

The Role of Mucin Expression in the Diagnosis of Oesophago-Gastric Cancer: A Systematic Literature Review

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
1.1. Current Technologies in Early Diagnosis of Oesophago-Gastric Cancer
1.2. The Structure and Function of Mucins
1.3. Mucins in Tumourigenesis
1.4. Methodologies in the Analysis of Mucin Expression in Oesophago-Gastric Tissue
2. Materials and Methods
2.1. Search Strategy
2.2. Data Extraction
2.3. Study Quality and Risk of Bias Assessments
2.4. Data Availability
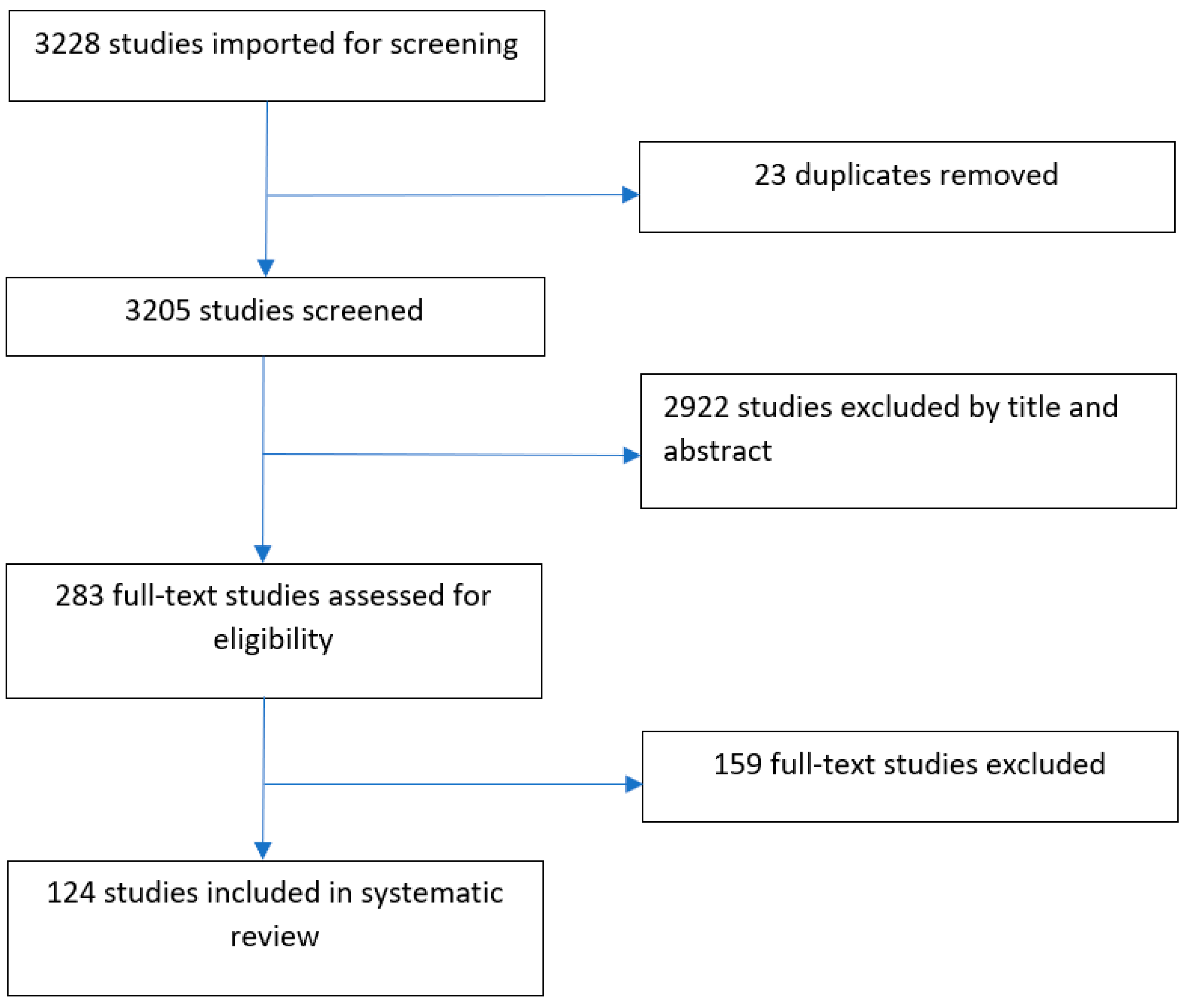
3. Results
4. Discussion
4.1. Oesophageal Squamous Cell Carcinoma
4.2. Oesophageal Adenocarcinoma
4.3. Gastric Adenocarcinoma
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Patruni, S.; Fayyaz, F.; Bien, J.; Phillip, T.; King, D.A. Immunotherapy in the Management of Oesophagogastric Cancer: A Practical Review. JCO Oncol. Pract. 2023, 19, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Butt, M.A.; Pye, H.; Haidry, R.J.; Oukrif, D.; Khan, S.-U.-R.; Puccio, I.; Gandy, M.; Reinert, H.W.; Bloom, E.; Rashid, M.; et al. Upregulation of mucin glycoprotein MUC1 in the progression to oesophageal adenocarcinoma and therapeutic potential with a targeted photoactive antibody-drug conjugate. Oncotarget 2017, 8, 25080–25096. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Park, M.H.; Wahedally, M.A.H.; Maynard, N.; Crosby, T.; Thomas, B.; Trudgill, N.; Geisler, J.; Napper, R.; Cromwell, D. National Oesophago-Gastric Cancer Audit; 2022 Annual Report; The Royal College of Surgeons of England: London, UK, 2023. [Google Scholar]
- Bird-Lieberman, E.L.; Fitzgerald, R.C. Early diagnosis of oesophageal cancer. Br. J. Cancer 2009, 101, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Rahman, S.; Thomas, B.; Maynard, N.; Park, M.H.; Wahedally, M.; Trudgill, N.; Crosby, T.; Cromwell, D.A.; Underwood, T. J Impact of postoperative chemotherapy on survival for oesophagogastric adenocarcinoma after preoperative chemotherapy and surgery. Br. J. Surg. 2022, 109, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Arnal, M.J.D.; Arenas, A.F.; Arbeloa, A.L. Esophageal cancer: Risk factors, screening and endoscopic treatment in Western and Eastern countries. World J. Gastroenterol. 2015, 21, 7933–7943. [Google Scholar] [CrossRef]
- Machlowska, J.; Baj, R.; Sitarz, M.; Maciejewski, R.; Sitarz, R. Gastric Cancer: Epidemiology, Risk Factors, Classification, Genomic Characteristics and Treatment Strategies. Int. J. Mol. Sci. 2020, 21, 4012. [Google Scholar] [CrossRef]
- Fitzgerald, R.C.; di Pietro, M.; O’Donovan, M.; Maroni, R.; Muldrew, B.; Debiram-Beecham, I.; Gehrung, M.; Offman, J.; Tripathi, M.; Smith, S.G.; et al. Cytosponge-trefoil factor 3 versus usual care to identify Barrett’s oesophagus in a primary care setting: A multicentre, pragmatic, randomised controlled trial. Lancet 2020, 396, 333–344. [Google Scholar] [CrossRef]
- Ross-Innes, C.S.; Debiram-Beecham, I.; O’Donovan, M.; Walker, E.; Varghese, S.; Lao-Sirieix, P.; Lovt, L.; Griffin, M.; Ragunath, K.; Haidry, R.; et al. Evaluation of a minimally invasive cell sampling device coupled with assessment of trefoil factor 3 expression for diagnosing Barrett’s oesophagus: A multi-center case-control study. PLoS Med. 2015, 12, e1001780. [Google Scholar] [CrossRef]
- Huang, J.; Kumar, S.; Abbassi-Ghadi, N.; Spanĕl, P.; Smith, D.; Hanna, G.B. Selected ion flow tube mass spectrometry analysis of volatile metabolites in urine headspace for the profiling of gastro-oesophageal cancer. Anal. Chem. 2013, 85, 3409–3416. [Google Scholar] [CrossRef]
- Kumar, S.; Huang, J.; Abbassi-Ghadi, N.; Spanĕl, P.; Smith, D.; Hanna, G.B. Selected ion flow tube mass spectrometry analysis of exhaled breath for volatile organic compound profiling of oesophago-gastric cancer. Anal. Chem. 2013, 85, 6121–6128. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Huang, J.; Abbassi-Ghadi, N.; Mackenzie, H.A.; Veselkov, K.A.; Hoare, J.M.; Lovat, L.B.; Spanĕl, P.; Smith, D.; Hanna, G.B. Mass Spectrometric Analysis of Exhaled Breath for the Identification of Volatile Organic Compound Biomarkers in Oesophageal and Gastric Adenocarcinoma. Ann. Surg. 2015, 262, 981–990. [Google Scholar] [CrossRef] [PubMed]
- Burjonrappa, S.C.; Reddimasu, S.; Nawaz, Z.; Gao, Z.; Sharma, P.; Loggie, B. Mucin expression profile in Barrett’s, dysplasia, adenocarcinoma sequence in the oesophagus. Indian J. Cancer 2007, 44, 1–5. [Google Scholar] [CrossRef]
- Lee, H.-W.; Yang, D.H.; Kim, H.K.; Lee, B.H.; Choi, K.C.; Choi, Y.H.; Park, Y. E Expression of MUC2 in gastric carcinomas and background mucosae. J. Gastroenterol. Hepatol. 2007, 22, 1336–1343. [Google Scholar] [CrossRef] [PubMed]
- Kufe, D.W. Mucins in cancer: Function, prognosis and therapy. Nat. Rev. Cancer 2009, 9, 874–885. [Google Scholar] [CrossRef]
- Kwon, J.-A.; Lee, S.-Y.; Ahn, E.-K.; Seol, S.-Y.; Kim, M.C.; Kim, S.J.; Kim, S.I.; Chu, I.-S.; Leem, S.-H. Short rare MUC6 minisatellites-5 alleles influence susceptibility to gastric carcinoma by regulating gene expression. Hum. Mutat. 2010, 31, 942–949. [Google Scholar] [CrossRef]
- Niv, Y.; Ho, S.B.; Fass, R.; Rokkas, T. Mucin Expression in the Oesophageal Malignant and Pre-malignant States: A Systematic Review and Meta-analysis. J. Clin. Gastroenterol. 2018, 52, 91–96. [Google Scholar] [CrossRef]
- Hansson, G.C. Mucins and the Microbiome. Annu. Rev. Biochem. 2020, 89, 769–793. [Google Scholar] [CrossRef]
- Cui, J.; Yin, Y.; Ma, Q.; Wang, G.; Olman, V.; Zhang, Y.; Chou, W.-C.; Hong, C.S.; Zhang, C.; Cao, S.; et al. Comprehensive characterization of the genomic alterations in human gastric cancer. Int. J. Cancer 2015, 137, 86–95. [Google Scholar] [CrossRef]
- Xiong, Z.F.; Shi, J.; Fu, Z.H.; Wan, H.P.; Tu, L.X. Phenotype classification of gastric signet ring cell carcinoma and its relationship with K-ras mutation. Genet. Mol. Res. 2017, 16, gmr16029181. [Google Scholar] [CrossRef]
- Toki, F.; Takahashi, A.; Aihara, R.; Ogata, K.; Ando, H.; Ohno, T.; Mochiki, E.; Kuwano, H. Relationship between clinicopathological features and mucin phenotypes of advanced gastric adenocarcinoma. World J. Gastroenterol. 2010, 16, 2764–2770. [Google Scholar] [CrossRef] [PubMed]
- Flucke, U.; Steinborn, E.; Dries, V.; Mönig, S.P.; Schneider, P.M.; Thiele, J.; Hölscher, A.H.; Dienes, H.P.; Baldus, S.E. Immunoreactivity of cytokeratins (CK7, CK20) and mucin peptide core antigens (MUC1, MUC2, MUC5AC) in adenocarcinomas, normal and metaplastic tissues of the distal oesophagus, oesophago-gastric junction and proximal stomach. Histopathology 2003, 43, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Singanayagam, A.; Footitt, J.; Marcynski, M.; Radicioni, G.; Cross, M.T.; Finney, L.J.; Trujillo-Torralbo, M.-B.; Calderazzo, M.; Zhu, J.; Aniscenko, J.; et al. Airway mucins promote immunopathology in virus-exacerbated chronic obstructive pulmonary disease. J. Clin. Investig. 2022, 132, e120901. [Google Scholar] [CrossRef] [PubMed]
- Palmer, A.J.; Lochhead, P.; Hold, G.L.; Rabkin, C.S.; Chow, W.-H.; Lossowska, J.; Vaughan, T.L.; Berry, S.; Gammon, M.; Risch, H.; et al. Genetic variation in C20orf54, PLCE1 and MUC1 and risk of upper gastrointestinal cancers in Caucasian populations. Eur. J. Cancer Prev. 2012, 21, 541–544. [Google Scholar] [CrossRef]
- Cascio, S.; Zhang, L.; Finn, O.J. MUC1 protein expression in tumor cells regulates transcription of proinflammatory cytokines by forming a complex with NF-κB p65 and binding to cytokine promoters: Importance of the extracellular domain. J. Biol. Chem. 2011, 286, 42248–42256. [Google Scholar] [CrossRef]
- Benjamin, J.B.E.; Jayanthi, V.; Devaraj, H. MUC1 expression and its association with other aetiological factors and localization to mitochondria in preneoplastic and neoplastic gastric tissues. Clin. Chim Acta 2010, 411, 2067–2072. [Google Scholar] [CrossRef]
- Yang, J. Identification of novel biomarkers, MUC5AC, MUC1, KRT7, GAPDH, CD44 for gastric cancer. Med. Oncol. 2020, 37, 34. [Google Scholar] [CrossRef]
- Piessen, G.; Jonckheere, N.; Vincent, A.; Hémon, B.; Ducourouble, M.-P.; Copin, M.-C.; Mariette, C.; Van Seuningen, I. Regulation of the human mucin MUC4 by taurodeoxycholic and taurochenodeoxycholic bile acids in oesophageal cancer cells is mediated by hepatocyte nuclear factor 1α. Biochem. J. 2007, 402, 81–91. [Google Scholar] [CrossRef]
- Babu, S.D.; Jayanthi, V.; Devaraj, N.; Reis, C.A.; Devaraj, H. Expression profile of mucins (MUC2, MUC5AC and MUC6) in Helicobacter pylori infected pre-neoplastic and neoplastic human gastric epithelium. Mol. Cancer 2006, 5, 10. [Google Scholar] [CrossRef]
- Tajima, Y.; Yamazaki, K.; Makino, R.; Nishino, N.; Masuda, Y.; Aoki, S.; Kato, M.; Morohara, K.; Kusano, M. Differences in the histological findings, phenotypic marker expressions and genetic alterations between adenocarcinoma of the gastric cardia and distal stomach. Br. J. Cancer 2007, 96, 631–638. [Google Scholar] [CrossRef]
- Rachagani, S.; Torres, M.P.; Moniaux, N.; Batra, S.K. Current status of mucins in the diagnosis and therapy of cancer. Biofactors 2009, 35, 509–527. [Google Scholar] [CrossRef]
- Guillem, P.; Billeret, V.; Bisine, M.P.; Flejou, J.F.; Lecomte-Houcke, M.; Degand, P.; Aubert, J.P.; Triboulet, J.P.; Porchet, N. Mucin gene expression and cell differentiation in human normal, premalignant and malignant oesophagus. Int. J. Cancer 2000, 88, 856–861. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.; McKenzie, J.E.; Sowden, A.; Katikireddi, S.V.; Brennan, S.E.; Ellis, S.; Hartmann-Boyce, J.; Ryan, R.; Shepperd, S.; Thomas, J.; et al. Synthesis without meta-analysis (SWiM) in systematic reviews: Reporting guideline. BMJ 2020, 368, l6890. [Google Scholar] [CrossRef] [PubMed]
- The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Vol. Ottawa, Ontario, Canada: Community Medicine, University of Ottawa. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm (accessed on 15 March 2022).
- Sun, Z.-G.; Yu, L.; Yang, F.; Gao, W.; Wang, Z.; Zhu, L.-M. Mucin 1 expression correlates with metastatic recurrence in postoperative patients with oesophageal squamous cell cancer. Pol. J. Pathol. 2016, 67, 384–391. [Google Scholar] [CrossRef]
- Sun, Z.-G.; Yu, L.; Gao, W.; Wang, Z.; Zhu, L.-M. Clinical and prognostic significance of MUC1 expression in patients with oesophageal squamous cell carcinoma after radical resection. Saudi J. Gastroenterol. 2018, 24, 165–170. [Google Scholar]
- Wang, Y.; Liao, X.; Ye, Q.; Huang, L. Clinic implication of MUC1 0-glycosylation and C1GALT1 in oesophagus squamous cell carcinoma. Sci. China Life Sci. 2018, 61, 1389–1395. [Google Scholar] [CrossRef]
- Song, Z.-B.; Gao, S.-S.; Yi, X.-N.; Li, Y.-J.; Wang, Q.-M.; Zhuang, Z.-H. Expression of MUC1 in oesophageal squamous-cell carcinoma and its relationship with prognosis of patients from Linzhou city, a high incidence area of northern China. World J. Gastroenterol. 2003, 9, 404–407. [Google Scholar] [CrossRef]
- Audie, J.P.; Janin, A.; Porchet, N.; Copin, M.C.; Gosselin, B.; Aubert, J.P. Expression of human mucin genes in respiratory, digestive, and reproductive tracts ascertained by in situ hybridization. J. Histochem. Cytochem. 1993, 41, 1479–1485. [Google Scholar] [CrossRef]
- Fitzgerald, R.C.; di Pietro, M.; Ragunath, K.; Ang, Y.; Kang, J.-Y.; Watson, P.; Trudgill, N.; Patel, P.; Kaye, P.V.; Sanders, S.; et al. British Society of Gastroenterology guidelines on the diagnosis and management of Barrett’s oesophagus. Gut 2013, 63, 7–42. [Google Scholar] [CrossRef]
- de Jonge, P.J.F.; van Blankenstein, M.; Grady, W.M.; Kuipers, E.J. Barrett’s oesophagus: Epidemiology, cancer risk and implications for management. Gut 2014, 63, 191–202. [Google Scholar] [CrossRef] [PubMed]
- Beg, S.; Ragunath, K.; Wyman, A.; Banks, M.; Trudgill, N.; Pritchard, D.M.; Riley, S.; Anderson, J.; Griffiths, H.; Bhandari, P.; et al. Quality standards in upper gastrointestinal endoscopy: A position statement of the British Society of Gastroenterology (BSG) and Association of Upper Gastrointestinal Surgeons of Great Britain and Ireland (AUGIS). Gut 2017, 66, 1886–1899. [Google Scholar] [CrossRef] [PubMed]
- de Jong, J.J.; Lantinga, M.A.; Drenth, J.P. Prevention of overuse: A view on upper gastrointestinal endoscopy. World J. Gastroenterol. 2019, 25, 178–189. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, J.W.; Albasri, A.; Nicholson, B.D.; Perera, R.; Aronson, J.K.; Roberts, N.; Heneghan, C. Overtesting and undertesting in primary care: A systematic review and meta-analysis. BMJ Open 2018, 8, e018557. [Google Scholar] [CrossRef]
- Piessen, G.; Wacrenier, A.; Briez, N.; Triboulet, J.-P.; Van Seuningen, I.; Mariette, C. Clinical impact of MUC1 and MUC4 expression in Barrett-associated oesophageal adenocarcinoma. J. Clin. Pathol. 2009, 62, 1144–1146. [Google Scholar] [CrossRef]
- Chinyama, C.N.; Marshall, R.E.; Owen, W.J.; Mason, R.J.; Kothari, D.; Wilkinson, M.L.; Sanderson, J.D. Expression of MUC1 and MUC2 mucin gene products in Barrett’s metaplasia, dysplasia and adenocarcinoma: An immunopathological study with clinical correlation. Histopathology 1999, 35, 517–524. [Google Scholar] [CrossRef]
- Dwertmann Rico, S.; Mahnken, M.; Büscheck, F.; Dum, D.; Luebke, A.M.; Kluth, M.; Hube-Magg, C.; Hinsch, A.; Höflmayer, D.; Möller-Koop, C.; et al. MUC5AC Expression in Various Tumor Types and Nonneoplastic Tissue: A Tissue Microarray Study on 10 399 Tissue Samples. Technol. Cancer Res. Treat. 2021, 20, 15330338211043328. [Google Scholar]
- Takami, H.; Sentani, K.; Matsuda, M.; Oue, N.; Sakamoto, N.; Yasui, W. Cytokeratin expression profiling in gastric carcinoma: Clinicopathologic significance and comparison with tumor-associated molecules. Pathobiology 2012, 79, 154–161. [Google Scholar] [CrossRef]
- Gulmann, C.; Counihan, I.; Grace, A.; Patchett, S.; Leen, E.; Leader, M.; Kay, E. Cytokeratin 7/20 and mucin expression patterns in oesophageal, cardia and distal gastric adenocarcinomas. Histopathology 2003, 43, 453–461. [Google Scholar] [CrossRef]
- Choi, J.S.; Kim, M.A.; Lee, H.E.; Lee, H.S.; Kim, W.H. Mucinous gastric carcinomas: Clinicopathologic and molecular analyses. Cancer 2009, 115, 3581–3590. [Google Scholar] [CrossRef]
- Guner, G.; Isik, A.; Karabulut, E.; Gedikoglu, G.; Sokmensuer, C.; Akyol, A. Morphologic and Immunohistochemical Appraisal of Primary Gastric carcinomas. Appl. Immunohistochem. Mol. Morphol. 2018, 26, e107–e115. [Google Scholar] [CrossRef] [PubMed]
- Puyan, F.O.; Can, N.; Ozyilmaz, F.; Usta, U.; Sut, N.; Tastekin, E.; Altaner, S. The relationship among PDX1, CDX2, and mucin profiles in gastric carcinomas; correlations with clinicopathologic parameters. J. Cancer Res. Clin. Oncol. 2011, 137, 1749–1762. [Google Scholar] [CrossRef] [PubMed]
- Ge, Y.; Ma, G.; Liu, H.; Lin, Y.; Zhang, G.; Du, M.; Wang, M.; Chu, H.; Zhang, H.; Zhang, Z. MUC1 is associated with TFF2 methylation in gastric cancer. Clin. Epigenetics 2020, 12, 37. [Google Scholar] [CrossRef] [PubMed]
- Ohba, R.; Iijima, K. Pathogenesis and risk factors for gastric cancer after Helicobacter pylori eradication. World J. Gastrointest. Oncol. 2016, 8, 663–672. [Google Scholar] [CrossRef]
- Qian, Z.; Jiang, Y.; Shou, C.; Yu, J.; Huang, D.; Xie, H.; Zhou, L.; Chen, D.; Zheng, S. Validation of the DNA Methylation Lanscape of TFF1/TFF2 in Gastric Cancer. Cancers 2022, 14, 5474. [Google Scholar] [CrossRef]
- Shi, D.; Xi, X.-x. Regulation of MUC6 Methylation Correlates with Progression of Gastric Cancer. Yonsei Med. J. 2021, 62, 1005–1015. [Google Scholar] [CrossRef]
- Yamanoi, K.; Nakayama, J. Reduced αGlcNAc glycosylation on gastric gland mucin is a biomarker of malignant potential for gastric cancer, Barrett’s adenocarcinoma, and pancreatic cancer. Histochem. Cell Biol. 2018, 149, 569–575. [Google Scholar] [CrossRef]
- Pinto-de-Sousa, J.; Reis, C.A.; David, L.; Pimenta, A.; Cardoso-de-Oliveira, M. MUC5B expression in gastric carcinoma: Relationship with clinic-pathological parameters and with expression of mucins MUC1, MUC2, MUC5AC and MUC6. Virchows Arch. 2004, 444, 224–230. [Google Scholar] [CrossRef]
- Kim, D.H.; Shin, N.; Kim, G.H.; Song, G.A.; Jeon, T.-Y.; Kim, D.-H.; Lauwers, G.Y.; Park, D.Y. Mucin expression in gastric cancer: Reappraisal of its clinicopathologic and prognostic significance. Arch. Pathol. Lab. Med. 2013, 137, 1047–1053. [Google Scholar] [CrossRef]
- Reis, C.A.; David, L.; Carvalho, F.; Mandel, U.; de Bolós, C.; Mirgorodskaya, E.; Clausen, H.; Sobrinho-Simões, M. Immunohistochemical study of the expression of MUC6 mucin and co-expression of other secreted mucins (MUC5AC and MUC2) in human gastric carcinomas. J. Histochem. Cytochem. 2000, 48, 377–388. [Google Scholar] [CrossRef]
- Javanbakht, M.; Akhavanmoghadam, J.; Talaei, A.K.; Aghyani, M.; Mozafari, M.; Khedmat, L.; Mohebbi, M. Differential expression of two genes Oct-4 and MUC5AC associates with poor outcome in patients with gastric cancer. Clin. Exp. Pharmacol. Physiol. 2017, 44, 1099–1105. [Google Scholar] [CrossRef] [PubMed]
- Li, X.-H.; Zheng, H.-C.; Wang, Z.-G.; Takahashi, H.; Yang, X.-H.; Guan, Y.-F.; Takano, Y. The clinicopathological and prognostic significance of MUC-1 expression in Japanese gastric carcinomas: An immunohistochemical study of tissue microarrays. Anticancer. Res. 2008, 28, 1061–1067. [Google Scholar] [PubMed]
- Leteurtre, E.; Zerimech, F.; Piessen, G.; Wacrenier, A.; Leroy, X.; Copin, M.-C.; Mariette, C.; Aubert, J.-P.; Porchet, N.; Buisine, M.-P. Relationships between mucinous gastric carcinoma, MUC2 expression and survival. World J. Gastroenterol. 2006, 12, 3324–3331. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, H.; Yonezawa, S.; Utsunomiya, T.; Tanaka, S.; Kim, Y.S.; Sato, E. Mucin antigen expression in gastric carcinomas of young and old adults. Hum. Pathol. 1997, 28, 1056–1065. [Google Scholar] [CrossRef]
- Conze, T.; Carvalho, A.S.; Langegren, U.; Almeida, R.; Reis, C.A.; David, L.; Söderberg, O. MUC2 mucin is a major carrier of the cancer-associated sialyl-Tn antigen in intestinal metaplasia and gastric carcinomas. Glycobiology 2010, 20, 199–206. [Google Scholar] [CrossRef]
- Myllykangas, S.; Junnila, S.; Kokkola, A.; Autio, R.; Scheinin, I.; Kiviluoto, T.; Karjalainen-Lindsberg, M.-L.; Hollmén, J.; Knuutila, S.; Puolakkainen, P.; et al. Integrated gene copy number and expression microarray analysis of gastric cancer highlights potential target genes. Int. J. Cancer 2008, 123, 817–825. [Google Scholar] [CrossRef]
- Croft, W.; Evans, R.P.T.; Pearce, H.; Elshafie, M.; Griffiths, E.A.; Moss, P. The single cell transcriptional landscape of oesophageal adenocarcinoma and its modulation by neoadjuvant chemotherapy. Mol. Cancer 2022, 21, 200. [Google Scholar] [CrossRef]
- Montagne, L.; Piel, C.; Lallès, J.P. Effect of diet on mucin kinetics and composition: Nutrition and health implications. Nutr. Rev. 2004, 62, 105–114. [Google Scholar] [CrossRef]
- Mitsuuchi, M.; Hinoda, Y.; Itoh, F.; Endo, T.; Satoh, M.; Xing, P.X.; Imai, K. Expression of MUC2 gene in gastric regenerative, metaplastic, and neoplastic epithelia. J. Clin. Lab. Anal. 1999, 13, 259–265. [Google Scholar] [CrossRef]
- Aihara, R.; Mochiki, E.; Nakabayashi, T.; Akazawa, K.; Asao, T.; Kuwano, H. Clinical significance of mucin phenotype, beta-catenin and matrix metalloproteinase 7 in early undifferentiated gastric carcinoma. Br. J. Surg. 2005, 92, 454–462. [Google Scholar] [CrossRef]
- Ando, H.; Aihara, R.; Ohno, T.; Ogata, K.; Mochiki, E.; Kuwano, H. Prognostic significance of the expression of MUC1 and collagen type IV in advanced gastric carcinoma. Br. J. Surg. 2009, 96, 901–909. [Google Scholar] [CrossRef] [PubMed]
- Boltin, D.; Gingold-Belfer, R.; Dickman, R.; Halpern, M.; Morgenstern, S.; Roth, M.; Layfer, O.; Vilkin, A.; Niv, Y.; Levi, Z. Gastric mucin expression in first-degree relatives of gastric cancer patients. Eur. J. Gastroenterol. Hepatol. 2014, 26, 710–714. [Google Scholar] [CrossRef] [PubMed]
- Chaves, P.; Cruz, C.; Dias Pereira, A.; Suspiro, A.; de Almeida, J.C.M.; Leitão Soares, J. Gastric and intestinal differentiation in Barrett’s metaplasia and associated adenocarcinoma. Dis. Esophagus. 2005, 18, 383–387. [Google Scholar] [CrossRef] [PubMed]
- Cheah, P.-L.; Ramachandran, K. Alterations in mucin type: An indicator for suspicion of malignant gastric transformation. Malaysian J. Pathol. 1994, 16, 39–42. [Google Scholar]
- Chlumská, A.; Mukenšnabl, P.; Waloschek, T.; Zámečník, M. Esophageal dysplasia and adenocarcinoma: A study with double immunostaining for intestinal and gastric markers. Cesk Patol. 2018, 54, 81–85. [Google Scholar]
- Cho, K.J.; Myong, N.H.; Jang, J.J. Mucin histochemistry by paradoxical concanavalin A staining in early gastric carcinomas. J. Korean Med. Sci. 1991, 6, 119–125. [Google Scholar] [CrossRef]
- Cui, S.-J.; Li, Y.; Zhou, R.-M.; Liu, L.; Cao, S.-R.; Huang, X.; Huo, X.-R.; Wang, N. TIM-3 polymorphism is involved in the progression of esophageal squamous cell carcinoma by regulating gene expression. Environ. Mol. Mutagen. 2021, 62, 273–283. [Google Scholar] [CrossRef]
- DiMaio, M.A.; Kwok, S.; Montgomery, K.D.; Lowe, A.W.; Pai, R.K. Immunohistochemical Panel for Distinguishing Esophageal Adenocarcinoma from Squamous Cell Carcinoma: A Combination of p63, Cytokeratin 5/6, MUC5AC, and AGR2 Allows Optimal Subtyping. Hum. Pathol. 2012, 43, 1799–1807. [Google Scholar] [CrossRef]
- Forné, M.; Fernández-Baňares, F.; González-Mínguez, C.; Casalots, J.; Garcia-Gil, L.J.; Esteve, M.; Esteve, M.; Rosinach, M.; Espinós, J.; Loras, C.; et al. Lack of Clinical Usefulness of Das-1 Monoclonal Antibody and Mucin Expression as Risk Markers of Gastric Carcinoma in Patients With Gastric Intestinal Metaplasia. Am. J. Clin. Pathol. 2009, 131, 99–105. [Google Scholar] [CrossRef]
- Fujita, Y.; Uesugi, N.; Sugimoto, R.; Eizuka, M.; Toya, Y.; Akasaka, R.; Matsumoto TSugai, T. Analysis of clinicopathological and molecular features of crawling-type gastric adenocarcinoma. Diagn Pathol. 2020, 15, 111. [Google Scholar] [CrossRef]
- Gűrbűz, Y.; Kahlke, V.; Klőppel, G. How do gastric carcinoma classification systems relate to mucin expression patterns? An immunohistochemical analysis in a series of advanced gastric carcinomas. Virchows Arch. 2002, 440, 505–511. [Google Scholar] [CrossRef]
- Han, H.S.; Lee, S.-Y.; Lee, K.Y.; Hong, S.N.; Kim, J.H.; Sung, I.-K.; Park, H.S.; Jin, C.J.; Min, Y.I. Unclassified mucin phenotype of gastric adenocarcinoma exhibits the highest invasiveness. J. Gastroenterol. Hepatol. 2009, 24, 658–666. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Qu, L.; Wei, L.; Chen, Y.; Suo, J. Reduction of miR-132-3p contributes to gastric cancer proliferation by targeting MUC13. Mol. Med. Rep. 2017, 15, 3055–3061. [Google Scholar] [CrossRef]
- Jia, Y.; Persson, C.; Hou, L.; Zheng, Z.; Yeager, M.; Lissowska, J.; Chanock, S.J.; Chow, W.-H.; Ye, W. A comprehensive analysis of common genetic variation in MUC1, MUC5AC, MUC6 genes and risk of stomach cancer. Cancer Causes Control. 2010, 21, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Kageyama-Yahara, N.; Yamamichi, N.; Takahashi, Y.; Nakayama, C.; Shiogama, K.; Inada, K.-I.; Konno-Shimizu, M.; Kodashima, S.; Fujishiro, M.; Tsutsumi, Y.; et al. Gli regulates MUC5AC transcription in human gastrointestinal cells. PLoS ONE 2014, 9, e106106. [Google Scholar]
- Khor, T.S.; Alfaro, E.E.; Ooi, E.M.M.; Li, Y.; Srivastava, A.; Fujita, H.; Park, Y.; Kumarasinghe, M.P.; Lauwers, G.Y. Divergent expression of MUC5AC, MUC6, MUC2, CD10, and CDX-2 in dysplasia and intramucosal adenocarcinomas with intestinal and foveolar morphology: Is this evidence of distinct gastric and intestinal pathways to carcinogenesis in Barrett Esophagus? Am. J. Surg. Pathol. 2012, 36, 331–342. [Google Scholar] [CrossRef]
- Li, H.; Yu, B.; Li, J.; Su, L.; Yan, M.; Zhang, J.; Li, C.; Zhu, Z.; Liu, B. Characterization of Differentially Expressed Genes Involved in Pathways Associated with Gastric Cancer. PLoS ONE 2015, 10, e0125013. [Google Scholar] [CrossRef]
- Machado, J.C.; Nogueira, A.M.M.F.; Carneiro, F.; Reis, C.A.; Sobrinho-Simŏes, M. Gastric carcinoma exhibits distinct types of cell differentiation: An immunohistochemical study of trefoil peptides (TFF1 and TFF2) and mucins (MUC1, MUC2, MUC5AC, and MUC6). J. Pathol. 2000, 190, 437–443. [Google Scholar] [CrossRef]
- Mall, A.; McConney, Z.; Lotz, Z.; Tyler, M.; McLeod, H.; Hickman, R.; Dent, D.; Kahn, D. Increased fragmentation of MUC 5AC mucins in gastric juice of patients with ulceration and carcinoma. S. Afr. J. Sci. 2000, 96, 39–43. [Google Scholar]
- Nakajima, K.; Ota, H.; Zhang, M.X.; Sano, K.; Honda, T.; Ishii, K.; Nakayama, J. Expression of gastric gland mucous cell-type mucin in normal and neoplastic human tissues. J. Histochem. Cytochem. 2003, 51, 1689–1698. [Google Scholar] [CrossRef]
- Ozcan, H.E.A.; Anuk, T.; Ozden, O. Expression profile and cellular localizations of mucin proteins, CK7, and cytoplasmic p27 in Barrett’s esophagus and esophageal adenocarcinoma. Adv. Med. Sci. 2018, 63, 296–300. [Google Scholar] [PubMed]
- Reis, C.A.; David, L.; Seixas, M.; Burchell, J.; Sobrinho-Simŏes, M. Expression of fully and under-glycosylated forms of MUC1 mucin in gastric carcinoma. Int. J. Cancer 1998, 79, 402–410. [Google Scholar] [PubMed]
- Song, K.; Yang, Q.; Yan, Y.; Yu, X.; Xu, K.; Xu, J. Gastric mucin phenotype indicates aggressive biological behaviour in early differentiated gastric adenocarcinomas following endoscopic treatment. Diagn Pathol. 2021, 16, 62. [Google Scholar] [PubMed]
- Sugai, T.; Habano, W.; Uesugi, N.; Jao, Y.-F.; Nakamura S-i Abe, K.; Takagane, A.; Terashima, M. Three independent genetic profiles based on mucin expression in early differentiated-types gastric cancers—A new concept of genetic carcinogenesis of early differentiated-type adenocarcinomas. Mod Pathol. 2004, 17, 1223–1234. [Google Scholar]
- Tamura, Y.; Higashi, M.; Kitamoto, S.; Yokoyama, S.; Osako, M.; Horinouchi, M.; Shimizu, T.; Tabata, M.; Batra, S.K.; Goto, M.; et al. MUC4 and MUC1 expression in adenocarcinoma of the stomach correlates with vessel invasion and lymph node metastasis: An immunohistochemical study of early gastric cancer. PLoS ONE 2012, 7, e49251. [Google Scholar]
- Tsukashita, S.; Kushima, R.; Bamba, M.; Sugihara, H.; Hattori, T. MUC gene expression and histogenesis of adenocarcinoma of the stomach. Int. J. Cancer 2001, 94, 166–170. [Google Scholar]
- Wang, R.-Q.; Fang, D.-C. Alterations of MUC1 and MUC3 expression in gastric carcinoma: Relevance to patient clinicopathological features. J. Clin. Pathol. 2003, 56, 378–384. [Google Scholar]
- Wang, K.; Yuen, S.T.; Xu, J.; Lee, S.P.; Yan, H.H.N.; Shi, S.T.; Siu, H.C.; Deng, S.; Chu, K.M.; Law, S.; et al. Whole-genome sequencing and comprehensive molecular profiling identify new driver mutations in gastric cancer. Nat. Genet. 2014, 46, 573–582. [Google Scholar]
- Yamada, S.; Yamanoi, K.; Sato, Y.; Nakayama, J. Diffuse MIST1 expression and decreased α1,4-linked N-acetylglucosamine (αGlcNAc) glycosylation on MUC6 are distinct hallmarks for gastric neoplasms showing oxyntic gland differentiation. Histopathology 2020, 77, 413–422. [Google Scholar]
- Endo, T.; Tamaki, K.; Arimura, Y.; Itoh, F.; Hinoda, Y.; Hareyama, M.; Irimura, T.; Fujita, M.; Imai, K. Expression of sulphated carbohydrate chain and core peptides of mucin detected by monoclonal antibodies in Barrett’s esophagus and esophageal adenocarcinoma. J. Gastroenterol. 1998, 33, 811–815. [Google Scholar]
- Higuchi, K.; Nishikura, K.; Ajioka, Y.; Watanabe, G. Macroscopic Findings and Mucous Phenotypes of Early Gastric Depressed Type Carcinomas. Acta Med. Biol. 2006, 54, 9–20. [Google Scholar]
- Yu, T.; Chen, X.; Lin, T.; Liu, J.; Li, M.; Zhang, W.; Xu, X.; Zhao, W.; Liu, M.; Napier, D.L.; et al. KLF4 deletion alters gastric cell lineage and induces MUC2 expression. Cell Death Dis. 2016, 7, e2255. [Google Scholar] [PubMed]
- Tian, Y.; Denda-Nagai, K.; Kamata-Sakurai, M.; Nakamori, S.; Tsukui, T.; Itoh, Y.; Okada, K.; Yi, Y.; Irimura, T. Mucin 21 in esophageal squamous epithelia and carcinomas: Analysis with glycoform-specific monoclonal antibodies. Glycobiology 2012, 22, 1218–1226. [Google Scholar] [PubMed]
- Setia, N.; Agoston, A.T.; Han, H.S.; Mullen, J.T.; Duda, D.G.; Clark, J.W.; Deshpande, V.; Mino-Kenudson, M.; Srivastava, A.; Lennerz, J.K.; et al. A protein and mRNA expression-based classification of gastric cancer. Mod. Pathol. 2016, 29, 772–784. [Google Scholar]
- Gűrbűz, Y.; Klőppel, G. Differentiation pathways in duodenal and ampullary carcinomas: A comparative study on mucin and trefoil peptide expression, including gastric and colon carcinomas. Virchows Arch. 2004, 444, 536–541. [Google Scholar] [CrossRef]
- Wang, Y.Z.; Mitomi, H.; Kurihara, M.; Ishihara, K.; Hotta, K.; Tanigawa Okayasu, I. Gastric adenomas and superficial adenocarcinomas display distinct patterns of mucin carbohydrate and core protein expression. Histopathology 2000, 37, 250–259. [Google Scholar]
- Semino-Mora, C.; Doi, S.Q.; Marty, A.; Simko, V.; Carlstedt, I.; Dubois, A. Intracellular and interstitial expression of Helicobacter pylori virulence genes in gastric precancerous intestinal metaplasia and adenocarcinoma. J. Infect. Dis. 2003, 187, 1165–1177. [Google Scholar]
- Fan, X.-N.; Karsten, U.; Goletz, S.; Cao, Y. Reactivity of a humanized antibody (hPankoMab) towards a tumor-related MUC1 epitope (TA-MUC1) with various human carcinomas. Pathol. Res. Pract. 2010, 206, 585–589. [Google Scholar]
- Buisine, M.P.; Devisme, L.; Maunoury, V.; Deschodt, E.; Gosselin, B.; Copin, M.C.; Aubert, J.P.; Porchet, N. Developmental mucin gene expression in the gastroduodenal tract and accessory digestive glands. I. Stomach. A relationship to gastric carcinoma. J. Histochem. Cytochem. 2000, 48, 1657–1666. [Google Scholar]
- Weimann, A.; Rieger, A.; Zimmermann, M.; Gross, M.; Hoffmann, P.; Slevogt, H.; Morawietz, L. Comparison of six immunohistochemical markers for the histologica diagnosis of neoplasia in Barrett’s esophagus. Virchows Arch. 2010, 457, 537–545. [Google Scholar]
- Begnami, M.D.; Fregnani, J.H.T.G.; Brentani, H.; Torres, C.; Costa, W.L., Jr.; Montagnini, A.; Nonogaki, S.; Soares, F.A. Identification of protein expression signatures in gastric carcinomas using clustering analysis. J. Gastroenterol. Hepatol. 2011, 27, 378–384. [Google Scholar]
- Ushiku, T.; Arnason, T.; Ban, S.; Hishima, T.; Shimizu, M.; Fukayama, M.; Lauwers, G.Y. Very well-differentiated gastric carcinoma of intestinal type: Analysis of diagnostic criteria. Mod. Pathol. 2013, 26, 1620–1631. [Google Scholar] [CrossRef] [PubMed]
- Szachnowicz, S.; Cecconello, I.; Ribeiro, U.; Iriya, K.; El Ibrahim, R.; Takeda, F.R.; Corbett, C.E.P.; Safatle-Ribeiro, A.V. Mucin pattern reflects the origin of the adenocarcinoma in Barrett’s esophagus: A retrospective clinical and laboratorial study. World J. Surg. Oncol. 2009, 7, 27. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.-K.; Zhang, Q.-M.; Zhao, T.-H.; Li, Y.-Y.; Yi, Y.-F. Expression of mucins and E-cadherin in gastric carcinoma and their clinical significance. World J. Gastroenterol. 2004, 10, 3044–3047. [Google Scholar] [CrossRef]
- Wang, J.Y.; Chang, C.T.; Hsieh, J.S.; Lee, L.W.; Huang, T.J.; Chai, C.Y.; Lin, S.R. Role of MUC1 and MUC5AC expressions as prognostic indicators in gastric carcinomas. J. Surg. Oncol. 2003, 83, 253–260. [Google Scholar]
- Kang, H.; An, H.J.; Song, J.Y.; Kim, T.H.; Heo, J.H.; Ahn, D.H.; Kim, G. Notch3 and Jagged2 contribute to gastric cancer development and to glandular differentiation associated with MUC2 and MUC5AC expression. Histopathology 2012, 61, 576–586. [Google Scholar] [CrossRef]
- Fujimoto, A.; Ishikawa, Y.; Ishii, T.; Yamada, A.; Igarashi, Y.; Ohmoto, Y.; Kaise, M. Differences between gastric signet-ring cell carcinoma and poorly differentiated adenocarcinoma: A comparison of histopathologic features determined by mucin core protein and trefoil factor family peptide immunohistochemistry. Pathol. Int. 2017, 67, 398–403. [Google Scholar] [CrossRef]
- Ide, M.; Kato, T.; Ogata, K.; Mochiki, E.; Kuwano, H.; Oyama, T. Keratin 17 expression correlates with tumor progression and poor prognosis in gastric adenocarcinoma. Ann. Surg. Oncol. 2012, 19, 3506–3514. [Google Scholar]
- Streppel, M.M.; Vincent, A.; Mukherjee, R.; Campbell, N.R.; Chen, S.H.; Konstantopoulos, K.; Goggins, M.G.; Van Seuningen, I.; Matria, A.; Montgomery, E.A. Mucin 16 (cancer antigen 125) expression in human tissues and cell lines and correlation with clinical outcome in adenocarcinomas of the pancreas, esophagus, stomach, and colon. Hum. Pathol. 2012, 43, 1755–1763. [Google Scholar]
- Kim, R.; Emi, M.; Tanabe, K.; Toge, T. Therapeutic potential of antisense BCl-2 as a chemosensitizer for cancer therapy. Cancer 2004, 101, 2491–2502. [Google Scholar]
- Han, J.P.; Hong, S.J.; Kim, H.K.; Kim, H.S.; Lee, Y.N.; Lee, T.H.; Lee, J.S. Expression of immunohistochemical markers according to histological type in patients with early gastric cancer. Scand J. Gastroenterol. 2016, 51, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Mejías-Luque, R.; Lindén, S.K.; Garrido, M.; Tye, H.; Najdovska, M.; Jenkins, B.J.; Iglesias, M.; Ernst, M.; de Bolós, C. Inflammation modulates the expression of the intestinal mucins MUC2 and MUC4 in gastric tumors. Oncogene 2010, 29, 1753–1762. [Google Scholar] [CrossRef] [PubMed]
- Hwang, I.; Kang, Y.N.; Kim, J.Y.; Do, Y.R.; Song, H.S.; Park, K.U. Prognostic significance of membrane-associated mucins 1 and 4 in gastric adenocarcinoma. Exp. Ther. Med. 2012, 4, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Baldus, S.E.; Mőnig, S.P.; Arkenau, V.; Hanisch, F.-Z.; Schneider, P.M.; Thiele, J.; Hőlscher, A.H.; Dienes, H.P. Correlation of MUC5AC immunoreactivity with histopathological subtypes and prognosis of gastric carcinoma. Ann. Surg. Oncol. 2002, 9, 887–893. [Google Scholar] [CrossRef] [PubMed]
- Baldus, S.E.; Zirbes, T.K.; Engel, S.; Hanisch, F.G.; Mőnig, S.P.; Lorenzen, J.; Glossmann, J.; Fromm, S.; Thiele, J.; Pichlmaier, H.; et al. Correlation of the immunohistochemical reactivity of mucin peptide cores MUC1 and MUC2 with the histopathological subtype and prognosis of gastric carcinomas. Int. J. Cancer 1998, 79, 133–138. [Google Scholar] [CrossRef]
- Terada, T. An immunohistochemical study of primary signet-ring cell carcinoma of the stomach and colorectum: II. Expression of MUC1, MUC2, MUC5AC, and MUC6 in normal mucosa and in 42 cases. Int. J. Clin. Exp. Pathol. 2013, 6, 613–621. [Google Scholar]
- Udhayakumar, G.; Jayanthi, V.; Devaraj, N.; Devaraj, H. Interaction of MUC1 with beta-catenin modulates the Wnt target gene cyclinD1 in H. pylori-induced gastric cancer. Mol. Carcinog. 2007, 46, 807–817. [Google Scholar] [CrossRef]
- Yonezawa, S.; Kitajima, S.; Higashi, M.; Osako, M.; Horinouchi, M.; Yokoyama, S.; Kitamoto, S.; Yamada, N.; Tamura, Y.; Shimizu, T.; et al. A novel anti-MUC1 antibody against the MUC1 cytoplasmic tail domain: Use in sensitive identification of poorly differentiated cells in adenocarcinoma of the stomach. Gastric Cancer 2012, 15, 370–381. [Google Scholar] [CrossRef]
- Tajima, Y.; Yamazaki, K.; Nishino, N.; Morohara, K.; Yamazaki, T.; Kaetsu, T.; Suzuki, S.; Kawamura, M.; Kumagai, K.; Kusano, M. Gastric and intestinal phenotypic marker expression in gastric carcinomas and recurrence pattern after surgery-imunohistochemical analysis of 213 lesions. Br. J. Cancer 2004, 91, 1342–1348. [Google Scholar] [CrossRef]
- Shinozaki, E.; Adachi, S.; Shoda, J.; Kawamoto, T.; Suzuki, H.; Irimura, T.; Ohkohchi, N. Subcellular localization of MUC1 recognized by a monoclonal antibody MY.1E12 correlates with postsurgical prognosis in differentiated-type gastric carcinomas of stage II and III. Int. J. Oncol. 2004, 25, 1257–1265. [Google Scholar] [CrossRef]
- Shimamura, T.; Ito, H.; Shibahara, J.; Watanabe, A.; Hippo, Y.; Taniguchi, H.; Chen, Y.; Kashima, T.; Ohtomo, T.; Tanioka, F.; et al. Overexpression of MUC13 is associated with intestinal-type gastric cancer. Cancer Sci. 2005, 96, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Shi, D.; Qiu, X.-M.; Yan, X.-J. The changes in MUC5AC expression in gastric cancer before and after Helicobacter pylori eradication. Clin. Res. Hepatol. Gastroenterol. 2014, 38, 235–240. [Google Scholar] [CrossRef]
- Retterspitz, M.F.; Mőnig, S.P.; Schreckenberg, S.; Schenider, P.M.; Hőlscher, A.H.; Dienes, H.P.; Baldus, S.E. Expression of {beta}-catenin, MUC1 and c-met in diffuse-type gastric carcinomas: Correlations with tumour progression and prognosis. Anticancer Res. 2010, 30, 4635–4641. [Google Scholar] [PubMed]
- Reis, C.A.; David, L.; Nielsen, P.A.; Clausen, H.; Mirgorodskaya, K.; Roepstorff, P.; Sobrinho-Simŏes, M. Immunohistochemical study of MUC5AC expression in human gastric carcinomas using a novel monoclonal antibody. Int. J. Cancer 1997, 74, 112–121. [Google Scholar] [CrossRef]
- Pinto-de-Sousa, J.; David, L.; Reis, C.A.; Gomes, R.; Silva, L.; Pimenta, A. Mucins MUC1, MUC2, MUC5AC and MUC6 expression in the evaluation of differentiation and clinico-biological behaviour of gastric carcinoma. Virchows Arch. 2002, 440, 304–310. [Google Scholar] [CrossRef]
- Mariette, C.; Piessen, G.; Leteurtre, E.; Hémon, B.; Triboulet, J.-P.; Van Seuningen, I. Activation of MUC1 mucin expression by bile acids in human esophageal adenocarcinomatous cells and tissues is mediated by the phosphatidylinositol 3-kinase. Surgery 2008, 143, 58–71. [Google Scholar] [CrossRef]
- Lin, S.; Zhang, Y.; Hu, Y.; Yang, B.; Cui, J.; Huang, J.; Wang, J.M.; Xing, R.; Lu, Y. Epigenetic downregulation of MUC17 by H.pylori infection facilitates NF-κB-mediated expression of CEACAM1-3S in human gastric cancer. Gastric Cancer 2019, 22, 941–954. [Google Scholar] [CrossRef]
- Lee, O.-J.; Kim, H.-J.; Kim, J.-R.; Watanabe, H. The prognostic significance of the mucin phenotype of gastric adenocarcinoma and its relationship with histologic classifications. Oncol. Rep. 2009, 21, 387–393. [Google Scholar] [CrossRef]
- Lee, H.S.; Lee, H.K.; Kim, H.S.; Yang, H.K.; Kim, Y.I.; Kim, W.H. MUC1, MUC2, MUC5Ac, and MUC6 expressions in gastric carcinomas: Their roles as prognostic indicators. Cancer 2001, 92, 1427–1434. [Google Scholar] [CrossRef]
- Kim, S.M.; Kwon, C.H.; Shin, N.; Park, D.Y.; Moon, H.J.; Kim, G.H.; Jeon, T.Y. Decreased MUC5AC expression is associated with poor prognosis in gastric cancer. Int. J. Cancer 2014, 134, 114–124. [Google Scholar] [CrossRef] [PubMed]
- Khattab, A.-Z.; Nasif, W.A.; Lotfy, M. MUC2 and MUC6 apomucins expression in human gastric neoplasm: An immunohistochemical analysis. Med. Oncol. 2011, 28, S207–S213. [Google Scholar] [CrossRef] [PubMed]
- Davison, J.M.; Ellis, S.T.; Foxwell, T.J.; Luketich, J.D.; Gibson, M.K.; Kuan, S.-F.; Nason, K.S. MUC2 expression is an adverse prognostic factor in superficial gastroesophageal adenocarcinomas. Hum. Pathol. 2014, 45, 540–548. [Google Scholar] [CrossRef] [PubMed]
- Akyűrek, N.; Akyol, G.; Dursun, A.; Yamaç, D.; Gűnel, N. Expression of MUC1 and MUC2 mucins in gastric carcinomas: Their relationship with clinicopathologic parameters and prognosis. Pathol. Res. Pract. 2002, 198, 665–674. [Google Scholar] [CrossRef] [PubMed]
- Mizoshita, T.; Tsukamoto, T.; Nakanishi, H.; Inada, K.-I.; Ogasawara, N.; Joh, T.; Itoh, M.; Yamamura, Y.; Tatematsu, M. Expression of Cdx2 and the phenotype of advanced gastric cancers: Relationship with prognosis. J. Cancer Res. Clin. Oncol. 2003, 129, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Bae, H.I.; Li, Y.-H.; Na, Y.K.; Jung, Y.W.; Lee, S.M.; Yang, J.S.; Kim, D.S. Overexpression of the MUC2 gene through promoter hypomethylation in mucinous cell carcinomas and signet ring cell carcinomas of gastric cancer. Genes Genom. 2010, 32, 429–435. [Google Scholar] [CrossRef]
- Park, K.K.; Yang, S.I.; Seo KWYoon, K.Y.; Lee, S.H.; Jang, H.K.; Shin, Y.M. Correlations of Human Epithelial Growth Factor Receptor 2 Overexpression with MUC2, MUC5AC, MUC6, p53, and Clinicopathological Characteristics in Gastric Cancer Patients with Curative Resection. Gastroenterol. Res. Pract. 2015, 2015, 946359. [Google Scholar] [CrossRef]
- Nakashima, H.; Yamasaki, T.; Owari, M.; Tokai, Y.; Kawachi, H.; Sakaki, N.; Yoshida, M. Mucin Phenotypic Expression and Submucosal Invasion of Gastric Differentiated-type Adenocarcinoma with Minimal Intestinal Metaplasia. J. Gastroenterol. Hepatol. Res. 2016, 5, 2058–2062. [Google Scholar] [CrossRef]
- Wakatsuki, K.; Yamada, Y.; Narikiyo, M.; Ueno, M.; Takayama, T.; Tamaki, H.; Miki, K.; Matsumoto, S.; Enomoto, K.; Yokotani, T.; et al. Clinicopathological and prognostic significance of mucin phenotype in gastric cancer. J. Surg. Oncol. 2008, 98, 124–129. [Google Scholar] [CrossRef]
- Yang, Y.; Fang, E.; Luo, J.; Wu, H.; Jiang, Y.; Liu, Y.; Tong, S.; Wang, Z.; Zhou, R.; Tong, Q. The Antioxidant Alpha-Lipoic Acid Inhibits Proliferation and Invasion of Human Gastric Cancer Cells via Suppression of STAT3-Mediated MUC4 Gene Expression. Oxid. Med. Cell Longev. 2019, 2019, 3643715. [Google Scholar] [CrossRef]
- Ohno, T.; Aihara, R.; Kamiyama, Y.; Mochiki, E.; Asao, T.; Kuwano, H. Prognostic significance of combined expression of MUC1 and adhesion molecules in advanced gastric cancer. Eur. J. Cancer 2006, 42, 256–263. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
Studies on the role of MUC genes in the diagnosis of OGC:
| Studies not assessing MUC gene expression in OGC diagnosis. |
| Studies on secondary oesophageal or gastric cancers or metastases to the oesophagus or stomach from a non-OG primary cancer. | |
| Studies assessing the role of mucins in treatment response or prognosis of OGC. | |
| Paediatric cohorts (<16 years) | |
| Systematic literature reviews, meta-analyses | |
| Articles not published in English | |
| Case reports | |
| Case series of <10 patients | |
| Letters to the editor | |
| Conference abstracts |
| n | |
|---|---|
| Total number of studies | 124 |
| Type of study | |
| Cohort | 11 |
| Clinicopathologic and molecular analyses | 108 |
| Population-based case–control study | 2 |
| Clinicopathologic and gene study | 3 |
| Females | 3801 |
| Males | 7585 |
| Median age (Calculated from all median ages in included studies) | 63.0 years |
| Sampling technique (9 studies used >1 sampling method) | |
| Endoscopic biopsy | 21 |
| Endoscopic mucosal resection/submucosal dissection | 8 |
| Surgical resection | 96 |
| Nasogastric aspirates | 1 |
| Not stated | 7 |
| Type of cancer | Number of studies analysing cancer (n) |
| Oesophageal adenocarcinoma | 24 |
| Oesophageal squamous cell carcinoma | 10 |
| Gastric adenocarcinoma | 101 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patel, N.M.; Geropoulos, G.; Patel, P.H.; Bhogal, R.H.; Harrington, K.J.; Singanayagam, A.; Kumar, S. The Role of Mucin Expression in the Diagnosis of Oesophago-Gastric Cancer: A Systematic Literature Review. Cancers 2023, 15, 5252. https://doi.org/10.3390/cancers15215252
Patel NM, Geropoulos G, Patel PH, Bhogal RH, Harrington KJ, Singanayagam A, Kumar S. The Role of Mucin Expression in the Diagnosis of Oesophago-Gastric Cancer: A Systematic Literature Review. Cancers. 2023; 15(21):5252. https://doi.org/10.3390/cancers15215252
Chicago/Turabian StylePatel, Nikhil Manish, Georgios Geropoulos, Pranav Harshad Patel, Ricky Harminder Bhogal, Kevin Joseph Harrington, Aran Singanayagam, and Sacheen Kumar. 2023. "The Role of Mucin Expression in the Diagnosis of Oesophago-Gastric Cancer: A Systematic Literature Review" Cancers 15, no. 21: 5252. https://doi.org/10.3390/cancers15215252
APA StylePatel, N. M., Geropoulos, G., Patel, P. H., Bhogal, R. H., Harrington, K. J., Singanayagam, A., & Kumar, S. (2023). The Role of Mucin Expression in the Diagnosis of Oesophago-Gastric Cancer: A Systematic Literature Review. Cancers, 15(21), 5252. https://doi.org/10.3390/cancers15215252