1. Introduction
The worldwide incidence of hepatocellular carcinoma (HCC) is increasing, and the mortality rate is high [
1]. Treatment choice and prognosis for HCC patients are generally determined using the Barcelona Clinical Liver Cancer (BCLC) staging system based on tumor burden, tumor staging, and liver function. Additionally, other prognostic scores such as the ALBI and ART scores have emerged, showing potential relevance in TACE patients [
2]. It is recommended that patients with BCLC 0 (very early stage) and BCLC A (early stage) undergo curative treatment involving surgical resection, liver transplantation, and/or local tumor ablation. For patients in the intermediate stage (BCLC B), transarterial chemoembolization (TACE) is recommended as a first-line treatment. There is a growing body of evidence supporting the use of locoregional therapy (LRT), i.e., TACE, radiofrequency ablation, or its combination, to improve clinical outcomes in cases of localized unresectable HCC [
3,
4]. However, the therapeutic outcomes of LRT are difficult to predict. Disease progression often occurs along the margins of the treated zone due to the development of untreated lesions and/or a failure to treat microsatellite lesions around HCC nodules. The notable recurrence pattern associated with HCC has been described as a double-peaked incidence, referring to early and late recurrences [
5]. Early recurrence, which accounts for approximately 40% of HCC patients after LRT [
6], generally involves intrahepatic local recurrence, whereas late recurrence generally involves de novo tumor development. Numerous researchers have reported that early recurrence after curative treatment is strongly associated with a poor prognosis. Thus, it is important to identify risk factors for the management of patients who are susceptible to early recurrence via prompt re-intervention. Researchers have identified several risk factors related to intrahepatic recurrence after LRT, including tumor size, tumor number, tumor location, serum tumor markers, and poor differentiation [
7,
8]. Note, however, that it can be difficult to determine a suitable therapeutic response based on current imaging modalities, such as ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI). Note also that these imaging modalities expose patients to radiation or toxic contrast agents and lack the ability to detect small nodules. In the detection of small HCC tumors, the sensitivity and specificity of these methods can vary considerably: MRI (78.82% and 78.46%), CT (62.35% and 73.85%), and ultrasound (44% and 92%) [
9,
10]. Furthermore, a recent meta-analysis comparing yttrium-90 radioembolization (Y90RE) and TACE suggests both methods exhibit similar impacts on survival, response rate, and safety, although radioembolization may offer a superior delay in tumor progression [
11]. In light of evaluating post-treatment outcomes, recent research suggests that a transient elevation in transaminase levels post-TACE may serve as an indicator of objective response, offering a straightforward tool for a tailored HCC treatment approach [
12].
Serum tumor markers are commonly used for HCC surveillance and the evaluation of therapeutic responses. Alpha-fetoprotein (AFP) is a widely used biomarker due to its objectivity, reasonable cost, and convenience; however, the sensitivity and specificity are insufficient for clinical use, and only 30% of patients present an observable increase in AFP serum levels. Researchers have developed other serum tumor markers for clinical use, including AFP-L3%, lectin-bound AFP, and PIVKA-II (protein induced by vitamin K absence or antagonists-II); however, those markers are unable to detect small HCC tumors in roughly 30% of patients [
13].
There is a growing body of evidence indicating the potential value of liquid biopsy in precision medicine for the treatment of cancer. Cell-free DNA in liquid biopsies can be used to obtain important genetic and epigenetic information related to malignant cells to facilitate cancer management, including screening, diagnosis, prognosis, and treatment. DNA methylation is an important epigenetic function that plays a fundamental role in every stage of carcinogenesis by regulating tumor-related gene expression. It is believed that DNA hypermethylation is involved in repressing tumor suppressors and DNA repair genes, whereas DNA hypomethylation appears to be responsible for the overexpression of oncogenes in many types of cancer [
14,
15]. In some cases, genes that undergo aberrant methylation can be used as tumor markers. Examples include cytosine methylation, which involves the covalent binding of a methyl group to genomic DNA. Note that it provides stability superior to that of protein or RNA markers [
16]. The detection of methylation markers in liquid biopsy (e.g., blood, urine, saliva, and stool) provides a non-invasive method to monitor cancer progression [
17].
A number of studies have reported on the clinical application of methylation markers in cancer diagnosis and prognosis; however, no previous studies have mentioned the application of methylation markers in HCC as a tumor biomarker after LRT. This is the first study to assess the feasibility of using methylation markers from liquid biopsy—blood to predict the response of HCC patients to LRT. We also compared the effectiveness of methylation markers with that of existing tumor markers.
4. Discussion
Tumor markers are critical to monitoring the therapeutic effects and early detection of HCC recurrence. Contrast-enhanced imaging has also proven useful; however, it is somewhat limited during post-operative follow-up due to the toxicity of contrast agents and their high costs. AFP is currently the serum marker most widely used for HCC screening, diagnosis, and the evaluation of therapeutic efficacy; however, more than 35% of HCC patients do not present elevated serum AFP levels even in the late stages [
26]. One multicenter study reported AFP levels lower than 20 ng/mL in 53.5% of cases involving early HCC and 41.5% of cases involving late HCC [
27]. Furthermore, PIVKA-II is no better than AFP in the detection of HCC [
28]. In the current study, 41 out of 72 patients (56.9%) were deemed AFP negative under a cut-off value of 20 ng/mL, and 27 out of 65 patients (41.5%) were deemed PIVKA-II negative at a cut-off value of 40 mAU/mL. The fact that these patients presented normal serum tumor markers means that they are ineligible for any assessments other than imaging. By contrast, the methylation indexes in this study are applicable to all patients.
DNA methylation is an important epigenetic phenomenon that manages gene expression in every phase of carcinogenesis. Numerous studies have reported that in many types of cancer, hypermethylation downregulates the expression of tumor suppressor genes or DNA repair genes, while hypomethylation upregulates various oncogenes [
14,
15]. This means that the aberrant methylation of genes could potentially be used as an indicator of cancer for diagnosis and prognosis prediction [
29]. This is the first study to explore the possibility of using methylation markers to assess the therapeutic response to LRT in HCC patients. The MMTR index based on 10 DNA methylation profiles was shown to vary consistently with the response to LRT among all HCC patients in a clinical setting. Overall, the proposed index performed at least as well as AFP and PIVKA-II in terms of prediction ability. Combining the proposed index with conventional tumor markers resulted in outstanding prediction ability (AUC = 0.880) with good sensitivity (75.0%) and specificity (66.7%).
BCLC guidelines recommend LRT as a standard treatment for patients with intermediate-stage (BCLC B stage); however, the high degree of variability in this group (in terms of tumor burden, biologic behavior, and liver function) can make it very difficult to characterize the therapeutic response to LRT or formulate a reliable prognosis. It is essential that physicians have the ability to identify patients for whom LRT would provide no benefit and those who are at risk of early progression to late-stage cancer, thereby making it possible to initiate alternative systemic therapies [
30,
31]. Researchers have compiled an extensive list of factors that are correlated with HCC recurrence, including tumor size, satellite tumor, capsular integrity, proximity to large vessels, vascular invasion, partial necrosis, AFP level, platelet count, antiviral treatment, and viral etiology [
8,
32]. In the current study, we sought to identify biomarkers associated with DNA methylation with which to formulate prognostic predictions for LRT.
This was achieved by constructing a methylation assessment model (MMTR) for LRT and a methylation prognostic model before therapy (MMEP) based on 10 methylation regions RASSF1A, miR-203, COX2, APC, ALX3, TBX4, TSPYL5, cg12582777, cg12714719, and cg08643930. In a previous study, we demonstrated the correlation between HCC and RASSF1A, miR-203, APC, and COX2 [
25]. All three of these genes and one microRNA present the characteristics of tumor suppressors and have an outstanding ability to identify HCC at an early stage. It is also possible that these genes could be used as prognostic markers by which to predict the survival of HCC patients with a high degree of specificity. ALX3 is a member of the homeobox family with oncogenic potential in cervical squamous cell carcinoma through the transactivation of CDC25A by recruiting lysine demethylase 2B [
33]. The methylation of ALX3 has been associated with neuroblastoma, colorectal carcinoma, and HCC [
34,
35]. TBX4 down-regulation is an independent prognostic marker for survival in patients with stage II pancreatic ductal adenocarcinoma [
36]. TBX4 hypermethylation has been observed in bladder cancer and lung cancer [
37,
38]. TSPYL5 repression via DNA methylation is frequently associated with cancer, including endometrioid endometrial adenocarcinoma, malignant glioma, gastric cancer, prostate cancer, and HCC [
39,
40,
41,
42,
43]. The expression of TSPYL5 can be used as a prognostic indicator for gastric cancer and breast cancer [
44]. This work extends the clinical application of these methylation markers to HCC.
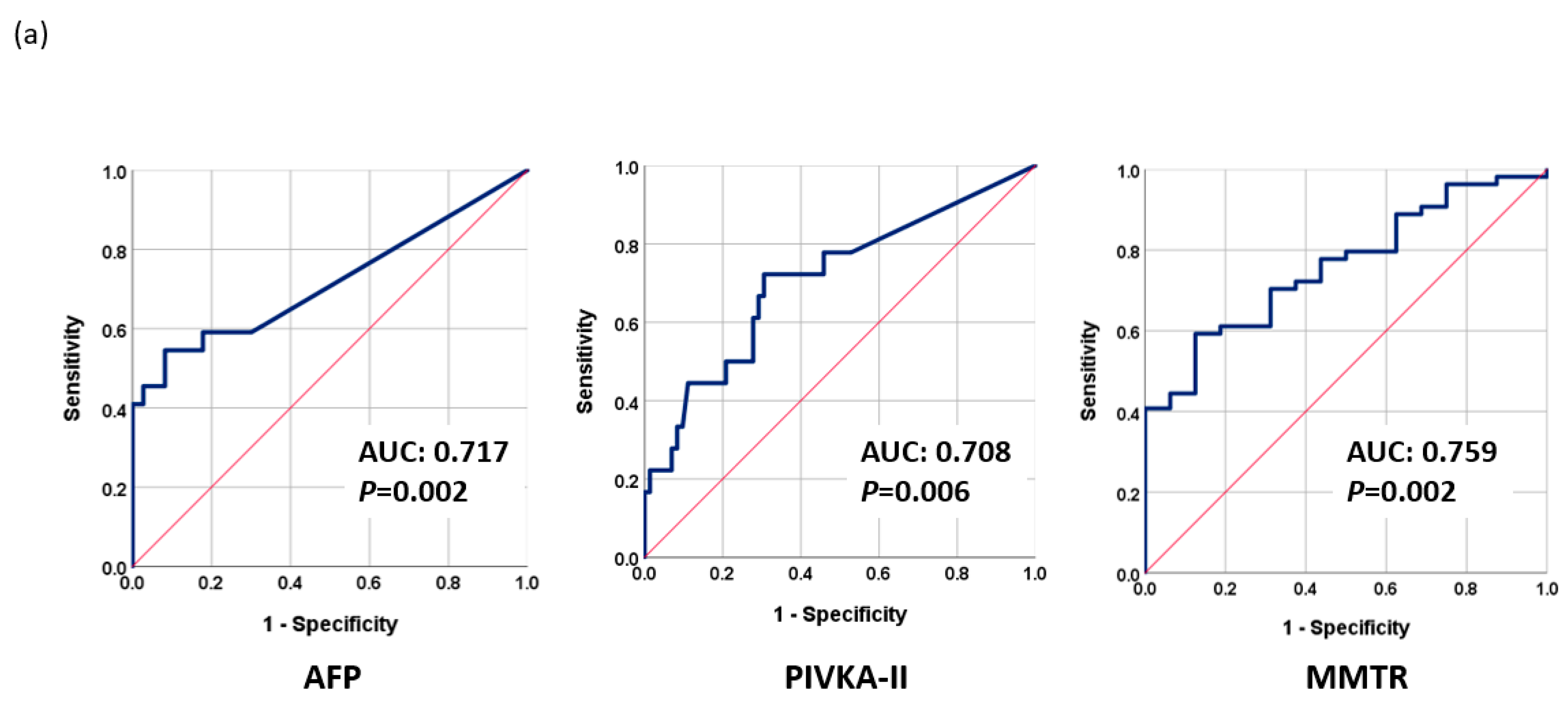
AFP is the most widely used marker for HCC surveillance due to its close association with tumor differentiation, vascular invasion, and progression of HCC tumors. Overall, we determined that AFP was more effective than PIVKA-II in predicting the response to LRT; however, the proposed MMTR index (AUC = 0.759,
p = 0.002) outperformed both AFP (AUC = 0.717,
p = 0.002) and PIVKA-II (AUC = 0.708,
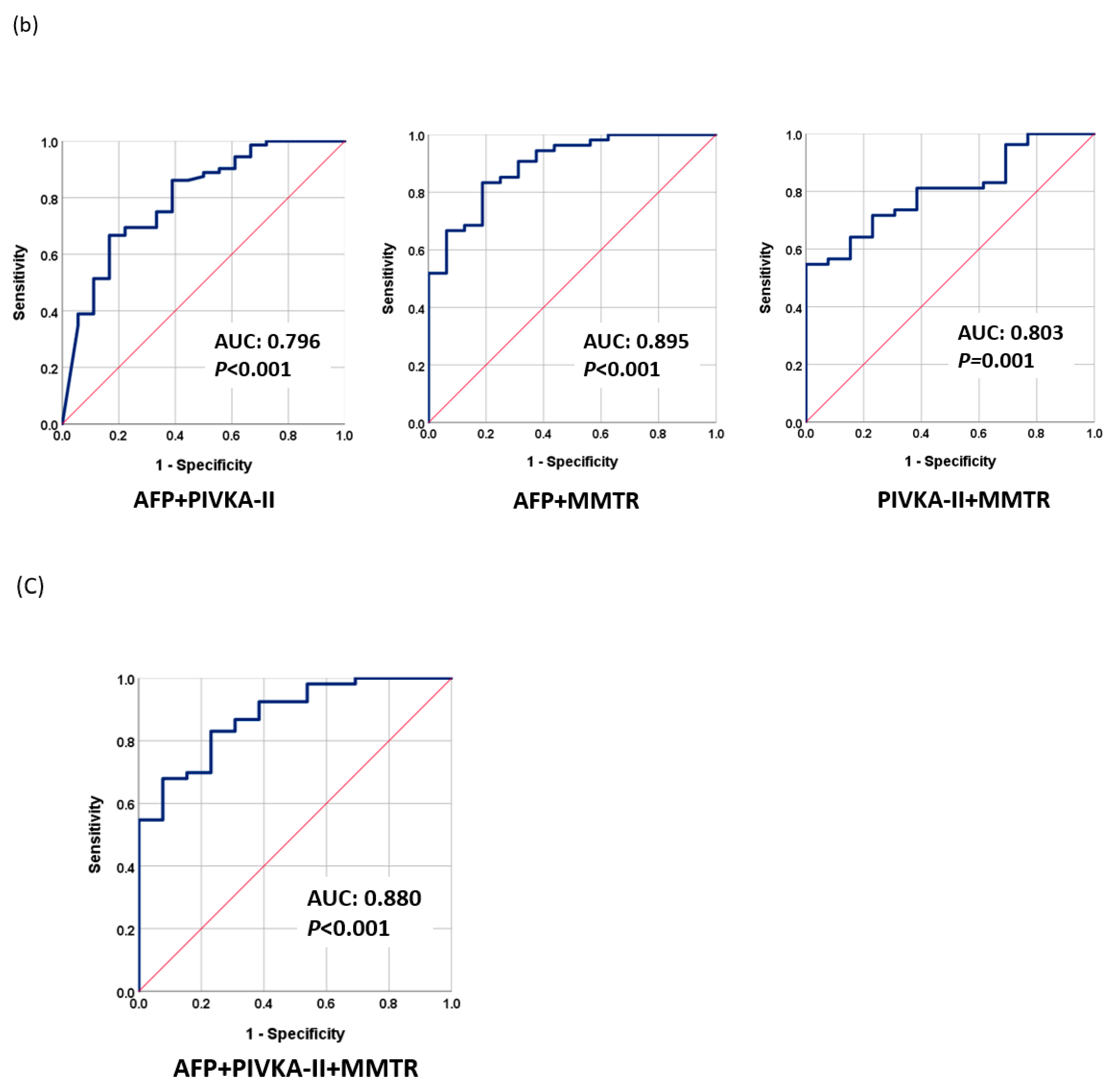
p = 0.006). As shown in
Figure 2, the high AUC values obtained by combining MMTR + AFP (0.895), MMTR + PIVKA-II (0.803), and MMTR + AFP + PIVKA-II (0.880) indicate that the overall most effective approach to predicting the treatment response involved combining the analysis results of AFP and methylation markers.
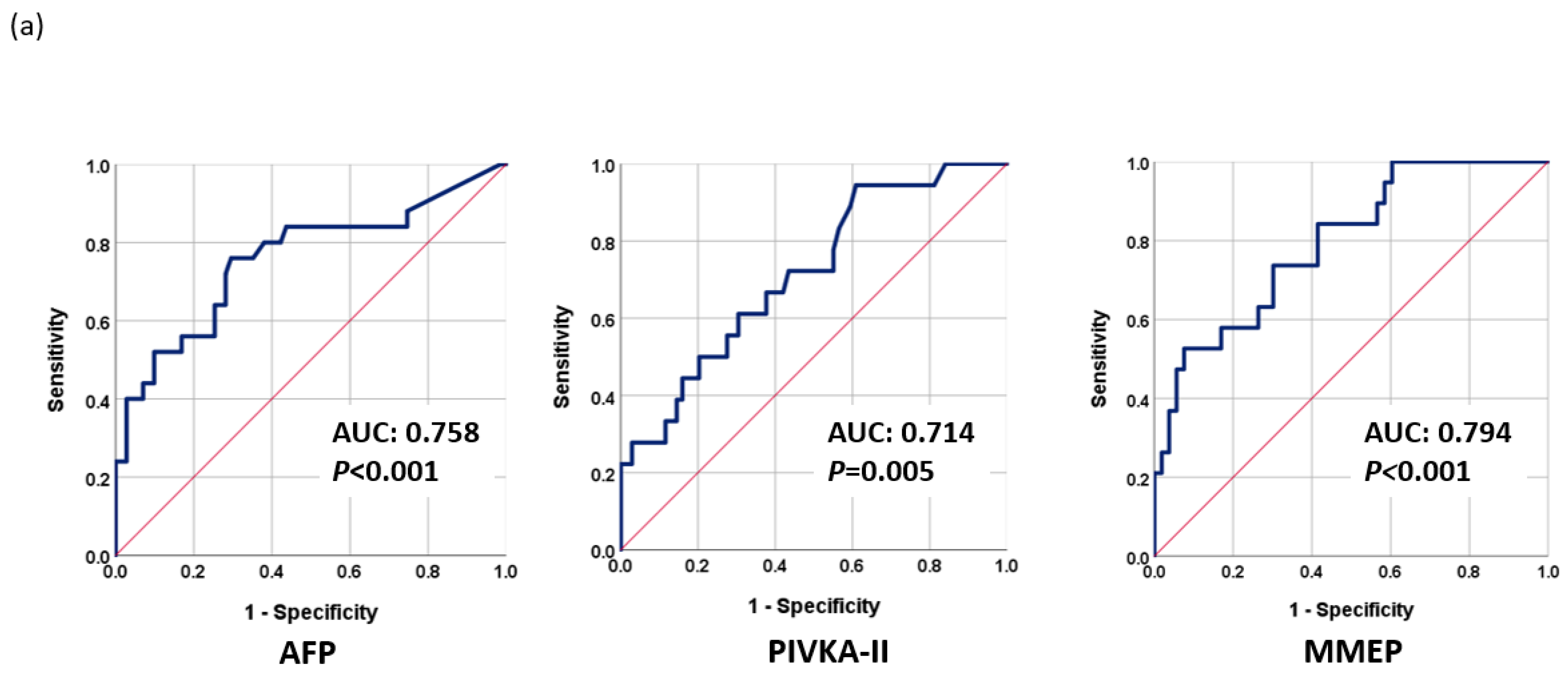
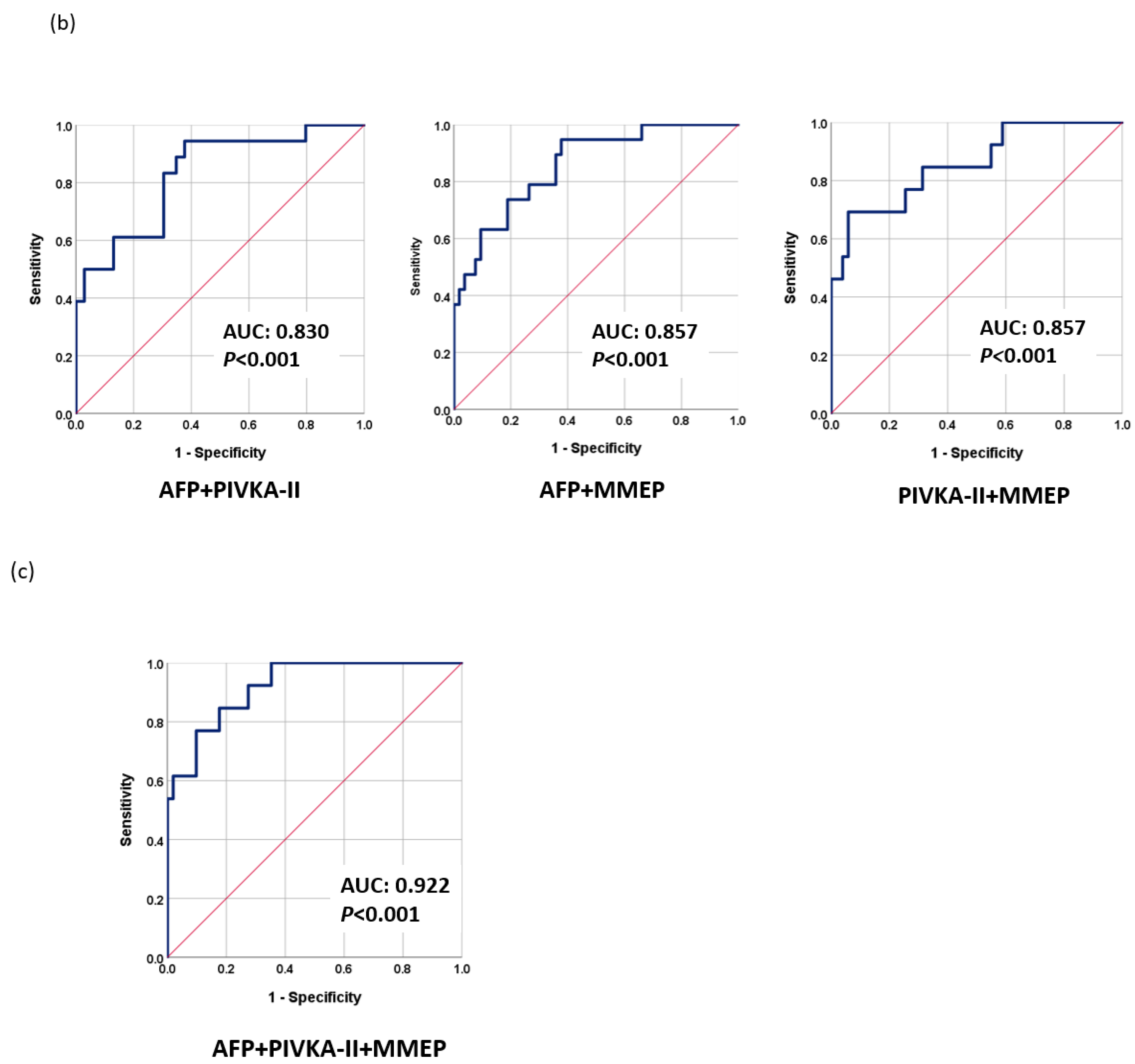
Our clinical data revealed that 26.4% of patients rapidly progressed to the late stage soon after LRT. It is possible that this can be attributed to the limitations of imaging tools and the shortcomings of current serum markers in formulating pre-operative evaluations. In predicting the prognosis prior to treatment, methylation markers proved superior to AFP or PIVKA-II (
Figure 3). Combining MMEP + AFP or PIVKA-II resulted in similar prediction performance (AUC = 0.857); however, combining MMEP + AFP + PIVKA-II resulted in a very high AUC of 0.922 (
p < 0.001). These results may reflect the biological characteristics of methylation markers, whose levels change very early (i.e., before the appearance of symptoms). The integration of both information from image tools and effective biomarkers provides a precise assessment tool for surveillance and prognosis and could help physicians make a more effective treatment strategy, including an earlier application of adjuvant therapy and more frequent monitoring.
In acknowledging the limitations of our study, it is important to note that the sample size is indeed limited, which could potentially impact the generalizability of our findings. This is a significant constraint that future research should seek to address by including a more extensive patient cohort. Additionally, our study did not incorporate an external validation cohort, which might have strengthened the reliability and applicability of our results. Future studies would benefit from incorporating such a validation set to bolster the robustness of the findings.

 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}