
Epidemiology of Gastric Cancer—Changing Trends and Global Disparities


Abstract
Simple Summary
Abstract
1. Introduction
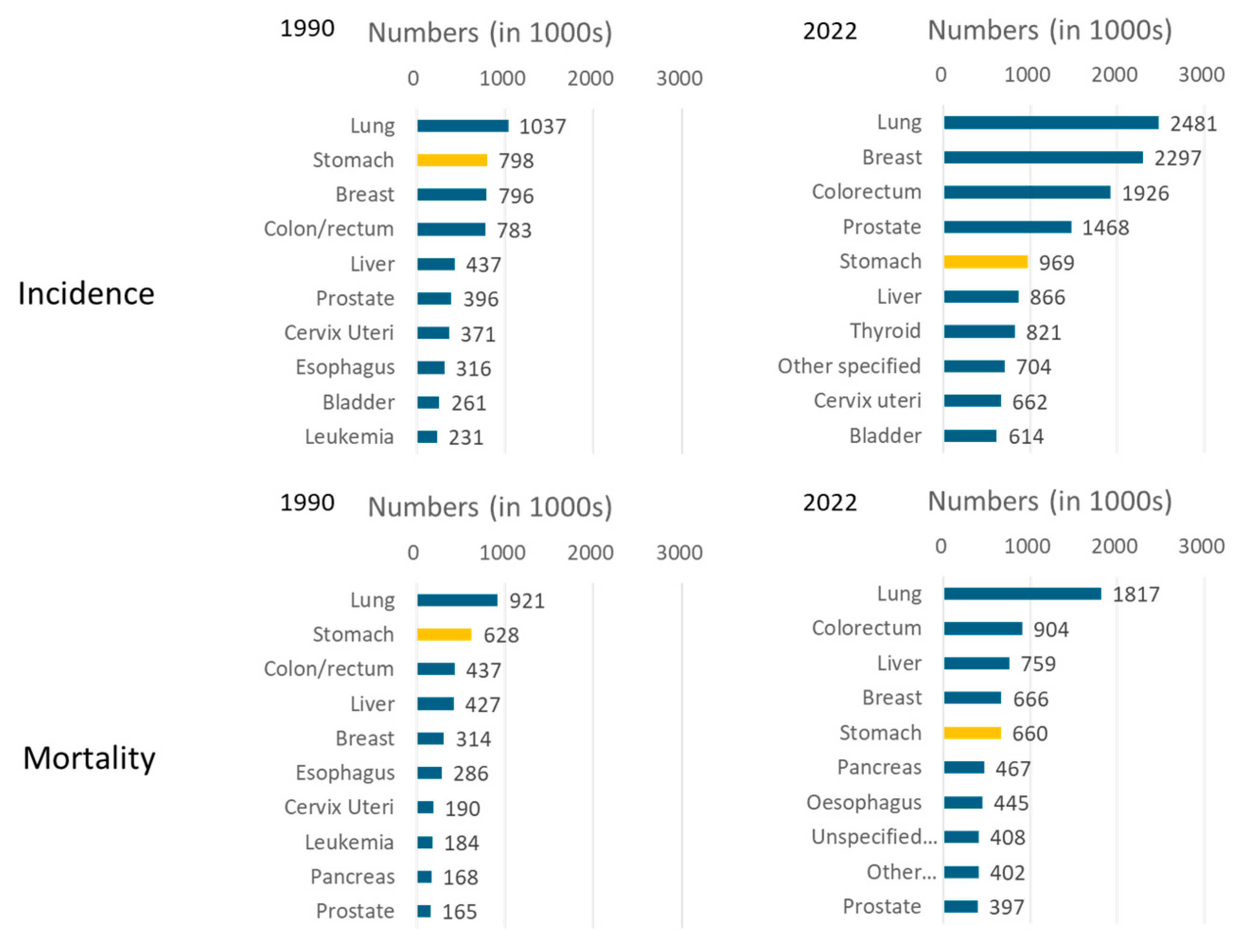
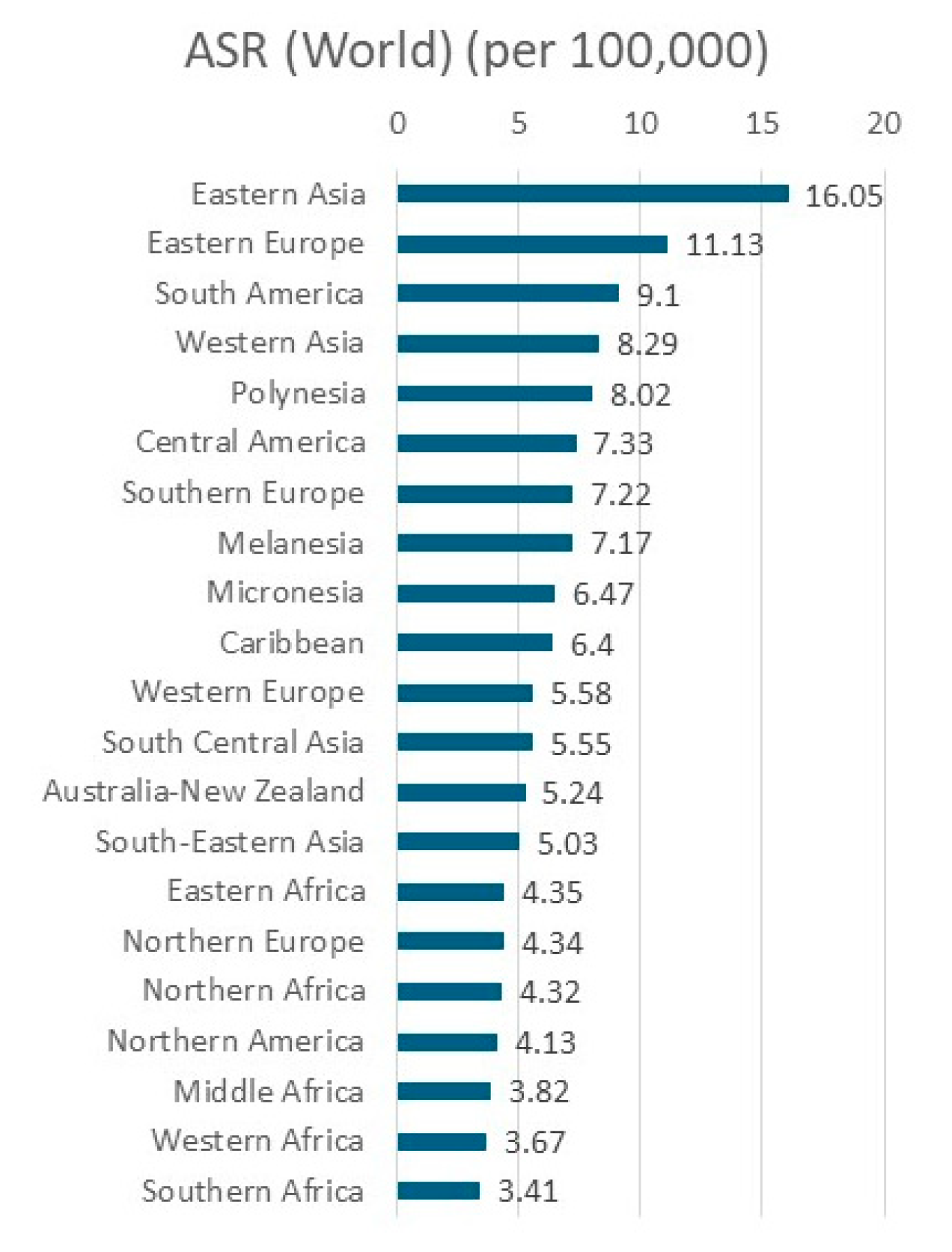
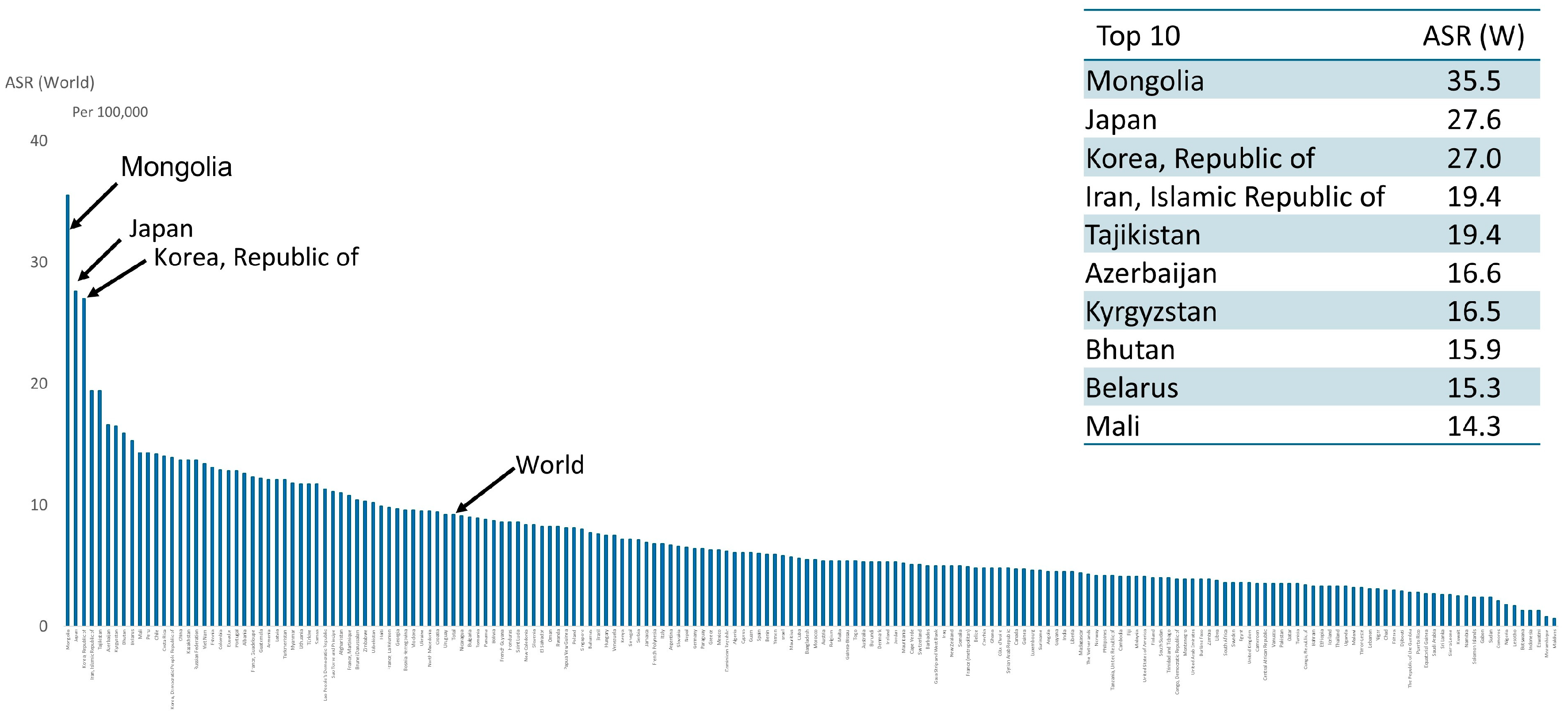
2. Global Descriptive Epidemiological Trends
2.1. Current Trends
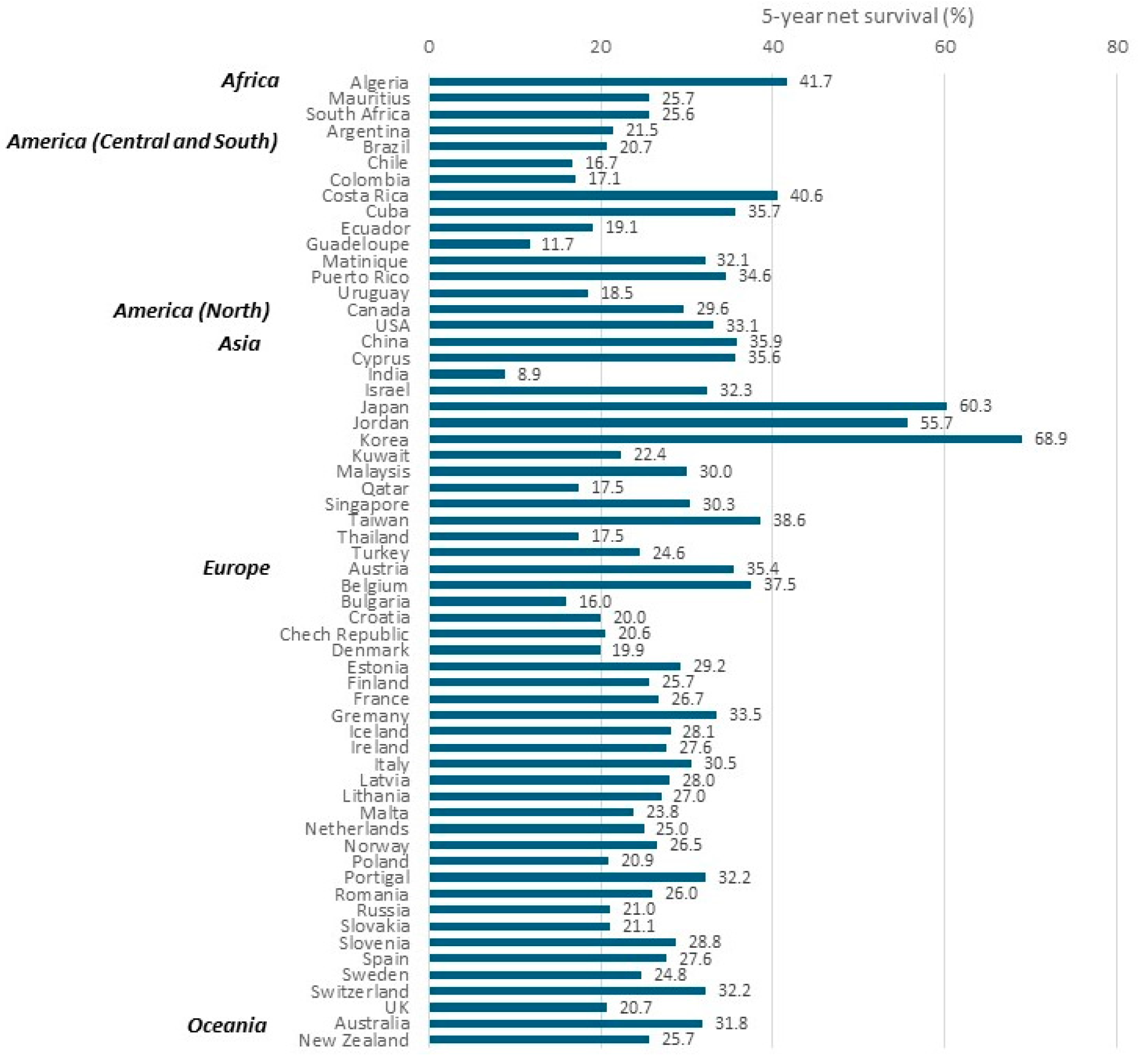
2.2. Survival Trends
3. Clinico-Epidemiological Features
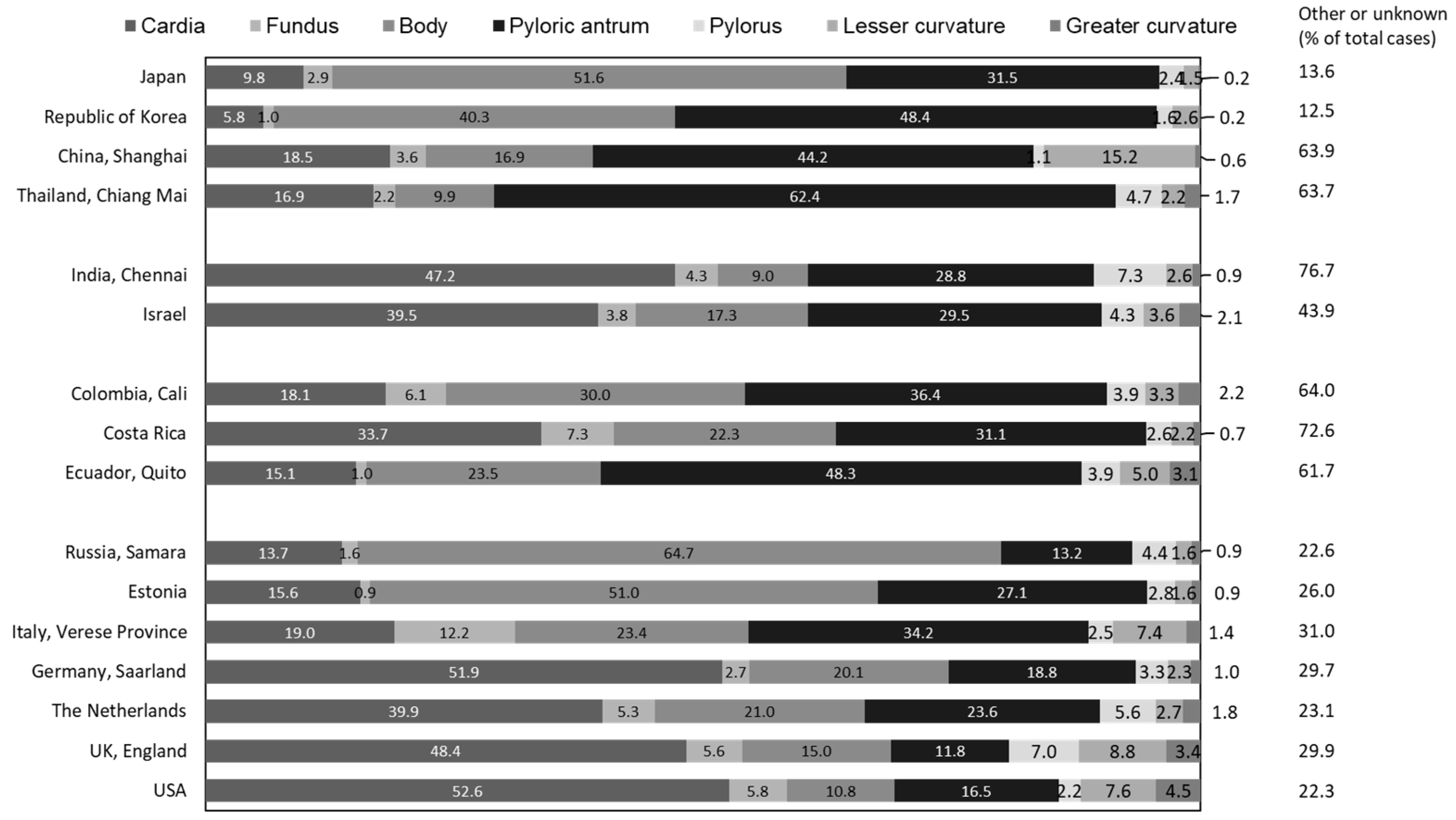
3.1. Subsite Distribution
3.2. Epidemiological Trends in Esophagogastric Junction Cancer
4. Risk Factors of Gastric Cancer
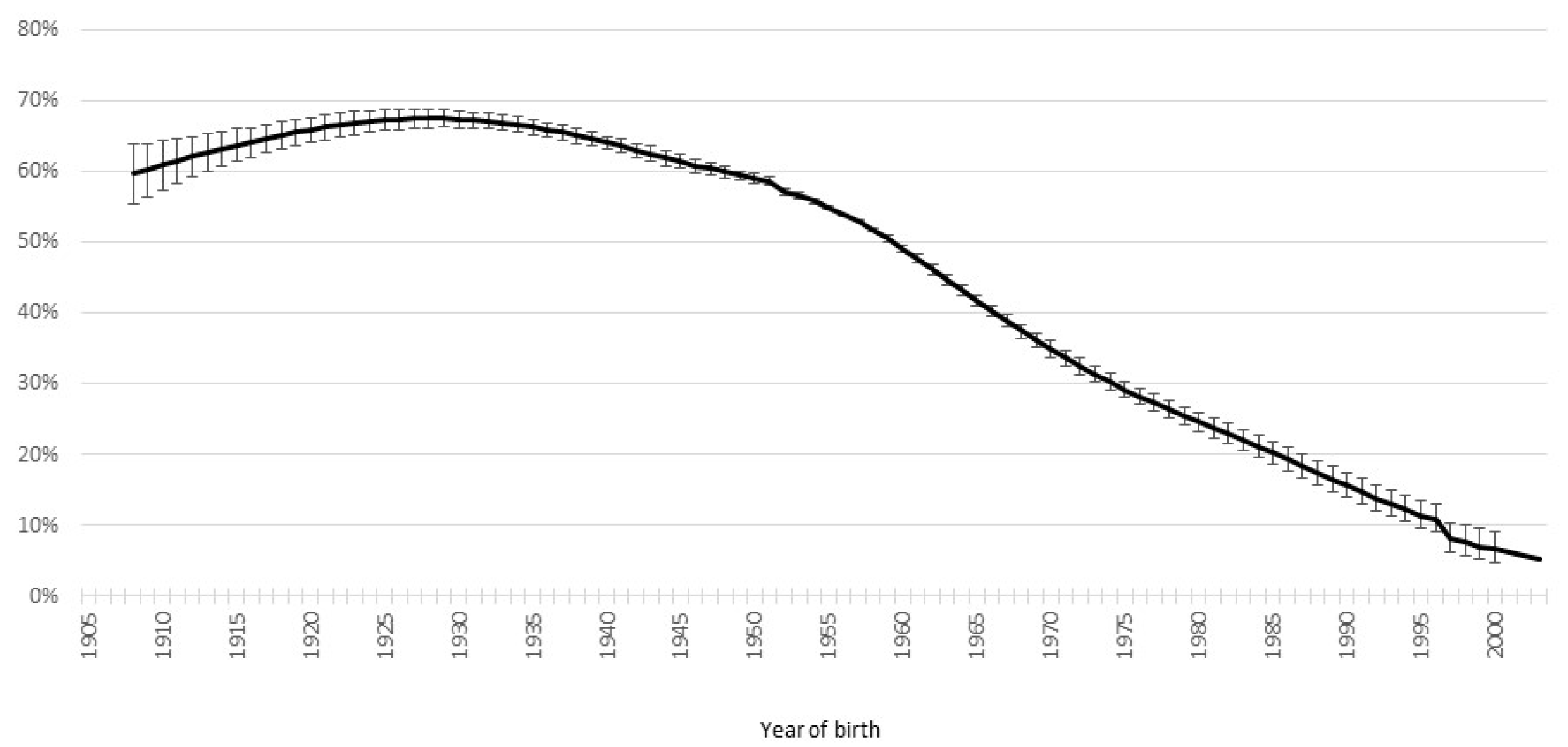
4.1. H. pylori Infection
4.2. Tobacco Smoking
4.3. Alcohol Drinking
4.4. Salt-Preserved Food
4.5. Obesity
5. Future Trends
6. Conclusions
Funding
Data Availability Statement
Conflicts of Interest
References
- Ferlay, J.; Ervik, M.; Lam, F.; Laversanne, M.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today (Version 1.1). Lyon, France: International Agency for Research on Cancer. 2024. Available online: https://gco.iarc.who.int/today (accessed on 1 July 2024).
- Parkin, D.M.; Pisani, P.; Ferlay, J. Global cancer statistics. CA Cancer J. Clin. 1999, 49, 33–64. [Google Scholar] [CrossRef] [PubMed]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Niksic, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; Esteve, J.; et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): Analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018, 391, 1023–1075. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Colombet, M.; Aitken, J.; Bardot, A.; Eser, S.; Galceran, J.; Hagenimana, M.; Matsuda, T.; Mery, L.; Piñeros, M.; et al. Cancer Incidence in Five Continents, XII (IARC CancerBase No. 19); International Agency for Research on Cancer: Lyon, France, 2023. [Google Scholar]
- Buas, M.F.; Vaughan, T.L. Epidemiology and risk factors for gastroesophageal junction tumors: Understanding the rising incidence of this disease. Semin. Radiat. Oncol. 2013, 23, 3–9. [Google Scholar] [CrossRef] [PubMed]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Personal habits and indoor combustions. IARC Monogr. Eval. Carcinog. Risks Hum. 2012, 100, 1–538. [Google Scholar]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Biological agents. IARC Monogr. Eval. Carcinog. Risks Hum. 2012, 100, 1–441. [Google Scholar]
- World Cancer Research Fund/American Institute for Cancer Research. Continuous Update Project Expert Report 2018. Diet, Nutrition, Physical Activity and Stomach Cancer. 2018. Available online: https://www.wcrf.org/wp-content/uploads/2021/02/stomach-cancer-report.pdf (accessed on 1 July 2024).
- Inoue, M. Changing epidemiology of Helicobacter pylori in Japan. Gastric Cancer 2017, 20, 3–7. [Google Scholar] [CrossRef]
- Wang, C.; Nishiyama, T.; Kikuchi, S.; Inoue, M.; Sawada, N.; Tsugane, S.; Lin, Y. Changing trends in the prevalence of H. pylori infection in Japan (1908–2003): A systematic review and meta-regression analysis of 170,752 individuals. Sci. Rep. 2017, 7, 15491. [Google Scholar] [CrossRef]
- Watanabe, M.; Ito, H.; Hosono, S.; Oze, I.; Ashida, C.; Tajima, K.; Katoh, H.; Matsuo, K.; Tanaka, H. Declining trends in prevalence of Helicobacter pylori infection by birth-year in a Japanese population. Cancer Sci. 2015, 106, 1738–1743. [Google Scholar] [CrossRef]
- Miyamoto, R.; Okuda, M.; Lin, Y.; Murotani, K.; Okumura, A.; Kikuchi, S. Rapidly decreasing prevalence of Helicobacter pylori among Japanese children and adolescents. J. Infect. Chemother. 2019, 25, 526–530. [Google Scholar] [CrossRef]
- Lim, S.H.; Kwon, J.W.; Kim, N.; Kim, G.H.; Kang, J.M.; Park, M.J.; Yim, J.Y.; Kim, H.U.; Baik, G.H.; Seo, G.S.; et al. Prevalence and risk factors of Helicobacter pylori infection in Korea: Nationwide multicenter study over 13 years. BMC Gastroenterol. 2013, 13, 104. [Google Scholar] [CrossRef]
- Park, J.S.; Jun, J.S.; Seo, J.H.; Youn, H.S.; Rhee, K.H. Changing prevalence of Helicobacter pylori infection in children and adolescents. Clin. Exp. Pediatr. 2021, 64, 21–25. [Google Scholar] [CrossRef]
- Fischbach, W.; Malfertheiner, P. Helicobacter Pylori Infection. Dtsch. Arztebl. Int. 2018, 115, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Watari, J.; Chen, N.; Amenta, P.S.; Fukui, H.; Oshima, T.; Tomita, T.; Miwa, H.; Lim, K.J.; Das, K.M. Helicobacter pylori associated chronic gastritis, clinical syndromes, precancerous lesions, and pathogenesis of gastric cancer development. World J. Gastroenterol. 2014, 20, 5461–5473. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.N.; Wang, Z.; Li, X.; Zhou, Z.G. Helicobacter pylori eradication cannot reduce the risk of gastric cancer in patients with intestinal metaplasia and dysplasia: Evidence from a meta-analysis. Gastric Cancer 2016, 19, 166–175. [Google Scholar] [CrossRef]
- Sugano, K. Effect of Helicobacter pylori eradication on the incidence of gastric cancer: A systematic review and meta-analysis. Gastric Cancer 2019, 22, 435–445. [Google Scholar] [CrossRef]
- Take, S.; Mizuno, M.; Ishiki, K.; Kusumoto, C.; Imada, T.; Hamada, F.; Yoshida, T.; Yokota, K.; Mitsuhashi, T.; Okada, H. Risk of gastric cancer in the second decade of follow-up after Helicobacter pylori eradication. J. Gastroenterol. 2020, 55, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.C.; Yuan, Y.; Forman, D.; Hunt, R.; Moayyedi, P. Helicobacter pylori eradication for the prevention of gastric neoplasia. Cochrane Database Syst. Rev. 2020, 7, CD005583. [Google Scholar] [CrossRef]
- Ladeiras-Lopes, R.; Pereira, A.K.; Nogueira, A.; Pinheiro-Torres, T.; Pinto, I.; Santos-Pereira, R.; Lunet, N. Smoking and gastric cancer: Systematic review and meta-analysis of cohort studies. Cancer Causes Control 2008, 19, 689–701. [Google Scholar] [CrossRef]
- Peleteiro, B.; Castro, C.; Morais, S.; Ferro, A.; Lunet, N. Worldwide Burden of Gastric Cancer Attributable to Tobacco Smoking in 2012 and Predictions for 2020. Dig. Dis. Sci. 2015, 60, 2470–2476. [Google Scholar] [CrossRef]
- Sasazuki, S.; Sasaki, S.; Tsugane, S.; Japan Public Health Center Study, G. Cigarette smoking, alcohol consumption and subsequent gastric cancer risk by subsite and histologic type. Int. J. Cancer 2002, 101, 560–566. [Google Scholar] [CrossRef]
- Johnson, R.D.; Horowitz, M.; Maddox, A.F.; Wishart, J.M.; Shearman, D.J. Cigarette smoking and rate of gastric emptying: Effect on alcohol absorption. BMJ 1991, 302, 20–23. [Google Scholar] [CrossRef] [PubMed]
- Ness-Jensen, E.; Lagergren, J. Tobacco smoking, alcohol consumption and gastro-oesophageal reflux disease. Best Pract. Res. Clin. Gastroenterol. 2017, 31, 501–508. [Google Scholar] [CrossRef]
- Ma, K.; Baloch, Z.; He, T.T.; Xia, X. Alcohol Consumption and Gastric Cancer Risk: A Meta-Analysis. Med. Sci. Monit. 2017, 23, 238–246. [Google Scholar] [CrossRef]
- Tramacere, I.; Negri, E.; Pelucchi, C.; Bagnardi, V.; Rota, M.; Scotti, L.; Islami, F.; Corrao, G.; La Vecchia, C.; Boffetta, P. A meta-analysis on alcohol drinking and gastric cancer risk. Ann. Oncol. 2012, 23, 28–36. [Google Scholar] [CrossRef]
- Aburto, N.J.; Ziolkovska, A.; Hooper, L.; Elliott, P.; Cappuccio, F.P.; Meerpohl, J.J. Effect of lower sodium intake on health: Systematic review and meta-analyses. BMJ 2013, 346, f1326. [Google Scholar] [CrossRef] [PubMed]
- Takachi, R.; Inoue, M.; Shimazu, T.; Sasazuki, S.; Ishihara, J.; Sawada, N.; Yamaji, T.; Iwasaki, M.; Iso, H.; Tsubono, Y.; et al. Consumption of sodium and salted foods in relation to cancer and cardiovascular disease: The Japan Public Health Center-based Prospective Study. Am. J. Clin. Nutr. 2010, 91, 456–464. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; MacGregor, G.A. A comprehensive review on salt and health and current experience of worldwide salt reduction programmes. J. Hum. Hypertens. 2009, 23, 363–384. [Google Scholar] [CrossRef]
- Howson, C.P.; Hiyama, T.; Wynder, E.L. The decline in gastric cancer: Epidemiology of an unplanned triumph. Epidemiol. Rev. 1986, 8, 1–27. [Google Scholar] [CrossRef]
- Tominaga, S.; Kuroishi, T. An ecological study on diet/nutrition and cancer in Japan. Int. J. Cancer 1997, 71, 2–6. [Google Scholar] [CrossRef]
- Ferlay, J.; Laversanne, M.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Tomorrow (Version 1.1). Lyon, France: International Agency for Research on Cancer. Available online: https://gco.iarc.who.int/tomorrow (accessed on 1 July 2024).
- Arnold, M.; Park, J.Y.; Camargo, M.C.; Lunet, N.; Forman, D.; Soerjomataram, I. Is gastric cancer becoming a rare disease? A global assessment of predicted incidence trends to 2035. Gut 2020, 69, 823–829. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Evidence Level | Risk Factor (Positive Association) | |
|---|---|---|
| Strong Evidence | Convincing/ established cause | Helicobacter pylori infection (non-cardia) Tobacco smoking |
| Probable | Body fatness (cardia) Alcoholic drinks (intake above 3 drinks or 45 g of ethanol per day) Food preserved by salting | |
| Limited Evidence | Limited-suggestive | Processed meat (non-cardia) Grilled (broiled) or barbecued (charbroiled) meat and fish Low fruit intake Low citrus fruit (cardia) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inoue, M. Epidemiology of Gastric Cancer—Changing Trends and Global Disparities. Cancers 2024, 16, 2948. https://doi.org/10.3390/cancers16172948
Inoue M. Epidemiology of Gastric Cancer—Changing Trends and Global Disparities. Cancers. 2024; 16(17):2948. https://doi.org/10.3390/cancers16172948
Chicago/Turabian StyleInoue, Manami. 2024. "Epidemiology of Gastric Cancer—Changing Trends and Global Disparities" Cancers 16, no. 17: 2948. https://doi.org/10.3390/cancers16172948
APA StyleInoue, M. (2024). Epidemiology of Gastric Cancer—Changing Trends and Global Disparities. Cancers, 16(17), 2948. https://doi.org/10.3390/cancers16172948