Female | 109 (28%) | II | 33 (10%) | Female | 77 (22%) |
| Smoking | Urinary cytology | III-IV | 218 (65%) | unknown | 3 | ||
| Former/current | 972 (62%) | Class I | 36 (10%) | Histology | Stage | ||
| Never | 594 (38%) | Class II | 115 (31%) | Serous | 182 (55%) | I | 123 (37%) |
| Histology | Class III | 73 (19%) | Clear cell | 64 (19%) | II | 108 (33%) | |
| Adenocarcinoma | 1217 (78%) | Class IV | 50 (13%) | Endometrioid | 43 (13%) | III | 80 (24%) |
| Squamous | 221 (14%) | Class V | 103 (27%) | Mucinous | 14 (4%) | IV | 19 (6%) |
| Adenosquamous | 18 (1%) | unknown | 15 | Other epithelial | 17 (5%) | unknown | 18 |
| Small cell | 23 (1%) | T stage | Non-epithelial | 13 (4%) | Child-Pugh | ||
| Other | 87 (6%) | <pT2 | 300 (77%) | A | 303 (88%) | ||
| Stage | ≥pT2 | 90 (23%) | Non-Cancer (n = 2759) | B | 40 (12%) | ||
| I | 1126 (72%) | unknown | 2 | Info Not Available | unknown | 5 | |
| II | 233 (15%) | Grade | Virus | ||||
| III-IV | 203 (13%) | Low | 77 (20%) | HBsAg+ | 57 (16%) | ||
| 0 | 4 (0%) | High | 315 (80%) | HCVAb+ | 141 (41%) | ||
| Nodal status | non-B non-C | 147 (43%) | |||||
| Non-Cancer (n = 2178) | N+ | 42 (12%) | unknown | 3 | |||
| Age (mean, SD) | 51 (11) | N0 | 320 (88%) | ||||
| Gender | unknown | 30 | Non-Cancer (n = 1033) | ||||
| Male | 1129 (52%) | M stage | Age (mean, SD) | 65 (10) | |||
| Female | 1049 (48%) | M1 | 17 (5%) | Gender | |||
| Smoking | M0 | 347 (95%) | Male | 239 (23%) | |||
| Former/current | 482 (22%) | Unknown | 28 | Female | 794 (77%) | ||
| Never | 1696 (78%) | ||||||
| Non-Cancer (n = 100) | |||||||
| Age (mean, SD) | 64 (16) | ||||||
| Gender | |||||||
| Male | 48 (48%) | ||||||
| Female | 52 (52%) | ||||||
| Clinical Subsets | n | Original 2-miRNA Model | New 4-miRNA Model | p-Value * | |
|---|---|---|---|---|---|
| Clinical Stage | IA | 686 | 96.1% | 99.6% | <0.001 |
| IB | 285 | 93.7% | 99.6% | <0.001 | |
| IIA | 146 | 97.3% | 97.9% | 0.99 | |
| IIB | 61 | 96.7% | 98.4% | 0.99 | |
| IIIA | 164 | 90.2% | 99.4% | <0.001 | |
| IIIB | 6 | 83.3% | 100.0% | 0.99 | |
| IV | 8 | 100.0% | 100.0% | 1.00 | |
| T Stage | T1a | 466 | 96.1% | 99.6% | <0.001 |
| T1b | 297 | 95.6% | 99.3% | 0.003 | |
| T2a | 435 | 93.6% | 99.1% | <0.001 | |
| T2b | 52 | 92.3% | 100.0% | 0.134 | |
| T3 | 89 | 94.4% | 98.9% | 0.221 | |
| T4 | 17 | 94.1% | 100.0% | 0.99 | |
| N Stage | N0 | 1047 | 95.5% | 99.5% | <0.001 |
| N1 | 166 | 95.8% | 98.2% | 0.289 | |
| N2 | 142 | 90.1% | 99.3% | <0.001 | |
| M Stage | M0 | 1348 | 94.7% | 99.3% | <0.001 |
| M1a | 8 | 100.0% | 100.0% | 1.00 | |
| Histology | ADC | 1038 | 95.1% | 99.2% | <0.001 |
| SqCC | 205 | 94.2% | 99.5% | 0.006 | |
| LCC | 34 | 97.1% | 100.0% | 0.99 | |
| SCLC | 22 | 90.9% | 100.0% | 0.480 | |
| Others | 57 | 96.5% | 100.0% | 0.480 | |
| Default Cut-Point Based on 99% Specificity | Alternative Cut-Point Based on 95% Specificity | |
|---|---|---|
| Biliary Tract Cancer | 97.5% | 100.0% |
| Bladder Cancer | 98.2% | 99.2% |
| Colorectal Cancer | 85.8% | 91.6% |
| Esophageal Cancer | 84.7% | 95.2% |
| Gastric Cancer | 100.0% | 100.0% |
| Glioma | 87.5% | 97.5% |
| Liver Cancer | 84.2% | 92.5% |
| Ovarian Cancer | 68.2% | 90.1% |
| Pancreatic Cancer | 83.2% | 95.3% |
| Prostate Cancer | 92.5% | 97.5% |
| Sarcoma | 72.0% | 76.5% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, A.; Hu, H. A Novel Blood-Based microRNA Diagnostic Model with High Accuracy for Multi-Cancer Early Detection. Cancers 2022, 14, 1450. https://doi.org/10.3390/cancers14061450
Zhang A, Hu H. A Novel Blood-Based microRNA Diagnostic Model with High Accuracy for Multi-Cancer Early Detection. Cancers. 2022; 14(6):1450. https://doi.org/10.3390/cancers14061450
Chicago/Turabian StyleZhang, Andrew, and Hai Hu. 2022. "A Novel Blood-Based microRNA Diagnostic Model with High Accuracy for Multi-Cancer Early Detection" Cancers 14, no. 6: 1450. https://doi.org/10.3390/cancers14061450
APA StyleZhang, A., & Hu, H. (2022). A Novel Blood-Based microRNA Diagnostic Model with High Accuracy for Multi-Cancer Early Detection. Cancers, 14(6), 1450. https://doi.org/10.3390/cancers14061450