1. Introduction
Distant metastasis is the primary cause (~90%) of death from breast cancer [
1]. However, current gene expression-based biomarkers for disease outcome (e.g., PAM50, Oncotype DX, MammaPrint) [
2,
3] are largely driven by proliferation and estrogen-regulation genes, and do not provide conclusive information about the risk of systemic dissemination with consequent distant metastasis [
3,
4,
5].
Previously, we reported the discovery of the “Tumor Microenvironment of Metastasis” (TMEM) doorway, a portal into the blood vasculature composed of a tumor cell overexpressing the actin regulatory protein Mena, a perivascular macrophage, and an endothelial cell, all in direct contact (
Figure S1A–D left,E). TMEM doorways function as vascular openings through which tumor cells intravasate and disseminate hematogenously [
6,
7]. We previously showed that a triple immunohistochemical stain for the three constituent cell types that make up TMEM doorways can be used as a biomarker (called TMEM Score) for prognosticating the development of distant metastasis [
8]. We further showed that TMEM Score prognosticates the risk of distant metastasis in HR+/HER2− breast cancer patients better than the IHC4 immunohistochemical assay score [
9] and independently of classical clinicopathologic features [
4]. Finally, we analytically validated a quantification of the TMEM Score using an automated, high-throughput assay implemented within a Clinical Laboratory Improvement Amendments (CLIA) certified clinical diagnostic laboratory and showed that TMEM Score is significantly associated with early distant recurrence (within 5-years of diagnosis) [
10].
While these studies clinically validated the use of TMEM Score for prognosticating metastatic outcome in HR+/HER2− patients (the largest subgroup of breast cancer patients), a statistically significant association between TMEM Score and distant recurrence outcome was not observed in the triple-negative or HER2+ breast cancer subpopulations, perhaps due to the smaller number of these subjects available for analysis. While there is currently no evidence of a connection between the HER2 receptor status and TMEM doorways or MenaCalc, we cannot rule out its existence.
To identify those cancer cells within the tumor that are capable of intravasation, we developed the in vivo invasion assay, a technique capable of isolating the motile fraction of cancer cells from the rest of the immobile bulk of the primary tumor [
11,
12,
13]. Using this assay in mouse models of breast cancer, we were able to determine that a subset of tumor cells and macrophages communicate with each other via a paracrine loop that enables them to co-migrate together along collagen fibers at 10–100 times the speed of the rest of the tumor cells within the bulk tumor. This type of coordinated cellular motion is known as “fast streaming migration” [
13]. We further determined that endothelial-cell-secreted Hepatocyte Growth Factor (HGF) gradients provide a directional chemoattractant signal which attracts fast-migrating cells that are less than 500 µm away from blood vessels [
14] (
Figure 1A). Expression profiling of these cells showed that Mena, a key actin polymerization regulatory protein, plays an important role in potentiating tumor cell motility as well as tumor cell intravasation near TMEM doorways [
15,
16,
17].
Mena consists of several splice-variant isoforms which confer distinct phenotypes to tumor cells [
18]. Of these isoforms, Mena11a, an anti-metastatic isoform that is strongly associated with an epithelial phenotype, is down-regulated during epithelial-to-mesenchymal transition (EMT) and in invasive tumor cells [
18]. Several other isoforms, including Mena
INV, have been shown to confer a pro-metastatic motile phenotype and are found to be expressed exclusively in invasive and disseminating tumor cells [
19]. We have found that tumor cells that have high levels of overall Mena expression, and also contain a Mena
INV-Hi and Mena11a
Low isoform expression pattern, are involved in invasion, fast streaming migration, and intravasation [
14,
16,
20]. Based upon these observations, we developed a quantitative immunofluorescence (IF)-based biomarker designed to quantify the relative amounts of pro-metastatic and anti-metastatic Mena isoforms. This metric, termed Mena
Calc, is computed by quantifying the abundance of the Mena11a isoform (
Figure S1A–D right) and subtracting the normalized value of this isoform from the normalized amount of PanMena (
Figure S1A–D middle), i.e., all Mena isoforms present.
In initial retrospective studies, Mena
Calc was shown to be prognostic of distant metastasis in the ER- and in the node-positive subsets of a cohort of patients [
21]. A second study in a different cohort [
22] showed that Mena
Calc is prognostic in a node-negative subset of patients.
Given the difference in performance of TMEM doorway and Mena
Calc scores in patients with diverse breast cancer subtypes, we asked how we might be able to improve the prognostic ability of these tests. We reasoned that no intravasation would be possible within the tumors of patients that contain TMEM doorways, but which lack Mena
Calc-Hi tumor cells capable of intravasating through the TMEM doorways (
Figure 1B). Similarly, no intravasation would be possible within tumors that contain fast streaming and highly invasive Mena
Calc-Hi tumor cells, but which lack TMEM doorways (
Figure 1C). Successful intravasation of tumor cells would require both motile Mena
Calc-Hi tumor cells and TMEM doorways (
Figure 1D). Thus, it is logical to suggest that patients with both high TMEM Score and high Mena
Calc Score would have higher risk of distant metastasis and a worse prognosis.
However, it is unclear from MenaCalc alone which subgroup would most benefit from a combined TMEM-MenaCalc biomarker. Since ER+/HER2− is the most common subtype of breast cancer with the longest time to recurrence, it is a high priority to determine if we can improve prognostication in this subtype.
Thus, our primary goal in this proof-of-principle initial study was to determine if a combined TMEM-Mena
Calc biomarker is able to improve upon the prognostication ability of either marker alone, all within a small cohort of patients with HR+/HER2− breast cancer (see
Section 4 Materials and Methods for cohort description). Since HR+/HER2− is the most common subtype of breast cancer and has the longest time to recurrence, there is an urgent need to find better prognosticators of metastatic outcome for this subtype. Furthermore, multivariate analysis (including tumor size, grade, and nodal status) showed that TMEM doorway density is prognostic for distant recurrence in patients with ER+ breast cancer [
10], independent of these clinical factors. Thus, it is of particular interest to determine if combining TMEM Score with Mena
Calc can improve TMEM Score performance in mixed-patient populations of the type studied previously. To accomplish this, we have evaluated several different ways of combining TMEM and Mena
Calc scores to create a multi-parameter quantitative analysis with much improved prognostic value for distant metastasis in breast cancer patients.
3. Discussion
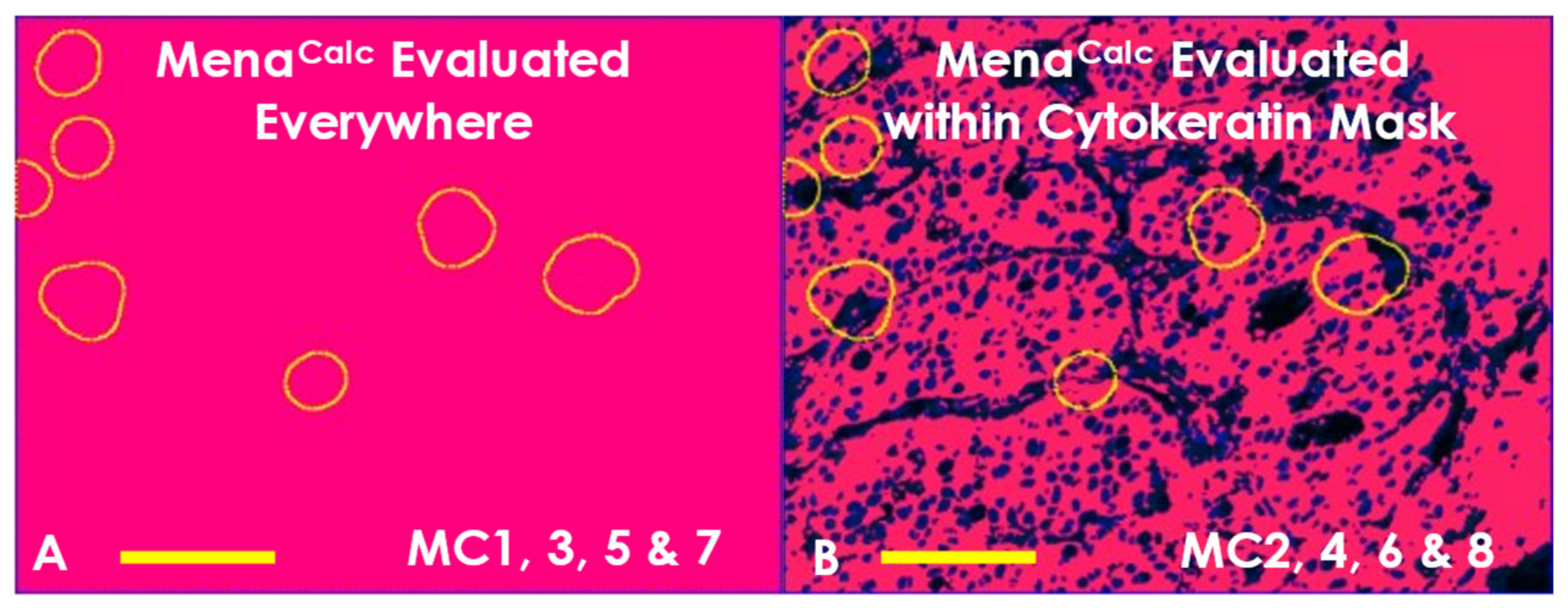
Our study of the different methods of combining TMEM doorway and Mena
Calc analyses showed a noticeable improvement in prognostic performance when measuring TMEM doorways and Mena
Calc over the entire range of the tumor tissue and utilizing a cytokeratin mask to limit the Mena
Calc evaluation to tumor cell cytoplasm only. This result can be understood by considering the interaction between tumor cell intravasation sites (TMEM doorways) and highly motile (Mena
Calc-Hi) tumor cells (
Figure 1D).
Using high-resolution intravital imaging, we have previously shown that, during intravasation, tumor cells respond to chemotactic signals, migrate towards blood vessels, and enter the blood stream through TMEM doorways [
6,
7,
14]. Tumor cells within a 500 µm radius of blood vessels are attracted towards the blood vessels by hepatocyte growth factor (HGF) gradients [
14]. In tumor cells lying between 500 µm and 1000 µm from blood vessels, migration is not directed towards the blood vessels but is toward macrophages which draws the tumor cell macrophage pairs into the HGF gradient. The tumor-cell–macrophage paired chemotaxis is driven by a paracrine loop between tumor-cell-secreted colony-stimulating factor 1 (CSF-1) and macrophage-secreted epidermal growth factor (EGF) [
13]. Both chemotaxis-mediated tumor cell movements are greatly amplified in tumor cells with high Mena
Calc levels [
14,
16,
17,
18]. Thus, there may be a high probability of tumor cell intravasation when Mena
Calc-Hi cells are close (within an area ~1 mm in radius) to blood vessels that contain TMEM doorways (
Figure 1A). By centering this area upon each TMEM doorway, we can define a “TMEM interaction zone” wherein Mena
Calc-Hi tumor cells are likely to intravasate.
In patients with a high TMEM Score, the density of TMEM doorways is high enough that the interaction zone for one TMEM doorway may overlap with that of adjacent TMEM doorways and thus the total interaction zone may cover the tumor volume nearly completely. Therefore, the improved performance when the Combined Marker is evaluated over the entire range of the tumor tissue (vs. just 10 fields of view) is to be expected as a result of increased sampling of the tissue which has the net effect of “averaging out” tissue heterogeneity.
Furthermore, the improved performance of the Combined Marker when utilizing the cytokeratin mask is to be expected as well, for two reasons. The first is that a cytokeratin mask limits the signal to only the tumor cells and excludes non-specific binding of antibody to stromal cells. Secondly, since Mena is a cytoplasmic and membrane-bound protein, exclusion of nuclei narrows the area for analysis to only the one where Mena is expected to be found. Both of these effects improve the specificity of detection and better separate signal from noise.


 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}






