
Outcomes of Cancer Patients with COVID-19 in a Hospital System in the Chicago Metropolitan Area

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Clinical Outcomes
3.2.1. Clotting Complications
3.2.2. Clinical Predictors of Mortality
3.2.3. Clinical Predictors of Critical Illness
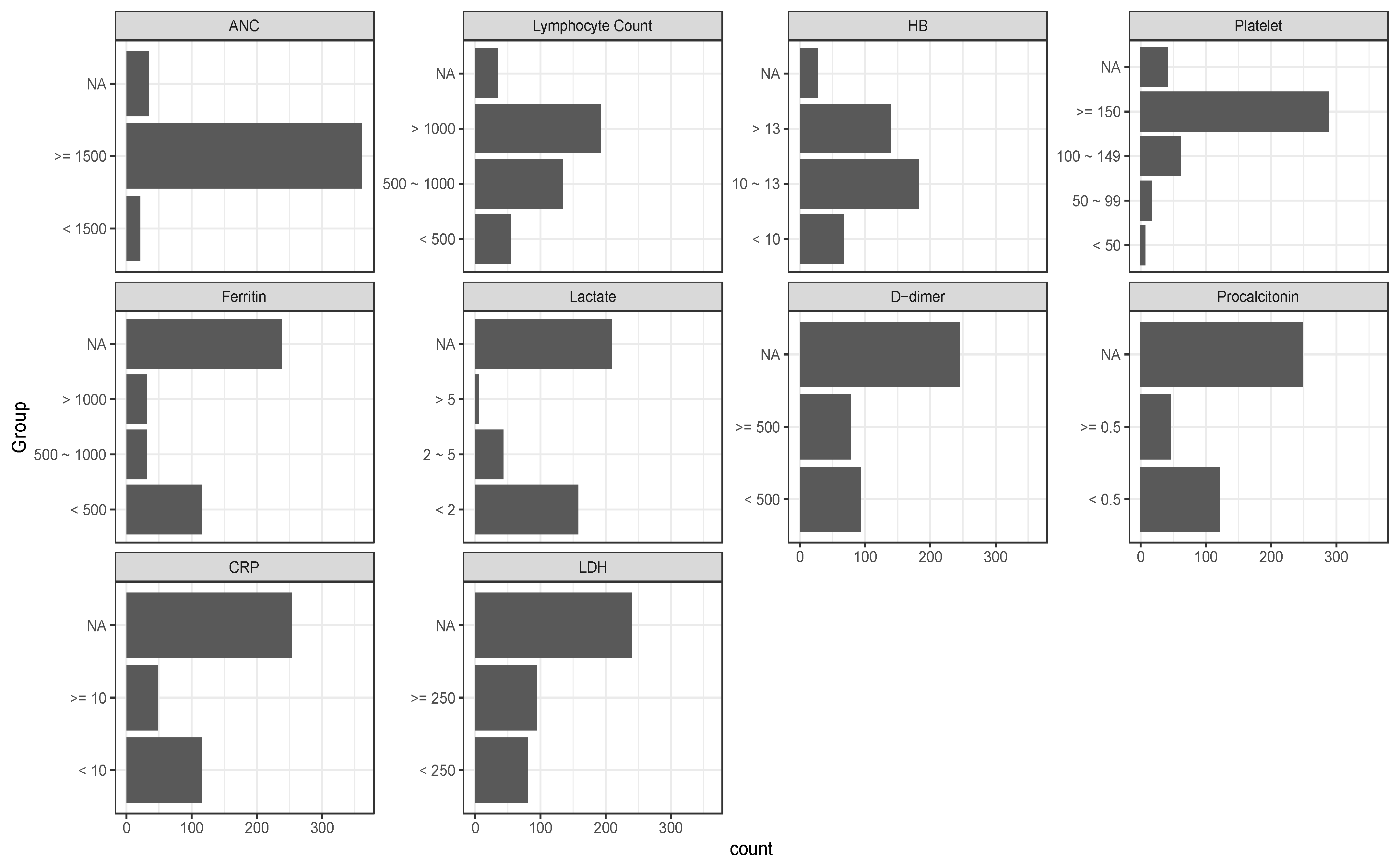
3.2.4. Laboratory Predictors of Mortality and Disease Severity
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coronavirus Disease (COVID-19)—World Health Organization, (n.d.). Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 1 November 2021).
- Su, C.; Xu, Z.; Hoffman, K.; Goyal, P.; Safford, M.M.; Lee, J.; Alvarez-Mulett, S.; Gomez-Escobar, L.; Price, D.R.; Harrington, J.S.; et al. Identifying organ dysfunction trajectory-based subphenotypes in critically ill patients with COVID-19. Sci. Rep. 2021, 11, 15872. [Google Scholar] [CrossRef]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.-S.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.; Liang, W.; Zhao, Y.; Liang, H.; Chen, Z.; Li, Y.; Liu, X.; Chen, R.; Tang, C.; Wang, T.; et al. Comorbidity and its impact on 1590 patients with Covid-19 in China: A Nationwide Analysis. Eur. Respir. J. 2020, 55, 2000547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.; Lau, E.H.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus–Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Bhatraju, P.K.; Ghassemieh, B.J.; Nichols, M.; Kim, R.; Jerome, K.R.; Nalla, A.K.; Greninger, A.L.; Pipavath, S.; Wurfel, M.M.; Evans, L.; et al. Covid-19 in Critically Ill Patients in the Seattle Region—Case Series. N. Engl. J. Med. 2020, 382, 2012–2022. [Google Scholar] [CrossRef] [PubMed]
- Ejaz, H.; Alsrhani, A.; Zafar, A.; Javed, H.; Junaid, K.; Abdalla, A.E.; Abosalif, K.O.A.; Ahmed, Z.; Younas, S. COVID-19 and comorbidities: Deleterious impact on infected patients. J. Infect. Public Health 2020, 13, 1833–1839. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Tao, Z.W.; Wang, L.; Yuan, M.L.; Liu, K.; Zhou, L.; Wei, S.; Deng, Y.; Liu, J.; Liu, H.G.; et al. Analysis of factors associated with disease outcomes in hospitalized patients with 2019 novel coronavirus disease. Chin. Med. J. 2020, 133, 1032–1038. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Zheng, Y.-Y.; Ma, Y.-T.; Zhang, J.-Y.; Xie, X. COVID-19 and the cardiovascular system. Nat. Rev. Cardiol. 2020, 17, 259–260. [Google Scholar] [CrossRef] [Green Version]
- Fang, L.; Karakiulakis, G.; Roth, M. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir. Med. 2020, 8, e21. [Google Scholar] [CrossRef]
- Sica, A.; Massarotti, M. Myeloid suppressor cells in cancer and autoimmunity. J. Autoimmun. 2017, 85, 117–125. [Google Scholar] [CrossRef]
- Li, J.-Y.; Duan, X.-F.; Wang, L.-P.; Xu, Y.-J.; Huang, L.; Zhang, T.-F.; Liu, J.-Y.; Li, F.; Zhang, Z.; Yue, D.-L.; et al. Selective Depletion of Regulatory T Cell Subsets by Docetaxel Treatment in Patients with Nonsmall Cell Lung Cancer. J. Immunol. Res. 2014, 2014, 286170. [Google Scholar] [CrossRef]
- Zhang, L.; Zhu, F.; Xie, L.; Wang, C.; Wang, J.; Chen, R.; Jia, P.; Guan, H.Q.; Peng, L.; Chen, Y.; et al. Clinical characteristics of COVID-19-infected cancer patients: A retrospective case study in three hospitals within Wuhan, China. Ann. Oncol. 2020, 31, 894–901. [Google Scholar] [CrossRef]
- Mehta, V.; Goel, S.; Kabarriti, R.; Cole, D.; Goldfinger, M.; Acuna-Villaorduna, A.; Pradhan, K.; Thota, R.; Reissman, S.; Sparano, J.A.; et al. Case Fatality Rate of Cancer Patients with COVID-19 in a New York Hospital System. Cancer Discov. 2020, 10, 935–941. [Google Scholar] [CrossRef]
- Kuderer, N.M.; Choueiri, T.K.; Shah, D.P.; Shyr, Y.; Rubinstein, S.M.; Rivera, D.R.; Shete, S.; Hsu, C.-Y.; Desai, A.; de Lima Lopes, G., Jr.; et al. Clinical impact of COVID-19 on patients with cancer (CCC19): A cohort study. Lancet 2020, 395, 1907–1918. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China. JAMA 2020, 323, 1239. [Google Scholar] [CrossRef]
- Liu, C.; Zhao, Y.; Okwan-Duodu, D.; Basho, R.; Cui, X. COVID-19 in cancer patients: Risk, clinical features, and management. Cancer Biol. Med. 2020, 17, 519–527. [Google Scholar] [CrossRef]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; Yu, T.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Miyashita, H.; Mikami, T.; Chopra, N.; Yamada, T.; Chernyavsky, S.; Rizk, D.; Cruz, C. Do patients with cancer have a poorer prognosis of COVID-19? An experience in New York City. Ann. Oncol. 2020, 31, 1088–1089. [Google Scholar] [CrossRef]
- Shoumariyeh, K.; Biavasco, F.; Ihorst, G.; Rieg, S.; Nieters, A.; Kern, W.V.; Miething, C.; Duyster, J.; Engelhardt, M.; Bertz, H. Covid-19 in patients with hematological and solid cancers at a Comprehensive Cancer Center in Germany. Cancer Med. 2020, 9, 8412–8422. [Google Scholar] [CrossRef]
- Lee, L.Y.; Cazier, J.B.; Angelis, V.; Arnold, R.; Bisht, V.; Campton, N.A.; Chackathayil, J.; Cheng, V.W.; Curley, H.M.; Fittall, M.W.; et al. COVID-19 mortality in patients with cancer on chemotherapy or other anticancer treatments: A prospective cohort study. Lancet 2020, 395, 1919–1926. [Google Scholar] [CrossRef]
- Miller, S.; Wherry, L.R.; Mazumder, B. Estimated Mortality Increases During The COVID-19 Pandemic By Socioeconomic Status, Race, and Ethnicity. Health Aff. 2021, 40, 1252–1260. [Google Scholar] [CrossRef] [PubMed]
- Dai, M.; Liu, D.; Liu, M.; Zhou, F.; Li, G.; Chen, Z.; Zhang, Z.; You, H.; Wu, M.; Zheng, Q.; et al. Patients with cancer appear more vulnerable to SARS-COV-2: A multi-center study during the COVID-19 outbreak. Cancer Discov. 2020, 10, 783–791. [Google Scholar] [PubMed]
- Chueh, T.-I.; Zheng, C.-M.; Hou, Y.-C.; Lu, K.-C. Novel Evidence of Acute Kidney Injury in COVID-19. J. Clin. Med. 2020, 9, 3547. [Google Scholar] [CrossRef] [PubMed]
- Mina, A.; van Besien, K.; Platanias, L.C. Hematological manifestations of COVID-19. Leuk. Lymphoma 2020, 61, 2790–2798. [Google Scholar] [CrossRef]
- Huang, Y.; Kim, B.Y.S.; Chan, C.K.; Hahn, S.M.; Weissman, I.L.; Jiang, W. Improving immune–vascular crosstalk for cancer immunotherapy. Nat. Rev. Immunol. 2018, 18, 195–203. [Google Scholar] [CrossRef]
- Rotz, S.J.; Leino, D.; Szabo, S.; Mangino, J.L.; Turpin, B.K.; Pressey, J.G. Severe cytokine release syndrome in a patient receiving PD-1-directed therapy. Pediatr. Blood Cancer 2017, 64, e26642. [Google Scholar] [CrossRef]
- Liang, W.; Guan, W.; Chen, R.; Wang, W.; Li, J.; Xu, K.; Li, C.; Ai, Q.; Lu, W.; Liang, H.; et al. Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. Lancet Oncol. 2020, 21, 335–337. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Characteristic | n = 416 1 |
|---|---|
| Age | |
| Median (Minimum–Maximum) | 60 (9–92) |
| Mean (SD) | 59 (16) |
| Days Since COVID Diagnosis | |
| Median (Minimum–Maximum) | 296 (0–462) |
| Mean (SD) | 240 (128) |
| Gender | |
| Female | 224 (53.8%) |
| Male | 192 (46.2%) |
| Race | |
| Asian | 12 (3.0%) |
| Black or African American | 70 (17.5%) |
| White | 288 (72.0%) |
| Other | 30 (7.5%) |
| Unknown | 16 |
| Ethnicity | |
| Hispanic or Latino | 71 (17.7%) |
| Not Hispanic or Latino | 330 (82.3%) |
| Unknown | 15 |
| Malignancy Type | |
| HM | 72 (17.3%) |
| Solid tumors | 344 (82.7%) |
| Tumor Stage | |
| Low | 263 (65.3%) |
| High | 68 (16.9%) |
| HM | 72 (17.9%) |
| Unknown | 13 |
| On Treatment | |
| No | 312 (75.5%) |
| Yes | 101 (24.5%) |
| Unknown | 3 |
| Treatment Completion History | |
| Complete >12mo before COVID | 237 (58.1%) |
| On Treatment | 101 (24.8%) |
| Complete <3mo before COVID | 14 (3.4%) |
| Complete 3–12mo before COVID | 22 (5.4%) |
| Never treated | 34 (8.3%) |
| Unknown | 8 |
| Treatment Type | |
| Completed Trt | 273 (66.9%) |
| On Immunotherapy | 14 (3.4%) |
| On Chemo | 44 (10.8%) |
| On Other Trt | 43 (10.5%) |
| Never Treated | 34 (8.3%) |
| Unknown | 8 |
| Clotting Events | |
| No | 371 (89.6%) |
| Yes | 43 (10.4%) |
| Unknown | 2 |
| Death | |
| No | 341 (82.0%) |
| Yes | 75 (18.0%) |
| Cause of Death (COVID) | |
| Alive | 341 (82.0%) |
| COVID related | 46 (11.1%) |
| Not COVID related | 23 (5.5%) |
| Unknown | 6 (1.4%) |
| ICU Care | |
| No | 336 (82.4%) |
| Yes | 72 (17.6%) |
| Unknown | 8 |
| ICU Intubation | |
| No | 367 (89.5%) |
| Yes | 43 (10.5%) |
| Unknown | 6 |
| Characteristic | No, n = 371 1 | Yes, n = 43 1 | n | p-Value 2 |
|---|---|---|---|---|
| Solid tumors or HM | 414 | 0.5 | ||
| HM | 66 (92%) | 6 (8.3%) | ||
| Solid tumors | 305 (89%) | 37 (11%) | ||
| Stage | 402 | 0.2 | ||
| Early | 239 (91%) | 24 (9.1%) | ||
| Advanced | 56 (84%) | 11 (16%) | ||
| HM | 66 (92%) | 6 (8.3%) | ||
| Unknown | 10 | 2 |
| Outcomes by Clinical Parameters | ICU Admission | ICU Intubation | Overall Survival | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Characteristic | n | OR 1 | 95% CI 1 | p-Value | OR 1 | 95% CI 1 | p-Value | HR 1 | 95% CI 1 | p-Value |
| Age | 408 | 1.03 | 1.01, 1.05 | <0.001 | 1.03 | 1.00, 1.05 | 0.023 | 1.05 | 1.03, 1.07 | <0.001 |
| Gender | ||||||||||
| Female | 219 | — | — | — | — | — | — | |||
| Male | 189 | 2.22 | 1.32, 3.79 | 0.003 | 2.16 | 1.14, 4.22 | 0.021 | 2.31 | 1.44, 3.73 | <0.001 |
| Race | 0.11 | 0.2 | 0.4 | |||||||
| White | 284 | — | — | — | — | — | — | |||
| Black or African American | 67 | 1.81 | 0.92, 3.42 | 0.074 | 1.83 | 0.80, 3.93 | 0.13 | 0.62 | 0.31, 1.26 | 0.2 |
| Other | 42 | 1.80 | 0.79, 3.83 | 0.14 | 1.74 | 0.61, 4.29 | 0.3 | 0.92 | 0.44, 1.93 | 0.8 |
| Ethnicity | ||||||||||
| Hispanic or Latino | 70 | — | — | — | — | — | — | |||
| Not Hispanic or Latino | 324 | 0.80 | 0.42, 1.59 | 0.5 | 0.75 | 0.35, 1.75 | 0.5 | 1.40 | 0.72, 2.72 | 0.3 |
| Malignancy Type | ||||||||||
| HM | 71 | — | — | — | — | — | — | |||
| Solid tumors | 337 | 0.42 | 0.24, 0.78 | 0.004 | 0.34 | 0.17, 0.68 | 0.002 | 0.61 | 0.36, 1.04 | 0.072 |
| Tumor Stage | 0.006 | 0.006 | 0.002 | |||||||
| Low | 260 | — | — | — | — | — | — | |||
| High | 65 | 1.35 | 0.62, 2.77 | 0.4 | 1.23 | 0.43, 3.04 | 0.7 | 2.41 | 1.37, 4.24 | 0.002 |
| HM | 71 | 2.79 | 1.48, 5.19 | 0.001 | 3.24 | 1.54, 6.71 | 0.002 | 2.16 | 1.22, 3.84 | 0.009 |
| On Treatment | ||||||||||
| No | 308 | — | — | — | — | — | — | |||
| Yes | 98 | 1.53 | 0.86, 2.66 | 0.14 | 1.70 | 0.84, 3.34 | 0.13 | 1.89 | 1.18, 3.05 | 0.008 |
| Treatment Completion History | 0.6 | 0.6 | 0.057 | |||||||
| Complete >12 mo before COVID | 234 | — | — | — | — | — | — | |||
| On Treatment | 98 | 1.54 | 0.84, 2.76 | 0.2 | 1.73 | 0.82, 3.53 | 0.14 | 2.16 | 1.29, 3.62 | 0.003 |
| Complete <3 mo before COVID | 14 | 1.45 | 0.32, 4.92 | 0.6 | 0.79 | 0.04, 4.26 | 0.8 | 1.09 | 0.26, 4.54 | >0.9 |
| Complete 3–12 mo before COVID | 21 | 0.89 | 0.20, 2.79 | 0.9 | 1.02 | 0.16, 3.85 | >0.9 | 1.55 | 0.55, 4.38 | 0.4 |
| Never treated | 34 | 0.92 | 0.30, 2.35 | 0.9 | 0.99 | 0.22, 3.09 | >0.9 | 1.84 | 0.85, 4.01 | 0.12 |
| Treatment Type | 0.5 | 0.6 | 0.001 | |||||||
| Completed Trt | 269 | — | — | — | — | — | — | |||
| On Immunotherapy | 13 | 1.58 | 0.34, 5.40 | 0.5 | 1.88 | 0.28, 7.54 | 0.4 | 4.89 | 2.27, 10.5 | <0.001 |
| On Chemo | 44 | 1.17 | 0.48, 2.58 | 0.7 | 1.68 | 0.59, 4.14 | 0.3 | 1.95 | 1.00, 3.83 | 0.051 |
| On Other Trt | 41 | 1.93 | 0.87, 4.05 | 0.092 | 1.77 | 0.62, 4.40 | 0.2 | 1.38 | 0.64, 2.96 | 0.4 |
| Never Treated | 34 | 0.91 | 0.30, 2.29 | 0.8 | 1.00 | 0.23, 3.08 | >0.9 | 1.76 | 0.82, 3.79 | 0.15 |
| Outcomes by Laboratory Parameters | ICU Admission | ICU Intubation | Overall Survival | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Characteristic | Summary Statistics 1 | OR 2 | 95% CI 2 | p-Value | OR 2 | 95% CI 2 | p-Value | HR 2 | 95% CI 2 | p-Value |
| ANC | ||||||||||
| <1500 | 21 (5.5%) | — | — | — | — | — | — | |||
| ≥1500 | 361 (95%) | 1.43 | 0.47, 6.23 | 0.6 | NA | NA | NA | 1.05 | 0.38, 2.86 | >0.9 |
| Unknown | 34 | |||||||||
| Lymphocyte Count | 0.002 | 0.007 | 0.011 | |||||||
| <500 | 55 (14%) | — | — | — | — | — | — | |||
| 500–1000 | 134 (35%) | 0.93 | 0.46, 1.94 | 0.9 | 0.72 | 0.32, 1.67 | 0.4 | 0.66 | 0.36, 1.20 | 0.2 |
| >1000 | 193 (51%) | 0.35 | 0.17, 0.75 | 0.006 | 0.27 | 0.11, 0.66 | 0.004 | 0.40 | 0.22, 0.74 | 0.003 |
| Unknown | 34 | |||||||||
| HB | <0.001 | 0.006 | <0.001 | |||||||
| <10 | 67 (17%) | — | — | — | — | — | — | |||
| 10–13 | 182 (47%) | 0.31 | 0.16, 0.61 | <0.001 | 0.33 | 0.15, 0.71 | 0.004 | 0.47 | 0.29, 0.78 | 0.003 |
| >13 | 140 (36%) | 0.32 | 0.16, 0.64 | 0.001 | 0.32 | 0.14, 0.72 | 0.007 | 0.13 | 0.06, 0.29 | <0.001 |
| Unknown | 27 | |||||||||
| Platelet | <0.001 | 0.008 | <0.001 | |||||||
| <50 | 7 (1.9%) | — | — | — | — | — | — | |||
| 50–99 | 17 (4.5%) | 0.31 | 0.04, 1.93 | 0.2 | 1.36 | 0.21, 11.6 | 0.8 | 0.96 | 0.26, 3.64 | >0.9 |
| 100–149 | 62 (17%) | 0.10 | 0.01, 0.51 | 0.010 | 0.22 | 0.04, 1.83 | 0.12 | 0.34 | 0.10, 1.20 | 0.093 |
| ≥150 | 288 (77%) | 0.07 | 0.01, 0.33 | 0.002 | 0.25 | 0.05, 1.83 | 0.11 | 0.23 | 0.07, 0.73 | 0.013 |
| Unknown | 42 | |||||||||
| Ferritin | 0.064 | 0.3 | 0.010 | |||||||
| <500 | 116 (65%) | — | — | — | — | — | — | |||
| 500–1000 | 31 (17%) | 2.53 | 1.06, 5.93 | 0.034 | 1.94 | 0.68, 5.17 | 0.2 | 2.80 | 1.39, 5.64 | 0.004 |
| >1000 | 31 (17%) | 2.00 | 0.80, 4.80 | 0.13 | 1.94 | 0.68, 5.17 | 0.2 | 2.13 | 1.00, 4.55 | 0.051 |
| Unknown | 238 | |||||||||
| Lactate | 0.14 | 0.7 | 0.018 | |||||||
| <2 | 158 (76%) | — | — | — | — | — | — | |||
| 2–5 | 43 (21%) | 1.08 | 0.50, 2.23 | 0.8 | 1.04 | 0.41, 2.39 | >0.9 | 1.17 | 0.63, 2.19 | 0.6 |
| >5 | 6 (2.9%) | 9.28 | 1.33, 184 | 0.049 | 2.27 | 0.30, 12.2 | 0.4 | 4.44 | 1.59, 12.4 | 0.004 |
| Unknown | 209 | |||||||||
| D-dimer | ||||||||||
| < 500 | 93 (54%) | — | — | — | — | — | — | |||
| ≥500 | 78 (46%) | 1.48 | 0.77, 2.89 | 0.2 | 1.53 | 0.73, 3.26 | 0.3 | 2.27 | 1.22, 4.22 | 0.009 |
| Unknown | 245 | |||||||||
| Procalcitonin | ||||||||||
| <0.5 | 121 (72%) | — | — | — | — | — | — | |||
| ≥0.5 | 46 (28%) | 1.52 | 0.73, 3.11 | 0.3 | 1.54 | 0.65, 3.49 | 0.3 | 2.27 | 1.30, 3.97 | 0.004 |
| Unknown | 249 | |||||||||
| CRP | ||||||||||
| <10 | 115 (71%) | — | — | — | — | — | — | |||
| ≥10 | 48 (29%) | 2.88 | 1.40, 5.96 | 0.004 | 2.47 | 1.13, 5.39 | 0.022 | 1.25 | 0.66, 2.35 | 0.5 |
| Unknown | 253 | |||||||||
| LDH | ||||||||||
| <250 | 81 (46%) | — | — | — | — | — | — | |||
| ≥250 | 95 (54%) | 4.67 | 2.25, 10.4 | <0.001 | 4.46 | 1.92, 11.7 | 0.001 | 1.29 | 0.70, 2.36 | 0.4 |
| Unknown | 240 | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mina, A.; Galvez, C.; Karmali, R.; Mulcahy, M.; Mi, X.; Kocherginsky, M.; Gurley, M.J.; Katam, N.; Gradishar, W.; Altman, J.K.; et al. Outcomes of Cancer Patients with COVID-19 in a Hospital System in the Chicago Metropolitan Area. Cancers 2022, 14, 2209. https://doi.org/10.3390/cancers14092209
Mina A, Galvez C, Karmali R, Mulcahy M, Mi X, Kocherginsky M, Gurley MJ, Katam N, Gradishar W, Altman JK, et al. Outcomes of Cancer Patients with COVID-19 in a Hospital System in the Chicago Metropolitan Area. Cancers. 2022; 14(9):2209. https://doi.org/10.3390/cancers14092209
Chicago/Turabian StyleMina, Alain, Carlos Galvez, Reem Karmali, Mary Mulcahy, Xinlei Mi, Masha Kocherginsky, Michael J Gurley, Neelima Katam, William Gradishar, Jessica K Altman, and et al. 2022. "Outcomes of Cancer Patients with COVID-19 in a Hospital System in the Chicago Metropolitan Area" Cancers 14, no. 9: 2209. https://doi.org/10.3390/cancers14092209