
Improvement in Post-Autologous Stem Cell Transplant Survival of Multiple Myeloma Patients: A Long-Term Institutional Experience

 , , ,
, , , 

Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
3. Statistical Analysis
4. Results
4.1. Patient Characteristics
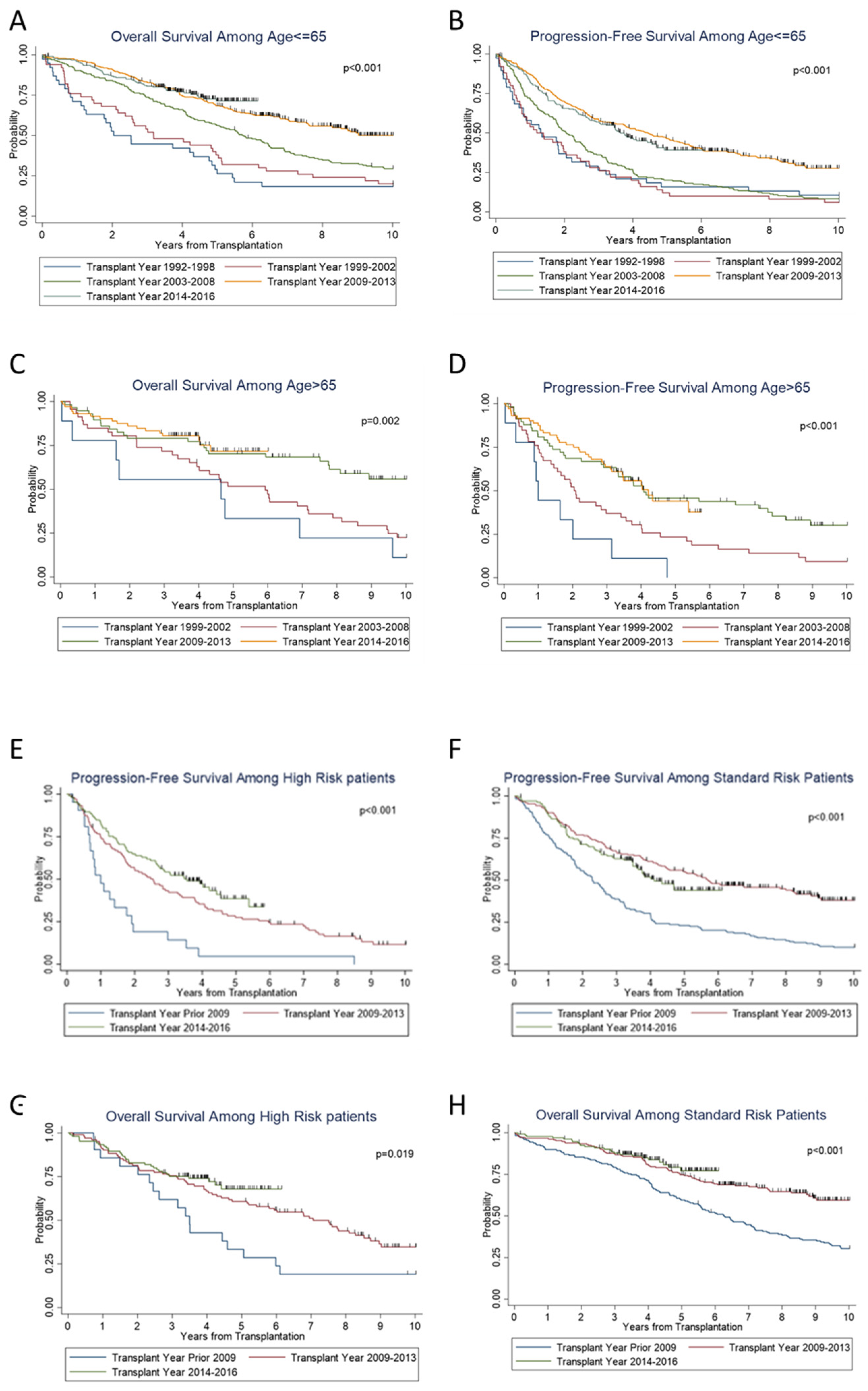
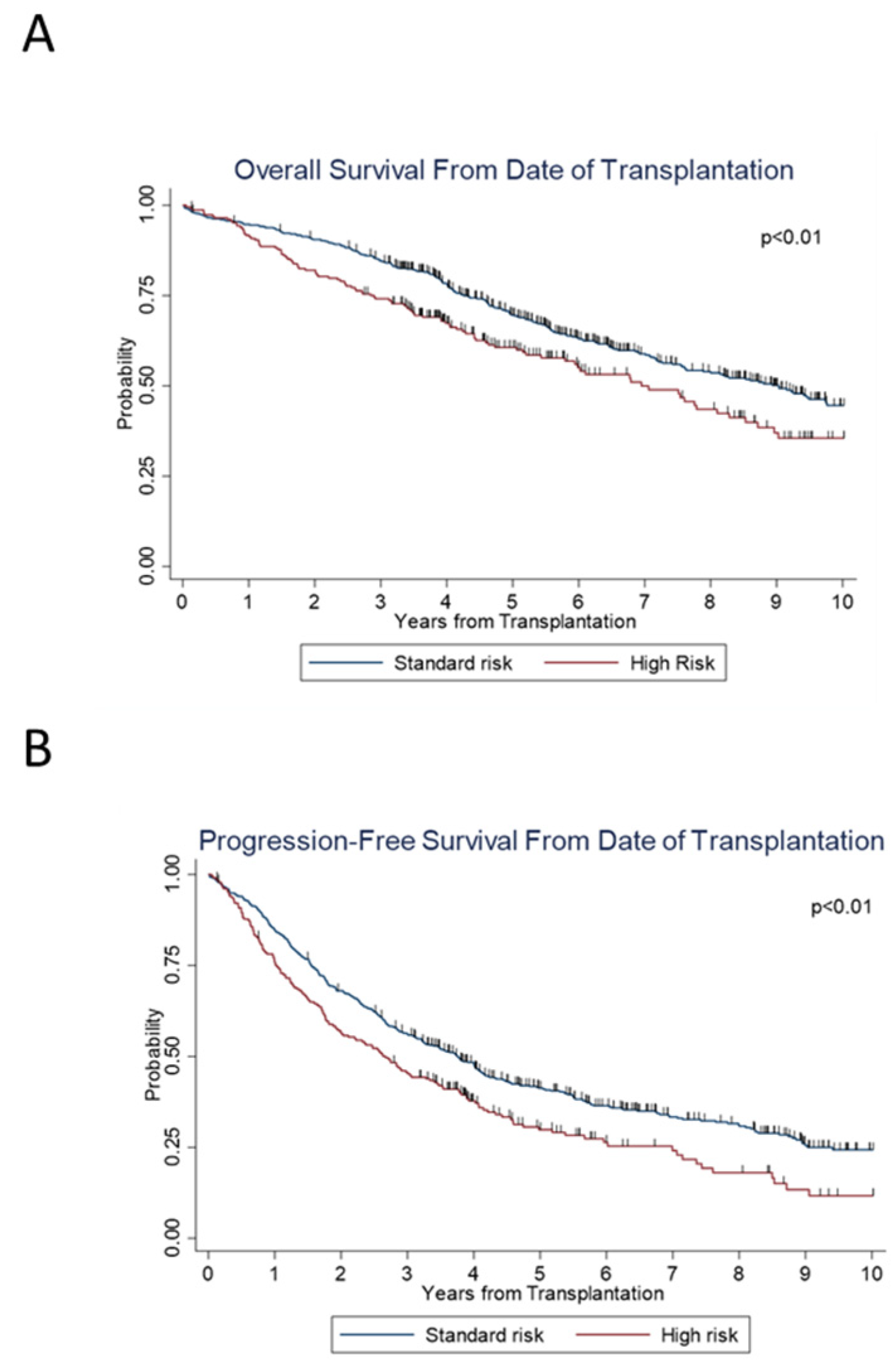
4.2. Survival Outcomes
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kumar, S.K.; Rajkumar, S.V.; Dispenzieri, A.; Lacy, M.Q.; Hayman, S.R.; Buadi, F.K.; Zeldenrust, S.R.; Dingli, D.; Russell, S.J.; Lust, J.A.; et al. Improved survival in multiple myeloma and the impact of novel therapies. Blood 2008, 111, 2516–2520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turesson, I.; Velez, R.; Kristinsson, S.Y.; Landgren, O. Patterns of Improved Survival in Patients with Multiple Myeloma in the Twenty-First Century: A Population-Based Study. J. Clin. Oncol. 2010, 28, 830–834. [Google Scholar] [CrossRef] [Green Version]
- Anderson, K.C. Progress and Paradigms in Multiple Myeloma. Clin. Cancer Res. 2016, 22, 5419. [Google Scholar] [CrossRef] [Green Version]
- Attal, M.; Harousseau, J.-L.; Stoppa, A.-M.; Sotto, J.-J.; Fuzibet, J.-G.; Rossi, J.-F.; Casassus, P.; Maisonneuve, H.; Facon, T.; Ifrah, N.; et al. A Prospective, Randomized Trial of Autologous Bone Marrow Transplantation and Chemotherapy in Multiple Myeloma. N. Engl. J. Med. 1996, 335, 91–97. [Google Scholar] [CrossRef]
- Shah, N.; Callander, N.; Ganguly, S.; Gul, Z.; Hamadani, M.; Costa, L.; Sengsayadeth, S.; Abidi, M.; Hari, P.; Mohty, M.; et al. Hematopoietic Stem Cell Transplantation for Multiple Myeloma: Guidelines from the American Society for Blood and Marrow Transplantation. Biol. Blood Marrow Transplant. 2015, 21, 1155–1166. [Google Scholar] [CrossRef] [Green Version]
- Bashir, Q.; Shah, N.; Parmar, S.; Wei, W.; Rondon, G.; Weber, D.M.; Wang, M.; Orlowski, R.Z.; Thomas, S.K.; Shah, J.; et al. Feasibility of autologous hematopoietic stem cell transplant in patients aged ≥ 70 years with multiple myeloma. Leuk. Lymphoma 2012, 53, 118–122. [Google Scholar] [CrossRef]
- Kumar, S.K.; Dingli, D.; Lacy, M.Q.; Dispenzieri, A.; Hayman, S.R.; Buadi, F.K.; Rajkumar, S.V.; Litzow, M.R.; Gertz, M.A. Autologous stem cell transplantation in patients of 70 years and older with multiple myeloma: Results from a matched pair analysis. Am. J. Hematol. 2008, 83, 614–617. [Google Scholar] [CrossRef]
- Paul, B.; Lipe, B.; Ocio, E.M.; Usmani, S.Z. Induction Therapy for Newly Diagnosed Multiple Myeloma. Am. Soc. Clin. Oncol. Educ. Book 2019, 39, e176–e186. [Google Scholar] [CrossRef]
- Ria, R.; Reale, A.; Solimando, A.G.; Mangialardi, G.; Moschetta, M.; Gelao, L.; Iodice, G.; Vacca, A. Induction therapy and stem cell mobilization in patients with newly diagnosed multiple myeloma. Stem Cells Int. 2012, 2012, 607260. [Google Scholar] [CrossRef] [Green Version]
- Latif, T.; Chauhan, N.; Khan, R.; Moran, A.; Usmani, S.Z. Thalidomide and its analogues in the treatment of Multiple Myeloma. Exp. Hematol. Oncol. 2012, 1, 27. [Google Scholar] [CrossRef] [Green Version]
- Cavo, M.; Zamagni, E.; Tosi, P.; Tacchetti, P.; Cellini, C.; Cangini, D.; de Vivo, A.; Testoni, N.; Nicci, C.; Terragna, C.; et al. Superiority of thalidomide and dexamethasone over vincristine-doxorubicindexamethasone (VAD) as primary therapy in preparation for autologous transplantation for multiple myeloma. Blood 2005, 106, 35–39. [Google Scholar] [CrossRef]
- Barlogie, B.; Jagannath, S.; Desikan, K.R.; Mattox, S.; Vesole, D.; Siegel, D.; Tricot, G.; Munshi, N.; Fassas, A.; Singhal, S.; et al. Total therapy with tandem transplants for newly diagnosed multiple myeloma. Blood 1999, 93, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Barlogie, B.; Kyle, R.A.; Anderson, K.C.; Greipp, P.R.; Lazarus, H.M.; Hurd, D.D.; McCoy, J.; Moore, D.F.; Dakhil, S.R.; Lanier, K.S.; et al. Standard Chemotherapy Compared with High-Dose Chemoradiotherapy for Multiple Myeloma: Final Results of Phase III US Intergroup Trial S9321. J. Clin. Oncol. 2006, 24, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Barlogie, B.; Jagannath, S.; Vesole, D.H.; Naucke, S.; Cheson, B.; Mattox, S.; Bracy, D.; Salmon, S.; Jacobson, J.; Crowley, J.; et al. Superiority of Tandem Autologous Transplantation Over Standard Therapy for Previously Untreated Multiple Myeloma. Blood 1997, 89, 789–793. [Google Scholar] [CrossRef]
- Rajkumar, S.V.; Hayman, S.R.; Lacy, M.Q.; Dispenzieri, A.; Geyer, S.M.; Kabat, B.; Zeldenrust, S.R.; Kumar, S.; Greipp, P.R.; Fonseca, R.; et al. Combination therapy with lenalidomide plus dexamethasone (Rev/Dex) for newly diagnosed myeloma. Blood 2005, 106, 4050–4053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sonneveld, P.; Schmidt-Wolf, I.G.H.; van der Holt, B.; el Jarari, L.; Bertsch, U.; Salwender, H.; Zweegman, S.; Vellenga, E.; Broyl, A.; Blau, I.W.; et al. Bortezomib Induction and Maintenance Treatment in Patients with Newly Diagnosed Multiple Myeloma: Results of the Randomized Phase III HOVON-65/ GMMG-HD4 Trial. J. Clin. Oncol. 2012, 30, 2946–2955. [Google Scholar] [CrossRef]
- Facon, T.; Lee, J.H.; Moreau, P.; Niesvizky, R.; Dimopoulos, M.A.; Hajek, R.; Osman, M.; Aggarwal, S.; Klippel, Z.; San Miguel, J. Phase 3 Study (CLARION) of Carfilzomib, Melphalan, Prednisone (KMP) v Bortezomib, Melphalan, Prednisone (VMP) in Newly Diagnosed Multiple Myeloma (NDMM). Clin. Lymphoma Myeloma Leuk. 2017, 17, e26–e27. [Google Scholar] [CrossRef]
- Tosi, P.; Zamagni, E.; Tacchetti, P.; Ceccolini, M.; Perrone, G.; Brioli, A.; Pallotti, M.C.; Pantani, L.; Petrucci, A.; Baccarani, M.; et al. Thalidomide-dexamethasone as induction therapy before autologous stem cell transplantation in patients with newly diagnosed multiple myeloma and renal insufficiency. Biol. Blood Marrow Transplant. 2010, 16, 1115–1121. [Google Scholar] [CrossRef] [Green Version]
- Cavo, M.; Tacchetti, P.; Patriarca, F.; Petrucci, M.T.; Pantani, L.; Galli, M.; Di Raimondo, F.; Crippa, C.; Zamagni, E.; Palumbo, A.; et al. Bortezomib with thalidomide plus dexamethasone compared with thalidomide plus dexamethasone as induction therapy before, and consolidation therapy after, double autologous stem-cell transplantation in newly diagnosed multiple myeloma: A randomised phase 3 study. Lancet 2010, 376, 2075–2085. [Google Scholar] [CrossRef]
- Rosiñol, L.; Oriol, A.; Teruel, A.I.; Hernández, D.; López-Jiménez, J.; de la Rubia, J.; Granell, M.; Besalduch, J.; Palomera, L.; González, Y.; et al. Superiority of bortezomib, thalidomide, and dexamethasone (VTD) as induction pretransplantation therapy in multiple myeloma: A randomized phase 3 PETHEMA/GEM study. Blood 2012, 120, 1589–1596. [Google Scholar] [CrossRef]
- Durie, B.G.M.; Hoering, A.; Abidi, M.H.; Rajkumar, S.V.; Epstein, J.; Kahanic, S.P.; Thakuri, M.; Reu, F.; Reynolds, C.M.; Sexton, R.; et al. Bortezomib with lenalidomide and dexamethasone versus lenalidomide and dexamethasone alone in patients with newly diagnosed myeloma without intent for immediate autologous stem-cell transplant (SWOG S0777): A randomised, open-label, phase 3 trial. Lancet 2017, 389, 519–527. [Google Scholar] [CrossRef] [Green Version]
- Attal, M.; Lauwers-Cances, V.; Hulin, C.; Leleu, X.; Caillot, D.; Escoffre, M.; Arnulf, B.; Macro, M.; Belhadj, K.; Garderet, L.; et al. Lenalidomide, Bortezomib, and Dexamethasone with Transplantation for Myeloma. N. Engl. J. Med. 2017, 376, 1311–1320. [Google Scholar] [CrossRef]
- Dhakal, B.; Szabo, A.; Chhabra, S.; Hamadani, M.; D’Souza, A.; Usmani, S.Z.; Sieracki, R.; Gyawali, B.; Jackson, J.L.; Asimakopoulos, F.; et al. Autologous Transplantation for Newly Diagnosed Multiple Myeloma in the Era of Novel Agent Induction: A Systematic Review and Meta-analysis. JAMA Oncol. 2018, 4, 343–350. [Google Scholar] [CrossRef]
- McCarthy, P.L.; Owzar, K.; Hofmeister, C.C.; Hurd, D.D.; Hassoun, H.; Richardson, P.G.; Giralt, S.; Stadtmauer, E.A.; Weisdorf, D.J.; Vij, R.; et al. Lenalidomide after stem-cell transplantation for multiple myeloma. N. Engl. J. Med. 2012, 366, 1770–1781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voorhees, P.M.; Kaufman, J.L.; Laubach, J.; Sborov, D.W.; Reeves, B.; Rodriguez, C.; Chari, A.; Silbermann, R.; Costa, L.J.; Anderson, L.D., Jr.; et al. Daratumumab, lenalidomide, bortezomib, and dexamethasone for transplant-eligible newly diagnosed multiple myeloma: The GRIFFIN trial. Blood 2020, 136, 936–945. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S.; Kim, K.; Cheong, J.-W.; Min, Y.H.; Suh, C.; Kim, H.; Jo, D.Y.; Ryoo, H.M.; Yoon, S.S.; Lee, J.H. Complete Remission Status before Autologous Stem Cell Transplantation Is an Important Prognostic Factor in Patients with Multiple Myeloma Undergoing Upfront Single Autologous Transplantation. Biol. Blood Marrow Transplant. 2009, 15, 463–470. [Google Scholar] [CrossRef] [Green Version]
- Vij, R.; Kumar, S.; Zhang, M.-J.; Zhong, X.; Huang, J.; Dispenzieri, A.; Abidi, M.H.; Bird, J.M.; Freytes, C.O.; Gale, R.P.; et al. Impact of Pretransplant Therapy and Depth of Disease Response before Autologous Transplantation for Multiple Myeloma. Biol. Blood Marrow Transplant. 2015, 21, 335–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harousseau, J.-L.; Avet-Loiseau, H.; Attal, M.; Charbonnel, C.; Garban, F.; Hulin, C.; Michallet, M.; Facon, T.; Garderet, L.; Marit, G.; et al. Achievement of at Least Very Good Partial Response Is a Simple and Robust Prognostic Factor in Patients with Multiple Myeloma Treated with High-Dose Therapy: Long-Term Analysis of the IFM 99-02 and 99-04 Trials. J. Clin. Oncol. 2009, 27, 5720–5726. [Google Scholar] [CrossRef]
- Martinez-Lopez, J.; Blade, J.; Mateos, M.-V.; Grande, C.; Alegre, A.; García-Laraña, J.; Sureda, A.; de la Rubia, J.; Conde, E.; Martinez, R.; et al. Long-term prognostic significance of response in multiple myeloma after stem cell transplantation. Blood 2011, 118, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Attal, M.; Lauwers-Cances, V.; Marit, G.; Caillot, D.; Moreau, P.; Facon, T.; Stoppa, A.M.; Hulin, C.; Benboubker, L.; Garderet, L.; et al. Lenalidomide maintenance after stem-cell transplantation for multiple myeloma. N. Engl. J. Med. 2012, 366, 1782–1791. [Google Scholar] [CrossRef] [Green Version]
- Attal, M.; Harousseau, J.-L.; Facon, T.; Guilhot, F.; Doyen, C.; Fuzibet, J.-G.; Monconduit, M.; Hulin, C.; Caillot, D.; Bouabdallah, R.; et al. Single versus Double Autologous Stem-Cell Transplantation for Multiple Myeloma. N. Engl. J. Med. 2003, 349, 2495–2502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavo, M.; Tosi, P.; Zamagni, E.; Cellini, C.; Tacchetti, P.; Patriarca, F.; Di Raimondo, F.; Volpe, E.; Ronconi, S.; Cangini, D.; et al. Prospective, randomized study of single compared with double autologous stem-cell transplantation for multiple myeloma: Bologna 96 clinical study. J. Clin. Oncol. 2007, 25, 2434–2441. [Google Scholar] [CrossRef]
- Sonneveld, P.; van der Holt, B.; Segeren, C.M.; Vellenga, E.; Croockewit, A.J.; Verhoe, G.E.; Cornelissen, J.J.; Schaafsma, M.R.; van Oers, M.H.; Wijermans, P.W.; et al. Intermediate-dose melphalan compared with myeloablative treatment in multiple myeloma: Long-term follow-up of the Dutch Cooperative Group HOVON 24 trial. Haematologica 2007, 92, 928–935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stadtmauer, E.A.; Pasquini, M.C.; Blackwell, B.; Hari, P.; Bashey, A.; Devine, S.; Efebera, Y.; Ganguly, S.; Gasparetto, C.; Geller, N.; et al. Autologous Transplantation, Consolidation, and Maintenance Therapy in Multiple Myeloma: Results of the BMT CTN 0702 Trial. J. Clin. Oncol. 2019, 37, 589–597. [Google Scholar] [CrossRef]
- Gay, F.; Musto, P.; Rota-Scalabrini, D.; Bertamini, L.; Belotti, A.; Galli, M.; Offidani, M.; Zamagni, E.; Ledda, A.; Grasso, M.; et al. Carfilzomib with cyclophosphamide and dexamethasone or lenalidomide and dexamethasone plus autologous transplantation or carfilzomib plus lenalidomide and dexamethasone, followed by maintenance with carfilzomib plus lenalidomide or lenalidomide alone for patients with newly diagnosed multiple myeloma (FORTE): A randomised, open-label, phase 2 trial. Lancet Oncol. 2021, 22, 1705–1720. [Google Scholar] [CrossRef]
- Ludwig, H.; Bolejack, V.; Crowley, J.; Bladé, J.; Miguel, J.S.; Kyle, R.A.; Rajkumar, S.V.; Shimizu, K.; Turesson, I.; Westin, J.; et al. Survival and Years of Life Lost in Different Age Cohorts of Patients with Multiple Myeloma. J. Clin. Oncol. 2010, 28, 1599–1605. [Google Scholar] [CrossRef] [Green Version]
- Kristinsson, S.Y.; Landgren, O.; Dickman, P.W.; Derolf, Å.R.; Björkholm, M. Patterns of Survival in Multiple Myeloma: A Population-Based Study of Patients Diagnosed in Sweden from 1973 to 2003. J. Clin. Oncol. 2007, 25, 1993–1999. [Google Scholar] [CrossRef]
- Kumar, S.K.; Dispenzieri, A.; Lacy, M.Q.; Gertz, M.A.; Buadi, F.K.; Pandey, S.; Kapoor, P.; Dingli, D.; Hayman, S.R.; Leung, N.; et al. Continued improvement in survival in multiple myeloma: Changes in early mortality and outcomes in older patients. Leukemia 2014, 28, 1122–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, M.; Zhang, M.-J.; Zhong, X.; Abidi, M.H.; Akpek, G.; Bacher, U.; Callander, N.S.; Dispenzieri, A.; Freytes, C.O.; Fung, H.C.; et al. Older patients with myeloma derive similar benefit from autologous transplantation. Biol. Blood Marrow Transplant. 2014, 20, 1796–1803. [Google Scholar] [CrossRef] [Green Version]
- Neben, K.; Jauch, A.; Bertsch, U.; Heiss, C.; Hielscher, T.; Seckinger, A.; Mors, T.; Müller, N.Z.; Hillengass, J.; Raab, M.S.; et al. Combining information regarding chromosomal aberrations t(4;14) and del(17p13) with the International Staging System classification allows stratification of myeloma patients undergoing autologous stem cell transplantation. Haematologica 2010, 95, 1150–1157. [Google Scholar] [CrossRef] [Green Version]
- Avet-Loiseau, H.; Durie, B.G.; Cavo, M.; Attal, M.; Gutierrez, N.; Haessler, J.; Goldschmidt, H.; Hajek, R.; Lee, J.H.; Sezer, O.; et al. Combining fluorescent in situ hybridization data with ISS staging improves risk assessment in myeloma: An International Myeloma Working Group collaborative project. Leukemia 2013, 27, 711–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sonneveld, P.; Avet-Loiseau, H.; Lonial, S.; Usmani, S.; Siegel, D.; Anderson, K.C.; Chng, W.-J.; Moreau, P.; Attal, M.; Kyle, R.A.; et al. Treatment of multiple myeloma with high-risk cytogenetics: A consensus of the International Myeloma Working Group. Blood 2016, 127, 2955–2962. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| ASCT Year | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total (n = 1001) | 1992–1998 (n = 38) | 1999–2002 (n = 59) | 2003–2008 (n = 241) | 2009–2013 (n = 376) | 2014–2016 (n = 287) | p-Value | |||||||
| Age at ASCT (median, range) | 58 | 18–81 | 54 | 36–65 | 57 | 39–71 | 57 | 30–76 | 58 | 18–81 | 60 | 28–75 | <0.01 |
| N | % | N | % | N | % | N | % | N | % | N | % | <0.01 | |
| Age ≤ 65 | 816 | 81.5 | 38 | 100.0 | 50 | 84.7 | 195 | 80.9 | 318 | 84.6 | 215 | 74.9 | |
| Age > 65 | 185 | 18.5 | 0 | 0.0 | 9 | 15.3 | 46 | 19.1 | 58 | 15.4 | 72 | 25.1 | |
| Gender | 0.69 | ||||||||||||
| Male | 585 | 58.4 | 22 | 57.9 | 31 | 52.5 | 144 | 59.8 | 227 | 60.4 | 161 | 56.1 | |
| Female | 416 | 41.6 | 16 | 42.1 | 28 | 47.5 | 97 | 40.2 | 149 | 39.6 | 126 | 43.9 | |
| Race | 0.52 | ||||||||||||
| Black | 141 | 14.1 | 4 | 10.5 | 7 | 11.9 | 42 | 17.4 | 49 | 13.0 | 39 | 13.6 | |
| White | 850 | 84.9 | 33 | 86.8 | 51 | 86.4 | 199 | 82.6 | 322 | 85.6 | 245 | 85.4 | |
| Others | 10 | 1.0 | 1 | 2.6 | 1 | 1.7 | 0 | 0.0 | 5 | 1.3 | 3 | 1.0 | |
| Myeloma type | 0.12 | ||||||||||||
| IGA | 226 | 22.7 | 6 | 16.7 | 16 | 28.1 | 62 | 25.7 | 72 | 19.1 | 70 | 24.4 | |
| IGG | 534 | 53.6 | 25 | 69.4 | 33 | 57.9 | 128 | 53.1 | 197 | 52.4 | 151 | 52.6 | |
| LC only | 193 | 19.4 | 2 | 5.6 | 5 | 8.8 | 37 | 15.4 | 91 | 24.2 | 58 | 20.2 | |
| Nonsecretory | 24 | 2.4 | 2 | 5.6 | 3 | 5.3 | 6 | 2.5 | 10 | 2.7 | 3 | 1.0 | |
| IGD | 15 | 1.5 | 1 | 2.8 | 0 | 0.0 | 5 | 2.1 | 5 | 1.3 | 4 | 1.4 | |
| Biclonal | 2 | 0.2 | 0 | 0.0 | 0 | 0.0 | 2 | 0.8 | 0 | 0.0 | 0 | 0.0 | |
| PLASMA CELL LEUKEMIA | 1 | 0.1 | 0 | 0.0 | 0 | 0.0 | 1 | 0.4 | 0 | 0.0 | 0 | 0.0 | |
| IGM | 1 | 0.1 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.3 | 0 | 0.0 | |
| IGE | 1 | 0.1 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.3 | |
| Unknown | 4 | 2 | 2 | 0 | 0 | 0 | |||||||
| ISS staging | 0.55 | ||||||||||||
| 1 | 286 | 38.1 | 1 | 100.0 | 9 | 32.1 | 58 | 33.7 | 116 | 37.7 | 102 | 42.3 | |
| 2 | 244 | 32.5 | 0 | 0.0 | 9 | 32.1 | 57 | 33.1 | 99 | 32.1 | 79 | 32.8 | |
| 3 | 220 | 29.3 | 0 | 0.0 | 10 | 35.7 | 57 | 33.1 | 93 | 30.2 | 60 | 24.9 | |
| Unknown | 251 | 37 | 31 | 69 | 68 | 46 | |||||||
| Cytogenetic risk | <0.01 | ||||||||||||
| Standard risk | 530 | 69.7 | 1 | 100.0 | 5 | 100.0 | 178 | 89.4 | 212 | 67.3 | 134 | 55.8 | |
| High risk | 230 | 30.3 | 0 | 0.0 | 0 | 0.0 | 21 | 10.6 | 103 | 32.7 | 106 | 44.2 | |
| NA | 241 | 37 | 54 | 42 | 61 | 47 | |||||||
| Melphalan use | <0.01 | ||||||||||||
| 140 | 127 | 12.7 | 0 | 0.0 | 5 | 8.5 | 18 | 7.5 | 56 | 14.9 | 48 | 16.7 | |
| 200 | 803 | 80.2 | 2 | 5.3 | 22 | 37.3 | 220 | 91.3 | 320 | 85.1 | 239 | 83.3 | |
| Missing or No Use | 71 | 7.1 | 36 | 94.7 | 32 | 54.2 | 3 | 1.2 | 0 | 0.0 | 0 | 0.0 | |
| Pre-Transplant response | <0.01 | ||||||||||||
| Others | 141 | 14.1 | 12 | 31.6 | 14 | 23.7 | 33 | 13.7 | 55 | 14.6 | 27 | 9.4 | |
| CR/VGPR | 455 | 45.5 | 2 | 5.3 | 9 | 15.3 | 96 | 39.8 | 193 | 51.3 | 155 | 54.0 | |
| PR | 405 | 40.5 | 24 | 63.2 | 36 | 61.0 | 112 | 46.5 | 128 | 34.0 | 105 | 36.6 | |
| Post-Transplant response | <0.01 | ||||||||||||
| Others | 103 | 10.3 | 24 | 63.2 | 18 | 30.5 | 29 | 12.0 | 18 | 4.8 | 14 | 4.9 | |
| CR/VGPR | 708 | 70.7 | 11 | 28.9 | 18 | 30.5 | 158 | 65.6 | 302 | 80.3 | 219 | 76.3 | |
| PR | 190 | 19.0 | 3 | 7.9 | 23 | 39.0 | 54 | 22.4 | 56 | 14.9 | 54 | 18.8 | |
| Induction Regimens | <0.01 | ||||||||||||
| Cytoxan based therapy | 5 | 0.5 | 2 | 5.3 | 2 | 3.4 | 1 | 0.4 | 0 | 0.0 | 0 | 0.0 | |
| MP based therapy | 8 | 0.8 | 6 | 15.8 | 2 | 3.4 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| VAD based therapy | 128 | 12.8 | 30 | 78.9 | 54 | 91.5 | 44 | 18.3 | 0 | 0.0 | 0 | 0.0 | |
| Lenalidomide based therapy | 119 | 11.9 | 0 | 0.0 | 0 | 0.0 | 37 | 15.4 | 63 | 16.8 | 19 | 6.6 | |
| Thalidomide and bortezomib based therapy | 29 | 2.9 | 0 | 0.0 | 0 | 0.0 | 22 | 9.1 | 7 | 1.9 | 0 | 0.0 | |
| Thalidomide based therapy | 61 | 6.1 | 0 | 0.0 | 0 | 0.0 | 57 | 23.7 | 4 | 1.1 | 0 | 0.0 | |
| bortezomib based therapy | 324 | 32.4 | 0 | 0.0 | 0 | 0.0 | 66 | 27.4 | 157 | 41.8 | 101 | 35.2 | |
| lenalidomide and Bortezomib based therapy | 323 | 32.3 | 0 | 0.0 | 0 | 0.0 | 14 | 5.8 | 142 | 37.8 | 167 | 58.2 | |
| Melphalan based regimen | 1 | 0.1 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.3 | 0 | 0.0 | |
| Unknown | 3 | 0.3 | 0 | 0.0 | 1 | 1.7 | 0 | 0.0 | 2 | 0.5 | 0 | 0.0 | |
| Received maintenance | 472 | 47.2 | 0 | 0.0 | 0 | 0.0 | 20 | 8.3 | 254 | 67.6 | 198 | 69.0 | <0.01 |
| Maintenance drugs | <0.01 | ||||||||||||
| Lenalidomide | 411 | 87.1 | 0 | 0 | 0 | 0 | 18 | 90 | 233 | 91.7 | 160 | 80.8 | |
| Bortezomib | 51 | 10.8 | 0 | 0 | 0 | 0 | 0 | 0 | 24 | 9.4 | 27 | 13.6 | |
| IXAZOMIB | 13 | 2.8 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0.8 | 11 | 5.6 | |
| LENOLIDIMIDE+bortezomib | 6 | 1.3 | 0 | 0 | 0 | 0 | 0 | 0 | 5 | 2.0 | 1 | 0.5 | |
| Lenalidomide+cyclophosphamide | 6 | 1.3 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0.8 | 4 | 2.0 | |
| Pomalidomide | 8 | 1.7 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0.0 | 8 | 4.0 | |
| Pomalidomide+cyclophosphamide | 2 | 0.4 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0.0 | 2 | 1.0 | |
| Thalidomide | 5 | 1.1 | 0 | 0 | 0 | 0 | 2 | 10 | 3 | 1.2 | 0 | 0.0 | |
| Characteristics | HR | 95% CI | p-Value | |
|---|---|---|---|---|
| Univariable modelTransplant year | ||||
| Transplant year ≤ 2008 | Reference | |||
| Transplant year 2009—2013 | 0.48 | 0.40 | 0.57 | <0.001 |
| Transplant year 2014—2016 | 0.52 | 0.42 | 0.63 | <0.001 |
| Age at ASCT | 1.00 | 0.99 | 1.01 | 0.814 |
| Age ≤ 65 | Reference | |||
| Age > 65 | 0.90 | 0.74 | 1.09 | 0.296 |
| Gender | ||||
| Male | Reference | |||
| Female | 0.98 | 0.85 | 1.14 | 0.824 |
| Race | ||||
| Black | Reference | |||
| White | 1.01 | 0.82 | 1.25 | 0.923 |
| Others | 0.63 | 0.26 | 1.54 | 0.308 |
| Melphalan dose (mg/m2) | ||||
| 140 | Reference | |||
| 200 | 0.90 | 0.72 | 1.13 | 0.362 |
| Missing or No use | 2.16 | 1.57 | 2.96 | <0.001 |
| Pre-transplant response | ||||
| Others | Reference | |||
| CR/VGPR | 0.44 | 0.36 | 0.55 | <0.001 |
| PR | 0.75 | 0.61 | 0.93 | 0.007 |
| ISS staging | ||||
| 1 | Reference | |||
| 2 | 1.16 | 0.94 | 1.43 | 0.156 |
| 3 | 1.54 | 1.25 | 1.90 | <0.001 |
| Cytogenetics risk | ||||
| Standard risk | Reference | |||
| High risk | 1.39 | 1.16 | 1.67 | <0.001 |
| Myeloma type | ||||
| IGA | Reference | |||
| IGG | 1.03 | 0.86 | 1.24 | 0.763 |
| LC only | 0.91 | 0.72 | 1.14 | 0.406 |
| Others | 1.06 | 0.75 | 1.50 | 0.754 |
| Multivariable model | ||||
| Transplant years | ||||
| Transplant year ≤ 2008 | Reference | |||
| Transplant year 2009–2013 | 0.49 | 0.38 | 0.62 | <0.001 |
| Transplant year 2014–2016 | 0.53 | 0.40 | 0.69 | <0.001 |
| Pre-transplant response | ||||
| Others | Reference | |||
| CR/VGPR | 0.54 | 0.40 | 0.73 | <0.001 |
| PR | 0.90 | 0.67 | 1.22 | 0.500 |
| ISS staging | ||||
| 1 | Reference | |||
| 2 | 1.21 | 0.96 | 1.53 | 0.104 |
| 3 | 1.51 | 1.18 | 1.94 | 0.001 |
| Cytogenetics risk | ||||
| Standard risk | ||||
| High risk | 1.80 | 1.45 | 2.25 | <0.001 |
| Melphalan dose (mg/m2) | ||||
| 140 | Reference | |||
| 200 | 1.10 | 0.81 | 1.50 | 0.535 |
| Missing or No use | 14.06 | 1.82 | 108.46 | 0.011 |
| Characteristics | HR | 95% CI | p-Value | |
|---|---|---|---|---|
| Univariable model | ||||
| Transplant year ≤ 2008 | ||||
| Transplant year 2009—2013 | 0.50 | 0.41 | 0.60 | <0.001 |
| Transplant year 2014—2016 | 0.46 | 0.35 | 0.60 | <0.001 |
| Age at ASCT | 1.01 | 1.00 | 1.02 | 0.219 |
| Age ≤ 65 | Reference | |||
| Age > 65 | 0.96 | 0.76 | 1.21 | 0.717 |
| Gender | ||||
| Male | Reference | |||
| Female | 0.86 | 0.72 | 1.03 | 0.100 |
| Race | ||||
| Black | Reference | |||
| White | 1.07 | 0.83 | 1.39 | 0.589 |
| Others | 0.70 | 0.22 | 2.24 | 0.553 |
| Melphalan dose (mg/m2) | ||||
| 140 | Reference | |||
| 200 | 0.74 | 0.57 | 0.96 | 0.026 |
| Missing or No use | 2.18 | 1.55 | 3.06 | <0.001 |
| Pre-transplant response | ||||
| Others | Reference | |||
| CR/VGPR | 0.45 | 0.35 | 0.58 | <0.001 |
| PR | 0.83 | 0.65 | 1.05 | 0.120 |
| ISS staging | ||||
| 1 | Reference | |||
| 2 | 1.37 | 1.05 | 1.79 | 0.020 |
| 3 | 2.03 | 1.57 | 2.63 | <0.001 |
| Cytogenetics risk | ||||
| Standard risk | Reference | |||
| High risk | 1.42 | 1.13 | 1.79 | 0.003 |
| Myeloma type | ||||
| IGA | Reference | |||
| IGG | 0.87 | 0.71 | 1.08 | 0.217 |
| LC only | 0.79 | 0.60 | 1.04 | 0.095 |
| Others | 0.89 | 0.59 | 1.34 | 0.564 |
| Multivariable model | ||||
| Transplant years | ||||
| Transplant year ≤ 2008 | Reference | |||
| Transplant year 2009–2013 | 0.54 | 0.41 | 0.72 | <0.001 |
| Transplant year 2014–2016 | 0.53 | 0.36 | 0.77 | 0.001 |
| Pre-transplant remission | ||||
| Others | Reference | |||
| CR/VGPR | 0.53 | 0.37 | 0.77 | 0.001 |
| PR | 0.92 | 0.64 | 1.32 | 0.653 |
| ISS staging | ||||
| 1 | Reference | |||
| 2 | 1.48 | 1.09 | 2.02 | 0.011 |
| 3 | 2.00 | 1.48 | 2.70 | <0.001 |
| Cytogenetics risk | ||||
| Standard risk | ||||
| High risk | 1.80 | 1.36 | 2.37 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nunnelee, J.; Cottini, F.; Zhao, Q.; Faisal, M.S.; Elder, P.; Rosko, A.; Bumma, N.; Khan, A.; Devarakonda, S.; Benson, D.M.; et al. Improvement in Post-Autologous Stem Cell Transplant Survival of Multiple Myeloma Patients: A Long-Term Institutional Experience. Cancers 2022, 14, 2277. https://doi.org/10.3390/cancers14092277
Nunnelee J, Cottini F, Zhao Q, Faisal MS, Elder P, Rosko A, Bumma N, Khan A, Devarakonda S, Benson DM, et al. Improvement in Post-Autologous Stem Cell Transplant Survival of Multiple Myeloma Patients: A Long-Term Institutional Experience. Cancers. 2022; 14(9):2277. https://doi.org/10.3390/cancers14092277
Chicago/Turabian StyleNunnelee, Jordan, Francesca Cottini, Qiuhong Zhao, Muhammad Salman Faisal, Patrick Elder, Ashley Rosko, Naresh Bumma, Abdullah Khan, Srinivas Devarakonda, Don M. Benson, and et al. 2022. "Improvement in Post-Autologous Stem Cell Transplant Survival of Multiple Myeloma Patients: A Long-Term Institutional Experience" Cancers 14, no. 9: 2277. https://doi.org/10.3390/cancers14092277
APA StyleNunnelee, J., Cottini, F., Zhao, Q., Faisal, M. S., Elder, P., Rosko, A., Bumma, N., Khan, A., Devarakonda, S., Benson, D. M., Efebera, Y., & Sharma, N. (2022). Improvement in Post-Autologous Stem Cell Transplant Survival of Multiple Myeloma Patients: A Long-Term Institutional Experience. Cancers, 14(9), 2277. https://doi.org/10.3390/cancers14092277