
Ablative vs. Non-Ablative Radiotherapy in Palliating Locally Advanced Pancreatic Cancer: A Single Institution Experience and a Systematic Review of the Literature


Abstract
:Simple Summary
Abstract
1. Introduction
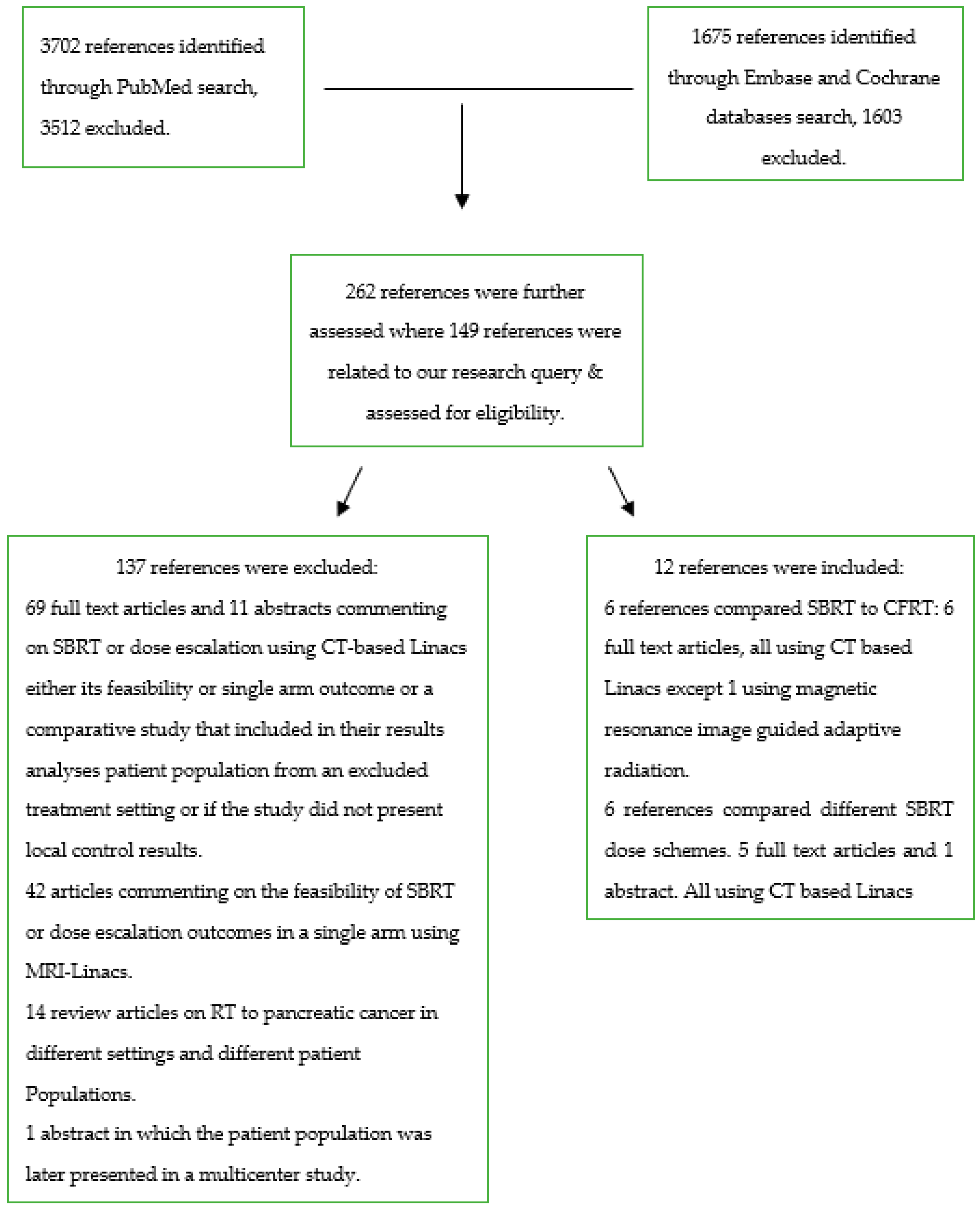
2. Materials and Methods
3. Results
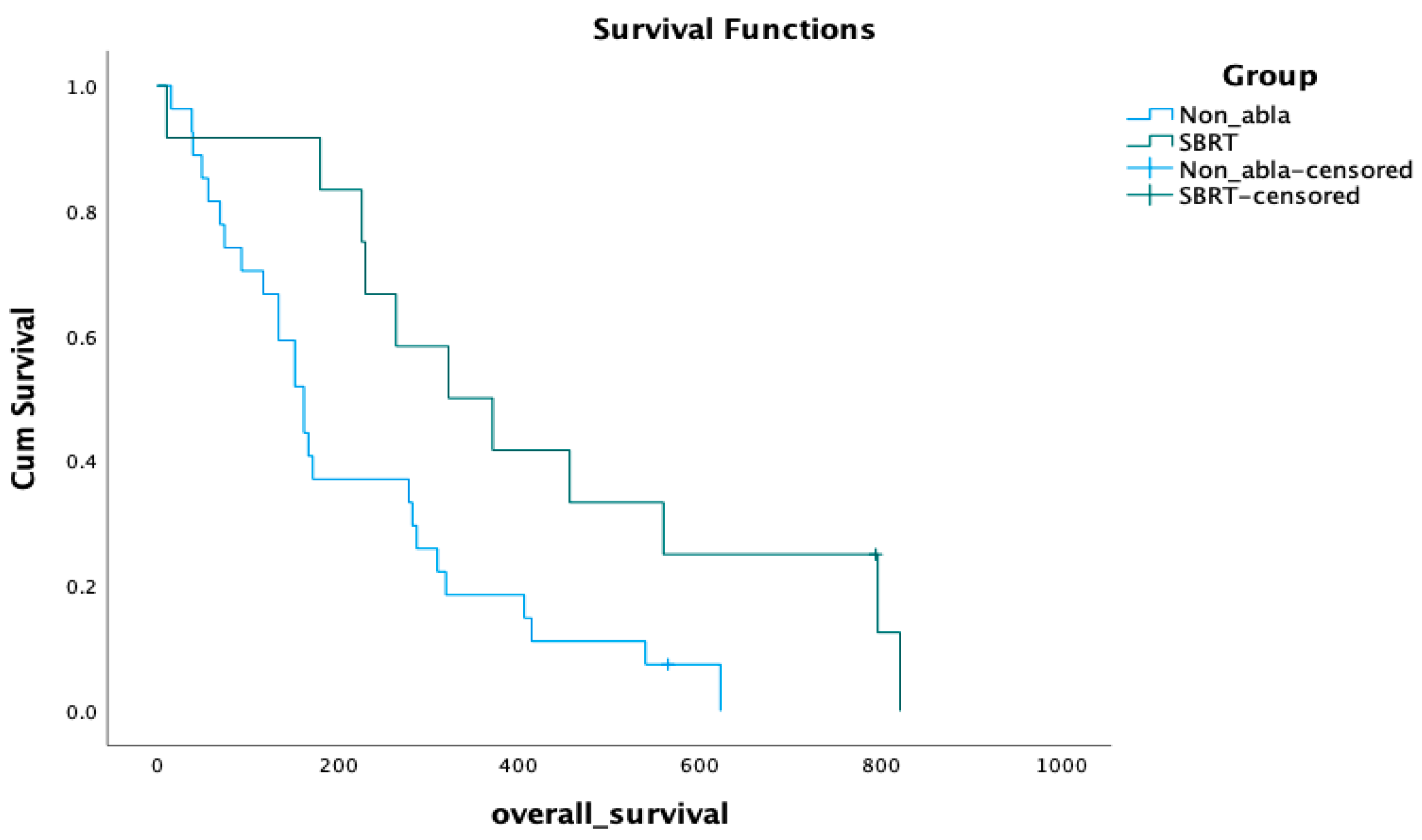
3.1. Overall Survival
3.2. Subgroup Analysis
3.3. Local Progression
3.4. Systematic Review Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Balaban, E.P.; Mangu, P.B.; Khorana, A.A.; Shah, M.A.; Mukherjee, S.; Crane, C.H.; Javle, M.M.; Eads, J.R.; Allen, P.; Ko, A.H.; et al. Locally Advanced, Unresectable Pancreatic Cancer: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2016, 34, 2654–2668. [Google Scholar] [CrossRef] [PubMed]
- Tonneau, M.; Lacornerie, T.; Mirabel, X.; Pasquier, D. Stereotactic body radiotherapy for locally advanced pancreatic cancer: A systemic review. Cancer Radiother. 2021, 25, 283–295. [Google Scholar] [CrossRef] [PubMed]
- Moningi, S.; Lei, X.; Fang, P.; Taniguchi, C.M.; Holliday, E.B.; Koay, E.J.; Koong, A.C.; Ludmir, E.B.; Minsky, B.D.; Das, P.; et al. Contemporary use and outcomes of radiation and chemotherapy for unresectable pancreatic cancer. Clin. Transl. Radiat. Oncol. 2022, 35, 9–16. [Google Scholar] [CrossRef]
- NCCN Guidelines v1. 2022. Available online: www.nccn.org (accessed on 1 September 2022).
- Palta, M.; Godfrey, D.; Goodman, K.A.; Hoffe, S.; Dawson, L.A.; Dessert, D.; Hall, W.A.; Herman, J.M.; Khorana, A.A.; Merchant, N.; et al. Radiation Therapy for Pancreatic Cancer: Executive Summary of an ASTRO Clinical Practice Guideline. Pract. Radiat. Oncol. 2019, 9, 322–332. [Google Scholar] [CrossRef] [PubMed]
- Koong, A.C.; Christofferson, E.; Le, Q.-T.; Goodman, K.A.; Ho, A.; Kuo, T.; Ford, J.M.; Fisher, G.A.; Greco, R.; Norton, J.; et al. Phase II study to assess the efficacy of conventionally fractionated radiotherapy followed by a stereotactic radiosurgery boost in patients with locally advanced pancreatic cancer. Int. J. Radiat. Oncol. 2005, 63, 320–323. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Pollom, E.L.; Alagappan, M.; von Eyben, R.; Kunz, P.L.; Fisher, G.A.; Ford, J.A.; Poultsides, G.A.; Visser, B.C.; Norton, J.A.; Kamaya, A.; et al. Single-versus multifraction stereotactic body radiation therapy for pancreatic adenocarcinoma: Outcomes and toxicity. Int. J. Radiat. Oncol. 2014, 90, 918–925. [Google Scholar] [CrossRef]
- Toesca, D.A.; Ahmed, F.; Kashyap, M.; Baclay, J.R.M.; von Eyben, R.; Pollom, E.L.; Koong, A.C.; Chang, D.T. Intensified systemic therapy and stereotactic ablative radiotherapy dose for patients with unresectable pancreatic adenocarcinoma. Radiother. Oncol. 2020, 152, 63–69. [Google Scholar] [CrossRef]
- Zhu, X.; Cao, Y.; Su, T.; Zhu, X.; Ju, X.; Zhao, X.; Jiang, L.; Ye, Y.; Cao, F.; Qing, S.; et al. Failure patterns and outcomes of dose escalation of stereotactic body radiotherapy for locally advanced pancreatic cancer: A multicenter cohort study. Ther. Adv. Med Oncol. 2020, 12, 1758835920977155. [Google Scholar] [CrossRef]
- Jaoude, J.A.; Niedzielski, J.; Yu, S.; Taniguchi, C. Dose Escalation SBRT in Patients with Localized Pancreatic Cancer. Int. J. Radiat. Oncol. 2022, 114, e188. [Google Scholar] [CrossRef]
- Mazzola, R.; Fersino, S.; Aiello, D.; Gregucci, F.; Tebano, U.; Corradini, S.; Di Paola, G.; Cirillo, M.; Tondulli, L.; Ruffo, G.; et al. Linac-based stereotactic body radiation therapy for unresectable locally advanced pancreatic cancer: Risk-adapted dose prescription and image-guided delivery. Strahlenther. Onkol. 2018, 194, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Arcelli, A.; Guido, A.; Buwenge, M.; Simoni, N.; Mazzarotto, R.; Macchia, G.; Deodato, F.; Cilla, S.; Bonomo, P.; Scotti, V.; et al. Higher Biologically Effective Dose Predicts Survival in SBRT of Pancreatic Cancer: A Multicentric Analysis (PAULA-1). Anticancer Res. 2020, 40, 465–472. [Google Scholar] [CrossRef]
- Rudra, S.; Jiang, N.; Rosenberg, S.A.; Olsen, J.R.; Roach, M.; Wan, L.; Portelance, L.; Mellon, E.A.; Bruynzeel, A.; Lagerwaard, F.; et al. Using adaptive magnetic resonance image-guided radiation therapy for treatment of inoperable pancreatic cancer. Cancer Med. 2019, 8, 2123–2132. [Google Scholar] [CrossRef] [PubMed]
- Arcelli, A.; Buwenge, M.; Macchia, G.; Bertini, F.; Guido, A.; Deodato, F.; Cilla, S.; Scotti, V.; Rosetto, M.E.; Djan, I.; et al. Stereotactic body radiotherapy vs conventionally fractionated chemoradiation in locally advanced pancreatic cancer: A multicenter case-control study (PAULA-1). Cancer Med. 2020, 9, 7879–7887. [Google Scholar] [CrossRef] [PubMed]
- Shin, Y.S.; Park, H.H.; Park, J.-H.; Seo, D.-W.; Lee, S.S.; Yoo, C.; Kim, S.; Yoon, S.M.; Jung, J.; Kim, M.-H.; et al. Stereotactic Body Radiation Therapy versus Concurrent Chemoradiotherapy for Locally Advanced Pancreatic Cancer: A Propensity Score-Matched Analysis. Cancers 2022, 14, 1166. [Google Scholar] [CrossRef]
- Park, J.J.; Hajj, C.; Reyngold, M.; Shi, W.; Zhang, Z.; Cuaron, J.J.; Crane, C.H.; O’reilly, E.M.; Lowery, M.A.; Yu, K.H.; et al. Stereotactic body radiation vs. intensity-modulated radiation for unresectable pancreatic cancer. Acta Oncol. 2017, 56, 1746–1753. [Google Scholar] [CrossRef]
- Lin, J.-C.; Jen, Y.-M.; Li, M.-H.; Chao, H.-L.; Tsai, J.-T. Comparing outcomes of stereotactic body radiotherapy with intensity-modulated radiotherapy for patients with locally advanced unresectable pancreatic cancer. Eur. J. Gastroenterol. Hepatol. 2015, 27, 259–264. [Google Scholar] [CrossRef]
- Jaoude, J.A.; Thunshelle, C.P.; Kouzy, R.; Nguyen, N.D.; Lin, D.; Prakash, L.; Bumanlag, I.M.; Noticewala, S.S.; Niedzielski, J.S.; Beddar, S.; et al. Stereotactic Versus Conventional Radiation Therapy for Patients with Pancreatic Cancer in the Modern Era. Adv. Radiat. Oncol. 2021, 6, 100763. [Google Scholar] [CrossRef]
- Petrelli, F.; Comito, T.; Ghidini, A.; Torri, V.; Scorsetti, M.; Barni, S. Stereotactic Body Radiation Therapy for Locally Advanced Pancreatic Cancer: A Systematic Review and Pooled Analysis of 19 Trials. Int. J. Radiat. Oncol. 2017, 97, 313–322. [Google Scholar] [CrossRef]
- Vornhülz, M.; Anton, S.; Eross, B.; Szakács, Z.; Hegyi, P.; Regel, I.; Belka, C.; Niyazi, M.; Mayerle, J.; Beyer, G. Role of stereotactic body radiation in the enhancement of the quality of life in locally advanced pancreatic adenocarcinoma: A systematic review. Radiat. Oncol. 2022, 17, 108. [Google Scholar] [CrossRef]
- Buwenge, M.; Arcelli, A.; Cellini, F.; Deodato, F.; Macchia, G.; Cilla, S.; Galietta, E.; Strigari, L.; Malizia, C.; Cammelli, S.; et al. Pain Relief after Stereotactic Radiotherapy of Pancreatic Adenocarcinoma: An Updated Systematic Review. Curr. Oncol. 2022, 29, 2616–2629. [Google Scholar] [CrossRef] [PubMed]
- Rosati, L.M.; Herman, J.M. Role of Stereotactic Body Radiotherapy in the Treatment of Elderly and Poor Performance Status Patients With Pancreatic Cancer. J. Oncol. Pract. 2017, 13, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Ciabatti, S.; Cammelli, S.; Frakulli, R.; Arcelli, A.; Macchia, G.; Deodato, F.; Cilla, S.; Giaccherini, L.; Buwenge, M.; Morganti, A.G. Radiotherapy of pancreatic cancer in older patients: A systematic review. J. Geriatr. Oncol. 2019, 10, 534–539. [Google Scholar] [CrossRef] [PubMed]
- de Geus, S.W.L.; Eskander, M.F.; Kasumova, G.G.; Ng, S.C.; Kent, T.S.; Mancias, J.D.; Callery, M.P.; Mahadevan, A.; Tseng, J.F. Stereotactic body radiotherapy for unresected pancreatic cancer: A nationwide review. Cancer 2017, 123, 4158–4167. [Google Scholar] [CrossRef]
- Dohopolski, M.J.; Glaser, S.M.; Vargo, J.A.; Balasubramani, G.K.; Beriwal, S. Stereotactic body radiotherapy for locally-advanced unresectable pancreatic cancer-patterns of care and overall survival. J. Gastrointest. Oncol. 2017, 8, 766–777. [Google Scholar] [CrossRef]
- Ma, S.J.; Serra, L.M.; Bartl, A.J.; Han, H.R.; Fekrmandi, F.; Iovoli, A.J.; Prezzano, K.M.; Hermann, G.M.; Yu, H.; Singh, A.K. Association of survival with stereotactic body radiation therapy following induction chemotherapy for unresected locally advanced pancreatic cancer. J. Radiother. Pract. 2022, 21, 403–410. [Google Scholar] [CrossRef]
- Ng, S.P.; Koay, E.J. Current and emerging radiotherapy strategies for pancreatic adenocarcinoma: Stereotactic, intensity modulated and particle radiotherapy. Ann. Pancreat. Cancer 2018, 1, 22. [Google Scholar] [CrossRef]
- Tchelebi, L.T.; Lehrer, E.J.; Trifiletti, D.M.; Do, N.K.S.; Gusani, N.J.; Crane, C.H.; Zaorsky, N.G. Conventionally fractionated radiation therapy versus stereotactic body radiation therapy for locally advanced pancreatic cancer (CRiSP): An international systematic review and meta-analysis. Cancer 2020, 126, 2120–2131. [Google Scholar] [CrossRef]
- Zhong, J.; Patel, K.; Switchenko, J.; Cassidy, R.J.; Hall, W.A.; Gillespie, T.; Patel, P.R.; Kooby, D.; Landry, J. Outcomes for patients with locally advanced pancreatic adenocarcinoma treated with stereotactic body radiation therapy versus conventionally fractionated radiation. Cancer 2017, 123, 3486–3493. [Google Scholar] [CrossRef]
- Mahadevan, A.; Moningi, S.; Grimm, J.; Li, X.A.; Forster, K.M.; Palta, M.; Prior, P.; Goodman, K.A.; Narang, A.; Heron, D.E.; et al. Maximizing Tumor Control and Limiting Complications with Stereotactic Body Radiation Therapy for Pancreatic Cancer. Int. J. Radiat. Oncol. 2021, 110, 206–216. [Google Scholar] [CrossRef]
- Reddy, A.V.; Hill, C.S.; Sehgal, S.; He, J.; Zheng, L.; Herman, J.M.; Meyer, J.; Narang, A.K. Stereotactic body radiation therapy for the treatment of locally recurrent pancreatic cancer after surgical resection. J. Gastrointest. Oncol. 2022, 13, 1402–1412. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Li, F.; Ju, X.; Cao, F.; Cao, Y.; Fang, F.; Qing, S.; Shen, Y.; Jia, Z.; Zhang, H. Prognostic role of stereotactic body radiation therapy for elderly patients with advanced and medically inoperable pancreatic cancer. Cancer Med. 2017, 6, 2263–2270. [Google Scholar] [CrossRef] [PubMed]
- Goldsmith, C.; Plowman, P.N.; Green, M.M.; Dale, R.G.; Price, P.M. Stereotactic ablative radiotherapy (SABR) as primary, adjuvant, consolidation and re-treatment option in pancreatic cancer: Scope for dose escalation and lessons for toxicity. Radiat. Oncol. 2018, 13, 204. [Google Scholar] [CrossRef] [PubMed]
- Jolissaint, J.S.; Reyngold, M.; Bassmann, J.; Seier, K.P.; Gönen, M.; Varghese, A.M.; Yu, K.H.; Park, W.; O’reilly, E.M.; Balachandran, V.P.; et al. Local Control and Survival after Induction Chemotherapy and Ablative Radiation Versus Resection for Pancreatic Ductal Adenocarcinoma with Vascular Involvement. Ann. Surg. 2021, 274, 894–901. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author, Year | Study Description and Total No. of Patients | Treatment Arms: Dose and No. of Fractions (fx) | BED10 | Chemotherapy Received | Median Follow-Up | LC Results | Overall Survival | Risk of Bias According to ROBINS-I Tool |
|---|---|---|---|---|---|---|---|---|
| Pollom, 2014 [8] | Retrospective single-institution study, 167 patients | 25 Gy in 1 “fraction (fx)”vs. median of 33 Gy (25–45 Gy) in 5 fx | 87.5 Gy vs. median 54.8 Gy (37.5–85.5 Gy) | Yes, (neo)adjuvant | 7.9 months | 1-year local recurrence rate 9.5 vs. 11.7%, p = 0.8 | Median 13.6 months; 30.8% vs. 34.9% at 1-year; no difference | Moderate |
| Toesca, 2020 [9] | Retrospective single-institution study, 149 patients | ≥40 Gy in 5 fx vs. <40 Gy | ≥72 Gy vs. less | Yes, neoadjuvant | 15 months | Median PFS 13 vs. 10 months, p = 0.007; 1-year PFS 57% vs. 36% | Median 16 months; 82% vs. 57% at 1 year; statistically significant | Moderate |
| Zhu, 2020 [10] | Retrospective multicenter study, 972 patients | 42 Gy in 5–8 fx (40–49.6 Gy) vs. 37 Gy in 5–8 fx (36–40.8 Gy) | 74.6 Gy (range: 71.4–88.3 Gy) vs. 64.4 Gy (60.2–69.4 Gy) | Yes, adjuvant | 20.2 months | Median PFS 15.4 vs. 13.3 months, p < 0.001 | Median OS 20.3 vs. 18.2 months, p < 0.001 | Moderate |
| Abi Jaoude, 2022 [11] | Retrospective single-institution study, 89 patients | ≥40 Gy vs. <40 Gy in 5 fx | ≥72 Gy vs. less | No information | No information | 16.7 vs. 30.4% at 1 year, not statistically significant | No information | Not enough information for a full assessment |
| Mazzola, 2018 [12] | Prospective single-institution study, 33 patients | 42–45 Gy in 6 fx vs. 36 Gy in 6 fx | >70 Gy vs. less | Yes | 18 months | Overall, 81% at 1 year | Whole group 75% at 1-year; no statistically significant survival benefit | Low |
| Arcelli, 2020 [13] | Retrospective multicenter study, 56 patients | ≥30 Gy with a median of 6 Gy per fx vs. <30 Gy | ≥48 Gy vs. less | Yes, (neo)adjuvant | 15 months | Better LC for BED ≥ 48 Gy and ≥6 Gy dose per fraction; p = 0.045 and p = 0.003, respectively | Median OS 20 vs. 15 months, p = 0.042 | Moderate |
| Rudra, 2019 [14] | Retrospective multicenter study using ViewRay MRIdian, 44 patients | 40–55 Gy in 25–28 fx vs. 30–35 Gy in 5 fx vs. 40–52 Gy in 5 fx vs. 50–67.5 Gy in 10–15 fx | Median 55.5 Gy vs. 55.8 Gy vs. 77.6 Gy vs. 82.7 Gy (divided in 2 groups > 70 Gy vs. less) | Yes, (neo)adjuvant | 17 months | 77 vs. 57% at 2 years, p = 0.15 | 49% vs. 30% at 2 years, p = 0.03 favoring high dose group | Moderate |
| Arcelli, 2020 [15] | Retrospective multicenter case control study, 80 patients | Median: 30 Gy in 6 Gy/fx vs. 50.4 Gy in 1.8 Gy/fx | Median 48 Gy vs. 59.4 Gy | Yes (neo)adjuvant | 15 months | Median LC 22 vs. 16 months; 1-year LC 80.4 vs. 53%, p = 0.017 | No difference | Moderate |
| Shin, 2022 [16] | Retrospective single-institution study, 161 patients | Median 28 Gy in 4 fx (24–36 Gy) vs. median 54 Gy in 1.8–2 Gy/fx (40–59.4 Gy) | Median 47.6 Gy (38.4–68.4 Gy) vs. median 64.8 Gy (48–70 Gy) | Yes, (neo)adjuvant | 15.5 months | Free from local progression 77.2 vs. 87.1%; p = 0.691 at 1-year | 66.7 vs. 80% at 1-year | Moderate to serious |
| Park, 2017 [17] | Retrospective single-institution study, 270 patients | 30–33 Gy in 5 fx vs. 45–56 Gy in 25–28 fx | 48–54.7 Gy vs. 53.1–67.2 Gy | Yes, (neo)adjuvant | 12.9 months | 34.4 vs. 30.2% at 1 year; not significant | Median 15.7 months, 56.2% vs. 59.6% at 1 year, p = 0.75 | Moderate |
| Lin, 2015 [18] | Retrospective single-institution study, 41 patients | 35–45 Gy in 7–9 Gy/fx vs. 45–50 Gy in 1.8–2 Gy/fx | 59.5–85.5 Gy vs. 53.1–60 Gy | Yes, adjuvant in CFRT group | 16 months | Significantly better LC favoring SBRT, p = 0.004 | 80 vs. 70.7% at 1 year, p = 0.127 | Moderate to serious |
| Abi Jaoude, 2021 [19] | Retrospective single-institution study, 104 patients | Median 36 Gy (25–55 Gy) in 5 fx vs. median 50.4 Gy (50–50.4 Gy) in 25–28 fx | Median 61.9 Gy (37.5–115.5 Gy) vs. median 59.4 Gy (59.4–60 Gy) | Yes, neoadjuvant | 22 months | PFS 16.1 vs. 12.3 months, p = 0.81 | Median 29.6 vs. 24.1 months, p = 0.18 | Moderate |
| Characteristics | Non-Ablative RT Group | SBRT Group |
|---|---|---|
| Number | N = 74 | N = 15 |
| Median Age | 67 years (44–89) | 69 years (53–83) |
| Gender | ||
| Male | 38 | 8 |
| Female | 36 | 7 |
| Performance Status | ||
| ECOG 0 | 3 | 0 |
| ECOG 1 | 36 | 15 |
| ECOG 2 | 20 | 0 |
| ECOG 3 | 15 | 0 |
| ECOG 4 | 0 | 0 |
| Hospitalization Status | ||
| Inpatient | 11 | 0 |
| Outpatient | 63 | 15 |
| TNM | ||
| T1 | 0 | 2 |
| T2 | 2 | 1 |
| T3 | 11 | 3 |
| T3/4 | 12 | 0 |
| T4 | 46 | 6 |
| Tx | 3 | 5 |
| N0 | 33 | 15 |
| N1 | 26 | 0 |
| N2 | 6 | 0 |
| Nx | 9 | 0 |
| M0 | 31 | 15 |
| M1 | 43 | 0 |
| Mx | 0 | 0 |
| Tumor Location | ||
| Head | 39 | 8 |
| Neck | 3 | 1 |
| Uncinate | 0 | 1 |
| Body | 16 | 5 |
| Tail | 16 | 0 |
| Histology | ||
| Adenocarcinoma | 70 | 15 |
| Neuroendocrine carcinoma | 2 | 0 |
| Non-small cell carcinoma | 1 | 0 |
| Squamous cell carcinoma | 1 | 0 |
| Stents In-Situ at RT start | ||
| Yes | 30 | 7 |
| No | 44 | 8 |
| Prior Systemic Therapy | ||
| Yes | 30 | 9 |
| No | 44 | 6 |
| Total Dose Received | Number of Fractions | BED10 | n | (% of 89 Patients) | |
|---|---|---|---|---|---|
| Non-ablative RT Group (n = 74) | 30 Gy | 10 | 39 Gy | 54 | 61% |
| 34 Gy | 15 | 41.7 Gy | 1 | 1% | |
| 35 Gy | 10 | 47.2 Gy | 6 | 7% | |
| 36 Gy | 15 | 44.6 Gy | 2 | 2% | |
| 40 Gy | 10 | 56 Gy | 1 | 1% | |
| 40 Gy | 15 | 50.6 Gy | 10 | 11% | |
| SBRT Group (n = 15) | 21 Gy | 3 | 35.7 Gy | 8 | 9% |
| 24 Gy | 3 | 43.2 Gy | 1 | 1% | |
| 30 Gy | 3 | 60 Gy | 3 | 3.5% | |
| 40 Gy | 5 | 72 Gy | 2 | 2% | |
| 50 Gy | 5 | 100 Gy | 1 | 1% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamel, R.; Dennis, K.; Doody, J.; Pantarotto, J. Ablative vs. Non-Ablative Radiotherapy in Palliating Locally Advanced Pancreatic Cancer: A Single Institution Experience and a Systematic Review of the Literature. Cancers 2023, 15, 3016. https://doi.org/10.3390/cancers15113016
Kamel R, Dennis K, Doody J, Pantarotto J. Ablative vs. Non-Ablative Radiotherapy in Palliating Locally Advanced Pancreatic Cancer: A Single Institution Experience and a Systematic Review of the Literature. Cancers. 2023; 15(11):3016. https://doi.org/10.3390/cancers15113016
Chicago/Turabian StyleKamel, Randa, Kristopher Dennis, Janice Doody, and Jason Pantarotto. 2023. "Ablative vs. Non-Ablative Radiotherapy in Palliating Locally Advanced Pancreatic Cancer: A Single Institution Experience and a Systematic Review of the Literature" Cancers 15, no. 11: 3016. https://doi.org/10.3390/cancers15113016
APA StyleKamel, R., Dennis, K., Doody, J., & Pantarotto, J. (2023). Ablative vs. Non-Ablative Radiotherapy in Palliating Locally Advanced Pancreatic Cancer: A Single Institution Experience and a Systematic Review of the Literature. Cancers, 15(11), 3016. https://doi.org/10.3390/cancers15113016