
Allergic Diseases and Risk of Malignancy of Gastrointestinal Cancers

 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
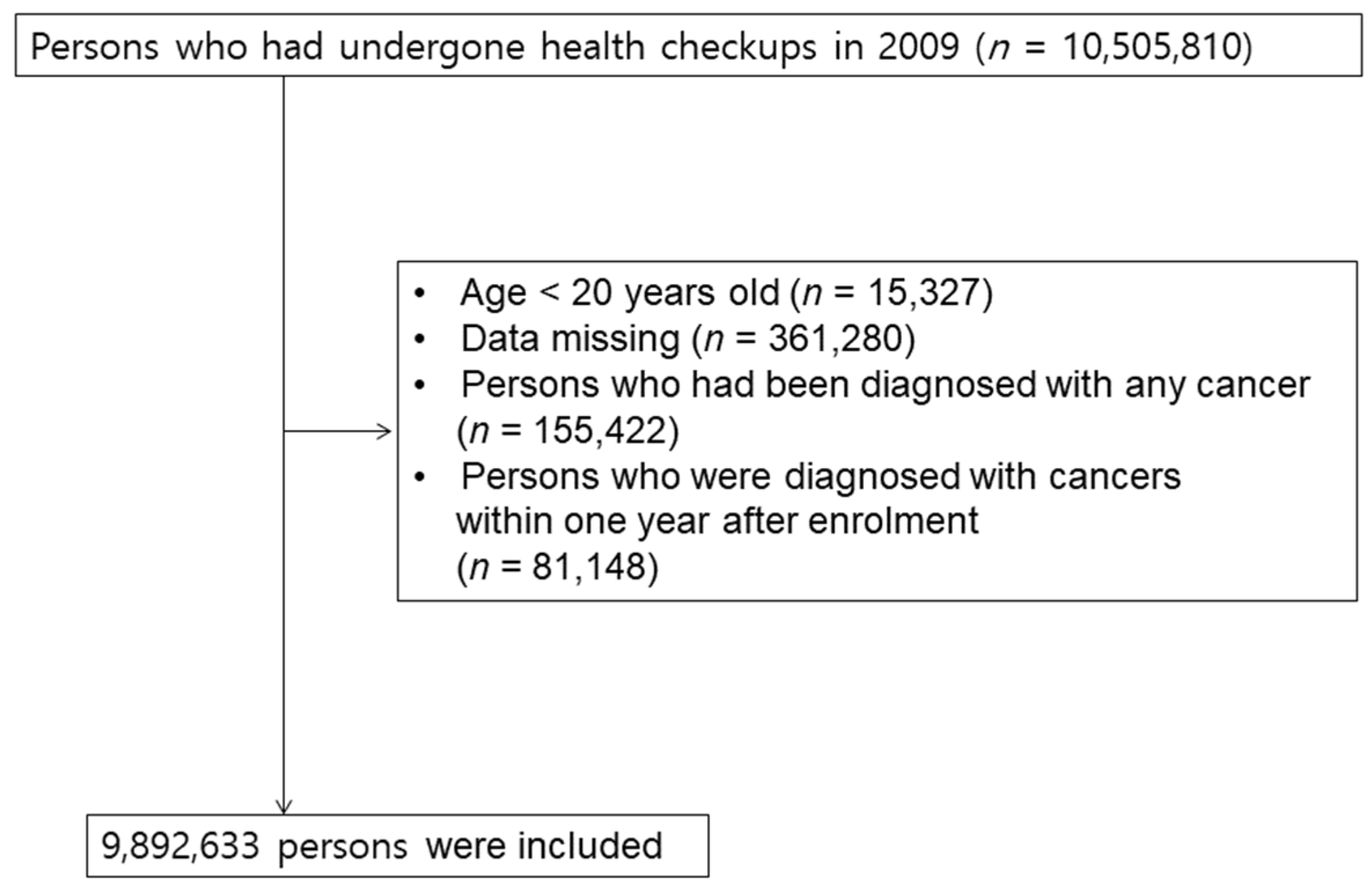
2.2. Study Population and Data Collection
2.3. Disease Identification and Study Outcomes
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Association between Allergic Diseases and the Risk of GI Cancers
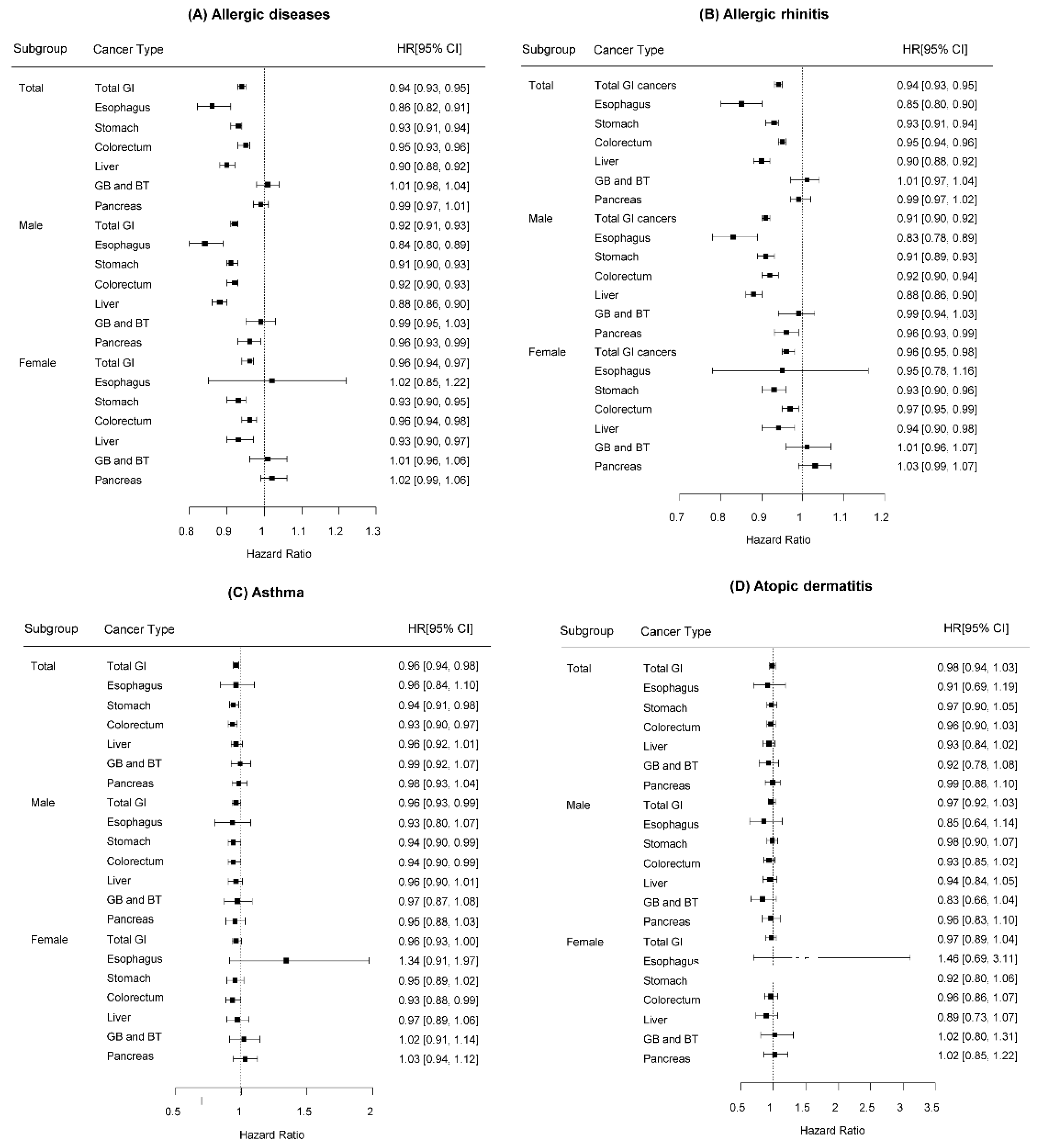
3.3. Association between Specific Allergic Diseases and the Risk of GI Cancers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Asher, M.I.; Montefort, S.; Bjorksten, B.; Lai, C.K.; Strachan, D.P.; Weiland, S.K.; Williams, H.; Group, I.P.T.S. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicountry cross-sectional surveys. Lancet 2006, 368, 733–743. [Google Scholar] [CrossRef] [PubMed]
- Alduraywish, S.A.; Lodge, C.J.; Campbell, B.; Allen, K.J.; Erbas, B.; Lowe, A.J.; Dharmage, S.C. The march from early life food sensitization to allergic disease: A systematic review and meta-analyses of birth cohort studies. Allergy 2016, 71, 77–89. [Google Scholar] [CrossRef] [PubMed]
- McWhorter, W.P. Allergy and risk of cancer. A prospective study using NHANESI followup data. Cancer 1988, 62, 451–455. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, N.E.; Mikoczy, Z.; Hagmar, L. Cancer incidence in 13811 patients skin tested for allergy. J. Investig. Allergol. Clin. Immunol. 2005, 15, 161–166. [Google Scholar]
- Cui, Y.; Hill, A.W. Atopy and Specific Cancer Sites: A Review of Epidemiological Studies. Clin. Rev. Allergy Immunol. 2016, 51, 338–352. [Google Scholar] [CrossRef]
- Lowcock, E.C.; Cotterchio, M.; Ahmad, N. Association between allergies, asthma, and breast cancer risk among women in Ontario, Canada. Cancer Causes Control 2013, 24, 1053–1056. [Google Scholar] [CrossRef]
- Cotterchio, M.; Lowcock, E.; Hudson, T.J.; Greenwood, C.; Gallinger, S. Association between allergies and risk of pancreatic cancer. Cancer Epidemiol. Biomark. Prev. 2014, 23, 469–480. [Google Scholar] [CrossRef] [Green Version]
- Gomez-Rubio, P.; Rosato, V.; Marquez, M.; Bosetti, C.; Molina-Montes, E.; Rava, M.; Pinero, J.; Michalski, C.W.; Farre, A.; Molero, X.; et al. A systems approach identifies time-dependent associations of multimorbidities with pancreatic cancer risk. Ann. Oncol. 2017, 28, 1618–1624. [Google Scholar] [CrossRef]
- Gandini, S.; Lowenfels, A.B.; Jaffee, E.M.; Armstrong, T.D.; Maisonneuve, P. Allergies and the risk of pancreatic cancer: A meta-analysis with review of epidemiology and biological mechanisms. Cancer Epidemiol. Biomark. Prev. 2005, 14, 1908–1916. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, E.J.; Gapstur, S.M.; Newton, C.C.; Turner, M.C.; Campbell, P.T. Hay Fever and asthma as markers of atopic immune response and risk of colorectal cancer in three large cohort studies. Cancer Epidemiol. Biomark. Prev. 2013, 22, 661–669. [Google Scholar] [CrossRef] [Green Version]
- Ribas, A.; Wolchok, J.D. Cancer immunotherapy using checkpoint blockade. Science 2018, 359, 1350–1355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Hemminki, K.; Forsti, A.; Sundquist, J.; Sundquist, K.; Ji, J. Cancer risk and mortality in asthma patients: A Swedish national cohort study. Acta Oncol. 2015, 54, 1120–1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amirian, E.S.; Zhou, R.; Wrensch, M.R.; Olson, S.H.; Scheurer, M.E.; Il’yasova, D.; Lachance, D.; Armstrong, G.N.; McCoy, L.S.; Lau, C.C.; et al. Approaching a Scientific Consensus on the Association between Allergies and Glioma Risk: A Report from the Glioma International Case-Control Study. Cancer Epidemiol. Biomark. Prev. 2016, 25, 282–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linos, E.; Raine, T.; Alonso, A.; Michaud, D. Atopy and risk of brain tumors: A meta-analysis. J. Natl. Cancer Inst. 2007, 99, 1544–1550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olson, S.H.; Hsu, M.; Satagopan, J.M.; Maisonneuve, P.; Silverman, D.T.; Lucenteforte, E.; Anderson, K.E.; Borgida, A.; Bracci, P.M.; Bueno-de-Mesquita, H.B.; et al. Allergies and risk of pancreatic cancer: A pooled analysis from the Pancreatic Cancer Case-Control Consortium. Am. J. Epidemiol. 2013, 178, 691–700. [Google Scholar] [CrossRef] [PubMed]
- Schwartzbaum, J.; Ding, B.; Johannesen, T.B.; Osnes, L.T.; Karavodin, L.; Ahlbom, A.; Feychting, M.; Grimsrud, T.K. Association between prediagnostic IgE levels and risk of glioma. J. Natl. Cancer Inst. 2012, 104, 1251–1259. [Google Scholar] [CrossRef]
- Rava, M.; Czachorowski, M.J.; Silverman, D.; Marquez, M.; Kishore, S.; Tardon, A.; Serra, C.; Garcia-Closas, M.; Garcia-Closas, R.; Carrato, A.; et al. Asthma status is associated with decreased risk of aggressive urothelial bladder cancer. Int. J. Cancer 2018, 142, 470–476. [Google Scholar] [CrossRef] [Green Version]
- Shadman, M.; White, E.; De Roos, A.J.; Walter, R.B. Associations between allergies and risk of hematologic malignancies: Results from the VITamins and lifestyle cohort study. Am. J. Hematol. 2013, 88, 1050–1054. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Diepgen, T.L. Is atopy a protective or a risk factor for cancer? A review of epidemiological studies. Allergy 2005, 60, 1098–1111. [Google Scholar] [CrossRef]
- Merrill, R.M.; Isakson, R.T.; Beck, R.E. The association between allergies and cancer: What is currently known? Ann. Allergy Asthma Immunol. 2007, 99, 102–116, quiz 117–109, 150. [Google Scholar] [CrossRef]
- Sherman, P.W.; Holland, E.; Sherman, J.S. Allergies: Their role in cancer prevention. Q. Rev. Biol. 2008, 83, 339–362. [Google Scholar] [CrossRef] [PubMed]
- Vojtechova, P.; Martin, R.M. The association of atopic diseases with breast, prostate, and colorectal cancers: A meta-analysis. Cancer Causes Control 2009, 20, 1091–1105. [Google Scholar] [CrossRef] [PubMed]
- Vighi, G.; Marcucci, F.; Sensi, L.; Di Cara, G.; Frati, F. Allergy and the gastrointestinal system. Clin. Exp. Immunol. 2008, 153 (Suppl. S1), 3–6. [Google Scholar] [CrossRef] [PubMed]
- Majamaa, H.; Isolauri, E. Evaluation of the gut mucosal barrier: Evidence for increased antigen transfer in children with atopic eczema. J. Allergy Clin. Immunol. 1996, 97, 985–990. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T. Introduction for inflammation and cancer. Semin. Immunopathol. 2013, 35, 121–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, P.R.; Wright, S.W.; Serrano, C.; Riera, F.; Duarte, I.; Torres, J.; Pena, A.; Rollan, A.; Viviani, P.; Guiraldes, E.; et al. Helicobacter pylori gastritis in children is associated with a regulatory T-cell response. Gastroenterology 2008, 134, 491–499. [Google Scholar] [CrossRef]
- Kim, M.; Choi, K.H.; Hwang, S.W.; Lee, Y.B.; Park, H.J.; Bae, J.M. Inflammatory bowel disease is associated with an increased risk of inflammatory skin diseases: A population-based cross-sectional study. J. Am. Acad. Dermatol. 2017, 76, 40–48. [Google Scholar] [CrossRef]
- Kim, B.K.; Kim, J.Y.; Kang, M.K.; Yang, M.S.; Park, H.W.; Min, K.U.; Cho, S.H.; Kang, H.R. Allergies are still on the rise? A 6-year nationwide population-based study in Korea. Allergol. Int. 2016, 65, 186–191. [Google Scholar] [CrossRef] [Green Version]
- Tambe, N.A.; Wilkens, L.R.; Wan, P.; Stram, D.O.; Gilliland, F.; Park, S.L.; Cozen, W.; Martinez-Maza, O.; Le Marchand, L.; Henderson, B.E.; et al. Atopic allergic conditions and colorectal cancer risk in the Multiethnic Cohort Study. Am. J. Epidemiol. 2015, 181, 889–897. [Google Scholar] [CrossRef] [Green Version]
- Prizment, A.E.; Folsom, A.R.; Cerhan, J.R.; Flood, A.; Ross, J.A.; Anderson, K.E. History of allergy and reduced incidence of colorectal cancer, Iowa Women’s Health Study. Cancer Epidemiol. Biomark. Prev. 2007, 16, 2357–2362. [Google Scholar] [CrossRef] [Green Version]
- Negri, E.; Bosetti, C.; La Vecchia, C.; Levi, F.; Tomei, F.; Franceschi, S. Allergy and other selected diseases and risk of colorectal cancer. Eur. J. Cancer 1999, 35, 1838–1841. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.; Yang, J.; Li, P.; Lu, X.; Cai, J. Association between allergic conditions and colorectal cancer risk/mortality: A meta-analysis of prospective studies. Sci. Rep. 2017, 7, 5589. [Google Scholar] [CrossRef] [PubMed]
- Ji, J.; Shu, X.; Li, X.; Sundquist, K.; Sundquist, J.; Hemminki, K. Cancer risk in hospitalised asthma patients. Br. J. Cancer 2009, 100, 829–833. [Google Scholar] [CrossRef] [Green Version]
- Chou, W.Y.; Lai, P.Y.; Hu, J.M.; Hsu, C.H.; Chen, Y.C.; Tian, Y.F.; You, S.L.; Hsiao, C.W.; Chou, Y.C.; Sun, C.A. Association between atopic dermatitis and colorectal cancer risk: A nationwide cohort study. Medicine 2020, 99, e18530. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.Z.; Le Marchand, L.; Haiman, C.A.; Monroe, K.R.; Wilkens, L.R.; Zhang, Z.F.; Setiawan, V.W. Atopic allergic conditions and pancreatic cancer risk: Results from the Multiethnic Cohort Study. Int. J. Cancer 2018, 142, 2019–2027. [Google Scholar] [CrossRef] [Green Version]
- Hwang, C.Y.; Chen, Y.J.; Lin, M.W.; Chen, T.J.; Chu, S.Y.; Chen, C.C.; Lee, D.D.; Chang, Y.T.; Wang, W.J.; Liu, H.N. Cancer risk in patients with allergic rhinitis, asthma and atopic dermatitis: A nationwide cohort study in Taiwan. Int. J. Cancer 2012, 130, 1160–1167. [Google Scholar] [CrossRef]
- Vesterinen, E.; Pukkala, E.; Timonen, T.; Aromaa, A. Cancer incidence among 78,000 asthmatic patients. Int. J. Epidemiol. 1993, 22, 976–982. [Google Scholar] [CrossRef]
- D’Arcy, M.; Rivera, D.R.; Grothen, A.; Engels, E.A. Allergies and the Subsequent Risk of Cancer among Elderly Adults in the United States. Cancer Epidemiol. Biomark. Prev. 2019, 28, 741–750. [Google Scholar] [CrossRef] [Green Version]
- Ribatti, D. The concept of immune surveillance against tumors. The first theories. Oncotarget 2017, 8, 7175–7180. [Google Scholar] [CrossRef] [Green Version]
- HS, L. Cellular and Humoral Aspects of the Hypersensitive States: A Symposium at the New York Academy of Medicine. J. Am. Med. Assoc. 1959, 170, 883. [Google Scholar] [CrossRef]
- Straumann, A.; Aceves, S.S.; Blanchard, C.; Collins, M.H.; Furuta, G.T.; Hirano, I.; Schoepfer, A.M.; Simon, D.; Simon, H.U. Pediatric and adult eosinophilic esophagitis: Similarities and differences. Allergy 2012, 67, 477–490. [Google Scholar] [CrossRef] [PubMed]
- Legrand, F.; Driss, V.; Delbeke, M.; Loiseau, S.; Hermann, E.; Dombrowicz, D.; Capron, M. Human eosinophils exert TNF-alpha and granzyme A-mediated tumoricidal activity toward colon carcinoma cells. J. Immunol. 2010, 185, 7443–7451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prizment, A.E.; Anderson, K.E.; Visvanathan, K.; Folsom, A.R. Inverse association of eosinophil count with colorectal cancer incidence: Atherosclerosis risk in communities study. Cancer Epidemiol. Biomark. Prev. 2011, 20, 1861–1864. [Google Scholar] [CrossRef] [Green Version]
- Karagiannis, S.N.; Bracher, M.G.; Beavil, R.L.; Beavil, A.J.; Hunt, J.; McCloskey, N.; Thompson, R.G.; East, N.; Burke, F.; Sutton, B.J.; et al. Role of IgE receptors in IgE antibody-dependent cytotoxicity and phagocytosis of ovarian tumor cells by human monocytic cells. Cancer Immunol. Immunother. 2008, 57, 247–263. [Google Scholar] [CrossRef]
- Ye, Z.S.; Fan, L.N.; Wang, L.; Yang, B.; Wang, L.F.; Liu, Y.S.; Ji, S.N.; Xu, H.Z.; Xiao, C.X. Immunoglobulin E induces colon cancer cell apoptosis via enhancing cyp27b1 expression. Am. J. Transl. Res. 2016, 8, 5715–5722. [Google Scholar]
- Salminen, S.; Bouley, C.; Boutron-Ruault, M.C.; Cummings, J.H.; Franck, A.; Gibson, G.R.; Isolauri, E.; Moreau, M.C.; Roberfroid, M.; Rowland, I. Functional food science and gastrointestinal physiology and function. Br. J. Nutr. 1998, 80 (Suppl. S1), S147–S171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burnett-Hartman, A.N.; Newcomb, P.A.; Potter, J.D. Infectious agents and colorectal cancer: A review of Helicobacter pylori, Streptococcus bovis, JC virus, and human papillomavirus. Cancer Epidemiol. Biomark. Prev. 2008, 17, 2970–2979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scadding, G.K.; Bousquet, J. Introduction: Allergic rhinitis. Allergy 2007, 62 (Suppl. S85), 3–5. [Google Scholar] [CrossRef]
- Lugovic, L.; Lipozencic, J. Are respiratory allergic diseases related to atopic dermatitis? Coll. Antropol. 2000, 24, 335–345. [Google Scholar]



{kind=link}
{kind=link}
| Variables | No Allergic Diseases | Allergic Diseases | p |
|---|---|---|---|
| (n = 4,766,745) | (n = 5,125,888) | ||
| Sex, Male | 2,958,412 (62.1) | 2,505,876 (48.9) | <0.0001 |
| Age (years) | 46.05 ± 13.82 | 47.6 ± 14.19 | <0.0001 |
| Smoking | <0.0001 | ||
| Non-smoker | 2,581,642 (54.2) | 3,266,772 (63.7) | |
| Ex-smoker | 687,730 (14.4) | 731,246 (14.3) | |
| Current-smoker | 1,497,373 (31.4) | 1,127,870 (22.0) | |
| Alcohol consumption | <0.0001 | ||
| Non | 2,246,070 (47.1) | 2,800,084 (54.6) | |
| Drinking | 2,520,675 (52.9) | 2,325,804 (45.4) | |
| Regular exercise | 866,087 (18.2) | 954,290 (18.6) | <0.0001 |
| Low income | 990,063 (20.8) | 1,050,500 (20.5) | <0.0001 |
| BMI (Kg/m2) | 23.69 ± 3.19 | 23.73 ± 3.22 | <0.0001 |
| Diabetes mellitus | 395,243 (8.3) | 451,024 (8.8) | <0.0001 |
| Hypertension | 1,161,169 (24.4) | 1,351,155 (26.4) | <0.0001 |
| Dyslipidemia | 796,386 (16.7) | 999,591 (19.5) | <0.0001 |
| Atopic dermatitis | 295,466 (5.8) | ||
| Allergic rhinitis | 4,779,445 (93.2) | ||
| Asthma | 1,184,035 (23.1) | ||
| Follow-up duration (years) | |||
| Mean ± SD | 7.15 ± 1.04 | 7.13 ± 1.10 | <0.0001 |
| Median (Q1–Q3) | 7.3 (7.10–7.57) | 7.31 (7.10–7.58) | <0.0001 |
| Cancer Type | All | Total | Male | Female | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | Event | HR a (95% CI) | n | Event | HR a (95% CI) | n | Event | HR a (95% CI) | ||
| Total | No | 4,766,745 | 99,826 | 1 (Ref) | 2,958,412 | 70,758 | 1 (Ref) | 1,808,333 | 29,068 | 1 (Ref) |
| Yes | 5,125,888 | 105,124 | 0.94 (0.93, 0.95) | 2,505,876 | 64,302 | 0.92 (0.91, 0.93) | 2,620,012 | 40,822 | 0.96 (0.94, 0.97) | |
| Esophagus | No | 4,766,745 | 3039 | 1 (Ref) | 2,958,412 | 2834 | 1 (Ref) | 1,808,333 | 205 | 1 (Ref) |
| Yes | 5,125,888 | 2660 | 0.86 (0.82, 0.91) | 2,505,876 | 2358 | 0.84 (0.80, 0.89) | 2,620,012 | 302 | 1.02 (0.85, 1.22) | |
| Stomach | No | 4,766,745 | 36,254 | 1 (Ref) | 2,958,412 | 27,283 | 1 (Ref) | 1,808,333 | 8971 | 1 (Ref) |
| Yes | 5,125,888 | 36,923 | 0.93 (0.91, 0.94) | 2,505,876 | 24,743 | 0.91 (0.90, 0.93) | 2,620,012 | 12,180 | 0.93 (0.90, 0.95) | |
| CRC | No | 4,766,745 | 41,460 | 1 (Ref) | 2,958,412 | 27,231 | 1 (Ref) | 1,808,333 | 14,229 | 1 (Ref) |
| Yes | 5,125,888 | 44,938 | 0.95 (0.93, 0.96) | 2,505,876 | 24,843 | 0.92 (0.90, 0.93) | 2,620,012 | 20,095 | 0.96 (0.94, 0.98) | |
| Liver | No | 4,766,745 | 22,801 | 1 (Ref) | 2,958,412 | 17,671 | 1 (Ref) | 1,808,333 | 5130 | 1 (Ref) |
| Yes | 5,125,888 | 22,572 | 0.90 (0.88, 0.92) | 2,505,876 | 15,472 | 0.88 (0.86, 0.90) | 2,620,012 | 7100 | 0.93 (0.90, 0.97) | |
| GB/BT | No | 4,766,745 | 7365 | 1 (Ref) | 2,958,412 | 4595 | 1 (Ref) | 1,808,333 | 2770 | 1 (Ref) |
| Yes | 5,125,888 | 8970 | 1.01 (0.98, 1.04) | 2,505,876 | 4842 | 0.99 (0.95, 1.03) | 2,620,012 | 4128 | 1.01 (0.96, 1.06) | |
| Pancreas | No | 4,766,745 | 15,921 | 1 (Ref) | 2,958,412 | 10,746 | 1 (Ref) | 1,808,333 | 5175 | 1 (Ref) |
| Yes | 5,125,888 | 18,178 | 0.99 (0.97, 1.01) | 2,505,876 | 10,370 | 0.96 (0.93, 0.99) | 2,620,012 | 7808 | 1.02 (0.99, 1.06) | |
| Type | AD/Asthma/AR | n | Event | HR (95% CI) a |
|---|---|---|---|---|
| Esophagus | (−/−/−) | 4,766,745 | 3039 | 1 (Ref) |
| (−/+/−) | 246,474 | 238 | 0.95 (0.83, 1.09) | |
| (−/−/+) | 3,705,553 | 1696 | 0.84 (0.80, 0.90) | |
| (−/+/+) | 878,395 | 573 | 0.91 (0.83, 0.99) | |
| (+/−/−) | 91,766 | 54 | 0.90 (0.69, 1.18) | |
| (+/+/−) | 8203 | 10 | 1.18 (0.63, 2.19) | |
| (+/−/+) | 144,534 | 58 | 0.71 (0.55, 0.92) | |
| (+/+/+) | 50,963 | 31 | 0.80 (0.56, 1.15) | |
| Stomach | (−/−/−) | 4,766,745 | 36,254 | 1 (Ref) |
| (−/+/−) | 246,474 | 2704 | 0.95 (0.91, 0.98) | |
| (−/−/+) | 3,705,553 | 24,534 | 0.93 (0.91, 0.94) | |
| (−/+/+) | 878,395 | 7526 | 0.92 (0.90, 0.94) | |
| (+/−/−) | 91,766 | 702 | 0.98 (0.91, 1.05) | |
| (+/+/−) | 8203 | 86 | 0.87 (0.71, 1.08) | |
| (+/−/+) | 144,534 | 951 | 0.89 (0.84, 0.95) | |
| (+/+/+) | 50,963 | 420 | 0.85 (0.77, 0.94) | |
| Colorectum | (−/−/−) | 4,766,745 | 41,460 | 1 (Ref) |
| (−/+/−) | 246,474 | 3139 | 0.94 (0.91, 0.97) | |
| (−/−/+) | 3,705,553 | 29,913 | 0.95 (0.94, 0.97) | |
| (−/+/+) | 878,395 | 9268 | 0.94 (0.92, 0.96) | |
| (+/−/−) | 91,766 | 805 | 0.96 (0.90, 1.03) | |
| (+/+/−) | 8203 | 92 | 0.79 (0.65, 0.97) | |
| (+/−/+) | 144,534 | 1188 | 0.94 (0.89, 0.99) | |
| (+/+/+) | 50,963 | 533 | 0.91 (0.83, 0.99) | |
| Liver | (−/−/−) | 4,766,745 | 22,801 | 1 (Ref) |
| (−/+/−) | 246,474 | 1739 | 0.95 (0.91, 1.00) | |
| (−/−/+) | 3,705,553 | 14,898 | 0.90 (0.88, 0.92) | |
| (−/+/+) | 878,395 | 4662 | 0.90 (0.87, 0.93) | |
| (+/−/−) | 91,766 | 422 | 0.93 (0.84, 1.02) | |
| (+/+/−) | 8203 | 44 | 0.69 (0.51, 0.93) | |
| (+/−/+) | 144,534 | 542 | 0.81 (0.743, 0.88) | |
| (+/+/+) | 50,963 | 265 | 0.84 (0.74, 0.95) | |
| Pancreas | (−/−/−) | 4,766,745 | 15,921 | 1 (Ref) |
| (−/+/−) | 246,474 | 1325 | 0.98 (0.93, 1.04) | |
| (−/−/+) | 3,705,553 | 11,887 | 0.99 (0.97, 1.02) | |
| (−/+/+) | 878,395 | 3881 | 1.00 (0.96, 1.03) | |
| (+/−/−) | 91,766 | 322 | 0.99 (0.88, 1.10) | |
| (+/+/−) | 8203 | 41 | 0.87 (0.64, 1.18) | |
| (+/−/+) | 144,534 | 495 | 1.01 (0.93, 1.11) | |
| (+/+/+) | 50,963 | 227 | 0.96 (0.85, 1.10) | |
| GB/BT | (−/−/−) | 4,766,745 | 7365 | 1 (Ref) |
| (−/+/−) | 246,474 | 719 | 0.99 (0.92, 1.07) | |
| (−/−/+) | 3,705,553 | 5662 | 1.01 (0.97, 1.04) | |
| (−/+/+) | 878,395 | 2062 | 1.03 (0.98, 1.08) | |
| (+/−/−) | 91,766 | 146 | 0.92 (0.78, 1.08) | |
| (+/+/−) | 8203 | 28 | 1.09 (0.75, 1.58) | |
| (+/−/+) | 144,534 | 235 | 1.00 (0.87, 1.13) | |
| (+/+/+) | 50,963 | 118 | 0.96 (0.80, 1.15) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, Y.J.; Han, K.; Jin, E.H.; Lim, J.H.; Shin, C.M.; Lee, D.H. Allergic Diseases and Risk of Malignancy of Gastrointestinal Cancers. Cancers 2023, 15, 3219. https://doi.org/10.3390/cancers15123219
Choi YJ, Han K, Jin EH, Lim JH, Shin CM, Lee DH. Allergic Diseases and Risk of Malignancy of Gastrointestinal Cancers. Cancers. 2023; 15(12):3219. https://doi.org/10.3390/cancers15123219
Chicago/Turabian StyleChoi, Yoon Jin, Kyungdo Han, Eun Hyo Jin, Joo Hyun Lim, Cheol Min Shin, and Dong Ho Lee. 2023. "Allergic Diseases and Risk of Malignancy of Gastrointestinal Cancers" Cancers 15, no. 12: 3219. https://doi.org/10.3390/cancers15123219
APA StyleChoi, Y. J., Han, K., Jin, E. H., Lim, J. H., Shin, C. M., & Lee, D. H. (2023). Allergic Diseases and Risk of Malignancy of Gastrointestinal Cancers. Cancers, 15(12), 3219. https://doi.org/10.3390/cancers15123219