
Free-Breathing StarVIBE Sequence for the Detection of Extranodal Extension in Head and Neck Cancer: An Image Quality and Diagnostic Performance Study

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
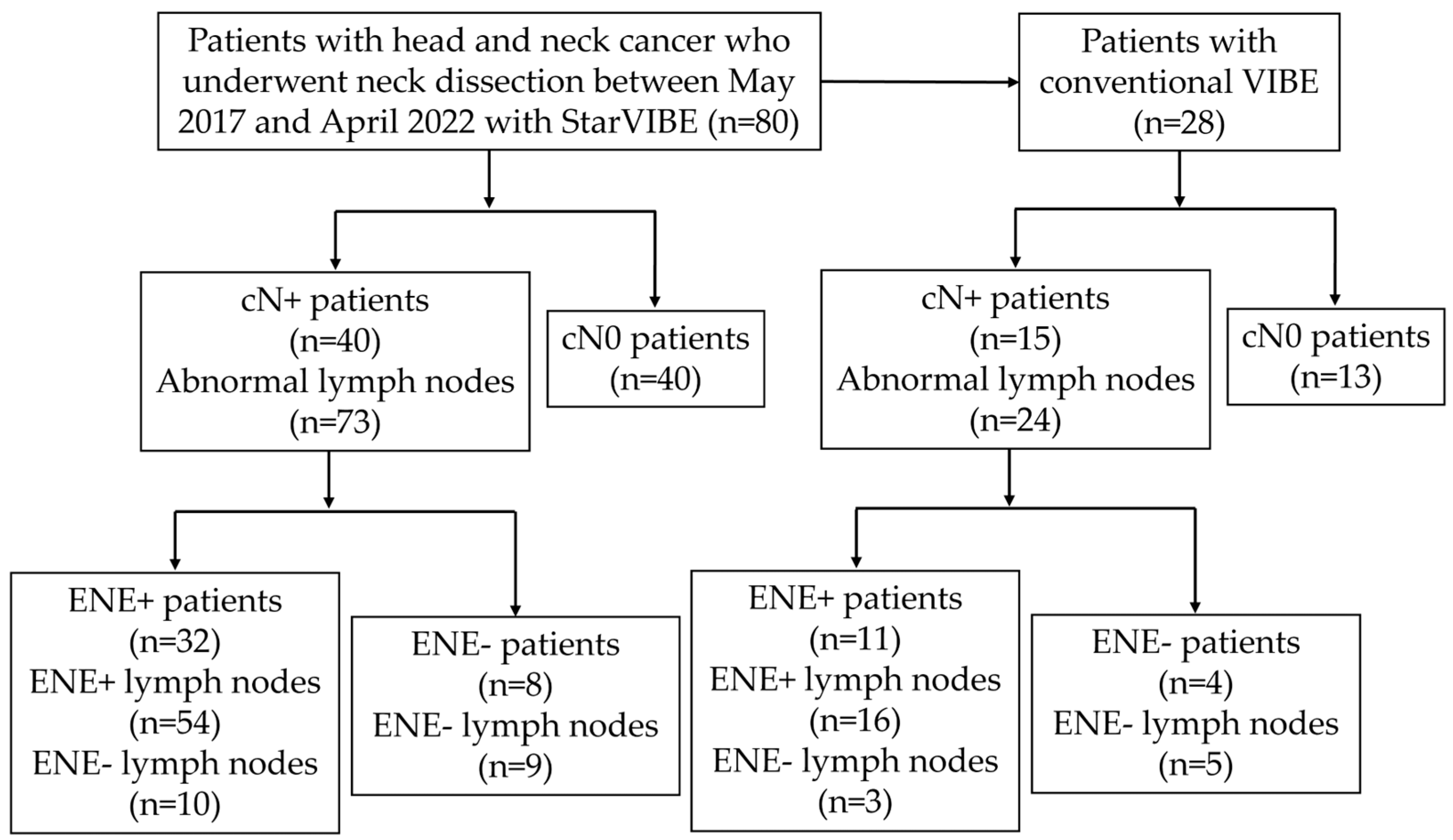
2.1. Patient Selection
2.2. MRI Acquisition
2.3. Radiological Assessment
2.4. Matching to Pathologic Examination
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Comparison between StarVIBE and VIBE
3.3. Association of MR Features with Histologically Confirmed ENE
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gau, M.; Fonseca, A.; Ozsahin, M.; Fayette, J.; Poupart, M.; Roux, P.E.; Schütz, F.; Zrounba, P.; Grégoire, V. Prognostic impact of extranodal extension in resected head and neck squamous cell carcinomas in the era of postoperative chemoradiation: A retrospective monocentric study. Oral Oncol. 2021, 123, 105605. [Google Scholar] [CrossRef]
- De Juan, J.; García, J.; López, M.; Orús, C.; Esteller, E.; Quer, M.; León, X. Inclusion of extracapsular spread in the pTNM classification system: A proposal for patients with head and neck carcinoma. JAMA Otolaryngol. Head Neck Surg. 2013, 139, 483–488. [Google Scholar] [CrossRef]
- Majercakova, K.; Valero, C.; López, M.; García, J.; Farré, N.; Quer, M.; León, X. Postoperative staging of the neck dissection using extracapsular spread and lymph node ratio as prognostic factors in HPV-negative head and neck squamous cell carcinoma patients. Oral Oncol. 2018, 77, 37–42. [Google Scholar] [CrossRef]
- Gal, T.J.; O’Brien, K.J.; Chen, Q.; Huang, B. Clinical vs Microscopic Extranodal Extension and Survival in Oropharyngeal Carcinoma in the Human Papillomavirus Era. Otolaryngol. Head Neck Surg. 2020, 162, 693–701. [Google Scholar] [CrossRef]
- Quinton, B.A.; Cabrera, C.I.; Tamaki, A.; Li, S.; Fowler, N.; Rezaee, R.; Lavertu, P.; Teknos, T.; Pan, Q.; Thuener, J. The impact of microscopic versus macroscopic extranodal extension in oral cavity squamous cell carcinoma: National cancer database analysis and review of the literature. Am. J. Otolaryngol. 2022, 43, 103511. [Google Scholar] [CrossRef]
- Mahajan, A.; Chand, A.; Agarwal, U.; Patil, V.; Vaish, R.; Noronha, V.; Joshi, A.; Kapoor, A.; Sable, N.; Ahuja, A.; et al. Prognostic Value of Radiological Extranodal Extension Detected by Computed Tomography for Predicting Outcomes in Patients with Locally Advanced Head and Neck Squamous Cell Cancer Treated with Radical Concurrent Chemoradiotherapy. Front. Oncol. 2022, 12, 814895. [Google Scholar] [CrossRef]
- Fan, K.H.; Yeh, C.H.; Hung, S.P.; Kang, C.J.; Huang, S.F.; Chang, K.P.; Wang, H.M.; Chia-Hsun Hsieh, J.; Lin, C.Y.; Cheng, A.J.; et al. Prognostic value of radiologic extranodal extension in patients with hypopharyngeal cancer treated with primary chemoradiation. Radiother. Oncol. 2021, 156, 217–222. [Google Scholar] [CrossRef]
- Kiong, K.L.; Bell, D.; Yao, C.M.; Ferrarotto, R.; Lewis, C.M. Multifocal regression and pathologic response predicts recurrence after neoadjuvant chemotherapy in head and neck squamous cell carcinoma. Oral Oncol. 2021, 122, 105520. [Google Scholar] [CrossRef]
- Park, S.I.; Guenette, J.P.; Suh, C.H.; Hanna, G.J.; Chung, S.R.; Baek, J.H.; Lee, J.H.; Choi, Y.J. The diagnostic performance of CT and MRI for detecting extranodal extension in patients with head and neck squamous cell carcinoma: A systematic review and diagnostic meta-analysis. Eur. Radiol. 2021, 31, 2048–2061. [Google Scholar] [CrossRef]
- Abdel-Halim, C.N.; Rosenberg, T.; Dyrvig, A.K.; Høilund-Carlsen, P.F.; Sørensen, J.A.; Rohde, M.; Godballe, C. Diagnostic accuracy of imaging modalities in detection of histopathological extranodal extension: A systematic review and meta-analysis. Oral Oncol. 2021, 114, 105169. [Google Scholar] [CrossRef]
- Jan, W.D.; Frank, A.P. Radiological assessment of extranodal extension in patients with head and neck squamous cell carcinoma. J. Cancer Metastasis Treat. 2021, 7, 56. [Google Scholar] [CrossRef]
- King, A.D.; Tse, G.M.; Yuen, E.H.; To, E.W.; Vlantis, A.C.; Zee, B.; Chan, A.B.; van Hasselt, A.C.; Ahuja, A.T. Comparison of CT and MR imaging for the detection of extranodal neoplastic spread in metastatic neck nodes. Eur. J. Radiol. 2004, 52, 264–270. [Google Scholar] [CrossRef]
- Kimura, Y.; Sumi, M.; Sakihama, N.; Tanaka, F.; Takahashi, H.; Nakamura, T. MR imaging criteria for the prediction of extranodal spread of metastatic cancer in the neck. AJNR Am. J. Neuroradiol. 2008, 29, 1355–1359. [Google Scholar] [CrossRef] [PubMed]
- Frood, R.; Palkhi, E.; Barnfield, M.; Prestwich, R.; Vaidyanathan, S.; Scarsbrook, A. Can MR textural analysis improve the prediction of extracapsular nodal spread in patients with oral cavity cancer? Eur. Radiol. 2018, 28, 5010–5018. [Google Scholar] [CrossRef]
- Lodder, W.L.; Lange, C.A.; van Velthuysen, M.L.; Hauptmann, M.; Balm, A.J.; van den Brekel, M.W.; Pameijer, F.A. Can extranodal spread in head and neck cancer be detected on MR imaging. Oral Oncol. 2013, 49, 626–633. [Google Scholar] [CrossRef]
- Shaw, R.J.; Lowe, D.; Woolgar, J.A.; Brown, J.S.; Vaughan, E.D.; Evans, C.; Lewis-Jones, H.; Hanlon, R.; Hall, G.L.; Rogers, S.N. Extracapsular spread in oral squamous cell carcinoma. Head Neck 2010, 32, 714–722. [Google Scholar] [CrossRef]
- Ding, Y.; Rao, S.X.; Chen, C.Z.; Li, R.C.; Zeng, M.S. Usefulness of two-point Dixon fat-water separation technique in gadoxetic acid-enhanced liver magnetic resonance imaging. World J. Gastroenterol. 2015, 21, 5017–5022. [Google Scholar] [CrossRef] [PubMed]
- Song, H.K.; Dougherty, L. Dynamic MRI with projection reconstruction and KWIC processing for simultaneous high spatial and temporal resolution. Magn. Reson. Med. 2004, 52, 815–824. [Google Scholar] [CrossRef]
- Chandarana, H.; Block, T.K.; Rosenkrantz, A.B.; Lim, R.P.; Kim, D.; Mossa, D.J.; Babb, J.S.; Kiefer, B.; Lee, V.S. Free-breathing radial 3D fat-suppressed T1-weighted gradient echo sequence: A viable alternative for contrast-enhanced liver imaging in patients unable to suspend respiration. Investig. Radiol. 2011, 46, 648–653. [Google Scholar] [CrossRef] [PubMed]
- Vermersch, M.; Emsen, B.; Monnet, A.; Chalaye, J.; Galletto Pregliasco, A.; Baranes, L.; Rahmouni, A.; Luciani, A.; Itti, E.; Mulé, S. Chest PET/MRI in Solid Cancers: Comparing the Diagnostic Performance of a Free-Breathing 3D-T1-GRE Stack-of-Stars Volume Interpolated Breath-Hold Examination (StarVIBE) Acquisition with That of a 3D-T1-GRE Volume Interpolated Breath-Hold Examination (VIBE) for Chest Staging During Whole-Body PET/MRI. J. Magn. Reson. Imaging 2022, 55, 1683–1693. [Google Scholar] [CrossRef]
- Wang, Z.; Guo, J.; Qin, J.; Zhang, H.; Zhao, Y.; Lu, Y.; Yan, X.; Zhang, F.; Zhang, Z.; Zhang, T.; et al. Accuracy of 3-T MRI for Preoperative T Staging of Esophageal Cancer After Neoadjuvant Chemotherapy, With Histopathologic Correlation. AJR Am. J. Roentgenol. 2019, 212, 788–795. [Google Scholar] [CrossRef]
- Duffy, P.B.; Stemmer, A.; Callahan, M.J.; Cravero, J.P.; Johnston, P.R.; Warfield, S.K.; Bixby, S.D. Free-breathing radial stack-of-stars three-dimensional Dixon gradient echo sequence in abdominal magnetic resonance imaging in sedated pediatric patients. Pediatr. Radiol. 2021, 51, 1645–1653. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.; Li, X.; Jia, F.; Ye, Z.; Ning, G.; Liu, S.; Li, P.; Fu, C.; Li, Q.; Wang, S.; et al. Optimization of the image contrast for the developing fetal brain using 3D radial VIBE sequence in 3 T magnetic resonance imaging. BMC Med. Imaging 2022, 22, 11. [Google Scholar] [CrossRef] [PubMed]
- Mermod, M.; Tolstonog, G.; Simon, C.; Monnier, Y. Extracapsular spread in head and neck squamous cell carcinoma: A systematic review and meta-analysis. Oral Oncol. 2016, 62, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.R.; Hudgins, P.A.; Beitler, J.J.; Magliocca, K.R.; Griffith, C.C.; Liu, Y.; Bougnon, K.; El-Deiry, M.; Saba, N.F.; Aiken, A.H. Radiographic Imaging Does Not Reliably Predict Macroscopic Extranodal Extension in Human Papilloma Virus-Associated Oropharyngeal Cancer. ORL J. Otorhinolaryngol. Relat. Spec. 2018, 80, 85–95. [Google Scholar] [CrossRef]
- Faraji, F.; Aygun, N.; Coquia, S.F.; Gourin, C.G.; Tan, M.; Rooper, L.M.; Eisele, D.W.; Fakhry, C. Computed tomography performance in predicting extranodal extension in HPV-positive oropharynx cancer. Laryngoscope 2020, 130, 1479–1486. [Google Scholar] [CrossRef]
- Carlton, J.A.; Maxwell, A.W.; Bauer, L.B.; McElroy, S.M.; Layfield, L.J.; Ahsan, H.; Agarwal, A. Computed tomography detection of extracapsular spread of squamous cell carcinoma of the head and neck in metastatic cervical lymph nodes. Neuroradiol. J. 2017, 30, 222–229. [Google Scholar] [CrossRef]
- Geltzeiler, M.; Clayburgh, D.; Gleysteen, J.; Gross, N.D.; Hamilton, B.; Andersen, P.; Brickman, D. Predictors of extracapsular extension in HPV-associated oropharyngeal cancer treated surgically. Oral Oncol. 2017, 65, 89–93. [Google Scholar] [CrossRef]
- Tran, N.A.; Palotai, M.; Hanna, G.J.; Schoenfeld, J.D.; Bay, C.P.; Rettig, E.M.; Bunch, P.M.; Juliano, A.F.; Kelly, H.R.; Suh, C.H.; et al. Diagnostic performance of computed tomography features in detecting oropharyngeal squamous cell carcinoma extranodal extension. Eur. Radiol. 2023, 33, 3693–3703. [Google Scholar] [CrossRef]
- Kim, S.; Park, H.; Yeou, S.H.; Roh, J.; Shin, Y.S.; Kim, C.H.; Ha, E.J.; Jang, J.Y. Assessment of Radiologic Extranodal Extension Using Combinatorial Analysis of Nodal Margin Breakdown and Metastatic Burden in Oropharyngeal Cancer. Cancers 2023, 15, 3276. [Google Scholar] [CrossRef]
- Ma, H.; Qiu, Y.; Li, H.; Xie, F.; Ruan, G.; Liu, L.; Cui, C.; Dong, A. Prognostic Value of Nodal Matting on MRI in Nasopharyngeal Carcinoma Patients. J. Magn. Reson. Imaging 2021, 53, 152–164. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Lu, T.; Huang, S.H.; Lin, S.; Chen, Y.; Fang, Y.; Zhou, H.; Chen, Y.; Zong, J.; Zhang, Y.; et al. High-grade radiologic extra-nodal extension predicts distant metastasis in stage II nasopharyngeal carcinoma. Head Neck 2019, 41, 3317–3327. [Google Scholar] [CrossRef] [PubMed]
- Lu, T.; Hu, Y.; Xiao, Y.; Guo, Q.; Huang, S.H.; O’Sullivan, B.; Fang, Y.; Zong, J.; Chen, Y.; Lin, S.; et al. Prognostic value of radiologic extranodal extension and its potential role in future N classification for nasopharyngeal carcinoma. Oral Oncol. 2019, 99, 104438. [Google Scholar] [CrossRef]
- Vainshtein, J.M.; Spector, M.E.; Ibrahim, M.; Bradford, C.R.; Wolf, G.T.; Stenmark, M.H.; Worden, F.P.; McHugh, J.B.; Prince, M.E.; Carey, T.; et al. Matted nodes: High distant-metastasis risk and a potential indication for intensification of systemic therapy in human papillomavirus-related oropharyngeal cancer. Head Neck 2016, 38 (Suppl. S1), E805–E814. [Google Scholar] [CrossRef] [PubMed]
- Spector, M.E.; Chinn, S.B.; Bellile, E.; Gallagher, K.K.; Ibrahim, M.; Vainshtein, J.; Chanowski, E.J.; Walline, H.M.; Moyer, J.S.; Prince, M.E.; et al. Matted nodes as a predictor of distant metastasis in advanced-stage III/IV oropharyngeal squamous cell carcinoma. Head Neck 2016, 38, 184–190. [Google Scholar] [CrossRef]
- De Bree, R.; Ljumanovic, R.; Hazewinkel, M.J.; Witte, B.I.; Castelijns, J.A. Radiologic extranodal spread and matted nodes: Important predictive factors for development of distant metastases in patients with high-risk head and neck cancer. Head Neck 2016, 38 (Suppl. S1), E1452–E1458. [Google Scholar] [CrossRef]
- Spector, M.E.; Gallagher, K.K.; Light, E.; Ibrahim, M.; Chanowski, E.J.; Moyer, J.S.; Prince, M.E.; Wolf, G.T.; Bradford, C.R.; Cordell, K.; et al. Matted nodes: Poor prognostic marker in oropharyngeal squamous cell carcinoma independent of HPV and EGFR status. Head Neck 2012, 34, 1727–1733. [Google Scholar] [CrossRef]
- Sabiq, F.; Huang, K.; Patel, A.; Banerjee, R.; Debenham, B.; Lau, H.; Skarsgard, D.; Chen, G.; Lysack, J.T.; Quon, H.C. Novel imaging classification system of nodal disease in human papillomavirus-mediated oropharyngeal squamous cell carcinoma prognostic of patient outcomes. Head Neck 2021, 43, 1854–1863. [Google Scholar] [CrossRef]
- Burningham, K.; Moore, W.; Moon, D.; Avkshtol, V.; Day, A.T.; Sumer, B.; Vo, D.; Bishop, J.A.; Hughes, R.; Sher, D.J. Prognostic impact of matted lymphadenopathy in patients with oropharyngeal squamous cell carcinoma treated with definitive chemoradiotherapy. Oral Oncol. 2021, 123, 105623. [Google Scholar] [CrossRef]
- Prabhu, R.S.; Magliocca, K.R.; Hanasoge, S.; Aiken, A.H.; Hudgins, P.A.; Hall, W.A.; Chen, S.A.; Eaton, B.R.; Higgins, K.A.; Saba, N.F.; et al. Accuracy of computed tomography for predicting pathologic nodal extracapsular extension in patients with head-and-neck cancer undergoing initial surgical resection. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 122–129. [Google Scholar] [CrossRef]
- Almulla, A.; Noel, C.W.; Lu, L.; Xu, W.; O’Sullivan, B.; Goldstein, D.P.; Hope, A.; Perez-Ordonez, B.; Weinreb, I.; Irish, J.; et al. Radiologic-Pathologic Correlation of Extranodal Extension in Patients with Squamous Cell Carcinoma of the Oral Cavity: Implications for Future Editions of the TNM Classification. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 698–708. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | n = 80 |
|---|---|
| Age, yrs (Mean ± SD) | 61.1 ± 11.8 |
| Gender | |
| Male | 67 (84%) |
| Female | 13 (16%) |
| Primary tumor site | |
| Oral cavity | 24 (30%) |
| Oropharynx | 1 (1%) |
| Larynx | 16 (20%) |
| Hypopharynx | 25 (31%) |
| Salivary gland | 4 (5%) |
| pT | |
| T1 | 5 (6%) |
| T2 | 28 (35%) |
| T3 | 21 (26%) |
| T4 | 26 (33%) |
| StarVIBE | VIBE | p-Value | ICC (95%CI) | |
|---|---|---|---|---|
| Overall image quality | 5 (1) | 3 (1) | <0.001 * | 0.90 (0.82–0.94) |
| Motion artifacts | 5 (0) | 4 (1) | <0.001 * | 0.90 (0.83–0.94) |
| Aliasing artifacts | 5 (0) | 4 (1) | <0.001 * | 0.92 (0.87–0.96) |
| SNR | 23.7 ± 9.8 | 15.1 ± 5.6 | 0.001 * | 0.51 (0.26–0.69) |
| CNR | 5.7 ± 3.2 | 3.0 ± 2.3 | <0.001 * | 0.79 (0.65–0.88) |
| ENE− (n = 8) | ENE+ (n = 32) | p-Value | |
|---|---|---|---|
| Age, yrs (Mean ± SD) | 57.3 ± 16.0 | 62.1 ± 10.5 | 0.44 |
| Gender | 0.53 | ||
| Male | 6 (75%) | 27 (84%) | |
| Female | 2 (25%) | 5 (16%) | |
| Primary tumor site | 0.09 | ||
| Oral cavity | 6 (75%) | 9 (28%) | |
| Larynx (Supraglottic) | 0 (0%) | 5 (16%) | |
| Hypopharynx | 2 (25%) | 15 (47%) | |
| Submandibular gland | 0 (0%) | 3 (9%) | |
| pT | 0.28 | ||
| T1 | 0 | 4 (13%) | |
| T2 | 2 (25%) | 10 (31) | |
| T3 | 1 (13%) | 9 (28%) | |
| T4 | 5 (63%) | 9 (28%) |
| Pathologic ENE | |||||
|---|---|---|---|---|---|
| No | Yes | Sensitivity | Specificity | Accuracy | |
| Irregular nodal margins | |||||
| No | 14 | 40 | 0.26 (0.15–0.40) | 0.74 (0.49–0.91) | 0.38 (0.27–0.50) |
| Yes | 5 | 14 | |||
| Invading adjacent planes | |||||
| No | 19 | 25 | 0.54 (0.40–0.67) | 1.00 (0.82–1.00) | 0.66 (0.54–0.76) |
| Yes | 0 | 29 | |||
| Nodal necrosis | |||||
| No | 11 | 14 | 0.74 (0.60–0.85) | 0.58 (0.34–0.80) | 0.70 (0.58–0.80) |
| Yes | 8 | 40 | |||
| Matted nodes | |||||
| No | 17 | 15 | 0.72 (0.58–0.84) | 0.89 (0.67–0.99) | 0.77 (0.65–0.86) |
| Yes | 2 | 39 | |||
| Size > 14.8 mm | |||||
| No | 17 | 14 | 0.74 (0.60–0.85) | 0.89 (0.67–0.99) | 0.78 (0.67–0.87) |
| Yes | 2 | 40 | |||
| Invading adjacent planes + matted nodes | |||||
| No | 17 | 4 | 0.93 (0.82–0.98) | 0.89 (0.67–0.99) | 0.92 (0.83–0.97) |
| Yes | 2 | 50 | |||
| Variables | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Irregular nodal margins | 0.98 | 0.30–3.22 | 0.98 | 0.31 | 0.02–5.00 | 0.41 |
| Invading adjacent planes | Inf. * | N/A | Inf. * | N/A | ||
| Nodal necrosis | 3.93 | 1.31–11.75 | 0.01 | 5.45 | 0.52–56.70 | 0.16 |
| Matted nodes | 22.10 | 4.55–107.46 | <0.001 | 57.52 | 3.48–951.95 | 0.005 |
| Long axial diameter | 1.36 | 1.14–1.62 | 0.001 | 1.11 | 0.81–1.52 | 0.51 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qu, J.; Su, T.; Pan, B.; Zhang, T.; Chen, X.; Zhu, X.; Chen, Y.; Zhang, Z.; Jin, Z. Free-Breathing StarVIBE Sequence for the Detection of Extranodal Extension in Head and Neck Cancer: An Image Quality and Diagnostic Performance Study. Cancers 2023, 15, 4992. https://doi.org/10.3390/cancers15204992
Qu J, Su T, Pan B, Zhang T, Chen X, Zhu X, Chen Y, Zhang Z, Jin Z. Free-Breathing StarVIBE Sequence for the Detection of Extranodal Extension in Head and Neck Cancer: An Image Quality and Diagnostic Performance Study. Cancers. 2023; 15(20):4992. https://doi.org/10.3390/cancers15204992
Chicago/Turabian StyleQu, Jiangming, Tong Su, Boju Pan, Tao Zhang, Xingming Chen, Xiaoli Zhu, Yu Chen, Zhuhua Zhang, and Zhengyu Jin. 2023. "Free-Breathing StarVIBE Sequence for the Detection of Extranodal Extension in Head and Neck Cancer: An Image Quality and Diagnostic Performance Study" Cancers 15, no. 20: 4992. https://doi.org/10.3390/cancers15204992
APA StyleQu, J., Su, T., Pan, B., Zhang, T., Chen, X., Zhu, X., Chen, Y., Zhang, Z., & Jin, Z. (2023). Free-Breathing StarVIBE Sequence for the Detection of Extranodal Extension in Head and Neck Cancer: An Image Quality and Diagnostic Performance Study. Cancers, 15(20), 4992. https://doi.org/10.3390/cancers15204992