
P-glycoprotein Mediates Resistance to the Anaplastic Lymphoma Kinase Inhibitor Ensartinib in Cancer Cells

 ,
,  , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Chemicals and Reagents
2.2. Cell Culture
2.3. Cytotoxicity Assays
2.4. Western Blots
2.5. Fluorescent Calcein and Pheophorbide A Accumulation Assay
2.6. Ultra-Performance Liquid Chromatography (UPLC)-Selected Reaction Monitoring Mass Spectrometry (SRM/MS)-Based Drug Accumulation Assay
2.7. Apoptosis Assays
2.8. Docking of Ensartinib in the Substrate-Binding Pocket of P-gp
2.9. Data Analysis
3. Results
3.1. P-gp Confers Resistance to Ensartinib
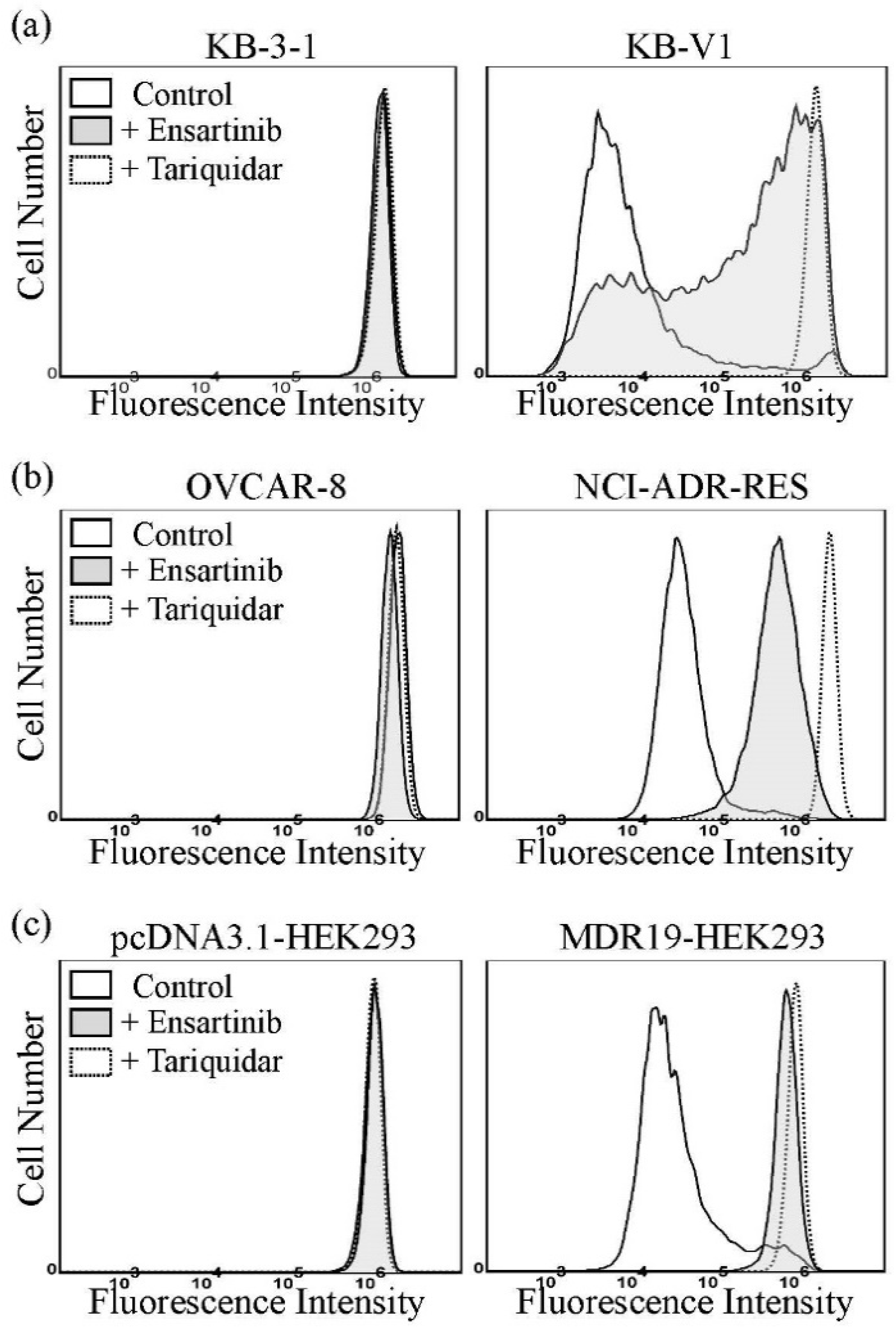
3.2. Ensartinib Attenuates the Drug Efflux Function of P-gp
3.3. P-gp Reduces the Intracellular Accumulation of Ensartinib in Human Cancer Cells
3.4. Docking of Ensartinib in the Drug-Binding Pocket of P-gp
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cameron, L.B.; Hitchen, N.; Chandran, E.; Morris, T.; Manser, R.; Solomon, B.J.; Jordan, V. Targeted therapy for advanced anaplastic lymphoma kinase (ALK)-rearranged non-small cell lung cancer. Cochrane Database Syst. Rev. 2022, 1, CD013453. [Google Scholar] [CrossRef] [PubMed]
- Lovly, C.M.; Heuckmann, J.M.; de Stanchina, E.; Chen, H.; Thomas, R.K.; Liang, C.; Pao, W. Insights into ALK-driven cancers revealed through development of novel ALK tyrosine kinase inhibitors. Cancer Res. 2011, 71, 4920–4931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caccese, M.; Ferrara, R.; Pilotto, S.; Carbognin, L.; Grizzi, G.; Calio, A.; Brunelli, M.; Cuppone, F.; Petraglia, S.; Scarpa, A.; et al. Current and developing therapies for the treatment of non-small cell lung cancer with ALK abnormalities: Update and perspectives for clinical practice. Expert Opin. Pharmacother. 2016, 17, 2253–2266. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Fong, T.; Xia, Z.; Zhang, J.; Luo, P. The efficacy and safety of ALK inhibitors in the treatment of ALK-positive non-small cell lung cancer: A network meta-analysis. Cancer Med. 2018, 7, 4993–5005. [Google Scholar] [CrossRef] [PubMed]
- Horn, L.; Infante, J.R.; Reckamp, K.L.; Blumenschein, G.R.; Leal, T.A.; Waqar, S.N.; Gitlitz, B.J.; Sanborn, R.E.; Whisenant, J.G.; Du, L.; et al. Ensartinib (X-396) in ALK-Positive Non-Small Cell Lung Cancer: Results from a First-in-Human Phase I/II, Multicenter Study. Clin. Cancer Res. 2018, 24, 2771–2779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gottesman, M.M.; Fojo, T.; Bates, S.E. Multidrug resistance in cancer: Role of ATP-dependent transporters. Nat. Rev. Cancer 2002, 2, 48–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brozik, A.; Hegedus, C.; Erdei, Z.; Hegedus, T.; Ozvegy-Laczka, C.; Szakacs, G.; Sarkadi, B. Tyrosine kinase inhibitors as modulators of ATP binding cassette multidrug transporters: Substrates, chemosensitizers or inducers of acquired multidrug resistance? Expert Opin. Drug Metab. Toxicol. 2011, 7, 623–642. [Google Scholar] [CrossRef] [PubMed]
- Camidge, D.R.; Pao, W.; Sequist, L.V. Acquired resistance to TKIs in solid tumours: Learning from lung cancer. Nat. Rev. Clin. Oncol. 2014, 11, 473–481. [Google Scholar] [CrossRef]
- Noguchi, K.; Katayama, K.; Sugimoto, Y. Human ABC transporter ABCG2/BCRP expression in chemoresistance: Basic and clinical perspectives for molecular cancer therapeutics. Pharm. Pers. Med. 2014, 7, 53–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robey, R.W.; Pluchino, K.M.; Hall, M.D.; Fojo, A.T.; Bates, S.E.; Gottesman, M.M. Revisiting the role of ABC transporters in multidrug-resistant cancer. Nat. Rev. Cancer 2018, 18, 452–464. [Google Scholar] [CrossRef]
- Gillet, J.P.; Gottesman, M.M. Mechanisms of multidrug resistance in cancer. Methods Mol. Biol. 2010, 596, 47–76. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.P.; Hsieh, C.H.; Wu, Y.S. The emergence of drug transporter-mediated multidrug resistance to cancer chemotherapy. Mol. Pharm. 2011, 8, 1996–2011. [Google Scholar] [CrossRef] [PubMed]
- Ross, D.D.; Karp, J.E.; Chen, T.T.; Doyle, L.A. Expression of breast cancer resistance protein in blast cells from patients with acute leukemia. Blood 2000, 96, 365–368. [Google Scholar] [CrossRef] [PubMed]
- Steinbach, D.; Sell, W.; Voigt, A.; Hermann, J.; Zintl, F.; Sauerbrey, A. BCRP gene expression is associated with a poor response to remission induction therapy in childhood acute myeloid leukemia. Leukemia 2002, 16, 1443–1447. [Google Scholar] [CrossRef] [PubMed]
- Uggla, B.; Stahl, E.; Wagsater, D.; Paul, C.; Karlsson, M.G.; Sirsjo, A.; Tidefelt, U. BCRP mRNA expression v. clinical outcome in 40 adult AML patients. Leuk. Res. 2005, 29, 141–146. [Google Scholar] [CrossRef]
- Matthews, C.; Catherwood, M.A.; Larkin, A.M.; Clynes, M.; Morris, T.C.; Alexander, H.D. MDR-1, but not MDR-3 gene expression, is associated with unmutated IgVH genes and poor prognosis chromosomal aberrations in chronic lymphocytic leukemia. Leuk. Lymphoma 2006, 47, 2308–2313. [Google Scholar] [CrossRef]
- Turner, J.G.; Gump, J.L.; Zhang, C.; Cook, J.M.; Marchion, D.; Hazlehurst, L.; Munster, P.; Schell, M.J.; Dalton, W.S.; Sullivan, D.M. ABCG2 expression, function, and promoter methylation in human multiple myeloma. Blood 2006, 108, 3881–3889. [Google Scholar] [CrossRef]
- Kovalev, A.A.; Tsvetaeva, D.A.; Grudinskaja, T.V. Role of ABC-cassette transporters (MDR1, MRP1, BCRP) in the development of primary and acquired multiple drug resistance in patients with early and metastatic breast cancer. Exp. Oncol. 2013, 35, 287–290. [Google Scholar]
- Pilarski, L.M.; Belch, A.R. Intrinsic expression of the multidrug transporter, P-glycoprotein 170, in multiple myeloma: Implications for treatment. Leuk. Lymphoma 1995, 17, 367–374. [Google Scholar] [CrossRef]
- Pilarski, L.M.; Szczepek, A.J.; Belch, A.R. Deficient drug transporter function of bone marrow-localized and leukemic plasma cells in multiple myeloma. Blood 1997, 90, 3751–3759. [Google Scholar] [CrossRef]
- Schwarzenbach, H. Expression of MDR1/P-glycoprotein, the multidrug resistance protein MRP, and the lung-resistance protein LRP in multiple myeloma. Med. Oncol. 2002, 19, 87–104. [Google Scholar] [CrossRef]
- Nakagawa, Y.; Abe, S.; Kurata, M.; Hasegawa, M.; Yamamoto, K.; Inoue, M.; Takemura, T.; Suzuki, K.; Kitagawa, M. IAP family protein expression correlates with poor outcome of multiple myeloma patients in association with chemotherapy-induced overexpression of multidrug resistance genes. Am. J. Hematol. 2006, 81, 824–831. [Google Scholar] [CrossRef] [PubMed]
- Tsubaki, M.; Satou, T.; Itoh, T.; Imano, M.; Komai, M.; Nishinobo, M.; Yamashita, M.; Yanae, M.; Yamazoe, Y.; Nishida, S. Overexpression of MDR1 and survivin, and decreased Bim expression mediate multidrug-resistance in multiple myeloma cells. Leuk. Res. 2012, 36, 1315–1322. [Google Scholar] [CrossRef] [PubMed]
- Tsunoda, S.; Okumura, T.; Ito, T.; Kondo, K.; Ortiz, C.; Tanaka, E.; Watanabe, G.; Itami, A.; Sakai, Y.; Shimada, Y. ABCG2 expression is an independent unfavorable prognostic factor in esophageal squamous cell carcinoma. Oncology 2006, 71, 251–258. [Google Scholar] [CrossRef]
- Li, F.; Zeng, H.; Ying, K. The combination of stem cell markers CD133 and ABCG2 predicts relapse in stage I non-small cell lung carcinomas. Med. Oncol. 2011, 28, 1458–1462. [Google Scholar] [CrossRef]
- Hang, D.; Dong, H.C.; Ning, T.; Dong, B.; Hou, D.L.; Xu, W.G. Prognostic value of the stem cell markers CD133 and ABCG2 expression in esophageal squamous cell carcinoma. Dis. Esophagus 2012, 25, 638–644. [Google Scholar] [CrossRef]
- Breedveld, P.; Pluim, D.; Cipriani, G.; Wielinga, P.; van Tellingen, O.; Schinkel, A.H.; Schellens, J.H. The effect of Bcrp1 (Abcg2) on the in vivo pharmacokinetics and brain penetration of imatinib mesylate (Gleevec): Implications for the use of breast cancer resistance protein and P-glycoprotein inhibitors to enable the brain penetration of imatinib in patients. Cancer Res. 2005, 65, 2577–2582. [Google Scholar]
- Sarkadi, B.; Homolya, L.; Szakacs, G.; Varadi, A. Human multidrug resistance ABCB and ABCG transporters: Participation in a chemoimmunity defense system. Physiol. Rev. 2006, 86, 1179–1236. [Google Scholar] [CrossRef]
- Paez, J.G.; Janne, P.A.; Lee, J.C.; Tracy, S.; Greulich, H.; Gabriel, S.; Herman, P.; Kaye, F.J.; Lindeman, N.; Boggon, T.J.; et al. EGFR mutations in lung cancer: Correlation with clinical response to gefitinib therapy. Science 2004, 304, 1497–1500. [Google Scholar] [CrossRef] [Green Version]
- Shen, D.W.; Cardarelli, C.; Hwang, J.; Cornwell, M.; Richert, N.; Ishii, S.; Pastan, I.; Gottesman, M.M. Multiple drug-resistant human KB carcinoma cells independently selected for high-level resistance to colchicine, adriamycin, or vinblastine show changes in expression of specific proteins. J. Biol. Chem. 1986, 261, 7762–7770. [Google Scholar] [CrossRef]
- Roschke, A.V.; Tonon, G.; Gehlhaus, K.S.; McTyre, N.; Bussey, K.J.; Lababidi, S.; Scudiero, D.A.; Weinstein, J.N.; Kirsch, I.R. Karyotypic complexity of the NCI-60 drug-screening panel. Cancer Res. 2003, 63, 8634–8647. [Google Scholar] [PubMed]
- Robey, R.W.; Shukla, S.; Finley, E.M.; Oldham, R.K.; Barnett, D.; Ambudkar, S.V.; Fojo, T.; Bates, S.E. Inhibition of P-glycoprotein (ABCB1)- and multidrug resistance-associated protein 1 (ABCC1)-mediated transport by the orally administered inhibitor, CBT-1((R)). Biochem. Pharmacol. 2008, 75, 1302–1312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robey, R.W.; Honjo, Y.; Morisaki, K.; Nadjem, T.A.; Runge, S.; Risbood, M.; Poruchynsky, M.S.; Bates, S.E. Mutations at amino-acid 482 in the ABCG2 gene affect substrate and antagonist specificity. Br. J. Cancer 2003, 89, 1971–1978. [Google Scholar] [CrossRef] [PubMed]
- Henrich, C.J.; Robey, R.W.; Bokesch, H.R.; Bates, S.E.; Shukla, S.; Ambudkar, S.V.; Dean, M.; McMahon, J.B. New inhibitors of ABCG2 identified by high-throughput screening. Mol. Cancer Ther. 2007, 6, 3271–3278. [Google Scholar] [CrossRef] [Green Version]
- Miyake, K.; Mickley, L.; Litman, T.; Zhan, Z.; Robey, R.; Cristensen, B.; Brangi, M.; Greenberger, L.; Dean, M.; Fojo, T.; et al. Molecular cloning of cDNAs which are highly overexpressed in mitoxantrone-resistant cells: Demonstration of homology to ABC transport genes. Cancer Res. 1999, 59, 8–13. [Google Scholar]
- Shen, D.W.; Fojo, A.; Chin, J.E.; Roninson, I.B.; Richert, N.; Pastan, I.; Gottesman, M.M. Human multidrug-resistant cell lines: Increased mdr1 expression can precede gene amplification. Science 1986, 232, 643–645. [Google Scholar] [CrossRef]
- Wu, C.P.; Shukla, S.; Calcagno, A.M.; Hall, M.D.; Gottesman, M.M.; Ambudkar, S.V. Evidence for dual mode of action of a thiosemicarbazone, NSC73306: A potent substrate of the multidrug resistance linked ABCG2 transporter. Mol. Cancer Ther. 2007, 6, 3287–3296. [Google Scholar] [CrossRef] [Green Version]
- Henrich, C.J.; Bokesch, H.R.; Dean, M.; Bates, S.E.; Robey, R.W.; Goncharova, E.I.; Wilson, J.A.; McMahon, J.B. A high-throughput cell-based assay for inhibitors of ABCG2 activity. J. Biomol. Screen. 2006, 11, 176–183. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.P.; Hung, C.Y.; Lusvarghi, S.; Huang, Y.H.; Tseng, P.J.; Hung, T.H.; Yu, J.S.; Ambudkar, S.V. Overexpression of ABCB1 and ABCG2 contributes to reduced efficacy of the PI3K/mTOR inhibitor samotolisib (LY3023414) in cancer cell lines. Biochem. Pharmacol. 2020, 180, 114137. [Google Scholar] [CrossRef]
- Wu, C.P.; Hsiao, S.H.; Su, C.Y.; Luo, S.Y.; Li, Y.Q.; Huang, Y.H.; Hsieh, C.H.; Huang, C.W. Human ATP-Binding Cassette transporters ABCB1 and ABCG2 confer resistance to CUDC-101, a multi-acting inhibitor of histone deacetylase, epidermal growth factor receptor and human epidermal growth factor receptor 2. Biochem. Pharmacol. 2014, 92, 567–576. [Google Scholar] [CrossRef]
- Wu, C.P.; Hsieh, Y.J.; Murakami, M.; Vahedi, S.; Hsiao, S.H.; Yeh, N.; Chou, A.W.; Li, Y.Q.; Wu, Y.S.; Yu, J.S.; et al. Human ATP-binding cassette transporters ABCB1 and ABCG2 confer resistance to histone deacetylase 6 inhibitor ricolinostat (ACY-1215) in cancer cell lines. Biochem. Pharmacol. 2018, 155, 316–325. [Google Scholar] [CrossRef] [PubMed]
- Robey, R.W.; Steadman, K.; Polgar, O.; Morisaki, K.; Blayney, M.; Mistry, P.; Bates, S.E. Pheophorbide a is a specific probe for ABCG2 function and inhibition. Cancer Res. 2004, 64, 1242–1246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.P.; Hung, C.Y.; Lusvarghi, S.; Chang, Y.F.; Hsiao, S.H.; Huang, Y.H.; Hung, T.H.; Yu, J.S.; Ambudkar, S.V. Overexpression of Human ABCB1 and ABCG2 Reduces the Susceptibility of Cancer Cells to the Histone Deacetylase 6-Specific Inhibitor Citarinostat. Int. J. Mol. Sci. 2021, 22, 2592. [Google Scholar] [CrossRef] [PubMed]
- Anderson, H.A.; Maylock, C.A.; Williams, J.A.; Paweletz, C.P.; Shu, H.; Shacter, E. Serum-derived protein S binds to phosphatidylserine and stimulates the phagocytosis of apoptotic cells. Nat. Immunol. 2003, 4, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Alam, A.; Kowal, J.; Broude, E.; Roninson, I.; Locher, K.P. Structural insight into substrate and inhibitor discrimination by human P-glycoprotein. Science 2019, 363, 753–756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.P.; Murakami, M.; Wu, Y.S.; Chi, Y.C.; Hsiao, S.H.; Huang, Y.H.; Hung, T.H.; Ambudkar, S.V. Branebrutinib (BMS-986195), a Bruton’s Tyrosine Kinase Inhibitor, Resensitizes P-Glycoprotein-Overexpressing Multidrug-Resistant Cancer Cells to Chemotherapeutic Agents. Front. Cell Dev. Biol. 2021, 9, 699571. [Google Scholar] [CrossRef]
- Sanner, M.F.; Olson, A.J.; Spehner, J.C. Reduced surface: An efficient way to compute molecular surfaces. Biopolymers 1996, 38, 305–320. [Google Scholar] [CrossRef]
- Dai, C.L.; Tiwari, A.K.; Wu, C.P.; Su, X.D.; Wang, S.R.; Liu, D.G.; Ashby, C.R., Jr.; Huang, Y.; Robey, R.W.; Liang, Y.J.; et al. Lapatinib (Tykerb, GW572016) reverses multidrug resistance in cancer cells by inhibiting the activity of ATP-binding cassette subfamily B member 1 and G member 2. Cancer Res. 2008, 68, 7905–7914. [Google Scholar] [CrossRef] [Green Version]
- Sodani, K.; Tiwari, A.K.; Singh, S.; Patel, A.; Xiao, Z.J.; Chen, J.J.; Sun, Y.L.; Talele, T.T.; Chen, Z.S. GW583340 and GW2974, human EGFR and HER-2 inhibitors, reverse ABCG2- and ABCB1-mediated drug resistance. Biochem. Pharmacol. 2012, 83, 1613–1622. [Google Scholar] [CrossRef] [Green Version]
- Kuang, Y.H.; Patel, J.P.; Sodani, K.; Wu, C.P.; Liao, L.Q.; Patel, A.; Tiwari, A.K.; Dai, C.L.; Chen, X.; Fu, L.W.; et al. OSI-930 analogues as novel reversal agents for ABCG2-mediated multidrug resistance. Biochem. Pharmacol. 2012, 84, 766–774. [Google Scholar] [CrossRef] [Green Version]
- Hollo, Z.; Homolya, L.; Davis, C.W.; Sarkadi, B. Calcein accumulation as a fluorometric functional assay of the multidrug transporter. Biochim. Biophys. Acta 1994, 1191, 384–388. [Google Scholar] [CrossRef]
- Wu, C.P.; Lusvarghi, S.; Wang, J.C.; Hsiao, S.H.; Huang, Y.H.; Hung, T.H.; Ambudkar, S.V. Avapritinib: A Selective Inhibitor of KIT and PDGFRalpha that Reverses ABCB1 and ABCG2-Mediated Multidrug Resistance in Cancer Cell Lines. Mol. Pharm. 2019, 16, 3040–3052. [Google Scholar] [CrossRef] [PubMed]
- Kartner, N.; Riordan, J.R.; Ling, V. Cell surface P-glycoprotein associated with multidrug resistance in mammalian cell lines. Science 1983, 221, 1285–1288. [Google Scholar] [CrossRef] [PubMed]
- Bates, S.E.; Medina-Perez, W.Y.; Kohlhagen, G.; Antony, S.; Nadjem, T.; Robey, R.W.; Pommier, Y. ABCG2 mediates differential resistance to SN-38 (7-ethyl-10-hydroxycamptothecin) and homocamptothecins. J. Pharmacol. Exp. Ther. 2004, 310, 836–842. [Google Scholar] [CrossRef] [Green Version]
- Maliepaard, M.; van Gastelen, M.A.; de Jong, L.A.; Pluim, D.; van Waardenburg, R.C.; Ruevekamp-Helmers, M.C.; Floot, B.G.; Schellens, J.H. Overexpression of the BCRP/MXR/ABCP gene in a topotecan-selected ovarian tumor cell line. Cancer Res. 1999, 59, 4559–4563. [Google Scholar]
- Nosol, K.; Romane, K.; Irobalieva, R.N.; Alam, A.; Kowal, J.; Fujita, N.; Locher, K.P. Cryo-EM structures reveal distinct mechanisms of inhibition of the human multidrug transporter ABCB1. Proc. Natl. Acad. Sci. USA 2020, 117, 26245–26253. [Google Scholar] [CrossRef]
- Tian, X.; Gu, T.; Lee, M.H.; Dong, Z. Challenge and countermeasures for EGFR targeted therapy in non-small cell lung cancer. Biochim. Biophys Acta Rev Cancer 2021, 1877, 188645. [Google Scholar] [CrossRef]
- Agarwal, S.; Sane, R.; Gallardo, J.L.; Ohlfest, J.R.; Elmquist, W.F. Distribution of gefitinib to the brain is limited by P-glycoprotein (ABCB1) and breast cancer resistance protein (ABCG2)-mediated active efflux. J. Pharmacol. Exp. Ther. 2010, 334, 147–155. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.; Laramy, J.K.; Mohammad, A.S.; Talele, S.; Fisher, J.; Sarkaria, J.N.; Elmquist, W.F. Brain Distribution of a Panel of Epidermal Growth Factor Receptor Inhibitors Using Cassette Dosing in Wild-Type and Abcb1/Abcg2-Deficient Mice. Drug Metab. Dispos. 2019, 47, 393–404. [Google Scholar] [CrossRef] [Green Version]
- van Hoppe, S.; Jamalpoor, A.; Rood, J.J.M.; Wagenaar, E.; Sparidans, R.W.; Beijnen, J.H.; Schinkel, A.H. Brain accumulation of osimertinib and its active metabolite AZ5104 is restricted by ABCB1 (P-glycoprotein) and ABCG2 (breast cancer resistance protein). Pharmacol. Res. 2019, 146, 104297. [Google Scholar] [CrossRef]
- Wang, T.; Agarwal, S.; Elmquist, W.F. Brain distribution of cediranib is limited by active efflux at the blood-brain barrier. J Pharmacol. Exp. Ther. 2012, 341, 386–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mittapalli, R.K.; Vaidhyanathan, S.; Sane, R.; Elmquist, W.F. Impact of P-glycoprotein (ABCB1) and breast cancer resistance protein (ABCG2) on the brain distribution of a novel BRAF inhibitor: Vemurafenib (PLX4032). J. Pharmacol. Exp. Ther. 2012, 342, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.P.; Sim, H.M.; Huang, Y.H.; Liu, Y.C.; Hsiao, S.H.; Cheng, H.W.; Li, Y.Q.; Ambudkar, S.V.; Hsu, S.C. Overexpression of ATP-binding cassette transporter ABCG2 as a potential mechanism of acquired resistance to vemurafenib in BRAF(V600E) mutant cancer cells. Biochem. Pharmacol. 2013, 85, 325–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Gan, C.; Sparidans, R.W.; Wagenaar, E.; van Hoppe, S.; Beijnen, J.H.; Schinkel, A.H. P-glycoprotein (MDR1/ABCB1) and Breast Cancer Resistance Protein (BCRP/ABCG2) affect brain accumulation and intestinal disposition of encorafenib in mice. Pharmacol. Res. 2018, 129, 414–423. [Google Scholar] [CrossRef]
- Gampa, G.; Kim, M.; Mohammad, A.S.; Parrish, K.E.; Mladek, A.C.; Sarkaria, J.N.; Elmquist, W.F. Brain Distribution and Active Efflux of Three panRAF Inhibitors: Considerations in the Treatment of Melanoma Brain Metastases. J. Pharmacol. Exp. Ther. 2019, 368, 446–461. [Google Scholar] [CrossRef] [Green Version]
- Parrish, K.E.; Cen, L.; Murray, J.; Calligaris, D.; Kizilbash, S.; Mittapalli, R.K.; Carlson, B.L.; Schroeder, M.A.; Sludden, J.; Boddy, A.V.; et al. Efficacy of PARP Inhibitor Rucaparib in Orthotopic Glioblastoma Xenografts Is Limited by Ineffective Drug Penetration into the Central Nervous System. Mol. Cancer. Ther. 2015, 14, 2735–2743. [Google Scholar] [CrossRef] [Green Version]
- Durmus, S.; Sparidans, R.W.; van Esch, A.; Wagenaar, E.; Beijnen, J.H.; Schinkel, A.H. Breast cancer resistance protein (BCRP/ABCG2) and P-glycoprotein (P-GP/ABCB1) restrict oral availability and brain accumulation of the PARP inhibitor rucaparib (AG-014699). Pharm. Res. 2015, 32, 37–46. [Google Scholar] [CrossRef]
- de Gooijer, M.C.; Buil, L.C.M.; Citirikkaya, C.H.; Hermans, J.; Beijnen, J.H.; van Tellingen, O. ABCB1 Attenuates the Brain Penetration of the PARP Inhibitor AZD2461. Mol. Pharm. 2018, 15, 5236–5243. [Google Scholar] [CrossRef]
- Tang, S.C.; Nguyen, L.N.; Sparidans, R.W.; Wagenaar, E.; Beijnen, J.H.; Schinkel, A.H. Increased oral availability and brain accumulation of the ALK inhibitor crizotinib by coadministration of the P-glycoprotein (ABCB1) and breast cancer resistance protein (ABCG2) inhibitor elacridar. Int. J. Cancer 2014, 134, 1484–1494. [Google Scholar] [CrossRef]
- Kort, A.; Sparidans, R.W.; Wagenaar, E.; Beijnen, J.H.; Schinkel, A.H. Brain accumulation of the EML4-ALK inhibitor ceritinib is restricted by P-glycoprotein (P-GP/ABCB1) and breast cancer resistance protein (BCRP/ABCG2). Pharmacol. Res. 2015, 102, 200–207. [Google Scholar] [CrossRef]
- Katayama, R.; Sakashita, T.; Yanagitani, N.; Ninomiya, H.; Horiike, A.; Friboulet, L.; Gainor, J.F.; Motoi, N.; Dobashi, A.; Sakata, S.; et al. P-glycoprotein Mediates Ceritinib Resistance in Anaplastic Lymphoma Kinase-rearranged Non-small Cell Lung Cancer. EBioMedicine 2016, 3, 54–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, W.; Sparidans, R.W.; Wang, Y.; Lebre, M.C.; Beijnen, J.H.; Schinkel, A.H. P-glycoprotein and breast cancer resistance protein restrict brigatinib brain accumulation and toxicity, and, alongside CYP3A, limit its oral availability. Pharmacol. Res. 2018, 137, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Di Paolo, D.; Yang, D.; Pastorino, F.; Emionite, L.; Cilli, M.; Daga, A.; Destafanis, E.; Di Fiore, A.; Piaggio, F.; Brignole, C.; et al. New therapeutic strategies in neuroblastoma: Combined targeting of a novel tyrosine kinase inhibitor and liposomal siRNAs against ALK. Oncotarget 2015, 6, 28774–28789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, J.Y.; Ong, R.C.; Suen, Y.K.; Ooi, V.; Wong, H.N.; Mak, T.C.; Fung, K.P.; Yu, B.; Kong, S.K. Polyphyllin D is a potent apoptosis inducer in drug-resistant HepG2 cells. Cancer Lett. 2005, 217, 203–211. [Google Scholar] [CrossRef]
- Manov, I.; Bashenko, Y.; Eliaz-Wolkowicz, A.; Mizrahi, M.; Liran, O.; Iancu, T.C. High-dose acetaminophen inhibits the lethal effect of doxorubicin in HepG2 cells: The role of P-glycoprotein and mitogen-activated protein kinase p44/42 pathway. J Pharmacol. Exp. Ther. 2007, 322, 1013–1022. [Google Scholar] [CrossRef]
- Liu, H.; Wang, M.; Liang, N.; Guan, L. PDCD2 sensitizes HepG2 cells to sorafenib by suppressing epithelialmesenchymal transition. Mol. Med. Rep. 2019, 19, 2173–2179. [Google Scholar] [CrossRef] [Green Version]
- Vagiannis, D.; Novotna, E.; Skarka, A.; Kammerer, S.; Kupper, J.H.; Chen, S.; Guo, L.; Staud, F.; Hofman, J. Ensartinib (X-396) Effectively Modulates Pharmacokinetic Resistance Mediated by ABCB1 and ABCG2 Drug Efflux Transporters and CYP3A4 Biotransformation Enzyme. Cancers 2020, 12, 813. [Google Scholar] [CrossRef] [Green Version]
- Gillet, J.P.; Wang, J.; Calcagno, A.M.; Green, L.J.; Varma, S.; Bunkholt Elstrand, M.; Trope, C.G.; Ambudkar, S.V.; Davidson, B.; Gottesman, M.M. Clinical relevance of multidrug resistance gene expression in ovarian serous carcinoma effusions. Mol. Pharm. 2011, 8, 2080–2088. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cell Line | Type | Transporter Expressed | IC50 ± SD [μM] 1 | |
|---|---|---|---|---|
| Ensartinib | Ensartinib + Tariquidar | |||
| KB-3-1 | Epidermal cancer | - | 0.92 ± 0.19 | 0.77 ± 0.14 |
| KB-V1 | Epidermal cancer | P-gp | 5.86 ± 1.17 ** | 0.88 ± 0.14 ** |
| OVCAR-8 | Ovarian cancer | - | 3.00 ± 0.57 | 3.01 ± 0.59 |
| NCI-ADR-RES | Ovarian cancer | P-gp | 9.20 ± 2.42 * | 5.57 ± 0.93 * |
| S1 | Colon cancer | - | 2.84 ± 0.33 | NA |
| S1-MI-80 | Colon cancer | ABCG2 | 3.69 ± 0.63 | NA |
| NCI-H460 | NSCLC | - | 1.75 ± 0.41 | NA |
| H460-MX20 | NSCLC | ABCG2 | 2.45 ± 0.51 | NA |
| pcDNA3.1-HEK293 | - | - | 1.30 ± 0.14 | 1.12 ± 0.09 |
| MDR19-HEK293 | - | P-gp | 4.42 ± 0.66 ** | 1.94 ± 0.23 ** |
| R482-HEK293 | - | ABCG2 | 1.80 ± 0.28 | NA |
| Compounds | Concentration (nM) | IC50 1 ± SD and (FR 2) | |
|---|---|---|---|
| KB-3-1 (Parental) [nM] | KB-V1 (ABCB1) [μM] | ||
| Paclitaxel | - | 2.45 ± 0.55 (1.0) | 7.08 ± 1.17 (1.0) |
| + ensartinib | 500 | 2.90 ± 0.70 (0.8) | 7.18 ± 1.19 (1.0) |
| + tariquidar | 1000 | 3.01 ± 0.80 (0.8) | 2.41 ± 0.61 [nM] *** (2938) |
| Vincristine | - | 2.18 ± 0.48 (1.0) | 3.25 ± 0.46 (1.0) |
| + ensartinib | 500 | 2.94 ± 0.62 (0.7) | 3.43 ± 0.29 (0.9) |
| + tariquidar | 1000 | 1.76 ± 0.40 (1.2) | 4.00 ± 0.81 [nM] *** (813) |
| Colchicine | - | 15.87 ± 5.22 (1.0) | 1.04 ± 0.05 (1.0) |
| + ensartinib | 500 | 19.85 ± 6.47 (0.8) | 1.38 ± 0.26 (0.8) |
| + tariquidar | 1000 | 14.65 ± 4.87 (1.1) | 16.31 ± 4.19 [nM] *** (64) |
| OVCAR-8 (Parental) [nM] | NCI-ADR-RES (ABCB1) [μM] | ||
| Paclitaxel | - | 5.10 ± 1.10 (1.0) | 9.81 ± 1.79 (1.0) |
| + ensartinib | 500 | 4.32 ± 0.95 (1.2) | 10.03 ± 1.71 (1.0) |
| + tariquidar | 1000 | 4.30 ± 1.04 (1.2) | 7.67 ± 0.73 [nM] *** (1279) |
| Vincristine | - | 9.38 ± 1.41 (1.0) | 5.74 ± 0.88 (1.0) |
| + ensartinib | 500 | 7.53 ± 1.17 (1.2) | 5.79 ± 0.82 (1.0) |
| + tariquidar | 1000 | 6.74 ± 1.21 (1.4) | 28.56 ± 3.24 [nM] *** (201) |
| Colchicine | - | 26.32 ± 7.57 (1.0) | 2.14 ± 0.45 (1.0) |
| + ensartinib | 500 | 28.26 ± 8.94 (0.9) | 2.33 ± 0.48 (0.9) |
| + tariquidar | 1000 | 24.07 ± 7.29 (1.1) | 45.70 ± 13.54 [nM] ** (47) |
| pcDNA3.1-HEK293 (Parental) [nM] | MDR19-HEK293 (ABCB1) [nM] | ||
| Paclitaxel | - | 2.10 ± 0.36 (1.0) | 1583.40 ± 212.71 (1.0) |
| + ensartinib | 500 | 1.73 ± 0.40 (1.2) | 1385.32 ± 174.42 (1.1) |
| + tariquidar | 1000 | 2.28 ± 0.42 (0.9) | 3.49 ± 0.61 *** (453.70) |
| Vincristine | - | 2.75 ± 0.25 (1.0) | 794.92 ± 123.55 (1.0) |
| + ensartinib | 500 | 3.33 ± 0.47 (0.8) | 769.60 ± 159.32 (1.0) |
| + tariquidar | 1000 | 2.89 ± 0.44 (1.0) | 1.44 ± 0.29 ** (552.03) |
| Colchicine | - | 12.76 ± 3.28 (1.0) | 195.23 ± 36.89 (1.0) |
| + ensartinib | 500 | 14.54 ± 2.94 (0.9) | 235.53 ± 66.08 (0.8) |
| + tariquidar | 1000 | 12.66 ± 2.98 (1.0) | 7.69 ± 1.44 *** (25.39) |
| Compounds | Concentration (nM) | IC50 1 ± SD and (FR 2) | |
|---|---|---|---|
| S1 (parental) [nM] | S1-MI-80 (ABCG2) [μM] | ||
| Mitoxantrone | - | 9.52 ± 2.63 (1.0) | 31.41 ± 6.49 (1.0) |
| + ensartinib | 500 | 7.08 ± 2.20 (1.3) | 27.51 ± 5.32 (1.1) |
| + Ko143 | 1000 | 7.52 ± 2.11 (1.3) | 0.94 ± 0.15 ** (33.4) |
| [nM] | [μM] | ||
| Topotecan | - | 57.09 ± 10.95 (1.0) | 33.20 ± 3.08 (1.0) |
| + ensartinib | 500 | 58.00 ± 9.59 (1.0) | 27.19 ± 3.25 (1.2) |
| + Ko143 | 1000 | 60.77 ± 11.40 (0.9) | 1.69 ± 0.32 *** (19.6) |
| [nM] | [μM] | ||
| SN-38 | - | 13.02 ± 2.67 (1.0) | 5.45 ± 1.25 (1.0) |
| + ensartinib | 500 | 11.97 ± 2.26 (1.1) | 9.04 ± 1.93 (0.6) |
| + Ko143 | 1000 | 12.56 ± 2.74 (1.0) | 0.12 ± 0.04 * (45.4) |
| NCI-H460 (parental) [nM] | H460-MX20 (ABCG2) [μM] | ||
| Mitoxantrone | - | 70.76 ± 10.55 (1.0) | 1.07 ± 0.15 (1.0) |
| + ensartinib | 500 | 50.67 ± 10.42 (1.4) | 0.94 ± 0.19 (1.1) |
| + Ko143 | 1000 | 35.22 ± 7.44 ** (2.0) | 0.12 ± 0.03 *** (8.9) |
| [nM] | [nM] | ||
| Topotecan | - | 105.58 ± 12.64 (1.0) | 799.88 ± 173.21 (1.0) |
| + ensartinib | 500 | 111.29 ± 17.03 (0.9) | 775.68 ± 146.16 (1.0) |
| + Ko143 | 1000 | 46.63 ± 6.32 ** (2.3) | 39.09 ± 10.01 ** (20.5) |
| [nM] | [nM] | ||
| SN-38 | - | 28.66 ± 3.10 (1.0) | 273.60 ± 52.10 (1.0) |
| + ensartinib | 500 | 27.42 ± 2.86 (1.0) | 247.83 ± 31.09 (1.1) |
| + Ko143 | 1000 | 8.27 ± 1.76 *** (3.5) | 4.23 ± 1.25 *** (64.7) |
| pcDNA3.1-HEK293 (parental) [μM] | R482-HEK293 (ABCG2) [μM] | ||
| Mitoxantrone | - | 4.99 ± 0.61 (1.0) | 114.63 ± 13.10 (1.0) |
| + ensartinib | 500 | 4.65 ± 0.40 (1.1) | 126.89 ± 11.12 (0.9) |
| + Ko143 | 1000 | 4.54 ± 0.46 (1.1) | 9.47 ± 0.86 *** (12.1) |
| [nM] | [nM] | ||
| Topotecan | - | 31.45 ± 5.00 (1.0) | 669.76 ± 77.52 (1.0) |
| + ensartinib | 500 | 29.76 ± 5.52 (1.1) | 810.79 ± 94.79 (0.8) |
| + Ko143 | 1000 | 33.30 ± 6.35 (0.9) | 144.57 ± 27.46 *** (4.6) |
| [nM] | [nM] | ||
| SN-38 | - | 4.06 ± 0.76 (1.0) | 322.50 ± 33.86 (1.0) |
| + ensartinib | 500 | 3.94 ± 0.89 (1.0) | 351.15 ± 41.89 (0.9) |
| + Ko143 | 1000 | 4.00 ± 0.76 (1.0) | 15.48 ± 3.51 *** (20.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, C.-P.; Hung, C.-Y.; Murakami, M.; Wu, Y.-S.; Lin, C.-L.; Huang, Y.-H.; Hung, T.-H.; Yu, J.-S.; Ambudkar, S.V. P-glycoprotein Mediates Resistance to the Anaplastic Lymphoma Kinase Inhibitor Ensartinib in Cancer Cells. Cancers 2022, 14, 2341. https://doi.org/10.3390/cancers14092341
Wu C-P, Hung C-Y, Murakami M, Wu Y-S, Lin C-L, Huang Y-H, Hung T-H, Yu J-S, Ambudkar SV. P-glycoprotein Mediates Resistance to the Anaplastic Lymphoma Kinase Inhibitor Ensartinib in Cancer Cells. Cancers. 2022; 14(9):2341. https://doi.org/10.3390/cancers14092341
Chicago/Turabian StyleWu, Chung-Pu, Cheng-Yu Hung, Megumi Murakami, Yu-Shan Wu, Chun-Ling Lin, Yang-Hui Huang, Tai-Ho Hung, Jau-Song Yu, and Suresh V. Ambudkar. 2022. "P-glycoprotein Mediates Resistance to the Anaplastic Lymphoma Kinase Inhibitor Ensartinib in Cancer Cells" Cancers 14, no. 9: 2341. https://doi.org/10.3390/cancers14092341
APA StyleWu, C.-P., Hung, C.-Y., Murakami, M., Wu, Y.-S., Lin, C.-L., Huang, Y.-H., Hung, T.-H., Yu, J.-S., & Ambudkar, S. V. (2022). P-glycoprotein Mediates Resistance to the Anaplastic Lymphoma Kinase Inhibitor Ensartinib in Cancer Cells. Cancers, 14(9), 2341. https://doi.org/10.3390/cancers14092341